Children's System: Aligned Home and Community Based Services (HCBS) - Authorization & Payment; Adaptive and Assistive Equipment, Vehicle ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Children’s System: Aligned Home and Community Based Services (HCBS) Authorization & Payment; Adaptive and Assistive Equipment, Vehicle Modifications, Environmental Modifications, & Non-Medical Transportation June 6, 2019
June 6, 2019 2
Introduction and Housekeeping
• Slides and recording will be posted at MCTAC.org
• Reminders:
• Information and timelines are current as of the date of the presentation
• This presentation is not an official document. For full details please refer to the provider and billing
manuals.June 6, 2019 3
Agenda
• Overview of Today’s Presentation
• Overview of the process for authorizing
• Environmental Modifications (E-MOD)
• Vehicle Modifications (V-MOD) and,
• Adaptive and Assistive Technology (AT)
• Paying for E-Mods, V-Mods and AT
• Overview of Service Descriptions (Non-Medical Transportation (NMT), EMOD,
VMOD, and, AT)
• Resources
• QuestionsJune 6, 2019 4
Overview of Today’s Discussion on E-Mods, V-Mods and AT
• Today’s webinar will review the overall process and role of the Health Home Care
Manager, Children and Youth Evaluation Service (C-YES) and Local Departments of Social
Services (LDSS) in service authorization and provisioning process for implementing
Environmental Modifications (E-Mods), Vehicle Modifications (V-Mods) and Assistive
Technology (AT).
• The process we will review today includes new elements to take into account concerns
raised from stakeholders, providers, LDSS’ and families regarding processes of E/V-Mods
• Additionally, the State wanted to ensure a consistent process was developed due to the
consolidation the previous 1915c waivers into the consolidated Children’s Waiver and the
pending Community First Choice Option (CFCO) implementationJune 6, 2019 5
Overview of Today’s Discussion on E-Mods, V-Mods and AT
• When an E/V-Mods and or AT is identified as a need for a child/youth, they are necessary
in assisting and enhancing the child’s independence in performing Activities of Daily Living
(ADLs), Instrumental Activities of Daily Living (IADLs), and/or health-related tasks and/or
will substitute for human assistance
• These E/V-Mods and or AT can make a huge impact in a child/youth and family’s everyday
living. Therefore it is important that Health Home Care Managers/C-YES, the LDSS’ and
NYSDOH work collaboratively and communicate well, so that the child/youth receive the
timely and appropriate E/V-Mods and or AT
• NYSDOH developed expedited payment processes for the LDSS so that county fiscal
implications would not delay progress regarding E/V-Mods and or AT
• NYSDOH Health Home Serving Children’s team and LTC are available to assist and work
with care managers, C-YES and the LDSSJune 6, 2019 6
Effective Timelines
• The role of the Health Home Care Manager, C-YES and LDSS described in today’s Webinar applies to all
children eligible for E-Mods, V-Mods and/or AT in the consolidated Children’s Waiver
• Effective October 1, 2019 when the Children’s Waiver HCBS including E-Mods, V-Mods, and AT become
part of the Managed Care Benefit package, children enrolled in plan will work with the plan (not the
LDSS) to arrange for these services
• These new processes will remain in effect when E-Mods, V-Mods, and AT are implemented under
Community First Choice Option, effective January 1, 2020.
• The Department has a draft April 1, 2019 Administrative Directive (ADM) which is now under final
review, that outlines the LDSS process for E/V-Mods and AT
• The Department is committed to continue to work on streamlining processes i.e. the contracting
process
NOTE: NYSDOH is tracking all EMOD, VMOD and AT requests that were being processed prior to April 1,
2019; those requests are being processed using the old payment process and pathways.June 6, 2019 7
Authorization and Payment process for
Environmental Modifications,
Vehicle Modifications and
Adaptive and Assistive TechnologyJune 6, 2019 8
Care Manager/C-YES Coordinator
• Children and youth who are enrolled in the Children’s Waiver and are getting Home and
Community Based Services (HCBS) need to have care management
• Health Homes will provide comprehensive care management services for children and youth
getting Home and Community Based Services (HCBS)
• If a child/youth and their family do not want Health Home care management and opt-out, they
can get HCBS care management from the Children and Youth Evaluation Service (C-YES)
• Health Home care managers and C-YES Coordinators assess whether the child/youth is eligible for
the Children’s Waiver and then develop a person-centered Plan of Care (POC) that would outline
the needs for E-Mods, V-Mods or AT.
• The role of the Health Home care manager and C-YES Coordinator is to assist with the
coordination of HCBS with the child/youth and family.
• The LDSS should assist the care managers and C-YES coordinators to arrange E-Mods, V-Mods and
AT identified in the POC.9
Authorization Process Part 1:
1. Identify a specific 2. Secure a 3. Assist the child/family to
assessed need for E-Mod, physician’s secure a clinical justification
V-Mod or AT service(s) and order/statement from the appropriate clinician
indicate the presented need supporting (e.g., Occupational Therapist,
in the child’s POC. the need for service Speech Language Therapist,
Driver Rehabilitation Specialist
or other licensed
professional).10 Authorization Process Part 1 (continued): 5. Explore potential 6. Collaborate with the payment sources including family and LDSS in securing 7. Submit all necessary private insurance, bids. The LDSS should help documentation to the community resources and wherever possible. LDSS other local/State/federal However, the ultimate programs prior to responsibility for obtaining requesting the Medicaid bids lies with the Care service. Manager/C-YES Coordinator.
