Alabama Obesity Task Force - Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Alabama Obesity
Task Force
Strategic Plan for the
Prevention and Control
of Overweight and
Obesity in Alabama
Alabama Depar tment of Public HealthTABLE OF CONTENTS
Letter from the State Health Officer ........1 Alabama State Obesity Task Force .........19
Executive Summary..................................2 History ..............................................20
Overview of the obesity epidemic.............3 General guiding principles
What is obesity?...................................4 of the task force .................................20
Body Mass Index..............................4 Multifaceted approach
Over-fat............................................4 guidelines .......................................20
Waist circumferences ........................5 Evidenced-based
Obesity trends......................................5 approaches that work .....................22
Influencing factors ...............................6 Alabama’s State Plan: ..............................23
Nutrition..........................................6 General comments .............................24
Physical activity................................7 How to use the state obesity plan ......24
General consequences ..........................7 Six working groups:
Health concerns ...............................7 Perspectives in Alabama .....................25
Economic .........................................9 Nutrition subcommittee.................25
Alabama specifics....................................11 Physical activity
Alabama trends (BRFSS) ...................12 subcommittee.................................26
Alabama adults...............................12 Data subcommittee ........................29
Alabama youth/ children ................12 Youth and family
Alabama racial and subcommittee.................................31
socioeconomic influences ...............13 Community subcommittee.............32
Influencing factors ............................14 Healthcare subcommittee ...............34
Nutrition........................................14 Additional areas of intervention .........34
Physical activity..............................14 Media and social marketing............34
Attitudes .......................................14 Research .........................................35
General Consequences .......................15 Funding concerns...........................35
Health ............................................15 Resources for Implementing
Economic burden...........................16 The Plan ...............................................36
Healthy Alabama 2010...........................17 References ..............................................45
Alabama Department of Public HealthLETTER FROM THE STATE HEALTH OFFICER
T
he goal of the State Obesity sis will be placed on a healthy relationship
Task Force was to develop and with food, a healthy body weight, and a phys-
implement a comprehensive, ically active lifestyle. Approaches include
realistic state plan which will learning to select appropriate amounts and
reduce the worsening obesity types of foods as well as learning personal
epidemic in Alabama. The coping mechanisms to replace comfort eating.
plan was not to change approaches already in There is a consensus that people know they
progress, but rather to create a uniform “should eat right”, but I am less convinced
approach to reduce obesity. The Alabama that people know what actually is right or
State Obesity Plan provides goals and objec- how to do it.
tives to follow at various social-ecological lev- The approach in this report is to address
els. The plan provides various approaches to good nutrition and physical activity through-
address the impact of obesity on Alabama’s out the lifecycle. Breastfeeding support is the
citizens including education and awareness, logical place to start, as breastfeeding decreas-
lifestyle and behavioral choices, community- es the chances of the child becoming over-
based environmental strategies, school and weight while assisting the mother to return to
worksite improvements, and policy develop- a pre-pregnancy weight. The importance of
ment or changes. This plan does not address the school day for our children and the work
pharmacological or medical interventions, place setting for adults cannot be understated.
however, these are also appropriate for certain The structured school/ work setting can help
individuals based on established medical cri- people to make good decisions as long as the
teria. It is our hope that the plan is used positive options are there. Communities
statewide as a reference for selecting developing walkable areas for all citizens,
approaches to implement. It can be benefi- resulting in physical activity opportunities
cial in setting formal goals, such as in a cor- that are readily available, can happen.
porate business plan, as well as in informal Data will be a key in evaluation and for
settings, such as a community project. future documentation. It will be helpful to
The various levels of influence, as noted in have standardized health data at the county or
the adaptation of a social-ecological model, town level.
are important since the question of whether To make this truly a plan for the entire
obesity is a personal concern versus a public state, new partners are encouraged to join.
health concern exists. I propose it is both. With all of us working together, we can make
Obesity is a public health issue because an a difference.
overwhelming majority (80 percent) of per-
sons who are obese have additional health “Alabama, together one choice, one step, and
problems. The individual has the ultimate one life at a time!”
responsibility in making wise choices, but at
the same time the environment must support,
encourage, and even reinforce personal deci-
sion-making processes.
In addressing weight concerns, an empha-
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 1EXECUTIVE SUMMARY
In the United States, obesity has risen at “Being overweight or obese is a very com-
an epidemic rate during the past 20 years. In plex issue with many different contributing
2003, 15 states had obesity prevalence rates factors. This plan must be passionate, cre-
of 15 to 19 percent; 31 states had rates of 20 ative, and innovative with solutions that do
to 24 percent; and four states had rates more not simply mimic other states.”
than 25 percent. Alabama was one of the four
states. “The severity of obesity in Alabama makes
our challenge even greater. Media campaigns
To develop a multifacet approach, a and public education are important but will
statewide task force was organized in 2004. not be the only or best solution to a problem
The task force included representatives from of this magnitude.”
state and local governments, medical profes-
sionals, academia and research, industry, com- “Task force members must be willing to
munity, and citizen representatives. This challenge current ideas and solutions. We
report is the result of their work. must "think outside the box" when develop-
ing approaches to this problem. Our
The Alabama Obesity State Plan provides approach needs to combine prevention, inter-
a statewide focus for reducing and preventing vention, evaluation, and research. This plan
obesity through healthy lifestyles that empha- must have realistic, workable solutions.”
size balanced eating patterns and adequate
physical activity. The strategies outlined in The format of this report includes individ-
the plan are targeted for all age groups, races, ual sections on obesity trends in the nation
and socioeconomic classes. This plan will not and in Alabama, specific goals and actions
eliminate existing efforts, but does encourage steps for each subcommittee, and tools or ref-
statewide collaboration. erences to assist implementing the plan at all
levels.
General statements and opinions from the
task force set the tone for the overall goals
and measurable objectives. These statements
included:
2 Strategic Plan for the Prevention and Control of Overweight and Obesity in AlabamaOverview of the
Obesity
Epidemic
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 3OVERVIEW OF THE OBESITY EPIDEMIC
WHAT IS OBESITY? Below is an example of calculating a BMI
using the English system and in the metric
Body Mass Index system.
