CONTRACEPTIVE USE AND AWARENESS - AMONG YOUNG PEOPLE IN THE EUROPEAN REGION Results from a cross-sectional survey
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION Results from a cross-sectional survey
CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Acknowledgements
We especially want to thank:
UNFPA Azerbaijan; Aysel Askerova, Azerbaijan, supporter; ACPD - Albanian Centre for Population and
Development; Hon. Pere Lopez, MP (Andorra); Women of Armenia Foundation; Pink Armenia; Yerevan State
Medical University; Hon. Petra Bayr, MP (Austria) EPF President; ÖJV - Austrian National Youth Council; Sensoa,
Belgium; Be-cause Health, Belgium; Forum Jongeren en Seksualiteit, Belgium; Master Global Health Students,
Belgium; Pimento, Belgium; Lucas Ramaut, School of Arts, Ghent; NYF - National Youth Forum of Bulgaria;
Bulgarian Association on Family Planning and Sexual Health; PaRiter, Croatia; Status M, Croatia; Organon
Czech Republic, Sexogsamfund, Denmark; University of Kopenhagen, Kai Part, Estonia; Estonian Sexual Health
Association, European Women’s Lobby, UNFPA Eastern Europe and Central Asia; Inserm, France; NCYOG
- National Council of Youth Organisations of Georgia, Association HERA XXI, Georgia; UNFPA Georgia; Anuki
Mosiashvili, youth activist, Georgia; Munich University; University Clinic Hamburg-Eppendorf; Dr Gerhard
Will, Hamburg, supporter; Paul Knapp, Hamburg, supporter; Dr Sabine Ritter, Uni Bremen; Lili Steffen - youth
activist, Germany; DSW - Deutsche Stiftung Weltbevoelkerung; Mr. Adreas Dounis , Socialpolicy.gr, Greece; Mr.
Nikos Dedes, President of ‘Positive Voice’, Association of People Living with HIV, Greece; Prof Dimitra Kogidou,
President of the Gender Equality Committee of the Aristotle University of Thessaloniki (AUTH); Ms. Evgenia
Kavvadia, Diotima - Centre for Gender Studies and Equality, Greece; Ms Paraskeva Dimitra - Hellenic Center
for Disease Control and Prevention, HIV/AIDS Surveillance”; Ms Giulia Paganelli (@evastaizitta), Italy; Mr
Matteo Di Maio (@dimaioquellogiusto), Italy; Mr Aldo Mastellone (@solodallamente), Italy; Dr Monica Calcagni
(@ginecologa. calcagni), Italy; AIDOS, Italy; Meagan O’Niel, Ireland; LJP - The National Youth Council of Latvia,
Papardes zieds, IPPF MA Latvia; Riga Stradins University; LiJOT - Lithuanian Youth Council; UNFPA Kosovo;
Luxembourg University; CNTM - National Youth Council of Moldova; State University of Medicine and Pharmacy
Nicolae Testemitanu, Moldova; Rutgers, Netherlands; University of Bergen, Norway; Health, Education and
Research Association (H.E.R.A.), North Macedonia; Foundation for Women and Family Planning FEDERA, Poland;
Hon. Joanna Scheuring-Wielgus, MP (Poland) EPF Executive Committee Member; Porto University; Hon. Lina
Lopes, MP (Portigal) EPF Executive Committee Member; Silviu Serban, Romanian All Party Parliamentary Group,
EPF Member; Sorana Toma, Romania; Ms. Stasa TKALEC, Office of Hon. Milan Brglez, MEP (Slovenia); Karolinska
Institutet, Karin Bage, supporter, Sweden; Alexandra Burovstveva, supporter, Russian Federation; Ecem
Demiroz, supporter, Türkiye; Prof Dr. Murat Gultekin, Türkiye; Salih Yüce, supporter, Türkiye; Kent University,
All Party Parliamentary Group on Sexual and Reproductive Health, United Kingdom; European Expert Group on
Sexuality Education (mailing list).
The study was conducted by Prof. dr. Kristien Michielsen,
with the support of Fiorella Farje De la Torre and Erica Selznick.
Dissemination survey : individuals and organisations.
The study was conducted with the support of Organon.
Organon didn’t have any influence on research methodology nor the results of this report.
2
CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Foreword
Access to knowledge about sexuality and contraception is a highly
relevant issue in terms of development policy. The avoidance of teenage
pregnancies with all their negative consequences and protection
against sexually transmitted diseases are of great importance for a
self-determined life.
Petra Bayr, EPF President
The new EPF study reveals that much more needs to be done.
Access to modern contraception is crucial to women’s empowerment
and fostering gender equality and I am convinced that these important
findings will contribute to our works at the European Parliament’s
Committee on Women Rights and Gender Equality.
Hon. Robert Biedroń, MEP (S&D, Poland)
Knowledge about contraceptive methods is a prerequisite for their
use. Over 60% of respondents are not aware of more innovative
contraception methods, such as implants or IUD, which are also the
most reliable methods according to the WHO.
Neil Datta, Executive Director
Educating young people on contraception ensures that they make
informed decisions on their sexual health and their bodies. But how
can we teach young people about contraception when we do not have
enough knowledge about the (long-term) side effects of certain methods
of contraception?
Maud Boey, young activist (Belgium)
Youth in Croatia knows very little about contraception - school doesn’t
even give them enough information to know how to use a condom
correctly - and that lack of knowledge is combined with the growing
culture of early, unsafe casual sex and unhealthy relationships. Our
youth needs CSE and support to develop healthy emotional and sexual
relationships.
Petra Linčić, educational expert and young activist (Croatia)
I do believe that contraception is so much more than just preventing
birth, it’s about agency, it’s about making your own mind and sticking
to it, it’s about saying what we want and getting it for ourselves. It might
be scary, but you have the possibility of making the decision. Hence,
I think that EPF study is one of the most important ones out there.
