Colorectal Cancer Screening Update: 2022 - Steven Itzkowitz, MD, FACP, FACG, AGAF Icahn School of Medicine at Mount Sinai National Colorectal ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Colorectal Cancer Screening Update: 2022 Steven Itzkowitz, MD, FACP, FACG, AGAF Icahn School of Medicine at Mount Sinai National Colorectal Cancer Roundtable March 16, 2022

2 Objectives
• Identify national and local CRC incidence, mortality and screening
data
• Discuss the impact of COVID-19 on CRC screening
• Review the evidence and rationale supporting clinical
recommendations for CRC screening
• Recognize common barriers to CRC screening and utilize appropriate
strategies to address those barriers
• Identify evidence-based CRC screening resources from the ACS, the
NCCRT and other organizations
3 The National Colorectal Cancer Roundtable (NCCRT)
The NCCRT is a national coalition of public,
private, and voluntary organizations dedicated to
reducing the incidence of and mortality from
colorectal cancer in the U.S., through coordinated
leadership, strategic planning, and advocacy.
The ultimate goal is to increase the use of proven
colorectal cancer screening tests among the entire
population for whom screening is appropriate.
Convene Identify Collaborate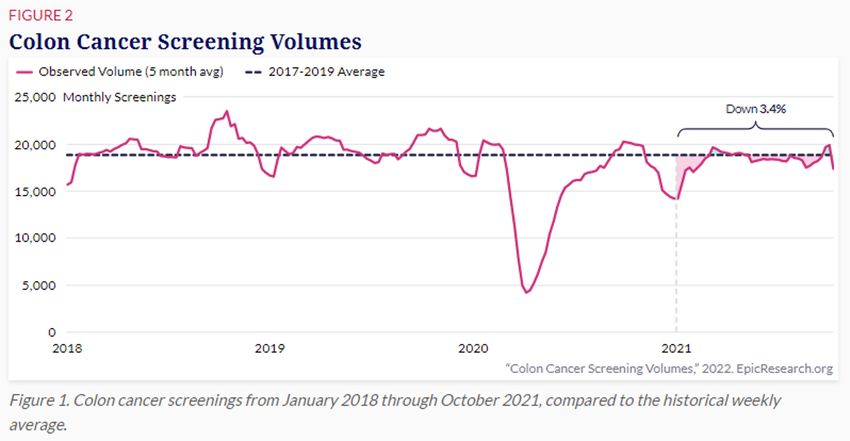
4 The National Colorectal Cancer Roundtable
History, Members, and Operations
• Co-founded by the ACS and the CDC in 1997
• Collaborative partnership of 150+ member
organizations
• Members include nationally known experts,
thought leaders, and decision makers
• Work is conducted year-round by Strategic
Priority Teams and in Special Topic Meetings
• Each year the 80% in Every Community
Conference & NCCRT Annual Meeting
addresses important topics and sets the
agenda for the following year
5 The Timeline of Two 80% Campaigns
2014 2018 2019
80% by 2018 80% in Every
Community
Dr. Howard Koh, then US
CDC data show Continue to bring down barriers and address
Assistant Secretary for
7.5 million more screening inequities so that everyone can live
Health, challenges NCCRT
people screened a life free of colorectal cancer
to take on a bold goal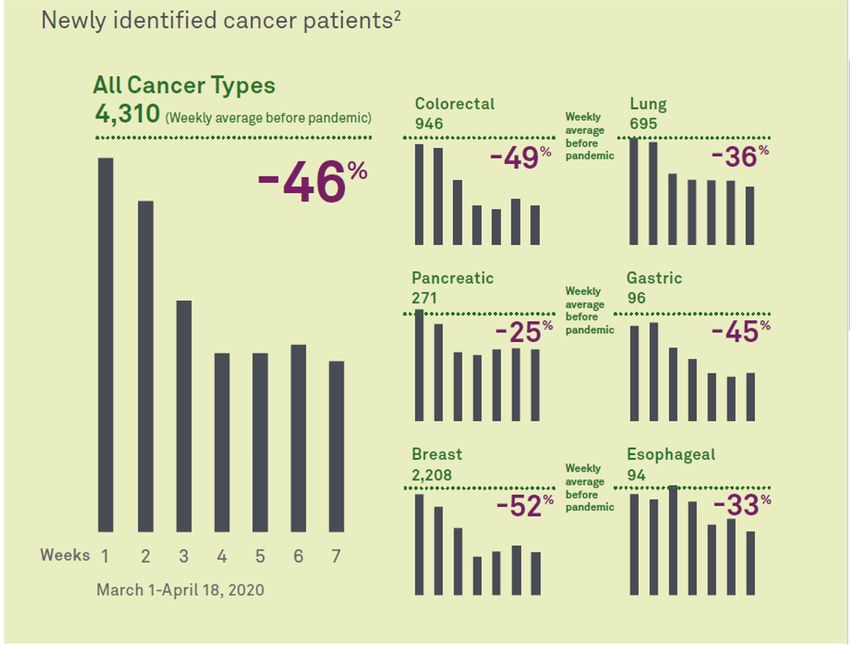
6 80% in Every Community has Widespread Support
More than 1800 organizations
have pledged their support!
