BY ANTONIO C. WOLFF, MD, FACP, MARY E. CIANFROCCA, DO, AND STEPHEN R. D. JOHNSTON, MA, PHD, FRCP
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Optimizing Endocrine Therapy for
Women with Breast Cancer Regardless
of Menopausal Status
By Antonio C. Wolff, MD, FACP, Mary E. Cianfrocca, DO, and
Stephen R. D. Johnston, MA, PhD, FRCP
Overview: Endocrine therapy is now accepted as the most part of endocrine therapy in postmenopausal women, al-
important component of adjuvant therapy for all patients though questions remain about its sequential use with
with hormone receptor-positive breast cancer, regardless tamoxifen and duration of therapy. However, not all patients
of menopausal status. There is now considerable interest in equally benefit from adjuvant endocrine therapy. This article
the role of ovarian suppression/ablation in younger women, reviews the optimal use of adjuvant endocrine therapy in
which is the subject of several large ongoing international breast cancer and the possible strategies to overcome
trials. Aromatase inhibitors are now considered an integral primary or secondary endocrine resistance.
L EVELS OF estrogen receptor (ER) alpha and proges-
terone receptor (PR) expression are modest prognos-
tic factors for breast cancer recurrence and survival that
Rather, these new guidelines reflect the increasing ability
to move beyond prognostic factors to focus on individual
predictive factors. In other words, one should first con-
were primarily used for risk stratification. However, the sider those unique features that could potentially deter-
true clinical utility of hormone receptor expression is to mine an individual’s likelihood of benefiting (or not) from
serve as a powerful predictive marker for benefit from specific therapies (e.g., hormone receptor and human
adjuvant endocrine therapy. About three-quarters of all epidermal growth factor receptor 2 [HER2] status), and
patients with invasive tumors and about one-half of those only then should traditional anatomic markers that aid in
who are premenopausal present with hormone receptor- prognostic but not predictive assessment (e.g., tumor size
positive disease. Many of the early adjuvant endocrine and lymph node status) come into play.
trials were small and not powered to detect improvements Patients with hormone receptor-positive disease do not
in specific subsets, and many studies conducted well into have a uniform response to various endocrine therapies.
the 1990s allowed patients with negative or unknown In addition to individual tumor characteristics, individual
receptor status. Therefore, not until the 1995 edition of host factors are likely to also influence response and
the Early Breast Cancer Trialists Collaborative Group toxicity to individual therapies.5 Gene expression profile
systematic review exercise were the notions finally put to assays seem to identify several major breast cancer sub-
rest1 that tamoxifen is ineffective in premenopausal types with prognostic implications, and there appears to
women and potentially effective in those with hormone be at least two major subtypes of ER-positive tumors.6 At
receptor-negative tumors. least one commercial assay using formalin-fixed paraffin-
embedded tissue has undergone strict assay standardiza-
TREATING AN INDIVIDUAL tion and was shown in retrospective validation studies to
AND NOT A POPULATION have a strong prognostic7 and predictive8 value for pa-
There is now clear evidence that breast cancer is not one tients with lymph node-negative, ER-positive disease.
but a collection of diseases that share a common name and This assay may in fact discriminate luminal A from the
have an extremely diverse biologic behavior. This is un- luminal B and the ER-positive HER2-positive tumor sub-
questionably a diagnosis where one treatment will not fit types described in gene expression profiles using frozen
all patients,2 a concept that is clearly reflected in the most tissue. A large prospective validation trial of this technol-
recent update of algorithms for adjuvant therapy selection ogy (the TAILORx trial) was activated in North America
issued by the 2005 St. Gallen International Consensus in early 2006. A separate international effort will attempt
Panel and the National Comprehensive Cancer Network to validate gene expression platforms that require fresh
in the United States.3,4 The two groups now place primary frozen tissue.
emphasis on measures of potential response to therapy
rather than measures of risk stratification, and these PREMENOPAUSAL SETTING
seemingly subtle changes must be interpreted as much
The well entrenched misconception that endocrine ther-
more than a simple switch in their order of consideration.
apy is ineffective in premenopausal women was perpetu-
ated by results from trials that were confounded by the
inclusion of patients with ER-negative disease, the limited
From The Johns Hopkins Kimmel Cancer Center, Baltimore, MD; Northwestern use of tamoxifen, and the indirect endocrine effects of
University Feinberg School of Medicine, Chicago, IL; and The Royal Marsden NHS chemotherapy.9 The Early Breast Cancer Trialists’ Col-
Trust, London, UK.
Authors’ disclosures of potential conflicts of interest are found at the end of this article.
laborative Group data have now confirmed the survival
Address reprint requests to Antonio C. Wolff, MD, FACP, The Johns Hopkins Kimmel benefit offered by adjuvant chemotherapy for the average
Cancer Center, Bunting-Blaustein Cancer Research Building, Room 189, 1650 Orleans patient with early-stage disease (especially younger
St, Baltimore, MD 21231-1000; e-mail: awolff@jhmi.edu.
© 2006 by American Society of Clinical Oncology. women) and by tamoxifen for any patient with ER-positive
1092-9118/06/22-29 disease regardless of age.1 Age is, therefore, an incomplete
22OPTIMAL ENDOCRINE THERAPY IN BREAST CANCER 23
surrogate for the interaction of host and tumor biologic mors had similar outcomes. Eastern Cooperative Oncology
features (e.g., expression of hormone receptors, tumor Group 5188 is the largest trial examining the role of
grade, mitotic rate, and lymphatic vascular invasion) combined endocrine therapy.23 It showed a benefit from
rather than an independent prognostic factor.9 adding goserelin plus tamoxifen (but not just goserelin)
Similar confounding factors explain the ongoing contro- after adjuvant anthracycline-based chemotherapy, while
versy on the role of ovarian suppression/ablation (OA) in suggesting that goserelin alone following chemotherapy
premenopausal women. Following the original reports on may be of benefit in patients younger than age 40. A
the palliative role of oophorectomy for patients with ad- tamoxifen-only arm after chemotherapy was unfortu-
vanced disease in the late 19th century and the first nately not included based on existing knowledge at the
randomized trials of adjuvant ovarian ablation in the late time.
