A systematic review of the associations between care home ownership and COVID-19 outbreaks, infections and mortality - Nature
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Analysis
https://doi.org/10.1038/s43587-021-00106-7
A systematic review of the associations between
care home ownership and COVID-19 outbreaks,
infections and mortality
Anders Malthe Bach-Mortensen 1 ✉, Ben Verboom 2,3
, Ani Movsisyan 2,3
and
Michelle Degli Esposti 1
Social care markets often rely on the for-profit sector to meet service demand. For-profit care homes have been reported to
suffer higher rates of coronavirus disease 2019 (COVID-19) infections and deaths, but it is unclear whether these worse out-
comes can be attributed to ownership status. To address this, we designed and prospectively registered a living systematic
review protocol (CRD42020218673). Here we report on the systematic review and quality appraisal of 32 studies across five
countries that investigated ownership variation in COVID-19 outcomes among care homes. We show that, although for-profit
ownership was not consistently associated with a higher risk of a COVID-19 outbreak, there was evidence that for-profit care
homes had higher rates of COVID-19 infections and deaths. We also found evidence that for-profit ownership was associated
with personal protective equipment (PPE) shortages. Variation in COVID-19 outcomes is not driven by ownership status alone,
and factors related to staffing, provider size and resident characteristics were also linked to poorer outcomes. However, this
synthesis finds that for-profit status and care home characteristics associated with for-profit status are linked to exacerbated
COVID-19 outcomes.
T
he COVID-19 pandemic has disproportionately affected of higher rates of COVID-19 infections and deaths in FP care
people living in residential care, who are estimated to account homes18,19. Although many of these reports are not peer-reviewed
for more than one-third of all COVID-19 deaths1–3. This dis- (located, for example, in newspaper publications), there is a growing
proportionate impact can be understood, in part, in terms of the body of academic research investigating the variation in COVID-19
vulnerability of people residing in care homes and a lack of early outcomes, such as outbreaks, infection rates and mortality, across
intervention and support4,5. However, the structural and institu- care home ownership types20,21. The disproportionate impact of the
tional risk factors exacerbating this crisis are not well understood. pandemic on FP care homes has been hypothesized to be driven
In many countries, adult social care services are delivered by a com- by some of the pre-existing ownership differences in, for example,
bination of for-profit (FP), non-profit (NP) and public providers6. resident vulnerability and staffing, but this evidence has not been
Although there is no universally applicable definition of ‘owner- systematically reviewed and synthesized.
ship’ across different country contexts, FP providers are commonly The COVID-19 pandemic has tested the capability of not only
understood as private companies operating on a FP basis, NPs are individual care homes but also that of commissioning systems in
understood as registered NP or charitable organizations, and ‘pub- which they operate. In many countries, the adult social care sector
lic’ providers are understood as those operated by central or local has had to adapt to substantial austerity measures22,23 at the expense
government. It is well documented that the outsourcing of social of staffing, quality and support, which may have been detrimen-
care has substantially increased the market share of private and, in tal to the capacity of care homes to cope with the pandemic24. As
particular, FP care providers7,8, which has motivated a large body such, the growing body of research on ownership variation across
of research investigating the association between care home owner- COVID-19 outcomes offers an important opportunity to revisit
ship and quality of care9. For example, several systematic reviews ownership-specific variation across care home providers.
on ownership variation among care homes have found that NP and The aim of this living systematic review is to identify, appraise
public providers typically deliver higher-quality services than FP and synthesize the available research on ownership variation in out-
providers10,11, a finding that has since been replicated7,8,12. There is breaks and infections across FP, public and NP care homes for older
no consensus on what organizational and/or behavioral features people and to update our findings as new research becomes avail-
drive these differences. However, a sizable literature has found con- able. A review protocol was registered prospectively on the Open
sistent correlations between, for example, FP ownership and infe- Science Framework25 and on the International Prospective Register
rior staffing qualifications and employment conditions, which are of Systematic Reviews (PROSPERO) (CRD42020218673).
considered important mediating factors9,13–16.
During the COVID-19 pandemic, some have expressed con- Results
cerns that FP providers have failed their residents by prioritizing Search results. Our combined searches yielded 6,434 records,
profits over care, prevention and caution17, resulting in reports of which 5,915 remained after removal of duplicates. In total,
Department of Social Policy and Intervention, University of Oxford, Oxford, UK. 2Institute for Medical Information Processing, Biometry and Epidemiology,
1
Chair of Public Health and Health Services Research, LMU Munich, Munich, Germany. 3Pettenkofer School of Public Health, Munich, Germany.
