Come possono cambiare gli schemi alimentari nell'era post-insulinica? - Andrea Poli NFI - Nutrition Foundation of Italy, Milano
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Come possono cambiare gli schemi
alimentari nell’era post-insulinica?
Andrea Poli
NFI - Nutrition Foundation of Italy, Milano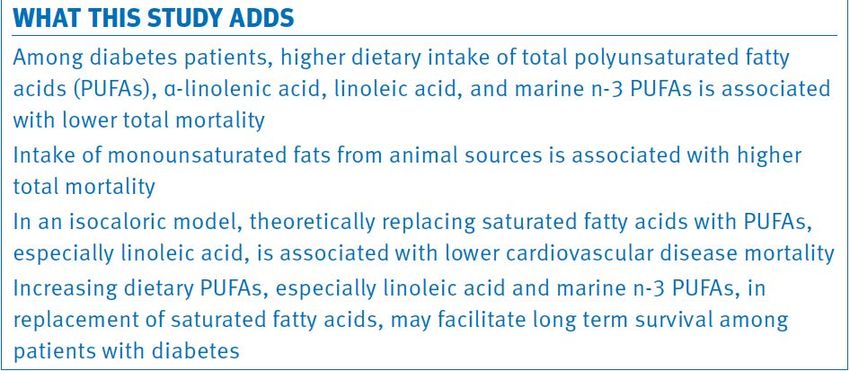
Health effects of dietary risks in 195 countries, 1990–2017:
a systematic analysis for the Global Burden of Disease Study 2017
GBD 2017 Diet Collaborators, Lancet, 2019
Recommendations for salt/sodium intake in
published guide-lines (NB: 4g Na = 10 g salt)
Source Salt (g/day) Sodium (g/day)
EFSA 2005 The available data are not sufficient to establish an upper level. It is not
possible to determine a threshold level of habitual sodium consumption
below which there is unlikely to be any adverse effect on blood pressure.
WHO 2013 5 2 Strong recommendation
WCRF/AICR 2016 5 2 Avoid salt-preserved, salted, or salty foods; preserve foods without using
salt (use refrigeration, freezing, drying, bottling, canning, fermentation).
Food Safety Authority 6 2.4 Achievable goal for the population at this time; it should not be regarded as
of Ireland 2016 an optimal or ideal level of consumption
Germany 2011, 2016 3.5-6 Adequate intake for adults: 1500 mg sodium per day.