Obesity is defined as an excessively high • English Formula:
amount of body fat or adipose tissue in rela-
tion to lean body mass. Body Mass Index BMI= (Weight in Pounds)
X 703
(BMI) is a common measure expressing the (Height in Inches X Height in Inches)
relationship (or ratio) of weight-to-height. It
is a mathematical formula in which a person's (220)
body weight in kilograms is divided by the x 703= 27.5
(75 X 75)
square of his or her height in meters squared
A person who weighs 220 pounds and is 6
(wt/(ht)2. The BMI is more highly correlated
feet 3 inches tall has a BMI of 27.5.
with body fat than any other indicator of
height and weight. Individuals with a BMI
of 25 to 29.9 are considered overweight and • Metric Formula:
are approximately 20 pounds above appropri- Weight in Kilograms
BMI=
ate weight for height. Individuals with a (Height in Meters)2
BMI of 30 or more are considered obese and
are 30 or more pounds over appropriate 99.79
= 27.5
weight for height. For adults over 20 years 1.905 X 1.905
old, BMI falls into one of these categories:
Adult (21 and over) A person who weighs 99.79 kilograms and is
1.905 meters tall has a BMI of 27.5.
BMI Weight Status
Below 18.5 Underweight Use of BMI for Children
18.5 – 24.9 Normal
25.0 – 29.9 Overweight The terms obese, overweight and at risk
for overweight are defined differently in pedi-
30.0 and Above Obese
atric populations than in adults (see chart
below). Body Mass Index (BMI) is the pri-
Children and Adolescent (2-20)
mary measure utilized to define weight stats
BMI Weight Status in both adults and children. BMI is calculat-
Underweightlation changes with age. Because of these dif- important in the disease process than subcu-
ferences between adult and children’s BMIs, taneous fat, which is just under the skin.
the BMI for the pediatric population must be Abdominal fat cells appear to produce certain
plotted on the CDC growth charts enabling compounds that may influence cholesterol
on to determine BMI-for-age percentiles and glucose metabolism. Men are at risk who
(www.edc.gov/growthcharts). The chart, have a waist measurement greater than 40
Children & Adolescents, summarizes the cat- inches (102 cm). Women who have a waist
egories by BMI and percentages in children. measurement greater than 35 inches (88 cm)
are at risk. The waist size appears to be an
independent risk predictor when BMI is at
BMI Limitations Obesity Trends*
Body Mass Index (BMI) reflects body Among U.S. and Adulth
composition and correlates well with body BRFSS, 1991, 1996, 2003
*BMI≥30, or about 30 lbs overweight for 5’4” person
fat; however, it has limitations. A very mus-
cular person may be in the overweight BMI 1991
category. For example, professional athletes
may be very lean and muscular, with very lit-
tle body fat, yet due to the weight of the
increased muscle, they may weigh more than
others of the same height. This would need
to be considered in reviewing their BMI.
While they may qualify as "overweight" due
to their large muscle mass, they are not neces-
1996
sarily "over fat," regardless of BMI.
It is possible for a person who is in an
appropriate BMI weight range to be “over
fat”. By using a skinfold or fat analysizer, the
percent of body fat can be determined.
Waist circumferences
The amount of body fat (or adiposity)
includes concern for both the distribution of 2003
fat throughout the body and the size of the
adipose tissue deposits. The waist size is an
additional, independent risk factor for certain
diseases and can be used in conjunction with
the BMI. Waist measurements reflect evi-
dence that excess visceral fat - surrounding
the abdominal organs - increases the chance
of heart disease or diabetes. Research indi-
No Data < 10% 10% - 14%
cates that visceral fat (waist size) is more
15% - 19% 20% - 24% 25%
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 525- 34.9 obesity. The array of associated physical dis-
NOTE: If a person has short stature (under orders and emotional problems that often
5 feet in height) or has a BMI of 35 or above, accompany obesity can persist, and frequently
waist circumference standards used for the gen- worsen, throughout life. Moreover, the prob-
eral population may not apply. ability of adult obesity increases as overweight
children age: 50 percent of children who are
overweight at age six will become overweight
OBESITY TRENDS adults, by adolescence, the probability esca-
lates to 80 percent. If one parent is over-
Obesity is occurring worldwide as well as weight or obese, the child has an 80 percent
nationally. The words “pandemic” and “epi- chance of being overweight or obese. Adults
demic” have been used to describe the dra- who were overweight as children are at
matic upward trends seen in adults and chil- increased risk for poor health for longer peri-
dren. According to the World Health ods than adults who were not overweight as
Organization, the United States has the great- children.
est incidence of overweight and obesity in the Disparities in overweight and obesity
world. The prevalence of obesity has prevalence exist in segments of the population
increased steadily and is at epidemic levels. based on race and ethnicity, gender, age, and
Results from the 1999–2002 National Health socioeconomic status. For example, over-
and Nutrition Examination Survey weight and obesity are particularly common
(NHANES), using measured heights and among minority groups and those with a
weights, indicate that an estimated 65 percent lower family income. The prevalence of over-
of U.S. adults are either overweight or obese. weight and obesity is higher in women of
The Centers for Disease Control (CDC) and minority populations than in caucasian
Prevention report that Alabama is ranked first women. Among men, Mexican Americans
in terms of number of adults with overweight have a higher prevalence of overweight and
and obesity. obesity than caucasians or African Americans.
