CASH AND VOUCHER ASSISTANCE IN RESPONSE TO THE COVID-19 PANDEMIC - LESSONS LEARNED FROM A CARE MULTI-COUNTRY PROGRAM JUNE 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

CARE Cash and Voucher Assistance CASH AND VOUCHER ASSISTANCE IN RESPONSE TO THE COVID-19 PANDEMIC LESSONS LEARNED FROM A CARE MULTI-COUNTRY PROGRAM JUNE 2021

Acknowledgements
This report was written by Sani Dan Aoude, Cash and Markets Officer at CARE.
The author would like to thank all project focal points and other CARE staff from the six countries studied in this report
who graciously participated in interviews and replied to numerous requests for data. Special recognition is due to Holly
Radice Welcome, CARE’s Global Cash Market Advisor, who provided valuable guidance on the design and review of this
study.
Acronyms and Abbreviations
AAR After Action Review queer/questioning, and intersex plus
ATM Automated Teller Machine MNO Mobile Network Operator
CLARA Cohort and livelihoods and risks analysis MEB Minimum expenditure basket
CNSA Haitian National Food Security Commission NGO Non-governmental organization
COVID-19 Coronavirus disease 2019 PDM Post-distribution monitoring
CVA Cash and Voucher Assistance RCCE Risks communication and
FONAMIH Foro Nacional Para Las Migraciones community engagement
en Honduras/National Forum RGA Rapid gender analysis
on Migration in Honduras SSN Social safety nets
FSP Financial service provider UN United Nations
GBV Gender-based violence VSLA Village Savings and Loan Association
HNO Humanitarian needs overview WHO World Health Organization
IPC Integrated Food Security Phase Classification WRO/WLO Women Rights Organizations/
KIIs Key informant interviews Women Led Organizations
KYC Know your Customer regulations
LGBTQI+ Lesbian, gay, bisexual, transgender,
2 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 Pandemic
CONTENTS
Acknowledgements. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Acronyms and Abbreviations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
EXECUTIVE SUMMARY 4
How Gender Sensitive Were the Processes for CARE’s CVA?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
How Gender Sensitive Were the Intended Outcomes of CARE’s CVA? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Lessons Learned and Recommendations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1. INTRODUCTION 6
1.1 Purpose and Research Questions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
1.2 MARS COVID-19 Response Program. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
1.3 CARE’s CVA Strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2. CVA IN THE MARS-FUNDED PROGRAM: ONE TOOL, DIVERSE PURPOSES 8
3. METHODOLOGY 10
4. FINDINGS 11
4.1 Program Design and Implementation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
4.1.1 Identification of Needs and Modality decisions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Transfers Values and Frequencies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
4.1.2 Targeting Process and Reaching the Most Vulnerable . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
4.1.3 Delivery Mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
4.1.4 Risk Assessment and Mitigation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
4.1.5 Localization: Working with Local and/or Women-Led Organizations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
4.2 CVA Outcomes: Meeting the Diverse Needs of Program Participants. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
4.2.1 Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
4.2.2 CVA Reach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
4.2.3 Transfer Amount. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
4.2.4 Use of Multipurpose Cash . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
4.2.5 Decision-Making. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
4.2.6 Participant Satisfaction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
4.2.7 Asset Recovery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
5. CONCLUSIONS AND LEARNING 24
5.1 How gender sensitive were the processes for CARE’s CVA?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .24
5.2 How gender sensitive were the intended outcomes of CARE’s CVA? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
6. LESSONS LEARNED AND RECOMMENDATIONS 26
ANNEX I: KEY INFORMANT INTERVIEW PARTICIPANTS 28
3 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 Pandemic
EXECUTIVE SUMMARY
In April 2020, CARE received a five million dollar grant from MARS to implement a multi-country program, including Cote
d’Ivoire, Ecuador, Ghana, Guatemala, Haiti, Honduras, India, Peru, Thailand, and Venezuela1, with the aim of reducing the
negative impacts of COVID-19 on vulnerable populations, especially women and girls, using complementary and multi-
modal approaches. A key activity of this program was the provision of cash and voucher assistance (CVA) to vulnerable
populations to meet their diverse basic needs. Program data indicated that CVA was implemented in Cote d’Ivoire,
Ecuador, Ghana, Guatemala, Haiti, Honduras, and Thailand. Monitoring data from different countries showed that CVA
was unconditional; with cash modality representing 95% of transfers. Key targets populations for CVA activities vary by
country and include: vulnerable households (Cote d’Ivoire, and Haiti); migrants and refugees (Honduras, Ecuador, and
Thailand); domestic workers (Guatemala and Ecuador); survivors of GBV and other forms of violence against women
(Guatemala and Ecuador); and lesbian, gay, bisexual, transgender, intersex, and queer/questioning (LGBTQI+) individuals
(Ecuador). Across all projects (or countries), participants reported numerous uses of CVA including purchase foods stuff,
payment of health services, hygiene services, rental/housing, savings and livelihoods activities.
Given the nature and scale of this program as well as its organizational commitment to learning, CARE was keen
to understand the extent to which the project supported and protected vulnerable populations against the loss or
disruption of their livelihoods in a gender sensitive manner. The study seeks to provide open-source learnings for peer
companies and agencies on how CVA was utilized in this program with two major questions: (i) How gender sensitive was
the process for CARE’s CVA? (ii) How gender sensitive was the intended outcome of CARE’s CVA?
This documentation report compiles lessons from across the projects implemented in the targeted countries and draws
from the diversity of their experiences to provide some recommendations on more gender sensitive CVA in the future.
1 Ecuador, Guatemala, Haiti, Honduras, Peru, and Venezuela were included as part of the dynamic programming approach.
4 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 Pandemic
How Gender Sensitive Were the Processes for CARE’s CVA?