11 Plan of Care (POC) • The POC provides an initial justification that the child can benefit from the service/adaptation/technology. • The POC will establish that the service is necessary to assist and enhance the child’s independence in performing ADLs, IADLs, and/or health-related tasks and/or will substitute for human assistance. • The HHCM/C-YES should not only identify the need in the POC but the rationale for that need and how it would impact the child/youth’s ADLs, IADLs, tasks, etc. ➢ The POC with this identified need(s) will need to be part of the submission E/V Mods and or AT submission packet to the LDSS
12 Physician’s Order The initial justification and request for service can be established by obtaining • A PHYSICIAN’S ORDER Examples: • An approved request for home care form such as the M11Q used by HRA or • Form 4539 or • a letter on physician’s letterhead stating the need for the service
13
Clinical Justification
• The clinical justification must be from the appropriate clinician (e.g., Occupational/Physical
Therapist, Home Evaluation Specialist, Driver Rehabilitation Specialist, Universal
Design/Accessibility Specialist).
• The justification must define the scope and appropriateness of the project.
• The clinician/evaluator conducts an evaluation to determine the most appropriate modification
to meet the child’s needs.
• For example, the clinician/evaluator determines
• installing a lift by the covered front stairs would be the best option for the child to fully
access the entryway
• determines that removing the bathtub and installing a roll-in shower and accessible
toilet will be the most effective option in the bathroom. The door to the bathroom will
also need to be modified to make the opening wide enough for the wheelchair to fit
through14 Clinical Justification – cont. • The clinician/evaluator completes the scope of the project detailing each part separately; this will serve as the basis of getting quotes from qualified providers. • Clinical Justifications will be included in the overall cost for the project and will be paid even if the project does not go to completion. Note: all other resources must be exhausted before seeking this service and should be documented in the request. ➢ Both of these items will be part of the submission packet to the LDSS
15
Securing Bids
Securing bids will be a collaborative effort between the family, LDSS and the Care Manager or C-
YES Coordinator. The LDSS may assist in obtaining bids, if necessary.
Bids should be based on the specifications delineated in the evaluation/clinical
assessment/project description.
The contractor must adhere to the following requirements when preparing a bid:
• Base the bid on contractor grade materials;
• Stipulate that all work will comply with applicable building and zoning codes;
• Obtain the local municipality’s permit to perform the adaptation;
• Provide verification that the work has been inspected by the local municipal branch of
government that issued the initial permit; and
• Submit verification that appropriate and adequate insurance coverage is maintained.
• All estimates must identify the costs of each component of the project e.g. inspections,
materials, permits and labor costs.16 Securing Bids – cont. The Care Manager/C-YES must secure three (3) bids If three (3) bids cannot be secured, the Care Manager/C-YES should contact the LDSS and a efforts should be documented ➢ All evaluations and bids will be part of the submission packet to the LDSS for review and approval. The LDSS will identify the preferred bid and execute a provider agreement.
June 6, 2019 17
What does the Care Manager/C-Yes Coordinator need
to send to the LDSS?
The Care Manager/C-YES Coordinator will send a Request for Service packet for submission to the LDSS.
Request for Service packet must include:
1. Child/youth’s Plan (POC) which identifies assessed need
2. Physician’s order supporting medical necessity (signed and dated)
3. Professional assessment/clinical justification identifying the scope of the project and documentation detailing
project/product specifications including scope, estimated material and labor costs and other required
expenditures
4. Bids: if the AT, E-Mod or V-Mod request costs $1,000 or more, 3 bids or justification for why 3 bids could not
be secured is required.
5. Any required documentation that is needed for the modification/service/adaptation/device such as landlord’s
permission if the home is leased or proof that a used car is less than 5 years old/less than 50,000 miles for a
V-Mod (all requirements are included in the HCBS Provider Manual).
6. Completed Clinical Justification with the description/scope of work and Cost Projection Form
The LDSS may request additional information necessary to consider the requestJune 6, 2019 18
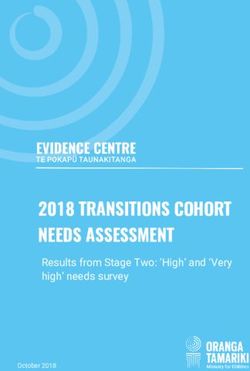
Authorization Process Part 2:
Questions &
Care Manager/C- Communication
LDSS LDSS
YES Coordinator NYSDOH
1. Select Preferred Support for/Denial
Request for Service Bid of: AT/E-Mod/V-
Packet Mod Project
2. Execute Provider Notice of
Agreement Decision (NOD)
Service Denial of Service
Authorization AuthorizationJune 6, 2019 19
LDSS Responsibility
• The LDSS is responsible for evaluating the bids and selecting the preferred vendor
to provide the service/adaptation/technology. This decision is based on an
assessment of whether the lowest responsible bid meets the assessed need of
the child.
