Children and young people's mental health resilience project - Dr Nicole Burchett & Dr Rebecca Clark Elford
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
1. Children and young people’s mental health resilience project Dr Nicole Burchett & Dr Rebecca Clark Elford With contributions from Heather Lewis, Jenny Burns, Dr Gwen O’Connor, the Resilience Project Staff and Darren Madden
Mental Health Foundation Children and young people’s mental health resilience project 2.
Table of contents
4. Executive Summary
8. Introduction
9. Resilience Project Design
10. Resilience Project Partners
12. Background
12. A trauma informed approach
13. The Missing Middle
15. Programme content and findings
17. Resources
17. Supporting Literature
18. Delivery
18. Evaluation
20. Training
20. Supporting Literature
20. Delivery
20. Evaluation
25. Consulation and Team Formulation
25. Supporting Literature
25. Delivery
26. Evaluation
32. Group Work
32. Supporting LiteratureMental Health Foundation Children and young people’s mental health resilience project 3.
32. Delivery and Evaluation
33. Direct Intervention:
33. Supporting Literature
34. Delivery
35. Evaluation
39. Case studies
48. Partnerships
48. Introduction
49. Findings
49. ‘Communication event’
50. Survey
53. Focus group
59. Recommendations
59. Service Delivery Recommendations
62. Evaluation Recommendations
63. Partnership Recommendations
64. Conclusion
66. References
71. Appendices
71. Other findings and Headlines
73 Press releasesMental Health Foundation Children and young people’s mental health resilience project 4.
Executive Summary
Our children and young people are precious to us all. We want the best
for them. Our system can often supply the educational and physical
requirements for our children, but are we getting the emotional
support right? Who does a parent call when her child’s behaviour
starts to become unmanageable? How does a teacher respond to a
pupil who is self-harming? What does a parent say when his teenager
is too anxious to go out and is not sleeping properly?
M
ore seriously, if these behaviours The Resilience Project wanted to try to
occur with a backdrop of address these issues by:
adverse childhood experiences
• Giving accessible, fast support to
like bullying, social exclusion, abuse,
parents whose children do not meet
neglect, abandonment, family separation
the criteria for mental health services.
or domestic violence - the child or young
• To build mental health capacity,
person’s brain is more than likely being
knowledge, and confidence within the
adversely affected.
education system.
Roll on 10 or 20 years, and 50% of
• To promote joint working between
these same children and young people
health and education.
are struggling with their mental health
and their children are now also at risk Since October 2019, and with a current
of developing their own mental health team of 6 Resilience Workers, 3 part time
problems – and so history repeats itself clinical psychologists, an occupational
(Mental Health Foundation, 2015). therapist, art therapist and project
manager, the Resilience Project has
Can our health, social care and education
achieved the following:
system work together to arrest this cycle?
Our current children and young people’s
mental health services are often not able
to receive children before they become
unwell. These children are often deemed as
the ‘missing middle’.Mental Health Foundation Children and young people’s mental health resilience project 5.
• Education staff requested support for 181 children and young
people, who received a professional consultation.
• 177 families have been supported through direct intervention
(Resilience Project and through other health teams).
‘… it’s like a weight off my shoulders and actually understanding
his behaviours…what he’s thinking and why he does what he
does, and it started to make a bit more sense. It was about us
coping together, so that the way I deal with him helps him, and
how he behaves and how I deal with it helps him…he’s a lot
happier as well…I’ve shared things with my mum and dad…and
they were like wow!’ (parent)
‘… it was absolutely heart-breaking … it got to the point where
she was not sleeping in the nights… it was a dark place for
everybody, I didn’ t want her suffering… but now, she’ ll go up
to him [teacher] and say “sir, can I read to you?” and Alice was
never like that. If you put her on the spot, she would absolutely
hate it…… the difference in Alice from May, June to now has
been tremendous… I spoke to her teacher yesterday…he said it’s
like seeing a different child. So, it’s been absolutely fantastic
the help they have given me’ (parent)
• 938 education staff including school nurses received training.
• 45 resources developed for educators, parents/carers and
children and young people.
• 13 YouTube resources produced that have been watched
2,468 times.
• 33% of children and young people receiving a consultation or
formulation for the Resilience Project indicated a key theme of
the request related to a developmental trauma.Mental Health Foundation Children and young people’s mental health resilience project 6.
• 83 CYP receiving a consultation or formulation had
been previously referred to either a mental health or
neurodevelopmental service at least once, and 55 had received 2
or more referrals to either or both of these services.
• 90% of educational staff felt confident using what they had
learned during training in their working practice.
• 82% of education staff felt confident in using what they had
learned from a formulation/consultation session.
• 90% of parents felt confident using what they had learned
during an intervention session in their everyday life.
• Increased joint working between education and health.
‘Every opportunity we take to work across sectors enables
us to better understand the reasons why we work in different
ways, the unique priorities, strengths and limitations that we
each have in addition to our shared aims (Engagement Service
Lead, Education) and
‘…it felt like education is over there and social services is over
there but actually it has, it feels like it has brought us much
more closer together and understanding how we work and
what the issues are and what the difficulties are (Lead of
Children’s Psychological Therapies)
The learning and recommendations from this project so far are:
• Clear leadership and authority from the start.
• Mapping the needs of the educational staff, children and
young people and not repeating existing provision.Mental Health Foundation Children and young people’s mental health resilience project 7.
• Improving the marketing of resources.
• Increasing the diversity of children and young people
reached including Welsh language speakers.
• Increasing face to face provision as the pandemic subsides.
• Considering scaling up this model throughout Cardiff and
the Vale as well as locally and nationally.
• More involvement of staff and children/young people in the
evaluation process.
