Treatment for Breast Cancer in Patients with Alzheimer's Disease
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Treatment for Breast Cancer in Patients with Alzheimer’s Disease
Sherri Sheinfeld Gorin, PhD, w§# Julia E. Heck, MPH, § Steven Albert, PhD,wz k and
Dawn Hershman, MD, MS z
OBJECTIVES: To report use of breast cancer treatment Key words: Alzheimer disease; dementia; breast neo-
(surgery, radiation, and chemotherapy) by patients with plasms; physician’s practice patterns; decision-making
Alzheimer’s disease (AD).
DESIGN: Retrospective cohort study.
SETTING: Surveillance, Epidemiology, and End Results
(SEER) is a population-based cancer registry covering 14%
of the U.S. population.
PARTICIPANTS: Fifty thousand four hundred sixty breast
cancer patients aged 65 and older, of whom 1,935 (3.8%)
B reast cancer is, to a large degree, a disease of aging,
with women aged 65 and older having five times the
incidence of disease of younger women.1 In the coming
had a diagnosis of AD before or up to 6 months after cancer years, the aging of the U.S. population, combined with
diagnosis. lengthening life expectancy, will dramatically increase the
MEASUREMENTS: Diagnosis of AD was taken from In- number of cancer patients aged 65 and older.2 In addition,
ternational Classification of Diseases, Ninth Revision, di- older age at onset of cancer may be associated with greater
agnostic codes accompanying Medicare billing claims risk of functional limitations.3,4
between 1992 and 1999. The SEER program reported sur- Alzheimer’s disease (AD), a progressive neurodegener-
gery and radiation. Chemotherapy was taken from Medi- ative disorder, is the most common cause of dementia in
care billing records. older adults in the United States.5 Current diagnostic cri-
RESULTS: Subjects with AD were diagnosed with breast teria for AD were published in 1987.6 Overall, the prev-
cancer at later stages, when tumors were larger and the alence of AD varies from 1.1% for U.S. adults aged 65 to 69
likelihood of lymph node involvement had increased. Pa- to 52.5% for adults aged 95 and older; for moderate or
tients with AD had a lower likelihood of surgery (odds ratio severe AD, the prevalence is from 0.6% to 27.4%.7 A recent
(OR) 5 0.60, 95% confidence interval (CI) 5 0.46–0.81), study using claims data from the Medicare population
radiation (OR 5 0.31, 95% CI 5 0.23–0.41), and chemo- found AD diagnosed at an overall rate of 40.9 per 1,000
therapy (OR 5 0.44, 95% CI 5 0.34–0.58) than those with- individuals aged 65 and older.8
out AD. Cancer patients with AD may be diagnosed at later
CONCLUSION: Overall, AD patients receive less treat- stages of disease because of poor symptom recognition,9
ment for breast cancer than do comparable female Medicare reporting differences, or noncompliance with recommend-
beneficiaries. Chemotherapy and radiation are administered ed screening. In one North Carolina study, cognitive im-
less frequently to women with AD than to other comparable pairment was related to a 29% decrease in fecal occult
patients. It is unclear whether suboptimal medical care has blood test screening and decreases in adherence to ma-
an effect on their survival. Further research on the effect of mmography, clinical breast examinations, and Papa-
screening and treatment decision-making for these patients is nicolaou smear.10 A combination of factors may decrease
warranted. J Am Geriatr Soc 53:1897–1904, 2005. treatment rates in patients with AD.
Older cancer patients or their families may be more
From the Departments of Epidemiology and wSociomedical Sciences, likely to choose less-invasive therapies or to forgo treatment
z
§
Gertrude H. Sergievsky Center, Mailman School of Public Health; if the patient has dementia or functional limitations or if life
Department of Health and Behavior Studies, Teacher’s College; expectancy is perceived to be brief.11 In particular, cancer
k
Department of Neurology, zSchool of Medicine; and #Herbert Irving
Comprehensive Cancer Center, Columbia University, New York, New York.
patients diagnosed at later stages are among the most likely
to refuse treatment.12 There are important medical reasons
Preliminary findings were presented at the Annual Meeting of the Geronto-
logical Society of America, Washington, DC, November 19–23, 2004. for less treatment in older persons, including a higher risk
Funded by the Centers for Disease Control and Prevention (SSG, PI). for chemotherapy-related toxicities.13
Address correspondence to Sherri Sheinfeld Gorin, PhD, Columbia There is limited literature about the management of
University, 525 West 120th St, PO Box 239, New York, NY 10027. breast cancer in older women, because most clinical trials
E-mail: ssg19@columbia.edu are conducted with younger, healthier women who are typ-
DOI: 10.1111/j.1532-5415.2005.00467.x ically cared for by providers affiliated with cancer centers.
JAGS 53:1897–1904, 2005
r 2005 by the American Geriatrics Society 0002-8614/05/$15.001898 GORIN ET AL. NOVEMBER 2005–VOL. 53, NO. 11 JAGS
Furthermore, few population-based data exist on the use of Identification of Study Subjects
any cancer treatments by patients with AD. This study used Because AD is a disease of older people, eligible subjects
Surveillance, Epidemiology, and End Results (SEER)-Medi- were women aged 65 and older who were diagnosed with
care–linked data to describe breast cancer treatment in pa- pathologically confirmed Stage I to III breast cancer be-
tients with AD. tween January 1, 1992, and December 31, 1999; none had a
previous SEER diagnosis of any cancer. Included subjects
METHODS were age-eligible for Medicare, had a known diagnosis date
and cancer stage, and were beneficiaries of Medicare Parts
Data Sources A and B. In this retrospective cohort, to enhance specificity,
The National Cancer Institute developed the SEER pro- women were included if they were diagnosed with AD on
gram to provide ongoing information on cancer incidence two separate claims before a new diagnosis of breast cancer.