Based on an analysis of the projects, the following aspects were noted that contributed to a gender sensitive processes:
■ Uptake of Rapid Gender Analysis and other data sources;
■ Working with the most vulnerable and marginalized populations;
■ Combination of modalities and delivery mechanisms to deliver CVA;
■ Partnerships with local organizations including VSLA and volunteers;
■ After Action Review (AAR) in some countries to reflect on the CVA process, outcomes, challenge, enablers as
well as what changes are needed to improve “readiness” for a gender sensitive CVA;
■ Linkage with existing CARE programs
Despite these considerable efforts to reflect into practice the CARE gender sensitive CVA process, some points that may
have hindered the intended impact of the interventions, including:
■ Lack of systematic analysis of CVA related risk, including GBV;
■ Sub-par monitoring systems: The review found that there was no harmonization of indicators across all the
countries and standard indicators for CVA were not used.
How Gender Sensitive Were the Intended Outcomes of CARE’s CVA?
Assessing the data there are two points that stand out that contributed to CVA with gender sensitive outcomes including:
Meeting diverse needs of recipient: The provision of Multipurpose Cash assistance offer recipient the flexibility to use
the transfers according to their priority needs. The results of the PDM surveys showed that transfers were used to meet
a variety of needs across countries and targets groups.
Decision making over the use of transfers: In the two contexts where it was measured, it was clear that cash transfers
allowed women to participate in decision-making on the use of resources within the household. However, the lack of
baseline data makes it difficult to assess the effect of the transfers compared to before they were given.
Lessons Learned and Recommendations
The MARS program offered an extensive use of CVA in multiple contexts during unprecedented times. In general, the
transfers had positive impacts and pointed towards an application of CARE’s gender sensitive approach. Based on the
findings from the study, the following recommendations are made for similar future interventions using CVA:
Invest more in preparedness for CVA: For future programming, it is critical to (i) build more technical capacities and (ii)
develop partnerships with various FSPs to better and faster implementation of efficient CVA.
Building a strong monitoring system: For future programs, it is strongly recommended that a minimum of two to three
common indicators (with disaggregated targets) are identified for easy assessment of program performance and potential
comparison between countries.
More cash is needed for basic needs and recovery: The economic loss that resulted from the COVID-19 pandemic was so
large that a one-off cash distribution was not enough to help many people in meeting their basics needs or starting/
resuming livelihoods activities.
Linking CVA to VSLA: The review highlighted the important role of VSLAs for communities during a crisis such as the
COVID-19 pandemic: as facilitators for the implementation of programs but also and especially for the role of support or
safety nets to their members.
5 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 Pandemic
1. INTRODUCTION
1.1 Purpose and Research Questions
Founded in 1945 with the creation of the CARE Package®, CARE is a leading humanitarian organization fighting global
poverty. CARE has more than seven decades of experience delivering emergency aid during times of crisis. In response
to the unprecedented disruptions and needs caused by the Coronavirus 2019 (COVID-19) pandemic, CARE provided
lifesaving and early recovery support to the most vulnerable populations, particularly girls and women affected by the
impacts of the pandemic. In response to the pandemic, CARE received a five million dollar grant from MARS to implement
a multi-country program with the aim of reducing the negative impacts of COVID-19 on vulnerable populations, especially
women and girls, using complementary and multi-modal approaches.
A key activity of this program was the provision of cash and voucher assistance (CVA) to vulnerable populations to
meet their diverse basic needs. Given the nature and scale of this program, as well as its organizational commitment to
learning, CARE was keen to understand the extent to which the project supported and protected vulnerable populations
against the loss or disruption of their livelihoods in a gender-sensitive manner.
This study seeks to provide learnings on how CVA was utilized in this program with two major questions:
■ How gender sensitive was the process for CARE’s CVA?
■ How gender sensitive was the intended outcome of CARE’s CVA?
6 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 Pandemic
1.2 MARS COVID-19 Response Program
The outbreak of COVID-19 followed by the World Health Organization (WHO) declaration of a pandemic in March 2020
resulted in a set of restrictions implemented by governments worldwide to limit the spread of the disease (e.g., closures
of borders and markets, travel restrictions, lockdowns, etc.). This caused devastating socioeconomic disruptions, such as
income loss, business closures, and stress, for the most vulnerable populations, especially women and girls.
The MARS program in CARE was implemented as a series of projects in Cote d’Ivoire, Ecuador, Ghana, Guatemala, Haiti,
Honduras, India, Peru, Thailand, and Venezuela. The funding aimed to enable CARE to deploy urgently needed support
quickly and efficiently as the crisis spread while filling gaps related to delays in institutional funding. This year and a
half long program aimed to cover multiple sectors (e.g., food, nutrition, livelihoods, health, gender-based violence (GBV),
and education) using different modalities such as CVA, in-kind support, technical assistance, and risks communication
and community engagement (RCCE).
1.3 CARE’s CVA Strategy
The humanitarian aid landscape has undergone numerous
reforms in the past two decades, particularly with the introduction
and scale up of CVA. Within CARE the use of CVA has gradually
gained momentum with research and evidence documenting the Responds to Recognizes
efficiency and effectiveness of programming with cash transfers unique needs diversity within
of all genders gender groups
and vouchers. CARE’s leadership envisions CVA as a springboard
that the organization needs to realize its vision of a more focused,
more agile, more horizontal, and more competitive organization
that truly puts women and girls at the center of concerns.
CARE is committed to ensuring that projects with CVA are designed Builds on Avoids exposing
social norms recipients to
with and for women and girls, addressing recipients’ needs, work harm and risk
challenges, and opportunities. CARE has invested in research
on how to make CVA work for women and girls through gender
sensitive approaches to framing processes and outcomes of the
modalities. CARE’s approach to gender sensitive CVA is based
on four key elements: (i) responding to the unique needs of all FIGURE 1: CARE’S DEFINITION OF GENDER-
genders; (ii) recognizing diversity within gender groups; (iii) SENSITIVE CVA
avoiding exposing recipients to harm and risk; and (iv) building
on social norms work.
