Bugs and Drugs Handbook 2020 - Children's Hospital Colorado
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Bugs and Drugs Handbook
2020
Amelia Velasquez
Age 9

Table of Contents
Page
How to Improve Infectious Disease Outcomes and Reduce Costs- Sutton’s
Law: “Culture Where the Infection Is!”................................................................................................. 1
Legend for Antimicrobial Tables ............................................................................................................ 2
Antibiogram Table 1 - Staphylococci ...................................................................................................... 3
Antibiogram Table 2A and 2B - Streptococci ........................................................................................ 4-5
Antibiogram Table 3 – Gram Negative Organisms Non-Urine ............................................................ 6
Antibiogram Table 4 – Gram Negative Organisms Urine .................................................................... 7
Antibiogram Table 5 – Gram Negative Orgs Non-Enterobacteriaceae............................................... 8
Antibiogram Table 6 – Candida spp ....................................................................................................... 9
Antibiogram Table 7 – Anaerobes........................................................................................................... 10
Microbiology Testing Schedule................................................................................................................ 11
Multiplex PCR Information .....................................................................................................................12-14
Culture Collection and Testing Information ..........................................................................................14-18
Critical and Urgent Value Reporting Policy for Microbiology ............................................................ 18
Blood Isolates............................................................................................................................................. 19
MRSA and VRE Rates .............................................................................................................................20-21
Influenza Virus Treatment and Antiviral Medications Recommended ..............................................22-24
Guidelines for Changing from IV to PO Antibiotics in Hospitalized Children ..................................25-26
Antimicrobial Formulary at Children’s Hospital Colorado .................................................................27-38
Collection Guidelines for Antimicrobial Levels .....................................................................................39-42Bugs and Drugs Authorship
For additional copies of this publication, please call the Microbiology Laboratory at 720-777-6703, download a
copy from My Children’s Colorado website or request an electronic copy from Elaine Dowell or Stacey
Hamilton.
Thanks to the following contributors to this booklet:
Sam Dominguez, MD, PhD
Medical Director, Clinical Microbiology Laboratory
Associate Medical Director, Infection Prevention and Control
Sarah Parker, MD
Professor of Pediatric Infectious Diseases
Medical Director of Antimicrobial Stewardship
Sarah Jung, PhD, D(ABMM)
Assistant Director of Microbiology
Elaine Dowell, MT(ASCP)SM
Senior Manager Microbiology and Precision Diagnostics
elaine.dowell@childrenscolorado.org
Stacey Hamilton, MT(ASCP)SM
Microbiology Manager
stacey.hamilton@childrenscolorado.org
Kristin Pretty, M(ASCP)MB
Supervisor Virology/Molecular Microbiology
Jason Child, PharmD, BCIDP
Infectious Disease Pharmacist
Christine MacBrayne, PharmD, MSCS, BCIDP
Infectious Disease Pharmacist
Ann-Christine Nyquist, MD, MSPH
Medical Director, Infection Prevention and Control
© Children's Hospital ColoradoHow to Improve Infectious Disease Outcomes and Reduce Costs
Sutton’s Law: Culture Where the Infection Is!
Key Principles for Culturing and Antimicrobial Use:
1. “Garbage In, Garbage Out” – Don’t order cultures if you won’t know
how to interpret the result. This often applies to surface (skin, mucous
membranes) cultures that are always colonized with normal flora.
2. “Tissue is the Issue” Don’t use swabs; get a tissue biopsy or needle
aspirate. Bacteria are absorbed into and die on swabs.
3. Sutton’s Law: “Culture where the infection is” – Blood cultures will only
be positive2019 Annual Antibiogram
Tables 1 – 8
Legend for Antibiogram Tables
Indicates first-line therapy, with susceptibility between 75-100%. This medication
has good penetration, limited side-effects and overall strong susceptibilities.
Second-line. Susceptibility between 75-100%, but not first choice due to overly
broad-spectrum, toxicities, or both. May be appropriate as initial therapy before
specific bacteria has been identified.
Susceptibility between 50-74%. Not initial treatment of choice, but can be used if
other medications are not available, patient has significant allergies, or
susceptibility known.
Susceptibility for these medications is less than 50%. Consult ID prior to using
these medications and/or use only if known susceptible.
- Not tested.
R This organism is known to have intrinsic resistance to this antibiotic.
This organism is known to be susceptible to this antibiotic.
S
Small number of organisms used for data collection.
()
Color scheme adapted from the Sanford Guide to Antimicrobial Therapy
2TABLE 1. Gram Positive Organisms: Staphylococcus (% Susceptible)
Antimicrobial Susceptibilities at Children’s Hospital Colorado – 2019
ANTIMICROBIALS
NUMBER OF ISOLATES
Trimethoprim / Sulfa
ORGANISMS
Vancomycin
Clindamycin
Oxacillin*
TESTED
Staph aureus (MSSA) 574 100 84 99 100
Staph aureus (MRSA) 230 100 83 99 R
Staph epidermidis 101 100 - 74 30
Staph hominis 32 100 - 84 41
Testing by Microscan Microtiter Panel.
* Includes agents: Nafcillin/Dicloxacillin/Methicillin. If susceptible, also susceptible to
cefazolin/cephalexin and beta lactam + beta lactamase combinations. If susceptible, this does
not infer susceptibility to clindamycin; please see specific clindamycin results.
Oxacillin resistance in Staphylococcus spp. predicts resistance to ALL beta-lactams including
penicillins, carbapenems, β-lactam/β-lactamase inhibitor combinations, cephems (except for
cephalosporins with anti-MRSA activity, namely ceftaroline).
Confirmation of MRSA is done by PBP2, Cefoxitin Screen or Microscan Panel.
Cefoxitin is tested as a surrogate for oxacillin. Oxacillin susceptible or resistant is based on the
Cefoxitin Screen result.
Clindamycin susceptibility is not determined by Cefoxitin Screen or oxacillin resistance.
The Inducible Clindamycin Test detects inducible clindamycin resistance, due to the erm genes.
The isolate is presumed resistant to clindamycin when the Inducible Clindamycin Test is positive.
3TABLE 2A. Gram Positive Organisms - Streptococcus and Enterococcus
(% Susceptible)
Antimicrobial Susceptibilities at Children’s Hospital Colorado – 2019
ANTIMICROBIALS
NUMBER OF
ISOLATES
Clindamycin
Vancomycin
Amoxicillin
Ceftriaxone
Ampicillin/
Penicillin^
ORGANISMS
Strep. anginosus Group1 – Invasive* ,+ 32 96 - 100 81 97
Strep. mitis1 * , ++ 49 49 - 100 94 90
Viridans Strep Group1 * ,+++ 96 73 - 100 89 94
Beta Strep Group A1 – Invasive 32 S S S 97 S
Beta Strep Group B 1 61 S S S 67 S
Beta Strep Group B 1 (prenatal screens) 568 S S 100 54 S
Enterococcus faecalis2 115 - 100 100 - -
Enterococcus faecium 2 (24) - 71 96 - -
1 Testing is by Sensititre microtiter panel. 2Testing is by Microscan microtiter panel.
Streptococci:
The Inducible Clindamycin Test (D-test) detects inducible clindamycin resistance due to the erm gene.
For streptococci, resistance to clindamycin is presumed when the D-Test is positive.
* Most penicillin non-susceptible streptococci that fall into the intermediate MIC
range (0.25 to 2 µg/mL) can be treated with high dose ampicillin/amoxicillin.
+ Of the penicillin non-susceptible S. anginosus isolates tested, 2% were intermediate and
2% were resistant.
