Baby Makes 3 Respect, Responsibility and Equality - VicHealth
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Respect, Responsibility and Equality Baby Makes 3
I kept telling the guys at work,
‘Guys, you should be doing this course’.
And they said, ‘why?’
And I said, ‘just flipping do it because it will open your eyes’.
Baby Makes 3: Project Report
Author: David Flynn
© WCHS, 2011
For copies of this report, or for further information about the Baby Makes 3 Project, contact:
Whitehorse Community Health Service
43 Carrington Road,
Box Hill, VIC 3128
Ph: (03) 9890 2220
www.wchs.org.auBaby Makes 3 – Project Report
Baby Makes 3
Acknowledgements
The Baby Makes 3 project could not have succeeded without the enthusiasm of members of the Project Reference
Group each of whom dedicated much of their precious time to support project activities. They include:
Pam Heselev Maternal Child Health Coordinator in the City of Whitehorse
Christine Haddrick Maternal Child Health Nurse, City of Whitehorse
Lea Fitcher Coordinator of Specialist Women’s Clinics, Birralee Maternity Centre
Tricia Kunek Childbirth Education Coordinator, Birralee Maternity Centre
Diane Johnson Just Families Project Counsellor, Drummond Street Services
Olive Aumann Health Development Manager, Whitehorse Community Health Service
Chris Grace Men’s Health Team Leader, Whitehorse Community Health Service
David Flynn Baby Makes 3 Project Coordinator, Whitehorse Community Health Service
Special mention needs to go to the following people who each made a significant contribution to the project:
• The Maternal Child Health nurses and staff in the City of Whitehorse, who recognised the value of the project
and whose support and efforts were often above and beyond the call of duty
• Pam Heselev, whose leadership was key to the project’s implementation and achievements
• Christine Haddrick for her pioneering work in developing fathers nights in the City of Whitehorse
• Chris Grace, for his decades long work with the Men Making Change program, who recognised the need and
opportunity for a primary prevention program of this kind
• The Baby Makes 3 Group facilitators – Christine Haddrick, Marelle Wolfkamp, Rodney Vlais, Mark Bennetts
and, most importantly, Denise Roberts – who contributed thoughts and ideas to the evolution of the group
program
• Jacqueline Hope, social work student at Monash University for her diligence and professionalism in
undertaking key evaluation activities
• Drummond Street Services for their work through the William Buckland Foundation funded Just Families
Project to add value to Baby Makes 3
• The Preventing Violence Against Women Team at VicHealth for their unwavering support and guidance,
especially Wei Leng Kwok (Research Leader) for her important contribution to the evaluation framework
• All the first time parents who participated in the Baby Makes 3 program, especially those involved in
evaluation activities that were essential to the preparation of this report
Baby Makes 3 – Project ReportBaby Makes 3
Table of Contents
Executive Summary ……………………………………………………………………………………………………………… 1
1. Introduction …………………………………………………………………………………………………………….….…… 3
2. Project Background …………….……………………………………………………………………………………….….. 4
2.1 Primary prevention of violence against women ……………………………….……….……. 4
2.2 Baby Makes 3 – phase one …………………………………………………………………….….…… 6
2.3 Why target first time parents? ………………………………………………………………….…… 7
2.4 Gender roles and equality during the transition to parenthood ………………..…... 8
2.5 The construction of motherhood and fatherhood ………………………………………..… 10
2.6 Maternal Child Health – a key setting for primary prevention …………….………….. 12
2.7 Rationale for Baby Makes 3 ................................................................................ 13
3. Project Description …………………………………………………………………………………………………….…… 14
3.1 Project goal, objectives, activities ……………………………………………………….………..… 16
3.2 Baby Makes 3 – group program ………………………………………………………….……..….. 17
3.2.1 Theory of change ………………………………………………………….……..……… 19
3.3 Fathers nights ……………………………………………………………………………………………….. 21
3.4 Maternal Child Health workforce capacity building ……………………………………..... 23
4. Evaluation Approach ..…………………………………………………………………………………………………….. 24
4.1 Baby Makes 3 – group program …………………………………………………………………….. 25
4.2 Fathers nights ……………………………………………………………………………………..……….. 27
4.3 Maternal Child Health workforce capacity building ……………………………..………. 27
4.4 Project implementation and partnerships ………………………………………………….… 27
5. Evaluation Findings ………………………………………………………………………………………………………. 28
5.1 Baby Makes 3 – group program ………………………………………………………….……….. 28
5.1.1 Experiencing the program ………………………………………………………..….. 28
5.1.2 Program impacts – quantitative data ……………………………………….….. 32
5.1.3 Program impacts – qualitative data ………………………………………….….. 36
5.2 Fathers nights ……………………………………………………………………………………………….. 43
5.3 Maternal Child Health workforce capacity building ………………………………………. 44
5.4 Project implementation and partnerships ………………………………….…………………. 46
6. Discussion …………………………………………………………………………………………………………………….. 49
6.1 Reflections of the Baby Makes 3 program ……………………………………………….……. 50
6.2 Future directions ……………………………………………………..………………………….…….…. 55
7. Conclusion …………………………………………………………………………………………………………………….. 58
