ACT ON AXIAL SPA: A GOLD STANDARD TIME TO DIAGNOSIS - GET AXIAL SPA DIAGNOSED FAST. FIND OUT MORE AT ACTONAXIALSPA.COM
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Act on Axial SpA:
A Gold Standard
Time to Diagnosis
Get axial SpA diagnosed fast.
Find out more at
actonaxialspa.com
Campaign fully
funded by UCB.
“Aged 17, I saw a rheumatologist.
I had been in pain for five years,
and I was exhausted. I could see
no hope of living in any other way.
Today, with a diagnosis,
I’m living my best life.”
Bethany
Photograph by: Jonathan Blackham
A Gold Standard Approach
Contents
Introduction from Dr Dale Webb 4
Calling Time on Delay – A Gold Standard Approach
Delayed diagnosis of axial SpA and its impact 6
The patient journey to diagnosis: sources 8
of delay in axial SpA
The roadmap to reducing delay to diagnosis 9
Driving change 10
Helping someone with inflammatory back pain to recognise 12
that it could be axial SpA and feel confident about the
actions they should take
Ensuring that patients who present at primary and community 16
care with potential axial SpA are appropriately identified and
urgently referred to rheumatology
Ensuring direct referral to rheumatology for patients with 18
suspected axial SpA attending secondary care services
Ensuring quick and accurate diagnosis 20
of axial SpA in rheumatology
Our supporters 22
Glossary of terms 24
References 25
©Copyright NASS | Published June 2021
This report should be cited as follows: Webb D, Swingler L, Barnett R, Sengupta R, Marshall L,
Hamilton J, Zhao S & Gaffney K. Act on axial SpA: A Gold Standard time for the
diagnosis of axial SpA (2021). London: National Axial Spondyloarthritis Society
3
Calling Time on Delay
– A Gold Standard Approach
In July 2019, I was in Parliament standard approach in collaboration anywhere in the world. It contains
for a meeting with parliamentary with clinicians. I was heartened by information and diagnosis support
officers of our newly formed how positively the idea was received, tools for the public, including an online
and developed a growing sense that symptom checker, as well as newly
All Party Parliamentary Group
a Gold Standard approach might created and curated resources for
(APPG) on axial SpA.
galvanise efforts to improve diagnosis healthcare professionals (HCPs),
They asked me to explain all of the in axial SpA. which guide them through research
reasons for the delay to diagnosis in articles, best practice examples,
Dr. Sengupta announced our quality improvement tools and case
axial SpA and to offer a route map of
ambitious goal at a meeting of the studies for each of our four solutions
solutions to address them. I left the
meeting feeling that I hadn’t answered APPG in January 2020, and in July as we follow the patient journey.
their questions satisfactorily. we launched a national consultation
process to engage patients, clinicians, We are publishing this report at a
I reflected on the literature, where
commissioners and policymakers, time when the UK is beginning to
studies on delayed diagnosis tend to
seeking their response to a document emerge from the Covid-19 pandemic.
talk about ‘factors associated with
we developed to set out our ideas. In England, the Best MSK Health
delay’, but what they don’t typically
The 202 responses to the consultation Collaborative has been established
do is follow the journey of the person
confirmed that we were on the right to restore and improve MSK
living with axial SpA to understand
track and led us to develop more services and reduce the variation
that journey from the moment of
specific proposals which we began to in service provision. One of the
symptom onset to diagnosis.
test out in the early part of 2021. My collaborative’s outputs is a new axial
With that realisation in mind, grateful thanks to all of those people SpA pathway and we were involved
I approached two of our medical who have contributed in various ways in its development. Act on axial
advisors, Prof. Karl Gaffney and to the consultation and programme SpA will encourage the widespread
Dr. Raj Sengupta, and we worked development process, culminating in implementation of the pathway in
together to map out the delay to a consensus development workshop order to achieve earlier diagnosis.
diagnosis from a ‘follow-the-patient’ in May 2021. The APPG on axial SpA will continue
perspective, identifying four broad to press the case for early diagnosis
sets of delays. We then created a set This report outlines our final set of and raise the profile of the condition
of proposals to address each of these, proposals to achieve a Gold Standard within Parliament. In Scotland, we
and wondered what quantum of time of one year, under the campaign continue to work through the Cross
to diagnosis might be achievable if our name Act on Axial SpA. We will work Party Group on MSK Health, in
proposed solutions were implemented closely with people living with axial Wales we will work with the newly
effectively. We concluded that it SpA, primary and community care, established MSK Pathway Steering
should be feasible for someone to be secondary care, professional bodies, Group and in Northern Ireland we will
diagnosed with axial SpA within commissioners, Parliamentarians and seek opportunities to engage the
12 months of symptom onset, and set policymakers as our campaign seeks administration.
out to develop a written proposal for a to focus and streamline efforts to
My heartfelt thanks to those
Gold Standard time to diagnosis with a achieve earlier diagnosis. The report
organisations that have given their
target of one year. set out proposals for programmes
support to this document; over the
addressing public awareness of axial
I then approached colleagues at coming months we will call for every
SpA, healthcare practitioner education,
UCB who shared our aspirations and NHS organisation and relevant
referral pathways, and service quality
emerging strategy and encouraged professional body to endorse
improvement in order to improve
me to consider a five year timescale it and commit to supporting its
patient experience, diagnosis and
in which we could develop a Gold implementation. My thanks to the
outcomes.
Standard proposal and implement Chair and Co-Chair of the APPG -
its recommendations in full. Spurred The campaign website, Tom Randall MP and Lord Campbell
on by the possibility of a larger actonaxialspa.com, provides an online Savours – former APPG Chair,
programme of work that would have resource which we hope will become Derek Thomas MP and all of the
the potential for significant impact, we the largest and most comprehensive Parliamentarians who are supporting
began to test out the idea of a gold resource on axial SpA diagnosis this work.
4
A Gold Standard Approach
Years to diagnosis
The current
average delay to
diagnosis from when
symptoms start is
8.5 years, during
which irreversible
damage to the spine
may have occurred.