++ Of the penicillin non-susceptible Strep. mitis group isolates tested, 43% were intermediate and 8%
were resistant.
+++ Of the penicillin non-susceptible viridans streptococci tested, 22% were intermediate and 5%
were resistant.
^ Streptococci susceptible to penicillin are also susceptible to ampicillin/amoxicillin.
Enterococci
Combination therapy should be used in serious Enterococcus spp. Infection (endocarditis & bacteremia).
Gentamicin Synergy Screen – E. faecalis = 90% susceptible
Gentamicin Synergy Screen – E. faecium = 88% susceptible
Isolates that are susceptible to ampicillin cannot be assumed to be susceptible to penicillin.
One new VRE patient was identified in 2019. For therapy choices, ID consult recommended.
4TABLE 2B. Gram Positive Organisms: Streptococcus pneumoniae (% Susceptible)
Antimicrobial Susceptibilities at Children’s Hospital Colorado - 2019
ANTIMICROBIALS
(Nonmeningitis breakpoint)
(Nonmeningitis breakpoint)
Trimethoprim/Sulfa
Number of isolates
(Meningitis breakpoint)
(Meningitis breakpoint)
Source
Vancomycin
Clindamycin
Ceftriaxone
Ceftriaxone
Penicillin^
Penicillin^
CSF* (12) NA 92 NA 100 - - 100
Blood or
Sterile 36 100 64 100 94 92 78 100
Aspirate
Respiratory
and 127 97 61 98 82 87 78 100
Other
Testing is by Sensititre microtiter panel.
Patients with pneumococcal meningitis should be started on vancomycin and ceftriaxone until
susceptibilities are available. Isolates were recovered in 2017, 2018 and 2019.
Refer to organism specific susceptibility. Isolates in the intermediate category to penicillin may be
treated with high dose ampicillin/amoxicillin unless in the CNS.
S. pneumoniae isolates that are susceptible to penicillin are also susceptible to ampicillin (and amoxicillin
if oral choice is appropriate).
Ceftriaxone susceptibility does not imply susceptibility to oral cephalosporins.
5TABLE 3. Gram Negative Organisms, Non-Urine (% Susceptible)
Antimicrobial Susceptibilities at Children’s Hospital Colorado – 2019
ANTIMICROBIALS
Ampicillin / Amoxicillin
NUMBER OF ISOLATES
Trimethoprim / Sulfa
ORGANISMS
Cefotaxime **
Ciprofloxacin
Gentamicin
Cefazolin
No further testing is routinely performed for beta-
Haemophilus influenzae1*
80 lactamase negative isolates. These isolates are
Beta-lactamase testing - all isolates
considered ampicillin susceptible.
Haemophilus influenzae1* 37 30 - 100 - - -
Escherichia coli2 96 41 81 88 90 68 81
Enterobacter cloacae complex2 39 R R IB^ 100 97 97
Klebsiella pneumoniae2 42 R 88 98 98 90 100
Klebsiella oxytoca2 (26) R 54 100 96 92 96
Serratia marcescens 2 (11) R R IB^ 100 100 91
SalmSalmonella species2 46 76 - 96 - 87 -
Shigella species2,*** 47 573 - 98 - 47 -
1
Tested by Sensititre microtiter panel. 2Tested by Microscan microtiter panel. 3Tested by disk diffusion.
Haemophilus influenzae isolates that test positive for beta-lactamase production are still considered
susceptible to ampicillin-sulbactam or amoxicillin-clavulanic acid.
**Cefotaxime susceptible isolates are also ceftriaxone susceptible.
***Isolates were recovered in 2017, 2018 and 2019.
When IB is indicated above, the organism may have an inducible beta-lactamase. Although the MIC may
indicate susceptibility, beta-lactams should only be used in combination with a drug from another class to
which the organism is susceptible. Cefepime and meropenem are exceptions and may be used alone.
6TABLE 4. Gram Negative Organisms Isolated from Urine (% Susceptible)
Antimicrobial Susceptibilities at Children’s Hospital Colorado – 2019+
ANTIMICROBIALS
Ampicillin / Amoxicillin
NUMBER OF ISOLATES
Ampicillin/Sulbactam
Trimethoprim / sulfa
ORGANISMS
Nitrofurantoin
Cefotaxime **
Cephalothin*
Ciprofloxacin
Ceftazidime
Gentamicin
Cefuroxime
Cefepime
E. coli 1366 63 56 68 94 95 92 98 74 90 96 -
Enterobacter cloacae
43 R R R R IB^ 95 33 84 98 98 -
complex
Klebsiella
106 R 75 78 89 94 88 52 80 88 96 -
pneumoniae
Klebsiella oxytoca 43 R 63 67 81 100 100 98 93 95 100 -
Proteus mirabilis 72 90 96 99 99 99 96 R 85 94 100 -
Citrobacter freundii
(21) R R R R IB^ 86 86 81 86 100 -
complex
Pseudomonas
44 R R R R R 89 R R 89 95 98
aeruginosa
Testing by Microscan microtiter panel.
+ Breakpoints used for interpretations have been established by the FDA and may not be consistent with current
CLSI guidelines. Isolates that test resistant may respond to high levels of antimicrobials present in urine.
Cephalothin results are a surrogate to predict susceptibility to the oral cephalosporin agents: cephalexin,
cefuroxime, cefpodoxime, and cefdinir. Notably for lower tract infection, low level resistance can often be
overcome by high-end dosages due to high concentrations of these agents in the urine.
**Isolates that are susceptible to cefotaxime are also susceptible to ceftriaxone.
When IB is indicated above, the organism may have an inducible beta-lactamase. Although the MIC may
indicate susceptibility, beta-lactams should only be used in combination with a drug from another class to
which the organism is susceptible. Cefepime and meropenem are exceptions and may be used alone.
7TABLE 5. Non-Enterobacteriaceae (% Susceptible)
Antimicrobial Susceptibilities at Children’s Hospital Colorado– 2019
ANTIMICROBIALS
NUMBER OF ISOLATES
Trimethoprim / Sulfa
ORGANISMS
Pip/Tazobactam
Ciprofloxacin
Meropenem
Levofloxacin
Minocycline
Ceftazidime
Tobramycin
Gentamicin
Aztreonam
Cefepime
Pseudomonas
aeruginosa
• Non CF1 96 94 86 - - - 93 76 90 97 - -
• CF-mucoid2,3 38 79 68 66 - - 58 - - - - 80
• CF-nonmucoid2,3 63 82 68 73 - - 67 - - - - 43
Stenotrophomonas
32 12 - - 90 72 - - - - 59 -
maltophilia2,3
1 Non-CF testing performed by Microscan microtiter panel.
2 Cystic fibrosis (CF) Pseudomonas spp. isolates and S. maltophilia isolates tested by E-test.
3
Isolates recovered in 2017, 2018 and 2019 were included in this data.
8TABLE 6. Candida species (% Susceptible)
Antimicrobial Susceptibilities at Children’s Hospital Colorado– 2019
ANTIFUNGALS
NUMBER OF ISOLATES
ORGANISMS
Amphotericin
Posaconazole
5-Flucytosine
Voriconazole
Itraconazole
Fluconazole
Micafungin
Candida albicans (21) NI NI 100 NI 100 NI 100
Candida parapsilosis (19) NI NI 100 NI 100 NI 100
Candida glabrata (13) NI NI (SDD)* NI 85 NI NI
Candida lusitaniae (7) NI NI NI NI NI NI NI
Testing performed at University of Colorado Microbiology lab by microbroth dilution
Isolates recovered in 2017, 2018 and 2019 were included in this table.