8. References ……………………………………………………………………………………………………………………… 60
Baby Makes 3 – Project ReportBaby Makes 3
Appendix A
Running an Effective Fathers Evening ……………………………………………………………………… ii
Appendix B – Evaluation tools
Approach to Evaluation ………………………………………………………………………………………….. iv
Baby Makes 3 Pre and Post-group Questionnaire ………………………………………………….. vi
Baby Makes 3 Post-group Feedback Form …………………………………………………………….. vii
Couples Interview – Plain Language Statement ………………………………………………….….. viii
Couples Interview – Consent Form ………………………………………………………………………… ix
Couples Interview – Schedule of Questions …………………………………………………………… x
Professional Development Workshop – Feedback Forms ………………………………………. xii
Maternal Child Health – Focus Group: Schedule of Questions ………………………………. xiv
Baby Makes 3 Project Reference Group – Focus Group: Schedule of Questions ……. xv
Appendix C – Evaluation Data
Pre and Post-group Questionnaire: Results from Section 1 …………………………………… xvi
Pre and Post-group Questionnaire: Section 1 – T-test Results ……………………………….. xvii
Pre and Post-group Questionnaire: Results from Section 2 ……………………………………. Xviii
Pre and Post-group Questionnaire: Section 2 – T-test Results ……………………………….. xix
Baby Makes 3 – Project ReportBaby Makes 3
Executive Summary
Project Background Project activities
The Baby Makes 3 project is an example of promising 1. The development and delivery of the Baby Makes
practice in the emerging field of preventing violence 3 group program.
against women. It is a primary prevention program A three-week discussion based program for new
that seeks to prevent violence before it occurs, by parents covering a number of key topics relevant
promoting equal and respectful relationships to the lifestyle and relationship changes that
between men and women during the transition to follow the birth of a child.
parenthood.
2. The facilitation of group discussions at Maternal
First time parents are a key target group for primary
Child Health fathers nights.
prevention activity. The transition to parenthood
represents a ‘window period’ during which it is One-off evening sessions for first time fathers
promoting positive father involvement in new
possible to engage and work with both men and
families.
women when traditional notions of parenthood are
exerting a powerful influence on how they approach
3. Workforce capacity building through the
and negotiate their parenting roles. The decisions
development and delivery of professional
that couples make during this key stage of life can
development workshops.
have important consequences on the level of equality
within their relationship, and between men and Professional development workshops for
women more generally. Maternal Child Health nurses focussing on
practical strategies for promoting gender
Funded by VicHealth, the Baby Makes 3 project equality during the transition to parenthood.
involved a partnership between Whitehorse
Community Health Service, the lead agency, and the Evaluation Approach
City of Whitehorse Maternal Child Health Service, a
The impact of the Baby Makes 3 project was
key service for engaging first time parents. A valuable
evaluated using a comprehensive evaluation
partnership was also established with Drummond
framework consisting of a combination of qualitative
Street Services Just Families project.
and quantitative methods including questionnaires,
Project goal interviews and focus groups.
To promote equal and respectful relationships
Evaluation findings
between men and women during the transition to
parenthood Over 90% of participants rated the Baby Makes 3
program either very good or excellent, with nearly all
Project objectives participants agreeing, or strongly agreeing, that the
1. To increase the capacity of first time parents program was relevant, helpful and enjoyable.
to build equal and respectful relationships in
The evaluation data indicated that despite couples
response to the lifestyle and relationship
professing minimal attitudinal support for traditional
changes that follow the birth of a child.
gender roles, the structure of couples’ relationships,
2. To increase the capacity of health in terms of ‘who does what’, became highly
professionals and organisations to promote traditional following the birth of their baby. Yet
equal and respectful relationships during the couples reported being generally unaware of how
transition to parenthood
Baby Makes 3 – Project Report 1Baby Makes 3
these traditional gender roles may be impacting on A key achievement of the program has been engaging
their relationship. men, overcoming their resistance and gaining their
support for gender equality.
A key impact of the Baby Makes 3 program was that
participants developed a greater awareness of how The future direction of the project involves
traditional attitudes to gender and parenting roles endeavouring to facilitate the implementation of
were shaping their new families. Through their Baby Makes 3 in other local government areas. To
involvement with the program couples developed a enable this, a number of key resources are being
shared understanding of the influence of gendered produced, including:
norms and expectations and a shared language for • A Baby Makes 3 group work manual
openly discussing their impacts and effects.