I want to acknowledge the
phenomenal leadership and
vision of our clinical collaborators
Prof. Karl Gaffney and Dr. Raj Sengupta,
and also thank Dr. Stephen Zhao
“As an MP living with
and Rosie Barnett for their incredible
help and support on the background
axial SpA, I am excited
literature and documentation and
Nick Clarke who provided a patient to see this programme
come to life. This will be
perspective. This programme would
not have been possible without the
outstanding and steadfast support of
UCB whose commitment, passion and
insight has been incredibly energising.
the springboard to a better
Finally, I want to thank the outstanding
team at NASS who have worked future for many young
tirelessly for the best part of a year to
bring this ambitious programme to life, people and a vehicle to
effect real change.”
and in particular Dr. Lisa Swinger and
Liz Marshall. Thank you!
Dr. Dale Webb, FRSA, FRSPH Tom Randall, MP
CEO, NASS
5
2021 In the Know
Delayed diagnosis of axial SpA and its impact
Axial spondyloarthritis (axial SpA) is a life-long inflammatory condition that primarily affects the
spine and sacroiliac joints. The term axial SpA encompasses both ankylosing spondylitis (AS),
where clear structural changes to the spine can be observed via x-ray, and non-radiographic
axial spondyloarthritis (nr-axial SpA) which is diagnosed from other clinical features and magnetic
resonance imaging (MRI) (1). The fact that cases present differently and may require different
diagnostic approaches to confirm the disease is one of the first clues as to why diagnosis of this
condition can prove challenging.
Axial SpA is more common than Sadly the current time to diagnosis that the disease had a significant
people realise, affecting 1 in 200 in the UK averages 8.5 years from societal impact, due to economic
adults in the UK, which is more than symptom onset (13) despite various factors such as work disability and
the number of people with multiple guidelines and recommendations healthcare cost. Diagnostic delay was
sclerosis and Parkinson’s disease to improve referral of patients with consistently related to a higher risk
combined (2, 3). The primary symptom chronic lower back pain, and two of work disability or unemployment
is chronic lower back pain, for which recent systematic reviews have and associated with job loss (8).
between three and seven million GP found significant delays to axial SpA Specifically, one study in Ireland
consultations take place each year in diagnosis worldwide with a global demonstrated that unemployment
the UK (4), therefore it is perhaps not mean of 6.7 years (13-21). This delay rose from 20% among people
surprising that this symptom alone is unacceptable. Axial SpA typically diagnosed with axial SpA within four
does not immediately trigger thoughts starts in the second or third decade years, to more than 40% among those
of axial SpA. of a person’s life, often derailing hopes with a delay of over 10 years.
and dreams at a critical time for
1 in 200 people attempting to establish careers and Several factors have been
independently associated with a
relationships (16). A delayed diagnosis
in the UK have during these formative years can longer diagnostic delay: including
female sex, HLA-B27 negativity, lower
axial SpA making it therefore be extremely disruptive.
education levels among patients,
Some people report not feeling
more common than listened to or believed about their prior diagnosis of mechanical back
symptoms, while others feel helpless pain, presence of uveitis, psoriasis
MS and Parkinson’s and withdraw from care completely, or enthesitis and young age of
combined. leading to further diagnostic delay symptom onset (18, 21-24). Presence
(17). People with delayed diagnosis of peripheral arthritis and IBD have
People with axial SpA also often may also suffer from a less favourable been associated with earlier diagnosis
experience other symptoms as part response to treatment and worse and treatment (13, 25, 26) leading
of their condition, such as fatigue, outcomes in disease activity, to better outcomes and treatment
morning stiffness, sleep disturbance fatigue, function, spinal mobility and responses (18, 19). The shorter time to
and reduced function/mobility radiographic damage to the spine diagnosis in individuals with peripheral
(5, 6), as well as other musculoskeletal (8, 18-20). These individuals also musculoskeletal manifestations
manifestations (hip or hind foot experience difficulty sleeping and is likely due to the fact that GPs
arthritis, enthesitis, dactylitis and have a higher prevalence of mental have been consistently prompted
extra-skeletal manifestations health and psychosomatic disorders via the early arthritis initiative to
including acute anterior uveitis (AAU), (20). One study demonstrated refer patients with swollen joints to
inflammatory bowel disease (IBD), impaired spinal mobility to be twice as rheumatology (13, 25, 26). This reflects
and psoriasis in one-third of patients high in individuals with a diagnostic the impact that educational tools
(7). All of these symptoms can impair delay of over six years, in comparison can have on improving early referral
quality of life further by adding to individuals diagnosed in less than to rheumatology for individuals with
considerable additional physical, six years (8). A recent systematic suspected inflammatory arthritis.
emotional and economic burden. It review of the literature found that
is therefore critical that individuals Evidence emphasises the importance
people with delayed diagnosis also
receive the care that they need as of recognising the condition early.
had a greater likelihood of depression,
soon as possible to improve their We know that targeted awareness-
negative psychological impacts,
quality of life (8-12) and long-term building and education can positively
work disability, worse quality of life
outcomes. impact time to diagnosis. GPs were
and higher healthcare costs (8) and
found to improve substantially the
6
A Gold Standard Approach
In the UK, people living with axial SpA wait an average (mean) of 8.5 years
to receive their diagnosis (1, 2) This means that there are potentially
thousands of people at any one time who are living with debilitating and
painful symptoms, but with no agreed clinical explanation or treatment path.
Almost
“Parenting my children was 10
times more difficult and I got
very low. Once I’d received
of individuals with my diagnosis and got the right
axial SpA do not treatment, I was able to trek
contact a healthcare along the Great Wall of China.”
practitioner within Poppy
a year of symptom
onset
(2) “My pain became so bad that,
recognition and referral of people
with suspected axial SpA (27, 28)
at times, I couldn’t get out of bed.
after receiving education about SpA,
with one recent multi-centre study
I relied on crutches to remain
demonstrating over 40% improvement mobile. It’s amazing to think of
in referral (27). Equally, among
physiotherapists, good awareness that now. An earlier diagnosis
of the NICE 2017 guidance on axial
SpA and continuing professional
may have prevented all of that.”
development was associated with
better awareness and knowledge of
Rowena
axial SpA features (29).