and mortality. The SEER registry encompasses 14% of the Because individuals who are enrolled in Medicare health
U.S. population from 11 geographic regions, including the maintenance organizations (HMOs) are not systematically
states of Connecticut, Hawaii, Utah, New Mexico, and Io- captured within these population-based administrative dat-
wa and the metropolitan areas of San Francisco/Oakland, abases, they were excluded to reduce missing values in the
Los Angeles, and San Jose/Monterey, California; Detroit, cohort. Patients with brain metastases were excluded. Be-
Michigan; Seattle, Washington; and Atlanta, Georgia. In- cause Stage IV patients are generally treated for palliation
formation from SEER registries is the most widely used rather than to prolong survival or to reduce recurrence, they
source of data on cancer incidence and treatment in the were excluded.
United States and is considered highly valid for clinical
pathologic information on tumor size, grade, and stage;
hormone receptor status; type of surgical treatment and Explanatory Variables
radiation therapy recommended or provided within 4 Sociodemographic factors of age, race, sex, and marital
months of diagnosis; follow-up of vital status; and cause status were obtained from the SEER database. SEER does
of death. Mortality data are provided through linkage to not report individual measures of socioeconomic status
death certificates. SEER collects annual audits of their data (SES). SES was measured using age- and race-specific cen-
to ensure quality and completeness, with an ascertainment sus-tract mean poverty level. Census-tract poverty is when
standard of 98%.14 20% of residences are below the federal poverty level.
Medicare is the primary health insurer for 97% of the Census-tract level percentage below poverty is considered a
U.S. population aged 65 and older. All Medicare benefici- reasonable and useful measure of economic deprivation.18
aries receive Part A benefits, and 95% of beneficiaries also Urban residence was defined as largest metropolitan
subscribe to Part B coverage.15 The Medicare Claims Data (41 million population), metropolitan (250,000–1 mil-
System, administered by the Centers for Medicare and lion), urban (20,000–250,000), less urban (2,500–20,000),
Medicaid Services, collects information on all services pro- and rural areas (o2,500 per county), from the source ge-
vided to Medicare beneficiaries under its hospital (Part A) ographic cancer registry. Tumor characteristics were de-
and supplemental (Part B) insurance plans.16 Claims from rived from SEER data.
three Medicare sources were used for the study: the Medi- AD was identified using the ICD-9 diagnostic code
care Provider Analysis and Review file (MedPAR), the Out- 331.0 that accompanies billings to Medicare. To capture
patient Standard Analytic File (SAF), and the 100% dementia more broadly for sensitivity purposes, in this
Physician/Supplier File. The MedPAR file includes all Part study, AD and related dementias were defined as including
A short-stay, long-stay, and skilled nursing facility bills and ICD-9-CM codes 331.0 and 290.0 (senile dementia,
contains one summarized record per admission, with up to uncomplicated), 290.1 (presenile dementia), 290.2
10 International Classification of Diseases, Ninth Revision, (senile dementia), 290.3 (senile dementia, with delirium),
Clinical Modification (ICD-9-CM) diagnoses. The SAF is and 797 (senility without mention of psychosis).8 To further
derived from the National Claims History File, which in- increase sensitivity, diagnoses of AD occurring up to 6
cludes all Medicare Part B (physician/supplier) claims for months after cancer diagnosis were included. This period
each calendar year. There are 10 fields for diagnoses and 10 was chosen to ensure that physicians had adequate expo-
fields for procedures codes in ICD-9-CM format; up to 10 sure to the patient to assess cognitive functioning, and to
procedures are coded in Current Procedural Terminology. reduce the likelihood of capturing any acute treatment
The 100% Physician/Supplier File is a subset of the Na- effects on cognition.19
tional Claims History file and is reported at the level of the Comorbidity was measured to determine whether there
claim. Each claim record includes some beneficiary demo- is a relationship between dementia and breast cancer treat-
graphic information, dates of service, procedure provided, ment independent of health status. The Deyo-Charlson co-
place of service, and diagnostic code in ICD-9-CM format. morbidity index, which was developed to identify and
Linkage between the SEER-Medicare files is based on classify comorbid disease from ICD-9 diagnoses, was
an algorithm involving a match of social security number, used.20 According to a previous study,21 depression was
name, sex, and date of birth, which has been described in measured using ICD-9-CM codes 300.4, 301.12, 309.0,
detail elsewhere.17 Individuals are not identifiable. Medi- 309.1, and 311.
care eligibility could be identified for 94% of persons aged The first course of treatment is defined in SEER as all
65 and older appearing in the SEER records.14 The linkage cancer-directed therapy before disease progression or treat-
allows for a population-based analysis of breast cancer di- ment failure or all planned therapy within the first year, as
agnosis and treatment. indicated in the medical record. Chemotherapy was iden-JAGS NOVEMBER 2005–VOL. 53, NO. 11 ALZHEIMER’S DISEASE AND BREAST CANCER TREATMENT 1899
tified from Medicare billings using the Health Care Financ- The study population thus included 50,460 breast can-
ing Administration Common Procedure Coding System cer patients, of whom 5,975 (11.8%) were diagnosed when
(HCPCS) J codes, which specify the specific chemotherapy the cancer was in situ, 23,779 (47.1%) at Stage I, 17,271
drug administered to an individual patient. Chemotherapy (34.2%) at Stage II, and 3,435 (6.8%) at Stage III. In this
codes included ICD-9-CM diagnostic codes V58.1 (chemo- study, access to Medicare records was from 1991 to 2001,
therapy), V66.2 (convalescence after administration of and breast cancer cases were diagnosed between 1992 and
chemotherapy), V67.2 (follow-up examination after chemo- 1999; thus, the mean follow-up time for surveillance of
therapy), 99.25 (procedural: injection or infusion of cancer dementia was 1,948 days (5.3 years). One thousand nine
chemotherapeutic substance) and HCPCS codes 964xx hundred thirty-five (3.8%) patients had a diagnosis of AD
(chemotherapy administration), 965xx (chemotherapy ad- within the period before or up to 6 months after cancer
ministration), and J9000-9999, J8510, J8520, J8521, and diagnosis.
