Appendectomy Hospital Stay: No Difference in Obese Adult or Pediatric Patient Length of Stay Compared to Nonobese Patients
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ORIGINAL RESEARCH Ochsner Journal 21:14–18, 2021 ©2021 by the author(s); Creative Commons Attribution License (CC BY) DOI: 10.31486/toj.19.0116 Appendectomy Hospital Stay: No Difference in Obese Adult or Pediatric Patient Length of Stay Compared to Nonobese Patients Eric Lorio, MD,1 David H. Ballard, MD,2 Elizabeth Guarisco, MD,1 James Hughes, MD,3 Forrest D. Griffen, MD,4 Navdeep S. Samra, MD, FACS4 1 Department of Internal Medicine, University of Texas Health Science Center at San Antonio, San Antonio, TX 2 Department of Radiology, Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, MO 3 Department of Anesthesiology, West Virginia University, Morgantown, WV 4 Department of Surgery, Louisiana State University School of Medicine–Shreveport, Shreveport, LA Background: Studies of adult and pediatric patients undergoing appendectomy have reported variable outcomes and operative metrics related to the effect of obesity. The purpose of this study was to investigate the effect of obesity in adult and pediatric patients undergoing appendectomy at our institution. Methods: This single-center retrospective study evaluated the relationship between length of hospital stay for appendectomy and body mass index (BMI). Data obtained from the electronic medical record included age, sex, weight, height, BMI, the number of hours the patient experienced symptoms prior to presentation to the emergency room, the number of hours the patient was admitted prior to surgery, the number of hours of hospital admission after surgery, perforated appendix, preoperative comorbidi- ties, and evidence of preoperative sepsis. Results: During the 3-year study period, 118 adults and 38 children who underwent appendectomy composed the study groups. Patients were stratified by obese and nonobese, with obesity defined as BMI ࣙ30.0 kg/m2 . In adults, we found no significant differ- ence between length of stay in obese (n=45) and nonobese (n=73) patients (79.6 ± 65.5 hours vs 101.6 ± 123.0 hours; P=0.21). In children, we found no significant difference between length of stay in obese (n=9) and nonobese (n=29) patients (92.9 ± 64.6 hours vs 109.0 ± 93.5 hours; P=0.54). Conclusion: Obesity did not affect length of stay in adults and children who underwent appendectomy in the present series. Keywords: Appendectomy, body mass index, inpatients, length of stay, obesity, postoperative complications Address correspondence to Navdeep S. Samra, MD, FACS, Department of Surgery, Louisiana State University School of Medicine–Shreveport, 1501 Kings Hwy., Shreveport, LA 71130. Tel: (318) 675-6355. Email: nsamra@lsuhsc.edu INTRODUCTION found that obesity was associated with increased comor- Appendectomy is one of the most common surgical pro- bid illness and with significantly longer intensive care unit cedures worldwide, whether performed for management of and hospital LOS.3 However, in a cohort of 272 patients acute appendicitis or as an addition to a larger abdomi- who underwent appendectomy, no significant differences nal surgery.1 In the United States, approximately 200,000 were found in postoperative recovery, appendix perforation appendectomies are performed annually.1 As such, patients status, or mortality between obese and nonobese patients, undergoing appendectomy represent a sizable proportion and Towfigh et al recommended no change in appendici- of the general surgery patient population, and obesity may tis management for obese patients.4 A study of a large be an important factor in determining patient morbidity national pediatric database that compared patients who related to appendectomy performed for management of underwent appendectomy to patients undergoing other acute appendicitis. intestinal operations showed that obese appendectomy Albeit not specific to appendectomy, studies suggest that pediatric patients had significantly longer hospital LOS high body mass index (BMI) is positively associated with compared nonobese patients, but no significant difference in-hospital mortality and increased length of stay (LOS).2,3 in LOS was seen between obese and nonobese patients Akinyemiju et al concluded that higher BMI was associated undergoing other intestinal operations.5 Other studies have with increased risk of mortality and longer hospital stay in reported worse outcomes in obese adults and longer oper- a cohort of more than 800,000 patients admitted for various ating times in obese adults and children.6-8 The purpose of medical and cancer-related diagnoses.2 Similarly, Lewis et al this study was to investigate the effect of obesity in adult 14 Ochsner Journal
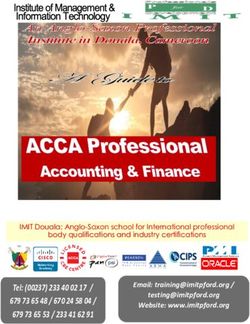
Lorio, E Figure. Length of stay factors including hours admitted after surgery, hours admitted prior to surgery, duration of symptoms prior to hospital arrival, and overall length of stay in the adult patients compared to the pediatric patients in the study cohort. Upper bars show pediatric data; lower bars show adult data. and pediatric patients undergoing appendectomy at our darily, controlling for the potential confounders of BMI, sex, institution. age, and number of comorbidities. P values
Appendectomy Outcomes in Obese Patients
Table 1. Adult Patient Characteristics, Overall and by Body Mass Index (BMI) Classification
Nonobese, Obese,
All Patients, BMI 0.05 in all comparisons). Comparing 0.05 in all comparisons) between obese and nonobese pediatric patients (P=0.54)
between obese and nonobese patients. However, duration (Table 2). Stratifying all patients—obese and nonobese—
of inpatient admission preoperatively was 11.3 hours longer who received 0.05 in all comparisons).