Nordic Nutrition 6 2.4 Feasible at the population level
Recommandations
2012
Scientific Advisory 6 2.4 Recommendation
Committee on
Nutrition 2003
Dietary Guideline for 2.3 Goal for the general population; strong evidence that 'adults who would
Americans Committee benefit from blood pressure lowering should combine the DASH dietary
2015 pattern with lower sodium intake'.
AHA/ACC 2013 2.4 For lowering blood pressure; 1.5 g/day can result in even greater reduction
in BP;
IOM 2013 5.8 2.3 Tolerable upper intake level (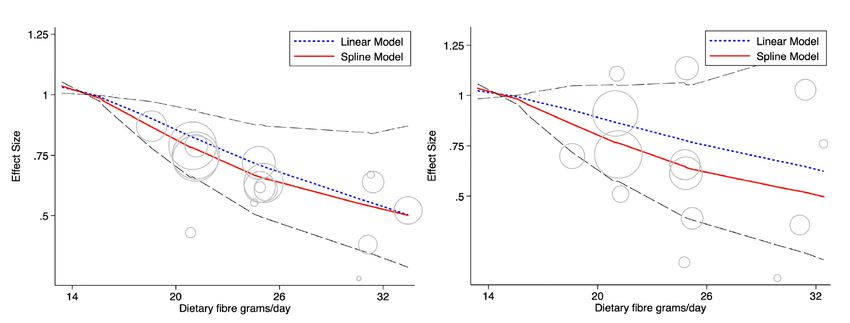
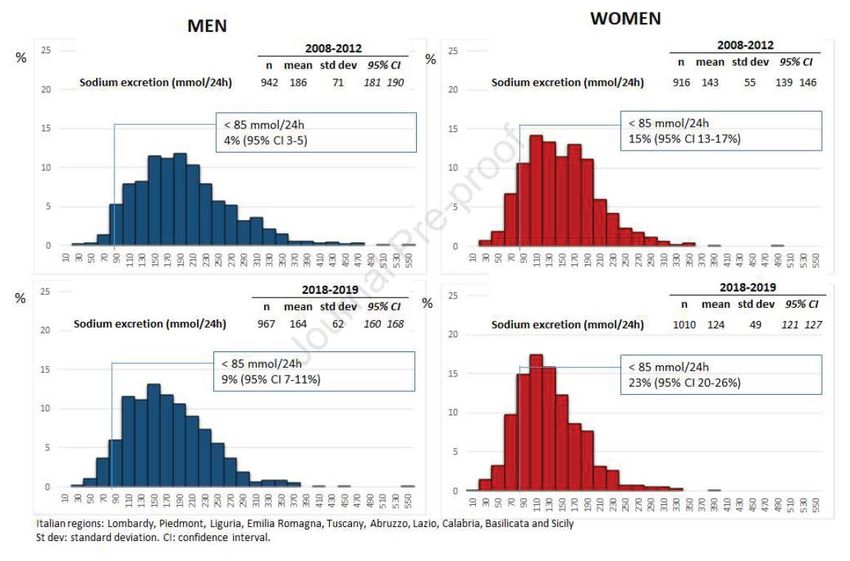
Trend of salt intake measured by 24-h urine collection in
the Italian adult population between the 2008 and 2018
(CUORE Project surveys)
10,5 g/sale 8,2 g/sale
9,5 g/sale 7,2 g/sale
Donfrancesco C et al, NMCD 2020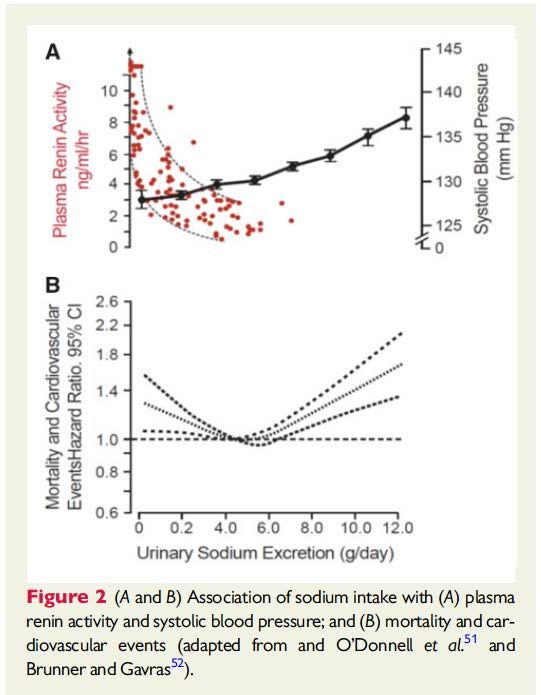
Sodium excretion, cardiovascular events and
overall mortality in subjects with and without
hypertension in the PURE Study
Risk of death and major cardiovascular events
5 g di sodio = 12,5 g di sale
Mente A et al, Lancet, 2016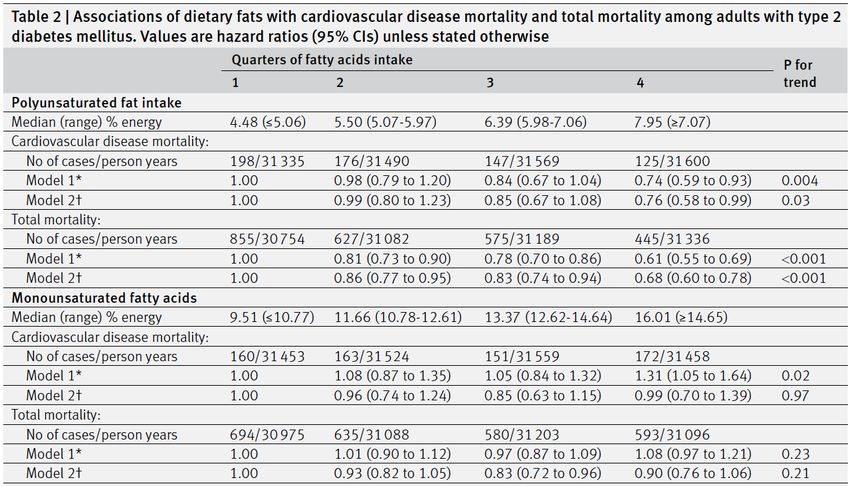
Sodium excretion, cardiovascular events and
overall mortality in subjects with and without
hypertension in the PURE Study