Evidence suggests that we need to
promote/provide sustained education
and awareness among the public and “Especially for younger people
healthcare professionals - as part of a
broader set of change mechanisms - to
this diagnosis doesn’t mean
ensure that axial SpA is at the forefront your ambitions and goals have
of clinical reasoning. It is therefore
critical that initiatives designed to to disappear. With the right
improve knowledge and awareness
and to ensure early specialist referral medication, and if you build
and diagnosis are embedded and
sustained within care pathways.
healthy habits, it’s possible to
Greater public awareness of axial SpA live the life you want to lead.”
and its wide range of symptoms will
also help to tackle this unacceptable Max
delay to diagnosis.
7
The patient journey to diagnosis
A person with back pain does not Common misconceptions about axial
realise that it might be axial SpA SpA also remain in primary care. The
Oxford Handbook of General Practice
Axial SpA represents a relatively still refers to late stages of axial
uncommon cause of a very common SpA, with a focus on males and late
symptom – chronic lower back pain disease features such as fusion of the
(30). Up to 80% of the population spine and SIJs (42). This perspective
may experience back pain at some persists from historical knowledge of cohort, 48% of people with psoriasis,
point within their lifetime. Thus, many the disease, for example its strong AAU or colitis, 3 months undiagnosed back pain
SpA, lacking awareness of axial SpA, leukocyte antigen B27 (HLA-B27) gene; were diagnosed with axial SpA if using
attribute their symptoms to over- yet up to 25% of axial SpA patients a three-stage evaluation approach
exercise, injury or other life stressors; are HLA-B27 negative (43). Women (clinical evaluation, laboratory results
only two thirds of people with axial are more likely to be HLA-B27 negative, [HLA-B27, CRP] and radiography, MRI)
SpA report contacting a healthcare contributing to the perception that it (46); 69% were diagnosed with axial
practitioner within 12-months of is a predominantly male disease. Also, SpA after the clinical evaluation alone
developing symptoms (31). the presence of radiographic changes, (47). These figures suggest that many
Many individuals attempt to historically critical for identifying opportunities to identify, diagnose and
self-manage their condition until either ankylosing spondylitis (AS), are more treat axial SpA are being missed.
self-management fails or the condition common in males. But we now know
worsens, and they are prompted to Rheumatologist may not have the
that early disease does not usually
seek professional advice (32-34). most up-to-date understanding
display as structural bony changes
Furthermore, those who have sought of axial SpA and appropriate
on radiographs, and ~50-70% of
clinical help but remain undiagnosed investigations
individuals with this non-radiographic
often feel dismissed or unheard by axial SpA are female. Despite this The diagnosis of axial SpA is complex,
the healthcare system and cease to knowledge, a recent study reported whereby individual symptoms or tests
come forward for long periods, as their that GPs still believe that AS is almost in isolation are insufficient to either
disease worsens. exclusively a male disease (35). diagnose or rule out axial SpA; rather
Primary care practitioner may not a combination of axial SpA symptoms,
Person with symptoms suggestive
recognise axial SpA physical examination, appropriate
of axial SpA is not directly referred to
diagnostic tests and imaging should
rheumatology services
People with undiagnosed axial SpA lead to diagnosis. However, not all
usually first present with chronic lower A 2019 APPG inquiry found that only rheumatologists have specialist
back pain to their general practitioners 21% of the 191 clinical commissioning knowledge of axial SpA or feel
(GPs) or other non-rheumatology groups (CCGs) and 99 provider Trusts confident implementing or interpreting
primary care providers. However, had a specific inflammatory back the appropriate investigations,
there is a low level of specialist pain pathway from primary care particularly MRI scans. Just one-
knowledge of axial SpA in primary to rheumatology (44). Without this third of NHS hospitals perform the
care (29, 35-40). Approximately 40% pathway, many cases of unexplained recommended MRI protocol for axial
of people with axial SpA also report chronic back pain may be referred SpA (48, 49). Interpretation of MRI is
seeking treatment pre-diagnosis to orthopaedics or chronic pain also challenging and depends on the
from osteopaths or chiropractors, management services, leading to expertise of the radiologist. A recent
many of whom may not have unnecessary, ineffective treatments study found inconsistencies in the
specialist knowledge on axial SpA or even surgery (45). use of MRI in clinical practice (50)
(41). In addition, in a recent survey of resulting in challenges in interpretating
chiropractors and osteopaths, the Similarly, consultants in MRI in diagnosis (50, 51). However,
principal perceived barrier to onward ophthalmology, gastroenterology consensus recommendations for
referral was reluctance by the GP and dermatology respectively miss MRI use in the diagnosis of axial
to accept their professional opinion axial SpA symptoms in individuals SpA have been published (51). Their
(16). Patients may also find difficulty presenting with AAU, IBD and adoption, supported by training of
conveying their symptoms, and as psoriasis, each of which, as an extra- rheumatologists/radiologists in the
reported in patient interviews skeletal manifestation of axial SpA, interpretation of MRI in the context
(17, 32) have experienced negativity could be indicative of the disease. In of suspected axial SpA, should help
or reluctance from GPs to investigate the multicentre Screening for Axial standardise practice and achieve
further. SpA in Psoriasis, Iritis (AAU), and Colitis consistent, reliable diagnosis (52).
