Very low energy diets in the treatment of obesity
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
obesity reviews
Very low energy diets in the treatment of obesity
P. Mustajoki and T. Pekkarinen
1
Peijas Hospital, Department of Medicine, Summary
Vantaa, Finland Very low energy diets (VLEDs) are defined as diets which contain energy levels
of less than 3.4 MJ (800 kcal) per day and contain daily allowances of all essen-
Received 14 September 2000; revised 29 tial nutritional requirements. These diets have been in clinical use for more than
October 2000; accepted 1 November 2000 20 years. They are used as the only source of nutrition for 8–16 weeks, which
usually achieves a weight loss of 1.5–2.5 kg per week. Before using this type of
Address reprint requests to: Pertti Mustajoki, diet a medical investigation is necessary to evaluate contraindications and to check
Peijas Hospital, Department of Medicine, medication use during the diet. To facilitate maintenance, cognitive behavioural
Sairaalakatu 1, 01400 Vantaa, Finland counselling should always be included in a weight reduction programme using a
E-mail: pertti.mustajoki@pine.pp.fi very low energy diet. VLEDs have no serious harmful effects and can safely be
used in patients with various chronic diseases. Programmes using VLEDs produce
better short-term weight loss than programmes without the diet. However, in ran-
domized controlled trials VLED-based programmes have not achieved signifi-
cantly better long-term maintenance than conventional programmes. VLEDs are
used when rapid weight loss is necessary because of an obesity-related disease. In
other patients with obesity it is an alternative to other conservative approaches
for treatment of obesity. In type 2 diabetes it may improve long-term glucose
metabolism better than conventional weight reducing diets. Some studies suggest
that after a VLED-based programme long-term maintenance is better among men
than women. This possible gender difference is an important topic for further
research.
Keywords: maintenance, obesity, therapy, very low energy diet.
obesity reviews (2001) 2, 61–72
In this paper we review the properties and current
Introduction
status of VLEDs in the management of obesity. Regarding
After 20 years of intensive research it is generally accepted some practical questions for which no research data are
that very low energy diets (VLEDs) are safe and usually available we present our recommendations based on our
achieve considerable weight loss in the short-term. How- experience with weight reduction groups (3–7) and
ever, long-term results are less satisfactory. VLEDs are individual patients (8).
used in weight reduction programmes in many obesity
clinics but the role of VLEDs in the treatment of obesity is
not fully established. Published guidelines for management Composition of the diet
of obesity give variable recommendations. Scottish guide-
Energy
lines recommend that VLEDs should usually be reserved
for use in specialist centres for patients on medical grounds, VLEDs are defined as diets containing energy62 Very low energy diets P. Mustajoki & T. Pekkarinen obesity reviews
loss while providing adequate nutrition and preserving length of a VLED is 8–16 weeks. The length may depend
vital lean body mass. on the amount of extra weight: in patients with morbid
obesity (BMI >40 kg m–2) the period may be 12–16 weeks,
VLED regimen for patients with moderate obesity (BMI 30–35 kg m–2)
8–10 weeks. In a select number of cases the use of a VLED
VLEDs can be composed of normal food when a protein has been reported to be longer than 16 weeks (8,20).
source, vitamins and trace elements are added (11–13). Periods of less than 6–8 weeks may not be meaningful
Usually, however, a commercial liquid or powder formula, because the diets have been intended to produce maximum
which contains all the essential elements of VLEDs are initial weight loss which cannot be reached during shorter
preferred. It is not known whether adherence to the periods.
programme or safety differs between self-composed diets
and commercial formulas. Commercial preparations usually
contain around 2.1 MJ (500 kcal) of energy. The optimal PreVLED
amount of energy is not known and may lie within quite Many manufacturers of VLEDs recommend a low calorie
broad limits. In a study by Foster and co-workers (14) diets diet for one or more weeks before a VLED to adapt to the
containing 1760, 2770 or 3360 kJ (420, 660 or 800 kcal) strict diet. As far as we know, the optimal way to start
of energy daily were associated with identical weight losses. a VLED has never been studied. In our weight reduction
programme VLED is started without a preparative diet and
Carbohydrates we have not seen any negative effects.
The amount of daily carbohydrate intake in VLED pre-
parations vary from 10 to 80 g. At present the optimal VLED period
amount of carbohydrate has not been established. An argu-
Torgerson and co-workers (21) compared three different
ment for low carbohydrate content is the fact that there is
ways to conduct a 12-week VLED period: (1) outpatient
better protein sparing and fat mobilization, however this is
strict, i.e. strict adherence to the diet was encouraged and
controversial (9). Higher amounts of carbohydrates have
no extra eating was allowed; (2) outpatient liberal, i.e. the
been suggested to prevent some disturbances in cognitive
patients were allowed to eat two small extra meals weekly
functions found in one study (15), but others have not
and (3) strict, but at the beginning of the diet patients spent
confirmed this.
1 week in a metabolic ward to adapt to the diet. After the
VLED-period best results were in both strict regimens. Still
Fibre 1 year later the strict outpatient regimen had significantly
better results than the liberal outpatient regimen. The result
Daily fibre intake with different preparations varies from
of the inpatient group was between the other two groups.
almost nothing to 20 g. Astrup and co-workers (16) have
The study shows that a strict VLED regimen probably gives
shown that adding 30 g fibre day-1 (mainly cellulose) to a
best results also in the long-term and that initial inpatient
VLED improves bowel movements and lessens hunger, but
management is of no help.
has no effect on weight. Low-energy vegetables, usually
allowed during a VLED, may partly compensate for the
low fibre content of VLED preparations. Re-feeding after VLED
After a VLED a re-feeding period is recommended to
Fat prevent abrupt retention of fluid and to prevent abdo-
The amount of fat obtained daily during a VLED varies minal discomfort. Generally, the recommended length of
in different preparations from 1 to 20 g. The fat content refeeding is 3–8 weeks (9,22,23). However, the optimal
of VLEDs may have an effect on the risk of developing length of the re-feeding period has not been studied, and
gallstones during the diet (17). Dietary fat is a stimulus for may depend on the nature of the weight reduction pro-
gall bladder contraction and during a fat-free VLED the gramme. We have used a shorter 2 week re-feeding period:
bladder does not empty. An important topic for research the first week on partial VLED use and the second week
would be to investigate the amount of fat in a VLED on a 5.0 MJ day-1 (1200 kcal) normal food diet. After this
necessary to prevent gallstone formation (18,19). the patients made individual changes based on their pre-
vious eating habits. The rationale for changing rapidly to
normal food was to ‘spare’ the sessions for the cognitive
Use of VLEDs
and behavioural part of the programme, as normal living
VLEDs have been developed to replace all meals and to be conditions are necessary, we believe, to learn and practise
used as a sole nutrition for a long period of time. The usual food related life style changes.