• Community health centers
• Cancer centers
• Hospitals/health systems
• State cancer coalitions
• Health plans
• Employers
• Elected leaders
• And more!
7 Nebraska 80% Pledge Partners & NCCRT Awardee
• CHI Health • Lancaster County Crusade Against
• CHI Health Good Samaritan Cancer
Hospital • Methodist Endoscopy Center, LLC
• CHI Health St. Francis • Midwest Endoscopy Services, LLC
• Great Plains Colon Cancer Task • Midwest Gastrointestinal
Force Associates, PC
• Great Plains QIO:CIMRO of • Partnership for a Healthy Lincoln
Nebraska • Nebraska Cancer
• Great Plains Quality Innovation Coalition - NC2
Network
• Lakeside Endoscopy Center, LLC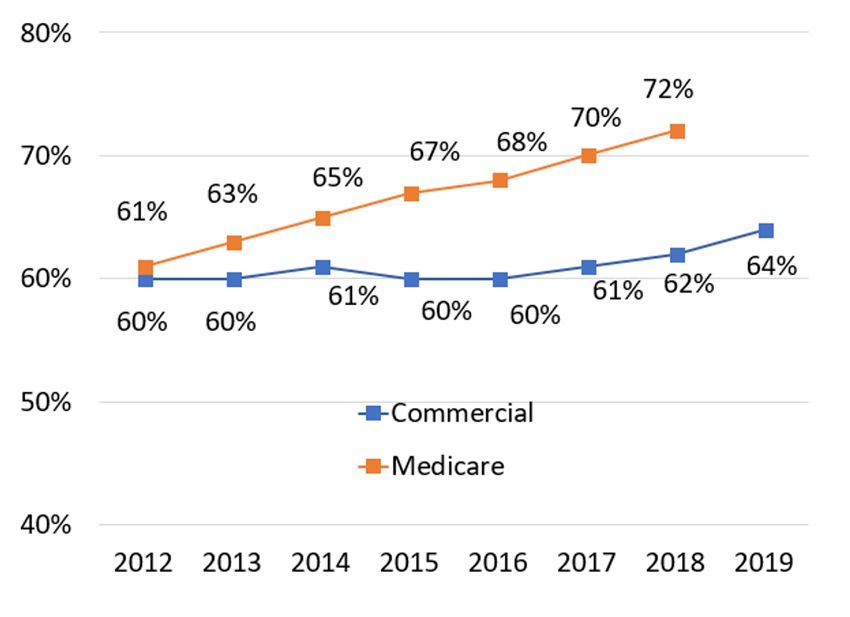
Colorectal Cancer Incidence & Mortality
9 Colorectal Cancer Burden in the U.S.
151,030 52,580 36.5 13.4
Estimated New Estimated New Incidence rates, Death rates,
Colorectal Cases in Colorectal Deaths 2014-2018* 2015-2019**
the U.S. in 2022 in the U.S. *Average annual rate **Average annual rate per
in 2022 per 100,000, age 100,000 age adjusted to
adjusted to the 2000 US the 2000 US standard
standard population population.