Antonina Lewandowska, sexual and reproductive rights activist (Poland)
3
CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Contents
3 Foreword
4 Contents
5 List of tables
5 List of figures
6 Introduction
9 Methodology
11 Results
11 Sample description
14 Contraceptive use
14 Overview of contraceptive use
15 Factors associated with contraceptive use
16 Factors associated with reason for contraceptive use
16 Factors associated with choice of contraceptive
17 Factors associated with reason for choosing contraceptive type
19 Contraceptive non-use
19 Overview of contraceptive non-use
19 Factors associated with contraceptive non-use
21 Potential unmet need for contraceptives
22 Knowledge and beliefs
22 Knowledge of contraceptive methods
23 Reliability of contraceptive methods
25 Beliefs regarding contraceptives
25 Knowledge on contraceptives
27 Barriers
30 Information sources
32 Conclusions
34 Call to action: Improving policies in access to contraception for young people in Europe
35 Annex 1. Tables
4
CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
List of tables
Table 1 Explanation of the colours used in the European Contraception Policy Atlas
Table 2 Division of respondents by country, ranked by number of respondents,
and by Atlas colour
Table 3 Respondents’ characteristics, by Atlas colour
Table 4 Overview of contraceptive use
Table 5 Associations between Atlas colour and reason for choosing contraceptives,
multivariate analyses controlling for respondents’ characteristics
Table 6 Reasons for not using contraceptives (N=675)
Table 8 Reasons for not using contraceptive methods, among respondents who are not gay
or lesbian and had a sexual partner at the time of the survey, by Atlas colour
Table 9 Associations between Atlas colour and assessment of reliability of contraceptive
methods, multivariate analyses controlling for respondent characteristics
Table 10 Respondents’ beliefs about contraceptives
Table 11 Respondents’ knowledge on contraceptives
Table 12 Barriers to accessing contraceptives
Table 13 Associations between Atlas colour and barriers to contraceptives mentioned
by respondents, multivariate analyses controlling for respondent characteristics
Table 14 Main information sources on contraceptives
Table 15 Average knowledge of contraceptives, by main information source
Table 16 Factors associated with contraceptive use, bivariate and multivariate
Table 17 Factors associated with reasons to use contraceptives, bivariate and multivariate analysis
Table 18 Associations between type of contraceptive used and respondent characteristics,
bivariate analysis
Table 19 Associations between reason for choosing a contraceptive method and respondent
characteristics, bivariate analysis
Table 20 Associations between reason for not using contraceptives and respondent
characteristics, bivariate analysis
Table 21 Reasons for choosing a contraceptive method, by method
Table 22 Association between knowledge of contraceptive methods and respondents’
characteristics, bivariate and multivariate analysis
Table 23 Associations between knowledge of contraceptive methods and respondents’
characteristics, bivariate analysis
Table 24 Reliability of contraceptive methods per method, by Atlas colour
Table 25 Associations between knowledge/beliefs and respondents’ characteristics,
bivariate analyses
Table 26 Associations between barriers to accessing contraceptives and respondents’
characteristics, bivariate analyses
Table 27 Barriers reported in the open question, by Atlas colour
Table 28 Associations between information source and respondents’ characteristics,
bivariate analyses
List of figures
Figure 1 EPF 2022 European Contraception Policy Atlas
Figure 2 Knowledge of contraceptive methods
Figure 3 Reliability of contraceptive methods in preventing pregnancy
Figure 4 Barriers regarding access to contraceptives, by Atlas colour
Figure 5 Main information source on contraceptives, by Atlas colour
Figure 6 Level of knowledge of contraceptive methods, by information source
5
CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Introduction
In 2020, the contraceptive pill, the world’s first commercially produced modern birth con-
trol method, turned 60 years. Since its development, a wide variety of additional contra-
ceptive methods have been marketed, which contributed substantially to ensuring wom-
en’s reproductive health and rights. Nevertheless, even today, access to modern, effective
and affordable contraception remains a challenge in Europe. The estimates on unintended
pregnancies range from 34% of pregnancies in Western Europe to 54% in Eastern Europe.1
This is linked to substantial differences in rates of contraceptive use across regions.2 Over-
all, in Europe, approximately 57% of women of child-bearing age (or their partners) use
some form of contraception (modern or traditional), ranging from 51% in Eastern Europe
to 68.5% in Northern Europe.3
Young people are a particular group when it comes to contraceptive use. The median age
of first sexual intercourse among young people in Europe is around 17–18 years,4 while the
mean age at first birth among women in the European Union has been gradually increas-
ing over the years and stood at 29.4 years in 2019.5 This means that there is a substantial
period of time during which the vast majority of young people are sexually active and do
not yet aspire to have children.
Little is known about contraceptive use among young people in Europe. Yet this group is
faced with particular challenges when it comes to accessing contraceptives. As students or
young professionals, young people often have limited financial means. This is particularly
relevant because the vast majority of European countries (72%) do not cover contracep-
tives in the national health systems for young people.6 As only 39% of European countries
have a government-supported website with comprehensive information on contracep-
tives,7 and only nine countries in the region have sexuality education programmes that can
be considered comprehensive,8 it is likely that there are information gaps concerning con-
traceptives among young European adults. This may result in misinformation and myths
generating distrust in contraceptives. Furthermore, in several European societies, the sex-
uality of unmarried young people is a taboo subject, which may be a barrier to accessing
contraceptives and also result in judgemental attitudes among health care providers.9 Even
when approving contraceptives for young people, there is evidence that health care pro-
viders may lack knowledge, in particular regarding long-acting reversible contraceptives.10
ESHRE Capri Workshop Group. 2018. Why after 50 years of effective contraception do we still have unintended pregnancy? A European perspective. Human
1
Reproduction, 33(5): 777–783. Retrieved from: https://doi.org/10.1093/humrep/dey089. Accessed: 5 September 2022.
Dereuddre, R., Van de Putte, B. & Bracke, P. 2016. Ready, Willing and Able: Contraceptive Use patterns Across Europe. European Journal of Population. 32:
2
543–573. Retrieved from: https://doi.org/10.1007/s10680-016-9378-0. Accessed: 5 September 2022.
United Nations Department of Economic and Social Affairs. 2020. World Fertility and Family Planning 2020 Highlights. New York: UN DESA. Retrieved from:
3
https://www.un.org/en/development/desa/population/publications/pdf/family/ World_Fertility_and_Family_Planning_2020_Highlights.pdf. Accessed 5 September
2022.
Ketting, E. & Winkelmann, C. 2011. Sexual health of young people in the WHO European Region. Entre Nous No. 72; Hansen, B., Kjaer, S.K., Arnheim-
4
Dahlström, L., Liaw, K., Juul, K., Thomsen, L., Frederiksen, K., Elfström, K., Munk, C. & Nygård, M. 2019. Age at first intercourse, number of partners and sex-
ually transmitted infection prevalence among Danish, Norwegian and Swedish women: estimates and trends from nationally representative cross-sectional
surveys of more than 100 000 women. Acta Obstetrica et Gynecologica Scandinavica 99(2): 175–185; Dierckens, M., De Clercq, B. & Deforche, B. 2019. Studie
Jongeren en Gezondheid, Deel 4: gezondheidsgedrag – Seksuele gezondheid en relaties.
Eurostat. 2021. Women in the EU are having their first child later. Retrieved from: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/ddn-20210224-1.
5
Accessed 5 September 2022.