• A Baby Makes 3 facilitator training program
Participation in the Baby Makes 3 program led to a • A local government step-by-step guide for
significant shift in couples’ attitudes characterised by implementing Baby Makes 3
greater understanding of their partner’s role, and
• Professional development workshops and
greater support for gender equality in new families. In
community education seminars
addition, there was evidence that some couples had
implemented changes to how they structured their
Conclusion
parenting and relationship roles, and that this was in
response to seeking a more equal relationship. The main achievement of the Baby Makes 3 project
has been the development and implementation of
The workforce capacity building aspects of the project
the ‘Baby Makes 3 model’, a unique contribution to
were successful in ensuring messages of gender
the field of primary prevention, consisting of a three-
equality were reinforced at an organisational level,
week group program exploring issues of gender
and in the day-to-day interactions between Maternal
equality from the perspective of first time parents,
Child Health nurses and the new parents who access
supported by organisational and workforce
their services.
development within a local government Maternal
Child Health setting.
Discussion
The evaluation findings demonstrate that Baby Makes
Issues of gender equality are central to the transition
3 is a successful and effective means of promoting
to parenthood. Following the birth of a baby men and
equal and respectful relationships between men and
women begin doing things differently, and often by
women. The program is readily transferable and given
default, adopt more traditional roles which in turn
the necessary resources and organisational support it
can lead to gender inequalities that stem from the
could easily be integrated into existing Maternal Child
‘undervaluing’ of women’s traditional contributions
Health Services and implemented in all local
(the baby care and housework).
governments.
A key objective of the Baby Makes 3 program is to
Given its ability to constructively engage large
give first time parents the awareness and
numbers of first time parents, particularly men, Baby
understanding required to critically reflect on the
Makes 3 has the potential to form an integral part of
new level of equality within their relationship. The
a population wide approach to the primary
program achieves this by encouraging participants to
prevention of violence against women.
acknowledge and value the contribution of the stay-
at-home parent and to share the tasks and
responsibilities of parenthood more equally.
Baby Makes 3 – Project Report 2Baby Makes 3
1. Introduction
As the name suggests, Baby Makes 3 is concerned practice in the emerging field of the primary
with that stage of life when the arrival of a new baby prevention of violence against women.
signifies the creation of a new family.
Funded by VicHealth, Baby Makes 3 is a partnership
For most couples, the birth of their first child is a between Whitehorse Community Health Service, the
major turning point as they transition into their new lead agency, and the City of Whitehorse located in
roles of ‘mother’ and ‘father’ and become acquainted the eastern metropolitan region of Melbourne,
with the demands and expectations of parenthood. It Australia. The project operates at the community and
is a time of major lifestyle changes, when many organisational levels, working with the local Maternal
practical adjustments need to be made, and a time of Child Health Service and the hundreds of first time
major relationship changes as couples increasingly parents who access the service every year.
focus their energy and attention on their baby. It is a
This report describes the implementation of the
time when couples expect to grow closer together,
project over the three year period from 2009 to 2011.
yet a significant number find it moves them further
It describes the project planning and outlines the
apart. It is time that families often expect to be filled
project objectives and activities. The evaluation
with happiness and joy but unfortunately, it is also a
framework is presented and the impacts of the
time when relationship difficulties can become
project are identified and discussed in detail.
established, and male family violence can escalate.
As an example of promising practice, the Baby Makes
The Baby Makes 3 project seeks to assist first time
3 Project Report seeks to build the evidence base in
parents adapt to the demands and expectations of
the primary prevention of violence against women.
parenthood. It is a community-based project that
aims to promote equal and respectful relationships
between men and women during the transition to
parenthood. As such, it is an example of promising
Baby Makes 3 – Project Report 3Baby Makes 3
2. Project Background
2.1 Primary prevention of violence against women
Violence against women is a significant problem with relationships across the state. There is also increasing
serious social, economic and health consequences for interest from Victorian local governments, primary
women, their families and communities. Over the care partnerships and community health services in
years society has sought to address this problem by developing primary prevention strategies. Yet in
focussing on reforming the response – by the police, Australia, and indeed the world, the primary
the courts, and the service sector – to incidents of prevention of violence against women is an emerging
violence, and on improving support for women and field of practice, and the evidence base for primary
children experiencing violence. Yet despite a range of prevention activities is still being accumulated.
efforts on these fronts the prevalence of violence
Throughout Victoria, VicHealth is playing a key role in
against women seems undiminished.
guiding this emerging field of practice. The Health
Violence against women is increasingly being seen as Costs of Violence report (VicHealth, 2004) established
a public health issue that is not only serious and violence against women as a major public health
prevalent but is wholly preventable. Consequently, issue. This report measured the health impacts of
while responding to incidents of violence remains intimate partner violence and found this violence to
critical in the first instance, attention is now turning be the largest preventable contributor to the disease
to efforts aimed at primary prevention. burden in women aged 15 to 44 years.
The prevention of violence against women can occur In 2007 VicHealth released Preventing Violence Before
at three levels: primary, secondary and tertiary. it Occurs: a framework and background paper to
Tertiary prevention occurs after an incident of guide the prevention of violence against women. This
violence and is focussed on preventing the violence publication provided a comprehensive evidence
from re-occurring. Secondary prevention occurs as based framework to guide primary prevention activity
the violent incident is taking place. The primary by the government, community, health and corporate
prevention of violence against women, however, is sectors. It is this document that provides the
focussed on preventing violence before it occurs. The framework for the planning and implementation of
Baby Makes 3 project is an example of primary the Baby Makes 3 project.
prevention.