For non-Hispanic men, the prevalence of
Adults are not the only ones with excessive overweight and obesity among Caucasians is
weight. Childhood obesity has become the slightly greater than among African
most prevalent pediatric nutritional problem Americans.
in the United States. Results from the Among school aged children, there is a
1999–2002 National Health and Nutrition higher occurence of obesity in African
Examination Survey (NHANES), using meas- American, Native American, Puerto Rican,
ured heights and weights, indicate that an Mexicans, and Native Hawaiins. Data from
estimated 16 percent of children and adoles- CDC shows African American and Hispanic
cents ages six to nineteen years are over- Children are at 21.5% as compared to 12.3%
weight. The prevalence rate has been rising of Caucasians children.
steadily in all age groups, with overweight
being seen at younger ages. Excess weight in
childhood is frequently a precursor to adult INFLUENCING OBESITY
6 Strategic Plan for the Prevention and Control of Overweight and Obesity in AlabamaFACTORS ing, whether it is out of boredom, seeking
comfort, relieving stress, or celebrating, can
Obesity is a complex issue. Body weight is add extra, unexpected calories.
the result of genes, metabolism, behavior, An emphasis is being placed on family
environment, culture, and socioeconomic sta- meals at home. Children eating more than
tus. three (3) meals per week with the family were
Specific rare hereditary diseases may less likely to skip breakfast. The children also
increase the risk of obesity. In addition, there had better consumption of fruits, vegetables,
seems to be a general tendency for obesity to and diary foods. Family meals frequency had
run in some families, though the reason for a strong positive association with energy
this is not well understood. Behavior and intake, percentage of calories from protein,
environment play a large role influencing calcium, iron, vitamins A, C, E, B6, folate,
people to be overweight and obese. However, and fiber.
generally and very simplistically speaking obe-
sity is a result of an energy imbalance. This Physical activity
means most Americans are eating too many The incidence of overweight and at risk of
calories and not getting enough physical overweight is directly linked to lack of physi-
activity. cal activity and increase in inactivity, such as
viewing television more than two hours per
Nutrition day. Our society has become very sedentary.
The American eating pattern has been Approximately 43 percent of adolescents
studied to identify reasons causing the obesity watch more than two hours of television each
epidemic. The studies indicate that day. Girls are less active than boys are and
Americans have lost perception of the stan- become even less active as they move through
dard serving size. Serving sizes started grow- adolescence. Numerous health-related organ-
ing in 1970, rose sharply in the 1980’s, and izations have recommended increased physical
continued to increase in the 1990’s. It was activity in order to decrease overweight and
during this time Americans lost the percep- the associated risk factors. The American
tion of a serving size. According to the Heart Association, the Institute of Medicine,
American Diabetic Association, most the United States Department of Health and
Americans overestimate how much food Human Services, the U. S. Surgeon General,
makes up one serving. Action for Healthy Kids, Centers for Disease
Americans are also eating away from home Control and Prevention, and the Robert
more now than in the past. The American Wood Johnson Foundation, are examples of
Cancer Society reports that servings in restau- health-related agencies calling for increased
rants are approximately two and a half times physical activity for children.
what the average female needs. When large There are numerous reports that evaluate
portion sizes are coupled with the types of the relationship between academic perform-
foods we consume, high fat, high sugar, high ance and health behavior. Action for Healthy
calorie, weight gain is not a surprise. Kids reports that in school districts across the
Eating for reasons not related to hunger United States, administrators, teachers, and
also plays an important role. Emotional eat- researchers are demonstrating that proper
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 7nutrition and physical activity are linked to • Infections following wounds
academic achievement, self-esteem, mental • Infertility
health, and improved school attendance. • Liver Disease
• Low Back Pain
• Obstetric and Gynecologic Complications
GENERAL • Pain
CONSEQUENCES • Severe acute biliary and alcoholic pancre-
atitis
Health concerns • Sleep apnea
Overweight and obesity are estimated to • Stroke
be second only to smoking as preventable • Surgical complications
causes of death. The proportion of deaths • Type 2 Diabetes (Non Insulin Dependant
where obesity is a major contributing factor Diabetes Mellitus)
will grow with continued increase in obesity • Urinary Stress Incontinence
prevalence. Life expectancy is predicted to
fall in coming years because of obesity, a star- Of these health concerns, the chart below lists
tling shift in a long-running trend toward the leading causes of death in 2002 according
longer lives. It is estimated that within 50 to the CDC Division of Vital Statistics. These
years, obesity will shorten the average life apply to both male and female adults.
span of 77.6 years by at least two to five
2002 Leading Causes of Death
years; more than the impact of cancer or
heart disease. Heart Disease . . . . . . . . . . . . . . . . .28.5%
Malignant Neoplasm (Cancer) . . . .22.8%
Cerebrovascular Diseases (Stroke) . . .6.7%
Obesity is linked to many health
diseases, such as: Chronic Lower Respiratory Disease . . .5.1%
• Arthritis - Osteoarthritis of knee and hip, Accidents (Unintentional) . . . . . . . . .4.4%
Rheumatoid Arthritis Diabetes Melitus . . . . . . . . . . . . . . . .3.0%
• Birth Defects Influenza/Pneumonia . . . . . . . . . . . .2.7%
• Cancers - Breast Cancer, Colorectal
Alzheimer’s . . . . . . . . . . . . . . . . . . . .2.4%
Cancer, Esophagus and Gastric Cancer,
Endometrial Cancer, Renal Cell Cancer
Obesity and overweight substantially
• Cardiovascular disease
• Carpal Tunnel Syndrome increase the risk of morbidity from hyperten-
• Daytime Sleepiness sion; dyslipidemia; type 2 diabetes; coronary
• Deep Vein Thrombosis heart disease; stroke; gallbladder disease;
• End Stage Renal Disease osteoarthritis; sleep apnea and respiratory
• Gallbladder Disease problems; and endometrial, breast, prostate,
• Gout and colon cancers. Higher body weights are
• Heart Disorders also associated with increases in all-cause
• Hypertension mortality. Significant health problems occur
• Impaired immune response in the pediatric age group as well as the adult
• Impaired respiratory function population.
8 Strategic Plan for the Prevention and Control of Overweight and Obesity in AlabamaObesity Related Morbidities death in the United States. They account for
Cardiovascular more than 40 percent of all deaths. About
Accelerated atherosclerosis 950,000 Americans die of cardiovascular dis-
Dyslipidemia (increased triglycerides, low ease each year, which amounts to one death
HDL cholesterol level, increased LDL every 33 seconds. It is estimated that 61 mil-
cholesterol level) lion Americans, almost one-fourth of the
Hypertension population, have some form of cardiovascular
Increased left ventricular mass disease. High blood pressure is a major risk
Endocrinologic factor for heart disease and the chief risk fac-
Hyperinsulinemia tor for stroke and heart failure, and also can
Insulin resistance lead to kidney damage. It affects about 50
Early puberty (accelerated linear growth million Americans–one in four adults. Studies
and bone age) show that the risk of death from heart disease
Polycystic ovaries, dysmenorrhea and stroke begins to rise at blood pressures as
Respiratory low as 115 over 75, and that it doubles for
Hypoventilation (Pickwickian syndrome) each 20 over 10 millimeters of mercury (mm
More frequent respiratory infections Hg) increase. So, the harm starts long before
Sleep apnea people get treatment.