European Parliamentary Forum for Sexual and Reproductive Rights. 2022. 2022 European Contraception Policy Atlas. Brussels: EPF. Retrieved from: https://
6
www.epfweb.org/node/89. Accessed: 5 September 2022.
Ibid.
7
Ketting, E., Brockschmidt, L. & Ivanova, O. 2021. Investigating the ‘C’ in CSE: implementation and effectiveness of comprehensive sexuality education in the
8
WHO European region. Sex Education 21(2).
UNFPA & IPPF-EN. 2012. Key factors influencing contraceptive use in Eastern Europe and Central Asia. Brussels: IPPF-EN.
9
Maes, I. 2017. Kennis, attitudes en praktijken van huisartsen in oost-Vlaander in verband met ‘long-acting reversiable contraceptives’ voor adolescenten.
10
Master’s thesis, Medicine, Universiteit Gent.
6
CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
The international community has long recognised that access to contraception for all is a
vital element of the development of societies and the attainment of human dignity. This
was reiterated in the 2015 United Nations Sustainable Development Goals (SDGs) – in
particular, targets 3.7 and 5.6 specifically address reproductive health and access to con-
traception – and this ambition was confirmed in the Nairobi Statement (2019), in which
governments committed to striving for zero unmet need for family planning information
and services, and universal availability of quality, accessible, affordable and safe modern
contraceptives, including for young people.
Access to contraceptives, with particular considerations for the needs of young people, should
therefore be a priority for policymakers and governments. However, this is not the case in all
European countries. The 2022 EPF European Contraception Policy Atlas evaluates 46 coun-
tries in the region on their government policies related to access to contraceptives (provi-
sion of contraceptive supplies, including for young people), access to counselling for family
planning, and the availability of government-supported online information on contraception.
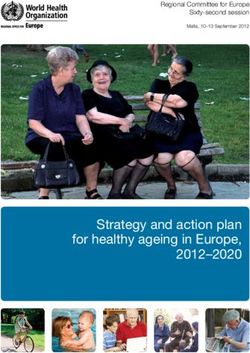
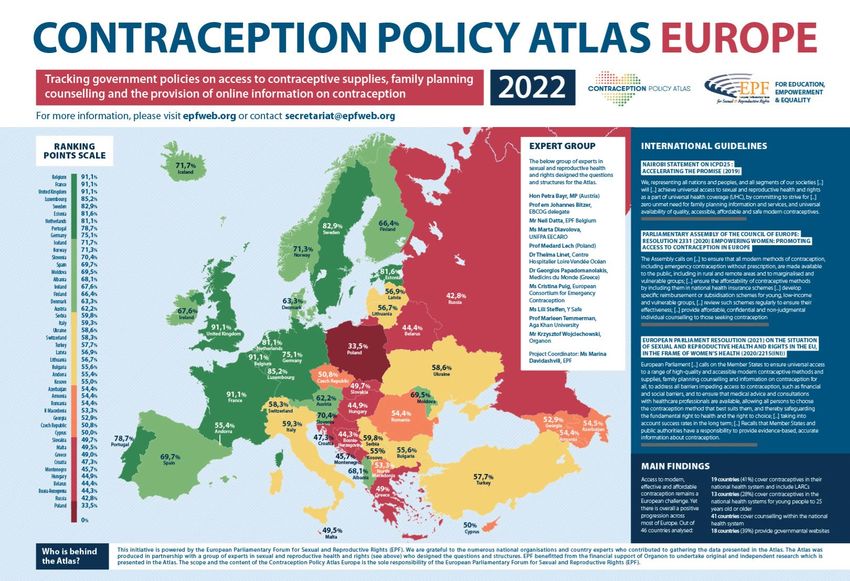
Categorising countries by colour the Atlas displays their rankings visually, with dark green
countries scoring highest in terms of policies supporting access to contraceptives, followed
by light green, yellow, orange, light red and dark red. The Atlas (Figure 1) provides a visual
demonstration of the disparities in contraceptive provision and accessibility across the region.
Figure 1: EPF 2022 European Contraception Policy Atlas
The dark green countries provide general reimbursement schemes for contraceptive sup-
plies, and specific reimbursements for young people, and women with low income. Fur-
ther, the State provides free counselling for family planning. With each colour change, the
services of the State diminish. For example, in the yellow countries, there is only minimal
or no reimbursement for the general population for contraceptive supplies, and no reim-
bursement for vulnerable groups (except in Ukraine). However, they score high on pro-
viding counselling. The countries in the red category provide no reimbursement for the
general population for supplies (except Andorra), and no reimbursement for vulnerable
groups (except Andorra). Further, they receive an average score on providing counselling.
7
CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
There are also vast differences in the provision of online information on contraceptives.
In the countries in the dark green category there is a website about contraception that is
provided by the public authority and there are two types of them. For instance, in the Unit-
ed Kingdom it is an integrated part of the general health website provided by the National
Health Service. In contrast, in Belgium and in France there are special websites dedicated
only to contraception, also provided by the State. In the yellow countries there are web-
sites provided by state or non-state actors, but they are not comprehensive – for example,
they do not provide information about where to get contraception and how much it costs.
Countries in the red category have no dedicated general websites on contraceptives.
Table 1: Explanation of the colours used in the European Contraception Policy Atlas
Very good Good Medium Poor Very poor Exceptionally
(>75%) (60–75%) (55–60%) (50–55%) (
CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Methodology
Study design. This is a cross-sectional study among young people (18–30 years) in countries
of the European Region.
Geographical region. The study collected data across the wide European Region. The
following countries were included: Albania, Andorra, Armenia, Austria, Azerbaijan,
Belarus, Belgium, Bosnia and Herzegovina, Bulgaria, Croatia, Cyprus, Czech Republic,
Denmark, Estonia, Finland, France, Georgia, Germany, Greece, Hungary, Iceland, Ireland,
Italy, Kosovo, Latvia, Liechtenstein, Lithuania, Luxembourg, Malta, Monaco, Montenegro,
Moldova, Netherlands, North Macedonia, Norway, Poland, Portugal, Romania, Russian
Federation, San Marino, Serbia, Slovak Republic, Slovenia, Spain, Sweden, Switzerland,
Türkiye, Ukraine, United Kingdom.
At the same time, a few countries are particularly targeted to allow for country-level data
analysis: Belgium, Germany, Greece, Italy and Romania.