7 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 Pandemic
2. CVA IN THE MARS-
FUNDED PROGRAM: ONE
TOOL, DIVERSE PURPOSES
While the program as a whole covered ten countries, CVA was used in seven countries: Cote d’Ivoire, Ecuador, Ghana,
Guatemala, Haiti, Honduras, and Thailand. CVA was initially included in the proposal for India. However, during the
planning of the activity, a new regulation on foreign funding for Non-Governmental Organizations (NGOs) issued by the
Indian government obliged CARE to suspend the use of these modalities in India.
Though this program is implemented in different contexts, all of these actions have the intended outcome of supporting
affected populations to meet their needs including protection. However, some countries – such as Cote d’Ivoire and
Ghana2 – included livelihoods protection or recovery objectives. Five countries used cash transfers (electronic and cash
in hand); two countries combined cash transfers with vouchers (electronic and paper). Honduras used only vouchers
(electronic). Key targets populations for CVA activities also varied by country and included: vulnerable households (Cote
d’Ivoire and Haiti); migrants and refugees (Honduras, Ecuador, and Thailand); domestic workers (Guatemala); survivors
of GBV and other forms of violence against women (Guatemala and Ecuador); and lesbian, gay, bisexual, transgender,
intersex, and queer/questioning plus (LGBTQI+) individuals (Ecuador).
2 At the time of writing CARE Ghana’s project was ongoing. There will be an additional report specifically on that intervention.
8 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 PandemicTABLE 1: SUMMARY OF INTERVENTIONS WITH CVA
DELIVERY
LOCATION CVA OBJECTIVE MODALITY MECHANISM TARGET POPULATION REACH
Cote d’Ivoire: Guyeo, Meagui, Securing the living conditions of vulnerable Cash Electronic Cash Vulnerable households and 22,440
and Soubre households due to the COVID-19 crisis. transfer individuals individuals
Haiti: Hinche and Cerca la Improve access to basic food commodities and GBV Cash Cash in Vulnerable and food insecure 2,400
Source municipalities and protection support to strengthen compliance transfer; hand; paper (Integrated Food Security individuals
with government-imposed COVID-19 restrictions to vouchers vouchers Phase Classification (IPC) 3
limit and contain the spread of the virus. and above) households
Ecuador: Ibarra, Manta, Quito, To provide primary emergency assistance through Cash Electronic Migrants and refugees; Local 2,042
Huaquillas, Ambato and CVA modalities in order to cover immediate basic transfer; Cash, populations in vulnerable individuals
Guayaquil needs according to people’s priorities. vouchers paper voucher, conditions; GBV survivors;
electronic LGBTQI+ people
voucher
Thailand: (Raks Thai) Pattani, To support highly vulnerable persons/families Cash Cash in hand Migrants who work in 1,920
Ranong, Rayong, Phang Nga, particularly in the fisheries and seafood processing transfer fisheries and seafood individuals
Phuket and Samutsakom industries in the selected provinces. processing with their families
Guatemala: Retalhuleu, San To safeguard the lives and food security of women Cash Electronic Women domestic workers; 5,208
Sebastián, San Felipe, Nuevo domestic workers, women survivors of violence, transfer Cash; Cash in women victims and survivors individuals
San Carlos, El Asintal, Santa and women who have various occupations hand of violence; women in various
Cruz Mulua, Champerico; excluded in society. occupations
Mazatenango, Santo Domingo,
Santo Tomás La Unión;
Masagua, and Escuintla
Honduras: Tegucigalpa The most vulnerable families will be provided with Vouchers Electronic Women returning migrants 765
food rations and hygiene kits to cover their basic voucher individuals
needs for at least one month.
9 March 2021 : Cash and Voucher Assistance for Sexual Reproductive Health and Rights3. METHODOLOGY
The study mainly used qualitative data collection methods. Tools utilized included key informant interviews (KIIs) with
country project staff and a desk review of the literature (internal and external documents). Quantitative data was used
from the desk review included the analysis of initial program documents, interim reports, post-distribution or satisfaction
survey reports, After Action Review (AAR) reports, and narratives/anecdotes from participants or affected populations.
As a baseline study was not done in advance of this program, there was no existing reference data for CVA related
indicators. Therefore, the study is unable to speak changes over time nor to do a comparison between countries. Due to
the current pandemic, the study did not collect direct (FGD or KII) data from program participants. However, the study did
work to ensure that participants’ perspectives and experiences were drawn out using country specific data.
10 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 Pandemic4. FINDINGS
Within the two objectives and the key elements of gender sensitive CVA, the study aimed to look at decisions on modality,
targeting process, delivery mechanisms, risk assessment and mitigation, and meeting participants’ needs.
4.1 Program Design and Implementation
4.1.1 IDENTIFICATION OF NEEDS AND MODALITY DECISIONS
The MARS program design and the decision to use CVA was informed by numerous assessments and analyses. The Rapid
Gender Analysis (RGA) was the most common data source for the identification of the needs, capacities, and preferences
of affected populations. Representatives for all six countries mentioned utilizing this tool during KIIs. This is a strong
indication of countries’ efforts to put into practice one of the six elements of gender sensitive CVA3.
This data source was complemented by other data sources like country-specific Humanitarian Needs Overview and
Humanitarian Response Plan (HNO/HRP), host government data (i.e., Social Safety Nets program), and other agency data
from previous and ongoing programs with CVA (i.e., Integrated Phase for food security Classification (IPC)).
In Cote d’Ivoire, early in implementation the project team conducted additional field-based data collection and
assessment (e.g., using tools like the Cohort and Livelihoods and Risks Analysis (CLARA)) to confirm the appropriateness
and feasibility of CVA to respond to identified needs. During these assessments, CVA was one of five needs prioritized
by respondents. These findings were used to confirm the choice to provide CVA for livelihoods activities along with the
multipurpose cash assistance.