J8530–J8999; codes reflecting types of chemotherapy; and To determine the sensitivity of AD diagnoses in the
Revenue Center Codes 0331 (radiology therapeutic-chem- SEER-Medicare file, 3-year prevalence of the examined
otherapy injected), 0332 (radiology therapeutic-chemother- ICD-9 diagnoses in breast cancer cases and noncancer con-
apy oral), and 0335 (radiology therapeutic-chemotherapy trols (SEER-Medicare 5% file) was compared with reported
IV).22–24 Diagnostic and procedural codes were taken from prevalence of AD in the U.S. population7 (Table 1). Non-
the ICD-9-CM and the American Medical Association’s breast cancer controls in the SEER-Medicare database aged
Physicians’ Current Procedural Terminology.22,25 By com- 65 to 89 had slightly higher prevalence of AD than pop-
parison with medical chart audits, chemotherapy claims in ulation-based controls or breast cancer cases; sensitivity
the SEER-Medicare linked database have 88% sensitivity was lower in those aged 90 and older.
and high internal validity, with 98% agreement (kap- Characteristics of patients with and without AD varied
pa 5 0.82).16 Because prognosis and chemotherapy treat- by stage, age, race, and other factors (Table 2). Subjects
ment choices for breast cancer are determined using nodal with AD were older than those without AD (12.9% 90 vs
status, tumor size, and estrogen receptor status,26 these 2.7%, Po.001). Women diagnosed with AD were more
factors were included in all analyses. Results were also likely to be African American (9.8% vs 5.4%, Po.001).
provided stratified by age, because it influences treatment Perhaps reflecting their older ages, women with AD were
choices.11 The guidelines developed by the National more frequently widowed (57.8%, Po.001) than women
Institutes of Health consensus conference and by the Na- without AD (40.1%). Women who were diagnosed with
tional Comprehensive Cancer Network27,28 for the treat- AD evidenced more comorbidities than those without AD
ment of breast cancer, including the dosing for cycles of (Deyo-Charlson index 3, 7.1% vs 2.4%, Po.001). There
chemotherapy, informed understanding of the selected were statistically significant differences by coded depres-
treatment regimens. sion (Po.001), with women diagnosed with AD more fre-
quently depressed than breast cancer controls. There were
no differences between women according to rural or urban
Analytic Methods
residence. At the community level, a larger proportion of
The use and types of therapy for localized and regional- individuals with AD lived in census tract areas with greater
stage breast cancer were the primary outcome measures for than 20% of the age- and race-specific population in pov-
the study. Chi-square analyses were used to compare pop- erty (11.1%) than in other census tracts (7.0%, Po.001).
ulation characteristics between patients with and without
AD and to report differences in treatment use. Two-sided
tests of significance were used. Multivariate logistic regres-
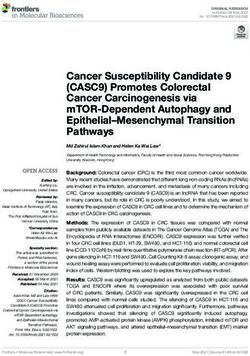
sion models were applied to the data to examine the effects Table 1. Prevalence of Alzheimer’s Disease (AD) Com-
of covariates. All statistical analyses were performed using pared with 3-Year Prevalence in the Surveillance, Epidemi-
SAS, version 9 (SAS Institute Inc., Cary, NC). ology, and End Results (SEER)-Medicare Database
SEER-Medicare 3-Year
RESULTS Prevalence
Differences Between Breast Cancer Patients with and Prevalence Breast Cancer
without AD of AD Controls Cases
Of the 137,391 female breast cancer cases abstracted from
SEER public-use databases, 33,589 (24.4%) were excluded, Age %
because their first cancer diagnosis occurred before age 65,
27,849 (20.2%) because they were members of Medicare 65–69 1.1 1.2 0.7
HMOs, 8,627 (6.2%) because they were not enrolled in 70–74 2.2 3.4 1.7
Medicare parts A and B, 8,573 (6.2%) because diagnosis 75–79 4.6 7.3 3.9
occurred before 1992, 3,200 (2.3%) because they were di- 80–84 9.2 12.4 7.4
agnosed at an unknown stage of cancer, 2,125 (1.5%) be- 85–89 17.8 18.7 12.1
cause they had brain metastases, 1,951 (1.4%) because they 90–94 31.5 22.4 15.2
95 52.5 20.5 19.4
were diagnosed at Stage IV, 985 (0.7%) because breast
cancer was not their first SEER diagnosis, and 32 (o0.1%)
Source: Alzheimer’s Disease: Estimates of Prevalence in the United States.
because their Medicare eligibility was based on disability or Washington, DC: General Accounting Office, 1998. Estimates are based on
end-stage renal disease. meta-analysis of 18 studies.1900 GORIN ET AL. NOVEMBER 2005–VOL. 53, NO. 11 JAGS
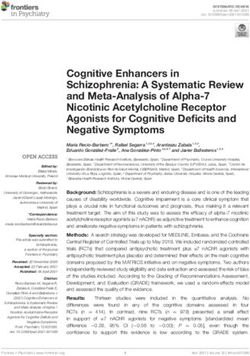
Table 2. Characteristics of Breast Cancer Patients with and Table 2. (Contd.)
