First Aid and Pre-Hospital Management of Venomous Snakebites - MDPI
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Tropical Medicine and
Infectious Disease
Review
First Aid and Pre-Hospital Management of
Venomous Snakebites
Jennifer Parker-Cote and William J. Meggs *
Division of Toxicology, Department of Emergency Medicine, Brody School of Medicine at East Carolina
University, Greenville, NC 27858, USA; parkercotej16@ecu.edu
* Correspondence: meggsw@ecu.edu; Tel.: +1-252-744-2954
Received: 21 February 2018; Accepted: 16 April 2018; Published: 24 April 2018
Abstract: Background: Antivenom is the definitive treatment for venomous snakebites, but is
expensive and not available in many rural and poorly developed regions. Timely transportation
to facilities that stock and administer antivenom may not be available in rural areas with poorly
developed emergency medical services. These factors have led to consideration of measures to
delay onset of toxicity or alternatives to antivenom therapy. Methods: PubMed searches were
conducted for articles on snakebite treatment, or that contained first aid, emergency medical services,
tourniquets, pressure immobilization bandages, suction devices, and lymphatic flow inhibitors.
Results: The reviewed articles describe how venoms spread after a venomous snakebite on an
extremity, list the proposed first aid measures for delaying the spread of venoms, and evaluate the
scientific studies that support or refute methods of snakebite first aid. The recommendations for
field treatment of venomous snakebites will be discussed. Conclusions: The evidence suggests that
pressure immobilization bandages and related strategies are the best interventions to delay onset of
systemic toxicity from venomous snakebites but may increase local toxicity for venoms that destroy
tissue at the site of the bite, so their use should be individualized to the circumstances and nature of
the venom.
Keywords: snakebites; first aid; emergency medicine services; pressure immobilization bandages
1. Introduction
Intravenous antivenom is the definitive treatment for venomous snakebites but is expensive,
often in short supply, and not available in many rural and poorly developed regions [1,2].
Timely transportation to facilities that stock and administer antivenom may not be available in
areas with poorly developed emergency medical services. These factors have led to consideration of
measures to delay onset of toxicity or alternatives to antivenom therapy.
This review will describe how venoms spread after a venomous snakebite on an extremity, list the
proposed first aid measures for delaying spread of venoms, and evaluate the scientific studies that
support or refute methods of snakebite first aid. The recommendations for field treatment of poisonous
snakebites will be discussed.
2. Methods
PubMed searches were conducted for articles on snakebite treatment, or that contained first aid,
emergency medical services, tourniquets, pressure immobilization bandages, suction devices, and
lymphatic flow inhibitors. The search encompassed articles from 1945 to 2017. This review emphasizes
articles that initially proposed a technique and recent experimental studies that support or refute
the technique.
Trop. Med. Infect. Dis. 2018, 3, 45; doi:10.3390/tropicalmed3020045 www.mdpi.com/journal/tropicalmed
Trop. Med. Infect. Dis. 2018, 3, 45 2 of 12
2.1. Systemic Spread of Venom
A venomous snake can inject venom into subcutaneous tissues, muscle, a vein, or an artery.
Intravascular injections result in rapid onset of systemic toxicity [3,4] and can be difficult to treat,
even when antivenom is readily available. No first aid measure, other than supportive care and
advanced life support, will be of benefit in intravascular venom injections.
In a classic study published in 1941, Barnes and Trueta [5] proved that lymphatic flow from
an extremity is the main route via which venoms spread from a subcutaneous extremity injection,
but demonstrated that systemic arrival of venom is delayed by lymphatic ligation. Rabbits were
injected in a hind leg with a fatal dose of tiger snake (Notechis scutatus) venom—a potent neurotoxin.
The treatment group had the groin lymphatic channels ligated. The endpoint was time to death from
respiratory paralysis. Rabbits in the control group expired after an average time of ten minutes, while
those with lymphatic channel ligation survived an hour. This historic study established that flow
through the lymphatic channels was the major route for venoms to reach the systemic circulation.
Further, the study suggested that methods to block lymphatic flow can be effective for delaying onset
of toxicity.
There are four known mechanisms to propel lymph from an extremity to the systemic circulation.
(a) Large lymphatic vessels have smooth muscles in their walls that contract, which is the primary
mode of lymph propulsion in an extremity at rest, suggesting pharmacologic blockade of the intrinsic
lymph pump can retard venom transport. (b) Contraction of skeletal muscles can also propel lymph
to the central circulation, which suggests that immobilization of an extremity can retard lymph flow.
(c) Lymph channels, like veins, have one-way valves that prevent backflow of lymph. (d) Another set
of valves, the contractile valves of lymph endothelial cells, also prevent backward flow of lymph [6].
2.2. Tourniquets
Tourniquets are constricting bands that block arterial, venous, and lymphatic flow. Tourniquets
are often used as first aid after snake envenomation, especially in rural areas where transport times to
a healthcare facility are increased. There are significant complications from their use, which can result
in worsening morbidity and mortality.
A prospective study in the Philippines of 36 hospitalized patients who developed neurotoxic
symptoms after bites from Naja naja philippinensis reported 4 patients who developed complete
respiratory paralysis requiring mechanical ventilation after removal of a tourniquet [7]. From these
findings, the authors recommended slowly releasing already-applied tourniquets. Amaral et al.,
found no difference in plasma creatine kinase enzyme activity, partial thromboplastic time,
plasma whole venom, crotoxin concentrations, and frequency of acute renal and respiratory failure,
or deaths between those who applied a tourniquet and those who did not, after Crotalus durissus
envenomation [8].
A prospective study in Nigeria revealed that patients who received any form of first aid had a
longer length of stay compared to those who received no form of first aid, and that those who had used
a tourniquet had a larger antivenom requirement [9]. One case report of death after the application
of a tourniquet for 48 h occurred; the patient suffered from thrombophlebitis, local necrosis, and gas
gangrene, followed by pulmonary thromboembolism [10].
The lymphatic system transports venom from the envenomation site to systemic circulation.
Application of a tourniquet will sequester venom locally, potentially leading to increased local tissue
destruction when the venom is from those snakes that cause local tissue damage. Additionally,
tourniquets can impede venous blood flow and arterial blood flow, leading to limb ischemia, gangrene,
and potentially amputation.
Guidelines do not support the use of tourniquets. According to World Health Organization
recommendations, arterial tourniquets are contraindicated; their effectiveness relies on occlusion
of peripheral pulses causing pain, ischemia, nerve injury, and gangrenous limbs (level of evidence:
expert opinion/consensus) [1,2]. Deleterious effects from tourniquets are seen within 20 min to 2 h ofTrop. Med. Infect. Dis. 2018, 3, 45 3 of 12
application. The Wilderness Medical Society does not recommend tourniquets for envenomations by
pit vipers in North America [11].