In Haiti, where the food insecurity crisis was already acute before COVID-19, the decision to use CVA was informed by a
desk review and the desire to fit with government and other interagency standards. In Thailand, the decision to use CVA
3 CARE. (2019). CVA that Works for Women.
11 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 Pandemicwas based on findings from a rapid situation assessment where compensation for lost income was rated as most needed
by affected populations (38.40%); with migrant women prioritizing this need more than men. This was further confirmed
by the gendered impact of the COVID-19 pandemic on migrants in Thailand study (June 2020).
Another reason that led to the use of CVA was the opportunity this grant gave to continue (i.e. Ecuador and Guatemala)
or complement previous and/or ongoing programming (Thailand) with similar activities or targeted populations/areas.
In Honduras, a CVA feasibility assessment was conducted in collaboration with local partner Foro National Para Las
Migraciones en Honduras (FONAMIH) and found that vouchers were the best option for the targeted population in
Tegucigalpa while in-kind distribution was more suitable in rural areas.
TABLE 2: DATA SOURCE USED TO INFORM ON NEEDS AND CVA DECISION
COUNTRY OF GOVERNMENT OR
PRESENCE REGIONAL RGA COUNTRY RGA INTERAGENCY CLARA OTHER
Cote d’Ivoire
Ecuador
Guatemala
Haiti
Honduras
Thailand
TRANSFERS VALUES AND FREQUENCIES
Based on the findings from assessment data and the urgency of identified needs, the majority of the projects provided
multipurpose cash transfers. However, in Haiti and Honduras, the provision of CVA was specifically intended to support
food security outcomes. Cote d’Ivoire provided some specific and targeted individual CVA support (e.g., agriculture
inputs, income generating activities) along with the household support.
Depending on the context, broadly two different approaches were used to determine transfer values. It should be noted
that all transfers were made in local currencies4. These approaches included:
Alignment with government and peer agencies standards: Project teams in Haiti, Honduras and Ecuador used this
approach to determine the transfer value. In Haiti, CARE used the transfer value set by the Haitian National Food Security
Commission (CNSA for its acronym in French). This amount was intended to cover approximately 70% of the value of a
one-month food basket; the remaining 30% was to be covered by the targeted households’ own resources. Each selected
household was provided with $114.6 ($91.7 through commodities voucher and $22.9 USD through a cash transfer).
In Ecuador, a Minimum Expenditure Basket (MEB) was not yet established by the national Cash Working Group. However,
as part of the national Social Protection scheme in response to COVID-19, the government set US$120 as the transfer
value. After consultations with government and other agencies, CARE aligned its transfer value with this figure. It is
worth noting that this value is similar to what CARE provided to participants of a previous CARE’s projects with CVA in
the country. In Honduras, the value of the redeemable voucher was determined according to the cost of the basic food
basket in the country, considering an average of five members per family and a package for approximately one month of
4 However, for the purposes of this report, the transfers amounts/value of are reported in U.S. dollars.
12 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 Pandemicfood consumption in compliance with humanitarian standards. The transfer value was $80, which is the average value
used by the humanitarian actors in the country that are part of the Food Security Group.
Budget availability and ideal package approach: in Guatemala, Cote d’Ivoire and Thailand, CVA transfer values were
set based on either one or combination of these approaches, as there were no standards transfer rates or MEBs in
the countries. Although this approach is not ideal, the project teams in these countries endeavored to ensure that
the transfer values were based on evidence from the field. Within this approach, there was some variation between
countries. In Cote d’Ivoire, the project used the Social Safety Nets (SSN) transfer rate as a reference to determine the
transfer amount for multipurpose cash assistance. However, based on informal feedback from SSN recipients, CARE
increased this amount slightly (+5%), demonstrating efforts to ensure that transfer values allowed targeted populations
to cover their needs. Each targeted household received a one-off transfer of $54.7 to meets their basics needs. For
livelihoods support, the project used a mix of budget availability and ideal package (e.g., food basket) to set the transfer
value. CARE conducted some consultations with traders and Village Savings and Loan Association (VSLA) members who
were implementing small, income generating activities before setting the transfer value.
In Thailand, the transfer value was set based of each targeted family/household needs through a case management
approach. After the identification people in need of assistance, the project team carried out a household needs and
capacities assessment. The findings were then used to identify gaps or severity of needs and then calculated the
monetary value based on price of items and or services in local markets. Overall, the transfer value ranged from $66.6
to $166.6 per family.
In Guatemala teams determined the transfer values based on the monetary value of items and/or services needed (e.g.,
food items, hygiene items, rent, health services, etc.) based on prices in local markets. The project teams conducted some
consultations with markets actors and aid agencies to gather data on the prices of items and services in local markets.
4.1.2 TARGETING PROCESS AND REACHING THE MOST VULNERABLE
Target Groups: The program targeted five different but overlapping populations across the implementing countries.
These groups include domestic workers, migrants, refugees, resident/host communities and LGBTQI+ people in both
rural and urban settings. The reason for targeting these groups was that they were the most affected by the COVID-19
crisis according to numerous assessment findings that informed the design of the program. The review found that four
out of seven projects targeted at least two of these groups. In Ecuador, the project targeted four groups with CVA
(migrants, refugees, host populations, and LGBTQI+ people) in both rural and urban areas/context. In Cote d’Ivoire, and
Haiti only resident households in rural areas were targeted. Table 3 summarizes the various groups targeted by the
project in each country.
13 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 PandemicTABLE 3: CVA TARGET GROUPS BY COUNTRY
COUNTRY OF DOMESTIC
PRESENCE RESIDENTS MIGRANTS REFUGEES LGBTQI+ WORKERS RURAL URBAN
Cote d’Ivoire
Ecuador
Guatemala
Haiti
Honduras
Thailand
Participant Targeting: There were multiple approaches used it in the program to target and register participants. Each
project developed and used specific methodologies with the desire of ensuring participatory and inclusive targeting.
There was a systematic effort to guarantee that most vulnerable groups are selected for the transfers as per CARE’s
mandate and priorities.