NI – No interpretative criteria available
SDD - Susceptible Dose Dependent
The susceptible dose dependent category implies that susceptibility of an isolate is
dependent upon the dosing regimen that is used in the patient. It is necessary to
use a dosing regimen (higher doses, more frequent doses or both) that results in
high drug exposure. ID consult recommended.
Please Note: C. krusei is intrinsically resistant to fluconazole (isolates not tested).
Yeast susceptibilities were performed from the following sources:
CSF/Shunt/Blood – 16
Sterile Aspirate/Tissue - 10
Stool – 2
Miscellaneous/Wound – 12
Urine – 8
Respiratory –5
Vaginal - 2
9Table 7. Cumulative Antimicrobial Susceptibility Report for Anaerobic Organisms
ANAEROBIC ORGANISMS
Isolates Collected from Selected US hospitals Jan 2013 through December 2016
ANTIMICROBIALS
Ampicillin-sulbactam (Unasyn®)
Piperacillin/tazobactam
Number of Isolates
Number of Isolates
Number of Isolates
Number of Isolates
Number of Isolates
Number of Isolates
Number of Isolates
Metronidazole
Clindamycin
Meropenem
Cefoxitin
Penicillin
Percent Susceptible (%S) (Zosyn®)
% % % % % % % % % % % % % % %
10
and Percent Resistant
S R S R S R S R S R S S R S R
(%R)
Breakpoints ug/ml 32/16 128/4 64 16 2 8 32
B. fragilis 129 84 2 1030 96 1 830 100 0 1505 93 5 - - - 1013 26 22 1140 100 0
Fusobacterium
(20) 100 0 55 96 2 - - - (20) 100 0 - - - 75 77 21 75 95 5
nucleatum- necrophorum
Anaerobic Gram- positive
- - - 1853 99 1 - - - 1647 100 0 1647 100 0 1826 97 3 1692 100 0
cocci
Cutibacterium acnes
- - - (18) 100 0 - - - - - - - - - (17) 53 35 (18) 0 100
(formerly P. acnes)
Data adapted from CLSI M100-S28 January 2019.
Data was generated from unique isolates from patient specimens submitted to selected US hospitals.
() Data collected from fewer than the CLSI documented M39 recommendation of 30 isolates.Microbiology Testing Schedule
Microbiology
CSF Gram Stain 45 minutes
Blood Culture 5 days to final negative
BCID on positive blood or broth culture 3 hours
Strep Only Culture 1 day to prelim, 48 hours
to final
Tissue or Aspirate Bacterial Culture 5-7 days to final negative
Urine Culture, Clean Catch 24 hours to final report
Urine Culture, Catheter 48 hours to final negative
Fungus Culture 4 weeks to final negative
Mycobacterial Culture 6 weeks to final negative
On-Demand Molecular Microbiology
C. trachomatis (CT)/N. gonorrheae (NG) PCR 24 hours
C. difficile PCR 3 hours
Gastrointestinal Pathogen Panel 3 hours
Influenza A and B PCR 3 hours (flu season only)
Meningitis/Encephalitis Pathogen PCR 3-5 hours
MRSA/SA PCR for NP Swabs 3 hours
MRSA/SA PCR SSTI for Musculoskeletal Specimens 3 hours
Respiratory Pathogen PCR 3 hours
Trichomonas spp. PCR 3 hours
Molecular Microbiology Batch Testing
Adenovirus PCR Monday, Wednesday and Thursday
CMV PCR Daily Monday -Friday
EBV PCR Daily Monday - Friday
Enterovirus PCR CSF 3 hours
All other sources batched once daily
HHV-6 PCR Monday, Wednesday and Thursday
HSV and VZV PCR Daily 7 days a week
Kingella PCR Daily (performed when MRSA/SAU neg,Multiplex PCR Panel Information
MEP (Meningitis/Encephalitis Pathogen Panel)
The Meningitis/Encephalitis Pathogen Panel tests for 14 pathogens associated with
meningitis/encephalitis. Testing is orderable in Epic for CSF by one of two avenues:
-Automatic MEP: CSF will be tested regardless of CSF cell count. Order is recommended if the
patient meets one of these criteria: patient is less than 2 months of age, patient has been diagnosed with
encephalitis, patient is immunocompromised, or test is approved by Infectious Disease or Neurology.
-Conditional MEP: CSF will only be tested if the CSF white cell count is greater or equal to 5. Order
is recommended for all patients not meeting the above requirements for automatic MEP.
Bacteria Viruses Yeast
Escherichia coli Cytomegalovirus Cryptococcus neoformans
Haemophilus influenzae Enterovirus
Listeria monocytogenes Herpes simplex virus 1, 2*
Neisseria meningitidis HHV6 DNA detected
Streptococcus agalactiae Parechovirus
Streptococcus pneumoniae Varicella-zoster virus
Positive results for any bacteria, Cryptococcus, HSV 1/2 or VZV are reported directly to the provider.
Positive results for CMV, enterovirus, HHV-6 or parechovirus are reported to Antimicrobial
Stewardship from 8am-5pm Monday-Friday and they relay the report to the clinician. On weekends,
holidays and outside of regular hours, the report is phoned directly to the clinician. Samples from
Network of Care (NOC) are sent to Children’s Anschutz Campus for processing.
*HSV PCR may be initially negative when sampling is performed early in disease course. Consider a
repeat spinal tap and HSV PCR if clinically indicated. When ordering MEP, do not order any single-
plex PCR (HSV PCR, ENTV PCR) on the same sample.
GIP (Gastrointestinal Pathogen Panel) with or without C. difficile Testing
The Gastrointestinal Pathogen Panel tests for 17 pathogens associated with infectious gastroenteritis.
The GIP can be ordered with or without C. difficile. Stool testing should not be performed on patients
who are receiving laxatives or who do not have evidence of diarrhea (> 3 Bristol scale= 6 or 7 stools in
24 hours). Positive GIP results for C. difficile are not reported on stools from children under a year of
age. Consider ordering Clostridium difficile PCR instead of GIP if C.difficile is the only clinical
concern in patients of any age. Samples from Network of Care (NOC) are sent to Children’s Anschutz
Campus for processing.
Bacteria Parasites Viruses
Campylobacter species Cryptosporidium species Adenovirus type 40/41
Clostridium difficile toxin Cyclospora cayetanesis Astrovirus
Plesiomonas shigelloides Entamoeba histolytica/dispar Norovirus
Salmonella species Giardia lamblia Rotavirus
Yersinia enterocolitica grp. Sapovirus
E.coli Shiga-like toxin Positive
E.coli 0157
Shigella species
Susceptibilities are performed and reported for Salmonella spp. and Shigella spp.
12RPP (Respiratory Pathogen Panel)
The Respiratory Pathogen Panel tests for 17 pathogens associated with infectious respiratory illness.
Samples from Network of Care are sent to Children’s Anschutz Campus for processing.
Viruses Bacteria
Rhinovirus/Enterovirus Parainfluenza 1-4 Mycoplasma pneumoniae
Human Metapneumovirus RSV Chlamydophila pneumoniae
Adenovirus Bordetella pertussis*
Influenza A (and H1 and H3 subtypes)
Influenza B (both clades detected)
Coronaviruses (HKU1, NL63, OC43, 229E)
* If concerned about pertussis, order Bordetella pertussis and Bordetella parapertussis specific PCR
tests.