2.3. Venom Extractors
Venom extractors are suction devices that are proposed to work by applying suction to the site of
a snakebite. These devices are marketed by companies that target outdoorsmen. The purported design
is supposed to apply negative pressure over fang marks to induce venom extraction. Venom extractors
can still be purchased through major retailors online and instores, despite several studies proving
their ineffectiveness [12,13]. A human study by Alberts et al., modeling western diamondback
envenomation, demonstrated only a mean 2.0% decrease in total body venom load and an average
0.04% decrease of mock venom at the site of envenomation after 15 min of extraction. A porcine model
with Crotalus atrox venom, by Bush et al., demonstrated concerns for injury by the extraction device
and no benefit in decreasing local tissue injury after 30 min of extraction [13]. Alberts et al. suggested
that the extractors could have collapsed the subcutaneous tissue, and pulled fluid from superficial
capillaries that contain minimal venom load [12]. Our opinion is that any significant change in clinical
outcomes is doubtful with such minute changes in venom load.
Proponents of extractors may counter with the difficulty in replicating a true envenomation with
simulated venom or in an animal model. Single puncture sites instead of two puncture sites were
used in the human study to decrease harm to patients, which is a less common presentation of snake
envenomation [12]. Other variables that are difficult to replicate in human studies are the specific
venom components, and the mechanism of action varies among species of snakes. Also, the volume of
venom typically increases with the size of the snake.
At the time of this review, there are two abstracts that support the suction device, but neither has
been peer reviewed and they include only limited descriptions of methodology. A rabbit study using
the Sawyer Extractor® to retrieve radiolabeled iodine-125 southern Pacific rattlesnake (Crotalus viridis
helleri) venom reportedly removed 23% of the venom within the first 3 min, and 34% after 30 min of
extraction [14]. The second abstract assessed the use of the Sawyer Extractor® pump in 3 individuals
envenomated by western diamondback rattlesnakes (Crotalus atrox) [15]. The volume of fluid extracted
from the victims’ wounds after the initial application of the extractor did not yield a significant
concentration to reduce toxicity. This small amount extracted is unlikely to be of clinical significance.
There are risks with use of these devices: local tissue destruction and a false sense of security.
Bush et al. noted necrosis of tissue with resultant tissue loss in two animals treated with extraction,
which was not seen in untreated animals [13]. Some have alleged that manufacturer claims provide
a ‘false sense of security,’ and may delay a patient from seeking definitive and effective care [16].
Instructional inserts on the Sawyer Products B4 Extractor Pump Kit® (Sawyer Products, Safety Harbor,
FL, USA) do provide a warning that ‘The pump is not a replacement for quickly seeking professional
medical treatment.’
Current guidelines from the Wilderness Medical Society and American Heart Association do
not support the use of mechanical suction for pit viper envenomations [7,17]. An initial search of
the medical literature did not yield results addressing the use of suction for other types of snake
envenomations, such as elapids. Despite the evidence against use of mechanical suction, there are
many unreliable sources available to the public. One study found that of 48 websites reviewed for
accuracy of information regarding pre-hospital care of snakebites, 26 (54.1%) contained inappropriate
recommendations [18]. Education for clinicians and the public regarding safe and effective pre-hospital
care is imperative in preventing further harm to snakebite victims.
2.4. Electric Shock
Electric shock has been advocated as a treatment for venomous snakebites, though there is no
scientific rationale for use of electric shock and no data to support its use, other than case reports. Its use
was advocated in a letter to the editor of Lancet in 1986, in which it was claimed that the experienceTrop. Med. Infect. Dis. 2018, 3, 45 4 of 12
in the jungles of Ecuador of applying a high-voltage, low-amperage electric current to the grounded
extremity prevented both local and systemic toxicity [19]. Electric shocks have been administered from
outboard motors and stun guns. It was ineffective in a controlled study of mice injected with northern
Pacific rattlesnake (Crotalus virldis oreganus) venom at varying doses [20]. The shocks neither reduced
toxicity in rats injected with sublethal doses of fer-de-lance (Bothrops atrox) venom nor lethality in
mice Trop. Med. Infect.
injected withDis. 2018, 3,
lethal x FOR [21].
doses PEER REVIEW 4 ofin11coma
In a case report, administration of electric shock resulted
and incontinence [22]. The United States Food and Drug Administration has banned the use of these
shocks neither reduced toxicity in rats injected with sublethal doses of fer-de-lance (Bothrops atrox)
devices, which were previously sold to the public for the treatment of snakebites and spider bites
venom nor lethality in mice injected with lethal doses [21]. In a case report, administration of electric
(United States of America vs. CONO).
shock resulted in coma and incontinence [22]. The United States Food and Drug Administration has
banned the use of these devices, which were previously sold to the public for the treatment of
2.5. Pressure Immobilization Bandages
snakebites and spider bites (United States of America vs. CONO).
The pressure immobilization bandage consists of an ace wrap and splint and is known as the
2.5. Pressure Immobilization
Commonwealth Bandages Method. A properly applied ace wrap is sufficient pressure to
Serum Laboratories
The pressure
block lymphatic flow immobilization
to an extremitybandage consists of an
while preserving ace wrap
arterial andand
venoussplintflow.
and is known
The splintasprevents
the
Commonwealth Serum Laboratories Method. A properly applied ace wrap
muscle contraction that squeezes lymph toward the central circulation. The result is to sequester is sufficient pressure to
block lymphatic flow to an extremity while preserving arterial and venous flow.
venom in the extremity, which is reasonably expected to delay systemic toxicity. For venoms that cause The splint prevents
local muscle
necrosis, contraction that squeezes
local damage at the bitelymph towardincrease
site could the central circulation.
while necrosis Thecouldresult is toaway
spread sequester
from the
venom in the extremity, which is reasonably expected to delay systemic toxicity. For venoms that cause
bite site.
local necrosis, local damage at the bite site could increase while necrosis could spread away from the bite
A study published in 1974 [23] injected monkeys with tiger snake (Notechis scutatus) venom
site.
and monitoredA studyplasma venom
published in 1974levels by radioimmunoassay.
[23] injected monkeys with tigerTreatment
snake (Notechiswasscutatus)
immobilization
venom andof the
extremity with a splint and the application of a firm crepe bandage
monitored plasma venom levels by radioimmunoassay. Treatment was immobilization to the length of theofextremity.
the
extremity with a splint and the application of a firm crepe bandage to the length of the extremity.
This intervention resulted in low levels of circulating venom relative to controls. Neither application
This intervention
of a splint alone nor of resulted in low levels
the pressure bandage of circulating venomsystemic
alone delayed relative todetection
controls. Neither application
of venom.
of controlled
A a splint alone nor of
study ofthe pressure
pressure bandage alone delayed
immobilization bandagessystemic
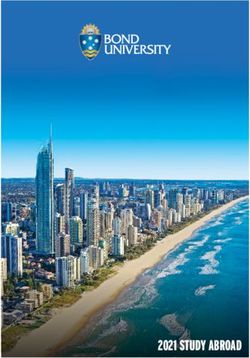
(Figuredetection of venom. pigs injected
1) in anesthetized
with eastern A controlled
coral snakestudy of pressure
(Micrurus immobilization
fulvius bandages
fulvius) venom had(Figure 1) in anesthetized
an endpoint of survival pigs
toinjected
eight hours
and used histological analysis of biopsies of the injection site [24]. Four of five subjects in thehours
with eastern coral snake (Micrurus fulvius fulvius) venom had an endpoint of survival to eight treatment
and used histological analysis of biopsies of the injection site [24]. Four of five subjects in the
group survived to 8 h, while no control group subjects survived. Mean time to onset of respiratory
treatment group survived to 8 h, while no control group subjects survived. Mean time to onset of
compromise was 170.4 ± 33.3 min in the control group (Figure 2). None of the pigs had histologic
respiratory compromise was 170.4 ± 33.3 min in the control group (Figure 2). None of the pigs had
changes at the changes
histologic envenomation site consistent
at the envenomation sitewith ischemia
consistent with or necrosis.
ischemia or necrosis.