without International Classification of Diseases, Revision
Nine, Diagnoses of Alzheimer’s Disease (AD) Subjects
with AD Controls
Subjects (n 5 1,935) (n 5 48,525)
with AD Controls
(n 5 1,935) (n 5 48,525) Characteristic %
Characteristic % Progesterone receptor status (n 5 36,224)
Negative 68.4 68.6
Individual-level Positive 30.4 30.1
Age at cancer diagnosisw Borderline/undetermined 1.2 1.3
65–69 4.0 25.8 Tumor size, cmw
70–74 11.1 27.9 o1 11.2 23.5
75–79 21.7 22.7 1–3 62.2 63.4
80–84 27.5 14.2 43 26.6 13.1
85–89 22.8 6.7 Nodal involvement
90 12.9 2.7 None 70.9 74.1
Racew Lymph node involvement 29.1 25.9
White 84.4 87.9
Black 9.8 5.4 Chi-square P-values: o.01, w o.001.
Hispanic 2.6 2.6 Using the Deyo-Charlson comorbidity index.21
z
Asian/Pacific Islander 2.4 3.3
Other/Unknown 0.7 0.8
Marital statusw Women with AD were more likely to be diagnosed with
Married 22.9 44.8 Stage III cancer than other female Medicare beneficiaries
Single 11.2 7.0 (10.8% vs 6.6% at Stage III, Po.001). Similarly, women
Divorced/separated 4.2 5.8 with AD had a higher probability of diagnosis with tumors
Widowed 57.8 40.1 larger than 3 cm (26.6% vs 13.1%, Po.001) and had a
Unknown 3.8 2.3 higher proportion reporting lymph node involvement
Depression diagnosisw 27.9 4.4 (29.1% vs 25.9%, Po.01). There were no statistically sig-
Presence of comorbiditieswz nificant differences by tumor grade, estrogen receptor or
0 66.6 85.9 progesterone receptor status.
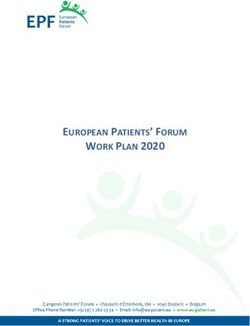
1 16.6 8.0 Overall, patients diagnosed with ICD-9 codes indicat-
2 9.7 3.7 ing AD had less treatment for breast cancer than those
3 7.1 2.4 without AD diagnoses, except for breast-conserving surgery
Rural/urban residence (population) (Table 3). There was no record of any treatment for 3.7% of
Largest metro areas (41 million) 61.6 60.9 patients with AD and 0.9% of patients without AD (odds
Metro area (250,000–1 million) 22.5 22.1 ratio (OR) 5 0.26, 95% confidence interval (CI) 5 0.21–
Urban area (20,000–249,999) 7.1 6.9 0.33). Compared with the 99.0% of patients without AD
Less urban (2,500–19,999) 7.1 8.4 who received surgery, 96.4% of those with AD received any
Rural (o2,500 per county) 1.8 1.7 surgery (OR 5 0.30, 95% CI 5 0.24–0.38). Only 11.7% of
Neighborhood-level factor Census tract poverty, race- and patients with AD received radiation therapy, compared
age-specific, %w with 36.8% of the comparison group (OR 5 0.24, 95%
o5 38.3 49.2 CI 5 0.21–0.27). Use of radiation therapy decreased with
5–9 29.0 25.7 age (Cochran-Armitage test for trend 5 7.9, Po.001) and
10–14 15.0 12.4 was lower in patients with AD across all age groups
15–19 6.6 5.8 (Po.001). Chemotherapy was used in 3.3% of patients
20 11.1 7.0 who were diagnosed with AD, compared with 10.5% of the
Tumor characteristics comparison group (OR 5 0.30, 95% CI 5 0.23–0.38). As
Cancer stagew they aged, women diagnosed with AD continued to receive
In situ 6.3 12.1 less chemotherapy than other female Medicare beneficiar-
1 35.5 47.6 ies, although the sample size was too small for analyses of
2 47.4 33.7 the oldest old (Cochran-Armitage test for trend 5 4.1,
3 10.8 6.6 Po.001). Women who were diagnosed with AD were less
Tumor grade (n 5 38,206) likely to receive a mastectomy than were controls (62.3% vs
Well-differentiated 17.6 19.8 71.0%), although they were more likely to receive breast-
Moderately differentiated 45.9 44.6 conserving surgery (37.7% vs 29.0%; OR 5 0.68, 95%
Poorly differentiated 33.9 32.4 CI 5 0.60–0.76).
Undifferentiated 2.7 3.2 The mean number of days between the first notation of
Estrogen receptor status (n 5 36,772)
AD in the medical chart and a diagnosis of cancer was 3.1
Negative 17.6 18.0
years. Length of time since diagnosis with AD was related to
Positive 82.4 82.0
likelihood of any treatment (Po.001), surgery (Po.001),JAGS NOVEMBER 2005–VOL. 53, NO. 11 ALZHEIMER’S DISEASE AND BREAST CANCER TREATMENT 1901
Table 3. Univariate Analysis of Cancer Treatment in Subjects with Alzheimer’s Disease (AD)
Subjects with AD Controls
Treatment n (%) Odds Ratio (95% Confidence Interval) P-value
Any treatment 1,863 (96.3) 48,087 (99.1) 0.26 (0.21–0.33) o.001
Surgery 1,851 (96.4) 47,917 (99.0) 0.30 (0.24–0.38) o.001
Type (if known)
Breast-conserving surgery 447 (37.7) 7,687 (29.0)
Mastectomy 738 (62.3) 18,803 (71.0) 0.68 (0.60–0.76) o.001
Radiation 224 (11.7) 17,684 (36.8) 0.24 (0.21–0.27) o.001
Chemotherapy 64 (3.3) 5,116 (10.5) 0.30 (0.23–0.38) o.001
Taken from Medicare billings. Only includes treatments within 6 months of cancer diagnosis. Oral medications are not available from this database.
and radiation (Po.001) but not chemotherapy (data not (OR 5 0.31, 95% CI 5 0.23–0.41) and chemotherapy
shown). (OR 5 0.44, 95% CI 5 0.34–0.58) were also significantly
lower in this population than in cancer patients not diag-
nosed with AD.