Orthopedic “Unless prevention steps are taken, stiffness and
Coxa vara other damage to arteries worsen with age and
Slipped capital femoral epiphyses make high blood pressure more and more diffi-
Blount's disease cult to treat. The new pre-hypertension category
Legg-Calve-Perthes disease reflects this risk and, we hope, will prompt peo-
ple to take preventive action early” said NHLBI
Obesity is linked to cardiovascular disease
Director Dr. Claude Lenfant.
and type 2 diabetes through the promotion of
Cancers
insulin resistance and other associated physio-
Fat cells are not static deposits. Visceral
logical abnormalities, including dyslipidemia,
fat is metabolically active and increased vis-
elevated blood pressure, and increased left
ceral fat is linked to certain cancers. Obesity
ventricular mass. Overweight and insulin
is strongly linked to cancer of the uterine lin-
resistance have been linked to the early devel-
ing or endometrium. An overweight woman
opment of atheromata in young adults inde-
has twice the risk of developing that cancer as
pendent of other cardiovascular risk factors.
a lean one; once she becomes obese the risk
Pulmonary, skeletal, dermatologic, immuno-
rises as much as three and a half (3.5) to five
logic, and endocrinologic systems display
(5) fold. A person who is obese has up to
obesity-related morbidities. These apply to
triple the risk of kidney cancer and of
male and female as noted in the chart above.
esophageal cancer as does someone in an
appropriate body weight range. Overweight
Cardiovascular Health
and obese men are 50 percent as likely as lean
Heart disease and stroke are the principal
men to get colon cancer; for women the extra
components of cardiovascular disease and are
risk is 20 to 50 percent. Fat is linked to
listed as the first and third leading causes of
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 9breast cancer in postmenopausal women and an increased risk for developing type 2 dia-
increases the risk of the disease by 30 percent betes during both childhood and later in life.
among the overweight and 50 percent among There is a reported association between obesi-
the obese. Prostate cancer is more common ty and type 2 diabetes, sugared beverage con-
in men who have BMI of 35 or higher. In sumption, long hours of television viewing,
addition, these men have a 60 percent risk of and reduced physical activity.
cancer recurrence within three years or more.
This is twice the rate seen in men at the Economics
appropriate weight. Obesity is associated with increased dis-
ability, decreased optimal health, increased
Diabetes health care use, and increased mortality, all of
During the past ten years, the incidence of which translate into increased health care
diabetes has nearly tripled. Overweight and cost. The direct and indirect costs of obesity
obesity are significant risk factors for diabetes. care for the nearly 119 million American
The majority of adults diagnosed with dia- adults, 65 percent of the population, who are
betes in the United States are either over- currently overweight or obese is more than
weight (85.2 percent) or obese (54.8 percent). $117 billion per year. This is an increase
Persons who have a body mass index (BMI) from previous studies. Taxpayers finance
of more than 30 are 10 times more likely to about half of these costs through Medicare
develop the illness; with a BMI above 35 for and Medicaid. "Obesity has become a crucial
10 years, the risk increases to 80 times com- health problem for our nation, and these
pared to a person of average weight. findings show that the medical costs alone
Projections are that 40 to 50 million United reflect the significance of the challenge," said
States residents could develop diabetes by previous Health and Human Services
2050. Secretary Tommy G. Thompson.
Type 2 diabetes in school children is a new Poor health is an economic burden on the
phenomenon. Twenty years ago, it was rare nation and costs millions of dollars in terms
for an adolescent or child to be diagnosed of diminished health and productivity. The
with type 2 diabetes. However, during the figures confirm earlier findings that obesity
last 20 years, childhood diabetes has increased accounts for a significant, and preventable,
10-fold. In several clinic-based studies, the portion of the nation's medical bill.
percentage of children with newly diagnosed
diabetes has risen fromAlabama
Specifics
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 11ALABAMA SPECIFICS
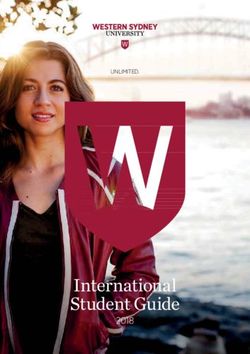
ALABAMA TRENDS Alabama Adult BMI Categories - 2003
Alabama is currently in an overweight and 40
obesity epidemic situation regarding the
health of its citizens. The nonprofit group, 35 36.8
34.8
Trust for America's Health, named Alabama
30
Percent of People
as the “fattest state” in the nation in October
28.4
2004. Mississippi and West Virginia followed 25
in second and third places. Alabama ranked
20
first in adult obesity based on 2003 data,
with 28.4 percent of adults in the obese cate- 15
gory.
10
Alabama adults
5
Sixty-three percent of Alabama adults are
overweight and or obese. Obesity is defined 0
as a BMI ≥30 and overweight is a BMI 25 to ≤ 24.9 25.0 - 29.9 ≥ 30
Body Mass Index
29.9. Of the 63 percent, 28.4 percent are
obese and 34.8 percent are overweight.