1940s, accumulated evidence and systematic review exer- Therefore, these data suggest that optimal endocrine
cises held by the Early Breast Cancer Trialists’ Collabo- therapy plays an important role in younger premeno-
rative Group every 5 years since 1985 confirmed that pausal patients with hormone receptor-positive disease
ablation of functioning ovaries significantly improves sur- are more likely to continue menstruating after adjuvant
vival in patients with breast cancer younger than age 50, chemotherapy and to benefit less from chemotherapy as
at least in the absence of chemotherapy.10 compared with patients with hormone-receptor–negative
disease. However, most of these trials did not use contem-
Ovarian Suppression With and Without porary chemotherapy regimens (e.g., anthracyclines or
Chemotherapy taxanes), allowed patients with hormone receptor-
negative or unknown status, and used tamoxifen inconsis-
Several studies that evaluated OA against cyclophosph-
tently. OA is not devoid of potential toxicities, including
amide, methotrexate, and fluorouracil (CMF) chemother-
weight gain, diabetes, and hot flashes.23 At present, OA
apy, such as the Zoladex Early Breast Cancer Research
should not yet be routinely used to replace or to comple-
Association,11 Scottish-Guys,12 Takeda Adjuvant Breast
ment adjuvant chemotherapy. Several ongoing trials de-
Cancer Study with Leuprolide Acetate, 13 and Interna-
scribed in Table 1 are expected to address definitively the
tional Breast Cancer Study Group (IBCSG) VIII14 trials,
various roles of combining chemotherapy, OA, tamoxifen,
showed that OA offered similar outcomes to patients with
and aromatase inhibitors (AIs) in premenopausal patients
hormone receptor-positive disease but was inferior to
with early stage hormone receptor-positive breast cancer.
CMF in patients whose tumors did not express hormone
receptors. Studies like the Austrian Breast and Colorectal POSTMENOPAUSAL SETTING
Study Group 5,15 French Adjuvant Study Group 06,16 and
Gruppo di Ricerca in Oncologia Clinica e Terapie Associ- Issues surrounding adjuvant endocrine therapy in post-
ate17 showed that combined endocrine therapy with OA menopausal women are somewhat less controversial. Sev-
and tamoxifen offers similar or improved outcome when eral AIs offer additional benefit to what was observed with
combined with CMF. just 5 years of tamoxifen, including an overall survival
benefit in patients with lymph node-positive disease,24
Ovarian Suppression after Chemotherapy and aromatase inhibitors are now considered an integral
part of endocrine therapy in postmenopausal women.25
Data from the use of OA after chemotherapy are more Until recently, 5 years of tamoxifen alone was the
limited. Although no significant survival benefit was seen standard adjuvant endocrine therapy for postmenopausal
with the use of CMF followed by goserelin over CMF in women. However, tamoxifen is associated with a small
IBCSG VIII, a retrospective subset analysis suggests that risk of complications (e.g., uterine cancer and thromboem-
any benefit might be restricted to women younger than bolic disease), and not all patients are helped. The risk of
age 40.14 The Zoladex in Premenopausal Patients four- recurrence in patients with hormone receptor-positive
arm trial compared 2 years of therapy with tamoxifen disease is not limited to the first 5 years,26 and the use of
and/or goserelin compared with placebo using a 2 ⫻ 2 tamoxifen beyond 5 years is not routinely recommended.27
factorial design, and showed a survival benefit in the The clinical activity and safety of AIs in the metastatic
goserelin arm that was less pronounced in patients setting led to their evaluation in adjuvant setting for
treated with tamoxifen or chemotherapy.18 A French postmenopausal women (Table 2). These trials used three
study with a mixed hormone receptor population did not different strategies as follows: replacement of tamoxifen
show a benefit from adding OA after various kinds of with an AI, sequencing of an AI after 2 years to 3 years of
chemotherapy.19 tamoxifen compared with continuation of tamoxifen for a
total of 5 years of therapy, and sequencing of an AI or
Endocrine Effects of Chemotherapy placebo after 5 years of tamoxifen for a total of 10 years of
Provocative data from international collaborators led by therapy.
the IBCSG20 and individual trials21,22 suggest that young
women (⬍ 35 years old) with hormone-receptor–positive Upfront Use of an Aromatase Inhibitor
tumors primarily treated with chemotherapy had a statis- The Arimidex Versus Tamoxifen Alone or in Combina-
tically significantly higher risk of relapse than older tion (ATAC) trial28 and the Breast International Group
premenopausal patients, although younger and older pre- (BIG) 1-98 trial29 compared 5 years of an AI (anastrozole
menopausal patients with hormone-receptor–negative tu- and letrozole, respectively) to 5 years of tamoxifen as24 WOLFF, CIANFROCCA, AND JOHNSTON
Table 1. Ongoing Adjuvant Trials of Ovarian Suppression in Premenopausal Women
Study Study Design Patient Population Issues
SOFT, Suppression of Ovarian TAM 5 years v OA 5 years ⫹ TAM 5 2,700 premenopausal women with Does OA add to chemotherapy in
Function Trial (IBCSG 24-02/ years v OA 5 years ⫹ EXE 5 years endocrine-responsive disease treated premenopausal women? Does OA
BIG 2-02) with no adjuvant chemotherapy or add to TAM (or EXE) in
remain premenopausal after premenopausal women not treated
chemotherapy with chemotherapy?