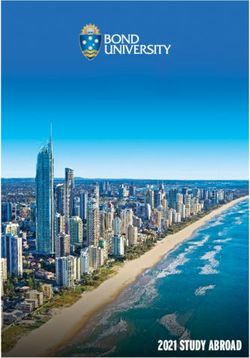
Figure 1. Pressure immobilization bandage consisting of an ace bandage wrapped beginning at the
Figure 1. Pressure immobilization bandage consisting of an ace bandage wrapped beginning at the
site of bite and wrapping the entire extremity, followed by a splint, in a porcine model of eastern coral
site ofsnake
bite envenomation.
and wrappingFrom
the entire extremity,
[24], used followedof
with permission bythe
a splint, in a porcine model of eastern coral
publisher.
snake envenomation. From [24], used with permission of the publisher.Trop.
Trop. Med.
Trop.
Med. Infect.
Med.
Infect. Dis.
Infect.
Dis. 2018,
Dis.
2018, x3,FOR
3,2018,x 3,
FOR45 PEER
PEER REVIEW
REVIEW 5 of
5 of 11 511of 12
Trop. Med. Infect. Dis. 2018, 3, x FOR PEER REVIEW 5 of 11
Figure
Figure 2. 2.
The
Figure The pressure
2.pressure
The pressureimmobilization
immobilization
immobilization bandage
bandage in in
bandage Figure
Figure
in 1 delayed
1 delayed
Figure onset
onset
1 delayed of of
onset ofrespiratory
respiratory depression
depression
respiratory depression in
Figure 2. The pressure immobilization bandage in Figure 1 delayed onset of respiratory depression
in in treated
treated pigs
pigs
treated ( (( ) relative
pigs )) relative
relative
tototo controls
controls
controls(( ( ))as) seen
as as
seenseen in
ininthethethe plot
plot
plot of of of respiratory
respiratory
respiratory rate
raterate versus
versus
versus time.[24],
time.time.
From
in treated pigs ( ) relative to controls ( ) as seen in the plot of respiratory rate versus time.
From
From [24],
[24],
used used
used
with with
with permission
permission
permission of the of of
thethe publisher.
publisher.
publisher.
From [24], used with permission of the publisher.
ThisThis result
result motivated
motivated a study
a study of of
thethe long-term
long-term efficacy
efficacy of of a pressure
a pressure immobilization
immobilization bandage
bandage forfor for
This result
This result motivated
motivated aastudy
study ofofthe thelong-term
long-term efficacy
efficacy ofofa pressure
a pressure immobilization
immobilization bandage
bandage
coral
coral snake
snake (Micrurus
(Micrurus fulvius
fulvius fulvius)
fulvius) [25][25] in inthe the porcine
porcine model.
model. The The hypothesis
hypothesis waswas that that
was by by by
coral
for coralsnake snake (Micrurus
(Micrurus fulvius
fulvius fulvius)
fulvius) [25][25]ininthe theporcine
porcine model. model. The The hypothesis
hypothesis was that
that by
sequestering
sequestering the the venom
venom in in
the the extremity
extremity with with pressure
pressure immobilization
immobilization for foran an extended
extended period,
period, the the
sequestering the
sequestering the venom
venomininthe theextremity
extremitywith with pressure
pressure immobilization
immobilization forfor an an extended
extended period, the
period,
venom
venom wouldbewould
would be degraded in intime time bylocal localprocesses
processes suchas ashydroxylation.
hydroxylation. A Arandomized,
randomized,
venom
the venom woulddegraded be be degraded
degraded in in bytime
time bybylocal local processessuch
processes such
such as hydroxylation.
as hydroxylation. A randomized,
A randomized,
controlled
controlled observational
observational pilot
pilot study
study was wasconducted
conductedwith withtentenpigs. pigs.Subjects
Subjects werewere anesthetized,
anesthetized,
controlled
controlled observational
observational pilot
pilot study
study was conducted
was conducted with with ten ten pigs.pigs. Subjects
Subjects were
were anesthetized,
anesthetized,
intubated,
intubated, andand injected
injected subcutaneously
subcutaneously with with 10 10mg mg of of lyophilized
lyophilized coral
coral snake
snake (Micrurus
(Micrurus fulvius)
fulvius)
intubated, and
intubated, and injected
injected subcutaneously
subcutaneously with with 10 10 mg mg of of lyophilized
lyophilized coral coral snake
snake (Micrurus
(Micrurus fulvius)
fulvius)
venom
venom suspended
suspended in in
1 1
mL mL of of water.
water. Treatment
Treatment waswas a a compression
compression bandage
bandage and and fiberglass
fiberglass castcast
venom suspended
venom suspendedinin1 mL 1 mL of water.
of water. TreatmentTreatment was awas a compression
compression bandage bandage
and fiberglass and fiberglass
cast cast
applied
applied
applied 1 minute
1 minute
1applied after
after envenomation.
envenomation. Pigs Pigs werewere monitored
monitored daily
daily for for
21 21
days days for for
signssigns of of respiratory
respiratory
minute 1 minute after envenomation. Pigs were monitored daily for 21 days for signs of respiratory
after envenomation. Pigs were monitored daily for 21 days for signs of respiratory depression,
depression,
depression, decreased
decreased oxygen
oxygen saturations,
saturations, and and paralysis.
paralysis. caseInof In
casecase of respiratory depression, pigs were
depression,
decreased decreased
oxygen oxygen
saturations, saturations,
and paralysis. andInparalysis. Inofcase
respiratory respiratory
of respiratory depression,
depression, depression,
pigs were pigs were
pigs were
humanely
humanely
humanely euthanized
euthanized and and time
time to to death
death recorded.
recorded. Median
Median survival
survival timetime of of control
control animals
animals was was 307 307
humanely euthanized
euthanized and time to and death time to death
recorded. recorded.
Median survivalMedian time survival
of controltime animalsof control
was 307 animals
min comparedwas 307
minmin compared
compared 1172with with 11721172 min min in treated animals (p = 0.10). Sixty ofpercent of ofthepigs in
thethe treatment group to
min compared
with min with
in 1172inanimals
treated treated
min animals
in treated
(p = 0.10). (pSixty
animals = 0.10). Sixty
(ppercent
= 0.10). percent
Sixty pigs percent
in pigs of inpigs
treatment treatment
in the treatment
group group
survived group
survived
survived to to
24 24
h h versus
versus 0% 0% of of control
control pigspigs (p (p
= = 0.08).