© 2001 The International Association for the Study of Obesity. obesity reviews 2, 61–72obesity reviews Very low energy diets P. Mustajoki & T. Pekkarinen 63
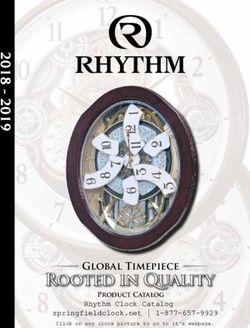
Repeated VLED Physiologic and metabolic effects of VLED
Smith and Wing (24) repeated a 12-week VLED period VLED causes many physiologic and metabolic changes,
4 months after an original VLED-period in 45 obese dia- which are summarized in Table 1. Because energy intake
betic patients. The first period produced a 15.5 kg mean in compliant patients is relatively constant during VLEDs,
weight loss, whereas the second only a 1.4 kg mean weight weight loss depends on daily energy expenditure. Men
loss. Poor results during the second VLED-period were due reduce weight, on average, more than women because they
to poor compliance. This is also our experience. There have higher energy expenditure due to bigger stature and
seems to be a high psychological threshold to begin another relatively more lean body mass. Similarly, severely obese
long VLED-period a few months after the first VLED persons expend more energy and loose more weight than
course. moderately obese persons. Figure 1 gives an example of
On the other hand, Rössner (25) compared a continuous weight loss during a VLED in moderately and severely
6-week VLED-period to an intermittent regimen consisting obese persons.
of three 2-week VLED periods separated by a monthly Many of the metabolic and physiologic effects of VLEDs
interval with a regular balanced low calorie diet. Mean (Table 1) are beneficial, such as improvement in insulin sen-
weight losses were identical in these groups at 14 and sitivity, lowering of blood pressure and lowering of serum
26 weeks. Thus, intermittent schedules of VLEDs may triglyceride values. Some deleterious effects of total fasting,
work but probably have no advantage over continuous use such as protein loss, can be avoided with VLEDs. However,
of VLEDs. there are some undesired metabolic consequences, e.g.
low serum HDL-cholesterol and high serum urate concen-
trations. The clinical importance of these changes is not
Partial use of VLED
known but may not be significant because of short dura-
Many obese subjects use VLED preparations to replace one tion and improvements soon after VLEDs when a eucaloric
or more daily meals or are on a VLED one or more days diet is introduced.
per week. Very little research on this partial use of VLEDs
has been published. In our study (26) obese diabetic
patients were instructed to eat normal breakfast and lun- Well-being and eating behaviour
cheon but to use a VLED during the rest of the day for
Mood and well-being
3 months. A control group received two short counselling
sessions for dietary changes. Weight loss was modest Psychological well-being during a VLED has been inten-
(about 2 kg) and there were no differences between groups. sively investigated. The majority of studies show improve-
These results suggest that partial use of VLEDs may not be ment in depression scores and anxiety but there may
useful in management of obesity but more investigations occasionally be individuals who have experienced adverse
are needed for final conclusions. psychological reactions (42). The positive effects are not
Table 1 Summary of metabolic and physiologic effects of VLEDs
Subject Effect
Weight loss BMI 30–35 kg m–2: around 1.5 kg per week
BMI 35–40 or >40 kg m–2: 1.5–2.5 kg per week
Protein loss and Initial increased nitrogen loss that levels off when diet is continued (27,28)
body composition Body composition normal after weight reduction (29–31)
Ketosis Blood concentrations and urinary excretion of ketoacids increases from the first week (27)
Lipid metabolism Serum total cholesterol, LDL-cholesterol and triglycerides decrease. In individuals with high initial values the change is marked
(5,22,27,33)
Serum HDL-cholesterol decreases slightly during VLED but increases after the diet (5)
Glucose metabolism Insulin resistance and blood glucose concentration decrease in type 2 diabetic patients (32,34)
May result in hypoglycaemia in patients on oral or insulin medications (32)
Blood pressure In hypertensive subjects diastolic and systolic blood pressure decrease clearly (5,9,21,35–37)
Cardiac function No increase in dysrhythmias on ambulatory ECG (38,39,40)
Other effects Serum electrolyte concentrations remain normal (22,27)
Serum urate concentration increases temporarily (10)
Serum triiodothyronine (T3) decreases and reverseT3 increases (27,41)
© 2001 The International Association for the Study of Obesity. obesity reviews 2, 61–7264 Very low energy diets P. Mustajoki & T. Pekkarinen obesity reviews
Figure 2 Mean scores of Binge Eating Scale (BES) in three outcome
classes after a weight reduction programme, which included an 8-week
VLED period. **P < 0.01, ***P < 0.001 as compared with the baseline
score. A good result is more than 10% weight loss (n = 19), partial
0–10% weight loss (n = 24) and poor result increased weight (n = 13)
Figure 1 Weight loss during an 8-week VLED period. (Derived from compared with pretreatment weight at the two year follow-up (derived
(2)). with permission from (2).
related to the degree of ketogenesis (42) or to changes in It has been proposed that dieting is a risk factor for
serum triiodothyronine concentrations (41). It seems that eating disorders and, thus, a VLED could induce binge
improvement of mood is seen only when behavioural eating. Several studies have shown that this does not
therapy is included in the programme whereas VLEDs happen. In our study (3) moderately obese non-bingers
alone may not have positive effects on mood (42). took part in a weight reduction programme which included
an 8-week VLED-period. The mean scores of the Binge
Eating Scale (Fig. 2), as well as of the Bulimic Investigatory
Hunger
Test Edinburgh, improved after the programme. The scores
Several studies have shown that during a VLED the sub- remained at the lower level for 2 years in those patients
jective feeling of hunger decreases or remains at pretreat- who succeeded in maintenance of weight loss. Also, other
ment levels (41,42). Some transient increase of hunger may studies have shown improvement of eating behaviour
be seen during the first week. In comparative studies obese during and after a weight reduction programme using a
subjects feel less hunger during a VLED than during a VLED (48).
balanced 5.0–6.7 MJ d-1 (1200–1600 kcal) low calorie diet LaPorte (49) compared obese binge eaters and non-
(43). During VLEDs food cravings are similar to those binge eaters in a weight reduction programme using VLEDs
experienced during low calorie diets and, in general, and behavioural therapy. No significant differences were
reduced compared to the pretreatment period (44). found between binge and non-binge groups on measures
of weight loss, adherence to the diet or drop-out rate.