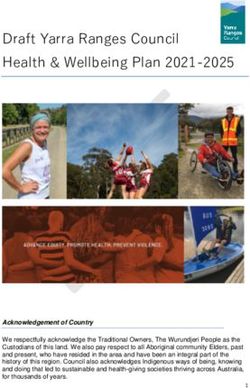
Preventing Violence Before it Occurs articulated the
There is currently growing momentum in support of need for an ecological approach (as shown in figure 1)
preventing violence against women from all levels of to understanding violence against women and
government. The National Council to Reduce Violence implementing primary prevention activities. The
against Women and their Children, in their plan for advantage of this approach is that it shifts attention
2009-2021, Time for Action (2009) argue for a away from single-factor explanations and accounts
sustained new level of investment in primary for the complex array of factors implicated in violence
prevention. The State Government of Victoria, in A against women. It locates the factors underlying or
Right to Respect (Office of Women’s Policy, 2009) has contributing to violence at a range of levels of
introduced a ten-year, whole-of-government influence, emphasising the need for many different
prevention strategy to promote gender-equitable and forms of action and recognising the value of working
non-violent communities, organisations and at different levels (VicHealth, 2007).
Baby Makes 3 – Project Report 4Baby Makes 3
Figure 1: An ecological approach to understanding violence against women
Societal: The cultural values and beliefs that shape Community / Organisational: The formal and informal
the other three levels of the social ecology social structures that impact on a person
Community / Individual /
Societal
Organisational Relationship
Individual: The developmental experiences and personality factors that
shape a persons response to stressors in their environment
Relationship: The intimate interactions a person has with others
From VicHealth (2007)
The VicHealth framework also identifies the social At the individual and relationship level the project is
determinants – the causes – and contributing factors concerned with understandings of gender roles,
to violence against women and recommends three particularly the roles of mothers and fathers, and
key themes for action. These are: understandings of femininity and masculinity and the
1. Promoting equal and respectful relationships extent to which individual attitudes and behaviours
between men and women are shaped by these understandings. At the
community and organisational level of the ecological
2. Promoting non-violent social norms and
model it is concerned with the cultural beliefs, norms
reducing the effects of prior exposure to
and expectations of men and women within
violence
communities and organisations.
3. Improving access to resources and systems of
support By critically examining these ideas and constructs, the
project seeks to engage individuals, families,
The Baby Makes 3 project is primarily located within communities and organisations in a conversation that
the first theme for action, although it does work, to a leads to greater gender equality, and in so doing, it
lesser extent, on the second and third themes. For represents a new and innovative approach to the
the most part though – operating at the individual primary prevention of violence against women.
and organisational levels of the ecological model –
Baby Makes 3 concentrates on promoting equal and
respectful relationships between men and women.
Baby Makes 3 – Project Report 5Baby Makes 3
2.2 Baby Makes 3 – phase one
The Baby Makes 3 project began as a research project The research from phase one put forward a number
exploring primary prevention activity with men during of recommendations relating to improving current
the transition to parenthood. In 2007 the project was services, including antenatal and postnatal services,
funded by VicHealth, for one year, to undertake this and developing new and innovative primary
research which served as a comprehensive needs prevention programs targeting first time parents. In
analysis for the current project (Baby Makes 3 – particular, the research identified that a primary
phase 2). The research project is described in the prevention project would need to:
phase one report (Flynn, 2008). • Target both men and women, rather than
The goal of phase one was to identify the means by solely men (the difficulties of engaging men in
which first time fathers could be supported in acting prevention work can be partly overcome if the
respectfully and responsibly and in non-violent ways men are engaged with their partners, as
through the various phases of starting a family. couples, rather than as individuals)
The activities undertaken included: • Promote relationship equality – by providing
education on gender roles, balancing work and
• A literature review investigating family
family, and the equal capacity of men and
violence prevention work with men, the
women to care for infants
challenges of engaging men in family violence
prevention, and programs targeting first time The current Baby Makes 3 project (phase 2)
fathers represents an implementation of the findings from
phase one. It applies the VicHealth framework to a
• A review of services engaging first time fathers
specific target group: men and women undergoing
• Interviews with first time fathers investigating the transition to parenthood, a time when their
their understandings of gender roles and lifestyles and relationships are undergoing significant
gender relations during the transition to change.
parenthood
Baby Makes 3 – Project Report 6Baby Makes 3
2.3 Why target first time parents?
The transition to parenthood can be a time of great between men and women. There are, therefore, two
joy. Yet it is a time of major lifestyle changes as additional fundamental reasons why it is important to
women and men transition into their new roles of engage first time parents in primary prevention
‘mothers’ and ‘fathers’ and become acquainted with activity.
the stress, difficulties and expectations associated
Firstly, the transition to parenthood is a key time for
with looking after a new born baby.
