An opinion of why HIV is disproportionately high in sub-Saharan Africa - Open ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Trends in Medicine
Opinion ISSN: 1594-2848
An opinion of why HIV is disproportionately high in sub-
Saharan Africa
Jiman He
Liver Research Center, Brown University, Providence, United States
The prevalence of HIV infection is disproportionately high in Thus, high infection rates among young children (especially girls)
Sub-Saharan Africa (SSA), and the reasons are largely unknown. are an important reason why HIV prevalence is disproportionately high
After a decades-long fight, HIV infection is still one of the deadliest in SSA. The infected girls would infect their male counterparts after
diseases. Since the time from infection to death is certain, this paper entering sexually active ages. The infected males further infect females,
analyzed HIV/AIDS mortality data to explore why HIV prevalence is and so on. However, strategies for HIV prevention have focused on
disproportionately high in SSA. adults, adolescents, and new borns.
Mortality data Having multiple sexual partners is a high-risk factor for HIV
transmission. A positive individual can infect his/her multiple sexual
The guidelines state that: HIV transmission is mainly through partners, and each infected partner further pass their infection on to
sexual intercourse; children acquire HIV mainly from infected mothers their partners and so on. Although having multiple sexual partners is
in utero, during delivery, or while being breastfed [1,2]; and that, “the common both in SSA and in western countries, HIV effectively jumps
time between HIV transmission and an AIDS diagnosis is usually 10-15 from adults to children in SSA, but not in Western countries.
years” in the absence of treatment [3,4]. According to these guidelines,
infections usually start appearing among 15-19, and 20-24 year-olds; Unfortunately, there were few studies exploring HIV infections
and without treatment, these infected youth would usually die after occurring during childhood before the widespread use of HAAT. The
age 25 and 30, respectively. This is exactly what is shown in Figure limited existing data were usually based on medical records. However,
1a which represents the United States census data on HIV mortality children infected during childhood rarely had symptoms that required
[5]. As shown, before 1997 when highly active antiretroviral therapy hospital visits. Moreover, in SSA, many infected mothers did not want
to test their children, because of fearing stigma, discrimination, and the
(HAAT) began, deaths among 15-24 year-olds were low, and increased
revelation to their partners. Therefore, our knowledge of HIV infections
dramatically in 25-34 year-olds. Similar observations occurred in other
occurring during childhood before 2000 were very limited. Infections
Western countries [6,7].