For the analysis, the countries were regrouped according to collapsed categories of the
2022 European Contraception Policy Atlas (further referred to as ‘Atlas colours’):
Dark and light green: Albania, Austria, Belgium, Denmark, Estonia, Finland, France,
Germany, Iceland, Ireland, Luxembourg, Moldova, Netherlands, Norway, Portugal,
Slovenia, Spain, Sweden, United Kingdom
Yellow: Andorra, Bulgaria, Italy, Kosovo, Latvia, Lithuania, Serbia, Switzerland,
Türkiye, Ukraine
Orange: Armenia, Azerbaijan, Cyprus, Czech Republic, Georgia, North Macedonia,
Romania
Light and dark red: Bosnia and Herzegovina, Croatia, Greece, Hungary, Montenegro,
Poland, Russian Federation, Slovak Republic
Population. The target population of the study are young people aged 18–30 years.
Language. The survey was available in the following languages: Arabic, Dutch, English,
French, German, Greek, Hungarian, Italian, Polish, Romanian, Russian, Spanish and Turkish.
Duration. The survey was short and took approximately 5 minutes to complete. It was
implemented in July and August 2022.
Topics. The following topics are included in the survey:
• Socio-demographic and socio-economic situation
• Sexual orientation and relationships
• Contraceptive use
• Contraceptive knowledge and awareness
• Contraceptive attitudes
• Information sources related to contraceptives
No identifiable information was collected.
9
CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Data collection. We used KoboCollect software to collect the data and convenience
sampling to recruit potential participants. We disseminated the link to the online survey
through networks and partners in the different European countries.
Analysis. The analysis took place in three steps:
• Univariate: First we developed descriptive tables for all variables.
• Bivariate: Subsequently, we did bivariate analyses for the key outcome
variables (contraceptive (non-)use, knowledge, reliability, beliefs, barriers and
information sources) to study associations with respondents’ characteristics
(socio-demographic characteristics, socio-economic characteristics, current
partner and sexual orientation). We used different tests depending on the type of
variable (Chi-square tests, t-tests or Kruskal Wallis H Test) to determine whether
the associations were statistically significant.
• Multivariate: Finally, for each of the key outcome variables (contraceptive (non-)
use, knowledge, reliability, attitudes, barriers and information sources), we did a
multivariate regression analysis, with the key outcome variable as the dependent
variable and the respondents’ characteristics as independent variables. This
allowed us to determine whether Atlas colour was significantly associated with
the outcome, controlling for respondents’ characteristics.
Ethics. Before starting the survey, we informed the respondents about the objective of
the study, its duration and the expectations of the respondent. We also informed them
that the study was voluntary and that they could withdraw from it at any time, and that
their responses were being collected anonymously. Respondents had to actively consent
to participate in the study by ticking a box.
10CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Results
Sample description
Overall, 2,603 respondents who fit both inclusion criteria (aged 18–30 years old and living in
the wide European Region) participated in the study. Countries that had most respondents
were the focus countries of this study: Belgium, Germany, Greece, Italy, and Romania. A large
number of countries only had a small number of respondents. Therefore, the countries were
restructured into the Atlas colour categories. The yellow and green categories of the Atlas
have the most respondents (31.5% and 30.7%, respectively), but the orange and red catego-
ries also contain a substantial number of respondents (21.5% and 16.5%, respectively).
Table 2: Division of respondents by country, ranked by number of respondents,
and by Atlas colour
Country
No. % No. %
Italy 521 20.0 Bulgaria 14 0.5
Romania 444 17.1 Georgia 14 0.5
Belgium 263 10.1 Hungary 13 0.5
Greece 192 7.4 Sweden 13 0.5
Lithuania 184 7.1 Austria 12 0.5
Germany 130 5.0 Moldova 8 0.3
Netherlands 127 4.9 Serbia 8 0.3
Croatia 107 4.1 Denmark 7 0.3
France 92 3.5 Andorra 6 0.2
Poland 78 3.0 Czech Republic 5 0.2
Latvia 60 2.3 Cyprus 4 0.2
Armenia 44 1.7 Bosnia and Herzegovina 3 0.1
Russian Federation 32 1.2 Finland 3 0.1
United Kingdom 31 1.2 Kosovo 3 0.1
North Macedonia 26 1.0 Luxembourg 3 0.1
Spain 25 1.0 Slovak Republic 3 0.1
Albania 24 0.9 Estonia 2 0.1
Switzerland 22 0.8 Slovenia 2 0.1
Norway 21 0.8 Türkiye 2 0.1
Portugal 19 0.7 Iceland 1 0.0
Azerbaijan 18 0.7 Montenegro 1 0.0
Ireland 15 0.6 Ukraine 1 0.0
Total 2,603 100.0
Atlas colour category
No. %
Green 798 30.7
Yellow 821 31.5
Orange 555 21.3
Red 429 16.5
Total 2,603 100.0
The overall median age of respondents was 24 years, with respondents from green and
red countries having the highest median age (25), and those from orange countries the
lowest (22). Most respondents were born in the country in which they were currently living
(88.9%), though this was substantially lower in the green category (72.2%). A significant
majority (84.9%) of respondents reported that their sex assigned at birth was female; the
11CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
red category has the most male respondents (27.3%). Four respondents reported that their
sex assigned at birth was X. Most respondents were cisgender (94.7%), which was similar
across colours. Most respondents were currently in or had completed higher education
(79.6%), with the highest proportion among respondents from green countries (87.2%).
Being a student was the most commonly reported main occupation (46.1%), followed by
being employed (42.5%). The socio-economic status of respondents differs substantially,
with substantially more of those from the green countries than those from the other coun-
tries reporting that it is (very) easy for them to cover their daily needs with the financial
means they have available (63.2%). Most respondents do not consider themselves to be
religious (66.5%), with the highest proportion of non-religious respondents coming from
green countries (76.9%), and the lowest from the orange countries (59.6%).