TEXT (IBCSG 25-02/BIG 3-02) OA 5 years ⫹ TAM 5 years v OA 5 2,025 premenopausal women with Is an AI superior to a SERM in
years ⫹ EXE 5 years endocrine-responsive disease who are premenopausal women treated with
candidates for OA, and who may or OA?
not receive chemotherapy
PERCHE (IBCSG 26-02/BIG OA 5 years ⫹ endocrine therapy 1,750 premenopausal women with Is chemotherapy necessary in
4-02) (TAM or EXE) 5 years endocrine-responsive disease premenopausal women receiving
⫾ chemotherapy combined endocrine therapy?
ABCSG AU12 Goserelin 3.6 mg SQ monthly/TAM 1 1,250 premenopausal women with stage Is OA plus an AI superior to OA plus
mg PO four times a day 3 years v I/II disease (⬍ 10 positive lymph TAM? Preliminary data suggest that
Goserelin 3.6 mg SQ monthly/ANZ nodes) the osteoporosis risk of OA ⫹ AI
56
1 mg PO four times a day 3 years v combination is reduced by ZOL
same arms ⫾ ZOL 4 mg IV twice a
year (2 ⫻ 2 design)
Abbreviations: TAM, tamoxifen; AI, aromatase inhibitor; ANZ, anastrozole; ER, estrogen-positive; EXE, exemestane; HR, hazard ratio; LTZ, letrozole; OA,
ovarian suppression/ablation; ZOL, zoledronate. SERM, selective estrogen receptor modulator; IBCSG, International Breast Cancer Study Group; BIG, Breast
International Group; PERCHE, Premenopausal Endocrine Responsive Chemotherapy Study; ABCSC, Austrian Breast and Colorectal Study Group; PO, orally.
adjuvant therapy for postmenopausal women with early- Sequential Therapy
stage breast cancer. The ATAC trial also included a
combination arm (concurrent anastrozole and tamoxifen), The Italian Tamoxifen Anastrozole trial,30 the joint
which was discontinued after the first analysis for lack of analysis of the Austrian Breast and Colorectal Cancer
benefit. The BIG 1-98 trial also included two sequential Study Group Trial 8 and the Arimidex-Nolvadex 95 tri-
arms (letrozole followed by tamoxifen and tamoxifen fol- al,31 and the International Exemestane Study32 compared
lowed by letrozole), but these data are not yet available. 5 years of tamoxifen to a sequential approach using 2
Both trials showed an improvement in disease-free sur- years to 3 years of tamoxifen followed by 2 years to 3 years
vival (DFS) favoring the AI over tamoxifen, but thus far of an AI. All trials showed a benefit in DFS for a sequential
none demonstrated a significant improvement in overall tamoxifen-AI approach compared with 5 years of tamox-
survival. ifen, but none other than MA-17 thus far showed a
Table 2. Results from Aromatase Inhibitor Trials in Postmenopausal Women
Results (primary end point ⫽ DFS;
Study Schema Eligibility Criteria n Median Follow-Up IES ⫽ EFS)
ATAC28 ANZ 5 years v TAM ⫻ 5 years Postmenopausal; ER-unknown 9,366 68 months ANZ alone better than TAM alone
v ANZ/TAM ⫻ 5 years and negative also allowed (DFS HR 0.87, p ⫽ 0.01); Similar
survival in combination arm
(discontinued after 1st analysis)
BIG 1–9829 LTZ ⫻ 5 years v TAM ⫻ 5 Postmenopausal, ER-positive 8,010 25.8 months First analysis favors LTZ v TAM (DFS
years v LTZ ⫻ 2 years 3 HR 0.81, p ⫽ 0.003); Cross-over
TAM ⫻ 3 years v TAM ⫻ 2 results not yet available
years 3 LTZ ⫻ 3 years
ITA30 TAM ⫻ 5 years v TAM ⫻ 2–3 Postmenopausal, ER-positive, 448 36 months TAM-⬎ ANZ better than TAM (DFS
years 3 ANZ ⫻ 3–2 years node-positive only; Free of HR 0.35, p ⫽0.001)
recurrence after 2–3 years
of TAM
ABCSG 8/ARNO 9531 TAM ⫻ 5 years v TAM ⫻ 2 Postmenopausal, ER-positive 3,224 28 months TAM-⬎ ANZ better than TAM ⫻ 5
years 3 ANZ ⫻ 3 years years (EFS HR 0.60, p ⫽ 0.0009)
IES32 TAM ⫻ 5 years v TAM ⫻ 2–3 Postmenopausal, ER-positive or 4,742 30.6 months TAM-⬎ EXE better than TAM ⫻ 5
years 3 EXE ⫻ 3–2 years unknown, Free of recurrence years (DFS HR 0.68, p ⬍ 0.001)
after 2–3 years of TAM
MA-1724 Years 6–10: LTZ ⫻ 5 years v Postmenopausal, ER-positive, 5,187 30 months LTZ better than placebo (DFS
Placebo ⫻ 5 years free of recurrence after HR ⫽ 0.58, p ⬍ 0.001; DDFS
4.5–6 years of TAM HR ⫽ 0.60, p ⫽ 0.002); Improved
survival in node-positive
(HR ⫽ 0.61, p ⫽ 0.04)
Abbreviations: ANZ, anastrozole; DFS, disease-free survival; DDFS, distant disease-free survival; EFS, event-free survival; ER, estrogen-receptor; EXE,
exemestane; HR, hazard ratio; LTZ, letrozole; TAM, tamoxifen; ATAC, Arimidex, Tamoxifen, Alone or in combination; BIG, Breast International Group; ITA, Italian
Tamoxifen Anastrozole trial; ABCSG8, Austrian Breast and Colorectal Study Group 8; ARNO, Arimidex-Nolvadex; IES, Intergroup Exemestane Study.OPTIMAL ENDOCRINE THERAPY IN BREAST CANCER 25
significant improvement in overall survival. The MA-17 first report from BIG 1-98.29 It is also not unreasonable to
trial randomly assigned patients who had completed 5 use tamoxifen first in a low-risk patient with ER-positive/
years of tamoxifen to 5 years of letrozole compared with PR-positive, HER2-negative disease at low risk for recur-
placebo.24 DFS was improved for the letrozole group rence, especially if lymph node-negative.7,8
compared with placebo, and an overall survival benefit It is now common practice to consider a switch from
was seen in the subgroup of lymph node-positive patients. tamoxifen to an AI after 2 years to 5 years, although
Patients completing 10 years of therapy are now being individual preferences and safety issues must be ad-
offered a second random assignment to 5 more years of dressed. There are no compelling safety or efficacy data to
letrozole compared with placebo. differentiate among the three approved AIs (anastrozole,
exemestane, and letrozole) in the United States. It is
Safety Profile important to emphasize, however, that AIs should only be
These studies also addressed safety and tolerability. considered in the postmenopausal setting, and caution is
Adjuvant AIs compared with tamoxifen result in fewer advised when offering AIs to women with chemotherapy-
endometrial malignancies and thromboembolic events. induced amenorrhea who may still have residual ovarian
However, they are consistently associated with a higher function, and some may resume menses even years later.
