An Experimental Test of the Theory of Planned Behavior
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
APPLIED PSYCHOLOGY: HEALTH AND WELL-BEING, 2009, 1 (2), 257–270
doi:10.1111/j.1758-0854.2009.01013.x
An Experimental Test of the Theory of
Planned Behavior
Falko Sniehotta*
University of Aberdeen, UK
The Theory of Planned Behavior (TPB) is one of the leading theories of health
behavior, yet supporting evidence is exclusively based on correlational research.
This study aims to test the TPB experimentally. N = 579 participants were
randomised to receive persuasive messages addressing salient beliefs elicited
in a pilot study, following a 2*2*2 factorial design. Participants were
randomised to a behavioral-belief-intervention (BBI) or not, a normative-
belief-intervention (NBI) or not, and a control-belief-intervention (CBI) or not.
The primary outcome was objectively recorded attendance at university sports
facilities over 2 months; and the secondary outcomes were post-intervention
TPB measures. Main effects of the BBI on attitudes and of the NBI on subjec-
tive norm, PBC, attitudes, and intentions were found. The CBI did not alter
post-intervention cognitions, but was the only intervention to change behavior
not mediated by cognitions. While the findings support the TPB’s assumptions
on intention formation, behavior change results are not in line with the theory
and therefore further question the TPB’s leading role in behavioral science.
Keywords: physical activity participation, randomised trial, theory
development, Theory of Planned Behavior
INTRODUCTION
Developing the science of behavior change is paramount for health psychol-
ogy. Behavior plays an increasingly important role in the prevention and
management of chronic disease. To date, the main causes of mortality and
morbidity in the US and the developed world are behaviors such as poor diet,
physical inactivity, smoking, and alcohol abuse (Mokdad, Marks, Stroup, &
Gerberding, 2004). Effective behavioral interventions addressing today’s key
health challenges should be based on tested scientific theory, rather than on
researchers’ and practitioners’ common sense and intuition (Campbell et al.,
2000; Rothman, 2004; Michie & Abraham, 2004).
* Address for correspondence: Falko Sniehotta, University of Aberdeen, School of Psychol-
ogy, William Guild Building, Aberdeen AB24 2UB, UK. Email: f.sniehotta@abdn.ac.uk
© 2009 The Author. Journal compilation © 2009 International Association of Applied
Psychology. Published by Blackwell Publishing Ltd., 9600 Garsington Road, Oxford OX4 2DQ,
UK and 350 Main Street, Malden, MA 02148, USA.258 SNIEHOTTA The Theory of Planned Behavior (TPB; Ajzen, 1991) is among the leading theories used to predict a range of health behaviors, such as physical activity (Armitage, 2005; Eng & Martin Ginis, 2007; Johnston et al., 2007), eating (Conner, Norman, & Bell, 2002), and other health behaviors (Kiene, Tennen, & Armeli, 2008; van den Berg et al., 2008). The TPB is a social cognition model that proposes that behavior is a linear function of behavioral inten- tions and perceived behavioral control (PBC), the perception of individual control over performing the behavior. Intentions, in turn, are assumed to be a linear function of three types of cognitions: Attitude (positive or negative evaluation of the behavior), subjective norm (perceived approval of perform- ing the behavior), and PBC. Attitudes, subjective norm, and PBC are based on a set of more specific salient behavioral, normative, and control beliefs that reflect perceived outcomes associated with the target behavior (behav- ioral beliefs), approval of important others (normative beliefs), and barriers and facilitators (control beliefs) (Ajzen, 1991; Sutton, 2002). Over the last three decades, researchers have conducted hundreds of studies applying and testing the TPB with regard to an array of social and health behaviors (Armitage & Conner, 2001; Noar & Zimmerman, 2005). This research is still dominated by “shortitudinal” research designs with very short follow-up periods and by self-reported measures of behavior. This body of research has not stimulated changes or development of the theory, i.e. the evidence found did not convince the scientific community to modify, extend, or abandon the TPB. This may be interpreted as an indication that the theory is either very successful, or that the research conducted testing this theory has been lacking rigor. The current evidence base for the TPB is dominated by between- participant correlational studies (Noar & Zimmerman, 2005; Weinstein, 2007). These studies show that behavioral intention and PBC are indeed predictive of behavior, accounting for about 28 per cent of its variance (Armitage & Conner, 2001; Hagger, Chatzisarantis & Biddle, 2002; Sheeran, 2002). Surprisingly, rigorous tests of the theory from randomised experimen- tal studies have been remarkably rare. A systematic review of studies apply- ing the TPB to develop and test behavior change interventions found a lack of studies systematically using the TPB to develop interventions and very little evidence for their effectiveness (Hardeman et al., 2002). Since Hard- eman’s review, some additional studies have been published testing the effects of interventions developed based on the TPB; for example, Stead and colle- ages found in a non-randomised longitudinal cohort study in Scotland that the introduction of their intervention to reduce speeding was associated with improved attitudes and affective beliefs (Stead, Tagg, MacKintosh, & Douglas, 2005). More recently, the ProActive UK study showed that seden- tary older adults with a parental history of type 2 diabetes randomly assigned to an intensive 1-year behavior change intervention program based on an © 2009 The Author. Journal compilation © 2009 International Association of Applied Psychology.