BCID (Blood Culture Identification Panel)
The BCID panel tests for 24 pathogens and 3 antibiotic resistance genes associated with bloodstream
infections and is run automatically on all initial positive blood cultures.
Gram Positive Bacteria Gram Negative Bacteria Yeast
Enterococcus spp. Acinetobacter baumannii Candida albicans
Listeria monocytogenes Haemophilus influenzae Candida glabrata
Staphylococcus spp. Neisseria meningitidis Candida krusei
Staphylococcus aureus Pseudomonas aeruginosa Candida parapsilosis
Streptococcus spp. Enterobacteriaceae (Enteric bacteria) Candida tropicalis
Streptococcus agalactiae Enterobacter cloacae complex
Streptococcus pyogenes Esherichia coli
Streptococcus pneumoniae Klebsiella oxytoca
Klebsiella pneumoniae
Serratia marcescens
Antibiotic Resistance Genes, if positive resistance is present:
mecA – methicillin resistance
vanA/B – vancomycin resistance associated with VRE
KPC – one type of carbapenem resistance associated with high level resistance in gram negatives
Positive results are reported directly to Antimicrobial Stewardship from 8am-5pm, Monday-Friday and
they relay the report to the clinician. On weekends, holidays and outside regular hours, the report is
phoned directly to the clinician.
BCID is performed on positive broth cultures from sterile site aspirates and tissues .
Same panel that is run on positive blood cultures is also run on positive broth culture from sterile sites.
Testing is performed on the first initial positive broth culture.
13MSK (Musculoskeletal) PCR Panel
The MSK PCR Panel can be run on bone tissue, bone aspirate, synovial fluid, synovial tissue, and other
deep MSK aspirates from patients with suspicion for infection. Once regular microbiologic testing
(cultures) is processed samples will undergo the Cepheid MRSA/SA SSTI PCR assay which will detect
the presence of SA and MRSA (performed 7 days a week, 24 hours a day, with a 3-hour turnaround
time). If that is negative, for children < 5 years old, Kingella kingae PCR will be performed with
results available 2 pm the following day (Mon-Fri).
Culture Collection and Testing Information
Blood Cultures
If antibiotics will be started or changed, CHCO policy recommends collection of two blood cultures in
advance. Separately prepare the IV caps when drawing from a central line. Place each blood specimen
into a separate blood culture bottle. When followed correctly, this practice provides a better
interpretation, as organisms detected in one of two cultures are likely to be a normal skin flora
contaminant.
Select the type of bottle type based on the volume of blood to be drawn from the patient (Table 1).
Collect at least 1 mL of blood with at an additional 1 mL of blood for each year of age to a maximum
of 10 mL. Volumes of blood less than 1 mL are generally insufficient for the accurate exclusion of
bacteremia. Although we never reject a blood culture, the volume of blood is critical (more is better).
If collecting blood from patients with suspected endocarditis, 3 large volume blood cultures are best, up
to 10mL each.
Table 1: Blood Culture Quantities by Age
Minimum (mL)
Blood Culture Bottle
Age Per Each Blood
Type
Culture
0y (less than 1 y) 1 mL (Pink) BD Bactec Peds Plus
1y 2 mL (Pink) BD Bactec Peds Plus
2y 3 mL (Pink) BD Bactec Peds Plus
3y 4 mL (Blue) BD Bactec Plus
etc. etc. (Blue) BD Bactec Plus
9 y and older 10 mL (Blue) BD Bactec Plus
Anaerobic blood cultures are infrequently utilized in pediatric patients due to the rare incidence of
anaerobic bacteremia in our population. In cases of suspected Lemierre’s disease or bacteremia due to
deep wound infection or abscess, request an anaerobic blood culture bottle from the Microbiology
Laboratory.
Single isolates: Susceptibility testing is automatically performed on clinically significant isolates on all
patients from all sites. Isolates that are known contaminates from peripheral draws will have
susceptibilities performed only upon clinician request. The exception is Bone Marrow Transplant and
Hematology/Oncology patients. Susceptibilities are performed on these patients on all isolates from
any source.
14Multiple isolates recovered in succession: Susceptibility testing is performed automatically on the first
two isolates from blood and CSF cultures. Susceptibilities are repeated on isolates obtained from
positive cultures collected 4 days or more after the initial susceptibility test. The first three isolates are
frozen for future reference.
Culture Results
Check the computer for culture status and updated reports. If results are pending, the culture has not
been read or does not meet the criteria for a negative report (i.e. not incubated long enough). Most
negative reports are not issued before 18-24 hours. Network of Care Urgent Values are reported by
Epic Inbox.
C. trachomatis, N. gonorrhoeae and Trichomonas vaginalis PCR
Urine for C. trachomatis and N. gonorrhoeae PCR should be from the first part of the stream without
self-cleaning. Patient should not have urinated in the previous hour before collection. Clean
catch/midstream urines are acceptable when submitting for both urine culture and CT NG PCR.
CSF Cultures
Bacterial culture is performed on the first tube collected. Cell count is performed on tube #3.
Susceptibility testing automatically performed for CSF shunt or lumbar puncture specimens.
Cystic Fibrosis Cultures
Respiratory cultures from CF patients are a specific order. Upon isolation of glucose -non-fermenting
gram-negative rods including P. aeruginosa, susceptibilities by E-test method are performed for
inpatients. Extended incubation times may be required for mucoid and slow growing CF isolates.
HSV Testing
Complete testing for neonatal HSV includes collection of surface swabs (eye, throat, nasal and rectum),
lesion swab (if present), blood, and CSF for HSV PCR. CSF can be tested for HSV by MEP or HSV
PCR. Collect lesion/ulcer specimens using special swabs and viral transport medium obtained from
Microbiology. Unroof lesion if possible and send for HSV PCR. If scab is present, collect whole scab
in transport medium and order HSV PCR. Call Microbiology if antiviral susceptibility testing is
needed.
Tissues and Aspirates
Tissues and aspirates (not swabs) are the preferred diagnostic specimens fo r wound and tissue
infection. The quantity of specimen contained on a swab is usually insufficient for a good culture and
does not permit a Gram stain to be performed. Swabs also retain >70% of the bacteria collected so
cultures are compromised: Get fluid in a syringe if possible. For minute specimen volumes (may not
be visible in the syringe), inoculate a blood culture bottle using the aspiration needle directly, drawing
up liquid from bottle and injecting it back into the bottle to rinse contents of syringe into bottle.
Isolates recovered from swabs and other sources that are potentially contaminated with normal flora are
only tested for susceptibilities when one or two recognized pathogens are recovered. Please see the
Laboratory Test Directory for specific collection instructions for each test and swab type , if swab
cannot be avoided.
15Tissues and Aspirates - Anaerobic Cultures
Isolation of anaerobes requires special collection and transport techniques. Please call Micro biology
for appropriate media. Aspirates that are collected from a site that is adjacent to a mucous membrane
are not appropriate for anaerobic culture due to the presence of normal anaerobic flora at these sites.
Susceptibility testing for anaerobes is not available at Children’s Hospital Colorado although most
anaerobes have a predictable susceptibility pattern (see Table 7).
Respiratory Cultures (Tracheal Aspirates)
Susceptibilities are not routinely performed on isolates from tracheal aspirates. Susceptibilities will be
performed on recognized pathogens when a single organism is seen on Gram stain with few or more
polymorphonuclear cells or when a single or predominant organism grows in culture.
TB Sputum and Quantiferon collection
Collect induced sputum or gastric aspirate for TB testing early in the morning for three consecutive
mornings. Blood for Quantiferon testing must be collected following special collection instructions per
laboratory protocol. Specimens that arrive by 6 p.m. will be tested the following Tuesday, Thursday
and Friday.