• Persevering with partnership working across sectors where
the following themes are considered: clear leadership,
governance, flexibility, clarity, time and openness.
In summary, this project has and is in turn can help prevent mental health
demonstrating that putting accessible, issues developing. In addition, working in
systemic, trauma-informed resources in partnership across all sectors can reduce
‘up-stream’ to support non-health staff duplication and increase understanding
and the families they work with, can indeed ultimately enhancing the provision for the
help prevent children and young people child and young person.
being left in the ‘missing middle’. ThisMental Health Foundation Children and young people’s mental health resilience project 8.
Introduction
‘Our children and young people’s mental health needs attention,
now more than ever! Those who have experienced difficult childhood
experiences particularly need our attention because of the potential
long-term effects on their health. The Resilience Project has navigated
a new way to connect directly with teachers and the children and
young people they work with, to help offset mental health issues
developing or deteriorating. The Mental Health Foundation have been
delighted to have helped shape this project with Cardiff and Vale
Health Board to the success that it is now.’
Jenny Burns (Associate Director, Mental Health Foundation)
“The Resilience Project has been set up to provide early help to those
children and young people beginning to display distress, but who do
not meet criteria for other services. It is breaking new ground because
we are bringing together education and clinical knowledge and skills
from health to improve the mental well-being of children and young
people.”
Dr Gwen O’Connor (Clinical Lead, Resilience Project)
T
he Children and Young People education with involvement from a third
(CYP) Resilience Project is a sector charity, is ground-breaking. CYP
pioneering partnership between are central to this project, however
the Mental Health Foundation (MHF) and building capacity, understanding and
Cardiff and Vale Health Board, bringing knowledge with CYP staff and workers
together the education and health sector is the focus of this project. This service
to support the wellbeing of our Welsh CYP. provision stands out from many others
with regard to this approach.
This innovative way of working, bringing
together health, social services and Different environments impact theMental Health Foundation Children and young people’s mental health resilience project 9.
health and wellbeing of CYP. Home, Resilience Project Design
community and school are integral to
This project was designed, based on a
their development and path through
needs-led service model which uses
life. Therefore, this project is a holistic,
clinical and psychological knowledge to
multifaceted approach that focuses on the
support different parts of the system
CYP in the context of their environment
around the child. This included providing
and the support network this offers.
resources for parents and staff, training
From the outset this project was designed for those supporting CYP, consultation
to be a preventative, transformative and and team formulation for professionals
capacity building, with the potential for with concerns about children, group work
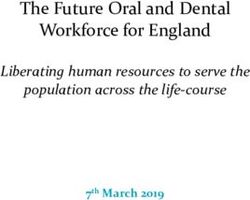
scaling up across Wales and UK. The and direct intervention (see Figure 1).
project vision was to build greater capacity, This model will form the structure of this
expertise and mental health resilience for report where each level will be described
CYP in educational settings across Cardiff and explored considering the findings of
and the Vale. By supporting and increasing the service evaluation carried out by MHF.
confidence of those supporting CYP,
this project hoped to increase resilience
and reduce the impact of mental health Direct
intervention
distress.
Group
The aims of the Resilience Project echo work
this vision and were as follows:
Consultation &
1. To enhance the joint working team formulation
between education and health,
Training
to improve mental well-being of
Children and Young People (CYP)
Resources
2. To increase mental well-being
support and interventions for CYP
through supporting education staff Figure 1. Service Model
3. To increase the confidence of all
those working with CYP in relation to The CYP Resilience Project was funded by
mental health Welsh Government- ‘A Healthier Wales’
4. To decrease inappropriate referrals Transformation Fund (TF), initially for up
to Child and Adolescent Mental Health to 2 years. This fund has been distributed
Services by providing support to the throughout Regional Partnership Boards
‘missing middle’ across Wales aimed at achieving a ‘long-
term future vision of a ‘whole system
approach to health and social care’ (BebbMental Health Foundation Children and young people’s mental health resilience project 10.
& Bryer, 2020; Welsh Government, roots level. At this stage it was noted that
2018). To be eligible for this fund a project education and care sector staff already
needed to demonstrate the capability to felt educated about ACE’s and their
be transformative and scalable, along with impact on mental health. Although this
one other ‘stream’. It was critical that any could be seen as having a detrimental
new support programme was affordable impact on the delivery of the service, in
and sustainable. That it changed and fact the service adapted itself to offer
replaced existing approaches, rather what the staff and parents felt they
than add an extra permanent service needed i.e., not information about ACEs,
layer. It was also critical to have the rather offering support in how to help
potential to scale up from local to regional, CYP. The Resilience Project then came
national or to other organisations (Welsh into its own, suiting the needs of the
Government, 2018). education staff and carers on the frontline,
and supporting our CYP.
This service, despite initial challenges, has
become an effective and critical aid to the Resilience Project Partners
education sector, CYP and psychological
There have been two main partners
services across Cardiff and the Vale. It
delivering this project; the Mental Health
bridges the gap between children and
Foundation (MHF) and Cardiff and Vale
young people and NHS psychological
University Health Board (C&V UHB)
services, by connecting directly with
working in partnership with education and
the local education authority. It provides
children’s services.
resources, training and consultation
opportunity for education staff to MHF has a vision of good mental health
support CYP who may be experiencing for all. It’s mission is to help people
psychological or emotional distress. With a understand, protect and sustain their
focus on prevention and building capacity, mental health through community and
it aims to capture children displaying peer programmes, research, public
distress early, to prevent escalation in engagement and advocacy. The Resilience
poor mental health and possible referral to Project fitted well with MHF’s vision and
a clinical health setting. they led on the evaluation, assisted with
the project logistics and initiated the
It is worth noting that this project began
original ideas.