0.08). Two Two of of
the the treatment
treatment pigspigs survived
survived to to
the theend end 21
survived
24 h versus to 0%24 hofversuscontrol 0% of control
pigs (p = 0.08). pigsTwo (p =of 0.08). Two of thepigs
the treatment treatment
survived pigs to survived
the end point to theofend
point
point of of21but
21daysdaysbut buthad hadnecrotic
necrotic lesions
oflesions of ofthethe distal extremity, which could have beenfrom from
point
days of 21 days
had necrotic butlesions
had necrotic the lesions
distal ofdistal
extremity, extremity,
the distal
which couldwhich
extremity, have could
which
been have
could
from been
have
mechanical been from
trauma
mechanical
mechanical trauma
trauma fromfrom the the splint
splint rather
rather than than necrotic
necrotic effects
effects of of
the the venom.
venom.
mechanical
from the splint trauma rather fromthanthe splint rather
necrotic effects than of thenecrotic
venom.effects of the venom.
Pressure
Pressure immobilization
immobilization bandages
bandages forfor snakebites
snakebites with
with local
local necrosis areare suspected to to increase
Pressure
Pressure immobilization
immobilization bandages
bandages for snakebites
for snakebites with necrosis
with local necrosis
local necrosis suspected
are suspected
are suspected increase
to increase
to increase
local
local local damage
damage and and are are generally
generally notnot recommended.
recommended. Despite
Despite thisthis admonition,
admonition, experimental
experimental studies
studies
local damage and are generally not recommended. Despite this admonition, experimental studies
damage and are generally not recommended. Despite this admonition, experimental studies
have
have been
been performed. AA study was performed of of eastern diamondback (Crotalus adamanteus) toxicity
have performed.
have been performed.
been performed. study A was
A study
study performed
was performed
was performed eastern
of diamondback
of eastern
eastern diamondback
diamondback (Crotalus adamanteus)
(Crotalus
(Crotalus adamanteus)
adamanteus) toxicity toxicity
toxicity
in in monkeys
monkeys
in monkeys
in monkeys
injected
injected injected
injected subcutaneously
subcutaneously
subcutaneously
subcutaneously withwith 6with
with
6 mg
mg 66ofmgof
mg
venom
venomof venom
of venom
[26].
[26]. Venom
Venom
[26]. Venom
[26]. Venom levels
levels in in
levels
levels urineurine and
in urine
in urine
and plasma
plasma
and plasma
and plasma
were
were measured
measured by by solid-phase
solid-phase radioimmunoassay.
radioimmunoassay. Plasma
Plasma levels
levels as ashighhigh as as
13001300 ng/mL
ng/mL occurred
occurred
were measured
were measured by by solid-phase
solid-phase radioimmunoassay.
radioimmunoassay. Plasma Plasma levels levels as as high
high as as13001300ng/mL ng/mL occurred occurred
within
within 1515 min min of injection in in controls, with progressive swelling in inthethe injected limb. Firm pressure
within
within 15of
15 min
min injection
of injection
of injection controls,
in controls,
in with
controls, progressive
with progressive
with progressive swelling swelling
swelling in
in injected limb.
the injected
the injected Firm
limb.
limb. pressure
Firm pressure
Firm pressure
to to
thethe injection
injection sitesite
and and
site immobilization
immobilization
and immobilization of of
limb limb
of with
limbwith a a splint
splint
to the injection site and immobilization of limb with a splint were effective in keeping venom levels
to the injection with a were
splint were effective
effective
were in
effective in keeping
keeping
in keeping venom
venom levels
levels
venom levels
lowlow until
until first aid was discontinued. The first aid measures prevented swelling. Animals treated with
low first
low until
until aid
firstwas
first aid
aiddiscontinued.
was
was discontinued.
discontinued. The first
The Theaid
first measures
firstaidaid prevented
measures
measures prevented swelling.
prevented Animals
swelling.
swelling. Animalstreated
Animals with
treated with
treated
thethe first aid
first
theaid
with first
the measures
measures
aid aidplus
firstmeasures plus
measures antivenom
antivenom
plus antivenom had
plus antivenomhad less less toxicity
hadtoxicity
less
hadtoxicity
less relative
relative to to
relative
toxicity those
those
relative treated
treated
to those with
to treated
those with antivenom
antivenom withalone,
with antivenom
treated alone,
antivenomalone,
particularly
particularly whenwhen first
first aid aid was given prior to to removal of
thethe pressure immobilization bandage and
particularly
alone, when
particularly firstwas
when aid given
firstwas prior
aidgiven
was prior
given removal
to removal
prior ofremoval
to pressure
of theimmobilization
theofpressure pressureimmobilization bandage
immobilization bandageand
bandage and
splint.
splint. TheThe authors
authors recommended
recommended basedbased on
onbased their
their study
study that that the the use use of
ofuse pressure
pressure immobilization
immobilization
splint.
and The The
splint. authors authors recommended
recommended based on on their
their study
study that
that the
the use of
of pressure
pressure immobilization
immobilization
bandages
bandages bebe considered
considered forfor humans
humans bitten
bitten byby C.
C. by adamanteus.
adamanteus.
bandages
bandages be considered
be considered for humans
for humans bitten
bitten by C. adamanteus.
C. adamanteus.
AA pilot
pilotA pilot
A study
study
pilot study of of
study of
pressure
pressure
of pressure
immobilization
immobilization
pressure immobilization
immobilization bandages
bandages
bandages forfor
bandages
rattlesnake
rattlesnake
for rattlesnake
for rattlesnake
bites
bites was waswas
bitesalso
bites alsoalsoperformed
wasperformed
also performed
performed in in inin
thethe porcine
porcine
the porcine
the model
model
porcine model usingusing
model using a a large
large
using aa large dosedose of
large dose of western
western
dose of of western diamondback
diamondback
western diamondback rattlesnake
rattlesnake
diamondback rattlesnake (Crotalus
(Crotalus
rattlesnake (Crotalus atrox)
atrox)
(Crotalus atrox) venom
venom
atrox) venom [27].
[27].
venom [27]. [27].
AA dose
dose AA of
of
dose
dose200 200
ofmg
of mg
200
200 ofmg of
mg
lyophilized
lyophilized
of lyophilized
of lyophilized
venom
venom was
venom
venom was chosen
chosen
was chosen
was to to
chosen testtest
tothe
to the
test
test concept,
concept,
the concept,
the concept,
because
because this
because
because this is
thethe
isthis
this
maximum
maximum
is
is the maximum
the maximum
amount
amount thatthat is
isthat obtained
obtained fromfrom a single
a single milking
milking of of thisthis species. AA randomized controlled study waswas
amount
amount that is obtained
is obtained from
from aa single
single milking
milking ofspecies.
of this species.
this species. randomized
A randomized
A randomized controlled controlled
controlled study was
study
study was
conducted
conducted with
with six six pigs.
pigs. The The ace ace bandage
bandage and and splint
splint werewere applied
applied immediately
immediately after
after subcutaneous
subcutaneous
conducted with
conducted with six six pigs.
pigs. The The ace ace bandage
bandage and and splint
splint were
were appliedapplied immediately
immediately after after subcutaneous
subcutaneous
administration
administration of ofvenomvenom in in aindistal
a distal hind hind paw. paw. Endpoint
Endpoint was was survival
survival to to2424 h. h. Three
Three subjects
subjects in inthethe
administration
administration of venom
of venom in aa distal
distal hind paw.
hind paw. Endpoint
Endpoint was survival
was survival to
to 24 h.