TEST OF THE THEORY OF PLANNED BEHAVIOR 259 extended TPB, delivered either face to face or via the telephone, did not show higher levels of objectively measured physical activity than participants in a measurement only control group (Kinmonth et al., 2008). Chatzisarantis and Hagger (2005) tested two persuasive communications targeting salient vs. non-salient behavioral beliefs about physical activity among young people. While the intervention targeting salient behavioral beliefs improved attitudes as hypothesised, this effect did not translate into significant differences in intention and behavior. This is in line with Webb and Sheeran’s (2006) findings that interventions that are successful in changing behavioral inten- tions result in effects on behavior which are much smaller in effect size than those on intentions. To provide a more stringent test of the TPB, full-factorial randomised studies are needed that test independent effects of manipulating behavioral, normative, and control beliefs, and use appropriate randomisation, sufficient sample sizes, and thoroughly developed interventions (Sutton, 2002; Wein- stein, 2007). The rationale for behavioral interventions within the TPB is to address and modify the salient beliefs underlying attitudes, subjective norms, and PBC, i.e. the most prevalent behavioral, normative, and control beliefs, hypothesised to affect attitudes, subjective norms, and PBC, and, in turn, intentions and, eventually, behavior (Ajzen, 2006). To our knowledge, no study has tested the TPB using a full-factorial experimental design. McCarty (1981) tested the precursor of the TPB, Fish- bein’s (1967) Theory of Reasoned Action, using an orthogonal experimental design aiming to independently manipulate attitudes and subjective norms using persuasive messages about contraceptive use. These interventions, however, failed to affect the immediate targets, attitudes and subjective norms. Thus the study does not provide evidence supporting the theory. Aims and Hypotheses This study provides the first full-factorial experimental test of the TPB using a 2 (behavioral belief (BB) intervention vs. control) * 2 (normative belief (NB) intervention vs. control) * (2 control belief (CB) intervention vs. control) factorial design with post-intervention measure of TPB cognitions, an addi- tional no-measurement control group to control for possible effects of this measurement, and an objective record of the outcome behavior over 2 months following the intervention. A physical activity behavior was chosen as the outcome to reflect the vast correlational evidence for the TPB in predicting physical activity behaviors (Hagger et al., 2002). It was hypoth- esised that (1a) the BB intervention will change attitudes, (1b) the NB inter- vention will change subjective norms, and (1c) the CB intervention PBC, (2) the interventions that successfully changed cognitions will also modify © 2009 The Author. Journal compilation © 2009 International Association of Applied Psychology.
260 SNIEHOTTA
intentions, and (3) the BB, NB, and CB interventions will increase behavior
and that this effect will be mediated by effects on intentions.
METHODS
Design
Participants were randomly assigned following a 2 (behavioral belief inter-
vention vs. no intervention) * 2 (normative belief intervention vs. no inter-
vention) * (2 control belief intervention vs. no CB intervention) factorial
design with immediate post-intervention measurement of TPB cognitions and
subsequent objective recording of behavior.
