CANDIDA AURIS PAM PONTONES, MA DEPUTY STATE HEALTH COMMISSIONER STATE EPIDEMIOLOGIST - Indiana Health Care Association
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

CANDIDA AURIS PAM PONTONES, MA DEPUTY STATE HEALTH COMMISSIONER STATE EPIDEMIOLOGIST May 12, 2022

Previous MDRO Challenges

MRSA
• Contact precautions for clinical
infections and enhanced barrier
precautions for colonization in LTC and
contact precautions in hospitals
• Meticulous hand hygiene
• Communication when handed off
• Environmental cleaning
• Being aware and vigilant
Courtesy of CDC Public Health Image Library
3
C. difficile
• Enhanced contact precautions
(hospitals) or contact isolation with and
washing using soap and water (LTC)
• Meticulous hand hygiene
• Communication when handed off
• Environmental cleaning
• Being aware and vigilant
Courtesy of CDC Public Health Image Library
4
COVID-19
You already know this!
5
New Challenge: Candida auris
Candida auris
• Candida species are common commensals in skin and GI tract and cause
disease when protective barrier is disrupted (wounds, GI perforation, invasive
devices)
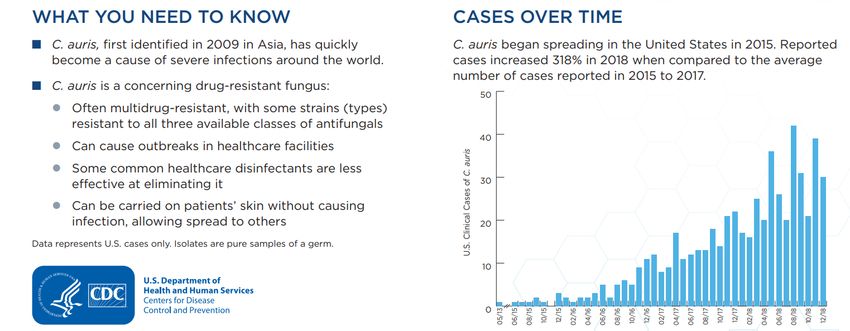
• Candida auris is an emerging fungus with serious global health threat
o To date, infections have been found in 30 countries, including the U.S.
o Often multi-drug resistant; some resistant to all known antifungals
o Can exhibit 30-60% mortality rate in clinically infected individuals
o Difficult to identify with standard laboratory methods; can be misidentified in labs
without specific technology
o Causes outbreaks in healthcare settings and is environmentally hardy
7
General Information about Candida auris | Candida auris | Fungal Diseases | CDC
Scope of Problem
8
https://www.cdc.gov/drugresistance/pdf/threats-report/candida-auris-508.pdf
Transmission
• Can spread between hospitalized patients and nursing home residents
• Can be acquired through contact with contaminated environmental surfaces
or equipment
• Can persist in the environment and withstand some commonly used
healthcare facility disinfectants
• More work is needed to further understand
• Can colonize patients for months but doesn’t mean infection
9Colonization
• Presence of the organism without causing any harm to the individual
• Usually tested by collecting swabs from the skin (axilla or groin) and
culturing
• May be present in skin, nares, oropharynx, rectum, and other body sites
• Individuals colonized with C. auris can transmit it to others who may develop
invasive infections if they have risk factors.
• Screening allows detection of those colonized, so infection control measures
can be implemented
• No protocols for decolonization--continued enhanced barrier precautions are
recommended by CDC.
10Infection
• Can cause bloodstream infections, wound infections, and ear infections
• Patients with invasive Candida infections usually have underlying medical conditions
or immunocompromise
• Diagnosed by culturing blood or body fluid with special tests to differentiate from
other types of yeast—important for appropriate treatment
o Risk factors: lines, tubes, open wounds, surgery, diabetes, nursing home residents, broad-
spectrum antibiotic use, and antifungal use
o Infections have been found in all ages from preterm infants to elderly
11Treatment
• Effectively treated with
echinocandin antifungals
• Some infections have been
resistant to all main classes of
antifungals known, making them
more difficult to treat and
requiring a higher dose
Courtesy of CDC Public Health Image Library
12Number of Cases
0
5
10
15
20
25
30
35
40
45
50
March
April
2017 2018
January
February
March
April
May
June
2019
July
August
September
October
November
December
January
February
March
Indiana Case Counts
April
May
Colonized
June
2020
July
August
Clinical
September
October
Month and Year of Specimen Collection
November
December
C. auris Identified in Indiana from 2017-2022
January
February
March
April
May
June
2021
July
August
September
October
November
December
January
February
2022
March
Data Collected by IDOH
13District Distribution – 2020 Clinical cases (23 total) District One: 17 District Two:
District Distribution – 2021