24 h. Three
Three subjects
subjects in the
in the
control
control group
group expired
expired between
between 191 191and and 305 min. All subjects in in thethe treatment group survived thethe 24
control group expired between 191305 andmin. 305 All min. subjects
All subjects treatment
in the treatment group survived
group survived 24the 24
h period.
h period. Antivenom
Antivenom was was administered
administered to tothethe subjects
subjects in in
thethe treatment
treatment group
group priorprior to to removal
removal of ofthethe
h period. Antivenom was administered to the subjects in the treatment group prior to removal of theTrop. Med. Infect. Dis. 2018, 3, 45 6 of 12
Trop. Med. Infect. Dis. 2018, 3, x FOR PEER REVIEW 6 of 11
control group expired between 191 and 305 min. All subjects in the treatment group survived the 24 h
bandage;
period. however, was
Antivenom one administered
subject expired
to after the bandage
the subjects in the was removed
treatment with
group hyperkalemia,
prior to removal ofmost
the
likely from
bandage; cell necrosis
however, from the
one subject venom.
expired While
after local necrosis
the bandage did occur
was removed andhyperkalemia,
with required treatment with
most likely
analgesia
from and antibiotics,
cell necrosis subjects
from the venom. who
While survived
local necrosiswere walking
did occur on the treatment
and required extremitywith7 days after
analgesia
envenomation.
and antibiotics, subjects who survived were walking on the extremity 7 days after envenomation.
2.6. Compression Pad
2.6. Compression Pad and
and Ring
Ring
A compression
A compression pad, pad, also
also known
known as as the
the Monash
Monash Method,
Method, consists
consists of of aa pad
pad placed
placed overover the
the site
site of
of
envenomation and
envenomation andheldheldin in place
place withwith a nonelastic
a nonelastic bandband
with awith a pressure
pressure of 70
of at least at mmleastHg,
70combined
mm Hg,
combined
with a splint with a splint tothe
to immobilize immobilize
extremity. the Thisextremity.
method was This method
tested was tested
in humans with ain humans with
radiolabeled mock a
radiolabeled mock venom with comparisons to an air splint and a pressure immobilization bandage
venom with comparisons to an air splint and a pressure immobilization bandage [28]. The air splint
[28].pressure
and The air splint and pressure
immobilization immobilization
bandage were usedbandage were used
with pressure with to
adjusted pressure
55 mmadjusted
Hg. Mock to venom
55 mm
Hg. Mock venom was measured in the serum. Venom in the serum was only retarded relative to
was measured in the serum. Venom in the serum was only retarded relative to controls by the pressure
controls
pad at 70by mm theHg.
pressure
Whether pad oratnot
70this
mmdifference
Hg. Whether was orduenotto this differencein
the difference was due to
devices orthe
thedifference
increased
in devicesused
pressure or the
forincreased pressurepad
the compression used for known.
is not the compression pad is not known.
A prospective study using the compression pad
A prospective study using the compression pad was
was conducted
conducted in 15 subjects
in 15 subjects bitten
bitten byby the
the
Russell’s viper
Russell’s viper (Daboia
(Daboia russelii
russelii siamensis)
siamensis) in in Myanmar.
Myanmar. Serum venom levels
Serum venom levels were monitored after
were monitored after the
the
application of a rubber pad placed over the bite site and attached with cotton bandages. The rubber
application of a rubber pad placed over the bite site and attached with cotton bandages. The rubber
pad measured
pad measured 65 65 ××6565× ×
2525mm mm andandthethecotton
cottonbandage
bandage measured
measured 65 mm
65 mm× 1.6×m,1.6except
m, exceptfor bites over
for bites
the fingers
over and toes,
the fingers and for
toes,which measurements
for which measurements were 55 × 3055× ×
were 2530mm × and
25 mm 55 ×and
25055mm × for
250the
mmpad forand
the
bandage, respectively. Proof that the pad retarded venom reaching the central circulation was
pad and bandage, respectively. Proof that the pad retarded venom reaching the central circulation
demonstrated
was demonstrated because venom
because venomlevels remained
levels remainedconstant in 15inof15
constant 23ofsubjects fromfrom
23 subjects the time the pad
the time the was
pad
placed
was untiluntil
placed the pad waswas
the pad removed.
removed. After the pad
After waswas
the pad removed,
removed, venom
venom levels increased
levels increased by by10 to
10 40
to
ng/mL. In the remaining 7 subjects, serum venom levels became undetectable while undergoing the
40 ng/mL. In the remaining 7 subjects, serum venom levels became undetectable while undergoing
padpad
the treatment
treatment[29].[29].
Since pressure immobilization
Since pressure immobilization bandages bandages could not be
could not be used
used forfor bites
bites on
on the
the torso,
torso, consideration
consideration
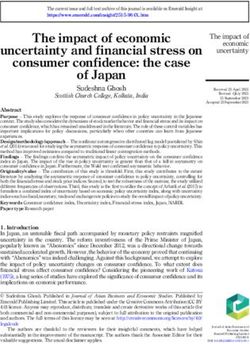
was given to a circumferential compression device consisting of a ring with two hooksfor
was given to a circumferential compression device consisting of a ring with two hooks forattaching
attachinga
a band
band to to apply
apply pressure
pressure (Figure
(Figure 3). This
3). This devicedevice
waswas tested
tested in theinporcine
the porcine
model model for experimental
for experimental torso
torso envenomations for both eastern coral snake (Micrurus fulvius fulvius) [30] and eastern
envenomations for both eastern coral snake (Micrurus fulvius fulvius) [30] and eastern diamondback
diamondback
rattlesnake rattlesnake [31].
[31].
Figure 3. Circumferential device applied with bands to inhibit lymphatic flow from a torso
Figure 3. Circumferential device applied with bands to inhibit lymphatic flow from a torso
envenomation. From [30], used with permission of the publisher.
envenomation. From [30], used with permission of the publisher.
The device consists of a ring with two hooks to attach an elastic belt. The dimensions were 8 × 5
× 3 cm. It was secured with an elastic belt wrapped around the animal. For the coral snake study, a
subcutaneous injection of a 10 mg lethal dose was injected in the torso. Endpoint was survival to 8 h.Trop. Med. Infect. Dis. 2018, 3, 45 7 of 12
The device consists of a ring with two hooks to attach an elastic belt. The dimensions were
8 × 5 × 3 cm. It was secured with an elastic belt wrapped around the animal. For the coral snake
study, a subcutaneous injection of a 10 mg lethal dose was injected in the torso. Endpoint was survival
to 8 h. Five of the six pigs in the treatment group survived 8 h, with one pig expiring after 293 min.
The three pigs in the control group developed respiratory failure at 322 min (range 272 to 382 min).
The result was significant, with Fisher’s exact test value of 0.04.