risk of osteoporosis and related complications and muscu-
MECHANISMS OF ENDOCRINE RESISTANCE
loskeletal complaints. Concerns about cardiovascular risk
are also being assessed. Long-term follow-up is needed to Resistance to endocrine therapy in ER-positive tumors
assess their safety in a population likely to survive a can be intrinsic occurring at first exposure (de novo) or
breast cancer diagnosis. develop over time after an initial response to endocrine
therapy (acquired). Identification of the key mechanisms
Aromatase Inhibitors in Clinical Practice involved is important to help predict response or resis-
The American Society of Clinical Oncology convened an tance to specific treatments, and to facilitate development
AI Technology Assessment Panel to review the available of new pharmaceutical agents targeted at the various
data and make recommendations regarding AIs optimal molecular components of endocrine resistance pathways.
use in the adjuvant setting.25 In the panel’s most recent
update, they concluded that optimal adjuvant endocrine De Novo Resistance in ER-positive Breast Cancer
therapy for a postmenopausal woman with hormone The expression of ER in breast cancer cells has always
receptor-positive breast cancer should include an AI either been perceived to be the single most important determi-
as initial therapy or after a period of treatment with nant for endocrine response in breast cancer. Tumors that
tamoxifen. Several issues regarding AIs await further do not express any ER are unable to respond to endocrine
evaluation. These include the optimal duration of total therapies and thus exhibit primary resistance. However,
endocrine therapy, optimal sequencing with tamoxifen, expression of ER alone is insufficient to accurately predict
efficacy in premenopausal women whether combined response to endocrine therapy in the clinical setting. For
with OA or in patients with chemotherapy-induced example, a second ER has been cloned (ERbeta) that has
amenorrhea, and long-term safety.25 BIG 1-98 is examin- different transcriptional activity compared with ERalpha
ing sequential therapy with an up-front AI followed by and has been implicated in tamoxifen resistance.36 In
tamoxifen.29 addition to the classical model of liganded ER that binds
It has been noted that the trials using the sequential DNA at defined estrogen-response elements upstream of
approach (tamoxifen followed by an AI) yielded larger ER-regulated genes, ER may also activate alternative
proportional benefits than trials using 5 years of mono- DNA sequences such as AP-1-response elements that
therapy with an AI. It is unfair, however, to compare the regulate genes involved in cell proliferation, motility, and
results of these trials for many reasons, including differ- apoptosis. Enhanced AP-1 activation has been associated
ences in populations studied and differences in the defini- with tamoxifen resistance both in models of breast cancer
tion of end points. For example, patients in the and in human tumors.37 Likewise, the relative balance of
International Exemestane Study and MA-17 trials had coactivator and corepressor proteins in a cell may deter-
completed 2 years to 5 years of tamoxifen without a mine response of ER to a particular ligand; overexpression
recurrence and were, therefore, more likely to truly have of the coactivator SRC-1 enhanced the agonist response to
endocrine-responsive disease than patients in the ATAC tamoxifen,38 whereas reduced nuclear receptor corepres-
and BIG 1-98 trials who started an AI up front. One sor N expression was associated with development of
theoretical model was proposed to select patients for the tamoxifen resistance in breast cancer xenografts.39
use of up-front AI compared with a sequential approach,33 More recently, the presence of nongenomic mechanisms
but its generalizability is not certain. for ER action has been postulated as an alternative
Data from the sequential arms of BIG 1-98 trial com- mechanism for endocrine resistance in ER-positive breast
paring 5 years of an AI to a sequential AI followed by cancers. Membrane-initiated signaling involves ER inter-
tamoxifen are awaited with interest.29 In the absence of acting with and/or activating several kinases, including
direct comparative data, an AI up front may be considered the insulin-like growth factor-1 receptor and the p85
for many patients such as those with HER2-positive34 or regulatory subunit of phosphatidylinositol 3-kinase via
ER-positive/progesterone receptor (PR)-negative dis- adaptor proteins Src and Shc, resulting in different cell
ease,35 although these patterns were not observed in the survival and proliferative signals via the AKT (protein26 WOLFF, CIANFROCCA, AND JOHNSTON
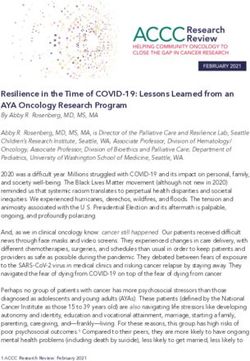
Fig 1. Bidirectional crosstalk pathways that may be active in endocrine-resistant breast cancer; liganded estrogen receptor can
interact at the plasma membrane with adaptor proteins (ie, Shc) and growth factor receptors, whereas epidermal growth factor
receptor/HER2 or insulin-like growth factor receptor can activate downstream of MEK/MAPK, pp90rsk, or the phosphatidylinositol
3-kinase-AKT pathways to phosphorylate nuclear coactivators/estrogen receptor to initiate hormone-dependent gene transcription, with
tamoxifen/estrogen functioning as agonist ligands. Abbreviations: IGFR, insulin-like growth factor receptor; EGFR, epidermal growth
factor receptor; HER2, human epidermal growth factor receptor2; ER, estrogen receptor.