8
A Gold Standard Approach
The roadmap to reducing delay to diagnosis
A national consultation process • First, are the top down or extrinsic commissioning a research study
levers, typically governmental to estimate the full economic costs
Over an 11 month period we undertook
approaches that include legislation, of delayed diagnosis in the UK in
a national consultation process which
regulation and performance order to influence policy makers
included people living with axial SpA,
management systems. In 2019 and commissioners and use in our
healthcare professionals, professional
NASS worked with Parliamentarians Parliamentary lobbying.
bodies, communications experts
to form the axial SpA APPG with
and commissioners. We undertook a • Professional levers include
the specific intention of creating a
scoping literature review, then created education and training, clinical audit,
top down lever that would seek to
a consultation document which peer review and guidelines. The UK
ensure the effective implementation
set out our analysis and proposals has multiple initiatives including
of the NICE Guideline on the
(53). We created a survey and sent regional SpA Academies, the
diagnosis and management of
it and the consultation document National Early Inflammatory Arthritis
spondyloarthritis. Act on axial SpA
to hundreds of organisations Audit and the Getting it Right First
will periodically report progress to
and individuals. We received 202 Time programme.
the APPG.
responses with all respondents
Another way to articulate this is to
supporting the principles behind the • Top down levers are balanced by
propose that interventions are either
proposals and the aspiration for a bottom up levers that tap into the
system focussed or people focussed.
Gold Standard time of one year. intrinsic motivators of clinicians
Some might argue that one or the
that want to provide the best
We had to adapt our consultation other is more important, and indeed
for their patients. In 2019 NASS
processes in light of the Covid-19 the debate about whether behaviour
created Aspiring to Excellence
pandemic and we were especially is shaped more by social structure
to provide rheumatology teams
grateful that clinicians were able or human agency is one that has
with the quality improvement
to remain engaged despite the occupied sociologists since Weber
tools and support to improve
enormous pressures that the and Durkheim in the late 19th century.
care at local level. Most of the
pandemic created on the NHS.
11 hospitals involved are trialling Act on axial SpA draws on both sets
We held a workshop with public
different approaches to reducing of interventions: system interventions
health specialists, journalists and
time to diagnosis and may provide including referral pathways to simplify
documentary makers and other
examples of best practice as the and standardise care, and the use
communications experts to develop
campaign unfolds. of automation in electronic patient
our thinking about public awareness
records, and people interventions
campaigning. We invited a group • Economic levers such as
including an online symptom checker
of stakeholders to comment on a incentives, sanctions,
for those with potential axial
‘concept note’ for a primary care competition, drug pricing
SpA and checklists for staff in
champions programme. In May 2021 and patient choice are
secondary care services.
we held a consensus development used to influence
workshop with 75 stakeholders to commissioning and
share our draft final recommendations clinical behaviours.
and seek their input. Act on axial SpA
is currently
An integrated campaign using
multiple change levers
• There is a wealth of literature
suggesting that the key to creating
sustainable improvements in
healthcare is an integrated whole-
system approach that uses multiple
change levers (54). Act on axial SpA
employs a multi-lever approach,
building on work that NASS has
already begun. The campaign
should, therefore be viewed in a
holistic way.
9
A Gold Standard Approach
Driving change
The Driver Diagram (below) summarises our thinking on the interventions required to ensure that we achieve our goal.
four primary changes that the campaign seeks to achieve, The remainder of this document sets out those proposals in
the strategy to achieve each of them and then the specific greater detail.
In order to achieve We need to
ensure... Which requires... Actions to ensure this happens
this aim...
Greater public awareness of axial Develop public awareness campaigns.
SpA symptoms Use the SPINE acronym and encourage its adoption
Help the person with
inflammatory back pain
to recognise that it might The public can check their
Create an 8-item online symptom checker
be axial SpA and feel symptoms easily online
confident about the
actions they should take Advice is avaiable to the public on preparing for Support patients in preparing for their primary care consultation
their primary care consultation
Create and strong visible leadership for axial SpA through a
Primary Care Clinical Champions Programme
Axial SpA to be higher within clinical
reasoning of primary care professionals
Ensure axial SpA is a core component of CPD in primary care
Ensure that patients Appropriate use of diagnostics
who present at primary Promote the use of the 8-item criteria & SPADE tool
by referrers
care and community
physiotherpay services
Use of IT systems to identify potential
with potential axial SpA Test and roll-out pop-up tools on electronic patient record system
Improve time are appropriately identified
axial SpA among patients with back pain
from symptom and urgently referred to
rheumatology Inflammatory back pain referral
onset to pathways are in place
Promote axial SpA pathway recommended by Best MSK Health Collaborative
diagnosis to a
maximum Secondary care services are aware of axial spa Create a national training programme, co-developed with relevant professional
of 12 months symptoms and how to assess if the patient associations to be implemented at a local level. Promote use of the 8-item
Ensure that patients who merits referral to rheumatology symptom checker & SPADE tool
present at secondary care
services with suspected
Every relevant secondary care service has a
axial SpA are identified Promote the use of appropriate secondary referral pathways,
rheumatology referral pathway and knows
at the first presentation and share best practice across the UK
when/how to use it
and urgently referred to
rheumatology
Every hospital in the UK seeing potential axial Review the status of radiology training in UK for axial SpA and audit the
SpA patients has an inflammatory spinal use of an inflammatory spinal protocol MRI
protocol MRI in place
Ensure quick and accurate Work with professional bodies to ensure updated and expanded training to
Every rheumatologist in the UK is able to improve diagnostic capabilities and case studies
diagnosis of axial SpA in
rheumatology access an axial SpA expert MSK radiologist
in house or via another specialist centre Assess the availability of regional MDTs offering axial SpA virtual imaging to
secondary care across the UK via tertiary referral
All radiologists/rheumatologists are aware Promote the routine implementation of appropriate imaging protocols using
of BRITSpA MRI guidelines the BRITSpA consensus guidelines
10 11Helping someone with inflammatory back pain
to recognise that it could be axial SpA and feel
confident about the actions they should take
The first delay to diagnosis of axial
SpA is late presentation by the
patient to primary care. Improving
public awareness of the condition
Our vision:
and its sign and symptoms, and General public awareness of axial SpA and its symptoms
understanding what to do if one is significantly improved. People with chronic, low-back
has the correct symptoms, is critical pain lasting longer than three months - particularly
to achieving earlier presentation in
those aged 40 and under - are aware that it could be
primary care.
related to axial SpA and are motivated to consult their
Public awareness campaigns GP/primary care professional at the earliest opportunity
We encourage NHS organisations,
and within four months of symptom onset. The public
professional bodies, and private can easily check their symptoms online, feel empowered
and public sector organisations and are aware of the referral pathway if the primary care
to support the Act on Axial SpA professional suspects axial SpA.