In the test of the compression ring device for the eastern diamondback rattlesnake experimental
envenomation to the torso in the porcine model, 50 mg of lyophilized venom reconstituted in sterile
water was injected subcutaneously in sedated subjects allowed to breathe spontaneously. Subjects were
monitored for cardiovascular collapse, fatal arrhythmia, loss of mean arterial pressure or pulse,
or respiratory arrest. Subjects in the treatment group had mean a time to toxicity of 355 ± 65 min
compared with a time of 32 ± 3.5 min in the control group, a result that was significant using a paired
t-test (with p < 0.03).
A study of pressure immobilization for intramuscular injections in a porcine model of
western diamondback rattlesnake (Crotalus atrox) envenomation found that pressure immobilization
prolonged survival and produced less edema than that observed in control animals, but increased
intracompartment pressures relative to in control animals without pressure immobilization [32].
2.7. Lymphatic Flow Inhibitors
Lymphatic flow inhibitors are pharmaceuticals that function by releasing nitric oxide, a compound
that inhibits the intrinsic lymphatic pump. Hence, nitric oxide releasing agents have been considered
as treatment to delay toxicity from venomous snakebites. Once such agent, glyceryl trinitrate ointment
(GTNO), has been studied as a topical agent in both humans and rats injected with mock venom. GTNO
(0.2% weight/weight) is commercially available (Rectogesic, Care Pharmaceuticals, Bondi Junction,
Australia). Human volunteers (6 male, 9 females, age range 20 to 65 years) were injected in the feet
with 50 microliters of sterile radiolabeled colloid. A crossover design was used, with each subject
having venom injected with and without treatment. Foot to groin transit time of the mock venom time
increased from 13 min (range 4 to 81 min) in the controls to 54 min (range 6.5 to 162 min) with treatment.
The result was reported as highly significant with p < 0.0001 (statistical method not specified [33]).
The treatment was also studied in anesthetized rats injected in the hind foot with eastern brown
snake venom (Pseudonaja textilits). The experiment demonstrated that smearing the entire extremity
with GTNO increased the time to respiratory arrest from 65 ± 4 min in control rats to 96 ± 6 min in
GTNO-treated rats (p < 0.001; log-rank test) [33].
2.8. Trypsin Injection
Trypsin is a proteolytic enzyme that has the potential to degrade protein toxins. The proposed
mechanism of action is to digest protein venoms. A randomized, blinded study in anesthetized pigs
was conducted [34]. One minute after injection in a distal hind limb of 10 mg of eastern coral snake
venom (Micrurus fulvius fulvius) dissolved in 1 mL of water, subjects were randomized to receive either
1 mL of saline or 1 mL of trypsin (100 mg/mL) at the envenomation site by a blinded investigator.
Endpoint was survival to 3 days. Respiratory depression occurred more frequently in control subjects
than in those that received trypsin (p = 0.009; Fisher’s exact test). Four of the six pigs that received
trypsin survived to the end of the 3-day study while no control pigs survived. Trypsin is inexpensive
and readily available and would most likely be used for highly potent protein venoms, but further
study is needed before trypsin could be recommended for general use.
2.9. Herbal Medicines
Medicinal plants are used to treat snakebites. A large volume of literature exists on the topic that
is too large to review in this article. A recent review focused on their use in Central America [35] and
concluded that ‘available pharmacological data suggest different plant species may target differentTrop. Med. Infect. Dis. 2018, 3, 45 8 of 12
symptoms of snakebites, such as pain or anxiety, although more studies are needed to further evaluate
the scientific basis for their use.’ A study in Brazil [36] found that extracts of the plant Jatropha mollissima
(Euphorbiaceae), used in folk medicine, had efficacy in reducing local effects from snakebites by the
Bothrops genus that cause the majority of snakebites in Brazil, and suggested that it be used as an
adjuvant to antivenom, which the authors report is less effective in reducing local effects than systemic
effects. A study in a mouse model of Bothrops envenomation found that the plant Costus spicatus,
used in folk medicine as an anti-inflammatory medication, reduced pain and inflammation [37].
Euphorbia hirta was found to reduce lethality in a mouse model of Indian cobra (Naja naja) experimental
snakebites, and the compound quercetin-3-O-alpha-rhamnoside extracted from the plant was found to
have activity against the venom [38]. These and many other studies suggest that traditional medicinal
plants reduce pain and suffering from snakebites and, in specific cases, may prevent lethality. Further
study in this area could lead to specific pharmaceuticals targeted to species against which they have
activity, though development in this area is expensive and unlikely to be widely funded.
2.10. Position Statements
According to the World Health Organization Guidelines for the Management of Snake-Bites [1],
Most of the familiar methods for first-aid treatment of snake-bite, both western and
‘traditional/herbal’, have been found to result in more harm (risk) than good (benefit).
Their use should be discouraged and they should never be allowed to delay the movement
of the patient to medical care at the hospital or dispensary. Recommended first-aid methods
emphasize reassurance, immobilization of the whole patient and particularly the bitten
limb and movement of the patient to a place where they can receive medical care as soon
as possible.
A joint position statement by the American College of Medical Toxicology, American Academy of
Clinical Toxicology, American Association of Poison Control Centers, European Association of Poison
Centers and Clinical Toxicology, International Society of Toxonology, and the Asian Pacific Association
of Medical Toxicology concluded [39],
Given that the primary toxic effect of envenomation is local tissue injury, mortality is not an ideal
outcome measure to extrapolate to human crotaline envenomation. Available evidence fails to
establish the efficacy of pressure immobilization in humans, but does indicate the possibility
of serious adverse events arising from its use. The use of pressure immobilization for the
pre-hospital treatment of North American Crotalinae envenomation is not recommended.
The American Heart Association first aid manual (combined 2010 and 2015 recommendations)
states that the use of pressure immobilization bandages for venomous snakebites be considered,
stating [17],
Applying a pressure immobilization bandage with a pressure between 40 and 70 mm Hg in
the upper extremity and between 55 and 70 mm Hg in the lower extremity around the entire
length of the bitten extremity is a reasonable way to slow the spread of venom by slowing
lymph flow.
For practical purposes pressure is sufficient if the bandage is comfortably tight and snug
but allows a finger to be slipped under it. Initially it was theorized that slowing lymphatic
flow by external pressure would only benefit victims bitten by snakes producing neurotoxic
venom, but the effectiveness of pressure immobilization has also been demonstrated for
bites by non-neurotoxic American snakes in an animal model. The challenge is to find a
way to teach the application of the correct snugness of the bandage because inadequate
pressure is ineffective and too much pressure may cause local tissue damage. It has also been
demonstrated that, once learned, retention of the skill of proper pressure and immobilization
application is poor.Trop. Med. Infect. Dis. 2018, 3, 45 9 of 12
In Australia, where there are neurotoxic elapid snakes, the recommendation for snakebite first aid
is pressure immobilization bandages [40]:
The first aid for a suspected or definite snake bite is a pressure bandage with immobilization
(PBI). The pressure bandage should be a broad (15 cm) elastic bandage, rather than a crepe
bandage. The bandage is applied over the bite site and then distally to proximally covering
the whole limb. It should be applied about as tight as that used for a sprained ankle. The limb
and whole patient should be immobilized for the first aid to be effective. The bandage and
immobilization should remain until the patient has been transferred and assessed in hospital.