Overweight and obesity are prevalent and of youth were at risk for being overweight
increasing in Alabama. According to the with an additional 14 percent already over-
Alabama Behavior Risk Factor Surveillance weight, as defined as body mass index at or
System (BRFSS), from 1991 to 2001 obesity above the 95th percentile for age.
rates increased 76 percent. The BRFSS eval- The Alabama Department of Public
uates weight status in Alabama adults by ask- Health (ADPH) and the Alabama State
ing height and weight questions in a random Department of Education collected height
digit telephone survey. Questions are devel- and weight data on 822 adolescent students
oped by the Centers for Disease Control and in six schools from different geographic
Prevention (CDC). In 2003 in Alabama, regions in Alabama in 2001. Forty four (44)
approximately 28 percent of adults were percent of the evaluated students were at risk
obese, with rates similar for men (27.1 per- for overweight or overweight based upon
cent) and women (29.6 percent). In addi- body mass index (BMI). In 2002, a study
tion, approximately 35 percent of the adults completed by ADPH staff of 1,182 students
were overweight -- considerably more males in the second, third, fourth, and fifth grades
(42.9 percent) than females (27.3 percent). in six public schools located in Monroe
County, Alabama found approximately 17
Alabama youth/ children percent were at risk for overweight and 27
Alabama youth are also overweight. Self- percent were overweight. Rates were higher
reported data from the 2003 Youth Risk for black students (29.8 percent) than for
Behavior Survey (YRBS) showed 14 percent white students (23.6 percent).
12 Strategic Plan for the Prevention and Control of Overweight and Obesity in AlabamaAs indicated in the chart below, obesity rates are above 20 percent in all age groups, with the excep-
tion of age 65 and older.
Age Neither Overweight Overweight Obese
nor Obese (BMI≤24.9) (BMI 25.0-29.9) BMI≥30
18-24 % 53.1 26.7 20.3
CI (45.3-60.9) (19.3-34.0) 14.5-26.0
n 124 49 54
25-34 % 39.8 31.2 29.0
CI 35.1-44.6 26.6-35.7 24.5-33.5
n 208 148 141
35-44 % 30.3 36.3 33.3
CI 26.1-34.5 31.7-40.9 28.8-37.9
n 190 187 181
45-54 % 28.9 37.3 33.8
CI 24.9-32.9 32.8-41.9 29.5-38.1
55-64 % 29.4 36.6 34.1
CI 25.3-33.5 32.1-41.0 29.7-38.4
n 179 202 199
65+ % 41.7 39.4 18.9
CI 37.7-45.6 35.4-43.4 15.7-22.1
n 310 268 129
Alabama racial and socioeconomic is in 16 counties, 15 of which are in
differences Alabama's economically depressed region.
Racial and socioeconomic differences in This area, known as the Black Belt of the
prevalence rates are also evident. In the over- state, was once known for the dark soil for
weight category, the Hispanic population was agriculture. Although the region is known for
at 50.3 percent, the White population at 34.7 timber production, rich hunting and fishing,
percent, and the Black population was at 32.4 and Civil Rights history, the term Black Belt,
percent. Obesity was prevalent in 37 percent has evolved to a reference to the predominate
of African american versus 26.5 percent of ethnicity in the area.
Caucasian, and only 14 percent of Hispanics.
Estimated Number of People at Risk for Obesity
The prevalence of obesity among persons at among Adults Aged 18 and Over Bases on
Distribution by Age, Race, and Sex and Assigned
the lowest income levels (less than $15,000 Risk from the BRFSS, Alabama 2000
LAUDERDALE
LIMESTONE JACKSON
annually) was approximately 32 percent, COLBERT
MADISON
FRANKLIN LAWRENCE MORGAN
compared to a prevalence of almost 25 per-
DEKALB
MARSHALL
MARION WINSTON CHEROKEE
CULLMAN
ETOWAH
cent among persons with annual incomes at LAMAR FAYETTE
WALKER
BLOUNT
ST. CLAIR
CALHOUN
or exceeding $50,000. Obesity occurred in JEFFERSON
TALLADEGA
CLEBURNE
PICKENS TUSCALOOSA CLAY
approximately 28 percent of adults with less
SHELBY RANDOLPH
BIBB
GREENE COOSA TALLAPOOSA CHAMBERS
CHILTON
than a high school education, compared to 22 HALE
PERRY
ELMORE LEE
SUMTER AUTAUGA
percent among college graduates. MARENGO
DALLAS MONTGOMERY
MACON
RUSSELL
LOWNDES BULLOCK
A geographic study of obesity in Alabama CHOCTAW WILCOX
PIKE
BARBOUR
BUTLER
was completed utilizing BRFSS obesity data WASHINGTON
CLARKE
MONROE
CRENSHAW
DALE
HENRY
CONECUH COFFEE
from 1995 to 2000 combined with US ESCAMBIA
COVINGTON
GENEVA
HOUSTON
Census 2000 data. The geographic distribu- MOBILE
BALDWIN
26.6-31.8%
24.5-26.5%
tion of obesity illustrates the highest burden 23.1-24.3%
21.8-23.0%
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 13INFLUENCING FACTORS is very important in weight control. Despite
all the benefits of being physically active,
Nutrition most Alabamians are sedentary.
It is well established that consuming five Alabama was ranked as the tenth worst
or more servings of fruits and vegetables a day state in terms of prevalence of no leisure time
and three servings of low fat milk are benefi- physical activity. Twenty-seven percent of
cial in weight control. However, in Alabama Alabama adults reported participating in no
77.4 percent of adults do not eat 5 servings of leisure time physical activity.
fruit and vegetables a day. Dietary Behaviors In addition, 60 percent of the population
of Alabama students indicate 85.5 percent of did not meet the national guidelines for mod-
ninth through twelfth graders ate less than erate physical activity, and 79 percent did not
five servings of fruits and vegetables per day meet the guidelines for strenuous activity.
during the past seven days. Ninety two (92) Forty two (42) percent of Alabama students
percent of Alabama students drank less than did not participate in sufficient vigorous
three glasses of milk per day during the past physical activity; 81 percent of students did
seven days, ranking the worst of all the states. not participate in sufficient moderate physical
activity; 59 percent were not enrolled in
Adult Consumption of physical education class; 14 percent did not
Fruits and Vegetables per Day participate in any vigorous or moderate phys-
Alabama 2003 ical activity; and 39 percent did not partici-
80 pate in a sufficient amount of physical activi-
70
77.4 ty.
Attitudes
60
Percent of People
In October 2001, the Alabama
50 Department of Public Health contracted with
the University of Alabama in Birmingham
40 (UAB) to conduct a baseline telephone survey
of 400 adults on obesity issues in Alabama.