Participants
Participants (N = 579; mean age 23.2 years, SD = 7.6; n = 382, 66% women)
were undergraduate students of a Scottish campus university participating in
a university-based online survey about physical activity and lifestyle behav-
iors at the beginning of the academic year (September/October 2007) prior to
randomisation.
Interventions
Interventions consisted of brief, online-delivered persuasive communications
providing information and addressing salient behavioral, normative, and
control beliefs identified in a previous belief elicitation study with 52 under-
graduate students of the same university with varying levels of physical
activity (diversity sampling), using a standard interview protocol (Ajzen,
2006; Francis et al., 2004).
All intervention components were introduced as follows:
We are interested in learning what factors are relevant for your decision to use
the university’s sport and recreation services or not. Based on feedback from
previous studies we have compiled a couple of statements summarising infor-
mation about the services and we would ask you to tell us to what degree you
were already aware of this information and how important this information is
for your decision to use the sport and recreation services or not (link to webpage
of S&R services).
For each type of belief, four brief paragraphs were presented providing
persuasive information addressing salient behavioral, normative, or control
beliefs elicited in the pilot study, respectively. Where possible, reference was
made to previous findings from the ongoing survey about students’ physical
activity and lifestyle behaviors.
© 2009 The Author. Journal compilation © 2009 International Association of Applied
Psychology.TEST OF THE THEORY OF PLANNED BEHAVIOR 261 The behavioral belief intervention emphasised: (a) the positive effects of regular physical activity on health, fitness, mood, stress, and ability, (b) that students attending the S&R (Sports and Recreation) services are more likely to be physically active and to maintain physical activity over the term time than students who do not attend the program (based on previous evidence from a larger ongoing study), (c) the safety and low injury risk of physical activity in the S&R facilities due to induction, monitoring, and availability of trained support, and (d) the wide range of exercise classes and individual activities (i.e. swimming, fitness suite, squash, etc.) and the flexibility of the timetable with a website that allows one to tailor the program to one’s fitness level, interests, and availability. The normative belief intervention emphasised: (a) that most students report that not having somebody to actively participate in physical activity with them is a major barrier to becoming more physically active. Students who attend the S&R services find that they meet people who do approve, support, and participate with them in physical activity which creates the necessary level of social approval and support, (b) that most friends and family actually approve of involvement in physical activity which is safe, secure, and healthy, (c) that misperceptions about others’ disapproval for involvement in regular physical activity often comes down to competing expectations about the time spent for oneself rather than disapproval for the activity, and that participants in the pilot study felt that this could often be turned into approval by explicitly talking to important others and addressing potential time conflicts together, and (d) that perceptions of regular S&R users as fit, well-trained super-athletes who look down on regular people trying to get fitter are far from reality and that the users of the services are a cross-section of the university community. The control belief intervention addressed the four key barriers to participa- tion found in the initial pilot study: (a) costs: our pilot studies have shown that students generally overestimate the costs for admittance. We therefore provided information about the actual costs of GBP£1.60 (approx. USD$2.65) for a single visit and GBP£82 (approx USD$135) for an annual membership for students to address this barrier, (b) time: students’ main concern of not having enough time was addressed by emphasising the long and flexible opening hours that allow students to schedule sessions before, between, and/or after their lectures, or over lunchtime, or choose from over 35 classes each week throughout the day, every day, using the services website as well as the possibility of combining socialising with physical activities, (c) access: ease of access was emphasised and information about locations, parking, and public transport from the university’s remote hospital campus were provided, and (d) feelings of discomfort and embarrassment about exercising in public were addressed. This issue came up frequently in the pilot study and showed that the idea about the typical user of the facilities is often quite biased. © 2009 The Author. Journal compilation © 2009 International Association of Applied Psychology.
262 SNIEHOTTA
TABLE 1
Bivariate Correlations between Post-Intervention TPB Measures
and Attendance Records, Means, Standard Deviations, Range and
Cronbach’s Alphas
1 2 3 4 5
1. Attitude .56** .63** .75** .22**
2. Subjective norm .61** .67** .19**
3. PBC .79** .31**
4. Intention .34**
5. Attendance
Cronbach’s alpha .95 .78 .90 .95 –
Mean (SD) 5.46 (1.44) 5.10 (1.52) 4.75 (1.64) 4.97 (1.87) 1.05 (2.15)
Range 1–7 1–7 1–7 1–7 0–9
In order to facilitate elaboration of the persuasive messages, two questions
were asked following each paragraph: (1) Were you aware of this information?