The majority of targeted participants (primary recipients) were women and girls. For Haiti, Guatemala, Honduras,
and Thailand, between 80% and 100% of direct recipients were women. This was intentional and was mentioned in
the workplans. The rationale for this decision was that women were more vulnerable and exposed to epidemics and
the socioeconomics impacts as based on assessment findings.5 The final targeting criteria were varied and based on
implementing countries’ CVA objectives. Table 4 provides the list of key criteria used for the selection of CVA recipients
in each country. It is worth to noting that these criteria were not mutually exclusive (i.e. someone may be a single parent,
a refugee and a nursing mother); additionally, if an individual or household meet more criteria, the more they were likely
to be selected.
5 https://www.unwomen.org/-/media/headquarters/attachments/sections/library/publications/2020/policy-brief-the-impact-of-covid-19-
on-women-en.pdf?la=en&vs=1406
14 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 PandemicTABLE 4: TARGETING CRITERIA BY COUNTRY OF PRESENCE
COUNTRY OF PRESENCE CRITERIA
Cote d’Ivoire VSLA members who meet one or more of the following characteristics:
❚ Female-headed household
❚ With children under 5 years old
❚ Pregnant or lactating women
❚ Living in household that has one meal per day
❚ Living in household with people with disability
❚ Living in household with people with a chronic disease
❚ Living in household affected by COVID 19 (COVID-19 cases)
Ecuador ❚ Families in vulnerable conditions who have not received any assistance;
❚ Female-headed households with children and adolescents;
❚ Single women (e.g. women traveling alone);
❚ Families with a single parent (i.e. children living with one parent);
❚ Families with disabled persons or catastrophic severe illnesses;
❚ Women who were pregnant or breast-feeding;
❚ Unaccompanied minors;
❚ LGBTQI+ individuals or couples;
❚ Women survivors of GBV;
❚ The elderly.
Guatemala ❚ Women domestic workers;
❚ Women survivors of violence;
❚ Women in various occupations;
❚ Women survivors of domestic violence.
Haiti Food insecure households (IPC6 3 and above), including:
❚ Pregnant and lactating women;
❚ Child-headed households;
❚ Widowed women;
❚ People with disabilities or chronic illness;
❚ Households headed by women in vulnerable situations.
Honduras ❚ Women returning migrants (e.g. deportees from USA);
❚ Staying in temporary reception centers;
❚ With eventual residence in Tegucigalpa.
Thailand ❚ Jobless;
❚ Unemployed;
❚ People with reduced working hours;
❚ Families with pregnant women;
❚ People with chronic illness;
❚ Families with young children;
❚ Those with house rental issues.
6 Integrated Food Security Phase Classification
15 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 PandemicCommunity Engagement: Community engagement is critical for the ownership of program activities and to prevent
potential tensions or conflicts. Community engagement in the countries of implementation took place primarily at two
key moments of the project: needs assessment and recipient targeting. During the needs assessments, each project team
consulted community representatives, local authorities, and representatives of vulnerable groups (mainly women) to
understand the impacts of the pandemic and preferred responses or modalities. During the implementation, participant
targeting was the principal step where communities (e.g., volunteers, religious leaders, VSLA groups, etc.) were involved.
In Cote d’Ivoire and Haiti, community engagement resulted in the establishment of various committees (e.g., Complaint
and Feedbacks Committees or Targeting committees) to ensure that the communities fully participated, and that their
needs and preferences are considered. In these countries, these committees were established after initial meetings with
communities’ leaders and often with local authorities. Key Informants from these countries mentioned that women were
fully represented in these committees especially in the VSLAs where up to 90% of the members were women.
In Guatemala, Honduras, and Thailand, the principal means
of community engagement was working with local7 or
“We have included highly vulnerable host
corporate8 organizations and volunteers. In Ecuador, where
the project was a continuation of a similar one, the inclusion populations to reduce the risk of tension,
of the host populations among the recipients was the main
stigmatization and xenophobia against
tool for community engagement. The project justified this
approach by the desire to reduce stigma and xenophobia other project participants: refugees,
against the main target group, which was migrants. migrants and LGBTQI+ groups.”
4.1.3 DELIVERY MECHANISMS CARE ECUADOR STAFF
The choice of appropriate and user-friendly delivery
mechanisms is critical to ensure safe and secure access to
CVA. In response to this requirement, numerous delivery mechanisms were used for CVA disbursement. Overall, the
selection of delivery mechanisms in each implementing country was based on two approaches: building on country
experience or drawing on assessment findings. The delivery mechanisms were banks, microfinance institutions, electronic
cash, including mobile money (via MNO) and ATMs, paper and electronic voucher and direct cash.
TABLE 5: DELIVERY MECHANISM USED TO PROVIDE CVA
COUNTRY OF ELECTRONIC
PRESENCE CASH IN HAND ELECTRONIC CASH VOUCHER PAPER VOUCHER
Cote d’Ivoire
Haiti
Ecuador
Thailand
Guatemala
Honduras
7 FONAMIH
8 Domestic workers Organizations in Honduras
16 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 PandemicHaiti and Guatemala used a combination of two delivery mechanisms to reflect participants’ needs and capacities. In
Haiti, the project built on CARE’s experience and provided paper vouchers and cash in hand. This decision was motivated
by several reasons including the low coverage of digital services in the targeted areas, low literacy (including digital)
levels of participants, familiarity of participants with the proposed delivery mechanisms, and the desire to save time
since CARE Haiti has agreements with local vendors and financial service providers (FSPs). The project organized COVID-
compliant fairs where participants exchanged their vouchers for dry food items with local suppliers. Food items and
quantities were established to allow the participants to access a rich and varied diet. The distribution of cash transfers,
through an FSP, was organized on the same day as the fairs. The participants received their transfer after redeeming their
vouchers. The cash transfer supplement was intended to allow households to access fresh food products (e.g., fish, meat,
vegetables, eggs, etc.). While this strategy was efficient for allowing access to diverse foods items, it led to a lengthy
distribution process during a very sensitive time like the COVID-19 pandemic. The project team mentioned that they did
extended the duration of distribution time to ensure that each participant received the full ration (cash transfer and
voucher), increasing the risk of exposure to the virus. According to the post-distribution monitoring (PDM) survey results,
23.81% of recipients spent more than one hour at the site before receiving assistance.