30
Attitudes, beliefs, and health practices regard-
20
ing weight were identified. The BMI's of
22.6 respondents were calculated from self-report-
10 ed heights and weights. Selected findings
included:
0 (1) Approximately ten percent of those
Consume 5 Consume less
or more than 5 who were calculated as overweight
servings per day servings per day responded they were not overweight.
(2) The most common reason for want-
Physical activity ing to lose weight was to be able to
There is little doubt that regular physical see a child(ren) grow up.
activity is good for overall health. Physical (3) The most frequent reasons for not eat-
activity decreases the risk for diseases such as ing a healthy diet were: "it is too hard
colon cancer, diabetes, and high blood pres- to count calories," "diets don't work,"
sure and is beneficial for bone health, enhanc- “I am tired of hearing about dieting”,
ing mental clarity, and as a stress reducer. It and "eating healthy is too expensive."
14 Strategic Plan for the Prevention and Control of Overweight and Obesity in AlabamaGENERAL of adult hypertension. Thirty-three percent of
CONSEQUENCES the total Alabama adult population indicated
they had been diagnosed with hypertension.
Health concerns In addition, 38 percent of the total adult
The life expectancy rate for an Alabama African American population is at risk for
citizen is 74.1 years as compared to 77.2 years hypertension. The Alabama Department of
for the average adult in the United States. In Public Health identified both high systolic
2001, the life expectancy for an Alabama and high diastolic blood pressures in Alabama
adult was comparable to the average adolescents.
American adult in 1981. This statistic places Cancer is the second leading cause of
Alabama 20 years behind the average state in death accounting for 29,013 or 21.7 percent
terms of average life expectancy in the United of all deaths from 1998 to 2000. The three-
States. Unless changes are made in lifestyles year crude death rate for cancer for the total
and behaviors, today’s youth may be the first population is 220.3 per 100,000 population.
generation in history to not outlive their par- The African American and other races crude
ents. death rate is 184.4 and the Caucasian crude
Some subgroups are at higher risk for obe- death rate is 234.1 per 100,000 race-specific
sity and its associated health problems. Rates population. The 1998 to 2000 age-adjusted
of chronic diseases in which obesity is a risk death rate1 for cancer for the total population
factor are high in Alabama and dispropor- is 216.2 per 100,000 population. The
tionately high in similar subgroups. For
example, in 1998 age-adjusted cardiovascular Leading Causes of Death
mortality rates were substantially higher for in Alabama - 2002
African Americans (473.9 per 100,000) com-
pared to Caucasian (383.9 per 100,000). In
1998, the stroke mortality rate for African
Americans was 44 percent higher than for 36.8
All Other Causes 33%34.8
Caucasian.
The top two causes of death in Alabama
are cardiovascular disease (CVD) and cancer. 28.4
Much research supports the nutrition and
Cardiovascular Cancer 21%
physical activity impact on these diseases. In
Disease 36%
2002, CVD accounted for 36 percent of all
deaths. More Alabamians die each year from
CVD than from all forms of cancer com-
bined. Alabama ranks 6th in the nation in
heart disease deaths and 7th in stroke deaths.
Accidents 5%
Alabama ranks above the national average in Respiratory Diseases %5
deaths due to heart disease. African
Americans have the highest stroke death rate African American and other races age-adjust-
in Alabama. Alabama ranked third in terms ed death rate is 243.1 and the Caucasian age
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 15adjusted death rate is 208.9. Economics
The report, "F as in Fat: How Obesity
Diabetes Policies are Failing in America," stated that
An estimated 17 million Americans (6.2 per- Alabama spent the equivalent of $293 per
cent of the population) now have diabetes. person on its 4 million plus residents last year
Alabama has one of the highest rate of diag- paying for health care costs related to obesity
nosed diabetes (8.4 percent). In 2003, the - the ninth highest amount in the nation.
age-adjusted prevalence of diagnosed diabetes Because of increases in health care costs and
ranged from a high of 10.9 percent in Puerto health insurance for state employees and pub-
Rico to a low of 4.9 percent in Colorado. lic education employees, the Legislature held
Diabetes is the sixth leading cause of death in a special session in November 2004 to address
Alabama with 3,964 or 3 percent of all deaths ways to contain the rise in health insurance
from 1998 to 2000. For African Americans costs.
and other races, diabetes is the fifth leading
cause of death. For Caucasians, diabetes is the
seventh leading cause of death.
True population statistics data and Alabama
data are not yet available regarding the preva-
lence of type 2 diabetes in school children.
However, verbal reports indicates that dia-
betes in children is growing. Because of ele-
vated risks in Alabama school students,
Alabama experiences an even greater potential
for type 2 diabetes in school-age children.
16 Strategic Plan for the Prevention and Control of Overweight and Obesity in AlabamaHealthy
Alabama 2010
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 17HEALTHY ALABAMA 2010
The overall goal for the Healthy Alabama usage, higher rates of obesity, and more people
2010 Objectives is to increase the life living a sedentary lifestyle and lower utilization
expectancy and quality of life for Alabamians. of preventive health care measures. These fac-
The disparity in life expectancy between tors result in higher death rates from chronic
Alabama and the remainder of the nation has conditions such as heart disease, stroke, and
actually grown wider in the past decade. A diabetes. The State Obesity Task force
number of factors that can adversely affect acknowledges these goals and will assist in
longevity include poverty, low levels of educa- efforts to reach them.
tional attainment, higher rates of tobacco
Physical Activity and Fitness
Adult Physical Activity
1.1 Increase to 25 percent or more the proportion of adults aged 18 and older who engage regu-
larly, preferably daily, in sustained physical activity for at least 30 minutes per day.
AL Baseline AL Target US Baseline US Target
Adults 18 and older 17 (1997) 25 23 (1995) 30
Adolescent Physical Activity
1.2 Increase to 60 percent or more the proportion of students in grades 9-12 who engage in
moderate physical activity for at least 20 minutes a day for 3 days per week.
AL Baseline AL Target US Baseline US Target
Students grades 9-12 55 (1997) 60 N/A N/A
Nutrition
Weight Status
1.3 Reduce to 20 percent or less the prevalence of being overweight (defined as a body mass
index at or above 27.8 for men and 27.3 for women) among adults aged 18 and older.