kinase B) and mitogen-activated protein kinase (MAPK) signaling pathway.45,46 More recently, changes have been
pathways.40-43 Tamoxifen may also exert agonist effects reported in intracellular signaling in clinical samples from
via the interaction of membrane ER with peptide growth patients with breast cancer taken at diagnosis and then
factor signaling (epidermal growth factor receptor (EGFR) subsequently at the time of relapse on adjuvant tamoxifen
or HER2).44 Likewise, crosstalk may occur in ER-positive several years later.47 In tumors with retained ER expres-
tumors with HER2 amplification additional by down- sion (the majority), there was enhanced expression of
stream activation from various HER2-driven intracellular HER2 in some patients and evidence that expression of
kinases (eg, p38 MAPK and ERK1/2), which in tamoxifen- the stress-activated kinase p38 MAPK was also enhanced.
treated tumors may result in the phosphorylation of These data support a concept that breast cancer cells use
nuclear tamoxifen-liganded ER and its associated coacti- alternative intracellular signaling pathways over time to
vators. As such, existence of these bi-directional crosstalk enhance and activate ER signaling and that this allows
pathways can result in tamoxifen stimulating (rather cells to escape from their initial endocrine therapy with
than inhibiting) the growth of ER-positive breast cancer tamoxifen.
(Fig 1). To date there have been fewer clinical or laboratory
studies of resistance to aromatase inhibition. Laboratory
Acquired Endocrine Resistance data from several groups support a concept of adaptation
Several experimental models and clinical studies have to a low estrogen environment with an enhanced sensitiv-
suggested that peptide growth factor receptor pathways ity to estrogen as a means of escape from estrogen depri-
(e.g., EGFR and HER2) become selectively upregulated in vation therapies.48,49 In part, this may be because of an
breast cancer cells that acquire resistance to tamoxifen increase in ER protein but may also relate to relocation of
during prolonged exposure. Enhanced expression of EGFR ER to the plasma membrane in association with Shc and
and subsequent downstream MAPK activation have been insulin-like growth factor-1 receptor together with in-
found in MCF-7 breast cancer cells that become resistant creased activation of Src and RAS/RAF/MEK/MAPK
over time to tamoxifen, and there is evidence that cotreat- signaling.40 Treatment with fulvestrant blocked MAPK ac-
ment with the EGFR receptor tyrosine kinase inhibitor tivation suggesting that ER-alpha is functioning upstream
gefitinib may prevent or delay resistance by blocking this of MAPK in a nongenomic membrane-associated fashion.OPTIMAL ENDOCRINE THERAPY IN BREAST CANCER 27
Molecularly Targeted Therapies to Treat nists with an AI. Cotreatment with temsirolimus (CCI-
or Prevent Endocrine Resistance 779) inhibited mTOR activity and restored sensitivity to
tamoxifen primarily through induction of apoptosis, sug-
Emerging data suggest that endocrine resistance (either
gesting that AKT-induced tamoxifen resistance may in
de novo or acquired) may involve bidirectional interaction
part be mediated by signaling through the mTOR path-
between ER and growth factor signaling, either via non-
way.54 Preliminary data from randomized phase II trials
genomic ER activation of growth factor receptors at the
showed higher clinical benefit rates for temsirolimus com-
plasma membrane or via intracellular activation of clas-
bined with letrozole compared with letrozole alone,55 and
sical genomic ER in the nucleus by various intracellular
a larger randomized placebo-controlled efficacy study is
kinases driven by upstream growth factor pathways. Hope
underway. Similarly, preoperative studies are addressing
now exists that by learning which intracellular signaling
whether everolimus (RAD-001) can enhance the efficacy of
pathways are operative, logical combinations of signal
4 months of preoperative letrozole.
transduction inhibitors (STIs) can be devised to target key
molecular pathways implicated in development of resis-
CONCLUSION
tance.50 In particular, EGFR- and HER2-targeted thera-
pies have been used in preclinical models to overcome Endocrine therapy is the most important treatment for
endocrine resistance by blocking upregulated signaling patients with hormone-receptor–positive breast cancer,
pathways. In MCF-7 cells that developed resistance to regardless of menopausal status. Questions about the role
tamoxifen, both gefitinib and trastuzumab were effective of OA in premenopausal women and optimal schedule of
at reducing downstream ERK1/2 MAPK signaling and AIs in postmenopausal women remain. Endocrine therapy
inhibiting cell growth. alone will not be enough for many patients. Those with
Of note, hormone-sensitive cells (in which neither recep- larger tumors and lymph node involvement often receive
tors are overexpressed) are unaffected by either gefitinib chemotherapy, but many are potentially overtreated. New
or trastuzumab therapy. However, because adaptive molecular assays and the resulting refinement of risk
changes in growth factor signaling occur during prolonged stratification and predictive models will help further dis-
endocrine therapy, strategies to combine endocrine with criminate those with endocrine-responsive compared with
STI therapies may prevent development of resistance and nonresponsive disease within the group of patients with
improve therapeutic efficacy. In vitro combination of ta- hormone-receptor–positive disease.