✉e-mail: anders.bach-mortensen@spi.ox.ac.uk
948 Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/natagingNaTuRE AgIng Analysis
Identification of studies via databases and registers Identification of studies via other methods
Records identified through
Identification
database searches Duplicate records removed Records identified through
(3 November 2020, n = 3,845) (n = 511) citation searching (n = 10)
(6 May 2021, n = 2,589)
Records screened Records excluded
(n = 5,915) (n = 5,815)
Reports not retrieved
Reports sought for retrieval Reports sought for retrieval Reports not retrieved
(n = 0)
(n = 100) (n = 10) (n = 0)
Screening
Reports excluded (n = 70): Reports excluded:
Reports assessed for eligibility Reports assessed for eligibility
No ownership comparison Also identified in second
(n = 100) (n = 10)
performed (n = 45) database search (n = 8)
Not empirical (n = 20)
Wrong outcome (n = 3)
No observational evidence
(n = 2)
Included
Studies included in review
(n = 32)
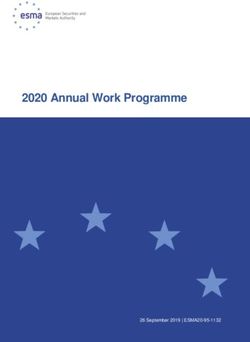
Fig. 1 | Preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 flow diagram79. A total of 32 studies fulfilled the eligibility
criteria.
100 studies were independently assessed in full text. Of these, COVID-19 outcomes. Four studies were published after initially
30 studies were deemed eligible for inclusion. Forward citation being included as preprints29,39,41, and we used results from pub-
searches of included studies from the first search identified an addi- lished versions in the results presented below.
tional two eligible studies. Thirty-two studies were thus included in
this review (Fig. 1). Data sources, time coverage and overlap. Most of the included
research merged multiple data sources on COVID-19 outcomes,
Description of studies. Descriptive characteristics of all included information on care homes and area characteristics to construct
studies are shown in Table 1. Most of the included studies were peer- the dataset. Less than 15% of included studies (four of 32) collected
reviewed publications (27 of 32), with two government reports26,27 primary data on investigated COVID-19 outcomes. The major-
and three preprints or working papers. The unit of analysis across all ity of studies used data routinely reported by care homes to pub-
studies was care homes. FP care homes were the largest ownership lic health departments and other government entities. Almost a
group in all studies that provided detailed sample information. All third of included studies (12 of 32) used data from the Centers for
but two studies28,29 were published in July 2020 or later. Most stud- Medicare & Medicaid Services (CMS), which required American
ies were conducted in the US (25 of 32), followed by Canada (three nursing homes to report COVID-19-related data, including con-
of 32), England (two of 32), Scotland (one of 32) and France (one firmed and suspected infections and deaths among residents and
of 32). Most included studies were cross-sectional, and only three staff42 from May 2020. Providers were encouraged, but not required,
studies included more than one time point in their analysis30–32. to retrospectively self-report COVID-19 outcomes before this date.
Ownership was usually analyzed by comparing FP, public and Supplementary Table 2 provides an overview of data sources and
NP care homes (18 of 32), usually with FPs as the reference category. the time period of dependent variables across all included studies.
Thirteen studies compared FP and NP care homes, in which the Twenty-one studies analyzed self-reported COVID-19 out-
NP category also included public sector care homes, although this comes (confirmed and suspected cases), whereas ten studies only
was not always explicitly described. Two studies focused on private investigated confirmed COVID-19 outcomes. In one study, it was
equity (PE) providers in their operationalization of ownership33,34. unclear whether the investigated outcomes were confirmed or self-
Twenty studies adjusted for whether care homes were chain affili- reported28. All studies that investigated PPE and staffing short-
ated (CA) to investigate COVID-19-related outcomes. ages relied on self-reported outcomes. Most studies investigated
The most investigated outcome was COVID-19 outbreaks (16 of COVID-19 outcomes collected during the time span of March 2020
32), followed by COVID-19-related mortality (15 of 32) and inci- to July 2020, and only two studies analyzed data from later than
dence of COVID-19 infection (14 of 32) among care home resi- September 2020 (refs. 43,44). Most studies investigated outcomes
dents. Six studies investigated staff access to PPE and/or shortage covering a 1–2-month period although five studies investigated a
of PPE31,33–36. Five studies investigated COVID-19-related outcomes period of less than 2 weeks34,35,37,45,46. The findings presented below
among care home staff34,37–40. Most studies investigated multiple thus relate to the first wave of the pandemic.
Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/nataging 949950
Table 1 | Study, sample and outcome characteristics
Study Type of study Publication Research Adjusted Country Main ownership Adjusted Sample Sample size across COVID-19 outcomes
date design results categorization for CA (Y size (care ownership groups
(Y or N) or N) homes)
Bui et al.26 Peer-reviewed September Cross-sectional N US (West Virginia) FP and NP N 123 FP: 95 (77%) Outbreaks (two or more
Analysis
publication 2020 NP: 28 (23%) cases)
Chatterjee et al.45 Peer-reviewed July 2020 Cross-sectional N US (the district of FP and NP N 8,943 FP: 6,473 (72%) Outbreaks (any cases)
publication Columbia and 23 NP: 2,470 (28%)
states)
Abrams et al.80 Peer-reviewed July 2020 Cross-sectional Y US (30 States) FP, NP and public Y 9,395 FP: 6,878 (73%) Outbreaks (any cases)
publication NP: 2,178 (23%) and number of infections
Public: 339 (4%) per bed
Braun et al.33 Peer-reviewed October 2020 Cross-sectional Y US (unclear PE, FP, NP and public Y 11,470 FP: 7,793 (67.9%) Number of infections
publication number of states) NP: 2,523 (22.0%) and deaths per 1,000
Public: 511 (5.3%) residents, supply of PPE
PE: 543 (4.7%) and staffing shortage
Li et al.20 Peer-reviewed June 2020 Cross-sectional Y US (Connecticut) FP and NP (including Y 215 FP: 179 (83%) Number of infections and
publication public providers) NP: 36 (17%) deaths
Li et al.46 Peer-reviewed October 2020 Cross-sectional Y US (unclear FP, NP and public Y 14,062 FP: 9,787 (70%) Supply of PPE
publication number of states) Public: 903 (6.5%)
NP: 3,286 (23.5%)
Stall et al.47 Peer-reviewed August 2020 Cross-sectional Y Canada (Ontario) FP, NP and public Y 623 FP: 360 (57.7%) Outbreaks (any cases),
publication NP: 162 (26.0%) number of infections and
Public: 101 (16.2%) deaths
He et al.53 Peer-reviewed June 2020 Cross-sectional Y US (California) FP, NP and public N 1,144 FP: 956 (84%) Number of infections and
publication Public: 35 (3%) deaths
NP: 153 (13%)
Sugg et al.81 Peer-reviewed August 2020 Cross-sectional Y US (ten CMS FP, NP and public N 13,709 Unclear Number of infections
publication regions)
Dean et al.55 Peer-reviewed November Cross-sectional Y US (NY state) FP and NP Y 621 Unclear Deaths
publication 2020
Harrington et al.58 Peer-reviewed July 2020 Cross-sectional Y US (California) FP, NP (including N 1,091 FP: 920 (84%) Outbreaks (any cases)
publication public) NP and public: 171
(16%)
Unruh et al.28 Peer-reviewed June 2020 Cross-sectional Y US (Connecticut, FP and NP Y 1,162 Unclear Deaths (dichotomized as
publication New Jersey, New six or more)
York)
Bowblis and Peer-reviewed October 2020 Cross-sectional Y US (Ohio) FP, NP and public Y 942 FP: 749 (79.4%) Outbreaks and number of
Applebaum30 publication NP: 178 (19%) infections (dichotomized
Public: 15 (1.6%) as more than 20% of
residents)
Li et al.37 Peer-reviewed September Cross-sectional Y US (unclear FP, NP and public Y 12,576 FP: 8,861 (70%) Number of infections and
publication 2020 number of states) NP: 2,938 (23%) deaths
Public: 777 (7%)
Continued
Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/nataging
NaTuRE AgIngTable 1 | Study, sample and outcome characteristics (Continued)
Study Type of study Publication Research Adjusted Country Main ownership Adjusted Sample Sample size across COVID-19 outcomes
date design results categorization for CA (Y size (care ownership groups
(Y or N) or N) homes)
Fisman et al.82 Peer-reviewed July 2020 Cross-sectional N Canada (Ontario) FP, NP, municipal N 627 FP: 361 (57%) Outbreaks (any cases)
NaTuRE AgIng
publication and charitable NP: 117 (18%)
Municipal: 101
(16%)
Charitable: 57 (9%)
Xu et al.35 Peer-reviewed August 2020 Cross-sectional Y US (unclear FP, NP and public Y 11,920 FP: 8,561 (72%) Shortage of staff
publication number of states) Public: 647 (5%)
NP: 2,712 (23%)
Gorges and Peer-reviewed August 2020 Cross-sectional Y US (unclear FP, NP and public Y 13,167 FP: 9,164 (69.6%) Outbreak (any cases),
Konetzka54 publication number of states) NP: 3,265 (24.8%) number of infections
Public: 737 (5.6%) (dichotomized as >10%
confirmed cases per bed
or >20% confirmed and
suspected cases per bed
Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/nataging
or 10+ deaths) and deaths
McGarry et al.31 Peer-reviewed October 2020 Cohort Y US (unclear FP, NP and public Y 15,035 FP: 10,539 (70.1%) PPE and staff shortage
publication number of states) NP: 3,518 (23.4%)
Public: 977 (6.5%)
Gibson and Peer-reviewed October 2020 Cross-sectional Y US (unclear FP, NP and public Y 13,445 FP: 9,398 (69.9%) Supply of PPE and staff
Greene36 publication number of states) NP: 3,200 (23.8%) shortage
Public: 847 (6.3%)
Rowan et al.27 Report by September Cross-sectional Y US (Connecticut) FP and NP Y 212 FP: 176 (83%) Outbreak (any cases),