AL Baseline AL Target US Baseline US Target
Adults 18 and older 35 (1997) 20 N/A N/A
Dietary Guidelines
1.4 Increase to 40 percent or more the proportion of adults aged 18 years and older who meet
the dietary recommendations of a minimum average daily goal of at least 5 servings of veg-
etables and fruits.
AL Baseline AL Target US Baseline US Target
Adults 18 and older 17 (1997) 40 N/A N/A
18 Strategic Plan for the Prevention and Control of Overweight and Obesity in AlabamaAlabama State
Obesity Task
Force
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 19ALABAMA STATE OBESITY TASK FORCE
HISTORY committee selected a chair. The task force,
Despite limited resources, the Alabama with 92 total members, became six, separate,
Department of Public Health (ADPH) and yet coordinated committees all creating posi-
the University of Alabama in Birmingham tive working relationships. The committees
(UAB) pledged to work together to address developed realistic action steps from the
healthy opportunities for all Alabamians. established goals and objectives.
The obesity epidemic was acknowledged as
were different approaches that were being GENERAL GUIDING
taken across the state to address it. The first PRINCIPLES
Obesity Task Force meeting was held on May
4, 2004 in Montgomery. Over 70 representa- Multifaceted approach guidelines
tives attended from public health, academia, In developing a state obesity plan, a social-
health care, education, businesses, and com- ecological approach was used. This model
munity groups. was especially appropriate in addressing the
The charge of the task force was to devel- very complicated weight issues as it includes
op and implement a comprehensive state plan influences at multiple levels: individual, inter-
to reduce obesity in Alabama among all seg- personal, organizational, community, and
ments of the population. The purpose was public policy. This ecological perspective
not to change the approaches already in includes the importance of approaching pub-
progress, but rather to help Alabama work lic health problems at multiple levels while
together as a whole. The task force members stressing interaction and integration of factors
agreed to utilize evidenced based practices in with and across the levels.
developing the plan. From the first meeting, Strategies compatible with this model include
it was clear the plan would be suitable for enhancing individual responsibility for posi-
Alabama, building on the state’s unique char- tive lifestyle change and garnering outside
acteristics and resources. Members agreed to forces through schools, worksites, and com-
address weight concerns through emphasizing munity settings.
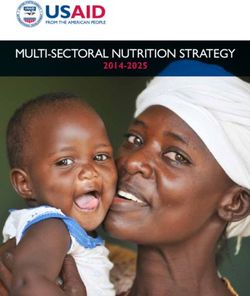
a healthy relationship with food, a healthy At the center of the SEA is the individual
body weight, and a physically active lifestyle. surrounded by increasing larger circles of influ-
During the first meeting, members self- ence. These areas, interpersonal, organization-
selected into committees: nutrition concerns, al, community, and policy will all influence
physical activity concerns, youth and families, personal choices. The relationship can be
community, data, and health care. The com- reciprocal; the environment affects health relat-
mittees met on a monthly basis from June ed behaviors and people through their actions
through November 2004 establishing goals, can affect the environment. The Alabama
adding additional partners, and reviewing State Obesity Plan is designed to enable per-
potential solutions. By January 2005, each sons to use the plan at any and all levels.
20 Strategic Plan for the Prevention and Control of Overweight and Obesity in AlabamaIndividual portive of others and be good role models in
Individuals are responsible for positive, maintaining a healthy weight, eating a
sound, life style behavior choices that pro- healthy meal pattern, and being physically
mote a healthy body. To encourage this, a active.
positive message that promotes healthy eating The task force will work to increase adult
and increased physical activity through cul- knowledge and skills about being role models
turally relevant approaches will be used. The for positive eating and physical activity
need to raise the awareness of the increased lifestyles in order to strengthen future genera-
obesity rates and decreased physical activity as tion’s health outcomes. Additionally a focus
a serious health issue, its economic cost to on training adults who are parents, who work
Alabama, and its negative impact on the qual- formally and informally with children and
ity of life exists. teens, and adults who influence policy and
funding decisions will be needed.
Interpersonal/Group Examples include an accountability system
Alabama citizens are in multiple roles at in families or with friends for eating healthy
any given time. A person may be a family food selections. Support can be offered
member, a friend, or a coworker/peer. All of through families and neighbors helping each
the roles provide a social identity and can other become more physically active by going
provide or offer support. In addressing obesi- for a bike ride, inviting a neighbor to take a
ty issues, Alabama citizens need to be sup- walk, or playing outside with the children.
A Social-Ecological Model For Nutrition Evaluation
Social Structure, Policy
1 Local, State federal
Spheres of Influence policies and laws that
regulate or support
healthy actions
Social Structure, Policy, Systems
Community: Social
Community networks, norms
standards (e.g. public
agenda, media agenda),
Institutional/Organization or other existing channels
Institutional/
Organizational: Rules,
Interpersonal regulation, policies and
Lifestyle Influences informal structures
(worksites, schools,
religious groups)
Individual Interpersonal
Interpersonal process
and primary groups
(family, peers, social
networks, associations)
that provide social
identity and role
definition
Individual: Individual
characteristics that
influence behavior such
1 McElroy KR, Bibeau D, Steckler A. Glanz K. A perspective on health promotion as Knowledge, attributes,
programs. Health Education Quarterly 15:351-377. 1988. beliefs, and personality
traits
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 21Institutional/Organizational nities for physical activity by modifying com-
Alabama’s businesses, industries, organiza- munity and school environments is needed.
tions, educational sites, including day care, Examples include churches, mosques, syna-
primary, secondary and higher education gogues and other faith organizations that
institutions, work places, medical settings, serve meals to members to provide healthy
and other places of employment will provide food selections and promote prayer walks or
opportunities to promote good health and exercise classes at the facility; and for civic
recommended behaviors. These increased groups to select a neighborhood environmen-
opportunities can be through formal chan- tal issue to address in efforts to promote
nels, such as rules and policies, or through walking.