Urine Cultures
Catheter specimens are preferred. Always exclude the first drops of urine. Avoid “clean catch” or bag
specimens for culture if urinary tract infection (UTI) is likely; especially if antibiotics are to be started.
Please refer to CHCO Clinical Care Guidelines for current recommendations for diagnosis of UTI.
“Clean Catch” or Bag urine cultures are most helpful when they are negative. Be aware that colony
counts may be < 100,000 cfu/mL in any age child with UTI if the specimen is not concentrated, and
that children may have true UTI with multiple organisms. A urine specific gra vity and nitrite test may
help interpret results. For “Catheter”, “Clean Catch” or “Bag” specimens, susceptibilities are
performed automatically on a single isolate with a colony count of 10,000 cfu/mL or greater;
susceptibilities on mixed cultures must be requested. Cotton ball samples are never appropriate for
clinical practice. Please refer to UTI Clinical Care Guideline for additional information.
Antimicrobial Susceptibility Testing
Antimicrobial Susceptibility Testing
Susceptibility testing is performed on significant isolates from the first positive culture from any
source. Additional positive cultures are referred to the first culture on the same or similar source for
three days. Organisms recovered four or more days later will be retested. MRSA, VRE and all
isolates recovered from blood, CSF, brain tissue or aspirate are frozen for future reference. All other
isolates are saved for 7 days before they are discarded.
Susceptibility testing, an important function of the Microbiology Laboratory, is expensive, time
consuming and not required for all isolates. Organisms that have predictable susceptibility patterns do
not require such testing and fastidious isolates may yield results that are difficult to interpret. Multiple
testing methods are utilized because all methods are not suitable for all isolates. The Microbiology
Laboratory has established protocols for testing and reporting of bacterial isolates c ommonly
encountered at CHCO to provide healthcare providers with reliable results. E-test MIC, Microscan
MIC, Sensititre MIC, Kirby Bauer Disk, PBP2A, D-test and Beta-lactamase are all methods utilized to
predict an organism’s antimicrobial susceptibility. CHCO adheres to Clinical and Laboratory
16Standards Institute (CLSI) guidelines for susceptibility testing and MICs are interpreted as susceptible,
intermediate and resistant per these guidelines. When choosing a drug for the treatment of an infection,
the site of infection and drug penetration to the site of infection must be considered. Pharmacists or
antimicrobial stewards should be consulted to answer questions re garding pharmacokinetics and
pharmacodynamics of drug-bug interactions.
CRE (Carbapenem Resistant Enterobacteriaceae) Confirmation
CRE are enteric Gram-negative rods that are carbapenem resistant. Different molecular mechanisms
can determine carbapenem resistance including production of a carbapenemase and/or p roduction of an
extended-spectrum Beta-lactamase (ESBL) and/or an AmpC Beta-lactamase in conjunction with
membrane impermeability or active drug efflux.
All enteric Gram-negative rods for which susceptibilities are performed are screened for carbapenem
resistance. Isolates with ertapenem, imipenem, and meropenem MICs in the intermediate or resistant
range are submitted to the CDPHE (Colorado Department of Health and Epidemiology) for screening
and confirmatory testing of carbapenemase production using molecular methods. Consult with
Epidemiology/Infection Control for isolation and Antimicrobial Stewardship and Infectious Disease for
treatment of these patients.
MRSA Confirmation
All S. aureus isolates are tested for vancomycin resistance. Detection of MRSA from a nasal swab
indicates colonization but does not imply systemic colonization. PBP2A Latex Detection, ChromAgar,
Microscan MIC, and cefoxitin screen are methods that the Microbiology Laboratory utilizes for MRSA
confirmation depending on the source.
VRE (Vancomycin Resistant Enterobacteriaceae) Confirmation
Vancomycin resistance in Enterococcus spp. isolates is mediated by van genes that encode enzymes
that modify the vancomycin binding target. Glycopeptide resistance in enterococci may be intrinsic or
acquired. Intrinsic vancomycin resistance is encoded by the vanC gene, which is found chromosomally
in Enterococcus gallinarum and Enterococcus casseliflavus. Intrinsic resistance typically produces
MICs of 2 – 32 mcg/mL for vancomycin, and these organisms are generally susceptible to ampicillin.
Organisms that display this low level intrinsic resistance mechanism are not particularly concerning
from an infection control standpoint and they are not considered to be vancomycin resistant enterococci
(VRE).
Acquired vancomycin resistance is encoded by the vanA and vanB genes and is found in E. faecalis, E.
faecium, and rarely in E. durans. Strains that harbor the vanA gene have high levels of resistance to
vancomycin and teicoplanin, whereas strains that harbor the vanB gene have variable levels of
resistance to vancomycin only. These organisms are true VRE and are an infection control concern
because the genes are transmitted between organisms on plasmids. This type of resistance is associated
with increased morbidity and mortality, particularly in immune-compromised patients.
Enterococcus spp. isolates that test resistant or intermediate to vancomycin by Microscan panel are re -
identified using Maldi-TOF. MICs to vancomycin are confirmed using the E-test method.
17Critical and Urgent Value Reporting Policy for Microbiology
Critical Values- The following critical results are phoned directly to the patient’s licensed caregiver
within 30 minutes for inpatients and within 60 minutes for outpatients:
1. Positive blood culture Gram stain report (first positive)
2. Positive CSF Gram stain report (first positive)
3. Positive CSF culture report (first positive)
4. Positive HSV PCR on CSF, blood or swab specimen from a neonate (first positive)
5. MEP positive for bacteria, Cryptococcus, HSV or VZV (first positive)
6. Positive Pneumocystis stain
Urgent Values- The following results are called to the patient’s licensed caregiver or nurse within 8
hours for inpatients or the next business day for outpatients (first positive stain, culture or PCR):
1. Blood or CSF culture definitive identification of isolate, including results of BCID
2. Subsequent CSF or Blood culture positives in a series
3. MEP positive for CMV, HHV6, enterovirus or parechovirus
4. Single organism isolated from a tissue, aspirate or surgical site or BCID on positive broth
5. Methicillin Resistant Staphylococcus aureus (MRSA) by culture or PCR (first positive)
6. Penicillin resistant Streptococcus pneumoniae
7. Vancomycin resistant Enterococcus faecalis, Enterococcus faecium, Enterococcus durans (VRE)
8. Drug Resistant Organism
9. Group A streptococcus throat or rectal (Network of Care and ED obtain reports via Epic In -box)
10. Group A streptococcus from non-throat or non-rectal sources are called to all sites
11. Fusobacterium spp. isolated from any site
12. GIP positive for Salmonella spp or, Shigella spp.in patients less than 6 months of age
13. GIP positive for E. coli 0157 or positive shiga-toxin
14. Legionella spp. isolated from any culture
15. Fungal mold isolates except CF sputa and dermatophytes
16. Mycobacterium spp.: positive stain for Acid-Fast Bacilli (AFB), Mycobacterium spp., first
positive culture, Mycobacterium tuberculosis detected/isolated
17. Positive test for syphilis (first positive)
18. Positive C. difficile PCR (first positive)
19. Positive N. gonorrhoeae or Chlamydia trachomatis PCR with confirmation requested or from a
CHIP patient
20. Positive B. pertussis or B. parapertussis PCR
21. Positive Enterovirus PCR
22. First positive CMV, EBV, Adenovirus, or HHV6 PCR
23. HSV PCR - non-CSF, Blood and subsequent positives
24. HSV or CMV detected by any method on any source from neonates19
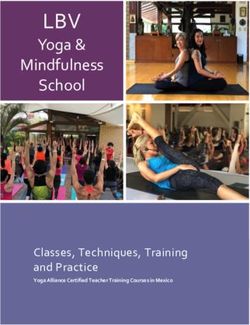
MRSA and VRE Rates Non-Surveillance Culture
Percent of all S. aureus that are identified as MRSA
Overall MRSA Rate
from Children's Patients
ED/NOC MRSA Rate
Inpatient MRSA Rate
60%
50%
40%
Rate
30%
20
20%
10%
0%
Year21
Influenza Virus Treatment
The viral neuraminidase inhibitors osteltamivir (Tamiflu®) is an FDA approved antiviral medication
currently available for the treatment or prophylaxis of influenza virus infections of children. Peramivir
(Rapivab ®) is a similar medication licensed only for treatment of patients 18 years old and older. The
neuraminidase inhibitors are active against influenza A and influenza B viruses. In the 2017-18
influenza season, almost all characterized influenza virus isolates were sensitive in vitro to these
medications.