Mathematica 2020 NP: 36 (17%) number of infections and
deaths per licensed bed
Brown et al.29 Peer-reviewed November Cross-sectional Y Canada (Ontario) FP, NP and public N 618 FP: 358 (58%) Outbreaks (any cases),
publication 2020 (municipal) NP: 159 (26%) number of infections and
(initially included Public: 101 (16%) deaths per 100 residents
as preprint)
Burton et al.83 Peer-reviewed October 2020 Cross-sectional Y Scotland FP, NP and public N 189 Private: 98 (52%) Outbreaks (any cases)
publication (local authority) Public: 54 (28%)
NP: 37 (20%)
Shen43 medRxiv preprint September Cross-sectional Y US (18 states) FP, NP and public Y 6,132 FP: 4,476 (73%) Number of deaths per 100
2020 NP: 1,472 (24%) beds
Public: 184 (3%)
Chen et al.41 Peer-reviewed December Cross-sectional Y US (22 states) FP and NP N 6,337 FP: 4,689 (74%) Number of infections
publication 2020 NP: 1,648 (26%) (inverse hyperbolic sine)
(initially included
as preprint)
Continued
951
Analysis952
Table 1 | Study, sample and outcome characteristics (continued)
Study Type of study Publication Research Adjusted Country Main ownership Adjusted Sample Sample size across COVID-19 outcomes
Analysis
date design results categorization for CA (Y size (care ownership groups
(Y or N) or N) homes)
Gandhi et al.34 Preprint October 2020 Cross-sectional Y US (49 states) PE, prior PE and FP Y 13,398 Non-PE: 11,788 Outbreaks (any cases),
(88%) number of confirmed and
Prior PE: 1,219 (9%) suspected infections,
PE: 391 (3%) deaths and PPE shortage
No information
on FP
Shallcross et al.39 Peer-reviewed February 2021 Cross-sectional Y England FP and NP Y 5,126 Profit: 4,289 Outbreaks (any cases)
publication (83.7%) and number of infections
(initially included NP: 837 (16.3%) (dichotomized as more
as preprint) than one-third of staff or
residents)
Rolland et al.21 Peer-reviewed July 2020 Cross-sectional Y France FP, NP and public N 124 FP: 54 (44%) Outbreaks (any cases)
publication NP: 35 (28%)
Public: 35 (28%)
Morciano et al.32 Peer-reviewed November Cohort Y England FP and NP Y 15,524 FP: 13,397 (86.3%) Deaths (defined as at
publication 2020 NP: 2,127 (14.7%) least one suspected or
(initially included confirmed COVID-19
as preprint) death)
Gopal et al.38 Peer-reviewed January 2021 Cross-sectional Y US (California) FP and NP N 713 FP: 613 (86%) Outbreaks (any cases)
publication NP: 100 (14%) and number of infections
among residents and staff
Ryskina et al.40 Peer-reviewed May 2021 Cross-sectional Y US (unclear FP and NP Y 11,585 FP: 8,446 (72.9%) Number of COVID-19
publication number of states) NP: 3,139 (27.1%) cases among staff per 100
care home beds
Gorges and Peer-reviewed February 2021 Cross-sectional Y US (unclear FP, NP and public Y 13,312 FP: 9,475 (71%) Number of COVID-19
Konetzka62 publication number of states) NP: 3,037 (22.8%) deaths
Public: 800 (6.2%)
Weech- Peer-reviewed March 2021 Cross-sectional Y US (unclear number FP and NP Y 11,178 Unclear Number of COVID-19
Maldonado et al.44 publication of states) deaths
Note that outcomes refer to care home residents unless otherwise specified. Outbreaks usually refer to the presence of at least one confirmed or suspected COVID-19 infection. Number of infections refer to the cumulative or relative number of confirmed or suspected COVID-19
infections. COVID-19 deaths refer to the cumulative or relative mortality number unless otherwise specified. Only outcomes investigated in relation to ownership are included in this table. Y, yes; N, no.
Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/nataging
NaTuRE AgIngNaTuRE AgIng Analysis
Supplementary Table 3 provides an overview of the temporal of effect was consistent across multiple research contexts, including
overlap of included studies across all outcomes. Although several the US, England and Canada, and the certainty of this evidence was
studies relied on similar data sources, there was relatively little tem- rated as moderate. No studies found FP ownership to be associated
poral overlap across studies using similar sources. The most obvious with fewer COVID-19 infections.
case of data overlap was in two studies that assessed similar out- Seven studies found higher rates of COVID-19-related deaths
comes using the same sample and time period but, notably, came to in FP care homes in Canada (Ontario29), California53 and across
different conclusions29,47. This is discussed further below. aggregated samples of US states28,34,43,44,54, whereas seven studies ana-
lyzing data from Canada (Ontario47), England32, Connecticut20,27,
Risk-of-bias assessments. Our risk-of-bias (RoB) assessments New York state55 and two studies using aggregate data from mul-
(based on the conducting systematic reviews and meta-analyses tiple states37,56 did not find a statistically significant association.