Pediatric Patients DISCUSSION
We identified 38 pediatric patients who had appendec- In this study, we found no difference in LOS between
tomies during the study period, 23 males (61%) and 15 obese and nonobese patients receiving appendectomy in
females (39%) with a mean age of 9 years (Table 3). Nine either the adult or pediatric subgroup. Secondary obser-
patients (24%) were obese. Most pediatric patients had vations included (1) a significantly higher incidence of
no comorbidities (76%). A greater percentage of the pedi- obese adult female patients vs obese adult male patients
atric patients had a perforated appendix (26%) compared to (P=0.012), (2) an increased length of inpatient hospital-
adults (15%). ization preoperatively in adult patients with comorbidities
We observed a significant difference in the duration of when controlling for all variables (P=0.015), and (3) a sig-
experiencing symptoms before presentation to the emer- nificant difference between the obese and the nonobese
gency department (P=0.015), with the obese population pre- pediatric patients in the duration of experiencing symp-
senting after a mean of 28.1 hours of symptoms and the toms before presentation to the emergency department
nonobese population presenting at a mean of 62.3 hours. We (P=0.015).
found no significant difference in the number of hours a pedi- The high proportion of adult obese female patients in part
atric patient spent admitted preoperatively (P=0.25) or post- may reflect the rising incidence of female obesity in the
operatively (P=0.78) between obese and nonobese patients. United States.10 Although Ballard et al did not investigate
Table 2. Hospital Length of Stay (LOS) in Adult (n=118) and Pediatric (n=38) Patients by Body Mass Index (BMI) Classification
Nonobese, BMILorio, E
Table 3. Pediatric Patient Characteristics, Overall and by Body Mass Index (BMI) Classification
Nonobese, Obese,
All Patients, BMIAppendectomy Outcomes in Obese Patients
5. Witt CE, Goldin AB, Vavilala MS, Rivara FP. Effect of body mass (sepsis-3). JAMA. 2016;315(8):801-810.
index percentile on pediatric gastrointestinal surgery doi: 10.1001/jama.2016.0287
outcomes. J Pediatr Surg. 2016;51(9):1473-1479. 10. Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL.
doi: 10.1016/j.jpedsurg.2016.02.085 Trends in obesity among adults in the United States, 2005 to
6. Garey CL, Laituri CA, Little DC, Ostlie DJ, St Peter SD. Outcomes 2014. JAMA. 2016;315(21):2284-2291.
of perforated appendicitis in obese and nonobese children. doi: 10.1001/jama.2016.6458
J Pediatr Surg. 2011;46(12):2346-2348. 11. Ballard DH, Raptis CA, Guerra J, et al. Preoperative CT findings
doi: 10.1016/j.jpedsurg.2011.09.024 and interobserver reliability of Fournier gangrene. AJR Am J
7. Knott EM, Gasior AC, Holcomb GWIII, Ostlie DJ, St Peter SD. Roentgenol. 2018;211(5):1051-1057. doi: 10.2214/AJR.18.19683
Impact of body habitus on single-site laparoscopic 12. Deugarte DA, Stark R, Kaji AH, Yaghoubian A, Tolan A, Lee SL.
appendectomy for nonperforated appendicitis: subset analysis Obesity does not impact outcomes for appendicitis. Am Surg.
from a prospective, randomized trial. J Laparoendosc Adv Surg 2012;78(2):254-257.
Tech A. 2012;22(4):404-407. doi: 10.1089/lap.2012.0056 13. Lee SL, Stark R, Yaghoubian A, Shekherdimian S, Kaji A. Does
8. Michailidou M, Sacco Casamassima MG, Goldstein SD, et al. The age affect the outcomes and management of pediatric
impact of obesity on laparoscopic appendectomy: results from appendicitis? J Pediatr Surg. 2011;46(12):2342-2345.
the ACS National Surgical Quality Improvement Program doi: 10.1016/j.jpedsurg.2011.09.030
pediatric database. J Pediatr Surg. 2015;50(11):1880-1884. 14. Blanco FC, Sandler AD, Nadler EP. Increased incidence of
doi: 10.1016/j.jpedsurg.2015.07.005 perforated appendicitis in children with obesity. Clin Pediatr
9. Singer M, Deutschman CS, Seymour CW, et al. The third (Phila). 2012;51(10):928-932. doi: 10.1177/0009922812441659
international consensus definitions for sepsis and septic shock
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical
Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
©2021 by the author(s); licensee Ochsner Journal, Ochsner Clinic Foundation, New Orleans, LA. This article is an open
access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license
(creativecommons.org/licenses/by/4.0/legalcode) that permits unrestricted use, distribution, and reproduction in
any medium, provided the original author(s) and source are credited.
18 Ochsner JournalYou can also read