(answer scale: yes/no) and (2) How important is this information for your
decision to personally use the S&R facilities? (Not important at all (1)–very
important (7)).
Control Measures
Attitudes, subjective norms, PBC, and behavioral intention were measured at
baseline to perform manipulation checks and mediation analyses using a
validated physical activity-based TPB questionnaire by Armitage (2005). The
behavior reference in each item was modified to “participate in the univer-
sity’s sports and recreation program throughout the next two months” to
optimise correspondence between predictors and behavioral measure (Ajzen,
2006). Means, standard deviations, ranges, and Cronbach’s alphas are
displayed in Table 1.
Outcomes
Primary outcome was the number of weeks that participants attended the
university’s sport and recreation facilities over 2 months between baseline
measurement and the university’s 2007 Christmas break, based on objective
attendance records. As the primary outcome measure is based on objective
records, no attrition was encountered. Students are required to swipe their
student ID cards to get access to S&R facilities.
Randomisation
Participants were randomly assigned to receive the BB intervention or not, to
receive the NB intervention or not, and to receive the CB intervention or not
© 2009 The Author. Journal compilation © 2009 International Association of Applied
Psychology.TEST OF THE THEORY OF PLANNED BEHAVIOR 263
following a 2*2*2 factorial design. Randomisation occurred after completing
a general health-related online questionnaire using a pearl script integrated
into the online questionnaire.
Blinding
Double-blinded randomised trial: Participants were unaware that the study
would include assignment to groups. Assessment of baseline measures was
blinded by online measurement and outcomes were measured objectively.
Ethical Approval
The study received ethical approval from the School of Psychology Ethical
Review Board at the University of Aberdeen.
Statistical Methods
Data were analysed using SPSS 16. Possible intervention effects on control
measures and outcomes were tested using analyses of variance (ANOVAs)
based on intention-to-treat analyses. Relationships between post-
intervention TPB measures and subsequent records of S&R attendance were
tested using linear regression analyses.
RESULTS
Table 1 shows bivariate correlations between post-intervention TPB mea-
sures and attendance records as well as means, standard deviations, and
Cronbach’s alphas. Generally, social cognitions towards using the sports and
recreation facilities were positive (above the mean of the 1–7 scales). Atten-
dance measures showed a mean of 1.05 weeks attended throughout the study
period. All post-intervention TPB variables showed significant intercorrela-
tions with large effects and moderate to large correlations with attendance,
with the highest correlations of r = .34, p < .001 for intentions and r = .31,
p < .001 for PBC. Using linear regression analyses, behavioral intentions were
accurately predicted by attitude (b = .37; p < .001), subjective norm (b = .20;
p < .001), and PBC (b = .43; p < .001) accounting for 75.5 per cent of variance
in intentions. Post-intervention TPB measures were predictive of attendance
over the following 2 months, with intention (b = .27; p < .001), but not PBC
(b = .10; p = .14), significantly contributing to the prediction (R2 = .124;
R2adjusted = .121; p < .001). This is in line with meta-analytical reviews of TPB–
behavior relationships in which the predictive power is lower for objective
outcome measures and longer follow-up periods (Hagger et al., 2002).