Multivariate Analyses After stratifying by age, the greatest differences in
Multivariate models were developed to examine the pre- treatment occurred between the ages of 80 and 89, with
dictors of treatment in patients with AD after controlling patients diagnosed with AD being half (OR 5 0.48) as likely
for the independent effects of race; stage; age; comorbidities to have surgery, one-quarter (OR 5 0.24) as likely to receive
other than dementia, including depression; and census-tract radiation treatment if they had breast-conserving surgery,
mean poverty level (Table 4). In multiple logistic regression and half (OR 5 0.56) as likely to receive of chemotherapy
analyses, patients with AD had significantly lower odds of as other female Medicare beneficiaries. The odds of women
any treatment (OR 5 0.55, 95% CI 5 0.42–0.74) than oth- diagnosed with AD receiving radiation treatment appeared
er female Medicare beneficiaries. The odds of having sur- to be relatively low across all ages (OR 5 0.24–0.66), as did
gery were 40% less than those of other patients (OR 5 0.60, the odds of receiving chemotherapy (OR 5 0.29–0.56).
95% CI 5 0.46–0.81). Odds of receiving radiation treat- After stratifying by several prognostic factors, AD pa-
ment for those who received breast-conserving surgery tients with positive estrogen receptor status were much less
Table 4. Adjusted Odds of Receiving Therapy for Breast Cancer in Patients with Alzheimer’s Disease (AD), Stratified by
Age and Tumor Characteristics
Any Treatment Surgery Radiation Chemotherapy
Characteristic Odds Ratio (95% Confidence Interval)
All subjects 0.55 (0.42–0.74) 0.60 (0.46–0.81) 0.31 (0.23–0.41) 0.44 (0.34–0.58)
Stratified by age at cancer diagnosisw
65–69 F§ F§ 0.66 (0.22-2.05) 0.29 (0.12–0.69)
70–79 0.56 (0.28–1.13) 0.82 (0.40–1.69) 0.31 (0.20–0.47) 0.36 (0.24–0.52)
80–89 0.48 (0.33–0.69) 0.50 (0.39–0.73) 0.24 (0.15–0.38) 0.56 (0.37–0.86)
90 0.67 (0.39–1.17) 0.62 (0.34–1.12) F§ F§
Stratified by estrogen receptor statusz
Negative F§ F§ 0.20 (0.08–0.51) 0.61 (0.38–0.97)
Positive 0.51 (0.28–0.93) 0.60 (0.34–1.05) 0.32 (0.22–0.45) 0.52 (0.36–0.77)
Stratified by nodal involvementz
None 0.57 (0.34–0.88) 0.55 (0.34–0.88) 0.42 (0.29–0.60) 0.68 (0.44–1.07)
Lymph node involvement 0.60 (0.32–1.13) 0.61 (0.35–1.10) F§ 0.39 (0.27–0.57)
Stratified by tumor size, cmz
o1 0.92 (0.11–7.48) 1.13 (0.14–9.03) 0.55 (0.31–0.99) 0.37 (0.09–1.53)
1–3 0.47 (0.28–0.78) 0.42 (0.26–0.70) 0.28 (0.20–0.41) 0.52 (0.37–0.75)
43 0.76 (0.47–1.23) 1.09 (0.64–1.86) 0.19 (0.06–0.56) 0.34 (0.21–0.56)
Includes only patients who had breast-conserving surgery.
w
Controlling for race, stage, comorbidities other than dementia, depression, and census-tract mean percentage in poverty.
z
Controlling for race, age, comorbidities other than dementia, depression, and census-tract mean percentage in poverty.
§
Numbers were too small to draw conclusions.1902 GORIN ET AL. NOVEMBER 2005–VOL. 53, NO. 11 JAGS
likely to have surgical (OR 5 0.60), radiation (OR 5 0.32), The relationship between the prevalence of AD and
or chemotherapeutic (OR 5 0.52) treatment than were SES, measured here using census-tract mean percentage of
comparable women in the study. Patients who were diag- persons in poverty, has been previously reported in the lit-
nosed with AD without metastases to axillary nodes had erature.37 Differences in levels of education and structural
significantly lower odds of receiving radiation (OR 5 0.42) effects of poverty on access to diagnostic or treatment re-
or surgery (OR 5 0.55) but not chemotherapy than the sources could explain an inverse relationship between SES
comparison group. In patients with the smallest tumors and AD.38
(o1 cm), patients with AD were approximately half (0.55) As would be expected, hormone receptor status did not
as likely as other female Medicare beneficiaries to receive influence the likelihood of surgery in patients with AD.
radiation. For AD patients with tumors 1 cm to 3 cm, there Breast cancer is largely a surgical disease, generally of min-
was less likelihood of all types of treatment. Patients with imal risk, regardless of estrogen receptor status. Although
the largest tumors (43 cm) who had a diagnosis of AD had hormone receptor negative status is considered a poor
a significantly lower likelihood of receiving radiation prognostic and predictive factor, and generally no hormonal
(OR 5 0.19) or chemotherapy with breast-conserving sur- therapy is offered to these patients, it had an influence on
gery (OR 5 0.34) than women not diagnosed with AD. the administration of chemotherapy and radiation. It is also
possible that these patients had a longer life expectancy on
the basis of limited comorbidities or were less severely im-
DISCUSSION paired by AD.