• The LDSS will contact the selected vendor and secure a provider agreement so
that the service request may proceed upon approval by NYSDOH.
• The LDSS collects all of the documents and submits the service request to
NYSDOH for review.June 6, 2019 20
What the LDSS will send to NYSDOH
The LDSS will submit the following information to the NYSDOH:
• POC
• Physician’s order
• Professional assessment/clinical justification identifying the scope of the project and supporting
documentation detailing project/product specifications including scope, estimated material and labor
costs and other required expenditures
• Bids, with the recommended bid identified
• Provider agreement from the selected bidder
• Any required documentation that is needed for the modification/service/adaptation/device such as
landlord’s permission if the home is leased or proof that a used car is less than 5 years old/less than
50,000 miles for a V-Mod (all requirements are included in the Authorizing Guidelines).
• Completed Description and Cost Projection Form
• Justification for the need to exceed soft service limits, if applicable
Note: The Department may request additional documentation and information as needed.
• The LDSS will not submit a request to the NYSDOH if it does not support the request.June 6, 2019 21
NYSDOH Receives the Packet
• Acknowledge receipt of the request from the LDSS
• Internally track all requests
• Review the content of the service request for completeness, accuracy and costJune 6, 2019 22
What NYSDOH Provides to the LDSS
• Approval determinations are made based on all information available at the time the
service is requested. NYSDOH may request additional documentation and information as
needed.
• Upon review of the information provided, the NYSDOH will send a letter of
support/denial of the project to the LDSS.
• Upon receipt of the letter of support/denial, the LDSS will issue the Notice of Decision
(NOD) to the child/family and the Care Manager/C-YES Coordinator.
• If the NOD is for approval, the selected vendor will be notified and work will begin.
Note: All NODs are subject to Fair Hearing when requested, this process is explained to the
waiver participant/family via their Care Manager/C-YES Coordinator.June 6, 2019 23
Notice of Decision (NOD)
• A NOD is a written document that notifies the individual of an action being taken by the
LDSS, including an explanation of the reasons for the action.
• Upon making a determination about a request for services and receiving prior approval
from NYSDOH to exceed the soft limit, if applicable, the LDSS is responsible for sending a
written NOD indicating authorization, denial or a reduction of the requested service to
the individual, legal guardian (if applicable), authorized representative (if applicable) and
the individual’s Care Manager or C-YES Coordinator.
• NODs denying or reducing services must also include information regarding Fair Hearing
rights and how to apply for a Fair Hearing.
• The form used is: Notice of Decision to Authorize or Deny Assistive Technology,
Environmental Modifications, Vehicle Modifications, Community Transitional Services and
Moving Assistance.June 6, 2019 24
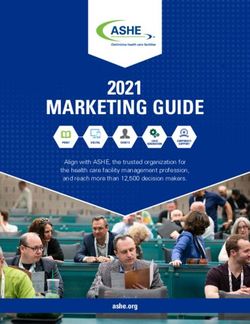
Authorization Process Part 3:
Care Manager/C-YES Child/Family
LDSS
Coordinator
Service
Authorized
E-Mod/V-Mod/AT
Provider
1. Review Bid
2. Project Initiated
3. On-site Evaluation
Final Cost Form goes to Care Manager/C-YESJune 6, 2019 25
Authorization Process
• The Care Manager/C-YES Coordinator advises the family of the decision and discusses the next
step in beginning the project, including the scope of the project and anticipated timelines.
• The Care Manager/C-YES Coordinator works with the family and the selected vendor to initiate
the project/request, including reviewing the bid and the terms of the project with the vendor.
• The provider/vendor will be responsible for the coordination of the project with the LDSS and will
provide detailed information regarding expenditures, compliance requirements and project
timelines.
• Throughout the process, the Care Manager/C-YES will work with the family and ensure their
cooperation to allow the provider/vendor/workers in the home and to be able to complete the
work
• Additionally, the Care Manager/C-YES will ensure that the work is be completed as agreed
and that the family is satisfied with the work26
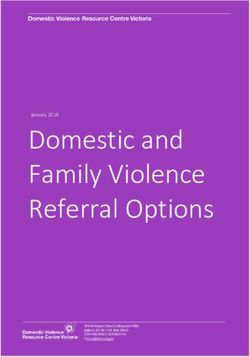
Authorization Process Part 4:
Care Manager/C-YES LDSS NYSDOH LDSS
Coordinator
Receives Final Cost from Care Approval of Final LDSS Issues Payment/Final
Final Cost Form Manager/C-YES Cost/Adjustment of Payment, if Payment to Service
necessary Provider
E-Mod/V-Mod/AT
Provider
Receives Payment
from LDSSJune 6, 2019 27
Completion of the Project
• Upon completion of the services, the Care Manager/C-YES Coordinator will
coordinate the final evaluation and complete the Final Cost Form and submit it to
the LDSS.