informal channels, such as suggestions or
guidelines. Examples include employers Policy
encouraging physical activity breaks; healthy Alabama’s decision makers will be support-
food items being available in vending ive at local and state levels in creating oppor-
machines and in cafeteria selections; wellness tunities for healthy eating and physical activi-
programs providing information for all ty through policies and laws. This will
employees; and employers encourage or pro- require citizens to raise awareness and pro-
vide early assistance and appropriate preven- mote action among elected and appointed
tion/treatment interventions. officials, foundations, and potential private
sector partners regarding the need for policy
Community change, environmental change, and adequate
Alabama’s communities, social networks, resources to address overweight/ obesity in
and faith communities that exist formally or Alabama.
informally among individuals, groups, and
organizations will promote and support Evidenced-based approaches that work
lifestyle choices to promote healthy bodies. The obesity epidemic is a serious health
To improve our communities and to make problem that calls for immediate action to
them places where people are healthy, safe, reduce its prevalence. Therefore, the task-
and cared for, will take a unified effort. force felt that actions should be based on evi-
Collaborating effectively with other individu- dence-based research. These interventions or
als and organizations, both inside and outside treatment approaches have been scientifically
the community, is necessary. This requires a demonstrated to be effective, regardless of the
process of people working together to address discipline that developed them. This plan is
key issues that are important to them. The based on research findings that validate the
community environment will establish and promoted concepts. However, the plan will
promote healthy eating and active lifestyles as not be limited only to printed evidenced-
the norm rather than the exception. based documentation.
Community based strategies to support
healthy eating and physical activity need to
be tailored for the individual community.
Access to healthy foods choices and opportu-
22 Strategic Plan for the Prevention and Control of Overweight and Obesity in AlabamaAlabama’s State
Plan Addressing
Obesity
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 23ALABAMA’S STATE PLAN ADDRESSING OBESITY
GENERAL COMMENTS made, specifically that schools should provide
healthy food choices and address physical
This report presents a plan with goals, rec- education options. Nutrition changes include
ommendations, strategies, and activities foods served through the cafeteria, in vending
encouraging interventions that promote machines, and school stores; that fund raising
healthy eating and physical activity as policies should utilize healthy foods or non-
approaches for Alabamians to reach and food items; and that teachers should use non-
maintain a healthy weight. In developing the food items as rewards for classroom perform-
plan, it was recognized that a great potential ance in place of candy. School environment
for synergy with enhanced communication approaches include the recommendation to
and coordination among various groups with- complete an assessment, such as The School
in the state exists. For example, media mes- Health Index, to identify potential areas for
sages can be tailored to be put into practice at needed change. Physical activity recommen-
schools, work places, and community sites. dations include evaluating all physical educa-
There will also be benefits of learning from tion (PE) waivers; having PE taught by certi-
successes across the state. The successful fied PE teachers in all grades; promoting life-
approaches can be tailored and implemented time, enjoyable activities; reviewing the quali-
in a different location. This coordinated ty of the classes taught; and limiting the stu-
focus will assist in using limited resources and dents in each class to a specified ratio of stu-
generating new resources by involving the dents to teachers.
whole state.
Committee members agreed that obesity is HOW TO USE THE STATE
a very complex issue. Therefore, approaches OBESITY PLAN
taken will consider the relationships with
food. These relationships will be explored to The outlined approaches will not be suc-
address cultural, emotional, and traditional cessful without support of representatives
beliefs that determine eating habits. from diverse segments of society, industries
The plan does not focus on changes need- and businesses, institutions, agencies, media,
ed in the school environment. This is health care, families, schools, communities,
because the State Department of Education non profit organizations, places of faith, and
developed a Student Health Task Force. The so on. Implementing the plan must be a
education task force met from September statewide effort. Special attention may be
2004 through May 2005 in developing nutri- needed in communities that experience health
tion and physical activity related recommen- disparities and have environments that are
dations for public schools. The State Obesity not supportive of healthy nutrition habits or
Task Force supports the recommendations physical activity opportunities. The plan can
24 Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabamabe used by individuals at both the statewide health consequences in individuals who are
and local levels. Agencies, institutions, and overweight or obese. The first group may or
groups can implement the strategies in work may not acknowledge they have a weight
plans. Key stakeholders and decosionmakers problem. In fact, based on a survey complet-
can use the report to increase awareness. It is ed in 2001, almost 10 percent of Alabamians
the Task Force’s hope that the plan can stimu- who were overweight did not realize they
late new ideas, partnerships, and coalitions. were. This group lacks an understanding in
the severity of the health risks associated with
obesity and does not display a working
SIX WORKING GROUPS: knowledge of how to transform eating pat-
terns into healthier food intakes.
PERSPECTIVES IN Interventions will include educational oppor-
ALABAMA tunities to include interactive sessions for
learning implementation skills. Topics will
NUTRITION include, but not be limited to:
SUBCOMMITTEE • Health problems associated with obesity
• Portion sizes
Summary: • Healthy food choices
The goal is to promote both primary and • How to read food labels
secondary prevention of obesity. • How to prepare foods
The committee’s consensus is there are
two groups who would greatly benefit from a The second group knows the importance
nutrition intervention plan. The first group of an appropriate body weight and increased
does not understand the health importance of physical activity level, but is not convinced to
weight control and does not display an make lifestyle changes. Educational efforts
understanding of how to transform eating for this group will need to address:
patterns to consume healthier foods. The • Changing knowledge into behavior
second group has “head knowledge”, but due • Making appropriate food choices that are
to environmental conveniences, personal easy and convenient
beliefs, and values is not convinced to make • Learning healthier ways to prepare favorite
lifestyle changes. foods
Both groups will benefit from a compre-
hensive media plan and other approaches to Both groups will benefit from environ-
promote healthy lifestyles. Such interven- mental improvements to foster healthier food
tions could include community level educa- as the easier, low-cost choice. The environ-
tion efforts, healthier eating choices to be mental changes will be supplemented with
readily available, and opportunities for reward educational messages that address overcoming
incentives through work or insurance plans. barriers to losing weight.
Educational strategies will include:
Specific details: • Providing programs to explore aspects of
The nutrition subcommittee agreed that emotional eating; the uses, values, and
there are different levels of understanding of
Strategic Plan for the Prevention and Control of Overweight and Obesity in Alabama 25You can also read