engaging men. It is a specific time in men’s lives when
During this time it is inevitable that couples’ they are in contact with health services and are open
relationships will undergo a significant shift. Whilst to receiving information and skills development
many couples find that becoming parents brings them (O’Brien & Rich, 2002). It represents a ‘window
closer together, others may experience a significant period’ where men are accessing support and
period of relationship decline (Twenge, Campbell, & focussing on family relationships (King, 2001 & 2005),
Foster, 2003). This change in couples’ relationships is during which it is possible to promote alternate
particularly evident following the birth of a first child models of masculinity based on the model of men as
but may go completely unnoticed by first time carers and nurturers of infants. As such, it provides a
parents who are primarily focussed on the near real opportunity which does not readily present itself
overwhelming task of caring for a baby. As a result, during other life stages.
relationship changes during the transition to
The second key reason why it is important to engage
parenthood can lead to significant impacts on the
first time parents in primary prevention activity is
long term quality of the relationship (Lawrence, et.al.,
that the transition to parenthood is a time when
2008).
gender roles and relations are changing. A recent
The transition to parenthood is also a time when briefing paper from the Australian Institute of Family
women are particularly vulnerable to violence Studies (Parker & Hunter, 2011) identified attitudes
(VicHealth, 2007). Family violence is often seen to connected with gender and gender roles as the key
intensify during pregnancy and in the period factor affecting relationship satisfaction across the
following the birth of a child (Dept. of Victorian transition to parenthood. These attitudes are heavily
Communities, 2007; Taft, 2002; Gielen, et.al, 1994) influenced by the gendered norms and expectations
and can have significant effects on child development that accompany the roles of ‘mother’ and ‘father’
(Doss, et.al., 2009). There is a wealth of research (Koivunen, et. al., 2009). Attitudes to gender roles
showing a wide range of impacts on children have been shown to become more traditional during
including psychological and behavioural impacts, the 12 months following the birth of a child (Katz-
health and socioeconomic impacts, as well as impacts wise, Priess & Hyde, 2008), so it is undeniably a time
connected to the inter-generational transmission of when gender equality is directly relevant to the lived
violence (Richards, K., 2011; Russel, et.al., 1999; Erel experience of first time parents.
& Burman, 1995; Sarkadi, et.al, 2007). So preventing
The transition to parenthood, therefore, presents a
violence during this key risk period is critical for both
major opportunity to engage and work with both men
women and children’s wellbeing.
and women, to challenge traditional attitudes to
But the primary prevention of violence against gender roles, and to promote gender equality during
women is about far more than just responding to risk this key life-stage in which gender roles are shaping
factors. It is about creating cultural change, the level of equality in relationships.
particularly in relation to the key theme for action –
promoting equal and respectful relationships
Baby Makes 3 – Project Report 7Baby Makes 3 2.4 Gender roles and equality during the transition to parenthood A generation ago, in Australia, our notions of fathering, there is also reason to suggest that motherhood and fatherhood were heavily influenced traditional notions of parenthood continue to exert a by what has come to be known as the ‘traditional’ powerful influence on how men and women model of family. Under this model, a father’s main approach and negotiate parenting roles (Berlyn, Wise role was to be a good economic provider – a & Soriano, 2008; Wall & Arnold, 2007). The traditional ‘breadwinner’ – and to work outside the home, while model of family still has considerable bearing on how a mother’s role was to be responsible for all the parents think about their roles (Hatten, Vinter, & unpaid work inside the home. It was not expected Williams, 2002). Our definitions of parenthood may that men would undertake more than a minimal role be changing, but the role of ‘mother’ and ‘father’ in the care and nurturing of children, which was remain stereotypically gendered (Russell, et.al., considered to be the natural domain of women. 1999). In contemporary Australia, however, the traditional While many men appear more visibly involved in child family is becoming far less common. The past care (it is not uncommon to see fathers out by generation has seen the emergence of a new ‘shared- themselves, or with their partners, pushing strollers parenting’ model of family, characterised by or carrying young babies) the available Australian increasing expectations of fathers’ involvement in evidence suggests there are still large differences childcare and household tasks, and greater equality between the amounts of time mothers and fathers between men and women. And while the majority of spend with children, and the types of care activities Australian fathers continue to define their role with they engage in (Berlyn, Wise & Soriano, 2008). This reference to ‘breadwinning’ there is, without doubt, has significant bearing on the level of equality within an increased expectation that contemporary fathers a relationship, and between men and women more will be more involved in the lives of their children generally. than men of previous generations (Berlyn, Wise & Soriano, 2008). Caring for children This change has been parallelled by an increasing The most recent statistics from the Growing Up in recognition of the developmental benefits for Australia: Longitudinal Study of Australian Children children of positive father involvement. It is now (LSAC) research shows a considerable difference in widely recognised that fathers have a significant the amount of hours children spend alone with their impact on child development outcomes, and there is father compared to their mother (AIFS, 2011). On substantial literature that establishes a number of average, fathers spend just 30 minutes alone with important ways in which positive father involvement their babies on weekdays, compared to mothers’ 5.8 can produce favourable cognitive, emotional and hours. On weekends, fathers spend more time with social development outcomes for children (Allen & their baby, but the actual time they spend alone with Daly 2002; Flood, 2003). However, it is important to their baby increases, on average, only 12 minutes to a establish that this is not because of any ‘unique’ total of 42 minutes per day. contribution that men make to parenting, but rather In relative terms fathers are rarely alone with their because of the increased capacity for caring and children, implying that fathers do not undertake child nurturing that father involvement brings to families care in a way that relieves women of responsibility. (Flood, 2003). And as Craig (2006) points out, men typically join Despite indications that our notions of family have their partners as ‘helpers’ in the task whilst mothers significantly shifted to place greater value on involved continue to carry the burden of responsibility for Baby Makes 3 – Project Report 8
Baby Makes 3
managing care. This also has potential effects on other household work such as cleaning. Women
father child relations, for if fathers are rarely alone also spent almost two and a half times as long on
with their children they are not forging independent food preparation and clean up, despite men doing
bonds with their children. more cooking than in the past.”