Number of C. auris Cases by District in 2021
120
Clinical cases (66 total)
District One: 29 100
District Five: 29
80
Colonization cases (124 total) 60
District One: 40
District Five: 79 40
20
0
1 2 3 4 5 6 7 8 9 10
Screening Clinical Less Than 5
Data Collected by IDOH
(current as of 5/1/2022)
15Infection Control
Core Principles for Colonization or Infection
• Report possible or confirmed C. auris test results to IDOH and send isolates to IDOHL
• Place patient with colonization in transmission-based precautions, preferably in single room or
cohort with same MDRO (contact isolation in acute care, contact isolation for cases and enhanced
barrier for colonization in LTC): gown, gloves
• Use rigorous hand hygiene: handwashing is best, alcohol-based sanitizer is effective
• After consulting with public health personnel, screen contacts of patients to identify anyone
colonized
• Communicate whenever the individual is transferred to any other unit or facility
• Surveillance for clinical cases: identify all yeast isolates from a normally sterile site (blood, CSF)
and treat appropriately
• Conduct appropriate environmental cleaning and monitor for additional cases
Information for Infection Preventionists | Fact Sheets | Candida auris | Fungal Diseases | CDC
17
Infection Prevention and Control for Candida auris | Candida auris | Fungal Diseases | CDCEnhanced Barrier Precautions
Infection Prevention and Control for Candida auris | Candida auris | Fungal Diseases | CDC
18Environmental Cleaning
• Thorough daily and terminal cleaning is essential, since C. auris can persist
on surfaces
• Use disinfectant with EPA claim for C. auris (if not available, use those with a
claim for C. difficile)
• Use appropriately, as use can impact effectiveness
• Disinfectants may have different directions for different pathogens
• Follow label directions for C. auris including the contact time
• Monitor cleaning process, especially for high-touch surfaces
https://www.epa.gov/pesticide-registration/list-p-antimicrobial-products-registered-epa-
claims-against-candida-auris#products
19Cohorting
Infection Prevention and Control for Candida auris | Candida auris | Fungal Diseases | CDC
20Cohorting
Infection Prevention and Control for Candida auris | Candida auris | Fungal Diseases | CDC
21Reassessing Colonization
Infection Prevention and Control for Candida auris | Candida auris | Fungal Diseases | CDC
22Preventing Transmission
23
https://www.cdc.gov/fungal/candida-auris/c-auris-drug-resistant.htmlResources
24
https://www.in.gov/health/erc/infectious-disease-epidemiology/healthcare-associated-infections-and-
antimicrobial-resistance-epidemiology/candida-auris/COVID-19 Update
Case Numbers and Trends • National: 7-day averages climbing overall • Cases—69,000 (up 20%) • Hospitalizations—2,400 (up 17%) • Deaths—340 (up 8.9%) • Tests—817,000 (up 28%) • LTC residents up-to-date with boosters show 47% lower rate of illness • Statewide: • Cases—762 (7-day average), increasing in 5-11, 12-17, 20-29, 60-69, 70-79 year age groups • Hospitalizations—6 (as of May 6), continue to decrease • Deaths—0 (7-day average) • Tests—8,176 (7-day average), increasing
Variants
• BA.2.12
• Genetic cousin of BA.2—1-2 mutations in spike protein
• Increased transmissibility compared to BA.2, highest percentage of cases in NY, NE US
• Treatments and vaccines still appear effective
• BA.4 and BA.5
• New omicron strains, both identified in South Africa; fewer than 1000 worldwide, most in South Africa
• Few cases in US: BA.4 = 13, BA.5 = 7, none in Indiana
• Learning more about transmissibility
• Treatments and vaccines still appear effective
• Layered prevention strategies still effective: vaccination, boosting, masking, symptom monitoring, testing, I/Q
• Still continue to monitor circulating variants at national and state levels
• Monitor CDC community levels at www.cdc.gov – all Indiana counties low except Montgomery (medium)
27Questions? Pam Pontones, MA Deputy Health Commissioner State Epidemiologist ppontones@isdh.in.gov Shireesha Vuppalanchi, MD Medical Director svuppalanchi@isdh.in.gov
You can also read

















