Binge eaters had more psychological disturbances at
Exercise
baseline. Their depression decreased but anxiety did not
Many VLED-based weight reduction programmes have change.
regular supervised exercise included (45–47). They show
that a VLED does not impair moderate submaximal
aerobic and weight training exercise. Safety and side-effects during VLED
Minor short-term harmful effects
Binge eating
VLEDs are associated with side effects which may cause
Two questions are related to binge eating and VLEDs: (1) some discomfort but do not threaten health. Many patients
does the diet induce binge eating in previous non-bingers? experience cold intolerance and dryness of the skin
and (2) how do binge eaters react to a weight reducing (Table 2) (10). These appear typically during 3–5 weeks on
programme using VLED? a VLED and are related to decreased metabolic rate during
© 2001 The International Association for the Study of Obesity. obesity reviews 2, 61–72obesity reviews Very low energy diets P. Mustajoki & T. Pekkarinen 65
Table 2 Subjective feelings during the last week of an 8-week VLED is not always known why some patients feel more tired
period. The study group comprised of 62 subjects, mean base-line
whereas most feel more energetic during VLED.
body mass index 36.4 kg m–2 and mean weight loss 12 kg (Unpublished
data from (3))
Cholelithiasis
Feeling of symptom Frequency
Rapid weight loss induces formation of gallstones and this
General well being*
has been observed also during VLEDs. Reported frequen-
Better 74%
Same 26
cies of new gallstones during VLEDs vary from 11 to 28%
Worse 0 (17,50–53). There are probably two different mechanisms
Feeling tired* for excessive stone formation. The bile is more saturated
Less tired 63 and lithogenic because of mobilisation of cholesterol from
Same 22
adipose tissue, and gallbladder contraction and emptying
More tired 15
Physical condition*
are imperfect due to minimal amount of fat in the diet.
Better 59 The studies which have demonstrated a high risk of
Same 33 cholelithiasis have used VLED preparations which contain
Worse 8 no, or negligible, amounts of fat. Addition of fat to the diet
Feeling hunger
stimulates emptying of the gall bladder and can prevent for-
No 44
Mild 52
mation of gallstones (18,19). Thus, the low fat content of
Moderate 4 the diet may be an important risk factor for cholelithiasis,
Cold intolerance but it is not known what the risk is for gallstone forma-
No 15 tion in VLED preparations containing moderate amounts
Moderate 63
of fat. Formation of gallstones can also be prevented
Much 22
Dry skin
by decreasing bile lithogenicity with ursodeoxycholic acid
No 4 (50,53).
Moderate 48
Much 48
Liver function
*The subjects were asked how they feel as compared with the Severe obesity is often associated with fatty infiltration
pretreatment time.
of the liver. Marked regression of fatty change is observed
during VLEDs (54,55). Liver function enzymes (serum
transaminases, LDH, alkaline phosphatase) may rise
dieting. The only measures needed are warm clothing and mildly during the first weeks of VLEDs but later,
basal skin ointments. during weight maintenance, they are lower than before
Significant hair loss occurs in about 10% of patients therapy.
using VLED for a longer period (22). It develops slowly In some patients slight degrees of portal inflammation
and becomes manifest usually after the diet period. Hair and fibrosis have been seen during a VLED (55). This
loss is diffuse and not complete. It may cause cosmetic occurred only in patients with rapid weight loss (more than
problems and patients find it annoying but otherwise it is 230 g day-1). Andersen and co-workers (55) hypothesized
harmless and temporary. Hair starts to grow again after a that rapid mobilization of intracellular triglycerides and
few months. subsequent secretion of fatty acids may induce portal
Use of VLEDs is often associated with altered bowel inflammation. The clinical significance of these changes is
function (10,22). These changes are individual. Constipa- not known. Liver failure or cirrhosis associated with the
tion seems to be more common but also loose stools or use of VLEDs has not been reported.
diarrhoea have been reported (22). Low energy vegetables
during a VLED period may diminish constipation. In more
Gout
severe cases bran or other fibre preparations can be used.
During the first 2–3 days on a VLED patients often experi- Serum uric acid increases during the first weeks on a VLED
ence headaches, dizziness and fatigue. Some may have (10,22). Despite this attacks of gout are rare although
orthostatic hypotension, which is probably caused by dehy- patients with a history of gout may occasionally develop
dration (31). Variable degrees of fatigue and dizziness have an acute attack (10). We have supervised some 1500
also been reported during later weeks on a VLED (10,22). patients who have used VLEDs and have never experienced
These are usually mild and do not cause discontinuation of attacks of gout during the diet (unpublished). In patients
the diet. In our experience dehydration is the most common with a history of gout we have used allopurinol
individual cause for fatigue and dizziness. However, it 300 mg day-1 during the diet as prophylaxis.
© 2001 The International Association for the Study of Obesity. obesity reviews 2, 61–7266 Very low energy diets P. Mustajoki & T. Pekkarinen obesity reviews
metabolic and physiologic adaptation to drastic diets may
Bone loss
be decreased. Thus, in people over 65 years it may be safer
In obese subjects bone mineral content is higher than to restrict use of VLEDs to cases in which weight loss is
in normal weight subjects. Weight loss with a VLED is imperative to restore functioning (59).
associated with decreased bone mineral density (56,57). For clinicians it is usually clear that during severe sys-
Decreased mineral content is also seen during weight reduc- temic or organ disease strict diets like VLEDs should not
tion using less intensive diets, such as low fat diet (58), and be used. The decision is more difficult, however, in diseases
the degree of mineral loss is associated strongly with the in which severe obesity considerably aggravate symptoms.
amount of weight lost. It is not known whether the In clinical practise this question arises often in severely
decrease in bone mineral density is a physiologic adap- obese patients with heart failure and pulmonary insuffi-
tation to reduced weight or whether a VLED has some ciency. In such cases clinicians must evaluate the risks
specific effects on the bone. of remaining severely obese against the risks of weight
loss with a VLED. We have used VLEDs in some severely
obese patients with end-stage heart failure without serious
Contraindications
harmful effects and with marked clinical improvement
Table 3 gives a summary of contraindications presented in (unpublished observations).
different reviews (9,10,32,59,60).