moxifen and gefitinib prevented the acquired expression of Substantial progress has been made in recent years to
EGFR/MAPK signaling and the subsequent resistance better understand some of the molecular mechanisms
that occurred after 5 weeks in tamoxifen-alone treated involved in both de novo and acquired endocrine resis-
cells,51 and this concept is now being tested in a random- tance. Laboratory and clinical data support the concept
ized phase II trial. Combined STIs and endocrine therapy that over time breast cancer cells utilize alternative intra-
may also be more effective than using STIs alone in cellular signaling pathways to enhance and activate ER,
hormone-resistant HER2-positive/ER-positive breast can- which then allow cells to escape from their initial endo-
cer cells. For example, the dual EGFR/HER2 inhibitor crine therapy. As these pathways are elucidated, strate-
lapatinib cooperates with tamoxifen to provide more rapid gies are emerging to block these signaling pathways from
and profound cell cycle arrest than either therapy alone in the outset by cotreatment with various STIs. Both in vitro
acquired hormone-resistant cells,52 and a large phase III and in vivo data now exist to show that this approach may
clinical trial in ER-positive advanced breast cancer is now delay resistance, and this is being tested in ongoing
in progress to see whether lapatinib combined with letro- randomized controlled trials in both the metastatic and
zole can prolong time to disease progression compared preoperative settings.
with letrozole alone. The identification of candidates for adjuvant endocrine
Other STIs may also be more effective when combined therapy relies heavily on the accuracy of laboratory assays
with endocrine therapy. The farnesyltransferase inhibitor for ER and PR. These assays serve as predictive markers
tipifarnib when combined with tamoxifen or estrogen of response and sole determinants of therapy selection,
deprivation induced greater tumor regression than either and pathologists and laboratories share responsibility
endocrine therapy alone. However, a randomized phase II with clinicians regarding patient outcome. Therefore, it is
trial in 120 patients that compared letrozole and tipi- crucial that all involved (including patients) understand
farnib with letrozole alone showed a longer duration of the nuances of these assays to avoid the risk of denying
objective response for the combination (23 months vs. 16 adjuvant endocrine therapy to a patient with a false-
months) but no actual improvement in response rate.53 A negative hormone receptor test. Our ability to identify
similar rationale has emerged to support the combination optimal candidates for various endocrine therapy ap-
of the mammalian target of rapamycin (mTOR) antago- proaches will continue to be refined in the years to come.28 WOLFF, CIANFROCCA, AND JOHNSTON
Authors’ Disclosures of Potential Conflicts of Interest
Employment or
Leadership
Positions Consultant or Stock Research Expert Other
Author (Commercial Firms) Advisory Role Ownership Honoraria Funding Testimony Remuneration
Mary Cianfrocca Pfizer Oncology;
AstraZeneca;
Bristol-Meyers
Squibb; Novartis
Oncology; sanofi-
aventis US
Stephen R. D. Johnston AstraZeneca;
OrthoBiotech
Antonio C. Wolff*
*No significant financial relationships to disclose.
REFERENCES
1. Early Breast Cancer Trialist Collaborative Group. Effects of chemo- 16. Roche H, Kerbrat P, Bonneterre J, et al: Complete hormonal block-
therapy and hormonal therapy for early breast cancer on recurrence and ade versus chemotherapy in premenopausal early stage breast cancer
15-year survival: An overview of the randomised trials. Lancet. 2005;365: patients with positive hormone receptor and 1-3 node-positive tumors:
1687-1717. Results of the FASG 06 trial. Proc Am Soc Clin Oncol. 2000;19:72a (abstr
2. Winer EP. Optimizing endocrine therapy for breast cancer. J Clin 279).
Oncol. 2005;23:1609-1610. 17. Boccardo F, Rubagotti A, Amoroso D, et al. Cyclophosphamide,
3. Goldhirsch A, Glick JH, Gelber RD, et al. Meeting highlights: Inter- methotrexate, and fluorouracil versus tamoxifen plus ovarian suppression
national expert consensus on the primary therapy of early breast cancer as adjuvant treatment of estrogen receptor-positive pre-/perimenopausal
2005. Ann Oncol. 2005;16:1569-1583. breast cancer patients: Results of the Italian Breast Cancer Adjuvant
4. National Comprehensive Cancer Network: Breast Cancer Clinical Study Group 02 randomized trial. J Clin Oncol. 2000;18:2718-2727.
Practice Guidelines, version 2.2006. Http://www.nccn.org/professionals/ 18. Houghton J, Baum M, Rutqvist LE, et al: The ZIPP trial of adjuvant
physician_gls/PDF/breast.pdf . Zoladex in premenopausal patients with early breast cancer: An update at
5. Stearns V, Davidson NE, Flockhart DA. Pharmacogenetics in the five years. Proc Am Soc Clin Oncol. 2000;19:93a (abstr 359).
treatment of breast cancer. Pharmacogenomics J. 2004;4:143-153. 19. Arriagada R, Le MG, Spielmann M, et al. Randomized trial of
6. Sorlie T, Perou CM, Tibshirani R, et al. Gene expression patterns of adjuvant ovarian suppression in 926 premenopausal patients with early
breast carcinomas distinguish tumor subclasses with clinical implications. breast cancer treated with adjuvant chemotherapy. Ann Oncol. 2005;16:
Proc Natl Acad Sci U S A. 2001;98:10869-10874. 389-396.
7. Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence 20. Goldhirsch A, Gelber RD, Yothers G, et al: Adjuvant therapy for very
of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004; young women with breast cancer: Need for tailored treatments. J Natl
351:2817-2826. Cancer Inst Monogr. 2001;44-51.