© 2009 The Author. Journal compilation © 2009 International Association of Applied
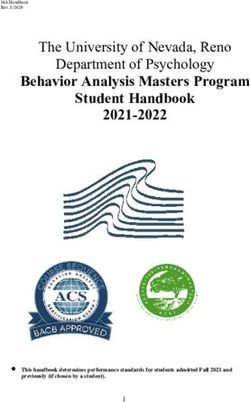
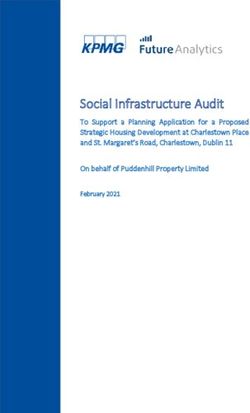
Psychology.264 SNIEHOTTA Adding attitude and subjective norm to the equation did not improve the prediction. Randomisation Checks (Effects on TPB Measures) Participants allocated to the behavioral belief intervention showed more favorable attitudes towards using the sport and recreation facilities (F(1, 530) = 6.05; p = .014; h2 = .011). Estimated marginal mean attitude for the behavioral belief condition was 5.59 (SE = .09) vs. 5.28 (SE = .09) for controls on a scale ranging from 1 to 7. No main effect of the control belief intervention was found (F(1, 530) = .295; ns) and the normative belief inter- vention approached significance (F(1, 530) = 3.69; p = .055) (Figure 1a). Neither of the two-way interactions nor the three-way interaction was significant. The normative belief intervention successfully manipulated subjective norms (F(1, 531) = 4.43; p = .036; h2 = .008), estimated marginal mean subjective norms was 5.22 (SE = .10) for the normative belief intervention and 4.94 (SE = .09) for controls (Figure 1b). While neither the control belief intervention (F(1, 531) = .08; ns) nor the behavioral belief intervention affected subjective norms (F(1, 531) = 1.53; ns), an unexpected interaction between the behavioral belief and the control belief interventions reached significance (F(1, 531) = 4.97; p = .026; h2 = .009), showing that the attitude intervention increased subjective norm in the absence of the PBC interven- tion. No other interaction was significant. PBC was not affected by the intervention addressing control beliefs (F(1, 533) = .06; ns). However, the normative belief intervention had a positive main effect on PBC (F(1, 533) = 5.08; p = .025; h2 = .010); estimated marginal mean PBC was 4.89 (SE = .10) for the normative belief condition and 4.58 (SE = .98) for controls. No other main or interaction effects were found. Behavioral intentions were significantly improved by the intervention addressing normative beliefs (F(1, 531) = 10.67; p < .001; h2 = .020; estimated marginal mean NB = 5.23 (SE = .12), estimated marginal mean con- trols = 4.71 (SE = .11)). No other effect reached significance. In conclusion, manipulation checks show that the interventions successfully manipulated all TPB measures including intentions. Effects on Primary Outcome The full-factorial ANOVA for the primary outcome, attendance to the sport and recreation services, showed a small main effect of the control belief intervention on attendance (F(1, 576) = 4.03; p = .045; h2 = .007). Participants attended the services an average of 1.22 (SE = .13) weeks in the past 2 months, whereas controls attended 0.86 (SE = .13) weeks (Figure 2). The © 2009 The Author. Journal compilation © 2009 International Association of Applied Psychology.
TEST OF THE THEORY OF PLANNED BEHAVIOR 265 FIGURE 1 a. Post-intervention Theory of Planned Behavior measures for participants assigned to the behavioral belief intervention vs. controls; b. Post-intervention Theory of Planned Behavior measures for participants assigned to the normative belief intervention vs. controls. interventions focusing on normative beliefs (F(1, 576) = 2.00; p = .16) and behavioral beliefs (F(1, 576) = .15; p = .70) as well as the two-way and three- way interactions were not significant. Mediation Analyses The effect of the normative belief intervention on intentions was partially mediated by subjective norms and PBC. An ANCOVA of the intervention effects on behavioral intentions shows that the main effect on intention remains significant (F(1, 529) = 3.87; p = .049) even after subjective norms (F(1, 529) = 95.63; p < .001) and PBC (F(1, 529) = 272.51; p < .001), both measures modified by the NB intervention, are controlled for as covariates. All other effects were not significant. © 2009 The Author. Journal compilation © 2009 International Association of Applied Psychology.
266 SNIEHOTTA
FIGURE 2. Mean weeks attended the sport and recreation facilities in the 2
months following intervention for participants assigned to the control belief
intervention vs. controls.
The control belief intervention was the only intervention to affect the
behavioral outcome. As the control belief intervention did not affect cogni-
tive TPB measures and, in turn, the normative belief and behavioral belief
interventions’ success in affecting TPB cognitions were unsuccessful in chang-
ing behavior, the conditions for mediation analyses were not fulfilled (Baron
& Kenny, 1986). The TPB measures did not mediate the intervention effect
on behavior.