Relative weight is an important factor. VLEDs should
Indications
never be used by normal weight subjects because it leads
to excessive loss of lean body mass. This warning should VLEDs may be indicated in obese subjects with
be widely communicated. VLEDs are not usually recom- BMI >30 kg m-2. It is not a first-hand method for obese
mended in the body weight range BMI 25–30 kg m-2 people but is an alternative for individuals who have failed
because dietary and behavioural programmes without with more conservative approaches to weight loss (10). In
VLEDs may also produce satisfactory weight loss. the management of obesity a patient-centred approach (61)
However, selected patents with central obesity and with is important for which reason a patient’s choice may
concomitant diseases (such as diabetes, dyslipidaemia and determine which weight loss method is used.
hypertension) may occasionally be targets for VLEDs if VLEDs may be the more advantageous the higher the
other approaches have failed (10). degree of overweight although this has not been confirmed
Certain physiological states with increased nutritional in any comparative trials. In patients with severe obesity
demands like pregnancy and lactation are contraindica- (BMI 35–40 kg m-2) our policy is usually to use a VLED-
tions for VLEDs. For children who are still growing a programme. In morbid obesity (BMI >40 kg m-2) we use a
VLED should usually be avoided. However, there may be VLED-based programme as a first-line therapy.
children in which severe obesity is resistant to other treat- One determinant for using VLEDs may be concomitant
ments. In such cases the risks of remaining obese should be diseases, which are responsive to weight loss (10). Among
individually weighed against the risks of using a VLED. them is type 2 (non-insulin dependent) diabetes, dyslipi-
VLEDs can be used in selected cases in experienced hands daemias, hypertension (and especially their combination,
and according to some reports this can be done without the metabolic syndrome) and sleep apnoea syndrome.
significant harmful effects (10). Rapid improvement of symptoms and laboratory
There are very little reports in which a VLED has been values may motivate patients to strive harder towards
used in elderly people aged more than 65 years. At that age maintenance.
Table 3 Contraindications to long courses
Absolute contraindications Relative contraindications
(6–16 weeks) of very low energy diets
Normal weight (body mass index 65 years
Any severe systemic or organ disease Childobesity reviews Very low energy diets P. Mustajoki & T. Pekkarinen 67
Special indications for VLEDs are situations in which reduces the plasma glucose concentration independently of
rapid weight loss is clinically important. Severe obesity may weight loss (23). For this reason hypoglycaemia is likely to
be a contraindication for orthopaedic or other surgery. In occur if antidiabetic medication has not been reduced. We
such cases relatively large and rather rapid weight loss is reduced the dose of oral anti-diabetic agents by 50% at the
often necessary (8). Morbidly obese patients with severe beginning of the VLEDs if blood glucose control has been
pulmonary failure may need immediate reduction of poor (glycohaemoglobinA1c more than 9–10% or fasting
weight, and there may be other conditions in which rapid blood glucose >10 mmol L-1) and discontinue them alto-
weight loss is mandatory. gether if glucose control has been better. If the patient is
on long-acting insulin we reduce the doses by at least 50%.
Home glucose monitoring is necessary, and during the diet
Concomitant medication
the medication should be tailored according to fasting
There are two questions when medication during a VLED glucose values.
is evaluated: does the diet affect the metabolism of a drug Combined hyperlipidaemia will respond markedly to
and what effects does the diet have on the disease for which VLEDs for which reason medication is usually not needed
a drug has been prescribed? during the diet. Medication for hypertension is continued
We found only one study in which drug metabolism has otherwise but stopping of diuretics is commonly recom-
been investigated during a VLED. Sonne and co-workers mended (10,22,32) because VLEDs themselves have a
(62) showed that during a 2 week VLED-period meta- diuretic effect. Our experience is that VLEDs do not cause
bolism of antipyrine remained unchanged but metabolism sudden changes in the dose of warfarin. Thus, we continue
of oxazepam decreased slightly. For the great majority of the pretreatment dose and monitor thrombotest value
drugs we must rely on clinical experience when evaluating weekly.
medication during VLED.
According to Henry and Gumbiner (32) patients on
VLEDs seem to be more sensitive to the side effects of most Medical monitoring
medications and, thus, require close monitoring and dose Pretreatment evaluation
adjustment. This is not our experience. More than 70% of
our patients in VLED-programmes are on regular medica- Before a long VLED-based period a medical evaluation is
tion for chronic diseases. They have continuous medication necessary. Many authors recommend extensive laboratory
for ischaemic coronary disease, hypertension, dysrhyth- investigations to ensure that a VLED can be used safely
mias, epilepsy, asthma (7), depression, etc. with the same (10,22,32). We do not use routine laboratory tests for pre-
doses as before the diet, and no increase in side effects treatment evaluation. We rely on comprehensive medical
observed. This suggests that VLEDs may not significantly history and physical examination, and use laboratory tests
alter drug metabolism. only if these give indications for further investigations. We
Table 4 summarizes situations in which medication have not observed any problems with that approach.
should be decreased or special care is needed. The most
important is diabetes because a VLED itself markedly Monitoring during VLEDs
Earlier reviews suggest that during VLEDs regular labora-
tory and clinical follow-up is important (10,22,32) but the
Table 4 Medication during very low energy diets usefulness of these tests has not been confirmed in studies.
We conduct VLED-programmes without routine labora-
Medication Action
tory investigations, and use laboratory tests only when
Insulin or oral hypoglycemic Decrease or stop patients’ diseases need monitoring, e.g. in diabetes, during
agents for type 2 diabetes anticoagulant medication, etc. A physician familiar with
Drugs for hyperlipidaemias Stop or decrease except in familial VLEDs must be available for consultation if patients
hypercholesterolaemia experience unexpected problems during the diet.