8. Paik S, Shak S, Tang G, et al: Expression of the 21 genes in the 21. Fisher B, Redmond C, Wickerham DL, et al. Systemic therapy in
recurrence score assay and prediction of clinical benefit from tamoxifen in patients with node-negative breast cancer. A commentary based on two
NSABP study B-14 and chemotherapy in NSABP study B-20. Breast National Surgical Adjuvant Breast and Bowel Project (NSABP) clinical
Cancer Res Treat. 2004;88 (supp 1):S15 (abstr 24). trials. Ann Intern Med. 1989;111:703-712.
9. Dellapasqua S, Colleoni M, Gelber RD, et al. Adjuvant endocrine 22. International Breast Cancer Study Group. Duration and reintroduc-
therapy for premenopausal women with early breast cancer. J Clin Oncol. tion of adjuvant chemotherapy for node-positive premenopausal breast
2005;23:1736-1750. cancer patients. J Clin Oncol. 1996;14:1885-1894.
10. Early Breast Cancer Trialists’ Collaborative Group. Ovarian abla- 23. Davidson NE, O’Neill AM, Vukov AM, et al. Chemoendocrine ther-
tion in early breast cancer: Overview of the randomised trials. Lancet. apy for premenopausal women with axillary lymph node-positive, steroid
1996;348:1189-1196. hormone Receptor-positive breast cancer: Results from INT 0101 (E5188).
11. Jonat W, Kaufmann M, Sauerbrei W, et al. Goserelin versus cyclo- J Clin Oncol. 2005;23:5973-5982.
phosphamide, methotrexate, and fluorouracil as adjuvant therapy in 24. Goss PE, Ingle JN, Martino S, et al. Randomized trial of letrozole
premenopausal patients with node-positive breast cancer: the Zoladex following tamoxifen as extended adjuvant therapy in receptor-positive
Early Breast Cancer Research Association Study. J Clin Oncol. 2002;20: breast cancer: Updated findings from NCIC CTG MA. 17. J Natl Cancer
4628-4635. Inst. 2005;97:1262-1271.
12. Scottish Cancer Trials Breast Group and ICRF Breast Unit, Guy’s 25. Winer EP, Hudis C, Burstein HJ, et al. American Society of Clinical
Hospital, London. Adjuvant ovarian ablation versus CMF chemotherapy in Oncology technology assessment on the use of aromatase inhibitors as
premenopausal women with pathological stage II breast carcinoma: The adjuvant therapy for postmenopausal women with hormone receptor-
Scottish trial. Lancet. 1993;341:1293-1298. positive breast cancer: Status report 2004. J Clin Oncol. 2005;23:619-629.
13. Schmid P, Untch M, Wallwiener D, et al. Cyclophosphamide, meth- 26. Saphner T, Tormey D, Gray R. Annual hazard rates of recurrence for
otrexate, and fluorouracil (CMF) versus hormonal ablation with leuprore- breast cancer after primary therapy. J Clin Oncol. 1996;14:2738-2746.
lin acetate as adjuvant treatment of node-positive, premenopausal breast 27. Fisher B, Dignam J, Bryant J, et al. Five versus more than 5 years
cancer patients: Preliminary results of the TABLE study (Takeda Adju- of tamoxifen for lymph node-negative breast cancer: Updated findings from
vant Breast cancer study with Leuprorelin Acetate). Anticancer Res. the National Surgical Adjuvant Breast and Bowel Project B-14 randomized
2002;22:2325-2332. trial. J Natl Cancer Inst. 2001;93:684-690.
14. Castiglione-Gertsch M, O’Neill A, Price KN, et al. Adjuvant chemo- 28. Howell A, Cuzick J, Baum M, et al. Results of the ATAC (Arimidex,
therapy followed by goserelin versus either modality alone for premeno- Tamoxifen, Alone or in Combination) trial after completion of 5 years of
pausal lymph node-negative breast cancer: A randomized trial. J Natl adjuvant treatment for breast cancer. Lancet. 2005;365:60-62.
Cancer Inst. 2003;95:1833-1846. 29. The Breast International Group (BIG) 1-98 Collaborative Group. A
15. Jakesz R, Hausmaninger H, Kubista E, et al. Randomized adjuvant comparison of letrozole and tamoxifen in postmenopausal women with
trial of tamoxifen and goserelin versus cyclophosphamide, methotrexate, early breast cancer. N Engl J Med. 2005;353:2747-2757.
and fluorouracil: Evidence for the superiority of treatment with endocrine 30. Boccardo F, Rubagotti A, Puntoni M, et al. Switching to anastrozole
blockade in premenopausal patients with hormone-responsive breast can- versus continued tamoxifen treatment of early breast cancer: Preliminary
cer, Austrian Breast and Colorectal Cancer Study Group Trial 5. J Clin results of the Italian tamoxifen anastrozole trial. J Clin Oncol. 2005;23:
Oncol. 2002;20:4621-4627. 5138-5147.OPTIMAL ENDOCRINE THERAPY IN BREAST CANCER 29
31. Jakesz R, Jonat W, Gnant M, et al. Switching of postmenopausal crine growth regulatory pathway in tamoxifen-resistant MCF-7 cells.
women with endocrine-responsive early breast cancer to anastrozole after Endocrinology. 2003;144:1032-1044.
2 years of adjuvant tamoxifen: Combined results of ABCSG trial 8 and 46. McClelland RA, Barrow D, Madden T-A, et al. Enhanced epidermal
ARNO 95 trial. Lancet. 2005;366:455-462. growth factor receptor signaling in MCF-7 breast cancer cells after long-
32. Coombes RC, Hall E, Gibson LJ, et al. A randomized trial of term culture in the presence of the pure antiestrogen ICI 182,780 (Faslo-
exemestane after 2 to 3 years of tamoxifen therapy in postmenopausal dex). Endocrinology. 2001;142:2776-2788.
women with primary breast cancer. N Engl J Med. 2004;350:1081-1092. 47. Gutierrez MC, Detre S, Johnston S, et al. Molecular changes in
33. Punglia RS, Kuntz KM, Winer EP, et al. Optimizing adjuvant tamoxifen-resistant breast cancer: Relationship between estrogen recep-
endocrine therapy in postmenopausal women with early-stage breast tor, HER2, and p38 mitogen-activated protein kinase. J Clin Oncol.
cancer: A decision analysis. J Clin Oncol. 2005;23:5178-5187.