of observational studies of etiology (COSMOS-E) guidance) are However, the English study only investigated variation in the
detailed in Supplementary Table 4. The main concerns related to probability of having at least one COVID-19-related death and did
systematically missing data and selection bias in the included stud- not analyze variation in the cumulative numbers of deaths32. More
ies. For example, studies that investigated characteristics of excluded importantly, most US studies (five of seven) that analyzed cumu-
observations from the CMS dataset (due to missing or incomplete lative state data (as opposed to data from single states) reported
data) found that excluded care homes were more likely to be FP a statistically significant relationship between FP ownership and
and were also associated with many risk factors, such as the ethnic- mortality28,34,43,54. Moreover, one of two studies using cumulative
ity and socio-economic status of care home residents (discussed in state data that did not identify statistically significant ownership
detail below)31,35–37. This is a potentially serious limitation of studies variation analyzed COVID-19 deaths for only 1 week (25 May
using this data source (for the purpose of this review), as it suggests 2020–31 May 2020)37. The certainty of evidence showing a posi-
that poorly performing FPs may be systematically under-repre- tive association between COVID-19 deaths and FP ownership was
sented in the sample, which may underestimate the observed effect rated as moderate. No studies found FP ownership to be associated
of FP ownership on COVID-19 outcomes. Because of this limita- with fewer COVID-19 deaths.
tion, all studies using this dataset were downgraded to (at least) All studies that investigated PPE outcomes found FP ownership
moderate risk. For studies using public and government data, we to be positively associated with insufficient access to or shortage of
assumed that the risk of information bias was low, unless given a PPE31,34,36,46, and the certainty of evidence underlying this associa-
reason to downgrade. tion was rated as moderate. FP ownership was not consistently asso-
All assessments of confounding bias performed as part of the ciated with staffing shortages, and the certainty of this evidence was
RoB were based on consideration of factors known either to exac- rated as low.
erbate the effect of COVID-19 (refs. 48–51) or to affect the perfor- Chain status was generally associated with a higher likelihood of
mance of care homes for older people7,8. Almost all studies adjusted COVID-19 outbreaks (moderate certainty of evidence) but not with
for care home size (27 of 32), and characteristics of quality and a higher incidence of infections (low certainty of evidence). Five
staffing were also commonly included. Only five studies reported studies from Canada, England and the US found CA ownership to
their outcome(s) as proportions of the number of beds or resi- be associated with a higher incidence of COVID-19 deaths, whereas
dents27,29,33,41,43. Twenty-one studies adjusted for ethnic composition, eight studies using both single and cumulative US state data did
and 17 studies included information about the socio-economic sta- not identify any statistically significant variation, and the certainty
tus of residents. Rurality and/or population density was included in of this body of evidence was considered low. The one Canadian
12 of the studies, and local or community incidence of COVID-19 study that investigated this ownership category found CA to be
was controlled for in 19 of the studies. See Supplementary Table 5 associated with more COVID-19 infections and deaths47. The two
for details on the direction of effect and model adjustments in all English studies investigating this group did not identify any varia-
included studies. tion in COVID-19 outbreaks and incidence across CA ownership39,
although one found CA to be associated with higher risk of at least
Direction of effects. Most included studies were conducted in the one COVID-19 death among a care home’s residents32.
US, Canada or the UK, which all have substantial FP care home PE ownership of care homes was not found to be consistently
provision. Although these countries differ with respect to commis- associated with worse outcomes compared to other ownership cat-
sioning systems in place, past research indicates important simi- egories, and one study even found PE providers to be less likely
larities in the behavior of FP care homes across these countries52. to report PPE shortages and confirmed COVID-19 outbreaks34.
However, to ensure that our results are sensitive to study context, we The certainty of evidence across all PE outcomes was considered
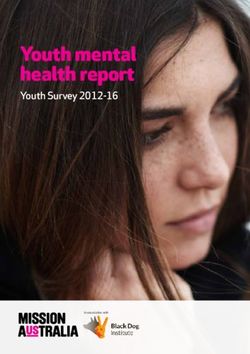
present all findings according to the country of origin. The harvest very low.
plot in Fig. 2 displays the direction of effect for all included stud-
ies across different ownership categories and COVID-19 outcomes. Staff outcomes. Evidence on the relationship between ownership
Bar height indicates sample size, and color denotes country context. variation and risk of infection among staff was scarce, with only
See Extended Data Fig. 1 for a harvest plot of the direction of effect five studies investigating variation in this population. In England,
across different data sources and RoB levels and Table 2 for details FP ownership was associated with a higher incidence of infection
on our Grading of Recommendations Assessment, Development among staff39, but no association was identified among CA care
and Evaluation (GRADE) assessments of the certainty of evidence homes. The three studies conducted in the US did not identify any
for each finding. statistically significant variation related to FP ownership, but one
study found CA to be correlated with a higher incidence of infec-
Resident outcomes. In most studies investigating COVID-19 out- tions and deaths among staff34. The certainty of evidence was rated
breaks among residents (12 of 15), FP ownership was not found to as low or very low across all investigated staffing outcomes.