among children had been decreasing since late 1990s. However, it is
However, mortality data from SSA in 1990s or earlier were very difficult to know by how much infections occurring during childhood
different [8-11]. Figure 1b shows the national registered deaths due to have declined, due to aforementioned limits. Our analysis of mortality
HIV in Zimbabwe in 1993 [8]. There were substantial deaths in 15-19 data was a novel attempt to examine childhood infections.
year-old women and 20-24 year-old men, and very high deaths in 20-
Data after 2000
24 year-old women. These young people were unlikely to have been
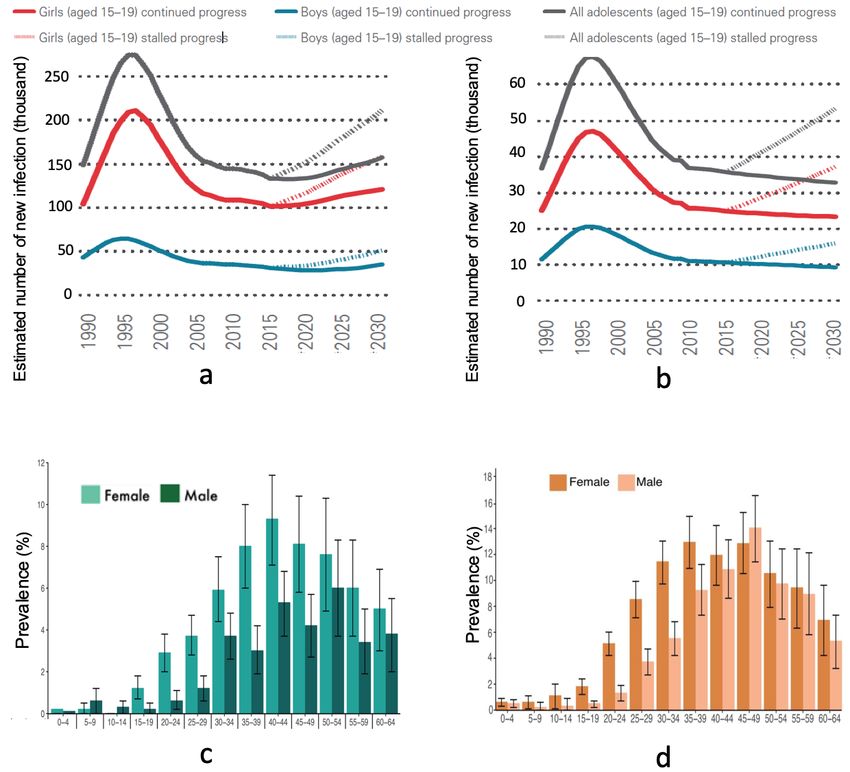
infected at ages 15-24; as, few young people who were infected at ages Extensive studies were made on adolescents ages 15-19. Figures 2a
15-24 died at ages 15-24. They were also unlikely to have been infected and 2b shows the dramatic decrease in annual new infections among
in utero, or during delivery or breastfeeding; because, absent effective adolescents ages 15-19 that, curiously occurred in Southern/Eastern
treatment, 80% infected during these stages would have died by age 5 and Western/Central SSA during 1997-2004 and stalled thereafter [13].
[12]. Therefore, these young people would mainly have obtained HIV Whether these adolescents acquired HIV during childhood or during
during childhood. According to Figure 1b, infection rate in childhood between ages 15-19, and how many in each period, was not known.
was quite high. According to the general prevention guidelines, the infections usually
occurred during age 15-19 due to sex. However, the following data
We have not found age-specific HIV mortality data collected in suggest potential different explanation.
1990s in Asia, South America and Eastern Europe. But it is well known
that a high rate of deaths due to HIV/AIDS among young people was a very Attitudes about HIV infection (e.g. fearing stigma, etc.) changed
unique observation in SSA. We did not analyze mortality data collected a lot thanks to HAAT. Early treatment of HAAT is important to
after 2000; because HAAT greatly prolonged infected peoples’ lives.
Children: An important reason
HIV transmission among young people entering sexually active *Correspondence to: Jiman He, Liver Research Center, Brown University,
ages in SSA began at prevalence levels dozens of times higher than in Providence, United States, E-mail: hejee99@yahoo.com; Jiman_he@brown.edu
Western countries. If children in Western countries had similar HIV
Key words: HIV, mortality, childhood, risk factor, oral bleeding
prevalence rates as children in SSA, HIV prevalence among adults
would be comparable to that in SSA. Received: April 17, 2021; Accepted: May 15, 2021; Published: May 18, 2021
Trends Med, 2021 doi: 10.15761/TiM.1000278 Volume 21: 1-4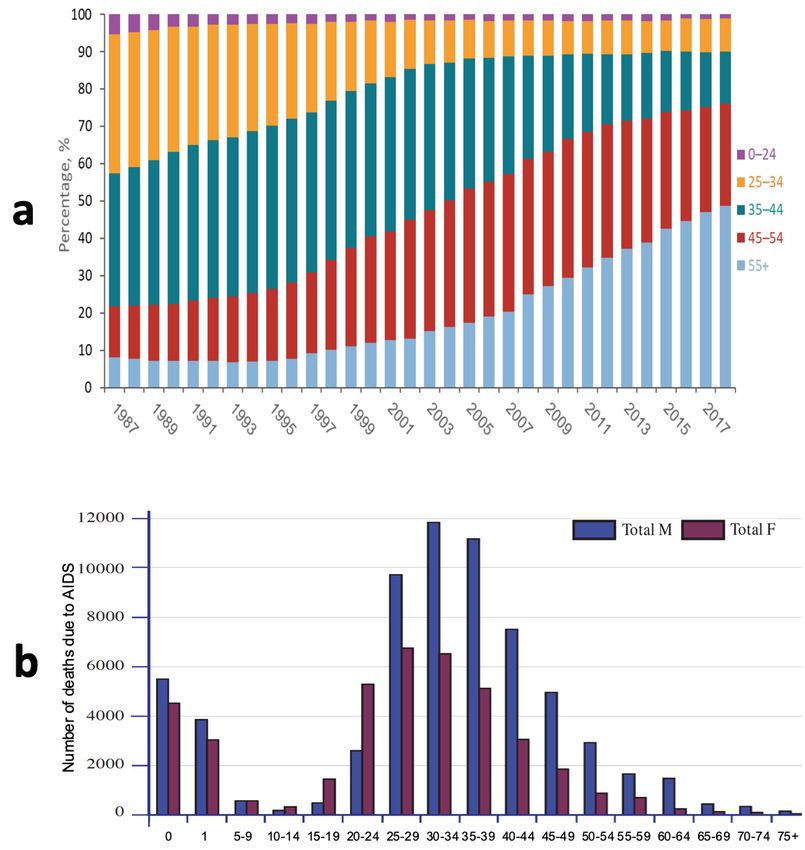