2005;23:2469-2476.
34. Ellis MJ, Coop A, Singh B, et al. Letrozole is more effective
48. Masamura S, Santner SJ, Heitjan DF, et al. Estrogen deprivation
neoadjuvant endocrine therapy than tamoxifen for ErbB-1- and/or ErbB-
causes estradiol hypersensitivity in human breast cancer cells. J Clin
2-positive, estrogen receptor-positive primary breast cancer: Evidence from
Endocrinol Metab. 1995;80:2918-2925.
a phase III randomized trial. J Clin Oncol. 2001;19:3808-3816.
49. Martin L-A, Farmer I, Johnston SRD, et al. Enhanced estrogen
35. Dowsett M, Cuzick J, Wale C, et al: Retrospective analysis of time to
recurrence in the ATAC trial according to hormone receptor status: An receptor (ER) alpha, ERBB2, and MAPK signal transduction pathways
hypothesis-generating study 10.1200/JCO. 2005.01.4829. J Clin Oncol. operate during the adaptation of MCF-7 cells to long-term estrogen
2005;23:7512-7517. deprivation. J Biol Chem. 2003;278:30458-30468.
36. Spiers V, Parkes AT, Kerin MJ, et al. Coexpression of estrogen 50. Johnston SRD: Combinations of endocrine and biological therapies;
receptor alpha and beta; poor prognostic factors in human breast cancer. Present status of therapeutic and preclinical studies. Clin Cancer Res.
Cancer Res. 1999;59:525-528. 2005;11:889-899s.
37. Johnston SRD, Lu B, Scott GK, et al. Increased activator protein-1 51. Gee JM, Harper ME, Hutcheson IR, et al. The anti-EGFR agent
DNA binding and c-jun NH2-terminal kinase activity in human breast gefitinib (ZD 1839/Iressa) improves anti-hormone response and prevents
tumors with acquired tamoxifen resistance. Clin Cancer Res. 1999;5:251- development of resistance in breast cancer in vitro. Endocrinology. 2003;
256. 144:5105-5117.
38. Smith CL, Nawaz Z, O’Malley BW, et al. Coactivator and corepressor 52. Chu I, Blackwell K, Chen S, et al. The dual ErbB1/ErbB2 inhibitor
regulation of the agonist/antagonist activity of the mixed antiestrogen lapatinib (GW572016) cooperates with tamoxifen to inhibit both cell
4-hydroxytamoxifen. Mol Endocrinol. 1997;11:657-666. proliferation and estrogen-dependent gene expression in antiestrogen
39. Lavinsky RM, Jepsen K, Heinzel T, et al. Diverse signaling path- resistant breast cancer. Cancer Res. 2005;65:18-25.
ways modulate nuclear receptor recruitment of N-CoR and SMRT com- 53. Johnston SRD, Semiglazov V, Manikas G, et al. A randomised,
plexes. Proc Natl Acad Sci U S A. 1998;95:2920-2925. blinded, phase II study of tipifarnib combined with letrozole in the
40. Song RX, McPherson RA, Adam L, et al. Linkage of rapid estrogen treatment of advanced breast cancer that has progressed with antioestro-
action to MAPK activation by ERalpha-Shc association and Shc pathway
gen therapy. Breast Cancer Res Treat. 2005;94:A5087.
activation. Mol Endocrinol. 2002;16:116-127.
54. Boulay A, Rudolf J, Ye J, et al. Dual inhibition of mTOR pathway
41. Kahlert S, Nuedling S, van Eickels M, et al. Estrogen receptor alpha
and estrogen signaling in vivo induces cell death in models of breast
rapidly activates the IGF-1 receptor pathway. J Biol Chem. 2000;275:
cancer. Clin Cancer Res. 2005;11:5319-5328.
18447-18453.
55. Baselga J, Roche H, Fumoleau P, et al. Treatment of postmeno-
42. Simoncini T, Hafezi-Moghadam A, Brazil DP, et al. Interaction of
oestrogen receptor with the regulatory subunit of phosphatidylinositol pausal women with locally advanced or metastatic breast cancer with
3-OH kinase. Nature. 2000;407:538-541. letrozole alone or in combinations with temsirolimus; a randomized 3-arm,
43. Levin ER. Bidirectional signaling between the estrogen receptor and phase 2 study. Breast Cancer Res. Treat 2005;94:A1068.
the epidermal growth factor receptor. Mol Endocrinol. 2003;17:309-317. 56. Gnant M, Jakesz R, Mineritsch B, et al: Zoledronic acid effectively
44. Shou J, Massarweh S, Osborne CK, et al. Mechanisms of tamoxifen counteracts cancer treatment-induced bone loss in premenopausal breast
resistance: Increased estrogen receptor-HER2/neu cross-talk in ER/HER2- cancer patients receiving adjuvant endocrine treatment with goserelin plus
positive breast cancer. J Natl Cancer Inst. 2004;96:926-935. anastrozole versus goserelin plus tamoxifen-bone density subprotocol re-
45. Knowlden JM, Hutcheson IR, Jones HE, et al. Elevated levels of sults of a randomized multicenter trial (ABCSG-12). Breast Cancer Res
epidermal growth factor receptor/c-erbB2 heterodimers mediate an auto- Treat. 2004;88 (supp 1):(abstr 6).You can also read