Risk of death and major cardiovascular events
5 g di sodio = 12,5 g di sale
Mente A et al, Lancet, 2016
Association Between Sodium Excretion, CVD
and Mortality in the Elderly: A Cohort Study
All-cause mortality
>5.4 g Na/day
3.7-5.4 g Na/day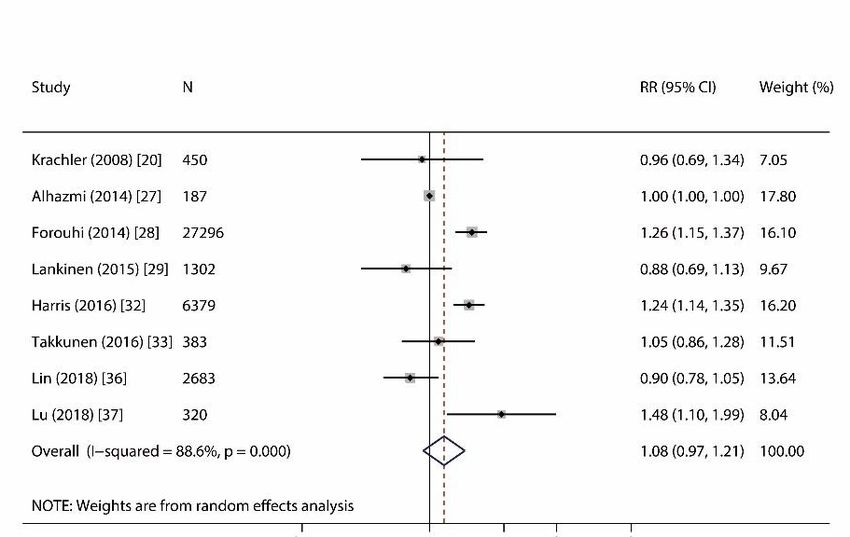
Dose-response relation between dietary sodium
and blood pressure:
a meta-regression analysis of 133 RCT
-1 mm Hg per -1 g/die di sale
-5 g/sale die
SR versus SBP effect in the upper 25th BP percentile of the population. SR versus DBP effect in the lower 75th BP percentile of the population.
1 mmol = 23 mg di sodio Graudal N et al, Am J Clin Nutr, 2019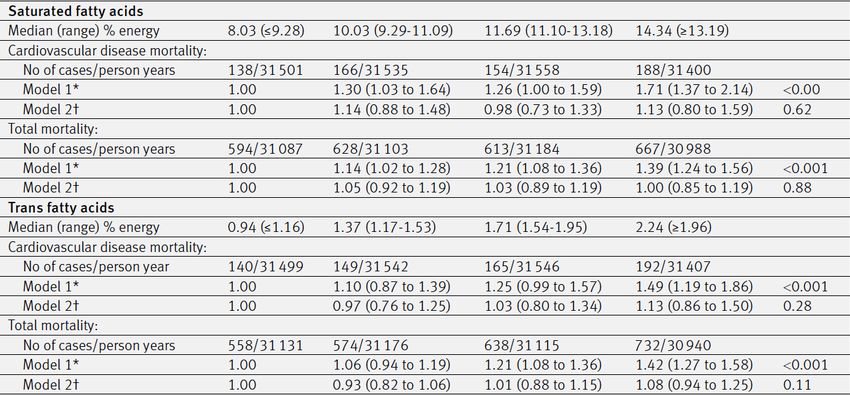
… current evidence suggests that most of the world’s population consume a moderate range of dietary sodium (2.3–4.6g/day) that is not associated with increased cardiovascular risk, and that the risk of cardiovascular disease increases when sodium intakes exceed 5 g/day. While current evidence has limitations, and there are differences of opinion in interpretation of existing evidence, it is reasonable, based upon observational studies, to suggest a population-level mean target of 5 g/day, while awaiting the results of large randomized controlled trials of sodium reduction on incidence of cardiovascular events and mortality.