• The form will include a description of the completed service and the final cost.
• The LDSS must maintain the form in the child’s case file and send a copy to
NYSDOH.
• The LDSS will review the submitted form and validate the completion of the
specification of the bid/purchase.
• Once validated, the LDSS will notify the provider that they may submit a claim for
payment/invoice to the LDSS.
• The Care Manager/C-YES will provide feedback to the LDSS regarding the work
if there are any concernsJune 6, 2019 28
Service Limits
• Service limits are as follows:
• Assistive Technology - $15,000 annual calendar year limit
• Environmental Modification - $15,000 annual calendar year limit
• Vehicle Modification - $15,000 annual calendar year limit
• In all cases, service limits are soft limits that may be exceeded due to medical necessity.
If the individual’s needs cannot be met within the established limits, the LDSS may
request to exceed the limit by proving sufficient medical justification. This justification
must be submitted to NYSDOH along with the request for service packet in order to
obtain approval of the request.June 6, 2019 29
Payment for AT, E-Mods and V-Mods
Due to feedback from the LDSSs, NYSDOH recognizes that implementation of these
services requires significant time, resources and funding. NYSDOH continues to seek
alternative methods to facilitate the provision of these services and reduce the burden to
the LDSS including exploring other payment mechanisms and service providers.
Current payment options:
• Option 1: Special Project Fund Advance Requests
• Option 2: Provider Medicaid Management Information System (MMIS)
Note: Projects currently in progress for CAH participants that were previously approved by
NYSDOH continue using CAH guidelines. These projects may be billed using Schedule E
payment requests.30 Information For LDSS • See CFCO Webinar from June 5, 2019 outlining payment options https://www.health.ny.gov/health_care/medicaid/redesign/co mmunity_first_choice_option.htm
31 Where to find the forms • CFCO EMod and VMod Description and Cost Projection Form – HTML – PDF • CFCO AT Description and Cost Projection Form – HTML – PDF • Uniform CFCO AT EMod VMod CTSMA Final Cost Form – HTML – PDF NOTE: Forms will be posted soon on the Children’s Behavioral Health Webpage here: https://www.health.ny.gov/health_care/medicaid/redesign/behavioral_health/children/11 15_waiver_amend.htm
June 6, 2019 32
Overview of Service Descriptions
(NMT, EMOD, VMOD, AT)June 6, 2019 33
Core PrinciplesJune 6, 2019 34 HCBS Settings Allowable settings in compliance with Medicaid regulations and the Home and Community Based Settings Final Rule (§441.301(c)(4) and §441.710) will exhibit characteristics and qualities most often articulated by the individual child/youth and family/caregiver as key determinants of independence and community integration. Services should be offered in the setting least restrictive for desired outcomes, including the most integrated home or other community-based settings where the beneficiary lives, works, engages in services and/or socializes. While remaining inclusive of those in the family and caregiver network. Family is broadly defined, and can include families created through: birth, foster care, adoption, or a self-created unit.
June 6, 2019 35 Billing HCBS between April 1 and September 30, 2019 Children’s HCBS waiver will be billed Fee for Service (FFS) for all children enrolled in the Children’s Waiver.
June 6, 2019 36
Billing 101: beginning October 1, 2019
Medicaid Managed Care (MMC) carve in
Fundamentals
• If child in Medicaid Managed Care Plan (MMCP) – bill Managed Care Plan
• MMCPs will be required to pay government rates [aka Medicaid fee-for-service rates] for at
least 24 months from the date the service was included in the Medicaid Managed Care
benefit package, or however long NYS mandates
• In order to bill MMCP you need to be in-network
• In order to be in network you have to be credentialed and contracted
• Managed Care Plan Matrix
• All designated agencies must be enrolled as Medicaid providers agencies.
• If child not in MMCP – bill Fee-For-ServiceJune 6, 2019 37
Non-Medical TransportationJune 6, 2019 38
What is Non-Medical Transportation
• Non-medical Transportation services are available for individuals to access
authorized HCBS and destinations that are related to a goal included on the
child/youth’s Plan of Care.
• Offered in addition to any medical transportation furnished under the 42 CFR
440.17(a) in the State Plan.
• Examples where this service may be requested include transportation to: HCBS that
a child/youth was determined eligible to receive, a job interview, college fair, a
wellness seminar, a GED preparatory class, etc.June 6, 2019 39 Non-Medical Transportation Health Home Care Manager Role • If the HHCM determines there is a need for Non-medical Transportation to support an individual’s identified goals, the HHCM will include justification for this service within the Person-Centered Plan of Care (POC). The HHCM should, at a minimum, list the goal from the POC; the specific activity, support, or task; the service provider (if applicable); and the start and end date along with their contact information if needed for clarification. • After completing the Plan of Care and the Grid, the HHCM will send these to the MCO if the child or youth is in Medicaid Managed Care. The MCO is responsible for approving the Person-Centered Plan of Care and for forwarding the completed Grid to the Department of Health’s Medicaid Transportation Manager. If the child/youth is not yet in a Medicaid Managed Care plan, the HHCM will send the Grid and POC directly to Department of Health’s Medicaid Transportation Manager for review. • The HHCM will complete the “NYS DOH Plan of Care Grid for Non-Medical Transportation for Children's Home and Community Based Services (HCBS)” ( known after as “Grid”) with all known information regarding the member and their trip request. • It is possible that the complete trip destination details may not be known (e.g. exact appointment time and date). This information can be provided by the enrollee to the Transportation Manager but at least 72 hours in advance of the appointment date prior to requesting transportation.