Jiman He (2021) An opinion of why HIV is disproportionately high in sub-Saharan Africa Figure 1. a) Percentage distribution of death with HIV infection, 1987-2018, United States. Source: CDC [5]. b) Age distribution of total death, Zimbabwe, 1995. Source: Dorrington et al. [8] Figure 2. a & b) Annual new HIV infections among adolescents ages 15-19. Source: UNAIDS [13]. c) Age specific HIV prevalence. Cameroon. 2016-2017. Source: Cameroon [16]. d) Age specific HIV prevalence. Uganda. 2016-2017. Source: Uganda [15] Trends Med, 2021 doi: 10.15761/TiM.1000278 Volume 21: 2-4
Jiman He (2021) An opinion of why HIV is disproportionately high in sub-Saharan Africa
infected people. These factors made studies among children much and 2011-2014, there was no correlation between the two factors from
more reliable. We then examined available age-specific data. A big 2009-2011 and 2014-2019 [26]. All these suggest that, exposure of oral
international project was launched in 15 high-burden HIV countries mucosa to blood of infected people may be one of the significant risk
in recent years [14]. Except for 2 countries with unavailable data, factors.
and 2 without children, 11 countries’ data included young children.
Children in SSA are often exposed to such blood. A common
Except for Rwanda, Tanzania, and Uganda (Figure 2d) [15], in 8
eating habit in SSA is sharing food, cups, etc. SSA was one of the
countries (Lesotho, Namibia, Malawi, Zimbabwe, Zambia, Cameroon,
most impoverished regions in the world. Traces of food left out by
Kenya, and Swaziland) (Figure 2c) [16], HIV prevalence increased
parents could easily be consumed by hungry children. Girls would be
in males ages 5-14, but increased little for ages 15-19 and 20-24. We
hungrier, because of gender inequality. Girls were required to care for
did not see the expected robust increase in HIV prevalence in people
their diseased elders, thus, were more likely exposed to blood through
ages 15-19 and 20-24 who became sexually active. These data clearly
aforementioned activities. In some of Asian countries, although these
suggest potential problems with the current understanding of HIV
observations are also common, having multiple sexual partners is
transmission. Although HIV prevalence increased dramatically among
much less common due to many reasons (e.g., religion, culture, etc.).
women ages 20-24, there was a considerable increase among girls ages
1-14 (Figure 2c, 2d). Moreover, if the patter in 1990s is similar to shown From high transmission among adults, to effective jumps to
in Figure 2c and 2d, there would unlikely be a dramatic increase in children, creates a continuous flow for effective amplification of HIV
deaths for ages 20-24 (Figure 1b), given that of the 10-year delay from in SSA. After generations of effective amplification, HIV prevalence
infection to death. became very high in SSA. In the rest of the world, such a flow was
limited at various points.
How does HIV jump from adults to children?