Among Medicare beneficiaries, women with AD were more The findings revealed lower prevalence of AD as indi-
likely to be diagnosed at later stages of breast cancer than viduals aged. These counterintuitive findings are consonant
women without AD. This may reflect poorer symptom rec- with those from a recent multistage screening study in a
ognition, delays in diagnostic testing, or lower use of cancer population with extended longevity in Cache County, Utah.
screening, but even after adjusting for comorbidity, AD was They also found a decline in the incidence of AD in women
still an independent predictor of treatment; women with aged 90 and older, perhaps due to insufficient sampling of
AD were approximately half as likely to receive treatment the oldest old in earlier studies or differential risk factors.39
for their breast cancer as comparable others. Bivariate find- The study’s findings may be limited because of biases
ings revealed that women diagnosed with AD were more inherent in the administrative nature of the SEER-Medicare
likely to receive breast-conserving surgery than other com- database. In particular, the study measured the rate of AD in
parable Medicare beneficiaries, although they were less claims and not the true prevalence of AD. Furthermore, the
likely to receive adjuvant chemotherapy. These treatment severity of AD cannot be assessed with this database, al-
differences persisted across all ages. Treatment for breast though the undercount of AD in persons with mild disease is
cancer was less comprehensive in women with AD whose likely to be greater than that in those with more-severe dis-
tumors had either poor or more favorable prognostic fea- ease. In this study, it was not known whether cognitive sta-
tures. tus was assessed in a standardized way, and AD may not be
The findings of reduced treatment are similar to those properly coded because of a lack of recognition, particu-
found in other groups, such as older patients, minorities, larly of mild cognitive impairment, by physicians, patients,
and persons with other chronic conditions.11,29,30 This and their families, leading to undercoding. Physicians may
propensity for people with AD to receive less-aggressive diagnose but not code AD, because they cannot provide the
treatment is consistent with findings from research on end- time-intensive counseling or because of other competing
of-life decision-making,31 on the effect of dementia on hos- diagnoses for reimbursement purposes, economic disincen-
pital-based treatment for acute myocardial infarction and tives, or family preference (see 40 for review).
all-cause mortality,32 on general patterns of care using a 5% Studies examining dementia diagnoses in medical
random sample of Medicare beneficiaries in Tennessee,29 claims have found that they have strong specificity but
and a recent study of patients presenting with colon cancer poor sensitivity. A recent study validated dementia diag-
and comorbid dementia using the linked SEER-Medicare noses that were not specific to AD; diagnoses had 19.7%
database,15 although to the authors’ knowledge, there have sensitivity and 99.4% specificity,41 although an analysis
been few other studies that examined use of preventive that specifically examined AD using a larger range of AD-
medicine or treatment for other conditions in patients with related ICD-9 diagnostic codes found that 87% of patients
dementia. One study found that women with AD or other with AD were so identified in Medicare claims. There is an
mental disorders had half the rates of mammography of improvement in sensitivity when using 3 or more years of
healthy women aged 75 and older.33 Another study10 found claims, as applied in this study.8,42 When the ICD-9-CM
a 5% decrease in mammography use in this subgroup, al- codes were limited to AD (331.0) only, few differences were
though the findings may be due to age differences. found between the women. Of 832 women with the 331.0
African Americans were disproportionately represent- diagnosis only, 96.5% had any treatment for breast cancer;
ed among patients with a diagnosis of AD. The clinical 96.2% of those had surgery, 10.3% had radiation, and
etiologies of dementia are thought to differ between African 2.9% had chemotherapy (including combined treatments).
Americans and Caucasian Americans,34 although there may The differences in the prevalence of AD in this database
be a higher prevalence of AD in African Americans, a find- relative to other population-based estimates, and their
ing that has been reported in population-based35 and com- validity, are likely related to the severity of disease and
munity studies.36,37 The racial difference in incidence may degree of patient interaction with the healthcare system.
be due to underlying risk factors such as variations in apo- From a methodological perspective, any misclassification
lipoprotein E status.37 of AD that is unrelated to the study exposure (i.e., breastJAGS NOVEMBER 2005–VOL. 53, NO. 11 ALZHEIMER’S DISEASE AND BREAST CANCER TREATMENT 1903
cancer treatment) will produce bias toward the null, sug- search Program, National Cancer Institute; the Office of
gesting that the study’s findings are robust. Research, Development and Information, Centers for
Because oral medications are not captured reliably in Medicare and Medicaid Services; Information Manage-
these databases, the administration of hormonal therapies ment Services, Inc.; and the SEER program tumor registries
(Noveldex/Arimidex) that are often administered as first- in the creation of the SEER-Medicare database.
line therapies in older people was not measured, although Financial Disclosure: Dr. Sheinfeld Gorin has grant
hormone receptor status was statistically controlled. In eld- support from the National Institutes of Health, the Depart-
erly women, especially those with early-stage disease, who ment of Defense, the Centers for Disease Control and Pre-
are dominant in this study, the decision to receive chemo- vention (CDC), the American Lung Association, and the
therapy depends on a number of factors, such as life ex- Susan G. Komen Breast Cancer Foundation. She has no
pectancy and comorbidities. Chemotherapy is usually given conflicts of interest to report. Ms. Heck receives financial
to prolong disease-free survival and overall survival. Be- support from the Department of Epidemiology, Mailman
cause a recent article43 reported that 86% of elderly initiate School of Public Health, Columbia University, and the
treatment with tamoxifen if they are hormone-receptor CDC. She has no conflicts of interest to report. Dr. Albert
positive, it is likely that most of the eligible women received has financial support from the National Institute of Mental
this type of therapy. Health and the National Institute for Aging. He has no
Although stage is a strong and consistent predictor of conflicts of interest to report. Dr. Hershman has financial
breast cancer prognosis,44 expected length of life for pa- support for clinical research from Novartis Pharmaceuti-
tients with AD can be highly variable, depending on age at cals. She has no conflicts of interest to report.