Similarly, in Ecuador, the project built on CARE’s previous experience to deliver CVA through “cardless” ATMs. A number
of factors support this decision, including the familiarity and acceptance of participants, lack of valid documentation to
meet Know Your Customer (KYC)9 regulations, duty of care given the ongoing pandemic, and the effectiveness of this tool.
CARE signed a contract with a local bank; CARE was in charge of generating the codes for withdrawals at ATMs without
cards, and for sending them via SMS or phone calls to participants. Building on previous lessons learned, CARE technical
staff accompanied the participants so that they could make the withdrawal without problems. The PDM survey results
indicated that this delivery mechanism fit well with participants’ capacities and preferences: 98% affirmed that the ATM
mechanisms was accessible and safe. Only 6% reported that they experienced some issue during the process of money
withdrawal.
In Honduras, electronic vouchers (gift cards) were provided to participants after a feasibility analysis that indicated that
participants could access the supermarket chain in various locations in the city. In Cote d’Ivoire, mobile money was
following an assessment indicating that 83% of participants had access to cell phones and 76% did not have safety and
security concerns in receiving the transfers through mobile payments. The PDM data found that 96% of participants were
satisfied with the delivery mechanism, indicating alignment with recipients’ preferences and capacities. Ninety-seven
percent of respondents were satisfied with their relations with agents where they cashed out the transfers.
In Guatemala, CARE used two delivery mechanisms based on accessibility and capacities of the participants--a bank and
mobile money. The project team thought it was strategic to use these two delivery mechanisms to provided options for
participants. It was also an opportunity for the CARE Guatemala team and partners to use a new FSP via mobile money.
Each participant was accompanied to fill out the forms required for the delivery mechanisms. Both delivery mechanisms
required the direct accompaniment of the participants for the presentation of adequate information; however, the
deadlines established for the execution of the project were met. For participants who were under 18 years of age, they
could not receive transfers from the bank and mobile money, as they did not meet the KYC requirements; they were
referred to in-kind assistance.
In general, the transfers through the bank worked well in Guatemala as it helped the project provide quality attention
for participants. The banks attended the participants at dedicated times. This, however, did cause some issues at not
all participants were able to arrive during that window of time. CARE and partners needed to reschedule the pick-ups at
later dates, thus delaying some transfers.
9 “This usually refers to the information that the local regulator requires financial service providers (FSPs) to collect about any potential new
customer in order to discourage financial products being used for money laundering or other crimes. Some countries allow FSPs greater flexibility
than others as to the source of this information, and some countries allow lower levels of information for accounts that they deem to be ‘low
risk’”. CaLP 2018.
17 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 PandemicWith mobile money in Guatemala, the Mobile Network Operator (MNO) required that participants fill out various forms
and provide high quality pictures/scans, but most participants did not have high quality cameras in their phones. In
the case of transfers through mobile phones, the service in the departments was poor due to poor customer service
and limited availability to serve a large number of people. The team and partners underestimated the amount of time
required for the registration for mobile money, which provided to be heavy. A team member was assigned to this task as
participants were often unable to manage the application alone.
In Thailand, direct cash in hand was used because of lockdowns ordered by the government in areas with seafood
factories. Additionally, many of the participants did not have valid documents to access transfers through other delivery
mechanisms like ATMs or mobile money.
4.1.4 RISK ASSESSMENT AND MITIGATION
CVA is not riskier than other modalities. However, it does have elements that can increase risks to participants, agencies,
and partners. Identification of CVA-related risks and mitigation measures are critical steps for program design and
implementation. However, risk assessments in this MARS-funded program was not done systematically in all projects.
The risks associated with fraud and corruption were addressed according to CARE standards and donor requirements in
all countries. Nevertheless, risks related to individuals’ safety were addressed differently in each context.
In Cote d’Ivoire, the project team used the GBV in CVA Risk Assessment Tool. Key risks identified through this assessment
included: abuse at cash out by agents; physical violence; denial of resources; and psychological violence. To mitigate
these risks, the project identified and implemented activities including sensitization campaigns before the distribution
and a feedback and complaint mechanism. During the assessment, the project team used CLARA to identify risks that
might hamper participants’ livelihoods activities.
In Guatemala, the main risk identified was violence related to household level decision-making on the use of the transfer,
since one of the main concerns/problems in the project area was domestic violence. To mitigate these risks, designated
CARE and partner staff called each of the participants to talk about the transfer and how to use the money and promote
the use of the transfer by the women. There were parallel discussions with recipients and virtual accompaniment.
In Thailand, a major issue was how to deliver CVA to undocumented individuals and people under lockdown. The latter
in turn encouraged the use of cash in hand, though this had certain security risks in the delivery of the transfer. For the
other countries, including Haiti, Honduras and Ecuador there were no specific assessments of CVA-related risks. However,
these issues were addressed through complementary activities like awareness and GBV prevention and response.
4.1.5 LOCALIZATION: WORKING WITH LOCAL AND/OR WOMEN-LED ORGANIZATIONS
CARE is committed to delivering its programs in partnership with others including, but not limited to, peer NGOs, local
and national governments, the United Nations (UN) agencies, Women’s Rights and Women-Led Organizations (WRO and
WLO), community-based organizations (including VSLAs), and the private sector. This commitment was upheld by the
MARS-funded program. The program worked with four types10 of civil society organizations: association, cooperative,
workers union and local NGOs.