Drugs for hypertension Stop diuretics, continue others. Taper
according to blood pressure values
Warfarin Continue prediet dose, monitor INR
Cognitive and behavioural approaches
often and change dose accordingly for maintenance
Drugs for angina pectoris, Continue with pretreatment doses
asthma, epilepsy,
There is a general agreement that VLEDs should not be
psychopharmacas for used alone but always in connection with cognitive and
depression or anxiety, etc. behaviour counselling (63–66) for permanent lifestyle
changes. This is mandatory because body weight will
© 2001 The International Association for the Study of Obesity. obesity reviews 2, 61–7268 Very low energy diets P. Mustajoki & T. Pekkarinen obesity reviews
invariably be regained after VLEDs if used without addi-
tional measures.
An ideal way to integrate cognitive behaviour coun-
selling with a VLED-period has not been studied. In prin-
ciple there are two possibilities. One is to conduct a
VLED-period first and to start the cognitive behaviour
counselling after that. Our approach is to begin counselling
from the first session, i.e. during the VLED-period in the
first half of the programme. During VLEDs it is not appro-
priate to address food-related topics like slowing the pace
of eating, separating eating from other activities, shopping
for food according to a list, etc. Instead, during VLEDs
exercise-related topics, stimulus control, etc. may be coun-
selled. After the VLED-period there must be enough ses-
sions to carry out cognitive behaviour counselling in more
normal living conditions.
During the recent years there has been a trend to longer
weight reduction programmes or to separate maintenance
visits to improve long-term outcome. Several researchers
have stressed the importance of continuous, long-term care
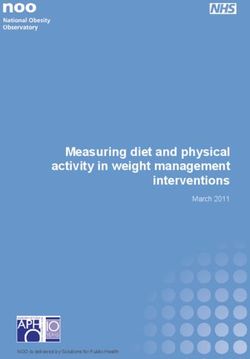
Figure 3 Individual variation after a weight reduction programme using
in the treatment of obesity as in any other chronic disor- a VLED-based or non-VLED programme. Percentage weight changes
der (66,67). Longer programmes with maintenance phase, from baseline at 5-year follow-up. Circles represent women, triangles
however, have been associated with weight gain already represent men. BT, behavioural therapy; VLED, very low calorie diet.
during intervention (68–71). Thus, longer and longer pro- (From (3) with permission).
grammes may not be an automatic solution for the problem
of maintenance in VLED-based programmes (72).
Results of weight reduction programmes
using VLEDs
Typically patients in the VLED programmes have initial
large weight losses, but they regain weight later, during or
after the treatment (4,5,68–71,73–80). Mean initial weight
losses during an 8–16-week VLED phase have ranged from
12 to 35 kg. Weight gain is a rule after the therapy but
amount of weight regained has varied.
Individual treatment outcomes usually include wide ranges
(Fig. 3) and, therefore, reporting of weight loss results as mean
values may not be informative. In clinical practise, it is useful
to know how many patients who have begun a programme Figure 4 Changes (mean ± SD) in weight during treatment and follow-
have a satisfactory long-term outcome. In some studies up in three outcome groups. A good result is more than 10% weight
almost all have regained their weight after a few years (79) loss, partial 0–10% weight loss and poor result increased compared to
but in others outcomes have been better. In our prospective pretreatment weight (from (2) with permission).
2-year-study (3) 35% of obese subjects maintained their
weight loss of 10% or more and 42% lost 0–10% of their
initial weight after 2 years (Fig. 4). In a recent study of atic review of the randomized trials with a minimum of 30
Anderson and co-workers a quarter of the patients had patients and an 1 year follow-up or more (Table 5). The
maintained a weight loss of 10% 7 years after therapy (76). non-VLED approach in these programmes has usually been
a 1200 kcal day-1 balanced diet combined with behavioural
therapy. The mean age of the patients has varied from 39
Comparison of behavioural therapies with
to 52 years and duration of the VLED periods from 8 to
and without VLEDs
16 weeks.
For the comparison of outcomes after weight reduction At the end of the programmes the mean weight loss with
programmes with and without VLEDs we made a system- VLEDs ranged from 9.2 to 19.3 kg and that of the non-
© 2001 The International Association for the Study of Obesity. obesity reviews 2, 61–72obesity reviews Very low energy diets P. Mustajoki & T. Pekkarinen 69
Table 5 Randomized controlled trials in which a VLED programme has been compared to a non-VLED programme
Study/Country (ref.) Number Mean initial Treatments and mean weight Drop-out Follow-up weight loss
F/M weight or BMI loss rate
Wadden et al. 1986,1988, 50/9 F 107 kg VLCD 4 mo: 14.1 kg 15.3% VLCD 1 yr 4.6 kg
USA (77,78) M 122 kg BT 6 mo: 14.3 kg BT 1 yr 9.5 kg
VLCD + BT 6 mo: 19.3 kg# VLCD + BT 1 yr 12.9 kg†
Wing et al. 1991, 26/10 BMI BT 20 wks 10.1 kg 8% BT 1 yr 6.8 kg
USA (80) 37–38 kg m–2 BT + VLCD 20 wks 18.6 kg# VLCD + BT 1 yr 8.6 kg
Wing et al. 1994, 60/33 BMI BT 50 wks 10.5 kg 15% BT 2 yr 5.7 kg
USA (68) 37–38 kg m–2 VLCD + BT 50 wks 14.2 kg VLCD + BT 2 yr 7.2 kg
Wadden et al. 1994, 49/0 BMI BT 1.5 yr 12.2 kg 24%
USA (69) 39.5 kg m–2 VLCD + BT 1.5 yr 10.9 kg
Ryttig et al. 1997, 44/36 BMI BT 26 mo 7% 48%
Sweden (70) 37.6 kg m–2 VLCD + BT 26 mo 10%
VLCD + BT* 26 mo 9.5%
Torgerson et al. 1997, 74/39 BMI BT 24 mo 6.2 kg 23%
Sweden (71) 40.4 kg m–2 VLCD + BT 24 mo 9.2 kg
BT, behavioural therapy; VLED, very low energy diet; F, female; M, male. *+1 sachet per day during maintenance. #significantly greater than the BT
group. †significantly better than the VLCD group.