June 6, 2019 40 Non-Medical Transportation C-YES Coordinator Role • For individuals not enrolled in a Health Home, Children and Youth Evaluation Service (C-YES) Coordinator will work with the individual and their family to determine if there is a need for Non-medical Transportation and, if so, develop the individual’s Person-Centered Plan of Care (POC) with goals that are directly linked and/or supported by Non-medical Transportation. • The C-YES Coordinator will also be responsible for completing the Grid based on the individual’s Plan of Care and forwarding the Grid and POC to the Transportation Manager. • The Grid will include documentation for Non-Medical Transportation, including documentation of which goals in an individual’s Plan of Care directly supported by the trips.
June 6, 2019 41 Non-Medical Transportation C-YES Coordinator Role • C-YES Coordinators are responsible for conducting and developing the Person-Centered Plan of Care (POC). If a need for Non-medical Transportation to support an individual’s identified goals is determined by the member with their family and C-YES Coordinator, the justification for this service within the Person-Centered Plan of Care (POC). The C-YES Coordinator will complete the “NYS DOH Plan of Care Grid for Non-Medical Transportation for Children's HCBS” (Grid) with all known information regarding the member and their trip request. • If the complete trip destination details are not known at the time of the Grid’s completion (e.g. exact appointment time and date), this information can be provided by the enrollee to the Transportation Manager but at least 72 hours in advance of the appointment date prior to requesting transportation.. • The C-YES IE should, at a minimum, list the goal from the POC; the specific activity, support, or task; the service provider (if applicable); and the start and end date and the C-YES Coordinator contact information for clarification if needed. After completing the Plan of Care and the Grid, the C-YES Coordinator will send it to the MCO if the child or youth is in Managed Care.
June 6, 2019 42 Managed Care Organization (MCO) Roles • The MCO is responsible for approving the Person-Centered Plan of Care and for forwarding the completed Grid to the Department of Health’s Medicaid Transportation Manager. • If the child/youth is not yet in a Managed Care plan, the C-YES IE or HHCM will send the Grid directly to Department of Health’s Medicaid Transportation Manager for review .
June 6, 2019 43 NMT-Transportation Manager Roles • The Transportation Manager is responsible for authorizing transportation services in accordance with Medicaid policy, by approved Medicaid Transportation providers, and as supported on the MCO-provided Grid. • Once the Grid is received the Transportation Manager should assume that the transportation been reviewed, approved and in the individual’s Plan of Care • The Transportation Manager is responsible for ensuring adherence to the guidelines below for Non-Medical Transportation, which include assigning the most medically appropriate, cost-effective mode of transportation. Enrollees have freedom of choice regarding the transportation provider within the assigned mode (e.g. ambulette, taxi, public transportation, etc.). • The Transportation Manager will provide a monthly report of Non-Medical Children's Waiver trips in a format requested by the Department.
June 6, 2019 44
Minor Children and the Use of Escorts
• A minor child is defined as an individual under the age of 18 who has not been emancipated.
Minor children who are unemancipated will not be transported by Non-medical Transportation
unless they are accompanied by an adult escort.
• The Children’s HCBS Non-medical Transportation Grid provides a place to indicate if a member
is a minor requiring an adult escort to accompany them on their Non-medical Transport trips.
The Grid also provides a place for contact information of the HHCM, C-YES Coordinator, or
MCO CM who completed the Grid so the Transportation Manager may seek additional
information if needed prior to the trip.
• The adult escort accompanying the child/youth on the Non-medical Transport is not billed for
transport but considered billed as one with the child/youth as long as the adult escort and the
child/youth are transported together at all times. The adult escort does not have to be related
to the child/youth to accompany them on the non-medical transport trip, however the adult
escort must be 18 years of age or older to qualify as an adult escort. The verification of the
proposed escort as being of adult age( defined as being at or over 18 years of age at the time
of the trip) must be done prior to the service trip by the HHCM or C-YES Coordinator.June 6, 2019 45
Minor Children and the Use of Escorts:
Emancipated youth
• For those youth who are under the age of 18, but who are self-consenting due to pregnancy,
being a parent, being married, or who are declared emancipated youth by the court system,
may use Non-medical Transportation without an accompanying adult escort. Both the POC
and Children's’ Transportation Grid should indicate specifically that although the youth
member is under age, they are able to travel without an accompanying adult escort. The Grid
has a place to indicate a youth needs to be accompanied or not. In the case of an
emancipated youth, the Grid would be marked for a member who travels unaccompanied.
The Transportation Manager may confirm the youth’s status with the HHCM, C-YES
Coordinator, the member, or family prior to any trip request for clarification.