In Honduras, CARE partnered with FONAMIH, a local NGO that specializes in providing support to migrants and other
marginalized groups. FONAMIH was in charge of housing the women who were returning migrants while in quarantine at
the reception center; FONAMIH also connected to the FSP, the supermarket chain, where e-voucher were redeemed for
foods items.
In Guatemala – where the project targeted mainly women domestic workers – CARE worked with twelve local organizations
10 CARE International. (2021). Partnership in CARE.
18 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 Pandemicthat support women domestic workers, survivors of GBV and other types of violence, as well as other marginalized groups.
CARE Ecuador implemented the project in partnership with the National Secretariat of Human Rights, a government
entity, in the municipalities of Guayaquil and Ambato; UNTHA (National Domestic Workers Union) in the municipality of
Guayaquil; Alas de Colibrí Foundation in the municipality of Quito and others; and the LGBTQI+ local movement in the
municipality of Quevedo.
In Haiti and Cote d’Ivoire, where the project was implemented in rural areas and VSLA groups. In Côte d’Ivoire VSLA
promoters played a key role during the assessment and participant targeting since women VSLA members were the main
target population for the project.
4.2 CVA Outcomes: Meeting the Diverse Needs of Program Participants
4.2.1 MONITORING
Monitoring systems are critical to effectively assess project design, implementation, and outcomes. All projects used
digital data collection systems due to the pandemic. The PDM survey is the most widely used monitoring tool in five
countries, including Cote d’Ivoire, Haiti, Ecuador, Thailand and Guatemala. Honduras had planned to conduct a PDM
but was unable to do so due to an emergency within an emergency. The impacts of hurricanes ETA and IOTA modified
the priorities and planning for the humanitarian response in the country. Another important monitoring tool used by
the program was the AAR. This was used by three countries, including Haiti, Guatemala and Honduras to reflect on
CVA processes and outcomes as well as “what changes are needed” to improve their “CVA readiness”. Cote d’Ivoire
completed an AAR for the whole project (i.e. not specific to CVA).
The monitoring system for this program appears to be one of the least robust elements. The review of the project work
plans from the various countries showed that there was no harmonization of CVA indicators to monitor. Most of the
indicators used are related to outputs/process, making it difficult to measure outcomes changes. Both Cote d’Ivoire
and Thailand have defined two to three indicators related to cash transfers in their proposal work plans based on
CARE’s global indicators for the response to COVID-19. In Guatemala, Honduras and Ecuador, there was no specific CVA
indicators in their project work plans. The review found that targets for CVA indicators were not disaggregated by gender,
which contradicts CARE’s policies and standards. The following table presents the indicators used in the projects for the
teams in Cote d’Ivoire and Thailand none of which were disaggregated by gender.
19 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 PandemicTABLE 6: CVA-RELATED INDICATORS
COUNTRY CVA-RELATED INDICATOR
Cote d’Ivoire # of people provided with additional food or cash support, in the form of either cash/voucher
assistance or transfers in kind (including fortified/complementary foods)
# of people receiving cash in response to COVID-19
Thailand # of people provided with additional food or cash support in the form of either cash/voucher
assistance or transfers in kind (including fortified/complimentary foods)
% of people who received food packages or cash and reported that the support had helped them
significantly in terms of meals or ability to cope with financial difficulty
4.2.2 CVA REACH
In total, the program reached 36,040 people with CVA. The overwhelming majority of these people were women and girls.
Ecuador is the only country where LGBTQI+ people were deliberately targeted, and their participation was measured by
the team.
TABLE 7: NUMBER OF PEOPLE REACHED WITH CVA
COUNTRY OF PRESENCE MALE FEMALE LGBTQI TOTAL
Cote d’Ivoire 5,304 18,700 24,004
Ecuador 906 1,116 20 2,042
Guatemala 2,552 2,656 5,208
Haiti 1,142 1,248 2,400
Honduras11 134 765
Thailand 669 1251 1,920
TOTAL 10,573 25,105 20 36,339
4.2.3 TRANSFER AMOUNT
Program distributed more than US$400,000 in transfers to recipients. The vast majority (95%) of this amount was
distributed cash transfers with Cote d’Ivoire leading this number followed by Ecuador and Thailand.
11 These numbers are based on the average household figure. CARE Honduras did not collect specific data on the gender of household members. It
is likely that some boys and men were reached, but the data is incomplete.
20 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 PandemicTABLE 8: TOTAL AMOUNT OF CASH DISTRIBUTED
COUNTRY OF PRESENCE CASH VOUCHER TOTAL
Cote d’Ivoire $180,320 $180,320
Ecuador $72,840 $72,840
Guatemala $57,861 $57,861
Haiti $36,680 $9,160 $45,840
Honduras $10,720 $10,720
Thailand $60, 625 $60, 625
TOTAL $408,146 $19,880 $428,026
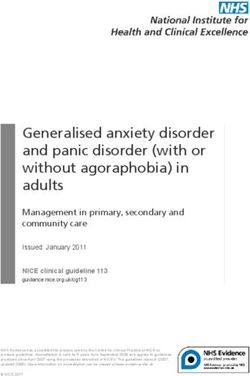
4.2.4 USE OF MULTIPURPOSE CASH
In Cote d’Ivoire, Ecuador, and Guatemala, 67% of the recipients on average used the cash transfer to purchase foods
items. Other principal expenditures reported by recipients included: health/medicine (19%); rent/accommodation (15%);
utilities (12%); hygiene items (11%); and savings/livelihoods (10%). However, there was some variation between these
countries, with the majority of recipients in Ecuador and Guatemala– 91% and 80%, respectively – who used the transfers
on food items, whereas relatively few (29%) recipients in Cote d’Ivoire did so.