VLED programmes from 6.2 to 14.3 kg. The studies with Maintenance is the greatest problem in all conservative
1- or 2-year follow-up have shown a mean weight loss of approaches to obesity management. There is no evidence
7.2–12.9 kg with VLEDs and 5.7–9.5 kg without VLEDs. that VLED-programmes lead to worse long-term results or
Thus, no study has conclusively shown that in the long- are associated with more untoward effects than pro-
term VLED-programmes are better than non-VLED grammes with low calorie or other dietary approaches.
programmes. Thus, VLED-programmes are alternatives for other con-
servative weight reduction programmes in patients who
meet the indications and do not have contraindications to
Gender difference?
using VLEDs. In diabetes a VLED-based programme may
The patients in the randomized controlled trials (Table 5) result in better long-term glucose metabolism than non-
were mainly severely obese females (70.5%). Other stud- VLED programmes (23). In clinical situations in which
ies, which have included men, suggest an interesting gender rapid weight loss is needed a VLED-programme is a prefer-
difference in the outcome. In the study of Torgerson able therapy.
and co-workers (71) a 24-month mean weight loss was The published studies on long-term results of VLED-
15.5 kg among men and 5.6 kg among women. In line programmes have given variable results. In some, series
with this, we (4) found after a VLED-programme consid- maintenance after a VLED has been satisfactory suggesting
erably better weight loss at 5-year follow among men than that in certain patient populations and with certain cogni-
among women (26.6 and 9.9 kg, respectively, the interac- tive behavioural approaches the results may be better. This
tion with sex P = 0.03). Interestingly, in a non-VLED gives direction for future research. We certainly do not yet
programme men succeeded less satisfactorily than women know which ways of counselling and cognitive behavioural
(5-year mean weight loss men 1.9 and women 7.9 kg) (4). therapy are optimal in VLED-programmes to ensure main-
Similar results have been reported by Nunn and co-workers tenance. Another important topic for future research is
(81). gender difference. If better long-term outcomes among men
are confirmed, it will provide guidelines to the selection of
patients for VLED-based weight reduction programmes.
Present status and future of VLEDs
VLEDs accomplish what they were intended to do – namely
produce maximum initial weight loss (23). It can be con- References
ducted safely in patients with obesity associated diseases, 1. Obesity in Scotland. Integrating prevention with weight
such as diabetes and hypertension, or with other chronic management. A national clinical guideline recommended for
diseases. use in Scotland by the Scottish intercollegiate guidelines network.
© 2001 The International Association for the Study of Obesity. obesity reviews 2, 61–7270 Very low energy diets P. Mustajoki & T. Pekkarinen obesity reviews
(1996). [WWW document]. URL http://www.show.scot.nhs.uk/ 21. Torgerson JS, Ågren L, Sjöström L. Effects on body weight of
sign/clinical.pdf/sign8.pdf strict or liberal adherence to an initial period of VLED treatment.
2. Clinical guidelines on the identification evaluation and treat- A randomised, one year clinical trial of obese subjects. Int J
ment of overweight and obesity in adults-the evidence report. Obesity 1999; 23: 190–197.
Obesity Res 1998; 6: 51S–209S. 22. Anderson JW, Hamilton CC, Brinkman-Kaplan V. Benefits
3. Pekkarinen T, Takala I, Mustajoki P. Two year maintenance and risks of an intensive very-low-calorie diet program for severe
of weight loss after a VLED and behavioural therapy for obesity: obesity. Am J Gastroenterol 1992; 87: 6–15.
correlation to the scores of questionnaires measuring eating 23. Wing RR. Use of very-low-calorie diets in the treatment of
behaviour. Int J Obesity 1996; 20: 332–337. obese persons with non-insulin-dependent diabetes mellitus. J Am
4. Pekkarinen T, Mustajoki P. Comparison of behavior therapy Diet Assoc 1995; 95: 569–572.
with and without very-low-energy diet in the treatment of morbid 24. Smith DE, Wing RR. Diminished weight loss and behavioral
obesity. Arch Intern Med 1997; 157: 1581–1585. compliance during repeated diets on obese patients with type II
5. Pekkarinen T, Takala I, Mustajoki P. Weight loss with very- diabetes. Health Psychol 1991; 10: 378–383.
low-calorie diet and cardiovascular risk factors in moderately 25. Rössner S. Intermittent vs. continuous VLED therapy in
obese women: One year follow-up study including ambulatory obesity treatment. Int J Obesity 1998; 22: 190–192.
blood pressure monitoring. Int J Obesity 1998; 22: 661–666. 26. Sane T, Mustajoki P. Poorly controlled obese patients with
6. Lojander J, Mustajoki P, Rönkä S, Mecklin P, Maasilta AP. A non-insulin-dependent diabetes, insulin or diet? Diabetologia
nurse-managed weight redustion programme for obstructive sleep 1992; 35: A195.
apnoea syndrome. J Int Med 1998; 244: 251–255. 27. Henry RR, West-Kent TA, Scheaffer L, Kolterman OG,
7. Stenius-Aarniala B, Poussa T, Kvarnströn J, Grönlund E-L, Olefsky JM. Metabolic consequences of very-low-calorie diet
Ylikahri M, Mustajoki P. Immediate and long term effects of therapy in obese non-insulin-dependent diabetic and nondiabetic
weight reduction in obese people with asthma: randomised subjects. Diabetes 1986; 35: 155–164.
controlled study. BMJ 2000; 320: 827–832. 28. Morgan WD, Ryde SJS, Birks JL, Thomas DW, Kreitzman
8. Pekkarinen T, Mustajoki P. Use of very-low-calorie diet in SN. Changes in total body nitrogen during weight reduction
preoperative weight loss: efficacy and safety. Obes Res 1997; by very-low-calorie diets. Am J Clin Nutr 1992; 56: 262S–
5: 595–602. 264S.
9. Wadden TA, Stunkard AJ, Brownell K. Very low calorie diets: 29. Burgess NS. Effect of a very-low-calorie diet on body compo-
their efficacy, safety and future. Ann Intern Med 1983; 99: sition and resting metabolic rate in obese men and women. J Am
675–684. Diet Assoc 1991; 91: 430–434.