campaign which has been designed
to target people who are aged 40
and under in particular. Its aim is
to help people understand the Stories about people who have • Community poster campaign
condition and its symptoms, empower faced a long delay to diagnosis across community centres, GP
people to consult primary care at will be central to the campaign surgeries, leisure centres and other
the earliest opportunity and make communications across all platforms, places that the key audience
clear the referral pathway if the bringing the issue to life. The campaign groups are likely to visit.
primary care professional suspects will adopt a phased test and learn
Phase Two is likely to include a
axial SpA. The campaign will seek approach, to see what works most
concentrated local campaign in
to create a sense of urgency but effectively in terms of messaging
a single area, combining learning
without scaremongering. The core and delivery, and from there will
from Phase One and adding new
components of the campaign make informed decisions regarding
communication tactics such as
strategy are: investment in bigger, more ambitious
outdoor advertising, with a particular
tactics.
• A clear articulation of the emphasis on public transport hubs.
problem: On average it takes over Phase one communications to drive If these tactics result in an increase
eight years for axial SpA to be public awareness will test the act on in rheumatology referrals the
diagnosed. This is too long. Every axial SpA brand and key messaging campaign may be extended to other
year that passes without diagnosis and will include: parts of the UK.
can lead to deeper damage.
• A media relations programme,
• A defined campaign purpose: with an emphasis on the TV,
To reduce the average time to
“At first, I just thought
radio programmes, podcasts and
diagnosis to one year. publications likely to be trusted by I had sports injuries,
our target audience. nothing serious.
• A definition of how we will
achieve our ambition: The • Social media activity targeted by Over the years, I saw
campaign will ensure that the age: Instagram for those under 25s
public recognise the symptoms of and Facebook for 25-45s. doctors, physios and
axial SpA, know what to do next chiropractors who put
• Engaging with social media
and what should happen if the
healthcare professional suspects
influencers to primarily reach the my chronic pain down
under 25s audience.
that they have axial SpA. to sport injuries, growing
• A core campaign concept of pains, or weight issues.”
‘a race to stop the progress of the
condition’ will underpin all of the
Paul
campaign communications.
12A Gold Standard Approach
Delay to diagnosis of axial SpA is
linked to poorer outcomes including
greater functional impairment and
higher prevalence of depression
(8,18,20)
13The SPINE acronym
Axial SpA is a complex condition to
articulate and explain. To be successful
in engaging the public requires a
graduated approach to communication
which takes the audience through an
information journey, as follows:
• State what the condition is and raise
awareness that someone’s back pain
might be axial SpA.
• Set out a small number of key
symptoms that will resonate with the
public and be easy to remember.
• Identify a larger number of symptoms
which have a high degree of sensitivity
and specificity and which provide a
sound basis for recommending that
the person consults primary health
care.
To that end, act on axial SpA has
developed the SPINE acronym, which
sets out the following key symptoms:
SPINE will be widely used in the act on axial SpA campaign and
we encourage all supporting organisations to adopt the acronym in
awareness raising work with the general public.
14A Gold Standard Approach
An eight-point set of inflammatory back pain
criteria and online symptom checker
Did your back pain start before the
1
The campaign communications goes beyond age of 40? YES
media messaging and creates value for
Did your back pain develop
audiences by empowering people to explore 2 gradually? YES
the condition and their symptoms via a new
online resource actonaxialspa.com. On the Has your back pain lasted more than
website, people can use an online symptom 3 3 months? YES
checker. It employs an eight-point set of
inflammatory back pain criteria that combine Do you experience stiffness in your
the three extant validated sets of criteria 4 back in the morning for at least 30
(55-57). If the person gives the correct minutes? YES
response to five or more items (see right) they
will then be given information about consulting Does your back pain improve when
5 you move around? YES
primary care.
Supporting patients in preparing for their Does your back pain improve when
6 you rest? NO
primary care consultation
Actonaxialspa.com will include a range of Do you have pain in your buttocks,
7 which moves from one buttock to the
resources for people to advise them about the
need to book a primary care consultation. It will other? YES
provide a print-out of the symptom checker
Do you wake in the second half of
results - with an explanation for the primary 8 the night because of your back pain?
care professional on the criteria used.
YES
15Ensuring that patients who present at primary
and community care with potential axial SpA are
appropriately identified and urgently referred to
rheumatology
Primary care and community services
have a key role in identifying patients Our vision:
with suspected axial SpA and referring
them directly to rheumatology. Most All patients who present to primary care with suspected
people with suspected axial SpA axial SpA are appropriately identified and urgently referred
will consult primary care in the first to rheumatology, as set out in a local inflammatory back
instance, and around 5% of patients pain referral pathway. Axial SpA is higher within the
with chronic back pain attending
clinical reasoning of primary care professionals, supported
primary care are estimated to have
axial SpA (58). However, people with
by alerts on electronic patient records which prompt
axial SpA frequently report to NASS consideration of axial SpA for appropriate patients. Within
that their primary care professionals England, there is widespread adoption of the Best MSK
failed to identify their axial SpA, Health Collaborative axial SpA pathway.
misdiagnosing it as mechanical pain or
sometimes ascribing psychosomatic
reasons.
Primary healthcare professionals screening for suspected axial SpA of CCGs have specific programmes
report numerous barriers to and referring to rheumatology is low, in place for educating primary care
diagnosing axial SpA, including low and a recent study concluded that professionals about axial SpA (60).
prevalence, the lack of a definitive this group of professionals may not be
diagnostic test, the slow progression giving adequate consideration to axial Consequently, axial SpA is likely to
of the condition and the intermittent SpA in back pain assessments (29). be low within the clinical reasoning
nature of the pain that patients of most GPs and MSK clinicians and
experience (59). Even amongst A recent national inquiry into axial SpA the condition lacks visibility within
MSK physiotherapists, awareness, services in England led by the APPG primary care.
knowledge and confidence in for axial SpA found that only 15%
“At the start of your
GP appointment,
explaining you are really
concerned that you
might have axial SpA is
super helpful, ensuring
you get what you need.”