diagnosis with AD, sex, and symptomatology.45 Using these Author Contributions: Dr. Sheinfeld Gorin designed
databases, it is not possible to measure the influence of the study, acquired the data, oversaw data analyses and
physicians’ own estimations of patients’ life expectancies or interpretation, and prepared the final manuscript. Ms. Heck
the severity of dementia; these factors may have influenced conducted the data analysis and prepared the initial drafts.
treatment choices. Dr. Albert helped to design the study, consulted on analytic
This study’s findings reflect lower rates of treatment for strategies, and reviewed the manuscript for intellectual
patients with AD and other diseases as they age. Although content. Dr. Hershman participated in data interpretation
patient functional status was not measured, differences and reviewed the manuscript for clinical content.
were accounted for by case mix. Mortality was not meas- Sponsor’s Role: The CDC played no role in the design,
ured in this study. For some women in the sample, only 3 methods, subject recruitment, data collection, analysis, or
years of claims would be available to 2002 (the most recent preparation of the manuscript.
data), thus limiting the generalizability of the findings. Pa-
tients with AD, particularly those with advanced disease,
may be expected to deteriorate in function over time; as that
occurs, it should precipitate renewed discussion of the ap- REFERENCES
propriate medical care regimen. 1. Ries L, Eisner M, Kosary C et al. SEER Cancer Statistics Review, 1975–2000.
Bethesda, MD: National Cancer Institute, 2003.
There are insufficient data to make chemotherapy rec- 2. Yancik R. Cancer burden in the aged. An epidemiologic and demographic
ommendations for patients aged 70 and older, so treatment overview. Cancer 1997;80:1273–1283.
may be individualized depending on the comorbidities. 3. Stafford RS, Cyr PL. The impact of cancer on the physical function of the
Even in the face of accepted clinical guidelines, healthcare elderly and their utilization of health care. Cancer 1997;80:1973–1980.
4. Engel J, Kerr J, Schlesinger-Raab A et al. Predictors of quality of life of breast
providers may appropriately offer less-aggressive care to cancer patients. Acta Oncol 2003;42:710–718.
their patients with AD. Factors that influence these deci- 5. Cummings JL, Cole G. Alzheimer disease. JAMA 2002;287:2335–2338.
sions may include life expectancy, quality of life, and the 6. Doraiswamy PM, Leon J, Cummings JL et al. Prevalence and impact of med-
risks of treatment or treatment-related toxicities, although ical comorbidity in Alzheimer’s disease. J Gerontol A Biol Sci Med Sci
2002;57A:M173–M177.
the general pattern of less-aggressive breast cancer treat- 7. Alzheimer’s Disease. Estimates of Prevalence in the United States. Washington,
ment for people with AD suggests that opportunities for DC: U.S. General Accounting Office, 1998.
reducing excess non-AD related morbidities may be under- 8. Taylor DH Jr, Fillenbaum GG, Ezell ME. The accuracy of medicare claims data
used in this population. It is uncertain what is the right mix in identifying Alzheimer’s disease. J Clin Epidemiol 2002;55:929–937.
9. Fisher-Morris M, Gellatly A. The experience and expression of pain in Al-
of curative and palliative breast cancer treatment for the zheimer patients. Age Ageing 1997;26:497–500.
person with AD.46,47 Further research on the effect of breast 10. Heflin MT, Oddone EZ, Pieper CF et al. The effect of comorbid illness
cancer screening and treatment decision-making for these on receipt of cancer screening by older people. J Am Geriatr Soc 2002;50:
patients is warranted. 1651–1658.
11. Hurria A, Leung D, Trainor K et al. Factors influencing treatment patterns of
breast cancer patients age 75 and older. Crit Rev Oncol Hematol 2003;46:
121–126.
ACKNOWLEDGMENTS 12. Bland KI, Menck HR, Scott-Conner CE et al. The National Cancer Data Base
We are grateful for the assistance of Dr. Alfred I. Neugut in 10-year survey of breast carcinoma treatment at hospitals in the United States.
Cancer 1998;83:1262–1273.
securing the early data and Dr. Joan Warren for her helpful 13. Monfardini S, Ferrucci L, Fratino L et al. Validation of a multidimensional
suggestions on the study model. We greatly appreciate the evaluation scale for use in elderly cancer patients. Cancer 1996;77:395–401.
comments of two anonymous reviewers who contributed 14. Potosky AL, Riley GF, Lubitz JD et al. Potential for cancer related health
considerably to the refinement of the paper. This study used services research using a linked Medicare-tumor registry database. Med Care
1993;31:732–748.