• In the case of a minor parent who is traveling on NMT with their own minor children, the
minor parent is considered an emancipated youth as long as they are self-consenting under
Health Home or C-YES guidelines, as stated on their POC, and their Transportation Grid
indicates they are to travel as an unaccompanied minor for NMT trips. In this example, the
minor parent would be the escort for their children on the NMT transport trip.June 6, 2019 46
Limitations and Exclusions
• Generally, the same rules used to determine reimbursement of trips to medical appointments should be
followed when considering reimbursement of non-medical trips for eligible participants.
• Only those services not reimbursable under the Community First Choice Option (CFCO) State Medicaid
Plan will be reimbursable under the HCBS Waiver.
• The following guidelines apply to Non-Medical Transportation:
• Transportation must be tied to a goal in the Plan of Care.
• Transportation is available for a specified duration
• Individuals receiving residential services are ineligible for Non-Medical Transportation.
• Use transportation available free of charge.
• Use the most medically appropriate, cost effective mode of transportation.
• Travel within the common marketing area.
• When possible, trips should be combined.
• Justify need for travel outside the common marketing area utilizing the Form 2020June 6, 2019 47 Limitations and Exclusions • Claims submitted for personal vehicle mileage reimbursement for Non-Medical Transportation must have prior approval from Transportation Manager. Prior approval is obtained by calling the Transportation Manager to receive an invoice number for every trip to be reimbursed. Reimbursement forms may be requested to be sent from the Transportation Manager or may be obtained from the Transportation Manager website (Medical Answering Service [MAS] for Upstate NY and NYC or Logisticare Solutions, LLC for Long Island- please see their contact information at the end of this section). • Claims must be submitted within 90 days of the date of service accompanied by the required mileage reimbursement form. Original receipts for expenses such as parking and tolls should be attached to the reimbursement form . The Department may consider reimbursement for trips submitted after the 90-day time period, but only when there are extenuating circumstances. Such requests will be considered on a case-by-case basis. • Reimbursement for travel can be denied when the destination does not support the participant’s integration into the community. • A participant’s Plan of Care outlines the general parameters of his or her Non-Medical Transportation needs. However, these needs can change or be amended based upon the participant’s stated goals and/or successful ongoing integration into the community.
June 6, 2019 48
Agency Qualifications
Agencies interested in providing Non-Medical Transportation must be enrolled in the FFS
program as a current Medicaid Transportation Provider. Please see the following links on
information on Medicaid Transportation:
• Link to transportation provider manuals:
https://www.emedny.org/ProviderManuals/Transportation/index.aspx
• Link to transportation provider enrollment application:
https://www.emedny.org/info/ProviderEnrollment/transportation/index.aspxJune 6, 2019 49 Contact Information for Transportation Managers NYC & Upstate: Medical Answering Services (MAS) https://www.medanswering.com/ https://www.medanswering.com/enrollee/enrollee-forms-resources/ https://www.medanswering.com/documents/Doc-MAS_Public_Site--2015-11-11-15-48-44.pdf Fax number for submitting all forms: (315) 299-2786 Secure email: Harp-info@medanswering.com (When sending completed Grids: “Attn: CHILDRENS HCBS GRID ”)
June 6, 2019 50 Contact Information for Transportation Managers Long Island: LogistiCare Solutions, LLC http://www.logisticare.com/ http://www.longislandmedicaidride.net/ http://www.longislandmedicaidride.net/Portals/51/DOH%20Mileage%20Reimbursment%20F orms-Logisticare.pdf?ver=2015-05-22-123216-000 Fax number for submitting mileage reimbursement forms: (866) 528-0462 Fax number for submitting completed Grids: 855-848-8640 (When sending completed Grids: “Attn: CHILDRENS HCBS GRID”)
June 6, 2019 51 Additional Contact Information: NYS Department of Health Transportation Unit: medtrans@health.ny.gov NYS Office of Mental Health: omh.sm.co.HCBS-Application@omh.ny.gov
June 6, 2019 52
Environmental ModificationsJune 6, 2019 53
What are Environmental Modifications?
• Provide internal and external physical adaptations to the home or other eligible residences of the enrolled child
which per the child’s plan of care (POC) are identified as necessary to support the health, welfare and safety of
the child or that enable the child to function with greater independence in the home and without which the
child would require institutional and/or more restrictive living setting.
• Modifications include but not limited to:
• Installation of ramps, hand rails, and grab-bars;
• widening of doorways (but not hallways);
• modifications of bathroom facilities,
• installation of specialized electric and plumbing systems that are necessary to accommodate the
medical equipment and supplies needed for the welfare of the recipient,
• lifts and related equipment,
• modifications of the kitchen necessary for the participant to function more independently in his
home,
• bed shaker alarm devices, strobe light smoke detection and alarm devices,
• The scope of environmental modifications will also include necessary assessments to determine the types of
modifications needed.June 6, 2019 54 Environmental Modifications Example During the Plan of Care (POC) development the care manager assists the family to get a clinical justification from Renee’s pediatrician, it is determined that Renee needs modifications to her family home to allow Renee to safely and independently function in her home while her parents are away. The Care Manager then works with the LDSS for authorization. An evaluator goes out to the home and determines that Renee’s house requires a bed shaker alarm device, a strobe light smoke and carbon monoxide detection and an alarm systems to ensure that Renee be able remain safe in her house even when staying on her own. The LDSS approves the scope of work and authorizes the services. The LDSS chose a provider through bidding/contracting. Once the work is completed the evaluator returns to the home an confirms the work is complete and satisfactory.