How does HIV jump from adults to children? A meta-analysis
Conclusion
study reported sexual abuse of girls was highest (20%-22%) in High rates of HIV infection among young children is an important
Australia, Africa and North America [17]. HIV prevalence among reason for the disproportionately high prevalence of HIV infection in
girls in Australia and North America were low despite high childhood SSA. Studies are urgently needed to examine family history (especially
sexual abuse rates, suggesting that, sexual abuse contributed to only before 2000) to explore whether many young people aged 15-24 got
a limited portion of infections among girls in SSA. Blood perfusion infected from their parents during childhood, for example, comparing
and careless medical use of syringes likely also contributed to a limited HIV prevalence between the parents of HIV positive and negative
number; because infection rates among older adults were low despite young pregnant women attending antenatal clinics.
greater likelihood of being exposed to the two factors. Injection drug References
use was not relevant for young children.
1. UNAIDS. HIV modes of transmission model. http://files.unaids.org/en/media/unaids/
contentassets/documents/countryreport/2010/201011_MOT_DominicanRepublic_
We recently reported that, current guidelines on HIV risk factors en.pdf.
are in conflict with each other over whether exposure of oral mucosa
2. UNAIDS. A review of HIV transmission through breastfeeding. http://data.unaids.org/
to blood is a risk of transmission [18]. This issue is important; because, publications/irc-pub03/jc180-hiv-infantfeeding-3_en.pdf.
30-80% of infected people have at least one oral manifestation [19],
3. WHO. HIV/AIDS. http://www.who.int/features/qa/71/en/. Accessed on March 21,
with the most frequently occurring ones often bleeding [20–22]. Family 2021.
members can be exposed to the blood in multiple ways. For example,
4. UNAIDS. Fast facts about HIV. http://data.unaids.org/pub/factsheet/2008/20080519_
kissing between partners leads to oral exposure. There is often blood fastfacts_hiv_en.pdf.
on food, cups and dishes used by infected people, which expose others
5. United States, CDC. HIV mortality 2018. https://www.cdc.gov/hiv/pdf/library/
who share them. In common practice, touching HIV+ blood without slidesets/cdc-hiv-surveillance-mortality-2018.pdf.
gloves is prohibited. No studies have shown that mucosa provides
6. National Centre in HIV Epidemiology and Clinical Research. Australian HIV
stronger protection than skin against HIV infection. Estimations surveillance report. April, 1995. https://kirby.unsw.edu.au/sites/default/files/kirby/
of dental occupational accidents data established that, the risk of report/SERP_v11n2-1995APR-Aust-HIV-Surv-Report.pdf.
HIV transmission per exposure was quite high (0.09%) [23]; studies 7. Simmons RD, Ciancio BC, Kall MM, Rice BD, Delpech VC (2013) Ten‐year mortality
in monkeys showed that the risk of oral exposure to HIV was very trends among persons diagnosed with HIV infection in England and Wales in the era of
antiretroviral therapy: AIDS remains a silent killer. HIV Med 14: 596-604.
high [24,25]. We recently also reported that, decline in annual new
HIV infections among children (age 0-9) in SSA over the past two 8. Dorrington R, Bourne D, Bradshaw D, Laubsher R, Timaus IM (2001) The impact
of HIV/ AIDS on adult mortality in South Africa. South African Medical Research
decades was closely correlated with an increase in the proportion of Council. 2001. https://www.researchgate.net/publication/221943220_The_impact_of_
women aware of their HIV status, suggesting that mothers’ behavioral HIVAIDS_on_adult_mortality_in_South_Africa.
change due to awareness of their HIV status played an important role 9. Ntozi JPM, Lubaale YMA, Nakanaabi IM (1997) AIDS mortality in Uganda:
in prevention of mother-to-child transmission [26]. Women aware of circumstances, factors and impact of death. Health Transition Review 7: 207-224.
their HIV status would be cautious with their activities to protect their 10. National Burden of Disease Steering Committee (1999) Analysis of the 1995 death
children, for example, avoiding kissing, sharing of spoons, cups, food, certification records. Zimbabwe Burden of Disease Study, Report 1. Harare, Zimbabwe.