While it is difficult to pinpoint the cause of this 100%
Ecudador
variation, there are several potential reasons:
Guatemala
(i) diverse contexts and target populations with 80% Cote d’Ivoire
specific needs and priorities; (ii) these countries Average
60%
did not formulate the question of cash transfer
use in the same way; and (iii) in the case of Cote 40%
d’Ivoire, some of the participants received cash
transfers to support their livelihoods, potentially 20%
explaining the number of recipients spending on
livelihoods activities. The timing of the transfer 0%
Food Health Rent Utilities Hygeine Saving
in correlation with the level of contagion, coupled Livelihoods
with quarantine measures could have also been FIGURE 1: MULTIPURPOSE CASH (MPC) USE: % OF PARTICIPANTS
factors in this variation.
In Thailand, the PDM survey indicated that the overwhelming majority of cash transfers were used to cover food and house
rental (74%). CVA recipients also used cash transfers to access civil documentation-such as birth registration document,
migrant health insurance cards (4%), payment of medical care (9%), childcare (7%) and livelihoods/business (6%).
In Haiti, where CVA was intended to support food security outcomes, the PDM results indicated that 100% of the recipients
declared that the CVA allowed them to cover their food needs for four weeks. Although the cash was intended to support
household access supplementary food items (fresh food), participants were able to use a portion of cash for other
purposes such as medicine, education, and savings (participation in VSLAs).
21 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 Pandemic4.2.5 DECISION-MAKING
In all projects, the majority of CVA recipients 100%
were women. There is the potential that would Guatemala
expose them to more risks, but it can also be 75%
Cote d’Ivoire
an opportunity for them to engage more and to
Average
fully participate in decision-making processes. 50%
While decision-making over the use of CVA is an
important indicator for the CARE gender sensitive 25%
CVA approach, only two projects (in Guatemala
and Cote d’Ivoire) collected data on this indicator.
0%
However, there was no baseline data in either Joint decision Individual decision Other family members
context, which makes it difficult to do any type of
comparison before and after the distribution. In FIGURE 2: DECISION-MAKING OVER THE USE OF CASH
terms of results, there were significant variations
between these two countries. In Guatemala,
more than 80% of recipients declared that they
individually determined how to use the cash “The project targeted people who are vulnerable. It
transfer; 8% reported that family members made was the first time I participated in a project. I was
this decision and 1% reported that it was a joint/
served with dignity. I was satisfied with the food
couple decision. On the other hand, in Cote
d’Ivoire 55% of recipients reported that decisions basket (voucher) and the cash (transfer). With this
around the use of cash were made jointly/as a
money, I was able to buy other ingredients to add to
couple. Twenty-one percent (21%) reported that
the decision was made by the individual decision; the other products received. I say thank you to the
7% of participants reported that the husband people in charge of the project who allowed me to
made the decision12; and 2% reported that other
family members made the decision. participate in this project. I was very satisfied.”
Decision-making is based on context and gender FEMALE PARTICIPANT, HAITI
roles; this data point in isolation of the baseline
is difficult to analyze for patterns. Although this
study did not identify specific reasons for this
variation, the fact that in Cote d’Ivoire most of the CVA recipients were VSLA members may have contributed to this
phenomenon. Indeed, numerous CARE13 and others peer agencies studies have demonstrated that women and girl’s
participation in VSLA groups is strongly connected to an increased participation in decision making process (both at
household and community level). Furthermore, in Guatemala as the majority of the use of the cash transfer was on food,
which traditionally is a role filled by women in the context.
4.2.6 PARTICIPANT SATISFACTION
Participant satisfaction is a fundamental pillar of humanitarian assistance. Questions related to participant satisfaction
on the CVA processes were included in some PDM surveys. In Ecuador, 98% of surveyed participants were satisfied
with the assistance received. An additional 99% of participants mentioned that the cash transfer was received in a
timely manner. Regarding the transfer value, 83% of participants felt that the amount of the monetary transfer was
enough, while 17% mentioned that it was not sufficient, which makes sense in a context in which the needs of vulnerable
populations are increasing daily.
12 This information is not included in the below graphic for ease of comparison.
13 CARE Nederland, 2021 Influence of Savings Groups on Women’s Public Participation
22 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 PandemicSimilarly, in Cote d’Ivoire 81% of participants declared that the amount of the transfer was enough while 3% of
respondents reported that it was not enough. Eighty-seven percent (87%) of respondents declared that the cash transfer
increased their capacity to meet their basics needs. In Haiti, 100% of recipients reported that CVA support allowed them
to cover their food needs for four weeks. According to PDM data, 100% of Haitian recipients were satisfied by the CVA
distribution process.
4.2.7 ASSET RECOVERY
The loss of income and assets has been one of the major impacts of the COVID-19 pandemic. This led to the adoption
of – often negative – livelihoods coping mechanisms by affected populations. During the PDM, some participants noted
that part of the cash transfer was used to resume or start livelihoods activities. A participant from Guatemala, said, “We
had to look for ways to have a little income and not spend it all. So, I bought two yards of fabric and thread ($12.6). The
rest of the fellow workers are also embroidering. Although it is with little material, but we are earning about $1.2.”
“COVID-19 is a disease that has had real negative effects on all of our activities. Before, I sold
dry fish and condiments on the market. With the profits I was able to support my family and
contribute to our VSLA savings. During COVID-19, it was really difficult for us to carry out our
activities because of the barrier measures and the fear of getting sick. People no longer came
to the market and prices had risen considerably. I had to use the money of my business to cook
for my children. And the longer the situation lasted, I had nothing left. It was really difficult; my
children and I could barely feed ourselves. The savings meetings of our VSLA were a concern for
me as I didn't know how to be able to contribute. As if God had listened to my prayers and seen
my difficulties, I was selected to receive the cash transfer from CARE. I admit that I didn’t believe
it. But one morning I received a deposit message (SMS), a sum of $75 on my phone. I was so happy
that I started dancing. I took this money to replenish my business; buy chile, fresh and dry okra,
onion and condiments to resell. I resumed my small business with this money. I sincerely say
thank you to CARE and MARS”.
VSLA MEMBER AND CVA RECIPIENT (COTE D’IVOIRE)
23 June 2021 : Cash and Voucher Assistance in Response to the COVID-19 PandemicYou can also read