Table 3: Respondents’ characteristics, by Atlas colour
Living Sex
Education
Age in country assigned Gender
level
of birth at birth
Secon Advanced College
Primary
Yes Female Cis dary technical or uni
education
education training versity
Median % % % % % % %
Green 25 72.2 83.3 94.9 0.5 7.5 4.3 87.2
Yellow 24 96.5 87.9 96.7 1.6 17.9 5.8 74.1
Orange 22 97.1 92.1 93.3 0.5 14.2 5.0 78.9
Red 25 95.1 72.7 92.5 0.0 16.1 6.1 77.2
Total 24 88.9 84.9 94.7 0.8 13.6 5.2 79.6
Main occupation Economic status Religiousness
Neither Not
Self- Job- Active-
Em- Stu- (Very) difficult (Very) actively
em- seek- Other ly prac No
ployed dent difficult nor easy prac
ployed ing tising
easy tising
% % % % % % % % % % %
Green 53.6 4.5 37.2 3.4 0.9 12.0 24.8 63.2 4.9 16.4 76.9
Yellow 35.9 4.4 51.6 6.1 1.2 19.0 37.0 44.0 5.2 28.9 60.2
Orange 38.0 2.0 51.9 5.2 0.9 18.0 42.9 39.1 3.6 34.1 59.6
Red 40.1 5.6 44.3 7.7 1.6 24.9 38.0 37.1 4.9 22.4 68.3
Total 42.5 4.1 46.1 5.3 1.1 17.6 34.7 47.7 4.7 25.1 66.5
Sexual orientation in four categories Current sex partner
Heterosexual Gay Lesbian Bisexual Other No Yes
% % % % % % %
Green 65.0 3.4 2.6 21.8 7.1 27.3 72.7
Yellow 75.8 5.0 0.7 12.9 5.6 24.0 76.0
Orange 68.5 0.4 1.8 21.8 7.6 35.9 64.1
Red 59.2 7.0 3.3 21.2 9.3 39.6 60.4
Total 68.2% 3.8 2.0 18.9 7.1 30.1 69.9
Over two thirds (68.2%) reported being heterosexual, with the lowest proportion coming
from red countries (59.2%), and the highest from yellow countries (75.8%). The majority of
the respondents reported they had a sexual partner at the time of the study (69.9%), while
10.9% reported never having had a sexual partner (mostly those from orange countries:
18.0%).
12CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Box 1: Limitations of the study
Limitations
Before moving to the results of the study, it is important to point out some inherent
weaknesses of this study that influence the results and need to be taken into ac-
count in their interpretation.
First, the survey used convenience sampling: the survey link was spread through
networks, partner organisations, friends and influencers. Anybody who saw the link
could decide themselves whether or not to read it, click on it and participate in the
study. This causes a double bias. First, the dissemination of the survey was done
through partners with similar rights-based views on access to contraceptives. Sec-
ond, it is also likely that those who participated in the survey have an intrinsic inter-
est in the topic. This is demonstrated, for example, by the high proportion of women
responding to the survey, compared to men. Furthermore, the respondents needed
to be literate and have internet access, thereby potentially excluding the most vul-
nerable groups. Therefore, our sample is not representative of the entire popu-
lation of young people in Europe.
A second important imitation is the grouping of the countries in Atlas colour cate-
gories. The study set out to analyse whether contraceptive policies translate into
practice – i.e. whether young people’ awareness and use of contraceptives differs
depending on the Atlas colour of the country in which they live. Therefore, the coun-
tries are grouped by colour. But, of course, contraceptive awareness and use are in-
fluenced by much more than policies alone, and there are more differences between
countries than only their policies. While our analyses took into account differences
in respondent characteristics, there are many more factors that influence con-
traceptive use and awareness that were not taken into account in the multi-
variate analyses, such as influence of the partner and friends or personal be-
liefs about contraception. This is also demonstrated by the explanatory value (R2)
of the statistical models that are reported in this study: they range between 5% and
20%, indicating that there are a number of other factors that explain contraceptive
use and awareness that are not included in the study.
Third, there are a number of countries that have a high number of respondents.
Because of their weight, they are likely to strongly influence the results from the
different Atlas colour categories.
In conclusion, the study provides interesting results and hints at associations be-
tween the policies and young people’ contraceptive use and awareness. However,
they are not representative of the entire population of young people in Europe and
should be interpreted and used with caution.
13CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Contraceptive use
Overview of contraceptive use
Seven out of ten respondents (70.7%) report currently using a contraceptive method (them-
selves or their partner), while one in four (25.9%) say they do not currently use a contracep-
tive method, and 3.4% do not know. Pregnancy prevention is by far the most commonly
reported reason for contraceptive use (91.7%), but other reasons are also reported: to
manage the menstrual cycle (22.1%) or to manage a medical condition (10.8%).
The most commonly used contraceptive method is the male condom (50.8%), followed
by the contraceptive pill (29.5%). Long-acting reversible contraceptives (LARCs), which are
considered the most reliable methods to prevent pregnancies, are rarely used by young
European adults. The Intra-uterine device (IUD) is used by 8.4% of respondents, and the
implant by 1.7%. A very small proportion of contraceptive users report relying on tradition-
al contraceptive methods such as withdrawal (2.9%) or periodic abstinence (1.0%) as their
main method of contraception.
The main reasons for choosing a specific contraceptive method are its reliability (62.1%), its
limited side effects (33.1%), its affordability (24.3%), its regulation of menstruation (20.7%)
and its lack of hormones (17.2%). Table 18 in the Annex presents the reasons for choosing
each contraceptive method separately. It shows that reliability is mostly the key reason
for choosing a modern contraceptive method, but that each method has its own specific
additional reasons.
The following sections will present the results of bivariate and multivariate analyses to
study factors associated with contraceptive use, reason for contraceptive use, choice of
contraceptive method and reason for choosing a contraceptive method.
Table 4: Overview of contraceptive use
No %
Are you or your partner using any contraceptive methods?
Yes 1,840 70.7
No 675 25.9
I don’t know 88 3.4
Which method is currently the main contraceptive method that you or your partner are using?
Diaphragm 8 0.4
Pill 543 29.5
Male condoms 934 50.8
Female condoms 5 0.3
Implant 31 1.7
Injection 5 0.3
Patch 6 0.3
Intrauterine device (IUD) 155 8.4
Calendar method (periodic abstinence) 18 1.0
Withdrawal 54 2.9
Vaginal ring 61 3.3
Male sterilisation 3 0.2
Female sterilisation 1 0.1
Other 12 0.7
I don’t know 4 0.2
14CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
No. %
Why are you or your partner using contraceptives? (up to two answers could be given)
To prevent pregnancy 1,684 91.7
To manage the menstrual cycle 406 22.1
To manage acne 58 3.2
To manage a medical condition 198 10.8
My partner requested it 29 1.6
Other 136 7.4
I don't know 4 0.2
What are the main reasons why you or your partner choose this contraceptive method?*
High reliability – It prevents against pregnancy well 1,142 62.1
Affordability – It doesn’t cost much 447 24.3
Short acting – Taken/used daily or monthly or at the time of intimacy 185 10.1
Long acting – It provides effective contraception for 3–5 years 156 8.5
Invisibility – It is easy to hide 43 2.3
Comfort – I/my partner find(s) it comfortable 321 17.4
User-friendly – I/my partner find(s) it easy to use 408 22.2
It has no/few side effects 609 33.1
Invasiveness – It does not require inserting something in the body 241 13.1
It does not require intervention from a health care provider 157 8,.5
Menstruation – It regulates, reduces or stops menstruation 381 20.7
My friends use it 15 0.8
It contains hormones 46 2.5
It is hormone-free 317 17.2
Other 50 2.7
I don’t know 23 1.3
* Up to three answers could be given.