be a statistically significant risk factor, suggesting that FP care homes
were neither more nor less likely to have at least one infected resi- Indirect ownership effects. The raw unadjusted incidences of
dent. The certainty of evidence for a higher incidence of COVID-19 deaths and infections were higher in FP care homes in all included
outbreaks among FP care homes was thus considered low. studies, but this association was not always statistically significant
FP care homes were found to be associated with a higher num- in adjusted models. This suggests that there are important medi-
ber of cumulative COVID-19 infections (nine of 14). This direction ating factors that influence the effect of ownership on COVID-19
Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/nataging 953Analysis NaTuRE AgIng
COVID-19 outbreak COVID-19 incidence COVID-19 mortality
Negative effect Null effect Positive effect
Negative effect Null effect Positive effect
Negative effect Null effect Positive effect
FP FP
FP
CA CA CA
PE PE
PE
PPE Staffing shortage
Negative effect Null effect Positive effect Negative effect Null effect Positive effect
FP FP
Sample sizeTable 2 | Overview of investigated outcomes and GRADE assessments
Comparison Number of Direction of effect and data Temporal RoB Indirectness Inconsistency Imprecision Publication bias Certainty of
studies coverage overlapa evidence
Higher incidence of COVID-19 outbreaks among residents
FP versus NP or 15 studies 3 studies: positive association 4 studies were No serious No serious Very serious concerns No serious No serious ⊗⊗◯◯
NaTuRE AgIng
NP and public (CMS data and France) considered to be concerns concerns due to most studies concerns concerns Low
11 studies: no association (US at some risk of finding no statistically
state and CMS data, Canada and temporal overlap significant association
the UK)
1 study: negative association
(CMS data)
CA versus no CA 7 studies 4 studies: positive association (US No serious No serious No serious Serious concerns due No serious No serious ⊗⊗⊗◯
state and CMS data) concerns concerns concerns to mixed direction of concerns concerns Moderate
2 studies: no association (Canada results
and the UK)
1 study: negative association (US
state data)
PE versus non-PE 1 study 1 study: negative association No serious Serious No serious No serious concerns Very serious No serious ⊗◯◯◯
Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/nataging
owned (CMS data) concerns concerns due concerns concerns due to concerns Very low
to moderate limited evidence
risk of selection
bias
Higher incidence of COVID-19 infections among residents
FP versus NP or 14 studies 9 studies: positive association (US 4 studies were No serious No serious Serious concerns due No serious No serious ⊗⊗⊗◯
NP and public state and CMS data, Canada and considered to be concerns concerns to mixed direction of concerns concerns Moderate
the UK) at some risk of results
5 studies: no association (US state temporal overlap
and CMS data and Canada)
CA versus no CA 10 studies 2 studies: positive association No serious No serious Serious Very serious concerns No serious No serious ⊗⊗◯◯
(CMS data and Canada) concerns concerns concerns due to most studies concerns concerns Low
8 studies: no association (US state finding no statistically
and CMS data and the UK) significant association
PE versus non-PE 2 studies 1 study: no association (CMS No serious Serious No serious Serious concerns due Serious concerns No serious ⊗◯◯◯
owned data) concerns concerns due concerns to mixed direction of due to limited concerns Very low
1 study: negative association to moderate results evidence
(CMS data) risk of selection
bias
Higher incidence of COVID-19 deaths among residents
FP versus NP or 14 studies 7 studies: positive association (US 2 studies were No serious No serious Serious concerns due No serious No serious ⊗⊗⊗◯
NP and public state and CMS data and Canada) considered to be concerns concerns to mixed direction of concerns concerns Moderate
7 studies: no association (US at some risk of results
state and CMS data, Canada and temporal overlap
the UK)
Continued
955
Analysis956
Table 2 | Overview of investigated outcomes and GRADE assessments (Continued)
Comparison Number of Direction of effect and data Temporal RoB Indirectness Inconsistency Imprecision Publication bias Certainty of
studies coverage overlapa evidence
CA versus no CA 13 studies 5 studies: positive association (US No serious No serious No serious Very serious concerns No serious No serious ⊗⊗◯◯
state and CMS data, Canada and concerns concerns concerns due to most studies concerns concerns Low
the UK) finding no statistically
Analysis
8 studies: no association (US state significant association
and CMS data)
PE versus non-PE 2 studies 2 studies: no association (CMS No serious Serious No serious Serious concerns due Serious concerns No serious ⊗◯◯◯
owned data) concerns concerns due concerns to mixed direction of due to limited concerns Very low
to moderate results evidence
risk of selection
bias
Higher incidence of PPE shortage
FP versus NP or 4 studies 4 studies: positive association No serious Serious No serious No serious concerns No serious No serious ⊗⊗⊗◯
NP and public (CMS data) concerns concerns due concerns concerns concerns Moderate
to moderate
risk of selection
bias
CA versus no CA 5 studies 2 studies: positive association No serious Serious No serious Serious concerns due No serious No serious ⊗⊗◯◯
(CMS data) concerns concerns due concerns to mixed direction of concerns concerns Low
3 studies: no association (CMS to moderate results
data) risk of selection
bias.