as an Adverse Childhood Experiences
(ACEs) education project. However, C&V UHB, C&V UHB Child Psychology
recently the concept of ACE’s has been clinically led this project. A Clinical
absorbed into mainstream thinking which Psychologist Lead and 10 Resilience
became apparent during the development Workers (graduate mental health workers)
of the Resilience Project. To help build a were originally employed to work across
picture of what was needed, the project Cardiff and the Vale with the local
was developed by exploration at a grass authority Inclusion and EngagementMental Health Foundation Children and young people’s mental health resilience project 11. Teams, who work alongside primary and promote joint working between health and secondary schools. This staff structure education, this included Primary Mental naturally changed over the lifetime of the Health, Neurodevelopmental Service, project, with the replacement of some Community Family Psychology, Enfys Resilience Workers as they left with (née Developmental Trauma Service) Clinical staff, to build in the support that and the Psychology Service for children became evident was required. To promote (0-5) with Global Developmental Delay further joint working Resilience Workers and Emerging Learning Disabilities and were also based in child health teams to their Families.
Mental Health Foundation Children and young people’s mental health resilience project 12.
Background
‘Young brains are like seedlings. Strong roots and good growth depend
on environmental conditions’
(Gerhardt, 2014).
A trauma informed approach or domestic violence contribute to poor
experiences, adversely shaping the child’s
A young brain cannot develop in a
brain. Stressors that ‘directly hurt a child
healthy way without positive social
or affect them through the environment
experiences. The Centre on the
in which they live’ have been termed
Developing Child states:
Adverse Childhood Experiences (ACEs)
‘Science tells us that early childhood (Bellis, 2016; Felitti et al., 1998)). Two
is a time of both great promise and reports commissioned in Wales in 2016
considerable risk. Having responsive and 2018 have found that at least 47%
relationships with adults, growth- of Welsh individuals have experienced
promoting experiences, and healthy one ACE or more. Of those, 14% have
environments for all young children experienced four or more ACE’s (Bellis,
helps build sturdy brain architecture 2016; Hughes et al., 2018).
and the foundations of resilience.
Moreover, chronic stress affects key
Meanwhile, significant disadvantages
areas of the brain involved in higher level
can disrupt the developmental
thought; cognition (thinking), emotion
process and lead to limited economic
(feelings) and behaviour (action), which
and social mobility that threatens
has implications across the lifespan.
the vitality, productivity, and
For instance, Welsh studies show that
sustainability of society’.
individuals experiencing four or more ACEs
(Centre on the Developing Child,
are at significant risk of problem alcohol
2021)
or drug use, risky behaviour including
It has been increasingly acknowledged teenage pregnancy or behaviour which
that chronic stress in childhood has long results in a prison sentence. Furthermore,
term health implications (Felitti et al., experiencing four or more ACE’s places
1998). Bullying, social exclusion, abuse, a person six times more likely to have
neglect, abandonment, family separation received treatment for a mental healthMental Health Foundation Children and young people’s mental health resilience project 13.
illness (Bellis, 2016; Hughes et al., 2018). adult health services in the future.
Given the prevalence of ACEs in Wales Providing safe and positive social
mentioned above, this is clearly an interactions with these children as early as
area that needs much attention. The possible in their life has a significant impact.
higher the risk of negative life events for Perry and Szalavitz (2017) state that:
those who experience ACEs, the more
‘the most therapeutic experiences do
likely an individual and their world, will
not occur in therapy, but within naturally
be negatively impacted. ACE’s have
occurring healthy relationships.’
been shown to affect people across
This suggests that there are many people
generations, indeed children that are
in the CYPs life that can provide space
affected by ACE’s are also more likely
for a safe and positive interaction with a
to expose their own children to ACE’s
child, not just a healthcare professional
(Renner & Slack, 2006) . This leads to
or therapist. Moreover, environments
cyclical behaviour over generations,
which are predictable and safe are often
which increases pressure on future
best placed to build resilience, skills in
statutory services.
self-regulation and positive interactions.
The Missing Middle It is therefore not surprising that if home
Within Wales, and across the UK, children is a less supportive environment, schools
experiencing behavioural or mental could provide a safe and affirming space
health issues are referred to a Primary for children. It is also a space where
Mental Health Support Service, CAMHS, teachers can notice detrimental, negative
a Paediatrician or a Neurodevelopmental or concerning behaviour and be role
service depending on the symptoms. models of good relationships themselves
However, there are a group of children (Department for Education, 2014).
who do not meet criteria for any of these In practice, although this can vary across
services. These children are described as locations, the education sector can refer
the ‘Missing Middle’ (Neagle et al., 2018). It to Primary Mental Health, a GP, the local
has been identified that there is currently CAHMS team for a CYP or draw on
insufficient support for these children, who other third sector organisations, school
will often enter into health service at a counselling or wellbeing teams to support
later stage of life, potentially at crisis point a child’s mental health (Department for
and requiring higher intensity intervention Education, 2014). Research indicates
(Action for Children, 2017; Neagle et that in order for support services to be
al., 2018). This gives more weight to the successful, a focus must also be placed on
argument of prevention as an approach; the coordination of services (Ungar et al.,
by supporting at an earlier stage, crisis 2014). This indicates that more positive
situations can, more often than not, be outcomes can be achieved when local
avoided and potentially prevent the use of services work together, as well as involvingMental Health Foundation Children and young people’s mental health resilience project 14.
the CYP and their family. It has also been become compounded, resulting in crises
found that a wide range of an evidence- in adulthood. It may also go some way to
based interventions which offer continuity address the transgenerational cycle of
are also most effective. Specifically, ACEs. Building capacity within the network
interventions focusing on protective of those surrounding CYP will ultimately
factors and aspects of resilience related benefit this population both mentally and
to promoting social support, a sense of physically, as well as wider society and the
consistency, or control and predictability services in place supporting adults in crisis.
are often the most effective (Smokowski et
Therefore, the CYP Resilience Project
al., 2004; Ungar, 2005).
was designed as a multiagency and
In conclusion, building capacity and coordinated approach of children’s
confidence for those surrounding a young services, education and mental health
person experiencing mental health distress support services. Its vision is anticipated
has significant potential to increase general to build greater capacity, expertise and
mental health wellbeing in our young mental health resilience for CYP across
population. Importantly this preventative Cardiff and the Vale.
approach may increase resilience and
reduce the distress of life events that oftenMental Health Foundation Children and young people’s mental health resilience project 15.