The other key observation from the LSAC data is that With regard to the transition to parenting, Baxter,
the time that fathers and mothers spend with their Haynes & Hewitt (2008) demonstrate that having a
children each day, varies very little during the first 9 baby dramatically increases the time spent on
years of life, with the only significant change being a housework for new mums, but has only minimal
reduction in mum’s hours when the child begins impact on the hours spent on housework for new
school (Baxter & Smart, 2010). This illustrates that the dads.
initial pattern of involvement that is established in And again, according to the Australian Bureau of
the months after birth can easily become entrenched, Statistics (2009):
and that if active father involvement is to be
“In 2006, mothers aged 20 to 49 years in couple
encouraged, then it needs to be encouraged early on.
relationships spent an extra 7 hours per week on
The transition to parenthood, then, is a key time to household work than those without children,
be engaging in a conversation about gender roles and (whereas) fathers aged 20 to 49 in couple
equality. relationships spent roughly the same amount of
It should come as no surprise that on average, time on domestic activities compared with those
mothers spend much longer than fathers in absolute without children.”
time caring for children. However, there are further Of course, caring for children and housework are not
significant differences in the type of care performed the only measures of relationship equality, but they
by mothers and fathers. Fathers spend more of their are important components, nonetheless. The Human
time involved in interactive care (i.e. talking, playing, Rights and Equal Opportunity Commission identifies
etc…) whereas mothers spend the greater proportion the widespread acceptance of traditional gender roles
of their time on physical care (i.e. bathing, feeding, in parenting as a key factor in explaining why
dressing, etc…)(Craig, 2006). The child care tasks in expectations of gender equality in terms of work and
which men mostly engage are arguably the more ‘fun’ family are not being realised (Squire & Tilly, 2007).
ones, which imply that a father’s time with children is The transition to parenthood is a key time when
less like ‘work’ than is a mother’s time. these gender disparities are emerging.
The transition to parenthood is a time when men and
Housework
women are negotiating new roles and responsibilities,
The dominance of traditional gender roles can also be and one of the greatest factors influencing this
seen in the vast inequalities in the amount of negotiation is new parents’ assumptions about what
housework undertaken by men and women. it means to be a ‘mother’ and ‘father’.
According to the Australian Bureau of Statistics
(2009):
“While men are doing slightly more household
work than in the past, in 2006, women still did 1.8
times as much as men. Although women are
spending less time cleaning and doing laundry, they
still spent almost six times as long on laundry as
men in 2006, and more than three times as long on
Baby Makes 3 – Project Report 9Baby Makes 3
2.5 The construction of fatherhood and motherhood
Many men clearly want to be involved in their number of men feel that a father’s involvement in,
children’s lives and invest heavily in their family and responsibility for, his children’s wellbeing should
relationships, yet the most recent statistics indicate be equal to that of mothers (Hatten, Vinter &
that despite most men expressing support for a Williams, 2002) and ultimately, these gendered
shared-parenting model of family, there are patterns of parenting are a major constraint on
substantial gaps between attitudes and actions. fathers’ interactions with children (Flood, 2003).
The factors that determine the level of father This understanding of fatherhood is reflected in the
involvement include the amount of paid employment approach of many services that tend to engage
undertaken, personal motivation, and the quality of fathers as a ‘support’ person, rather than as an
the relationship between mum and dad. However, actively involved parent. Engaging fathers in this way,
the most fundamental factor relates to how a father’s as a ‘support’ for mothers, only reinforces traditional
role is socially constructed and understood. As Berlyn, gender norms and can give permission for men to
Wise and Soriano (2008) explain: avoid responsibility for childcare and, by extension,
“Social discourses surrounding involved and housework.
traditional constructions of fathering can be Conversely, the same argument can be mounted with
understood as the overarching context shaping
respect to mothers. The belief that women are
how contemporary men practice fathering.