Factors associated with contraceptive use
The bivariate analysis finds a difference in contraceptive use depending on Atlas colour:
respondents living in green and yellow countries report significantly higher contraceptive
use (79.7% and 76.6%, respectively) than those from orange and red countries (64.4% and
64.9%, respectively). The median age of contraceptive users and non-users is the same (24),
and also men and women report similar levels of contraceptive use. People who report li
ving in the country in which they were born have a lower level of contraceptive use (72.3%)
than those who were not born in the country in which they are currently living (79.7%).
There is no significant difference in contraceptive use by main occupation, education level
or religiousness. However, there is a difference when it comes to economic status, with
respondents who say that they can (very) easily cover their daily needs with the financial
resources they have available reporting a higher rate of contraceptive use. Respondents
who currently have a sexual partner are more likely to report using contraceptives (77.6%
vs. 61.7%). Heterosexual and bisexual respondents report more contraceptive use (77.8%
and 74.1%, respectively) than gay and lesbian respondents (36.6% and 17.6%, respectively).
Controlling for respondents’ characteristics in a multivariate logistic regression model, the
difference in contraceptive use by Atlas colour remains: respondents from orange and red
countries are significantly less likely to report using contraceptives than those from green
countries, controlling for all factors in the model.
The details of the bivariate and multivariate analysis can be found in Table 16 in the Annex.
15CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Factors associated with reason for contraceptive use
The reason for using contraceptives differs by colour of the country, sex assigned at birth,
education level, current sexual partner and sexual orientation. While most respondents
say that preventing pregnancy is the main reason for using contraceptives, this is re-
ported less often by respondents from red countries (87.5%) than by respondents from
other countries. This is linked to the higher proportion of gay and lesbian respondents
from those countries, and this difference does not hold when controlling for respond-
ents’ characteristics in the multivariate analysis. Respondents from green and yellow
countries are more likely than those from orange and red countries to say that managing
the menstrual cycle is among the main reasons for using contraceptives. Respondents
from yellow and red countries are more likely to use contraceptives to manage a medical
condition.
More women than men report using contraceptives to prevent pregnancy and to manage
the menstrual cycle. More men than women report using contraceptives to manage a
medical condition or because their partner requested it. Respondents who actively prac-
tise religion are more likely to report using contraceptives to manage a medical condition
than those who are not practising or non-religious. Those respondents who currently
have a sexual partner are more likely to use contraceptives to prevent pregnancy, and
less likely to use them to manage acne or a medical condition, than those without a
sexual partner. Lesbian respondents predominantly use contraceptives to manage their
menstrual cycle or acne, and gay respondents to manage a medical condition, while het-
erosexual and bisexual respondents use them more to prevent pregnancy.
In the multivariate logistic regression analysis, the differences between countries remain
for three reasons for using contraceptives:
• Menstrual cycle management: reported less by respondents from orange and
red countries than those from green countries
• Managing a medical condition: reported by more respondents from yellow and
red countries than those from green countries.
• Requested by partner: reported by more respondents from red countries than
those from green countries
The details of the bivariate and multivariate analysis can be found in Table 17 in the Annex..
Factors associated with choice of contraceptive
The type of contraceptive used varies by Atlas colour and respondent characteristics.
Respondents from green and yellow countries are more likely to report using the pill than
those from orange and red countries. LARCs are almost uniquely used by respondents
from green countries, and the vaginal ring is most popular in yellow countries. Respond-
ents from orange and red countries are more likely to use male condoms and withdrawal
as the main contraceptive method than those from green and yellow countries.
Women are more likely to report using the pill, the IUD and the vaginal ring than men, while
men are more likely to report using male condoms as the main contraceptive method. In
terms of economic status, the largest difference is in IUD use, which is reported by substan-
tially more of those reporting finding it (very) easy to cover their daily expenses (11.2%) than
16CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
those who find it (very) difficult (5.2%) or neither easy nor difficult (6.0%). At the same time,
condoms are reported by more of those who find it (very) difficult to cover their daily needs
(55.7%) than those who find it (very) easy (46.3%). Contraceptive choice also varies accord-
ing to education level: those reporting primary education as their highest education level are
more likely to report using the pill and the implant, and less likely to use condoms. Those who
are employed are less likely to report using condoms, and more likely to report using an IUD.
Those without a current partner are more likely to report male condoms (60.1% vs. 47.9%),
and less likely to report using an IUD (3.5% vs. 10.0%), than those who do have a sexual
partner. Gay respondents report only using male condoms (100%), while the majority of
lesbian respondents report using the pill (77.8%), and heterosexual respondents report a
variety of contraceptives.
Details of the bivariate analysis can be found in Table 18 in the Annex. No multivariate re-
gression analysis was done for this variable.
Factors associated with reason for choosing contraceptive type
There are several significant differences in the reasons for choosing contraceptives (for
details, see Table 19 in the Annex). For respondents from green countries, the fact that
the contraceptive method is hormone-free and long-acting is more important, while the
partner’s comfort is found to be less relevant than for respondents from other countries.
For respondents from orange and red countries, affordability is more important, while re-
ducing or regulating menstruation is less important than for respondents from green and
yellow countries.
Men are more likely to find affordability and partner’s ease of using the method more
important than women. Women find non-invasiveness, menstruation management and
the fact that it is hormone-free more important than male respondents. Those who are
employed are less likely to find affordability important, and more likely than students or
job-seekers to find long-term use of the method important. Respondents who report not
being religious find the duration of the contraception (long-acting), the lack of side effects
and the lack of hormones more important than those who report being religious. Practis-
ing religious respondents find it more important that the contraceptive method is easy to
hide than non-practising respondents and non-religious respondents.
Those with a sexual partner find reliability, long-term effectiveness, partner comfort and
lack of hormones more important than those currently without a sexual partner. Those
without a sexual partner find affordability and short-acting methods more important than
those who currently have a sexual partner. Gay respondents are more likely to find af-
fordability and not requiring medical intervention more important. Lesbian respondents
are more likely to find menstruation management and ease of use for the partner more
important factors in the choice of a contraception. Heterosexual and bisexual respondents
pay more attention to reliability, long-term effectiveness, lack of side effects and lack of
hormones in their choice of contraceptive method.
For each of the reasons for choosing a particular contraceptive method, a multivariate re-
gression analysis was done to study whether there are any differences between the Atlas
colours after controlling for respondents’ characteristics (Table 19 in the Annex). For all but
four reasons – reliability, user-friendliness, non-invasiveness and friends use it – there is
still a significant association between reason to choose a particular contraceptive method
and Atlas colour.
17CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
For the other reasons, there are significant differences between EPF colour after controlling
for respondents’ characteristics. For example, the long-acting property of the contraceptive
and the lack of hormones is less important for respondents from yellow, orange and red
countries than it is for respondents from green countries. The same respondents find the
short-acting property, the comfort and the fact that no medical intervention is needed
more important in their choice for a contraceptive method than respondents from green
countries. Other differences can be seen in Table 5.
Table 5: Associations between Atlas colour and reason for choosing contraceptives,
multivariate analyses controlling for respondents’ characteristics
Yellow Orange Red
Reliability
Affordability more more
Short-acting more more more
Long-acting less less less
Invisibility less
Comfort more more more
User-friendliness
No side effects more
Non-invasiveness
No medical intervention more more more
Menstruation management less less
Friends use it
Contains hormones more
Hormone-free less less less
The reference Atlas colour is green. Grey cells indicate that respondents from that Atlas colour report the reason significantly more than respondents
from green countries, while blue cells indicate that respondents from that Atlas colour report the reason significantly less than respondents from
green countries. White cells indicate that there is no significant difference between respondents from that Atlas colour and respondents from green
countries.
18CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Contraceptive non-use
Overview of contraceptive non-use
About one in four respondents (25.9%; 675 respondents) say they do not currently use
any contraceptive method. Respondents could indicate up to three reasons why they are
not using contraceptives. The main reasons are that the respondent is not sexually active
(40.3%), that they do not want to use hormones (27.1%), ‘other reason’ (21.3%), that they
are scared of the side effects (16.9%) and that it makes sex less pleasurable (13.8%). There
are only a few respondents who say that the reason for non-use is that they do not know
where to get contraceptives or that there is social stigma around contraceptives.
Table 6: Reasons for not using contraceptives (N=675)
Main reason for not using contraception %
I am not (regularly) sexually active (nd) 40.3
I don’t want to use hormones (nFR) 27.1
Other (nd) 21.3
I am scared of the side effects (nFR) 16.9
It make sex less pleasurable (nFR) 13.8
I am/my partner is pregnant – we are trying to have a child (FR) 7.9
I don’t know what the best method is for me / my partner (nFR) 4.9
I am or my partner is infertile/unable to have children (FR) 4.4
Prefer not to answer (nd) 3.1
I can’t afford it (nFR) 2.5
I am or my partner is sterilised (FR) 2.4
My partner objects (nFR) 2.1
I don’t know where to get contraceptives (nFR) 0.7
There is social stigma around contraceptives (nFR) 0.6
FR=fertility-related; nFR=not fertility-related; nd=not defined
The survey included an open question on the reasons for not using contraceptives. Many
respondents provided similar explanations. Half of the respondents to this question said
that they were having sex with others of the same sex. Respondents from all Atlas colours
explained that they do not use contraceptives with their partner because they are in a long-
term or monogamous relationship, with many adding that both partners have been tested
for sexually transmitted infections. In all three categories (long-term relationship, monog-
amy and tested for sexually transmitted infections), most respondents were from yellow
countries. Additionally, only respondents from yellow countries stated that although they
are not seeking to become pregnant, they would be fine with having a child, and therefore
do not use contraception. Medical reasons were another common reason for not using
contraceptives and existed across all Atlas colours, with fewest reported from red coun-
tries. A few respondents from orange and green countries wrote that they rely on tradi-
tional methods for contraception. Respondents from all regions explained they are not
sexually active, with the most coming from orange countries. Side effects were reported as
a reason for not using contraception by respondents from green, yellow and red countries.
Factors associated with contraceptive non-use
In bivariate analysis (Table 20 in the Annex), the Atlas colours are significantly associated
with several reasons for not using contraceptives. Respondents from orange countries are
more likely to report not being sexually active as a main reason for not using contracep-
19CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
tives (48.1%). Respondents from green countries are more likely to say that hormones are
the reason for non-use (38.0%). They are also more likely to say that they or their partner
are sterilised (5.7%).
Female respondents are more likely to report that they are trying to get pregnant (9.2%),
do not want to use hormones (32.2%) or are scared of the side effects (20.0%) than male
respondents (0.9% for the three reasons). They are less likely to report that their partner
objects (1.6%), that they cannot have children (3.0%) or that they or their partner are steri-
lised (1.6%) than male respondents (4.7%, 11.2% and 6.5%, respectively). Respondents who
report not being born in their country of residence are significantly more likely to report
that their partner objects to contraceptives (1.6% vs. 7.0%). Those who find it (very) easy to
cover their daily needs with their available resources are more likely to report that they are
pregnant or are trying to become pregnant (11.3%) compared to those that find this (very)
difficult (5.4%) or neither difficult nor easy (5.2%). Those who find it (very) difficult to cover
their basic needs are more likely to report that they cannot afford contraceptives (7.7%)
than those who find it neither difficult nor easy (2.0%) and those who find it (very) easy
(0.7%). Students (58.2%) and job-seekers (46.3%) are more likely to report that they are not
regularly sexually active as a reason for non-use of contraceptives. Students are less likely
to say that they do not want to use hormones (19.2%). Those who are employed are more
likely to report that they are (trying to get) pregnant (14.3%). Those who are currently in
or have completed college/university are less likely to say that not being regularly sexually
active is the main reason for non-use of contraceptives (35.7%). Those who indicate that
primary education is their highest level of education are more likely to report that their
partner objects to contraceptives (33.3%). Respondents who are actively practising religion
are more likely to say that they are (trying to get) pregnant (21.1%) or that they do not know
where to get contraceptives (5.3%) than those who are not practising (10.0% and 1.2%, re-
spectively) or non-religious (5.9% and 0.2%, respectively). Those who are not practising are
more likely to report that they are not regularly sexually active (51.2%) compared to those
who are practising religious (31.6%) or non-religious (36.1%).
Those who do not have a current sexual partner are less likely to indicate the following as
reasons for non-use of contraceptives: trying to have children (0.0%), do not want to use hor-
mones (15.6%), do not know what the best method is (2.6%), being scared of side effects
(12.6%), objection from partner (0.4%), unable to have children (2.2%), partner is sterilised
(1.1%) and making sex less pleasurable (4.5%) – compared to those with a sexual partner
(13.1%, 34.7%, 6.4%, 19.7%, 3.2%, 5.9%, 3.2% and 20.0%, respectively). They are more likely
to report not being regularly sexually active as the main reason for non-use of contraceptives
(85.1% vs. 10.6%). Heterosexual and bisexual respondents are more likely to indicate the fol-
lowing reasons for non-use of contraceptives: not being regularly sexually active, trying to get
pregnant, do not want to use hormones and being scared of side effects. They are less likely
to report that they cannot have children and that they or their partner are sterilised.