Dr Daniel Murphy, GP,
Devon, UK
16A Gold Standard Approach
Strong, visible clinical leadership for SpA patients: with an up-skilled checks whether the person is under
axial SpA at local level in primary care primary care workforce, one would the age of 45, and whether they
expect to see a better understanding have previously had back pain. If the
To strengthen clinical leadership and of medication, exercise, fatigue and answer to these is yes, it prompts
visibility for axial SpA in primary care mental health in axial SpA. consideration of axial SpA. It can also
and community services, we will be programmed to alert the GP of
create and support a cadre of clinical Axial SpA as a core component of possible axial SpA if the patient has
champions including First Contact continued professional development had AAU, psoriasis or IBD in the past.
Practitioners, GPs, community MSK
physiotherapists, nurse practitioners Act on axial SpA will work in Widespread adoption of the Best
and others. They will receive partnership to encourage the MSK Health Collaborative axial SpA
prioritisation of MSK as a core pathway
leadership development, training in
component of continued professional
using quality improvement methods,
development within primary care and The Best MSK Health Collaborative
and support to identify and implement
to ensure screening for inflammatory was developed in 2021 by NHS
improvement projects within their local
conditions. The campaign will support England and Improvement and is
healthcare system. They will work
Health Education England’s Primary led by the National Clinical Director,
together in a national learning network
and Community Care Training Hubs, Musculoskeletal Conditions. It seeks
to foster community-building, the
workforce education initiatives in to restore and improve MSK services
exchange of ideas and good practice
NHS Education and Improvement and reduce the variation in service
and they will act as catalysts for
Wales, and NHS Education for provision. One of the Collaborative’s
change.
Scotland. We will promote our online outputs is the development of
Axial SpA clinical champions will be resource, actonaxialspa.com, which an axial SpA pathway. It reflects
active within the wider healthcare brings together a wide range of recommendations in this document,
system, connecting to the national educational resources for primary and is now being promoted to
policy environment. Axial SpA care professionals. The campaign will NHS regions. The campaign will
clinical champions will co-produce disseminate and embed axial SpA promote the widespread adoption
a body of knowledge, methods, resources that are developed through of the pathway and will monitor its
tools and experience and work to the primary care clinical champions implementation through Freedom of
share their learning with primary programme. Information requests.
and community services across
We want to ensure that primary care
the UK, collaborating with relevant
referrers have access to and use
professional bodies. They will promote
appropriate tools: we will promote the
relevant frameworks including the
eight-item inflammatory back pain
forthcoming rheumatology specialist
(IBP) criteria as well as the SPADE
physiotherapy Competency
tool (www.spadetool.co.uk) which
Framework (61).
has been designed to assist medical
Participating clinical champions will professionals define the probability
benefit from enhanced leadership of axial SpA in a patient with chronic
skills and greater confidence in back pain, below the age of 40.
undertaking service improvement
Primary care information systems
work. They will develop their
that can flag patients with suspected
networking skills and enlarge their axial SpA
professional network. They will gain
access to resources and expertise To support primary care professionals
as well as create new resources to identify appropriate patients
for other healthcare professionals. early, we will support the uptake
Their work will directly result in of a pilot project in Bath that has
earlier identification of patients with successfully implemented a tool
suspected axial SpA and quicker on the GP electronic patient record
referral to rheumatology. We also system. Under this pilot, when a
anticipate benefits in terms of better GP types “back pain” the system
primary care management of axial
17Ensuring direct referral to rheumatology for patients
with suspected axial SpA attending secondary
care services
Given the high prevalence of
peripheral and extra-musculoskeletal Our vision:
manifestations of axial SpA,
clinicians across ophthalmology, Patients with suspected axial SpA who present
gastroenterology, dermatology and at a range of services - including ophthalmology,
orthopaedic spinal surgery have a key gastroenterology, dermatology, orthopaedics - are
role in screening undiagnosed patients
identified at the first presentation and urgently
for referral to rheumatology. These
specialists may not be familiar with referred to rheumatology. Relevant secondary care
axial SpA or know how to assess for services should be aware of axial SpA symptoms
its probability. If they do suspect axial and how to assess if the patient merits referral to
SpA, they may reroute the patient rheumatology. Every UK hospital seeing potential
back to the GP or follow a standard axial SpA patients should have a rheumatology
18-week secondary referral route, all of
referral pathway, and all specialists know when/
which adds to delay.
how to use it.
A national training programme
The act on axial SpA campaign will
develop a national training programme
for secondary care services to be It will also create a toolkit to help its use will be promoted through the
implemented at a local level, led by rheumatology teams with the delivery education programme.
rheumatologists and their teams. of the educational package (digital/
It will be developed in consultation online and face to face). There will be Sharing best practice of referrals
with the professional organisations a targeted media and professional
representing these specialist The campaign will collect best
communications programme
disciplines, piloted across the NASS practice examples of relevant referrals/
including presentations, exhibitions
Aspiring to Excellence sites and pathways, creating digital publications
and poster case studies at events.
then refined for national roll-out. We and promoting these widely among
The educational programme will be
envisage that the education package the relevant stakeholder groups
designed with sustainability in mind,
will resonate most effectively through via actonaxialspa.com. It will build
to help ensure that the education
a combination of online access to awareness of the website amongst
of healthcare professionals in these
learning and face to face teaching our target healthcare professional
disciplines can be embedded into local
sessions on site at the hospital base, audiences and ensure the highest
NHS practice.
such as lunch-time seminars on quality data, clinical practice
axial SpA signs and symptoms as Internal referral pathways information and evidence-based best
well as reviews of real case studies practice learning is made available
on delay. The campaign will support To reduce diagnostic delay, it is vital to them to enhance their axial SpA
rheumatology teams with promotional that specialists who suspect axial diagnostic capabilities.
materials to promote the training SpA are aware of and use their
delivery and its key messages. hospital’s internal referral pathway to
rheumatology, rather than sending the
The programme will create a set of patient back to their GP. The campaign
learning tools to raise awareness of will audit this through Freedom of
axial SpA symptoms and to ensure Information requests. Where there
that the condition is on the checklist at are gaps, we will engage with the
first presentation of a new referral. A list relevant CCGs, Locality Networks,
of screening questions to raise during NHS Boards, Local Commissioning
the consultation will also be provided. Groups, hospitals and regional NHS
The programme will include statistics bodies to encourage implementation
on the likely incidence of undiagnosed of appropriate referral infrastructure/
axial SpA among new patient referrals. training. The referral pathway and
18A Gold Standard Approach
“Pain had been my
reality for such a long
time I didn’t know what
was normal. At this
point the rheumatologist
diagnosed me with
non-radiographic
axial spondyloarthritis.