Project content and findings
The service model was structured using a multi-layered needs lead
approach, which had its origins in previously effective community
based mental health services for CYP in education.
A
n important factor in the signposting to other services an option
successful implementation of a (Callaghan et al., 2004; Early Intervention
pilot or programme of support, Foundation, 2017; Holtom & Lloyd-Jones,
was the presence of a multi-disciplinary 2020; Owens et al., 2008). Furthermore,
team who built direct and consistent training was common practice in previously
relationships with education staff successful community programmes,
(Callaghan et al., 2004; Early Intervention providing opportunities for learning across
Foundation, 2017; Holtom & Lloyd-Jones, a wide range of audiences; including
2020; Owens et al., 2008; Pearlman et al., education staff, primary care givers
2018; Reinke et al., 2018). In practice this and CYP (Callaghan et al., 2004; Early
equates to bringing together professionals Intervention Foundation, 2017; Holtom &
from health, including psychologists, Lloyd-Jones, 2020; Pearlman et al., 2018).
clinicians and Resilience Workers, who
Therefore, this scoping of evidence and
build a consistent relationship with
need, as outlined above, fed into the
education staff or family to support a CYP
development of the current service model,
over a period of time.
see Figure 2. The report will now focus on
It has been recognised that in previously each area of the service model, in turn,
effective pilots or support services, exploring delivery, supporting research and
consultations are utilised as a basis for service evaluation.
accepting referrals into the service, withMental Health Foundation Children and young people’s mental health resilience project 16.
Direct Key:
Intervention:
Intended audience for intervention
Aimed at supporting
CYP/Parents directly Intervention
in school/home.
Pathway for requesting support
Group Work:
Training/resources
in schools
Consultation and Team Formulation:
Including RP resources, interventions,
and signposting.
Training: e.g., Understanding ACE’s, mental
health, distress and self-harm.
Figure 2. Service Model implementation: Support and intervention pathwaysMental Health Foundation Children and young people’s mental health resilience project 17.
Resources
the internet for mental health resources
(Headstrong, 2012), in a more recent
survey this increased to 88% (Pretorius
Direct
intervention
et al., 2019). It is also worth considering
Group
work the impact of the COVID-19 pandemic
and whether this has and will continue to
Consultation &
team formulation impact the utilisation of online resources.
However, a potential downfall for online
Training help seeking behaviour is whether a
person is able to find material which suits
Resources their need and importantly the real impact
of digital poverty as an exclusion criterion
for access to these resources.
Supporting literature
Much of the research surrounding online
It has become increasingly accepted
help seeking behaviour is centred on
that the internet plays a major role in
establishing a person’s preferences
help seeking behaviour. This is especially
when online. The literature indicates
relevant following the advent of the
that people are influenced by online
COVID-19 pandemic and the limited
resources in different ways. For example
clinical capacity to see CYP or families
young people searching the internet find
face-to-face. Internet based information
resources with a health website logo, and
takes many forms including; information
endorsement from the education sector,
guides or websites, forums and online
more reliable and trustworthy (Pretorius
therapy, all with the potential to help
et al., 2019). Parents are likely to engage
young people (Chambers et al., 2018). The
in online resources where the literature
use of such resources is likely to be based
is accessible and aimed different reading
on several facilitating factors including;
levels, for example those that do not
the assurance that searching the internet
use medical terminology (Wozney et al.,
for self-help advice is free, anonymous and
2018). Moreover, in designing mental
confidential (Pretorius et al., 2019). Indeed
health training for non-mental health
it has been established that potentially
professionals, takeaway resources are
77% of young people are likely to use
recommended to help consolidate theMental Health Foundation Children and young people’s mental health resilience project 18.
learning and for reference (Scantlebury care. It has been established that training
et al., 2018). Therefore, the Resilience in staff self care can improve teacher
Project has aimed to make their resources wellbeing which has a direct influence and
flexible, practical, accessible, engaging impact on student wellbeing. For instance
and evidence based. Although they are teachers with improved wellbeing, that
designed by mental health professionals, feel able to manage work related stress
they are tailored to suit various audiences. are also more likely to have the capacity to
identify and provide early mental health
Delivery
interventions for their students.
The resources include a bi-monthly
The resources are hosted on a NHS
newsletter, videos and guides centred
website - Resilience Project - Cardiff and
around mental health and wellbing. Due
Vale University Health Board (nhs.wales)
to the onset of the COVID-19 pandemic,
and depending on whether you are a CYP,
the focus shifted to developing more
parent or education staff, you access tailor
online resources. This is opposed to
designed material.
physical or paper resources that had
been planned, at the start of the project. Evaluation
These include guides for transitioning
The Resilience Project has, thus far,
between primary and secondary school,
developed seven videos (five translated to
as well as building healthy relationships,
Welsh), 38 online resources (32 translated
emotional understanding, confidence, and
to Welsh) and a further six resources are in
communication skills. Additionally, there
progress (all in Welsh, with two in English
are also symptom specific guides, aimed
and Welsh). Videos and resources have
at understanding anxiety or low mood for
been translated into the Welsh language to
example. Finally, resources are provided
support CYP, families and education staff
that are specifically aimed at those
in Welsh speaking schools. The resources
working in education and related to self-
have been distributed by Resilience Project
Platform Outcome
YouTube 2486 views
CAV Website 1623 views
CAV resource downloads 401 downloads
CAV website: Average time on site 2 minutes 13 seconds
Table 1. Resource website and YouTube analyticsMental Health Foundation Children and young people’s mental health resilience project 19.