DISCUSSION
This study conducted the first full-factorial experimental test of the TPB
using post-intervention assessment of TPB cognitions and objectively
recorded behavioral outcome measures over a meaningful time period
following the interventions. The three brief persuasive communications to
address modal salient behavioral, normative, and control beliefs were devel-
oped based on standard procedures within the TPB, including a prior belief
elicitation study using a standard protocol (Ajzen, 2006). These brief inter-
ventions, delivered online as part of a survey, resulted in small changes in
cognitions related to the use of the university’s sport and recreation facilities.
Both attitudes and subjective norms were successfully increased by the inter-
ventions addressing the respective behavioral and normative beliefs. PBC was
also manipulated, but not as hypothesised by the control belief intervention
but rather by the subjective norm intervention. This may reflect the proposed
overlapping nature of TPB cognitions, supported by an abundance of studies
showing that they are highly correlated (Armitage & Conner, 2001). Beliefs
© 2009 The Author. Journal compilation © 2009 International Association of Applied
Psychology.TEST OF THE THEORY OF PLANNED BEHAVIOR 267 elicited by questions about social approval might also bring up issues that have implications for the controllability and ease of performing a behavior. For instance, in our pilot study, questions eliciting both normative and control beliefs brought up beliefs about social disapproval from stereotypical users of sports services (e.g. lean, muscular, athletic) serving as a social barrier to participation, causing social embarrassment of new users perceiv- ing themselves as less in shape. This might explain the unexpected side effect of the subjective norm intervention. The question of the discriminant con- struct validity (Pollard, Johnston, & Dieppe, 2006) of interventions is a challenge to social cognition models that will need addressing in the future. All three TPB predictors of behavioral intentions were manipulated by the interventions. The normative belief intervention increased intentions, which was partly mediated by changes in subjective norm and PBC. These effects, therefore, confirm the TPB’s assumptions regarding intention formation. However, the effect of the normative belief intervention on intention did not translate into an effect on behavior. Instead, the control belief intervention had a small significant effect, increasing attendance behavior. This is in line with evidence that interventions targeting control or self-efficacy beliefs are effective in changing behavior directly (Bandura, 1997). It has also previously been shown that interventions targeting behavioral control beliefs may influ- ence behavior without affecting self-report measures of control beliefs (Johnston et al., 2007). It is also possible that the effect might have been mediated by more specific control beliefs than those measured in the present study (Rodgers, Murray, Courneya, Bell, & Harber, 2009). All effect sizes were very small. This partly reflects the challenge of changing cognitions about physical activity behaviors and service use among well- informed students who will likely have formed stable beliefs prior to entering the study. However, it also indicates that the proposed procedures for inter- vention development within the TPB (Ajzen, 2006) and the prevalent research traditions associated with the theory do not provide effective tools and tech- niques to change cognitions (Sniehotta, 2009). For example, the effectiveness of persuasive messages on behavior change is very limited (Hillsdon, Foster, Cavill, Crombie, & Naidoo, 2005). Thus, theories explicitly incorporating behavior change techniques such as Social Learning Theory (Bandura, 1986) are more useful for theory testing and intervention design. This study shows that small changes in cognitions do not lead to behavior change; it is possible that large changes in cognitions do (cf. Webb & Sheeran, 2006). However, the TPB provides no guidance on how to achieve such large changes in cognitions. In contrast to the experimental findings, regression of intention and behav- ior on post-intervention TPB measures confirms TPB assumptions that atti- tudes, subjective norms, and PBC are highly (cross-sectionally) predictive of intentions, and PBC and intention (in our study only intentions) are predictive of behavior. While these predictive findings are well in line with existing © 2009 The Author. Journal compilation © 2009 International Association of Applied Psychology.
268 SNIEHOTTA
evidence (Armitage & Conner, 2001; Sheeran, 2002), they are misleading
because the experimental findings in the same study suggest that the TPB does
not explain behavior (see Weinstein, 2007). This study suggests that TPB
assumptions do not stand up to experimental tests, despite strong predictive
effects using correlational approaches. While the changes in intention found
in this study are in line with TPB assumptions, the theory does not account for
the findings on behavior change found in this experimental study. This limits
the TPB’s potential to contribute to the science of behavior change.