SOURCE: https://cancerstatisticscenter.cancer.org/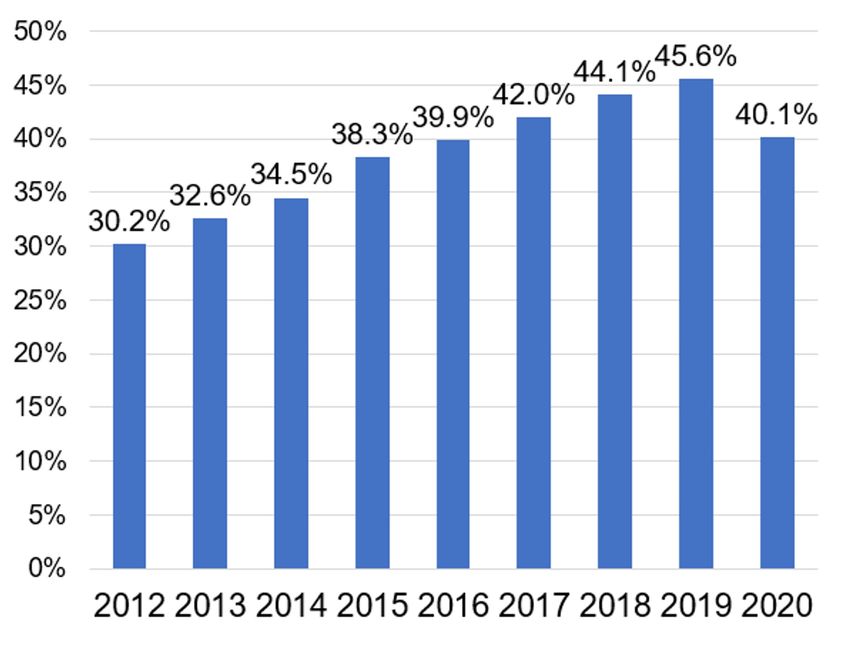
10 Incidence/Death Rates in the U.S. By Race/Ethnicity
SOURCE: https://cancerstatisticscenter.cancer.org/11 Colorectal Cancer Trends
SOURCE: https://cancerstatisticscenter.cancer.org/12 Colorectal Incidence Trends
13 CRC Incidence and Mortality Estimates, Nebraska 2022
Estimated New Cases/Nebraska 960
Estimated Deaths/Nebraska 320
SOURCE: ACS. Cancer Statistics Center. 2022. Accessed March 11, 2022. http://cancerstatisticscenter.cancer.org/#!/data-analysis/NewCaseEstimates/compare/DeathEstimates14 Nebraska CRC Incidence/Mortality (Significant Findings)
• NE incidence = 42 (2015-2019) vs US = 38 (2014-2018)
• NE incidence & mortality lower in Hispanics (2019 & 2015-2019)
• NE incidence lower in urban large (2019)
• NE mortality lower in urban large (2019 & 2015-2019)
SOURCE: Nebraska Department of Health and Human Services. NE Cancer Registry, 2015-2019. Accessed March 8, 2022.Nebraska Screening Rate: A Closer Look
There is significant variability in screening rates in Nebraska depending on
race/ethnicity, geography, and income (2020, NE BRFSS).