10. National Task Force on the Prevention and Treatment of 30. Kamrath RO, Plummer LJ, Sadur CS, Weinstein RL. Body
Obesity. Very Low-calorie diets. JAMA 1993; 270: 967–974. composition and weight maintenace with a very-low-calorie diet
11. Wadden TA, Stunkard AJ. Controlled trial of very low calorie for treatment of moderate obesity. Am J Clin Nutr 1992; 56:
diet, behavior therapy, and their combination in the treatment of 286S–287S.
obesity. J Consult Clin Psychol 1986; 54: 482–488. 31. Hoie LH, Bruusgaard D, Thom E. Reduction of body mass
12. Garrow JS, Webster JD, Pearson M, Pacy PJ, Harpin G. and change in body composition on a very low calorie diet. Int J
Inpatient-outpatient randomized comparison of Cambridge diet Obes 1993; 17: 17–20.
versus milk diet in 17 obese women over 24 weeks. Int J Obesity 32. Henry R, Gumbiner B. Benefits and limitations of very-low-
1989; 13: 521–529. calorie diet therapy in obese NIDDM. Diabetes Care 1991; 14:
13. Sakata T. A very-low-calorie conventional Japanese diet: its 802–823.
implications for prevention of obesity. Obes Res 1995; 3: 33. Uusitupa MIJ, Laakso M, Sarlund H, Majander H, Takala J,
233s–239s. Penttilä I. Effects of a very-low-calorie diet on metabolic control
14. Foster GD, Wadden TA, Peterson FJ, Letizia KA, Barlett SJ, and cardiovascular risk factors in the treatment of obese non-
Conill AM. A controlled comparison of three very-low-calorie insulin-dependent diabetics. Am J Clin Nutr 1990; 51: 768–
diets: effects on weight, body composition, and symptoms. Am J 773.
Clin Nutr 1992; 55: 811–817. 34. Kelley DE, Winf RR, Buonocore C, Sturis J, Polonsky K,
15. Wing RR, Vazquez JA, Ryan CA. Cognitive effects of keto- Fitxsimmons M. Relative effects of calorie restriction and weight
genic weight reduction diets. Int J Obes 1995; 19: 811–816. loss on noninsulin-dependent diabetes mellitus. J Clin Endocr
16. Astrup A, Vrist E, Quaade F. Dietary fibre added to very low Metab 1993; 77: 1287–1293.
calorie diet reduces hunger and alleviates constipation. Int J 35. Atkinson RL, Kaiser DL. Nonphysician supervision of a very-
Obesity 1990; 14: 105–112. low-calorie diet. Results Over 200 Cases Int J Obesity 1981; 5:
17. Kamrath RO, Plummer LJ, Sadur CN, Adler MA, Strader WJ, 237–241.
Young RL, Weinstein RL. Cholelithiasis in patients with a very low 36. Maxwell MH, Kushiro T, Dornfeld LP, Tuck ML, Waks AU.
calorie diet. Am J Clin Nutr 1992; 56: 255S–257S. BP changes in obese hypertensive subjects during rapid weight loss.
18. Hoy MK, Heshka S, Allison DB, Grasset E, Abiri M, Heyms- Arch Intern Med 1984; 19: 67–73.
field SB. Reduced risk of liver-function-test abnormalities and new 37. DasGupta P, Bridgen G, Ramhamdany E, Lahiri A, Baird IM,
gallstone formation. Am J Clin Nutr 1994; 60: 249–254. Raftery EB. Circadian cariation and blood pressure: response to
19. Festi D, Colecchia A, Orsini M, Sangermano A, Sottili S, rapid weight loss by hypocaloric hyponatraemic diet in obesity.
Simoni P, Mazzella G, Villanova N, Bazzoli F, Lapenna D, Petroni J Hypertens 1991; 9: 441–447.
ML, Pavesi S, Neri M, Roda E. Gallbladder motility and gallstone 38. Moyer CL, Holly RG, Amsterdam EA, Atkinson RL. Effects
formation in obese patients following very low calorie diets. Use of cardias stress during a very-low-calorie diet and exercise
it (fat) to lose it (well). Int J Obesity 1998; 22: 592–600. program in obese women. Am J Clin Nutr 1989; 50: 1324–
20. Rössner S. Effects of 46 weeks of very-low-calorie-diet treat- 1327.
ment on weight loss and cardiac function. Obes Res 1998; 6: 39. Doherty JU, Wadden TA, Zuk L, Letizia A, Foster GD, Day
462–463. SC. Long-term evaluation of cardiac function in obese patients
© 2001 The International Association for the Study of Obesity. obesity reviews 2, 61–72obesity reviews Very low energy diets P. Mustajoki & T. Pekkarinen 71 treated with a very-low-calorie diet: a controlled clinical study of 59. Pi-Sunyer FX. The role of very-low-calorie diets in obesity. Am patients without underlying cardiac disease. Am J Clin Nutr 1991; J Clin Nutr 1992; 56: 240S–243S. 53: 854–858. 60. van Gaal L. Dietary treatment of obesity. In: Bray GA, 40. Seim HC, Mithcell JE, Pomeroy C, de Zwaan M. Electro- Bouchard C, James WPT (eds). Handbook of Obesity. Marcel cardiographic findings associated with very low calorie dieting. Dekker: New York, 1998, pp 875–890. Int J Obesity 1995; 19: 817–819. 61. Rollnick S. Behaviur change in practice: targeting individuals. 41. Wadden TA, Mason G, Foster GD, Stunkard AJ, Prange AJ. In J Obes 1996; 20: S22–S26. Effects of very low calorie diet on weight, thyroid hormones and 62. Sonne J, Dragsted J, Loft S, Dosing M, Andreasen F. Influence mood. Int J Obes 1990; 14: 249–258. of very low calorie diet on the clearance of oxazepam and 42. O’Neil POM, Jarrell MP. Psychological aspects of obesity and antipyrine in man. Eur J Clin Pharmacol 1989; 36: 407– very low calorie diets. Am J Clin Nutr 1992; 54: 185S–189S. 409. 43. Rosen JC, Hunt DA, Sims EAH, Bogardus C. Comparison of 63. Mustajoki P. Management of individuals who are obese. carbohydrate-containing and carbohydrate-resticted hypocaloric Behaviour modification and other aspects. Dis Manage Health diets in the treatment of obesity: effects on appetite and mood. Am Outcomes 1998; 4: 267–275. J Clin Nut 1982; 36: 463–469. 64. Wing RR. Behavioral approaches to the treatment of obesity. 44. Harvey J, Wing RR, Mullen M. Effects on food cravings of In: Bray GA, Bouchard C, James WPT (eds). Handbook of very low calorie diet or a balanced, low calorie diet. Appetite 1993; Obesity. Marcel Dekker: New York, 1998, pp 855–873. 21: 101–115. 