PE versus non-PE 2 studies 1 study: positive association (CMS No serious Serious No serious Serious concerns due Serious concerns No serious ⊗◯◯◯
owned data) concerns concerns due concerns to mixed direction of due to limited concerns Very low
1 study: negative association to moderate results evidence
(CMS data) risk of selection
bias
Higher incidence of staffing shortage
FP versus NP or 3 studies 1 study: positive association (CMS No serious Serious No serious Serious concerns due No serious No serious ⊗⊗◯◯
NP and public data) concerns concerns due concerns to mixed direction of concerns concerns Low
2 studies: no association (CMS to moderate results
data) risk of selection
bias
CA versus no CA 3 studies 1 study: negative association No serious Serious No serious Serious concerns due No serious No serious ⊗⊗◯◯
(CMS data) concerns concerns due concerns to mixed direction of concerns concerns Low
2 studies: no association (CMS to moderate results
data) risk of selection
bias
PE versus non-PE 1 study 1 study: no association (CMS No serious Serious No serious Serious concerns due Serious concerns No serious ⊗◯◯◯
owned data) concerns concerns due concerns to limited evidence due to limited concerns Very low
to moderate evidence
risk of selection
bias
Continued
Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/nataging
NaTuRE AgIngTable 2 | Overview of investigated outcomes and GRADE assessments (Continued)
Comparison Number of Direction of effect and data Temporal RoB Indirectness Inconsistency Imprecision Publication bias Certainty of
studies coverage overlapa evidence
Higher incidence of COVID-19 outbreaks among staff
FP versus NP or 2 studies 1 study: positive association (UK) No serious Serious No serious Serious concerns due Serious concerns No serious ⊗◯◯◯
NP and public 1 study: no association (CMS concerns concerns due concerns to limited evidence due to limited concerns Very low
NaTuRE AgIng
data) to moderate evidence
risk of selection
bias
CA versus no CA 1 study 1 study: no association (UK) No serious Serious No serious Serious concerns due Serious concerns No serious ⊗◯◯◯
concerns concerns due concerns to limited evidence due to limited concerns Very low
to moderate evidence
risk of selection
bias
Higher incidence of COVID-19 infections among staff
FP versus NP or 4 studies 1 study: positive association (UK) No serious Serious No serious Serious concerns due No serious No serious ⊗⊗◯◯
NP and public 3 studies: no association (state concerns concerns due concerns to mixed direction of concerns concerns Low
and CMS data) to moderate results
risk of selection
bias
Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/nataging
CA versus no CA 3 studies 1 study: positive association (CMS No serious Serious No serious Serious concerns due Serious concerns No serious ⊗◯◯◯
data) concerns concerns due concerns to limited evidence due to limited concerns Very low
2 studies: no association (CMS to moderate evidence
data and UK) risk of selection
bias
PE versus non-PE 1 study 1 study: negative association No serious Serious No serious Serious concerns due Serious concerns No serious ⊗◯◯◯
owned (CMS data) concerns concerns due concerns to limited evidence due to limited concerns Very low
to moderate evidence
risk of selection
bias
Higher incidence of COVID-19 mortality among staff
FP versus NP or 1 study 1 study: no association (CMS No serious Serious No serious Serious concerns due Serious concerns No serious ⊗◯◯◯
NP and public data) concerns concerns due concerns to limited evidence due to limited concerns Very low
to moderate evidence
risk of selection
bias
CA versus no CA 1 study 1 study: positive association (CMS No serious Serious No serious Serious concerns due Serious concerns No serious ⊗◯◯◯
data) concerns concerns due concerns to limited evidence due to limited concerns Very low
to moderate evidence
risk of selection
bias
PE versus non-PE 1 study 1 study: no association (CMS data) No serious Serious No serious Serious concerns due Serious concerns No serious ⊗◯◯◯
owned concerns concerns due to concerns to limited evidence due to limited concerns Very low
moderate risk of evidence
selection bias
Note that, if available, we evaluated adjusted results. Positive and negative associations are understood as associations in either direction that are statistically significant (P < 0.05). ‘No association’ is understood as differences that are not statistically significant. Outbreaks
usually refer to the presence of any COVID-19 infections, except for one study that defined outbreaks as at least two cases26. COVID-19 incidence usually refers to the cumulative number of COVID-19 infections but also includes binary outcomes on large outbreaks (for example,
refs. 39,54). COVID-19 mortality usually refers to cumulative cases, except for a study that used a binary indicator of at least six deaths28 and another that analyzed a dichotomized outcome of any number of deaths versus no deaths32. aFor more details on temporal overlap, see
Supplementary Table 3.