staff to over 340 recipients following the website has received 1623 page views.
consultation, training, or intervention. Furthermore, 42% of viewers remain on
the site after landing on the page, to look
The resources are hosted on two platforms;
at other parts of the website and the
firstly, YouTube which up until March 2021
resources have been downloaded 401
had received 2,486 combined views (of
times (See Table 1, CAV website analytics
all resources). During the last quarter of
from 1st Jan-23 March, 2021. More in-
the Resilience Project, all the resources
depth information regarding the analytics
were hosted on a new platform; the Cardiff
is available on request).
and Vale (CAV) University Health Board
website. Since hosting on this platform,Mental Health Foundation Children and young people’s mental health resilience project 20.
Training
staff could well be beneficial for CYP
Direct
wellbeing, as well as for staff wellbeing.
intervention
A review of many studies evaluating
Group
work
mental health training for non-mental
health professionals, has found that
Consultation &
training effectively increases knowledge,
team formulation
attitudes, confidence and mental health
Training self awareness (Booth et al., 2017). A
further review of studies also compliments
Resources this evidence, by showing that support
programmes which focus on resilience and
coping skills have positive impacts on the
Supporting literature ability for CYP to manage their wellbeing
CYP encounter many non-mental health (Fenwick-Smith et al., 2018).
professionals as part of daily routines or as
Delivery
part of a statutory services, like education.
Indeed it has been reported that teachers This evidence supports the focus of
are a common contact point utilised by training for educational staff developed
CYP and parents for emotional difficulties by the Resilience Project, which include
(Banwell et al., 2021; Ford et al., 2005). courses providing information on CYP
However, previous research has indicated mental health, ACEs and developmental
that educators report reduced confidence trauma. These are also aligned with
and knowledge of the impact of mental the aims of the project, to increase
health on CYP, as well as on their own mental well-being support and provide
mental wellbeing (O’Reilly et al., 2018; interventions for CYP through supporting
Parker et al., 2021). It is also reported education staff as well as increasing the
that this inexperience can increase work confidence of all those working with CYP
related distress, which can impact staff in relation to mental health.
mental health as well as that of their
Evaluation
students (Oberle & Schonert-Reichl,
Quantitative findings
2016). Therefore the evidence indicates
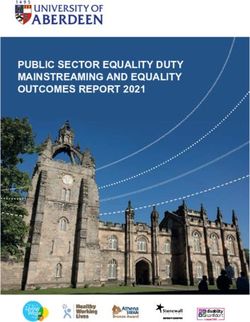
that mental health training for education In total 8 separate training courses haveMental Health Foundation Children and young people’s mental health resilience project 21.
been developed by the Resilience Project, Shame/Distress’, ‘Unpicking Mental Health
aimed at education staff across Cardiff Difficulties Through an ACEs Lens’ and
and the Vale. Twenty-nine training courses ‘Self Harm Awareness’ training. This could
have been delivered since the start of the be an indicator of need, or an indication
Resilience Project and 938 education staff of which courses had been developed in
have accessed training up to the end of the early stages of the project, therefore
February 2021. Most attendees accessed had more opportunity to be delivered. See
the ‘Understanding and Responding to Figure 3.
Figure 3. Training delivery:
School Based
Anxiety - 37 Number of staff attending
(4%) each training course.
Self-harm
awareness - 163
(18%)
Storytelling- 44
(5%)
The Three R’s of Responding:
Understanding Strategies for Supporting
and Responding to Learners with Emotion
Distress/Shame - Regulation (PART 1) - 59
384 (42%) (6%)
Tree of Life - 26
(3%)
Of those that accessed training, 318 convenient (91%) and was appropriate
education staff completed a training and relevant to their working practice
feedback form. Over 90% of attendees (95%). Furthermore, 76% of attendees
agreed* that the training was in line with agreed* that they felt supported by the
their expectations (92%), was easy to Resilience Project. Moreover, over 90%
access (91%), was at a time and place agreed that they can apply what they
*For the purposes of this report “agreed” refers to either strongly agreeing or agreeing with the feedback statementMental Health Foundation Children and young people’s mental health resilience project 22.
have learned into their everyday practice (90%). Finally, 77% agreed that what they
(92%) or felt confident using what they had learned will change their working
have learned in their working practice practice in the future. See Figure 4.
Figure 4. Training feedback for confidence and how training will change working practice
What I have learnerd will change
my working practice (n=318)
Neutral
Strongly agree 10%
Disagree
24%
3%
Agree Strongly agree
Agree Neutral 57% 33%
53% 20%
Strongly disagree 0% Strongly disagree 0%
Disagree 0%
Qualitative findings training. This resonated well with the focus
on the importance of good self-care and
Each training course has been qualitatively
highlighting the importance of reflection and
analysed separately. Below are the findings.
the part it plays. Although the feedback was
Wellbeing
positive, participants suggested that more
‘Fantastic tips and opportunities to group discussions, setting up a social media
discuss things with others’ page for CYP and additional training in this
area would be welcomed.
Comments about what was most helpful
for participants were centred on the aspect
of gratitude and positivity within theMental Health Foundation Children and young people’s mental health resilience project 23.