The bandage should only be removed if antivenom is available and after there is no evidence
of envenoming based on the admission laboratory tests and clinical examination. If the
patient is envenomed the bandage can be removed after antivenom has been administered.
3. Conclusions
Antivenom is the definitive treatment for venomous snakebites and should be administered
as soon as possible after a bite. First aid measures should be directed at reducing systemic toxicity
by limiting lymphatic flow. Splints, rest, and avoidance of movement should reduce movement of
the involved extremity. Positioning of the extremity below or at the level of the heart should be
individualized—for snakebites with severe and potentially fatal systemic toxicity, systemic toxicity
might be delayed by positioning the extremity below the heart, while for snakebites with severe local
tissue damage and less systemic toxicity, positioning the extremity below the heart could increase
local toxicity.
Pressure immobilization bandages, compression pads, and compression rings have been shown
in experimental studies to delay systemic absorption of venom and to reduce mortality in some
models. Limited human data supports their use in specific circumstances. They have not been as
effective in field use relative to the laboratory settings because bandages have been applied too loosely,
have not been applied to the entire extremity, and use of a splint has been inconsistent [41]. In a
simulated setting, neither health professionals nor members of the general public performed well in
applying pressure immobilization bandages [42]. The materials necessary for applying this and other
techniques may not be readily available in many circumstances. Their use should be individualized to
the circumstances of the bite, including region, species, timeliness of definitive treatment, and local
guidelines. They are expected to be most helpful in snakebites with lethal systemic toxicity, limited
local toxicity, and a long delay to definitive treatment with antivenom.
Pharmacological treatment with the topical nitric oxide inhibitor GTNO and injection of trypsin
delayed toxicity in experimental studies but need further study. At this time, it is not possible to
give a recommendation for the use of GTNO. Injection of trypsin at the site of the bite has likewise
been efficacious in the treatment of eastern coral snake envenomations in an experimental study but
is not sufficiently developed to recommend its use at this time. Plant extracts used in traditional
medicine have been shown to help with pain and inflammation, and in certain cases to reduce lethality
in experimental studies, and can be considered in rural areas in which folk remedies are available, but
not antivenom.
Injection of trypsin at the site of envenomation had efficacy in one experimental study in a
porcine model and could conceivably play a role in selected situations. However, this approach needs
further investigation.
A number of treatments are generally not recommended. Tourniquets cause limb ischemia
and amputations. Electric shock is dangerous in experimental studies and is not recommended.
Suction devices have no efficacy in experimental studies and cannot be recommended.
Author Contributions: J.P.-C. and W.J.M. wrote the paper.
Conflicts of Interest: The authors declare no conflict of interest.Trop. Med. Infect. Dis. 2018, 3, 45 10 of 12
References
1. Warrell, D.A. Guidelines for the Management of Snake-Bites in South-East Asia. Available online:
http://apps.searo.who.int/PDS_DOCS/B4508.pdf (accessed on 28 January 2018).
2. World Health Organization. Guidelines for the Prevention and Clinical Management of Snakebites in Africa.
Available online: http://www.who.int/ipcs/poisons/snakebite/en/ (accessed on 28 January 2018).
3. Fish, L.R.; O’Rourke, D.P.; Lust, R.; Brewer, K.L.; Meggs, W.J. Cardiovascular effects of intravenous rattlesnake
envenomation. Ann. Emerg. Med. 2008, 52, S140. [CrossRef]
4. Tan, C.H.; Sim, S.M.; Gnanathasan, C.A.; Fung, S.Y.; Tan, N.H. Pharmacokinetics of the Sri Lankan
hump-nosed pit viper (Hypnale hypnale) venom following intravenous and intramuscular injections of
the venom into rabbits. Toxicon 2014, 79, 37–44. [CrossRef] [PubMed]
5. Barnes, J.M.; Trueta, J. Absorption of bacteria, toxins, and snake venoms from the tissues: Importance of the
lymphatic circulation. Lancet 1941, 237, 623–626. [CrossRef]
6. Scallan, J.P.; Zawieja, S.D.; Castorena-Gonzalez, J.A.; Davis, M.J. Lymphatic pumping: Mechanics,
mechanisms and malfunction. J. Physiol. 2016, 594, 5749–5768. [CrossRef] [PubMed]
7. Watt, G.; Padre, L.; Tuazon, M.L.; Theakston, R.D.; Laughlin, L.W. Tourniquet application after cobra bite:
Delay in the onset of neurotoxicity and the dangers of sudden release. Am. J. Trop. Med. Hyg. 1988, 38,
618–622. [CrossRef] [PubMed]
8. Amaral, C.F.; Campolina, D.; Dias, M.B.; Bueno, C.M.; Rezende, N.A. Tourniquet ineffectiveness to reduce
the severity of envenoming after Crotalus durissus snake bite in Belo Horizonte, Minas Gerais, Brazil. Toxicon
1998, 36, 805–808. [CrossRef]
9. Michael, G.C.; Thacher, T.D.; Shehu, M.I. The effect of pre-hospital care for venomous snake bite on outcome
in Nigeria. Trans. R. Soc. Trop. Med. Hyg. 2011, 105, 95–101. [CrossRef] [PubMed]
10. Pugh, R.N.; Theakston, R.D. Fatality following use of a tourniquet after viper bite envenoming. Ann. Trop.
Med. Parasitol. 1987, 81, 77–78. [CrossRef] [PubMed]
11. Kanaan, N.C.; Ray, J.; Stewart, M.; Russell, K.W.; Fuller, M.; Bush, S.P.; Caravati, E.M.; Cardwell, J.;
Norris, R.L.; Weinstein, S.A. Wilderness Medical Society practice guidelines for the treatment of pit viper
envenomations in the United States and Canada. Wilderness Environ. Med. 2015, 26, 427–487. [CrossRef]
[PubMed]
12. Alberts, M.B.; Shalit, M.; LoGalbo, F. Suction for venomous snakebite: A study of ‘mock venom’ extraction
in a human model. Ann. Emerg. Med. 2004, 43, 181–186. [CrossRef]
13. Bush, S.P.; Hegewald, K.G.; Green, S.M.; Cardwell, M.D.; Hayes, W.K. Effects of a negative pressure venom
extraction device (Extractor) on local tissue injury after artificial rattlesnake envenomation in a porcine
model. Wilderness Environ. Med. 2000, 11, 180–188. [CrossRef]
14. Bronstein, A.C.; Russell, F.E.; Sullivan, J.B. Negative pressure suction in the field treatment of rattlesnake
bite. Vet. Hum. Toxicol. 1985, 28, 297, (Abstract).
15. Bronstein, A.C.; Russell, F.E.; Sullivan, J.B. Negative pressure suction in the field treatment of rattlesnake
bite victims. Vet. Hum. Toxicol. 1986, 28, 485, (Abstract).
16. Gellert, G.A. Snake-venom and insect-venom extractors: an unproved therapy (letter). N. Engl. J. Med. 1992,
327, 1322. [CrossRef] [PubMed]
17. American Heart Association. Part 15. First Aid. Web-Based Integrated 2010 & 2015 American Heart Association
and American Red Cross Guidelines for First Aid. Available online: https://eccguidelines.heart.org/index.
php/circulation/aha-red-cross-first-aid-guidelines/part-15-first-aid/ (accessed on 28 January 2018).