the linked SEER-Medicare database. The interpretation and 15. Gupta SK, Lamont EB. Patterns of presentation, diagnosis, and treatment in
reporting of these data are the sole responsibility of the older patients with colon cancer and comorbid dementia. J Am Geriatr Soc
authors. We acknowledge the efforts of the Applied Re- 2004;52:1681–1687.1904 GORIN ET AL. NOVEMBER 2005–VOL. 53, NO. 11 JAGS
16. Warren JL, Harlan LC, Fahey A et al. Utility of the SEER-Medicare data to 32. Sloan FA, Trogdon JG, Curtis LH et al. The effect of dementia on outcomes
identify chemotherapy use. Med Care 2002;40:55–61. and process of care for Medicare beneficiaries admitted with acute myocardial
17. Warren JL, Klabunde CN, Schrag D et al. Overview of the SEER-Medicare infarction. J Am Geriatr Soc 2004;52:173–181.
data: Content, research applications, and generalizability to the United States 33. Blustein J, Weiss LJ. The use of mammography by women aged 75 and older:
elderly population. Med Care 2002;40:3–18. Factors related to health, functioning, and age. J Am Geriatr Soc 1998;46:941–
18. Krieger N, Chen JT, Waterman PD et al. Race/ethnicity, gender, and moni- 946.
toring socioeconomic gradients in health: A comparison of area-based soci- 34. Froehlich TE, Bogardus ST Jr, Inouye SK. Dementia and race: Are there dif-
oeconomic measuresFthe public health disparities geocoding project. Am J ferences between African Americans and Caucasians? J Am Geriatr Soc
Public Health 2003;93:1655–1671. 2001;49:477–484.
19. Phillips KA, Bernhard J. Adjuvant breast cancer treatment and cognitive func- 35. Husaini BA, Sherkat DE, Moonis M et al. Racial differences in the diagnosis of
tion: Current knowledge and research directions. J Natl Cancer Inst 2003;95: dementia and in its effects on the use and costs of health care services. Psychiatr
190–197. Serv 2003;54:92–96.
20. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index 36. Tang MX, Cross P, Andrews H et al. Incidence of AD in African-Americans,
for use with ICD-9-CM administrative databases. J Clin Epidemiol 1992; Caribbean Hispanics, and Caucasians in northern Manhattan. Neurology
45:613–619. 2001;56:49–56.
21. Elixhauser A, Steiner C, Harris DR et al. Comorbidity measures for use with 37. Evans DA, Bennett DA, Wilson RS et al. Incidence of Alzheimer disease in a
administrative data. Med Care 1998;36:8–27. biracial urban community: Relation to apolipoprotein E allele status. Arch
22. International Classification of Diseases, 9th Revision, Clinical Modification, Neurol 2003;60:185–189.
5th Ed. Geneva, Switzerland: World Health Organization, 1996. 38. Karp A, Kareholt I, Qiu C et al. Relation of education and occupation-based
23. HCFA Data Dictionary: Revenue Center Codes. Baltimore, MD: Health Care socioeconomic status to incident Alzheimer’s disease. Am J Epidemiol
Financing Administration, 1999. 2004;159:175–183.
24. Health Care Financing Administration. HCFA Common Procedure Coding 39. Miech RA, Breitner JC, Zandi PP et al. Incidence of AD may decline in the
System (HCPCS): National Level II Medicare Codes. Los Angeles, CA: Prac- early 90 s for men, later for women: The Cache County Study. Neurology
tice Management Information Corporation, 2000. 2002;58:209–218.
25. Physicians’ Current Procedural Terminology-CPT 94. Chicago, IL: American 40. Fillit H, Geldmacher DS, Welter RT et al. Optimizing coding and reimburse-
Medical Association, 1993. ment to improve management of Alzheimer’s disease and related dementias. J
26. Harlan LC, Abrams J, Warren JL et al. Adjuvant therapy for breast Am Geriatr Soc 2002;50:1871–1878.
cancer. Practice patterns of community physicians. J Clin Oncol 2002; 41. Wilchesky M, Tamblyn RM, Huang A. Validation of diagnostic codes within
20:1809–1817. medical services claims. J Clin Epidemiol 2004;57:131–141.
27. Goldhirsch A, Glick JH, Gelber RD et al. Meeting highlights. International 42. Taylor DH Jr, Sloan FA, Doraiswamy PM. Marked increase in Alzheimer’s
Consensus Panel on the Treatment of Primary Breast Cancer. J Natl Cancer disease identified in medicare claims records between 1991 and 1999. J Ger-
Inst 1998;90:1601–1608. ontol A Biol Sci Med Sci 2004;59A:M762–M766.
28. Eifel P, Axelson JA, Costa J et al. National Institutes of Health Consensus 43. Fink AK, Gurwitz J, Rakowski W et al. Patient beliefs and tamoxifen discon-
Development Conference Statement: Adjuvant therapy for breast cancer, No- tinuance in older women with estrogen receptor–positive breast cancer. J Clin
vember 1–3, 2000. J Natl Cancer Inst 2001;93:979–989. Oncol 2004;22:3309–3315.
29. McWhorter WP, Mayer WJ. Black/white differences in type of initial breast 44. Carter CL, Allen C, Henson DE. Relation of tumor size, lymph node status,
cancer treatment and implications for survival. Am J Public Health 1987;77: and survival in 24,740 breast cancer cases. Cancer 1989;63:181–187.
1515–1517. 45. Stern Y, Tang MX, Albert MS et al. Predicting time to nursing home care and
30. Kiefe CI, Funkhouser E, Fouad MN et al. Chronic disease as a barrier to breast death in individuals with Alzheimer disease. JAMA 1997;277:806–812.
and cervical cancer screening. J Gen Intern Med 1998;13:357–365. 46. Cassel CK. Breast cancer screening in older women: Ethical issues. J Gerontol
31. van der Steen JT, Kruse RL, Ooms ME et al. Treatment of nursing home 1992;47:126–130.
residents with dementia and lower respiratory tract infection in the United 47. Raik BL, Miller FG, Fins JJ. Screening and cognitive impairment: Ethics
States and the Netherlands: An ocean apart. J Am Geriatr Soc 2004;52: of forgoing mammography in older women. J Am Geriatr Soc 2004;52:
691–699. 440–444.You can also read