etc. which lead to less exposure of their children to their blood. Anti- 11. Ngom P, Clark S. Adult mortality in the era of HIV/AIDS: sub-Sahran Africa.
retroviral therapy is often claimed to be the reason for the decline in Workshop on HIV/AIDS and adult mortality in developing countries. 2003. New
YorK. UN/POP/MORT/2003/3.
mother-to-children transmission over the past decades. Although the
data did show a close correction between the decline in annual new 12. UNICEF. UNICEF follow-up to the recommendations and decisions of the thirty-ninth
and fortieth Joint United Nations Programme on HIV/AIDS Programme Coordinating
HIV infections among children and the increase in the percentage of Board meetings. https://www.unicef.org/spanish/about/execboard/files/2018-EB2-
pregnant women receiving antiretroviral therapy between 2005-2009 HIV-AIDS-2017.12.12-EN.pdf.
Trends Med, 2021 doi: 10.15761/TiM.1000278 Volume 21: 3-4Jiman He (2021) An opinion of why HIV is disproportionately high in sub-Saharan Africa
13. UNICEF. For every child end aids, seventh stocktaking report, 2016. 21. Saravani S, Nosratzehi T, Mir S (2017) Oral manifestations and related factors of HIV
positive patients in south-east of Iran. J Dent Mater Tech 6: 11-18.
14. https://www.unicef.org/media/49751/file/Children_and_AIDS_Seventh_Stocktaking_
Report_2016_EN.pdf. 22. Coogan MM, Greenspan J, Challacombe SJ (2005) Oral lesions in infection with human
immunodeficiency virus. Bulletin of the World Health Organization 83: 700-706.
15. PHIA project. https://phia.icap.columbia.edu/about/.
23. Sen S, Mandal S, Bhattacharya S, Halder S, Bhaumik R (2010) Oral manifestations
16. Ministry of Health, Uganda. UGANDA POPULATION-BASED HIV IMPACT
in human immunodeficiency virus infected patients. Indian J Dermatol 55: 116-118.
ASSESSMENT (UPHIA) 2016-2017. https://phia.icap.columbia.edu/wp-content/
uploads/2020/02/UPHIA_Final_Report_Revise_07.11.2019_Final_for-web.pdf. 24. United States Public Health Service. Updated US Public Health Service guidelines
17. Ministry of Health, Cameroon. UGANDA POPULATION-BASED HIV IMPACT for the management of occupational exposures to human immunodeficiency virus and
ASSESSMENT (UPHIA) 2016-2017. https://phia.icap.columbia.edu/wp-content/ recommendations for postexposure prophylaxis.
uploads/2021/04/53059-CAMPHIA-Report_EN_Web_V4.pdf. 25. Stahl-Hennig C, Steinman RM, Tenner-Racz K, Pope M, Stolte N, et al. (1999) Rapid
18. Stoltenborgh M, Van Ijzendoorn Mh, Euser EM, Bakermans Kranenburg MJ (2011) A infection of oral mucosal-associated lymphoid tissue with simian immunodeficiency
global perspective on child sexual abuse: meta-analysis of prevalence around the world. virus. Science 285: 126-125.
Child Maltreat 16: 79-101.
26. Baba TW, Trichel AM, An L, Liska V, Martin LN, et al. (1996) Infection and AIDS in
19. He J (2020) Guidelines on risk ractors for HIV transmission are conflicting. World adult macaques after nontraumatic oral exposure to cell-free SIV. Science 272: 1486-
Journal of AIDS 10: 195-199. 1489.
20. Saini R (2011) Oral lesions: a true clinical indicator in human immunodeficiency virus. 27. He J (2021) Role of mothers’ awareness of HIV status in prevention of mother-to-child
J Nat Sci Biol Med 2: 145-150. transmission. J Adv Med Med Res 33: 77-81.
Copyright: ©2021 Jiman He. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution, and reproduction in any medium, provided the original author and source are credited.
Trends Med, 2021 doi: 10.15761/TiM.1000278 Volume 21: 4-4You can also read

















