When started within the first two days of onset of influenza illness, oseltamivir can reduce illness
severity and shorten the duration of fever and symptoms of uncomplicated influenza by an average of
1-2 days in healthy outpatients. These medications may also reduce the risk of serious influenza-
related complications (e.g., pneumonia, respiratory failure, exacerbation of chronic diseases and death).
When clinically indicated, oseltamivir should be started as soon as possible after symptom onse t,
ideally within 48 hours of symptom onset. Treatment should not wait for laboratory
confirmation of influenza. Many experts would start antiviral treatment for any child ill enough
to be hospitalized with a clinical diagnosis of influenza. Treatment started 4-5 days after symptom
onset may still be beneficial in preventing influenza-related complications and deaths in patients at
high risk of such complication or with severe or progressive influenza.
Duration of Treatment or Chemoprophylaxis
Treatment Recommended duration for antiviral treatment is 5
days.
Chemoprophylaxis Recommended duration is 7 days after exposure. For
control of outbreaks in long-term care facilities and
hospitals, CDC recommends antiviral
chemoprophylaxis for a minimum of 2 weeks,
included vaccinated persons, and up to 1 week after
the last known case was identified.
22Antiviral Medications Recommended for Treatment and Chemoprophylaxis of Influenza,
2017 – 2018 Influenza Season
FDA Not
Antiviral Activity
Use approved recommended Children Adults Adverse events
agent against
for for use in
Oseltamivir Influenza Treatment 2 weeks If < 1 yr old, the dose is 3 75 mg Adverse events:
(Tamiflu®) A and B and older mg/kg/dose twice daily. twice daily nausea, vomiting.
Transient
If > 1 yr old and weight 15 kg neuropsychiatric events
or less, the dose is 30 mg twice (self-injury or delirium)
a day; weight > 15 to 23 kg, the mainly reported among
dose is 45 mg twice a day; Japanese adolescents
weight > 23 to 40 kg, the dose and adults.
is 60 mg twice a day; more than
40 kg, the dose is 75 mg twice a
day.
Chemo- 1 yr and If child is < 3 months old, 75 mg once
prophylaxis older chemoprophylactic use is not daily
recommended unless situation
23
is judged critical because of
limited data on use in the age
group.
If child is 3 months - 1 year,
dose is 3 mg/kg once daily.
Greater than 1 yr:
weight 15 kg or less, the dose is
30 mg once daily;
weight > 15 to 23 kg, the dose
is 45 mg once daily;
weight > 23 to 40 kg, the dose
is 60 mg once daily;
more than 40 kg, the dose is 75
mg once daily.Antiviral Medications Recommended for Treatment and Chemoprophylaxis of Influenza,
2017 – 2018 Influenza Season
FDA Not
Antiviral Activity
Use approved recommended Children Adults Adverse events
agent against
for for use in
Peramivir Influenza Treatment 2 years Birth – 3 months, 6 – 10 600 mg IV Diarrhea, vomiting,
(Rapivab®) A and B and older mg/kg IV once daily; greater once daily neutropenia
than 3 months – 17 years, 10
mg/kg IV once daily
Zanamivir* Influenza Treatment 7 years People with 10 mg (2 inhalations) twice 10 mg (2 Allergic reactions:
(Relenza®) A and B and older underlying daily inhalations) oropharyngeal or facial
respiratory twice daily edema.
disease (e.g. (Not FDA approved for use Adverse events:
asthma, in children < 7 years old) diarrhea, nausea,
COPD) sinusitis, nasal signs
and symptoms,
bronchitis, cough,
headache, dizziness,
and ear, nose and throat
24
infections.
Chemo- 5 years 10 mg (2 inhalations) once 10 mg (2
prophylaxis and older daily inhalations)
once daily
*Not on CHCO (Not FDA approved for use
formulary in children < 5 years old)Guidelines for Changing from IV to PO Antibiotics in Hospitalized Children
Over 2 Months of Age at Children’s Hospital Colorado
CONSIDERATIONS / BASIC PRINCIPLES:
Advantages of an IV to PO conversion are to provide an oral or enteral dosage form with comparable
bioavailability to the intravenous form. This could reduce hospital length of stay and will avoid added
risks associated with continued intravenous therapy. This will lower the overall medication and
associated costs to the patient and the hospital.
PROTOCOL:
1) Antimicrobial Therapy
a) The following antimicrobials have an oral analogue with greater than or equal to 90%
bioavailability and may be switched at or after initiation of treatment:
i) Antimicrobials
• Rifampin
• Metronidazole
• Levofloxacin / ciprofloxacin*
• Clindamycin
• Linezolid
• Fluconazole
• Bactrim (sulfamethoxazole / trimethoprim) [dose based on trimethoprim]
* ciprofloxacin is 80% bioavailable
ii) Recommend changing from IV to PO if:
1) Clinically stable
2) Tolerating enteral nutrition by the oral, gastric, or other appropriate enteral tube
3) Tolerating other medications by the oral route
4) Medical and social situation will allow patient to comply with oral antibiotic therapy once
discharged from the hospital
iii) Consider continuing IV therapy if:
1) NPO including medications
2) Unable to tolerate oral formulation
3) Presence of vomiting or diarrhea in the previous 24 hours, gastrointestinal obstruction,
malabsorption syndrome, or ileus
4) Antimicrobial being used for bacteremia/line infection
5) Conversion to oral dose of clindamycin greater than 1.8 gm/day
6) Receiving continuous enteral feeds that cannot be interrupted and the antibiotic must be
given on an empty stomach
7) Severe Sepsis (with organ dysfunction)
8) CNS Infection, endovascular infection
9) Fever and Neutropenia
25b) Changing from IV to PO when there is LESS THAN 90% bioavailability. The following
related antimicrobial alternatives* may be switched after initial intravenous therapy once
the patient has met the following inclusion criteria and does not meet the following exclusion
criteria:
i) Recommend changing from IV to PO if:
1) Clinically stable
2) Tolerating enteral nutrition by the oral, gastric, or another appropriate enteral route
3) Tolerating other medications by the oral route
4) Signs, symptoms (fever, pain) and indicators of infection (CBC, ESR, CRP) have resolved
or are improving
5) Medical and social situation will allow patient to comply with oral antibiotic therapy once
discharged from the hospital
ii) Consider continuing IV therapy under the following circumstances:
1) NPO including medications
2) Unable to tolerate oral formulation
3) Presence of vomiting or diarrhea in the previous 24 hours, gastrointestinal obstruction,
malabsorption syndrome, or ileus
4) Antimicrobial being used for bacteremia/line infection
5) Receiving continuous enteral feeds that cannot be interrupted and the antibiotic must be
given on an empty stomach
6) Severe Sepsis (with organ dysfunction)
7) CNS infection or endovascular infection
8) Fever and Neutropenia
Intravenous Antibiotic Oral Alternative*
Cefotaxime, ceftriaxone **
Ampicillin Amoxicillin
Ampicillin / sulbactam Amoxicillin / clavulanic acid
Cefazolin Cephalexin
* Bacterial infections with a known organism and susceptibilities can help guide choosing a well
absorbed unrelated alternative.