Unpicking mental health difficulties through ‘Brilliant. Thanks.’
an ACEs lens
One participant suggested that
‘The session was very informative, great understanding the differences between
how it all links with other courses that I shame and guilt stood out for them on this
have attended’ course. Others found the three R’s (Regulate,
Relate and Reason), the ‘learner meetings’
Reinforcing the participants own daily
and an understanding of a way forward,
practice, was of help to some participants.
helpful and requested further training.
Many noted the benefit of the evidence-
based knowledge of the Resilience Project Tree of life
facilitators and discussion with them helped
‘I enjoyed the workshop and found it
recognise the resources available to them.
helpful. I hope I will be able to use it
This was made more relevant with the use
with pupils, young people or staff in the
of case studies to inform real life situations
future. Thank you.’
that may occur, this was also helped by
This, for many, was a new approach to
acknowledging changed interactions in
facilitate opening up conversations with CYP.
the context of the pandemic. Suggestions
The practical use of it appealed and being
included making the information relevant to
able to complete a Tree of Life themselves,
younger children, an open ‘Q&A’ at the end
created an opportunity for self-reflection
and perhaps incorporating it into sessions
and learning. It was seen to be a useful tool
with pupils.
when working with adopted and Looked
Understanding and responding to distress/
After Children (LAC) and others suggested
shame
transferring it to use within their staff group.
‘The training was interesting and
The three R’s of responding: Strategies for
informative and gives you lots of things
learners with emotional regulation
to think about with regards to how I
‘Reassurance that strategies we already
Interact with children in school and
use are appropriate’
reasons for their behaviour.’
Many participants had not heard of the
The provision of information about brain
use of PACE (Playfulness, Acceptance,
development was highlighted as helpful
Curiosity and Empathy) when working with
in gaining an understanding of responses
CYP. Exploring this helped reinforce their
to distress. The introduction of practical
usual practice with CYP and found that the
strategies, especially helping calm a
time spent advising on practical use of this
distressed CYP, was noted as helpful. The
theory, was of help. Some, however, already
resources were also appreciated, however,
had this information from other courses and
one participant suggested that the training
had preferences for other methods (such as
be delivered with an appreciation of Welsh
Socratic questioning).
language and terminology, to be able to
apply the training in Welsh-medium schools. Self-Harm awarenessMental Health Foundation Children and young people’s mental health resilience project 24.
‘I enjoyed all aspects. I found it all of storytelling in a range of circumstances.
relevant to my practice.’ Some participants would have preferred
some smaller group discussion and others
Again, practical strategies when working
requested additional resources.
with CYP who self-harm was seen as of great
benefit by the participants. The evidence Training summary
base and statistics that accompanied the
Overall, the training was very well received
course helped form a context and this,
by the majority of participants. The
together with an understanding of why
comments on how to improve each of the
people self-harm, were areas appreciated
training sessions had some converging
by the participants in increasing their
themes. Many stated they would have liked
knowledge. Some would have preferred
the training to be face-to-face, however, they
more interaction, such as the use of
also acknowledged this was not the fault of
questions and running polls within the
the Resilience Project and the pandemic
training, and others suggested more real-
restricted this request. Timings were also
life examples and videos to embed the
noted for amendment: either the sessions
knowledge.
were considered too long or too short,
Emotional regulation and storytelling whilst other participants suggested further
training in the same area. Interestingly other
‘Knowing how storytelling can provide
information learned in these sessions was
a thinking, safe environment to open up
not limited to the content of the course
without being intrusive.’
and many stated that the information given
The use of storytelling to make sense of a
about the Resilience Project was, indeed,
situation was thought to be very relevant
helpful in itself.
to the participants. Specifically, the use of
‘I would love to do more with the
this method to help CYP learn and develop
resilience project.’
emotional intelligence in a practical way
and as a new approach. Some participants The training was very well delivered in a
queried the relevance to use of this method friendly and interesting manner. Left me
with older CYP who have behavioural issues, wanting to know more. Many thanks.
but in the main the method and training were
‘Such an enjoyable morning! I am feeling
felt to be beneficial.
very relaxed. Thank you so much. The
‘Easy to understand - relevant’ trainer…was engaging, interesting,
knowledgeable and very relaxing.’
The practical use of this strategy was
appreciated alongside the space to think ‘The resilience team is very
about our stories and the stories of others. approachable. Great training and
Some participants suggested that giving amazing staff.’
examples of a greater variety of stories,
would allow a wider understanding of the useMental Health Foundation Children and young people’s mental health resilience project 25.
Consulation and team
formulation
a ‘formulation‘ of the child’s need. This
Direct
supports education staff to effectively
intervention
understand and plan how to respond to
Group a child’s needs. Formulations are more
work
in-depth and take into account the person
Consultation & as a ‘whole’, exploring social, biological
team formulation
and psychological factors contributing
to difficulties, taking into account clinical
Training
and psychological knowledge and theory
without necessarily coming to a specific
Resources
diagnosis. This allows an ongoing and
collaborative approach which can be
Supporting literature revised and ‘reformulated’ as more
information is gathered, or as progress is
The scoping of literature at the
made (Macneil et al., 2012). As discussed,
developmental stage of the service model,
CYP may not meet diagnostic criteria
noted the use of consultation as a basis
for support from mental health services
for advice, guidance and referral. This
(see The Missing Middle) so formulation
type of intervention has been used in
has also been proposed as an alternative
previously successful support services
approach for CYP who have experienced
for CYP (Callaghan et al., 2004; Early
ACE’s or difficulties with attachment
Intervention Foundation, 2017; Holtom &
(Rahim, 2014).
Lloyd-Jones, 2020; Owens et al., 2008).