Race/Ethnicity Urban/Rural
Black Rural
American Indian Urb an-Small
Wh ite Urb an-Large
62% 64% 66% 68% 70% 72% 74% 76% 0% 10% 20% 30% 40% 50% 60% 70% 80%
Income
$75K
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
SOURCE: Nebraska Department of Health and Human Services. Colorectal cancer screening rates based on race/ethnicity, geography, and income. NE Cancer Registry and NE
BRFSS data, 2020. Accessed March 8, 2022.16 Personal Barriers to CRC Screening
URBAN/RURAL RURAL SPECIFIC
• Embarrassment/Discomfort • Lack of nearby clinic or screening
• Fear of finding cancer facilities or specialists
• Lack of physician recommendation • Lack of privacy as result of knowing
medical staff
• Lack of knowledge & lower level of
recognition on benefits of CRC • Lack of prevention attitude resulting
screening from rural culture
• Fear of screening test
• High cost of screening
SOURCE: Wang, H., Roy, S., Kim, J., Farazi, P., Siahpush, M., & Su, D. (2019). Barriers of colorectal cancer screening in rural USA: a systematic review. Rural and
Remote Health. https://doi.org/10.22605/rrh5181Progress Towards 80%
18 BRFSS Measures 2012 - 2020
75%
BRFSS Screening Rates
Up-to-Date (UTD) 70% 68.8% 69.7%
67.3%
66.2%
US Adults 50-75 Years 65%
65.2%
Nebraska's BRFSS CRC 60%
Screening rate for 2020
= 72.53% 55%
2012 2014 2016 2018 2020
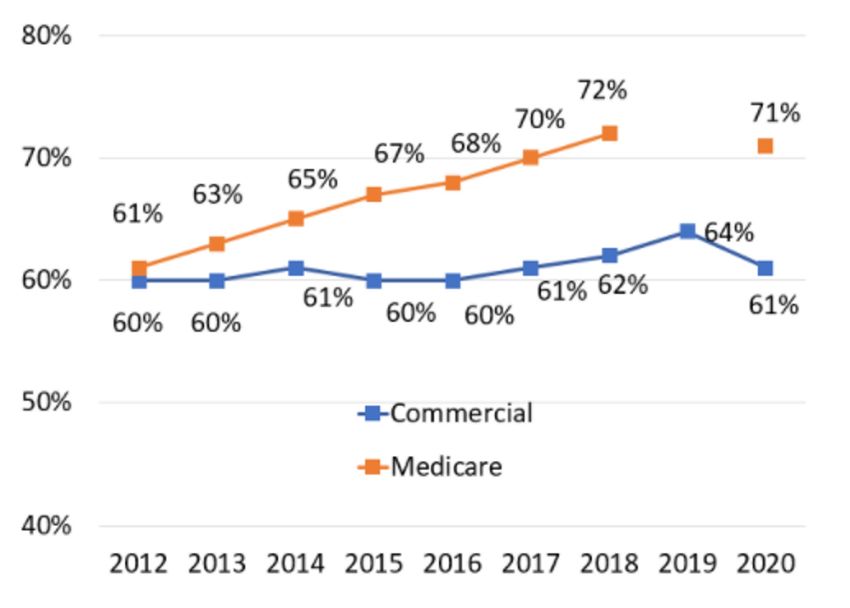
Percent of US Adults Aged 50-75 Up To Date with CRC Screening19 HEDIS Measures 2012 - 2019
HEDIS Screening Rates
Medicare and
Commercial, ages 50-75
**Screening rate data for Medicare plans is not
available for 2019 because CMS suspended Medicare
quality reporting requirements in response to
COVID-19.