65. Foreyt JP, Poston WS. The role of the behavioral counselor in 45. Shinney S. Exercise during and after very-low-calorie dieting. obesity treatment. J Am Diet Ass 1998; 98: S27–S30. Am J Clin Nut 1992; 56: 190S–194S. 66. Wadden TA, Foster GD. Behavioral treatment of obesity. Med 46. Donnelly JE, Jacobsen DJ, Jakicic JM, Whatley JE. Very low Clin NA 2000; 84: 441–461. calorie diet with concurrent versus delayed and sequential exer- 67. Hill J. Dealing with obesity as a chronic disease. Obesity Res cise. Int J Obes 1999; 18: 469–475. 1998; 6: S34–S38. 47. Fogelholm M, Kukkonen-Harjula K, Oja P. Eating control and 68. Wing RR, Blair E, Marcus M, Epstein LH, Harvey J. Year- physical activity as determinants of short-term weight maintenance long weight loss treatment for obese patients with type II diabetes: after a very-low-calorie diet among obese women. Int J Obes does including an intermittent very-low-calorie diet improve 1999; 23: 203–210. outcome? Am J Med 1994; 97: 354–362. 48. Wadden TA, Foster GD, Letizia KA. One-year behavioral 69. Wadden TA, Foster GD, Letizia KA. One-year behavioral treatment of obesity: comparison of moderate and severe caloric treatment of obesity: comparison of moderate and severe caloric restriction and the effects of weight maintenance therapy. J restriction and the effects of weight maintenance therapy. Consult Clin Psychol 1994; 62: 165–171. J Consult Clin Psychol 1994; 62: 165–171. 49. LaPorte DJ. Treatment response in obese binge eaters: 70. Ryttig KR, Flaten H, Rössner S. Long-term effects of a very preliminary results using a very low calorie diet (VLCD) and low calorie diet in obesity treatment. A prospective, randomized, behavior therapy. Addict Behav 1992; 17: 247–257. comparison between VLED and a hypocaloric diet+behavior 50. Broomfield PH, Chopra R, Sheinbaum RC, Bonorris GG, modification and their combination. Int J Obes 1997; 21: Silverman A, Schoenfield LJ, Marks JW. Effects of ursodeoxy- 574–579. cholic acid and aspirin on the formation of lithogenic bile and gall- 71. Torgerson JS, Lissner L, Lindroos AK, Kruijer H, Sjöström L. stones during weight loss. New Engl J Med 1989; 319: 1567– VLED plus dietary and behavioral support versus support alone 1572. in the treatment of severe obesity. A randomized two-year clinical 51. Liddle RA, Goldstein RB, Saxton J. Gallstone formation trial. Int J Obes 1997; 21: 987–994. during weight-reduction dieting. Arch Intern Med 1989; 149: 72. Mustajoki P, Pekkarinen T. Maintenance programmes after 1750–1753. weight reduction – how useful are they? Int J Obes 1999; 23: 52. Kamrath RO, Plummer LJ, Sadur CN, Adler MA, Strader WJ, 535–555. Young RL, Weinstein RL. Cholelithiasis in patients treated with a 73. Wadden TA, Foster GD, Letizia K, Stunkard AJ. A multi- very-low-calorie diet. Am J Clin Nutr 1992; 56: 255S–257S. center evaluation of a proprietary weight reduction program for 53. Shiffman ML, Kaplan GD, Brinkman-Kaplan V, Vickers FF. treatment of marked obesity. Arch Intern Med 1992; 152: 961– Prophylaxis against gallstone formation with ursodeoxycholic acid 966. in patients participating in a very-low-calorie diet program. Ann 74. Anderson JW, Brinkman VL, Hamilton CC. Weight loss and Intern Med 1995; 122: 899–905. 2-y follow-up for 80 morbidly obese patients trated with intensive 54. Andersen T. Liver and gallbladder disease before and after very-low-calorie diet and an education program. Am J Clin Nutr very-low-calorie diets. Am J Clin Nutr 1992; 56: 235S–239S. 1992; 56: 244S–246S. 55. Andersen T, Gluud C, Franzmann M-B, Christoffersen P. 75. Flynn TJ, Walsh MF. Thirty-month evaluation of a popular Hepatiec effects of dietary weight loss in morbidly obese subjects. very-low-calorie diet Program- Arch Fam Med 1993; 2: J Hepatol 1991; 12: 224–229. 1042–1048. 56. Hylstrup L, Andersen T, McNair P, Breum L, Transbol I. 76. Anderson JA, Vichitbatra S, QiAN w, Kryscio RJ. Long-term Bone metabolism in obesity: changes related to severe overweight weight maintenance after an intensive weight-loss program. J Am and dietary weight reduction. Acta Endocrinol 1992; 129: Coll Nutr 1999; 18: 620–627. 393–398. 77. Wadden TA, Stunkard AJ. Controlled trial of very low calorie 57. Andersen RE, Wadden TA, Herzog RJ. Changes in bone diet, behavior therapy, and their combination in the treatment of mineral content in obese dieting women. Metabolism 1997; 46: obesity. J Consult Clin Psychol 1986; 54: 482–488. 857–861. 78. Wadden TA, Stunkard AJ, Liebschutz J. Three-year follow-up 58. Pritchard JE, Nowson CA, Wark JD. Bone loss accompany- of the treatment of obesity by very low calorie diet, behavioral ing diet-induced or exercise-induced weight loss: a randomised therapy, and their combination. J Consult Clin Psychol 1988; 56: controlled study. Int J Obes 1996; 20: 513–520. 925–928. © 2001 The International Association for the Study of Obesity. obesity reviews 2, 61–72
72 Very low energy diets P. Mustajoki & T. Pekkarinen obesity reviews
79. Wadden TA, Sternberg JA, Letizia KA, Stunkard AJ, Foster control in obese type 2 diabetic subjects. Arch Intern Med 1991;
GD. Treatment of obesity by very low calorie diet, behavior 151: 1334–1340.
therapy, and their combination: a five year perspective. Int J Obes 81. Nunn RG, Newton KS, Faucher P. 2. 5 year follow-up of
1989; 13: 39–46. weight and body mass index values in the Weight control for
80. Wing RR, Marcus MD, Salata R, Epstein LH, Miaskiewicz S, life! program. A descriptive analysis. Addict Behav 1992; 17:
Blair EH. Effects of a very-low-calorie diet on long term glycemic 579–585.
© 2001 The International Association for the Study of Obesity. obesity reviews 2, 61–72You can also read