naturally and instinctively better carers than men has
Fatherhood and motherhood have historically been
played a major role in the delineation of parenting
defined dichotomously in terms of contrasting and
roles between mothers and fathers. Proponents of
complementary roles, identities and traits (that is,
mothers as natural carers speak of a bond that is
the ‘breadwinner’ father and ‘stay-at-home’
created between mother and child through childbirth,
mother). These broad stereotypes deeply
penetrate cultural scripts about parenting and of a ‘maternal instinct’ and of a capacity for patience
affect (consciously and subconsciously) how and sympathy. These widely held beliefs inevitably
parenting is performed and constructed at place mothers in the position of gatekeepers with
individual, interpersonal and institutional levels. regard to the tasks of parenting and caring within
Traditional ideas about parenting affect men’s families (Goward, et al. , 2005).
predisposition and ability to be involved parents,
Maternal gatekeeping is deeply rooted in women’s
and women’s ability to let men be more
profoundly felt obligation to care for their children
involved….”
(Doucet, 2004). For example, the vast majority of
A common view of fatherhood is that fathers do not mothers say they are comfortable taking on the bulk
have the natural ability that mothers have to care for of childcare responsibility while their husband is the
and nurture children. It is a view that, whilst not main provider (Hatten, Vinter & Williams, 2002).
denying that fathers make an important contribution Similarly, mothers are major contributors to the
to the upbringing of children, argues that a father’s decision for some families to adopt a pattern in which
contribution is fundamentally and inherently different fathers are significant caregivers (Russell, et.al.,
to that made by mothers. 1999). Indeed, if mothers are not supportive of
Unfortunately, this view of fatherhood is common. increasing the involvement of their male partners,
There is a widespread belief in society that traditional new fathers can experience difficulty in finding the
gender roles are rooted in the natural abilities of men time and space to interact with their babies.
and women (Hatten, Vinter & Williams, 2002). A Understandings of what it means to be a ‘mother’
product of this belief is the fact that only a very small
Baby Makes 3 – Project Report 10Baby Makes 3
and a ‘father’ are integral to the structuring of family The idea of fathers making a unique contribution to
roles. their children is a popular belief that many men (and
women) support and are likely to respond positively
The notion that the roles of mothers and fathers are
to. But in order to argue that the distinctive
largely determined by the natural ability of women
contribution of fathers is desirable and valuable, we
and men is pervasive but it is simply not supported by
do not have to make the further claim that this
the evidence. Yes, it is true that we can observe
contribution is unique and exclusive to men. This
different parenting styles between men and women,
serves only to ensnare families in traditional
but these gender differences in parenting emerge in
gendered patterns of relating, that more often than
response to societal pressures and expectations –
not reflects a gendered power imbalance. Promoting
they are not based on biology (Flood, 2003). Fathers
gender equality demands that we must instead focus
do tend to exhibit more traditionally masculine
on the reality that gender does not play a part in an
qualities in their caring, but men and women are
individual’s capacity to care for children, and that
equally capable of caring for children (Flood, 2003;
men can be caring, loving and nurturing, to the same
Doucet, 2004). Fathers’ contribution to parenting is
degree to which women can be caring, loving and
distinctive, but not unique (Flood, 2003).
nurturing.
Baby Makes 3 – Project Report 11Baby Makes 3
2.6 Maternal Child Health – a key setting for primary prevention
The most accessible and appropriate setting for come to be culturally understood as a woman’s rite of
engaging first time parents in primary prevention passage into motherhood. Anecdotal evidence
work throughout Victoria is undoubtedly the suggests this is a common dynamic in new parent
Maternal Child Health Service. In local governments groups throughout Victoria, illustrating the powerful
throughout Victoria these services play a central role influence that traditional gender roles continue to
in providing all families with children, from birth to exert over contemporary families.
school age, on-going primary health care to improve
So although Maternal Child Health Services are surely
their health and development. For first time families
the most appropriate setting for engaging first time
in particular, the Maternal Child Health Service is an
parents, a pressing issue relates to just how this key
important source of knowledge, skills and support.
target group is engaged. A fundamental challenge for
The service is in regular contact (through home visits
Maternal Child Health is to develop ways of engaging
and centre-based appointments) with new families,
new families that avoid traditional gender norms and
especially during the early months of parenthood.
promote gender equality.
In addition to the regular visits and appointments, a
It is completely fitting that after the birth of a child
key service provided by Maternal Child Health is the
the wellbeing of women and children should be of
formation of ‘New Parent Groups’. These groups are
paramount importance and that this be where
coordinated and facilitated by Maternal Child Health
Maternal Child Health services are rightly focussed.
nurses and run weekly, over five to six sessions. All
But it is worth considering how the structure of these
new parents within a local catchment area are invited
services may reinforce traditional gender roles and
to attend a group when their baby is approximately
have unintended consequences for the level of
four to eight weeks old, the purpose being (from
equality between mothers and fathers.