Cook N et al, BMJ, 2020
Dietary total fat, fatty acids intake, and risk of cardiovascular
disease: a dose-response meta-analysis of cohort studies
Total fats
0.97 (0.93-1.01)
Zhu L et al, Lipid Health Dis 2019Health effects of dietary risks in 195 countries, 1990–2017:
a systematic analysis for the Global Burden of Disease Study 2017
GBD 2017 Diet Collaborators, Lancet, 2019Parallel declines in erythrocyte trans fatty acids
and US fatal ischemic heart disease rates
Rates of fatal ischemic heart disease in the United States between 2009 and 2016
as a function of red blood cell levels of industrially produced trans fatty acids
Sala-Vila A et al, Nutr Res 2019Average Intake of Trans Fatty Acids in Various Countries
10
8
6
4
2
0
Intake of trans fatty acids with chain lengths of 16 or 18 carbon
atoms in seven countries: assessment by chemical analysis in
1987 of diet as reported in 1960 (De Vries et al. 1997).
Zock 1997June 12th, 2014
Dietary total fat, fatty acids intake, and risk of cardiovascular
disease: a dose-response meta-analysis of cohort studies
SFA Total fats
0.97 (0.93-1.01)
0.97 (0.93-1.02)
Zhu L et al, Lipid Health Dis 2019Dietary fats and mortality among patients with type 2 diabetes:
analysis in two population based cohort studies
Polyunsaturated Fatty Acids
Monounsaturated Fatty Acids
Jiao J et al, BMJ 2019Dietary fats and mortality among patients with type 2 diabetes:
analysis in two population based cohort studies
Saturated Fatty Acids
Trans-unsaturated Fatty Acids
Jiao J et al, BMJ 2019Dietary fats and mortality among patients with type 2 diabetes:
analysis in two population based cohort studies
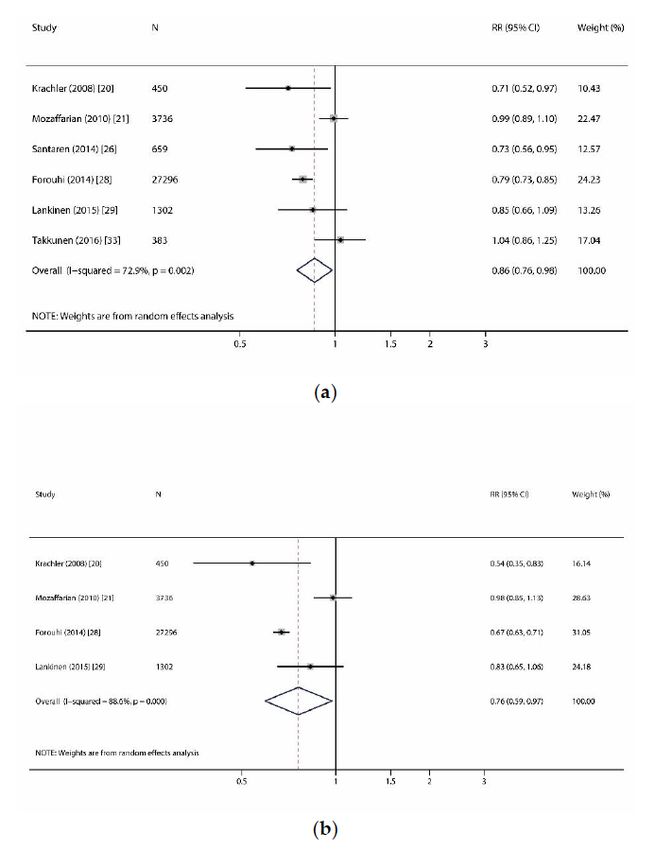
Jiao J et al, BMJ 2019Circulating Saturated Fatty Acids and Incident Type 2
Diabetes: A Systematic Review and Meta-Analysis
Milk/dairy
DNL
pentadecanoic acid (C15:0)
palmitic acid (C16:0)
heptadecanoic acid (C17:0)
Huang L et al, Nutrients 2019Fontecha J et al, Adv Nutr 2019
APOA2 - 256T>C polymorphism interacts with SFA intake to affect
anthropometric and hormonal variables in type 2 diabetic patients
Basiri MG et al, Nutr Genes 2015APOA2 - 256T>C polymorphism interacts with SFA intake to affect
anthropometric and hormonal variables in type 2 diabetic patients
Basiri MG et al, Nutr Genes 2015Olio di oliva V/EV o “normale”
Major CVD events
Guasch-Ferrè M et al, BMC Medicine 2014Olio di oliva V/EV o “normale”
Major CVD events
Guasch-Ferrè M et al, BMC Medicine 2014Polyphenol intake and all-cause mortality
risk: a re-analysis of the PREDIMED trial
-37%