So what is wrong with the TPB? The theory’s various conceptual problems
have been discussed (Ogden, 2003; Sniehotta, 2009). The key shortcomings
from an experimental and behavior change point of view are that (a) the
theory does not specify techniques to modify hypothesised cognitive deter-
minants of intention and behavior, (b) possible changes in beliefs will be
attenuated through the hypothesised causal chain of events from beliefs, to
intention, to behavior caused by the imperfect empirical relationships
between these variables, and (c) the TPB does not account for intention–
behavior discrepancies (Sniehotta, 2009). Thus, the Theory of Planned
Behavior is neither about planning, as it does not address how people trans-
late their intention into behavior, nor an accurate theory of behavior
(Schwarzer, 2008; Sniehotta, Scholz, & Schwarzer, 2005). While future
research is needed to confirm these findings, it calls into serious question the
leading role of the TPB in the health psychology literature.
It is time for a new research agenda to be set, aimed at testing and devel-
oping theories of health behavior by using more rigorous tests and designs
(Weinstein, 2007) and setting criteria for abandoning theories which fail these
tests (West, 2005).
ACKNOWLEDGEMENTS
The author would like to thank Silje Skår for her support in conducting this
study, Justin Presseau for proofreading the manuscript, and Vera Araújo-
Soares and Justin Presseau for helpful comments on a previous version of this
manuscript.
REFERENCES
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human
Decision Processes, 50, 179–211.
Ajzen, I. (2006). Designing a TPB questionnaire. Retrieved 10 October 2008 from
http://people.umass.edu/aizen/pdf/tpb.measurement.pdf.
Armitage, C.J. (2005). Can the theory of planned behaviour predict the maintenance
of physical activity? Health Psychology, 24, 235–245.
Armitage, C.J., & Conner, M. (2001). Efficacy of the theory of planned behaviour: A
meta-analytic review. British Journal of Social Psychology, 40, 471–499.
© 2009 The Author. Journal compilation © 2009 International Association of Applied
Psychology.TEST OF THE THEORY OF PLANNED BEHAVIOR 269 Bandura, A. (1986). Social foundations of thought and action. Englewood Cliffs, NJ: Prentice Hall. Bandura, A. (1997). Self-efficacy: The exercise of control. New York: W.H. Freeman. Baron, R.M., & Kenny, D.A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173–1182. Campbell, M., Fitzpatrick, R., Haines, A., Kinmonth, A.L., Sandercock, P., Spiegelhalter, D. et al. (2000). Framework for design and evaluation of complex interventions to improve health. British Medical Journal, 321, 694–696. Chatzisarantis, N., & Hagger, M. (2005). Effects of a brief intervention based on the theory of planned behaviour on leisure time physical activity participation. Journal of Sport and Exercise Psychology, 27, 470–487. Conner, M., Norman, P., & Bell, R. (2002). The theory of planned behavior and healthy eating. Health Psychology, 21, 194–201. Eng, J.J., & Martin Ginis, K.A. (2007). Using the theory of planned behavior to predict leisure time physical activity among people with chronic kidney disease. Rehabilitation Psychology, 52, 435–442. Fishbein, M. (1967). Readings in attitude theory and measurement. New York: Wiley. Francis, J.J., Eccles, M.P., Johnston, M., Walker, A.E., Grimshaw, J.M., Foy, R. et al. (2004). Constructing questionnaires based on the theory of planned behav- iour. In A manual for health services researchers. Centre for Health Services Research, University of Newcastle upon Tyne. Hagger, M.S., Chatzisarantis, N.L.D., & Biddle, S.J.H. (2002). A meta-analytic review of the theories of reasoned action and planned behavior in physical activity: Predictive validity and the contribution of additional variables. Journal of Sport and Exercise Psychology, 24, 3–32. Hardeman, W., Johnston, M., Johnston, D.W., Bonetti, D., Wareham, N.J., & Kin- month, A.L. (2002). Application of the Theory of Planned Behaviour in behaviour change interventions: A systematic review. Psychology and Health, 17, 123–158. Hillsdon, M., Foster, C., Cavill, N., Crombie, H., & Naidoo, B. (2005). The effectiveness of public health interventions for increasing physical activity among adults: A review of reviews. London: Health Development Agency (http:// www.publichealth.nice.org.uk/page.aspx?o=505281). Johnston, M., Bonetti, D., Joice, S., Pollard, B., Morrison, V., Francis, J.J. et al. (2007). Recovery from disability after stroke as a target for a behavioural inter- vention: Results of a randomised controlled trial. Disability and Rehabilitation, 29, 1117–1127. Kiene, S.M., Tennen, H., & Armeli, S. (2008). Today I’ll use a condom, but who knows about tomorrow: A daily process study of variability in predictors of condom use. Health Psychology, 27, 463–472. Kinmonth, A.-L., Wareham, N.J., Hardeman, W., Sutton, S., Prevost, A.T., Fan- shawe, T. et al. (2008). Efficacy of a theory-based behavioural intervention to increase physical activity in an at-risk group in primary care (ProActive UK): A randomised trial. The Lancet, 371, 5–7. McCarty, D. (1981). Changing contraceptive usage intentions: A test of the Fishbein model of intention. Journal of Applied Social Psychology, 11, 192–211. © 2009 The Author. Journal compilation © 2009 International Association of Applied Psychology.