** Oral 3 rd gen cephalosporins (i.e. cefdinir) are not well absorbed and do no t provide adequate step-
down therapy. Recommend oral amoxicillin or amoxicillin/clavulanate if sensitive. For PCN allergic,
may use cefuroxime or cefpodoxime; cefdinir has inferior serum levels.
26Children’s Hospital Colorado Antimicrobial Formulary
June 1, 2018
IV Oral Monitor DOSE Information
Antimicrobial
Formulations at
Oral Adjust for Bioavailability (Oral
Children’s Hospital IV Cost IV PO
Cost Food Alternatives)**
Colorado
Antivirals
ACYCLOVIR $$$ $ w/wo 10-20% R HSV encephalitis 3 months or Suppressive therapy for
less, 20 mg/kg/dose q8h; 4 mos neonates and recurrent
or greater, 10 mg/kg/dose qh8 herpes 20 mg/kg/dose TID
HSV/Varicella treatment: 20
mg/kg/dose QID
VZV treatment 20 mg/kg/dose
5 times daily (max 800
mg/dose)
27
Available dosage forms: 200
mg caps; 400, 800 mg tabs; 200
mg/6 mL susp
CIDOFOVIR $$$$$ R 5 mg/kg/dose q1-2 weeks; must
be given with probenecid
FOSCARNET $$$$ R CMV Treatment 60 mg/kg/dose
q8h or 90 mg/kg/dose q12h
Maintenance 90 – 120
mg/kg/dose q24h
GANICICLOVIR $$$ $$$ w 6 – 9% R, CBC CMV prophylaxis 5 mg/kg/dose
q24h
CMV treatment 5 mg/kg/dose
q12h
Neonatal CMV treatment 6
mg/kg/dose q12h
* refer to specific transplant
protocol for dosingIV Oral Monitor DOSE Information
Antimicrobial
Formulations at
Oral Adjust for Bioavailability (Oral
Children’s Hospital IV Cost IV PO
Cost Food Alternatives)**
Colorado
VALACYCLOVIR $$ w/wo 55% once R Treatment of HSV
converted to > 3months: 40-60 mg/kg/day
acyclovir divided TID (max 2000-3000mg
daily)
> 12 yrs: 40-60 mg/kg/day
divided BID-TID
Treatment of VZV
> 3 months: 60 mg/kg/day
divided TID (max 3000mg daily;
1000mg per dose)
Suppression of HSV
> 3months: 40-60 mg/kg/day
divided BID (max 1000mg per
day)
28
> 12 yrs: 40-60 mg/kg/day
divided daily or BID (max
1000mg per day)
VALGANCICLOVIR $$ w/wo 60% once R, CBC Treatment of CMV
converted to 15-18 mg/kg/dose BID (Max
ganciclovir 900 mg/dose)
Prophylaxis/suppression
15-18 mg/kg/dose Qday (Max
900 mg/dose)IV Oral Monitor DOSE Information
Antimicrobial
Formulations at
Oral Adjust for Bioavailability (Oral
Children’s Hospital IV Cost IV PO
Cost Food Alternatives)**
Colorado
Antifungals
AMPHOTERICIN B $$ See Azoles R, L 0.5 – 1 mg/kg/day q24h
DEOXYCHOLATE
AMPHOTERICIN B $$$$$ See Azoles R, L 3 – 5 mg/kg/day q24h, may use 7.5
LIPOSOME mg/kg/dose for lung infections,
doses as high as 10 mg/kg/dose
q24h have been used for CNS
infections
FLUCONAZOLE $$ $ – $$ w/wo 90% R, L Prophylaxis/oral thrush/urinary Prophylaxis/oral
tract 3 mg/kg/day; thrush/urinary tract 3
mg/kg/day
Oral candidiasis 3 – 6 mg/kg/day
Oral candidiasis 3 – 6
Candidemia 6 – 12 mg/kg/day mg/kg/day
Esophageal invasive disease Candidemia 6 – 12
(endocarditis/CNS/endoph mg/kg/day
thalmitis, etc) 10 – 12 mg/kg/day
29
Systemic 6 – 12 mg/kg/day Esophageal invasive
disease (endocarditis/
***all q24h dosing*** CNS/ endophthalmitis,
etc.) 10 – 12 mg/kg/day
Systemic 6 – 12
mg/kg/day
*** all q24h dosing***
Available dosage
forms: 25, 50, 100, 150,
200 mg tabs; 40 mg/mL
susp
ITRACONAZOLE $$$ w(caps) 55% L, TDM 3 – 10 mg/kg/day
wo(soln)
Available dosage
forms: 100 mg caps; 10
mg/mL solIV Oral Monitor DOSE Information
Antimicrobial
Formulations at
Oral Adjust for Bioavailability (Oral
Children’s Hospital IV Cost IV PO
Cost Food Alternatives)**
Colorado
MICAFUNGIN $$$$ See Azoles R, L, Prophylaxis
CBC, Less than 8 years old: 2mg/kg/day
TDM q24h (max 50mg/dose)
Greater than 8 years old: 1mg/kg/day
q 24 hours (max 50mg/dose)
Treatment:
less than 6 mos: 8 – 10 mg/kg/day
q24h
6 mos – 8 yrs: 4 mg/kg/day q24h
Greater than 8 yrs: 2-3 mg/kg/day
q24h
VORICONAZOLE $$$$$ $$$$ – wo 96% R, L, Adult: 12 mg/kg/day divided q12h x 12 years and older: > 40kg
$$$$$ CBC, 2 doses then 8 mg/kg/day divided 200 – 300 mg PO BID
TDM q12h
Neonate: 12 – 20 mg/kg/day
Neonate: 12 – 20 mg/kg/day divided divided q12h
q8 – 12h
Greater than 2 years: 18
30
Less than 2 yrs: 18 mg/kg/day mg/kg/day divided q12h
divided q12h
Available dosage forms:
Greater than 2 yrs: 18 mg/kg/day 50, 100, 200 mg tabs; 40
divided q12h mg/mL susp
POSACONAZOLE $$$$$ $$$$ – Liquid with Liquid (variable) R, L, Adult: 300 mg IV q24h 100 mg DR tab:
$$$$$ food Tablet (54-70%) CBC, Adult 300 mg po daily
TDM Children: 7 – 10 mg/kg/day has Children 7-10 mg/kg/day
been used
40 mg/ml Liquid:
Adult 400 mg BID or 200 mg
QID
Children 12 – 20 mg/kg/day
divided QID has been usedIV Oral Monitor DOSE Information
Antimicrobial
Formulations at
Oral Adjust for Bioavailability
Children’s Hospital IV Cost IV PO
Cost Food (Oral Alternatives)**
Colorado
Antibacterials
AMIKACIN $$ Check Susceptibilities R, TDM 7.5 mg/kg/dose q8h
GENTAMICIN $ Check Susceptibilities R, TDM Neonates: see formulary;
Children: 2.5 mg/kg/dose
q8h
TOBRAMYCIN $$ Check Susceptibilities R, TDM 2.5 mg/kg/dose q8h
AMOXICILLIN $ w/wo 89% R AOM 90 mg/kg/day divided BID
(preferred regimen for
CAP) CAP 90 mg/kg/day divided TID
UTI 25-50 mg/kg/day divided TID
Strep throat 50 mg/kg/day divided BID
or Qday
Available dosage forms: 250, 500 mg