This is where a team consult regarding a Delivery
CYPs needs, provide clinical advice and
The Resilience Project brought
guidance, resources and signposting as
together psychologists, mental health
well as consider suitability for the service.
clinicans, education staff (e.g. school
Moreover, the Resilience Project benefits
staff, Engagement Teams, Educational
from an additional layer of support within
Psychologists), the third sector and
consultations, as clinicians co-developMental Health Foundation Children and young people’s mental health resilience project 26.
other health services (e.g. Primary Evaluation
Mental Health Service, CAMHS) to
Quantitative findings
support children displaying distress
In total the Resilience Project has been
in their educational environments.
contacted regarding support for 193 CYP
Education establishments could also
across Cardiff and the Vale. See Figure
use consultation sessions to discuss
5 for available information regarding
whole classroom, or whole school
request for support origin. Information
approaches to improve the wellbeing
obtained from 150 CYP, where the
of CYP in the school enviroment. It
resilience project were contacted for
offered consultations for school staff,
support, indicates that a key theme of
local authority education inclusion/
the request related to developmental
engagement services, and educational
trauma (33% of requests). A number of
psychologists, to think about the needs
previous referrals to mental health and/
of individual CYP, service suitability and
or Neurodevelopmental services were
signposting. It also provided bespoke
available for 101 CYP, of these 83 (82%)
psychologically- informed interventions
had been referred to either mental health/
for families, utilising a collaborative and
neurodevelopmental or both at least once
formulative approach.
and 55 (46%) had received 2 or more
referrals. See Figure 6 for further details.
Request for support (n=128)
Teacher
19% PMHS
5%
Other
40% Headteacher
2%
CAMHS
2%
ALNCo
32%
Figure 5. Request for support origin for CYP discussed at Resilience Project consultationMental Health Foundation Children and young people’s mental health resilience project 27.
Figure 6. Theme of request for CYP discussed in Resilience Project consultations.
Frequency counts of the number of previous referrals to mental health,
neurodevelopmental services and total number of referrals
Theme of request: CYP who have contacted the Resilience Project (n=135)
Developmental Undiagnosed
Developmental trauma trauma neuro-
(non-LAC) developmental
6%
(post-adoption)
D
9% 24% traits
H
D
7%
A
Educational
concerns
Other
11%
11%
Mental
health
32%
Simple bar count of number of
neurodevelopmental referrals (n=101) Simple bar count of number of
50 mental health services referrals (n=101)
Number of children
Number of children
46
and young people
and young people
40 40
37 37 38
30 30
20 20
10 10 12
10 5 2 4
1 8 2
0 0
0 1 2 3 4 5 0 1 2 3 4 5
Number of mental health services referrals Number of mental health services referrals
Simple bar count of total numner of referrals (n=101)
30
28
Number of children
and young people
25
23
20
18
15
15
10
9
5
4 1
3
0
0 1 2 3 4 5 6 8
Total number of referrals (mental health & neurodevelopmental)Mental Health Foundation Children and young people’s mental health resilience project 28.
Figure 7. Referral location information for CYP receiving a consultation or formulation
Request for support location (n=167)
Cardiff
37% EHWT
6%
PMH
1%
Vale
56%
Autism support team 0%
Educational 0%
Figure 8. Consultation and formulation feedback for confidence
and how consultation will change working practice.
I feel confident using what I have What I have learned will change my
learned in my working practice (n=66) working practice (n=66)
Neutral Neutral
18% 18% Disagree
3%
Strongly Strongly
agree agree
55% Agree 49%
27% Agree
30%
Strongly disagree 0% Strongly disagree 0%
Disagree 0%Mental Health Foundation Children and young people’s mental health resilience project 29.
One hundred and eighty-one CYP to discuss the difficulties arising with
received a professional’s consultation or a CYP, it was a space that brought
formulation session from the Resilience together knowledgeable professionals,
Project. Request for support location that were external to Education. These
information was available for 167 of those discussions provided a platform for open
CYP, see Figure 7. Advice, guidance and conversation about concerns and acted
signposting were provided for 119 CYP as a sounding board to gain support
discussed at consultation. 62 (34% of and encouragement as well as practical
those discussed) CYP were taken into the advice. The development of knowledge
Resilience Project for intervention. and understanding of the type of
behaviours expressed by some CYP was
Sixty-eight education staff gave
enhanced by sharing the evidence base
feedback regarding the formulation
that accompanied it.
or consultation session for a CYP that
they had requested support from ‘Having a clinical psychology insight
the Resilience Project. Over 90% of into what the pupil in question was
attendees agreed that the process was experiencing and how to support
in line with their expectations (96%), (him/ her) with transitioning to the
was easy to access (92%), was at a next stage of secondary education...
time and place convenient (100%) and Support suggestions on how best to
was relevant to their working practice make new relationships.’
(99%). Furthermore, 87% of attendees
‘Able to get a different perspective
agreed that they felt well supported
on the issues relating to the pupils
by the Resilience Project. Moreover,
and specialist insight into other
88% agreed that they can apply what
underlying problems that may be
they have learned into their everyday
impacting them. Also useful to talk
practice. Likewise, 82% felt confident
through and ‘rationalise’ some of the
using what they have learned in their
concerns with specialists in the area.’
working practice. Finally, 79% agreed
‘Collaborative conversation for
that what they had learned will change
forward planning’
their working practice in the future. See
Figure 8 for further information. When considering the least helpful part
of the team formulation the respondents
Qualitative findings
were in the main satisfied. Although
The qualitative feedback from those
acknowledging that the pandemic had
who accessed the ‘team consultation
changed the way of delivery, it was also
and formulation’ was positive. The main
noted that the pandemic had a negative
theme for staff was the reassurance
impact on the benefits of face-to-face
and practical advice given by the team.
meetings for the team formulations.