I had mixed emotions.
I was over the moon to
have an answer but
all I really wanted to get
was a diagnosis and
a magic pill to cure me”
Max
Photograph by: Jonathan Blackham
up to
of individuals with
of individuals with IBD patients with acute with psoriatic arthritis
may have axial SpA anterior uveitis (AAU) may also fulfil criteria
(62) may have axial SpA for axial SpA
(60, 61) (63)
19Ensuring quick and accurate diagnosis of axial SpA
in rheumatology
The delays when the patient is being Lack of general awareness of the a more consistent, reliable approach
assessed by rheumatology span term axial SpA among UK radiologists: to diagnosis (51). Radiologists have
several aspects of diagnosis, including survey responses of 269 UK an important role in the diagnostic
the use of biomarkers, the application radiologists found that just 75% were pathway; therefore their engagement
of classification criteria, imaging aware of the term axial SpA and only alongside rheumatologists will
choices and the interpretation of 31% and 25% were aware of the ASAS be critical. The imaging problems
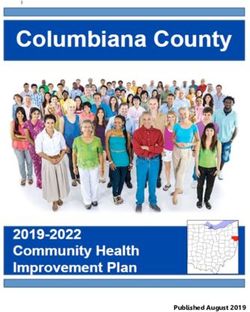
these results (Figure 1). Our solutions definitions of positive MRI for the SI described call for better training of
to help reduce delay are focused joints and spine, respectively (50). rheumatologists and radiologists in
primarily on the issue of imaging the use and interpretation of MRI in
challenges and how these impact a Consensus recommendations for the the context of suspected axial SpA
swift and accurate diagnosis. Some of acquisition and interpretation of MRI in (52). We will also identify and promote
the imaging challenges include: the diagnosis of axial SpA have been best practice examples of NHS Trusts
recently developed by BRITSpA (51). and regional rheumatology/radiology
Inconsistencies in MRI acquisition: just Their national implementation should MDTs that meet to discuss complex
one-third of NHS Trusts perform the help standardise practice and allow for complex and challenging cases.
recommended MRI protocol for axial
SpA (48, 49).
High inter- and intra-observer
variability when assessing
conventional SI joint X-rays (62-67).
Our vision:
Lack of significant improvement in Every hospital in the UK seeing potential axial SpA
reproducibility and performance of patients has an inflammatory spinal MRI protocol
identification of radiographic sacroiliitis in place. Every rheumatologist in the UK is able
after training (62). to access an axial SpA expert MSK radiologist
Lack of agreement around what
in-house or via another specialist centre.
constitutes a ‘positive’ MRI suggestive All radiologists and rheumatologists are aware of
of axial SpA (68, 69) potentially
and use the BRITSpA MRI guidelines.
leading to over-diagnosis or
misclassification if used for diagnostic
purposes without context (68, 70-77).
Imaging
difficulties
• Challenging to assess SIJ
Misleading x-rays/MRI, high inter-/intra-
observer variability
Lack of
biomarkers • Inconsistent use of MRI diagnostic criteria
protocol for axSpA
• CRP lacking sensitivity/ • Classification criteria not
responsiveness intended for use as a
• Not all patients HLA-B27 diagnostic tool
positive • Not validated diagnostic
criteria
Figure 1
20A Gold Standard Approach
graphic on diagnosis issues
Understanding the radiology medical students, foundation and
axial SpA diagnostic landscape specialty HCPs. The campaign will
across the UK support ongoing accreditation training
and voluntary expert additional training
The campaign will work with relevant via the NHS or professional bodies/
national bodies to review radiology third parties. It will provide training
training in axial SpA as well as audit
the use of an inflammatory spinal
materials through online learning, face Average age
to face teaching sessions on-site at of onset
protocol MRI through a Freedom of the hospital and case studies. Using
Information request to hospitals. This the BRITSpA consensus papers (50,
will deliver a full understanding of the 51) the campaign will promote best
current UK curriculum/opportunities on practice for the routine implementation
radiology diagnostics for axial SpA, for of appropriate imaging protocols.
all levels of HCPs. It will also indicate
which hospital sites require an MRI Utilising rheumatology and radiology
protocol update. services with axial SpA expertise
or capacity
Updating radiology axial SpA
diagnostics training curricula Tertiary referral pathways have
also been shown to be valuable.
Act on axial SpA will develop an The campaign will promote tertiary
up-to-date axial SpA MRI training referral centres to assist with
programme, co-developed with interpretation of difficult imaging
rheumatologists and radiologists cases and explore ways to create
and endorsed by the British Society greater access to diagnostic imaging
for Skeletal Radiologists, the British interpretation support across the UK.
Society for Rheumatology and the
Royal College of Radiologists. it will
encourage professional organisations
to update and expand their own
training materials and promote
guidance to reach undergraduate
21Our supporters
This document has been endorsed by key stakeholders in the field of musculoskeletal health, supporting the
vision for a better future for people with axial SpA. You can find a full list of endorsements at
www.actonaxialspa.com
22A Gold Standard
for the diagnosis
of axial SpA
Years for diagnosis of
axial SpA is too long
Go to www.actonaxialspa.com for information and advice
from some of the world’s leading experts on the condition.