The multivariate logistic regression analysis, which controls for respondents’ character-
istics, shows that there is still a significant association between Atlas colour and several
reasons for non-use of contraceptives:
• (Trying to become) pregnant: less reported by respondents from yellow and
red countries compared to respondents from green countries
• Don’t want to use hormones: less reported by respondents from yellow, orange
and red countries compared to respondents from green countries
• Partner objects: more reported by respondents from yellow countries com-
pared to respondents from green countries
20CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
• Not able to have children: more reported by respondents from yellow coun-
tries compared to respondents from green countries
• Being sterilised: less reported by respondents from yellow and red countries
compared respondents from to green countries
• Makes sex less pleasurable: more reported by respondents from red countries
compared to respondents from green countries
For the following reasons there is no significant differences between Atals colour after
controlling for respondents’ characteristics: not regularly sexually active, cannot afford it,
don’t know where to get it, don’t know best method, scared of side-effects, social stigma
on contraceptives.
Potential unmet need for contraceptives
Overall, 44.9% of non-users report at least one reason for non-use that is fertility related,
and 14.5% report at least one reason that is not fertility related. If we analyse the subgroup
of respondents who are not gay or lesbian and who currently have a sexual partner – i.e.
those who can get pregnant – 64.2% report at least one reason that is not fertility related,
and 21.4% report at least one reason that is fertility related.
Controlling for respondents’ characteristics, respondents from yellow countries are less
likely than respondents from green countries to report fertility-related reasons for not us-
ing contraception.
Table 8: Reasons for not using contraceptive methods, among respondents who are not gay or
lesbian and had a sexual partner at the time of the survey, by Atlas colour
Reasons for Reasons for
not using contraceptives not using contraceptives
that are not fertility related that are fertility related
% %
Green 62.2 33.8
Yellow 69.3 18.8
Orange 66.3 14.1
Red 55.4 21.5
Total 64.2 21.4
21CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
Knowledge and beliefs
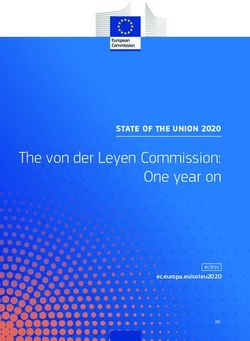
Knowledge of contraceptive methods
Knowledge of contraceptive methods was tested by one question which listed 13
contraceptive methods and asked respondents to indicate the methods they knew well
(defined as knowing what the method looks like and/or how it is used). The most commonly
used contraceptive methods are also the most known: male condoms (94.1%) and the pill
(89.0%). There are also a few methods that are known by about half of the respondents:
the IUD, male sterilisation, withdrawal and calendar method. The implant, the patch, the
KNOWLEDGE OF CONTRACEPTIVE METHODS
diaphragm and the injection are least known.
Figure 2: Knowledge of contraceptive methods
100%
80%
60%
40%
20%
0
s l D) al s nt
om Pil ion ion ho
d
om ing tch agm ction
d (IU
isat raw
isat et d a lr pla Pa hr je
con ice ril it hd ril rm ec on gin I m
ap In
ev ste ste da a i
ale d W n al V D
M ine ale ale ale m
er M m C Fe
ut Fe
ra
I nt
The mean number of contraceptive methods mentioned by respondents was 6.18, and the
median was 6 out of a maximum of 13. In bivariate analysis (Table 22 in the Annex), there was a
difference across Atlas colours in terms of knowledge of contraceptive methods. Respondents
from red countries (5.31) know fewer contraceptive methods on average than respondents
from other countries, in particular green countries (6.8). The mean score for respondents
from yellow countries is 6.09, and for respondents from orange countries it is 6.11.
Furthermore, the overall knowledge score differs significantly depending on respondents’
characteristics. Women (6.39) know more contraceptive methods on average than men
(5.02). Those with secondary education (6.09) and those currently in or who have completed
college/university (6.27) know more contraceptive methods than those with primary
education (4.15) and advanced technical education (5.49) as their highest education level.
Those with higher economic status (6.49) know more contraceptive methods than those
with low economic status (5.75). Non-religious respondents (6.49) know more contraceptive
methods than those who are religious (5.35–5.67). Those with a current sexual partner (6.30)
know more contraceptive methods than those without (5.93). Bisexual (7.12) and lesbian
(6.86) respondents know more contraceptive methods than heterosexual (5.96) and gay
respondents (5.13).
Table 23 in the Annex provides more detail on the proportion of respondents who know the
specific contraceptive methods, divided by Atlas colour and respondents’ characteristics.
22CONTRACEPTIVE USE AND AWARENESS AMONG YOUNG PEOPLE IN THE EUROPEAN REGION
For the multivariate logistic regression analysis (Table 22 in the Annex), the knowledge scale
was split into two parts: low knowledge (knowing 0–6 contraceptive methods) and high
knowledge (knowing 7–13 contraceptive methods). Several associations remain significant
in the multivariate analysis:
• Respondents from red and yellow countries have less knowledge than those
from green countries
• Bisexual respondents have more knowledge than heterosexual respondents
• Those currently in or who have completed college/university have more
knowledge than those who report primary education as their highest education
level
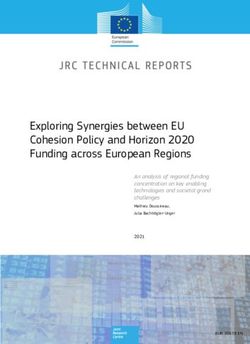
Reliability of contraceptive methods
Respondents were asked which contraceptive methods they find reliable to prevent
pregnancy. Figure 3 shows the proportion of respondents from the overall sample who find
the method reliable (light blue) and the proportion of respondents that find the method
reliable among those that know the method (dark blue). For example, a bit over 30% of
all respondents report finding the vaginal rind reliable in preventing pregnancy, and this
proportion increases to a bit over 60% of respondents if we only analyse respondents that
know the vaginal ring. There is no single contraceptive method which all respondents find
reliable. Male condoms and the pill are indicated as reliable methods by most respondents,
followed by male and female sterilisation and the IUD. Periodic abstinence and withdrawal
are rightfully considered least effective in preventing pregnancy, yet 1.9% and 4.6%,
respectively, of respondents consider them effective.
KNOWLEDGE OF CONTRACEPTIVE METHODS
Figure 3: Reliability of contraceptive methods in preventing pregnancy
% of respondents who know the method % of all respondents
Female sterilisation
Male sterilisation
Vaginal ring
Withdrawal
Calendar method
Intrauterine device (IUD)
Patch
Injection
Implant
Female condoms
Male condoms
Pill
Diaphragm
0 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
23You can also read