Edgecombe, et.al., 2009) to:
The pervasive influence of traditional gender roles
• Enhance parental and emotional wellbeing
cannot help but influence the way workers and
• Enhance parent child interaction services engage with families (Berlyn, Wise & Soriano,
• Provide an opportunity to establish informal 2008). And whilst, to some extent, this is unavoidable,
networks and social supports Maternal Child Health nurses and health
• Increase parental confidence and professionals in general must remain mindful of the
independence in child rearing. risk of reinforcing traditional gender roles and
sustaining gendered power inequalities between men
Whilst the new parent groups are aimed at both and women, remembering that this has been
mothers and fathers, in reality it is mostly mothers identified as the fundamental social determinant of
who attend, and informally the groups are known as violence against women.
new ‘mums’ groups. It is rare for fathers to attend.
This is, in part, due to the timing of the groups – The ecological approach to understanding violence
usually during the day, when many men are at work provides importance guidance here. The cultural
and unable to attend. But the absence of men from change necessary for preventing violence before it
the first time parents groups is also a reflection of the occurs is best achieved through a multi-level
gendered expectations about whose role it is to care approach of mutually reinforcing strategies, where
for a baby. Many men, for example, perceive these activity at the individual level is complemented by
groups as being exclusively for new mums, whilst the activity at the community level. This is the primary
mums, themselves, can be protective of what has prevention approach adopted by Baby Makes 3.
Baby Makes 3 – Project Report 12Baby Makes 3
2.7 Rationale for Baby Makes 3
The primary prevention of violence against women is following the birth of a child. Current programs for
focussed on preventing violence before it occurs, with first time parents focus on practical aspects of caring
a key theme for action being the promotion of equal for a baby and, to a lesser extent, adjusting to
and respectful relationships between men and lifestyle changes, but they pay scant attention to the
women. One approach to primary prevention, then, is nature of the changing relationship between mum
to address the gendered inequalities in terms of work and dad. There is a clear need then, for some form of
and family that present during the transition to relationship education for first time parents, and this
parenthood. education should take the form of raising awareness
of the gendered norms and expectations that
Despite increasing expectations of men’s involvement
accompany the transition to parenthood and the
in childcare and housework tasks, the roles of
ways of responding to these changes that lead to
mothers and fathers in contemporary Australian
healthier relationships based on equality and respect.
families remain stereotypically gendered. It is this
widespread acceptance of these traditional gender The Baby Makes 3 project has responded to this need
roles in parenting that is a key factor in explaining by developing an innovative and promising approach
why expectations of gender equality in terms of work to primary prevention, that focuses on raising
and family are not being realised. awareness of the importance of maintaining equal
and respectful relationships during the transition to
The transition to parenthood provides a major
parenthood, and in a way that provides first time
opportunity to engage women and men, in particular,
parents with practical strategies for doing so.
in the work of primary prevention, to challenge
traditional attitudes to gender roles, and to promote
gender equality. Maternal Child Health Services are
the ideal setting in which this work can take place.
However, current services fail to address the
relationship changes between men and women
Baby Makes 3 – Project Report 13Baby Makes 3
3. Project Description
Following the initial research and needs analysis that
was undertaken during phase one of Baby Makes 3,
Subsequently, the project adopted an ecological
the second phase of the Baby Makes 3 project began
approach that would entail working with first time
in January, 2009. Baby Makes 3 was envisaged as a
parents and the organisations that support and
three-year project addressing the primary prevention
interact with them, and as much as possible,
of violence against women, focussing on first time
integrating with and building on existing services.
parents and the organisations and services that
Action theme one from the framework document –
support them. The project was located in the City of
promoting equal and respectful relationships
Whitehorse (in the eastern metropolitan region of
between men and women – was identified as a
Melbourne) and began as a partnership between the
priority on which to concentrate activity.
following:
Significant energy was invested in the program
• Whitehorse Community Health Service
planning stage of the project to develop project
• The City of Whitehorse Maternal Child Health objectives and proposed activities, and from these,
Service identifying a number of expected impacts. Figure 2 –
• Birralee Maternity Service1 at Box Hill Hospital the program logic for the Baby Makes 3 project –
A project coordinator was employed to coordinate shows the links and relationships between each of
and implement the project and a project reference these components of the planning framework.
group was established, consisting of representatives
from the partner organisations, to assist in guiding (Note: the expected impacts shown in fig.2 are the
the project. impacts that were envisaged during the planning
process. A fuller identification of project impacts is
Being the first project of its kind, anywhere in the
provided in sections 4 and 5, detailing the project’s
world to focus on addressing gender role equality in
evaluation activities and findings.)
couples during the transition to parenthood Baby
Makes 3 had no existing examples of successful
primary prevention work with first time families from
which to guide the planning process and project
activities. Instead, the project planning drew heavily
from the VicHealth (2007) framework, Preventing
Violence Before it Occurs to develop its approach and
priorities.
1
Originally, it was planned to locate some of the project
activity at Birralee Maternity Service, however, due to
organisational restraints, Birralee was unable to take part
in phase two of Baby Makes 3
Baby Makes 3 – Project Report 14You can also read