Campaign fully
funded by UCB.Glossary of terms
All Party Parliamentary Group (APPG) Enthesitis Multiple sclerosis
All-Party Parliamentary Groups (APPGs) Enthesitis is inflammation of the entheses, Multiple sclerosis (MS) is a condition that can
are informal cross-party groups that meet, the sites where tendons or ligaments insert affect the brain and spinal cord, causing a
relatively informally, to discuss a particular into the bone. wide range of potential symptoms, including
issue of concern. problems with vision, arm or leg movement,
Extant
sensation or balance.
Acute anterior uveitis (AAU) Still in existence
Acute anterior uveitis is an eye condition MRI / magnetic resonance imaging
Extra-musculoskeletal manifestations
caused by inflammation in the front part Magnetic resonance imaging (MRI) is a type
(EMMS)
of the eye between the cornea (the clear of scan that uses strong magnetic fields and
Disease-related characteristics that are not
window at the front of the eye) and the lens. radio waves to produce detailed images of
related to the musculoskeletal system - in
It is also sometimes referred to as iritis. the inside of the body.
axial SpA this includes inflammatory bowel
Ankylosing spondylitis (AS) disease (IBD), psoriasis, and acute anterior Osteopath /osteopathy
See axial spondyloarthritis uveitis (AAU). Osteopaths are allied healthcare
professionals, who are trained in the
Axial spondyloarthritis (Axial SpA) First Contact Practitioners
musculoskeletal (MSK) system and its
Axial spondyloarthritis (axial SpA) is an First contact practitioners (FCPs) are
relationship with other systems of the body.
inflammatory arthritis where the main experts in musculoskeletal health such
symptom is back pain. Axial SpA is an as physiotherapists and osteopaths, who Parkinson’s disease
umbrella term and it includes: ankylosing form part of a primary care practice. FCPs Parkinson’s disease is a brain disorder
spondylitis (AS), where changes to the are usually the first health professional a in which parts of the brain become
sacroiliac joints or the spine can be seen patient will see in a GP practice about a progressively damaged over many years.
on x-ray and non-radiographic axial musculoskeletal complaint.
Peripheral arthritis
spondyloarthritis where x-ray changes are
Generic back pain Peripheral arthritis usually affects the large
not present but inflammation is visible on MRI
About 8 in 10 people have one or more bouts joints of the arms and legs, including the
or you have symptoms.
of low back pain over their lifetime. In most elbows, wrists, knees, and ankles.
Best MSK Health Collaborative cases, it is not due to a serious disease or
Peripheral musculoskeletal manifestations
This new initiative is part of the Pathways for serious back problem, and the exact cause of
In axial SpA, peripheral manifestations
Better Health Programme by NHS England, the pain is not clear. This is called nonspecific
include peripheral joint disease, enthesitis and
will significantly increase the resource to or generic lower back pain.
dactylitis
support MSK service delivery.
Getting It Right First Time (GIRFT)
Psoriasis
Biomarkers Getting It Right First Time (GIRFT) is a national
Psoriasis is an inflammatory skin condition
A biological molecule found in blood, other programme designed to improve medical care
that causes red, flaky, crusty patches of skin
body fluids, or tissues that is a sign of a within the NHS by reducing unwarranted
covered with silvery scales.
normal or abnormal process, or of a condition variations.
or disease. Psoriatic arthritis (PsA)
HCPs
Psoriatic arthritis (PsA) affects joints (such
Clinical Commissioning Groups (CCGs) Health Care Professionals: anyone who is
as the knees or those in the hands and feet),
NHS commissioning is the process of professionally qualified to deliver clinical /
as well as areas where tendons join to bone
assessing needs, planning and prioritising, medical healthcare.
(such as the heel and lower back).
purchasing and monitoring health services.
Health Education England’s Primary and
CCGs operate in England. Psychosomatic disorders
Community Care Training Hubs
A psychosomatic disorder is a physical illness
Chiropractor Health Educations England’s training
which is caused or made worse by mental
Chiropractors are healthcare professionals hubs provide the infrastructure for multi-
health.
who work to help treat problems with the professional training and education in primary
bones, joints and muscles that support the care to support recruitment, retention and Radiography
body (the ‘musculoskeletal system’). return of all staff groups. Radiography is an imaging technique using
x-ray.
Classification criteria HLA-B27/Human leukocyte antigen B27
Classification criteria are standardised HLA-B27 gene Radiographic damage
definitions that are primarily intended to There is a strong association between axial Where changes to the sacroiliac joints and
create well-defined picture of the key shared SpA and the HLA B27 gene. Although HLA B27 spine can be seen on x-ray.
features in the majority of patients with a is present in over 75% of people with axial
Rheumatologist / rheumatology
disease or condition. SpA, only about 1 in 15 people who are HLA
Specialists in the diagnosis and treatment of
B27 positive go on to develop the condition.
CRP conditions which affect the joints, muscles,
A CRP or c-reactive protein blood test is used Inflammatory bowel disease / IBD and bones.
to measure levels of inflammation. Inflammatory bowel disease (IBD) is a term
Sacroiliac joints / SIJs
mainly used to describe two long-term
Dactylitis The sacroiliac joints at the base of the spine,
conditions that involve inflammation of the
Dactylitis is severe inflammation of the finger connecting the spine to the hips.
gut: ulcerative colitis and Crohn’s disease.
and/or toe joints.
SpA Academies
Mechanical back pain
Early arthritis initiative SpA academy is a series of educational
Mechanical back pain arises from structural
The National Early Inflammatory Arthritis Audit events relating to spondyloarthritis for health
changes which may be in the spinal joints,
(NEIAA) aims to improve the quality of care care professionals.
vertebrae or soft tissues.
for people living with inflammatory arthritis,
SPADE tool
collecting information on all new patients Musculoskeletal (MSK)
The SPADE tool is an online tool designed
over the age of 16 in specialist rheumatology Musculoskeletal (MSK) conditions affect the
to assist medical professionals define the
departments in England and Wales. It was joints, bones and muscles.
probability of axial spondyloarthritis.
commissioned by the Healthcare Quality
Improvement Partnership as part of the Uveitis
National Clinical Audit Programme. See acute anterior uveitis.
24You can also read