**Trending caution: added required exclusion to the
Medicare product line for members 65 years of age
and older living long-term in institutional settings.20 UDS Measures 2012 - 2020
UDS Screening Rates
Up-to-Date (UTD)
U.S. Adults 50-75 Years
Percent of US Adults Aged 50-75 Up To Date with CRC Screening21 UDS Measures 2012 – 2020, Nebraska
UDS Screening Rates
Up-to-Date (UTD)
Nebraska Adults 50-75
Years
Percent of Nebraska Adults Aged 50-75 Up To Date
with CRC ScreeningCOVID-19 & Colorectal Cancer
SOURCE: https://epicresearch.org/articles/troubling-cancer-screening-rates-still-seen-nearly-two-years-into-the-pandemic
23An overall drop in cancer
diagnoses was not just due
to declines in screening, but
also to delays in diagnosis of
symptomatic cancers and
those detected incidentally
due to patients' distancing
from health services
SOURCE: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2768946SOURCE: NATIONAL CANCER INSTITUTE, https://science.sciencemag.org/content/368/6497/1290
25Colorectal Cancer Screening Guidelines
27 Screening Options
STOOL-BASED TESTS
Fecal immunochemical test (FIT) every year
High sensitivity guaiac-based fecal occult blood test
(HS-gFOBT) every year
Multi-targeted stool DNA test (mt-sDNA) every 3
years
STRUCTURAL (VISUAL) EXAMS
Colonoscopy every 10 years
CT Colongraphy every 5 years
Flexible sigmoidoscopy every 5 years28 ACS Screening Guidelines
29 Patient Preferences
Offering patients more choices can help increase the rate of CRC screening
• In a published study, only 38% of
patients that were recommended
colonoscopy got screened
• 67% of those that had FOBT
recommended were screened
• When given a choice between FOBT
or colonoscopy, 69% of patients
completed screening
SOURCE: Inadomi, Arch Intern Med 201230 Changes to Insurance Rulings on Cost-sharing
• On January 10, 2022, the U.S. Departments of Labor, Health and
Human Services, and the U.S. Treasury issued FAQs regarding
coverage of colonoscopies.
• Beginning May 31, 2022, insurance plans will be required to cover
without cost sharing, a follow-up colonoscopy performed to
evaluate a positive non-invasive stool-based screening test or direct
visualization test.
• The policy does not apply to Medicare or to non-expansion Medicaid
programs.
SOURCES:
https://www.fightcancer.org/releases/new-guidance-administration-helps-ensure-coverage-follow-colonoscopies-will-save-lives
https://www.dol.gov/sites/dolgov/files/EBSA/about-ebsa/our-activities/resource-center/faqs/aca-part-51.pdf31 Legislative Work Being Done in Nebraska
• Working with Fight CRC on policy changes for CRC screening in NE
• LB 836 – change NE statute for CRC screenings from 50 to 45
• Coupled with priority bills for Banking, Commerce and
Insurance Committee
• Awaiting final approval this session
• Continuing work on eliminating cost-sharing for follow-up
colonoscopies from positive stool testsBarriers to CRC Screening & Strategies to Overcome them
33 The NCCRT Messaging Guidebook
The NCCRT Messaging Guidebook
shares the market research
findings of tested CRC screening
messages for priority populations.
It also provides an in-depth look at
barriers to CRC screening and
strategies to breakthrough these
barriers.
nccrt.org/resource-center34 Barriers to CRC Screening
35 Barriers to CRC Screening
36 How to Break Through Barriers to CRC Screening
37 How to Break Through Barriers to CRC Screening
Procrastination is the leading barrier affecting colorectal cancer
screening.Evidence-based CRC Screening Resources
39 The NCCRT Resource Center
The NCCRT Resource Center
contains evidence-based
resources and tools to help you
increase quality colorectal cancer
screening in a range of settings
and populations.
nccrt.org/resource-center40 The NCCRT Steps Guide
The NCCRT Steps Guide
provides step-by step-
instructions to help health
centers implement processes to
reduce physician workload and
increase colorectal cancer
screening.
New version arrives in spring
2022!
nccrt.org/resource-center41 The NCCRT Clinician’s Reference
The NCCRT Clinician’s Reference
explains the different types of stool-
based tests and provides guidance
on implementing high-quality stool-
based screening programs.
nccrt.org/resource-center42 The NCCRT Risk Assessment and Screening Toolkit
The NCCRT Risk Assessment and
Screening Toolkit helps providers to
detect familial, hereditary, and early-
onset colorectal cancer.
Screening should be initiated at age 45
(or 50) for those at average risk.
nccrt.org/resource-center
42How to Get Involved
44 Take Action and Follow Us or Join Us!
• Follow us on social media
• @NCCRTnews
• #80inEveryCommunity
• Sign up to the newsletter
• Take the 80% Pledge
• Apply for NCCRT membership
nccrt.org/get-involved/45 Thank You!
nccrt.org Questions? Contact nccrt@cancer.orgYou can also read