June 6, 2019 55
Limitations and Exclusions
• Excluded are those adaptations or improvements to the home that are of general utility, and are not
of direct medical or remedial benefit to the child.
• Adaptations that add to the total square footage of the home's footprint are excluded from this
benefit except when necessary to complete an adaptation (e.g., in order to improve
entrance/egress to a residence or to configure a bathroom to accommodate a wheelchair).
• Also excluded are pools and hot tubs and associated modifications for entering or exiting the pool
or hot tub.
• Repair & Replacement of Modification: In most instances, a specific type of Environmental
Modification is a one-time benefit. However, in reasonable circumstances determined and
approved by the State, a second modification may be considered for funding as follows: if a person
moves to another home; if the current modifications are in need of repair, worn-out or unsafe; or if
a participant wishes to spend considerable time with a non-cohabitating parent in their home and
such modifications are required to ensure health and safety during these periods.
• State policy places certain limitations on environmental modifications requested when the
home/apartment is a leased space, including property owner sign-off on the modification and
limitations on federal/state liability for the cost of removal/replacement/repair of items in public
spaces of rental properties.June 6, 2019 56
Limitations and Exclusions Continued
Modification Limits
• Only those services not reimbursable under the Community First Choice Option (CFCO) State
Medicaid Plan, Medicaid State Plan under 1905(a) of the Social Security Act or other
federal/state funding streams will be reimbursable under the HCBS Waiver.
• All Environmental Modifications require prior approval from the LDSS or MCO in conjunction with
NYSDOH or MCO.
• Contracts for Home modifications may not exceed $15,000 per year without prior approval from
the LDSS in conjunction with NYSDOH or MCO. For Environmental Modifications, the LDSS or
MCO is the provider of record for billing purposes. The State may consider exceptions when
medically necessary, including but not limited to a significant change in the child’s needs or
capabilities.
• Note: This service does not duplicate other services available through the New York Medicaid
State Plan. All services require prior authorization by the LDSS in conjunction with NYSDOH if
exceeding established limits or MCO.June 6, 2019 57
Adaptive and Assistive EquipmentJune 6, 2019 58
What is Adaptive and Assistive Equipment?
• Provides technological aids and devices identified within the child’s Plan of Care (POC) which enable him/her to
accomplish daily living tasks that are necessary to support the health, welfare, and safety of the child.
• Adaptive and Assistive Equipment includes but not limited to:
• Direct selection communicators,
• Alphanumeric communicators,
• Scanning communicators,
• Encoding communicators,
• Speech amplifiers,
• Electronic speech aids/devices, Voice activated, light activated, motion activated and electronic
devices;
• Standing boards/frames and therapeutic equipment for the purpose of maintaining or improving
the participant's strength, mobility or flexibility to perform activities of daily living;
• Adaptive switches/devices,June 6, 2019 59
What is Adaptive and Assistive Equipment
(continued)?
• Adaptive and Assistive Equipment Services include:
• the evaluation of the assistive technology needs of a participant, including a functional
evaluation of the impact of the provision of appropriate assistive technology and appropriate
services to the participant in the customary environment of the participant;
• services consisting of purchasing, leasing, or otherwise providing for the acquisition of assistive
technology devices for the participants;
• services consisting of selecting, designing, fitting, customizing, adapting, applying, maintaining,
repairing, or replacing assistive technology devices;
• training or technical assistance for the participant, or, where appropriate, the family members,
guardians, advocates or authorized representatives of the participant; and
• training or technical assistance for professionals or other individuals who provide services to,
employ, or are otherwise substantially involved in the major life functions of participants.June 6, 2019 60
Adaptive and Assistive Equipment Example
Sunny, a 14 year old with Muscular Dystrophy and her family use Adaptive and
Assistive Equipment to purchase a motorized wheelchair. Having this equipment allows
Sunny more independence to perform her daily activities. Sunny’s Care Manager assists
the family with getting clinical justification, evaluation and LDSS/NYSDOH approvals for
the wheelchair.June 6, 2019 61
Limitations and Exclusions
• The adaptive and assistive equipment available through the HCBS authorities including both CFCO
and the 1915c authorities cannot duplicate equipment otherwise available through the Medicaid
State Plan at 1905(a) of the Social Security Act or other federal/state funding streams. Equipment
must be beyond the scope of Durable Medical Equipment (DME). Only those services not
reimbursable under the Community First Choice Option (CFCO) State Medicaid Plan will be
reimbursable under the HCBS Waiver.