This was not simply a space created
Some also highlighted aspects that,Mental Health Foundation Children and young people’s mental health resilience project 30.
interestingly, were in contradiction spend time in schools working directly
to the above positive narrative. Some with the teachers. It was felt that the
staff found that not enough time was teachers were best placed to highlight
taken in providing advice and practical the CYP that would benefit most from
strategies that could be used in schools. involvement with the Project staff.
This was coupled with the wish for
‘Being able to access the project for
additional capacity and time to use the
pupils when the need arises. I now
expertise of the Resilience Project and
know how to make this referral. I think
some difficulties in the accessing the
it would be more helpful for the project
Resilience Project.
to make direct contact with school
‘There was relatively little time to staff, who are usually the professionals
discuss with member of staff how this ‘most concerned’ with pupils and in
would be translated into practical the best position to carry out any
classroom approaches/strategies. agreed actions. EPs [Educational
It was discussed at the end but Psychologists] tend to have very limited
this was relatively brief due to time contact with pupils and families due to
constraints.’ the current nature of service delivery.’
‘Specific advice, for example ‘I would like the Resilience Project
creating a calm/safe box, easy to to have first-hand experience of the
implement tips and strategies to try. school environment to enable further
discussion about new strategies that
Coming up with a satisfactory
have been recently put into place such
solution for this child’s complex
as the Bridge Intervention and the
needs’
Graduated response for Climate and
‘This has been a positive experience
Behaviour.’
and the only negative is that we
‘An opportunity to have more
can’ t do a team formulation meeting
clinical psychology sessions for the
for every pupil that needs it.’
Engagement Service to access for
‘I wasn’ t anticipating help, I was
mainstream schools.’
making referrals on behalf of
General advertisement and knowing
Inclusion Services. It was helpful to
about the Resilience Project offer, was also
know how I could make referrals in
noted by one staff member as an area for
the future.’
improvement.
Suggested changes that could improve
‘Potentially, my limited knowledge
the project were also requested from
of what the project involved. Maybe
staff. These echoed a wish for face-to-
a brief introduction regarding the
face contact, additional capacity and
purpose and scope of the project from
to have the Resilience Project staff
the outset would be helpful?’Mental Health Foundation Children and young people’s mental health resilience project 31.
This was also a point of attention for a parent. Another comment worth noting was that
of a staff member who noted the need
‘People need to know about the
for the involvement of a Welsh speaker.
Resilience Project and what they do
and how to get engage with them. ‘Having a Welsh speaker who would
Schools need to know of RP too and be able to offer advice/work with
what they do, what they can provide pupils in Secondary setting.’
for schools and parents.’Mental Health Foundation Children and young people’s mental health resilience project 32.
Group work
Delivery and evaluation
Direct
The groupwork provision of the
intervention
Group Resilience Project uses storytelling
work
to develop confidence in talking
Consultation & about emotions and communication
team formulation skills. Adapted from the ‘Feelings are
Funny Things’ model, which has been
Training
recognised as best practise for Children
Looked After in schools in Wales. This is
Resources
a six-session group program for school
staff, to support the development
of children’s emotional literacy. The
Supporting literature
Resilience Project has also developed
The penultimate part of the service a single session plan to encourage the
model for the Resilience Project is group discussion and exploration of feelings of
work. Group work has been successfully loneliness and isolation from COVID -19.
utilised to support CYP as well as
Seven groups are planned in secondary
parents and carers of children who
schools across Cardiff and the Vale
have experienced poor mental health
for the summer term 2021. The groups
or ACEs. For example various group
will be run by Resilience Workers in
interventions have been evaluated to
conjunction with school staff. The
support children who have experienced
intention is for schools to run the
trauma (Colegrove et al., 2019; Mitchell
groups independently in future, building
et al., 2007) and anxiety (Haugland et
capacity within the education sector.
al., 2020; Pandya, 2017). There is also
evidence supporting the effectiveness A small-scale evaluation of the groups is
of programs aimed at parents and to planned following these initial sessions in
prevent future risk of maladaptive 2021. It is also hoped that more groups
behaviour or health adverse behaviour in will start across Cardiff and the Vale, as
children (Borden et al., 2010; Brennan et well as continued training in using stories
al., 2016). and storytelling techniques.
The restrictions due to the pandemicMental Health Foundation Children and young people’s mental health resilience project 33.
had an enormous impact on the delivery however Resilience Project staff have
of groups. They were initially planned anticipated that the content of the
for the Summer term 2020 and again groups would not be easily adapted to
in the Spring term 2021 but this was online and therefore not be as beneficial
not possible. Groups can be run online, as face-to-face sessions.
Direct intervention
As such interventions were multi modal
Direct
intervention
with a range of models being drawn
upon as appropriate including Dyadic
Group
work
Developmental Psychotherapy (DDP),
traditional and Third Wave Cognitive
Consultation &
Behavioural (CBT), systemic and
team formulation
behavioural approaches.
Training
CBT is an umbrella term for
psychological therapy founded in
Resources behavioural and cognitive theories of
human psychology, established by Aaron
Beck (Beck et al., 1979). The premise
Supporting literature for CBT is based on the concept that
The final level of the Resilience Project thoughts, feelings and behaviours are
service model is direct intervention. interconnected and that by challenging
Resilience project intervention lasted negative thought patterns you can
up to 12 sessions and could be carried improve how you feel (NHS, 2019).
out with CYP individually, CYP and their CBT is now one of the worlds most
families or indirectly with parents/carers researched psychological therapies
or school staff depending on identified (Beck, 2005) and is recommended by
needs. The interventions that were National Institute for Health and Care
provided within the Resilience Project Excellence for the treatment of a range
are based on individual formulations of of mental health diagnoses in CYP
the child’s needs and subsequently a including, but not limited to, depression,
bespoke intervention plan was created. anxiety, Obsessive Compulsive DisorderYou can also read