caps; 250, 400 chewable; 875 mg tab
31
AMOXICILLIN- $$ w/wo 89% R High dose formulation:
CLAVULANATE
CAP 90 mg/kg/day divided
TID
AOM 90 mg/kg/day divided BID
Available dosage forms: 600-42.9
mg/5 mL susp, 875-125 mg tabs
Regular formulation:
UTI 25-50 mg/kg/day divided TID
Available dosage forms: 200-28.5,
250-62.5, 400-57 mL susp; chewable
tabs; 250-125, 500-125 tabsIV Oral Monitor DOSE Information
Antimicrobial
Formulations at
Oral Adjust for Bioavailability (Oral
Children’s Hospital IV Cost IV PO
Cost Food Alternatives)**
Colorado
Antibacterials
AMPICILLIN- $$$ See Check Susceptibilities R UTI 100 – 200 mg/kg/day divided q6h
SULBACTAM Amox/
Clav Bacteremia/CAP/SSTI 200 mg/kg/day
divided q6h
Meningitis 200 – 400 mg/kg/day
divided q4 – 6h (max 2gm/dose)
NAFCILLIN $$$ See Check Susceptibilities R, CBC, Moderate infection 50 – 100
Cephalexin UA mg/kg/day divided q6h
Diclox
Severe 100 – 200 mg/kg/day divided q4
– 6h (max dose 2 gm/dose)
Can infuse as continuous infusion (200
mg/kg/day max 10gm /day)
PENICILLIN G $ See Pen R Mild to moderate infections 100,000
Potassium V to 250,000 units/kg/24 hours in divided
doses every 4 – 6 hours;
32
Severe infections Up to 400,000
units/kg/24 hours in divided doses ever
4 – 6 hours (max dose 24 million
units/24 hours)
PENICILLIN G $$$ See Pen R (For IM Administration ONLY)
BENZATHINE V Group A streptococcal upper
600000 UNIT/ML respiratory infection
IM SUSP (For IM 25,000 units/kg as a single dose;
Administration maximum 1.2 million units;
Only)
Prophylaxis of recurrent rheumatic
fever 25,000 units/kg every 3 – 4
weeks; maximum: 1.2 million units per
dose
Syphilis – please refer to CDC
recommendations for dosing and
duration.IV Oral Monitor DOSE Information
Antimicrobial
Formulations at
Oral Adjust Bioavailability (Oral
Children’s Hospital IV Cost IV PO
Cost for Food Alternatives)**
Colorado
PENICILLIN V $ wo 25 – 60% R 25 – 50 mg/kg/24 hrs divided every 6
POTASSIUM – 8 hrs (max 500 mg/dose)
Available dosage forms: 125, 250,
500 mg tabs; 250 mg/5 mL susp
PIPERACILLIN- $$$$$ Check R, L Dose based on piperacillin: 240
TAZOBACTAM Susceptibilities – 400 mg/kg/day (max 4
gm/dose) divided 6-8 hrs
Cephalosporins
First Generation
CEFAZOLIN $$ See Check R 50 – 150 mg/kg/day divided q6-
SODIUM Ceph- Susceptibilities 8h (max 2 gm/dose, 6 gm/day)
alexin
Diclox
CEPHALEXIN $ w/wo 90% R General dosing 50 mg/kg/day
divided QID
Osteo 100 -150 divided QID (max
1gm/dose)
33
Available dosage forms: 250, 500
mg caps; 250 mg/5 mL susp
Second Generation
CEFOXITIN $$$ R Neonates: 90 – 100 mg/kg/day
divided q8h
Children: 160 mg/kg/day
divided q4 – 6h (max 2
gm/dose)
CEFUROXIME SODIUM $$$ $$ w/wo 37 – 52% R 75 -150 mg/kg/day divided q8h 20 – 30 mg/kg/day divided BID (max
(tabs) (max 2 gm/dose) 500 mg/dose)
w(susp)
Available dosage forms: 62.5, 125,
250, 500 mg tab; 125 mg/5 mL suspIV Oral Monitor DOSE Information
Antimicrobial
Formulations at
Oral Adjust for Bioavailability (Oral
Children’s Hospital IV Cost IV PO
Cost Food Alternatives)**
Colorado
Third Generation
CEFOTAXIME $$$ Check Susceptibilities R General dosing 100-200 mg/kg/day
divided q6 – 8h
Meningitis 200 – 300 mg/kg/day
divided q6 (max 2 gm/dose)
CEFTRIAXONE $$ Check Susceptibilities General dosing 50 – 75 mg/kg/day
divided q12 – 24
Meningitis and osteo 100
mg/kg/day divided q12 – 24h (max 2
gm/dose)
CEFIXIME $$$ w/wo 40 – 50% R 8 mg/kg/day in 1 – 2
divided doses (max 400
mg/day)
Available dosage forms:
100, 200, 400 mg tabs; 100
mg/5 mL susp
34
CEFTAZIDIME $$$ Check Susceptibilities R 100 – 150 mg/kg/day divided q8h
(max 2 gm/dose)
CEFTAZIDIME- $$$ Check Susceptibilities R 100-150 mg/kg/day divided q8h (max
AVIBACTAM 2 gm/dose)
Fourth Generation
CEFEPIME HCL INJ $$$ Check Susceptibilities R 100 mg/kg/day divided q12h
F&N and serious infections 150
mg/kg/day divided q8h (max 2
gm/dose)
Fifth Generation
CEFTAROLINE $$$ Check Susceptibilities R Infants 2 months to under 6
months of age: 10 mg/kg/dose
every 8 hours
Infants (6 months of age and
older), Children, Adolescents: 15
mg/kg/dose (max: 600 mg per dose)
every 8 hoursIV Oral Monitor DOSE Information
Antimicrobial
Formulations at
Oral Adjust for Bioavailability (Oral
Children’s Hospital IV Cost IV PO
Cost Food Alternatives)**
Colorado
CEFTOLOZANE- $$$ Check Susceptibilities R General Dosing: 20 to 40
TAZOBACTAM mg/kg/dose (based on ceftolozane
component) IV q 8 hours, max dose
of 2000 mg of ceftolozane
Cystic Fibrosis and VAP/HAP:
40 mg/kg/dose (based on ceftolozane
component) IV q 8 hours, max dose
of 2000 mg of ceftolozane
Carbapenems
MEROPENEM $$$ Check R, L, Moderate infection 60 mg/kg/day
Susceptibilities CBC divided q8h (max 1 gm/dose);
Meningitis 120 mg/kg/day divided
q8h (max 2gm/dose)
Macrolide/Azalides
35
AZITHROMYCIN $ w/wo 38% 10 mg/kg/day q24h (max 500 mg) 10 mg/kg/day, day 1 (max
500 mg), then 5 mg/kg/day
(max 250 mg)
Campylobacter and
shigellosis 10 mg/kg/day x
3 days
Salmonella (enteric
fever/typhoid)
10mg/kg/day X 5-7 days
Available dosage forms:
125, 250 mg tabs; 200
mg/5 mL suspYou can also read