• Adaptive Devices are expected to be a one-time only purchase. Replacements, repairs, upgrades,
or enhancements made to existing equipment will be paid if documented as a necessity and
approved by the State or its designee. Ongoing monitoring associated with telecare support
services or other approved systems authorized under this definition may be provided if necessary
for health and safety and documented to the satisfaction of the State or designee.June 6, 2019 62
Limitations and Exclusions Continued
• Warranties, repairs or maintenance on assistive technology only when most cost effective and
efficient means to meet the need, and are not available through the Medicaid state plan at
1905(a), CFCO or third-party resources.
Cost Limits
• ALL AT costs require prior approval from the LDSS or MCO in conjunction with NYSDOH
• AT costs cannot exceed $15,000 per year without prior approval from the LDSS in conjunction with
NYSDOH or MCO approval if exceeding established limits.
• The State may consider exceptions when medically necessary, including but not limited to a
significant change in the child’s needs or capabilities.June 6, 2019 63
Vehicle ModificationsJune 6, 2019 64
What are Vehicle Modifications?
• Provides physical adaptations to the primary vehicle of the enrolled child which per the
child’s plan of care (POC) are identified as necessary to support the health, welfare and
safety of the child or that enable the child to function with greater independence.
• Include but not limited to: Portable electric/hydraulic and manual lifts, ramps, foot controls,
wheelchair lock downs, deep dish steering wheel, spinner knobs, hand controls, parking
break extension, replacement of roof with a fiberglass top, floor cut outs, extension of
steering wheel column, raised door, repositioning of seats, wheelchair floor, dashboard
adaptations and other ancillary equipment or modifications necessary to guarantee full
access to, and safety in, a motor vehicle.
• Activities include and are not limited to determining the need for the service, the safety of
the proposed modification, its expected benefit to the child, and the most cost effective
approach to fulfill the child’s need.June 6, 2019 65
Vehicle Modifications Example
Maria and her family use Vehicle Modifications in order to reposition seats and add a
wheelchair floor to their vehicle. These modifications allow them to more easily travel
to Maria’s appointments as well as help achieve Maria’s goal of attending more
community events in her suburban town. Maria’s Care Manager assists the family with
getting clinical justification, evaluation and LDSS approvals for the modification.June 6, 2019 66 Limitations and Exclusions • Vehicle Modifications are limited to the primary means of transportation for the child. The vehicle may be owned by the child or by a family member or non-relative who provides primary, consistent and ongoing transportation for the child. • All equipment and technology used for entertainment is prohibited. • Costs may not exceed current market value of vehicle. • Other exclusions include the purchase, installation or maintenance of items such as cellular phones, global positioning/tracking devices, or other mobile communication devices; repair or replacement of modified equipment damaged or destroyed in an accident; alarm systems; auto loan payments, insurance coverage; costs related to obtaining a driver’s license, title/registration, license plates, emergency road service, or rental vehicles when a vehicle modification is in process. • Repair & Replacement of modification: In most instances a specific type of Vehicle Modification is a one-time benefit to motor vehicles used by the child. However, in reasonable circumstances determined and approved by the State, a second modification may be considered for funding if the current modifications are in need of repair, worn-out, or unsafe.
June 6, 2019 67
Limitations and Exclusions Continued
Modification Limits
• Only those services not reimbursable under the Community First Choice Option (CFCO) State
Medicaid Plan, Medicaid State Plan under 1905(a) of the Social Security Act or other
federal/state funding streams will be reimbursable under the HCBS Waiver.
• Contracts for Vehicle Modifications under $15,000 require prior approval from the LDSS or
MCO
• Contracts for Vehicle modifications may not exceed $15,000 per year without prior approval
from the LDSS in conjunction with NYSDOH or MCO.
• The State may consider exceptions when medically necessary, including but not limited to a
significant change in the child’s needs or capabilities.June 6, 2019 68 Resources and Information List of NYS Health Homes by County https://www.health.ny.gov/health_care/medicaid/program/medicaid_health_hom es/hh_map/index.htm C-YES Contact info: 1-833-333-CYES (1-833-333-2937); TTY: 1-888-329-1541 https://nymedicaidchoice.com/information-care-management-agencies Children’s Behavioral Health Transition to Managed Care https://www.health.ny.gov/health_care/medicaid/redesign/behavioral_health/chil dren/index.htm
June 6, 2019 69
Email Resources
Please specify if kids system/managed care specific in subject line:
DOH Transition Mailbox
BH.Transition@health.ny.gov
NYS OMH Managed Care Mailbox
OMH-MC-Children@omh.ny.gov
NYS OASAS Mailbox:
PICM@oasas.ny.gov
NYSDOH Health Homes for Children:
HHSC@health.ny.gov
NYS OCFS Mailbox:
OCFS-Managed-Care@ocfs.ny.govJune 6, 2019 70
Questions
Please send questions to:
mctac.info@nyu.edu
Logistical questions
usually receive a response
in 1 business day or less.
Longer & more complicated
questions
can take longer.
Visit www.ctacny.org to view past
We appreciate your interest and trainings, sign-up for updates and event
patience! announcements, and access resourcesYou can also read