270 SNIEHOTTA Michie, S., & Abraham, C. (2004). Interventions to change health behaviours: Evidence-based or evidence inspired? Psychology and Health, 19, 29–49. Mokdad, A.H., Marks, J.S., Stroup, D.F., & Gerberding, J.L. (2004). Actual causes of death in the United States, 2000. Journal of the American Medical Association, 291, 1238–1245. Noar, S.M., & Zimmerman, R.S. (2005). Health behavior theory and cumulative knowledge regarding health behaviors: Are we moving in the right direction? Health Education Research, 20, 275–290. Ogden, J. (2003). Some problems with social cognition models: A pragmatic and conceptual analysis. Health Psychology, 22, 424–428. Pollard, B., Johnston, M., & Dieppe, P. (2006). What do osteoarthritis health outcome instruments measure? Impairment, activity limitation, or participation restriction? Journal of Rheumatology, 33, 757–763. Rodgers, W., Murray, T., Courneya, K.S., Bell, G., & Harber, V.J. (2009). The specificity of self-efficacy over the course of a progressive exercise programme. Applied Psychology: Health and Well-Being, 1. Rothman, A.J. (2004). Is there nothing more practical than a good theory? Why innovations and advances in health behavior change will arise if interventions are more theory-friendly. International Journal of Behavioral Nutrition and Physical Activity, 1, 11. Schwarzer, R. (2008). Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Applied Psychology: An International Review, 57, 1–29. Sheeran, P. (2002). Intention–behaviour relations: A conceptual and empirical review. European Review of Social Psychology, 13, 1–36. Sniehotta, F.F. (2009). Towards a theory of intentional behavior change: Plans, planning and self-regulation. British Journal of Health Psychology, 14, 261–273. Sniehotta, F.F., Scholz, U., & Schwarzer, R. (2005). Bridging the intention–behaviour gap: Planning, self-efficacy, and action control in the adoption and maintenance of physical exercise. Psychology and Health, 20, 143–160. Stead, M., Tagg, S., MacKintosh, A.M., & Douglas, E. (2005). Development and evaluation of a mass media Theory of Planned Behaviour intervention to reduce speeding. Health Education Research, 20, 36–50. Sutton, S. (2002). Testing attitude–behaviour theories using non-experimental data: An examination of some hidden assumptions. European Review of Social Psychology, 13, 293–323. van den Berg, M., Timmermans, D.R.M., Knol, D.L., van Eijk, J.T.M., de Smit, D.J., van Vugt, J.M.G. et al. (2008). Understanding pregnant women’s decision making concerning prenatal screening. Health Psychology, 27, 430–437. Webb, T.L., & Sheeran, P. (2006). Does changing intentions engender behavior change? A meta-analysis of the experimental evidence. Psychological Bulletin, 132, 249–268. Weinstein, N.D. (2007). Misleading tests of health behavior theories. Annals of Behavioral Medicine, 33, 1–10. West, R. (2005). What does it take for a theory to be abandoned? The transtheoretical model of behaviour change as a test case. Addiction, 100, 1048–1050. © 2009 The Author. Journal compilation © 2009 International Association of Applied Psychology.
You can also read