Tresserra-Rimbau A et al, BMC Medicine 2014Coffee consumption and all-cause and cause-specific
mortality: a meta-analysis by potential modifiers
40 studies including 3,852,651 subjects and 450,256 all-cause and cause-specific deaths.
Kim Y et al, Eur J Epidemiol 2019Chocolate and risk of chronic disease: a systematic
review and dose response metanalysis
type 2 diabetes mellitus coronary heart disease
stroke heart failure
Morze J et al, Eur J Nutr 2019Chocolate and risk of chronic disease: a systematic
review and dose response metanalysis
type 2 diabetes mellitus coronary heart disease
Fondente
70% 25% zucchero
85% 12% zucchero
stroke heart failure
20 g 2,5-5,0 g zucchero
Morze J et al, Eur J Nutr 2019Fruit and vegetable consumption and all-cause
mortality: a dose response analysis in 71,000
swedish men and women
3 years of life less Average follow-up: 13 yrs
Frutti rossi!
Bellavia A et al, Am J Clin Nutr 2013Fresh fruit consumption in relation to incident diabetes and
diabetic vascular complications:
A 7-y prospective study of 0.5 million Chinese adults
Du H et al, PLOS 2017Dietary fibre and whole grains in diabetes
management: systematic review and metanalysis
Dietary fibre intake and all-cause (left) and CVD mortality (right) in cohorts with type 1 or type 2 diabetes
Reynolds AN et al, PLOS 2019HR for all-cause death by Tertiles of
Carbohydrate Quality Index (CQI) in the SUN study
Fernandez-Lazaro CI et al, Clin Nutr 2020Colesterolo dietetico: rispondiamo
tutti allo stesso modo?
Effetto del
consumo di 4
uova al
giorno per 4
settimane,
sui lipidi e le
LPs, in
volontari IS,
IR ed OIR
IS IR OIR IS IR OIR
Knopp, ATVB, 2003Eggs, CVD, diabetes and all-cause mortality
Guo J et al, Eur J Nutr 2017Conclusioni La nutrizione attraversa una fase molto complessa Le associazioni statistiche rilevate negli studi osservazionali sono soggette ad una rilettura critica molto attenta, che riserva sorprese importanti (sodio, saturi, carne rossa…) Il dibattito scientifico, che assume talvolta toni del tutto irrituali, e la «vischiosità» delle posizioni di molti nutrizionisti di rango rallentano lo sviluppo di una vera Evidence Based Nutrition Una maggiore focalizzazione sugli aspetti protettivi della dieta («positive nutrition»), rispetto a quelli meno favorevoli (specie grassi e zuccheri), prestando attenzione ad evitare l’aumento eccessivo di peso, sembra allo stato attuale, la scelta più ragionevole (anche nel diabetico?)
www.nutrition-foundation.it
You can also read

















