18. Barker, S.; Charlton, N.P.; Holstege, C.P. Accuracy of internet recommendations for prehospital care of
venomous snake bites. Wilderness Environ. Med. 2010, 21, 298–302. [CrossRef] [PubMed]
19. Guderian, R.H.; Mackenzie, C.D.; Williams, J.F. High voltage shock treatment for snakebite. Lancet 1986, 2, 229.
[CrossRef]
20. Johnson, E.K.; Kardong, K.V.; Mackessy, S.P. Electric shocks are ineffective in treatment of lethal effects of
rattlesnake envenomation in mice. Toxicon 1987, 25, 1347–1349. [CrossRef]
21. Howe, N.R.; Meisenheimer, J.L. Electric shock does not save snakebitten rats. Ann. Emerg. Med. 1988, 17,
254–256. [CrossRef]
22. Dart, R.C.; Gustafson, R.A. Failure of electric shock treatment for rattlesnake envenomation. Ann. Emerg. Med.
1991, 6, 659–661. [CrossRef]Trop. Med. Infect. Dis. 2018, 3, 45 11 of 12
23. Sutherland, S.K.; Coulter, A.R.; Harris, R.D. Rationalisation of first-aid measures for elapid snakebite. Lancet
1979, 313, 183–186. [CrossRef]
24. German, B.T.; Hack, J.B.; Brewer, K.L.; Meggs, W.J. Pressure-immobilization bandages delay toxicity in a
porcine model of eastern coral snake (Micrurus fulvius fulvius) Envenomation. Ann. Emerg. Med. 2005, 45,
603–608. [CrossRef] [PubMed]
25. Smyrnioudis, M.E.; O’Rourke, D.P.; Rosenbaum, M.D.; Brewer, K.L.; Meggs, W.J. Long-term efficacy of
pressure immobilization bandages in a porcine model of coral snake envenomation. Am. J. Emerg. Med. 2014,
32, 1024–1026. [CrossRef] [PubMed]
26. Sutherland, S.K.; Coulter, A.R. Early management of bites by the eastern diamondback rattlesnake (Crotalus
adamanteus): Studies in monkeys (Macaca fascicularis). Am. J. Trop. Med. Hyg. 1981, 30, 497–500. [CrossRef]
[PubMed]
27. Meggs, W.J.; Courtney, C.; O’Rourke, D.P.; Brewer, K.L. Pilot studies of pressure-immobilization bandages
for rattlesnake envenomations. Clin. Toxicol. 2010, 48, 61–63. [CrossRef] [PubMed]
28. Anker, R.L.; Straffon, W.G.; Loiselle, D.S.; Anker, K.M. Retarding the uptake of ‘mock venom’ in humans:
Comparison of three first-aid treatments. Med. J. Aust. 1982, 5, 212–214.
29. Pe, T.; Myint, A.A.; Han, K.E.; Ha, T.; Swe, T.N. Local compression pads as a first-aid measure for victims
of bites by Russell’s viper (Daboia russelii siamensis) in Myanmar. Trans. R. Soc. Trop. Med. Hyg. 1995, 31,
346–348.
30. Hack, J.B.; Deguzman, J.M.; Brewer, K.L.; Meggs, W.J.; O’Rourke, D.P. A localizing circumferential
compression device increases survival after coral snake evenomation to the torso of an animal model.
J. Emerg. Med. 2011, 41, 102–107. [CrossRef] [PubMed]
31. Hack, J.B.; Orogbemi, B.; Deguzman, J.M.; Brewer, K.L.; Meggs, W.J.; O’Rourke, D.P. A localizing
circumferential compression device delayed death after artificial eastern diamondback rattlesnake
envenomation to the torso of an animal model in a pilot study. J. Med. Toxicol. 2010, 6, 207–211. [CrossRef]
[PubMed]
32. Bush, S.P.; Green, S.M.; Laack, T.A.; Hayes, W.K.; Cardwell, J.; Tanen, D.A. Pressure immobilization delays
mortality and increases intracompartmental pressure after artificial intramuscular rattlesnake envenomation
in a porcine model. Ann. Emerg. Med. 2004, 6, 599–604. [CrossRef]
33. Saul, M.E.; Thomas, P.A.; Dosen, P.J.; Isbister, G.K.; O’Leary, M.A.; Whyte, I.M.; McFadden, S.A.;
van Helden, D.F. A pharmacological approach to first-aid treatment of snakebite. Nat. Med. 2011, 17,
809–811. [CrossRef] [PubMed]
34. Parker-Cote, J.L.; O’Rourke, D.P.; Brewer, K.L.; Lertpiriyapong, K.; Punja, M.; Bush, S.P.; Miller, S.N.;
Meggs, W.J. Efficacy of trypsin in treating coral snake envenomation in the porcine model. J. Med. Toxicol.
2015, 4, 430–432. [CrossRef] [PubMed]
35. Giovannini, P.; Howes, M.R. Medicinal plants used to treat snakebite in Central America: Review and
assessment of scientific evidence. J. Ethnopharmacol. 2017, 199, 240–256. [CrossRef] [PubMed]
36. Gomes, J.A.; Felix-Silva, J.; Fernandes, M.J.; Amaral, J.G.; Lopes, N.P.; Tabosa do Egito, E.S.;
da Silva-Junior, A.A.; Zucolotto, S.M.; Fernandes-Pedrosa, M.F. Aqueous leaf extract of Jatropha mollissima
(Pohl) Bail decreases local effects induced by bothropic venom. BioMed Res. Int. 2016, 2016, 6101742.
[CrossRef] [PubMed]
37. Picanco, L.C.; Bittencourt, J.A.; Henriques, S.V.; da Silva, J.S.; Oliveira, J.M.; Ribeiro, J.R.; Sanjay, A.B.;
Carvalho, J.C.; Stien, D.; Silva, J.O. Pharmacological activity of Costus spicatus in experimental Bothrops atrox
envenomation. Pharm. Biol. 2016, 54, 2103–2110. [CrossRef] [PubMed]
38. Gopi, K.; Anbarasu, K.; Renu, K.; Jayanthi, S.; Vishwanath, B.S.; Jayaraman, G. Quercetin-3-O-rhamnoside
from Euphorbia hirta protects against snake venom induced toxicity. Biochim. Biophys. Acta 2016, 1860,
1528–1540. [CrossRef] [PubMed]
39. American College of Medical Toxicology; American Academy of Clinical Toxicology; American Association
of Poison Control Centers; European Association of Poison Control Centres; International Society of
Toxinology; Asian Pacific Association of Medical Toxicology. Pressure immobilization after North American
Crotalinae snake envenomation. J. Med. Toxicol. 2011, 49, 881–882.
40. Ministry of Health, NSW Government. Snakebite and Spiderbite Clinical Management Guidelines 2013.
Third Edition. (2013). Available online: http://www1.health.nsw.gov.au/pds/ActivePDSDocuments/
GL2014_005.pdf (accessed on 21 February 2018).You can also read