957
AnalysisAnalysis NaTuRE AgIng
Table 3 | Overview of risk factors associated with both FP ownership and COVID-19 outcomes
COVID-19 risk factors correlated Evidence supporting correlation between risk factor and FP Importance of risk factor
with FP ownership ownership
CA Research conducted in Connecticut20, Canada (Ontario)47 Of the 20 studies adjusting for chain ownership,
and England32 32 found FP care homes more likely to be 12 found FP ownership to exacerbate one or more
affiliated with a chain. COVID-19 outcomes.
Resident ethnicity One study using cumulative US state data found that FP Of the 19 studies that adjusted for ethnicity, 13 found
care homes serve a higher proportion of ethnic minority FP ownership to exacerbate one or more COVID-19
residents37. outcomes.
Older design standards One study conducted in Canada (Ontario) found that The one study adjusting for outdated design
outdated design standards were more prevalent in FP care standards did not find FP ownership to be associated
homes47. with inferior COVID-19 outcomes.
Crowding One study conducted in Canada (Ontario)29 found that FP The one study adjusting for crowding found that
care homes were more crowded in terms of the number both crowding and FP ownership were statistically
residents per bathroom and bedroom. significant risk factors of COVID-19 deaths and
infections.
Staffing One study conducted in California58 found FP ownership to Of the 20 studies adjusting for staffing conditions,
be associated with inferior staffing conditions. two found FP ownership to exacerbate one or more
COVID-19 outcomes.
Quality Research conducted in West Virginia26 and California58 Of the 19 studies adjusting for quality, ten found FP
found FP ownership to be correlated with poor quality ownership to exacerbate one or more COVID-19
ratings. outcomes.
Union membership One study conducted in New York state found that FP care The one study adjusting for union membership did not
home staff were more likely to be part of a union55. find FP ownership to be associated with one or more
inferior COVID-19 outcomes.
Care home size Research conducted in Scotland83 and Connecticut20 reported Of the 26 studies adjusting for care home size, 15
FP ownership to be correlated with care home size. found FP ownership to exacerbate one or more COVID-
19 outcomes.
Note that this table only reports risk factors that were found to be associated with FP ownership. Most studies that included the above-mentioned risk factors as covariates did not report their correlation
with FP ownership. See Supplementary Table 5 for details on model adjustment and direction of effect.
care homes will prioritize financial gains over client concerns to the aggregate, have important consequences for the quality of care ser-
extent that regulation allows15,59. vices for the aging population. Whether or not future regulation
However, there are many factors that should be considered when should focus on the legal ownership status or individual underlying
evaluating the performance of care homes, as there is plenty of characteristics remains unclear. Yet, in our synthesis of the cumula-
variation among these organizations independent of ownership. For tive body of evidence, we identified a systematic pattern of exacer-
example, both NP and FP care homes are commonly affiliated with bated COVID-19 outcomes among FP care homes, which was only
multifacility chains and vary widely in size and client groups served. partly explained by an array of possible mediating factors. This sug-
Further, care homes of all ownership types receive poor quality gests that regulations targeting single risk factors, rather than the
ratings7,8. Thus, the purpose of analyzing variation across owner- market structure responsible for the outsourcing and privatization
ship is not that it is a guaranteed marker of quality, deficiency or of social care, may not suffice.
irresponsible management; rather, it constitutes a proxy for certain The findings of this review highlight the importance of own-
characteristics and behaviors that may (or may not) be associated ership in accounting for poor COVID-19 outcomes across care
with relevant outcomes. For example, FP care homes are com- homes. The adult social care sector found itself exceedingly exposed
monly associated with inferior staffing conditions58, which previous at the beginning of the pandemic63, in large part due to delayed gov-
research has found to be an important driver of lower performance ernment support and intervention, but also as a result of many years
and service quality14–16. Moreover, multiple recent studies found that of political and financial neglect17. With this review, we do not sug-
minority and Medicaid residents are housed at higher rates in FP gest that challenges faced by care homes during the pandemic can
care homes, which may also help to explain poor COVID-19 out- (or should) be understood through the lens of ownership alone. It
comes60–62. In other words, if FP care homes are consistently and is clear that care homes have faced severe challenges that cannot
systematically correlated, on average, with risk factors, such as out- be reduced to ownership. However, outsourcing to FP providers
dated design standards, inferior staffing conditions, crowding, cli- has become the status quo in many care markets, often based on
ent vulnerably, etc., this should be considered part of the (average) the rationale that open-market competition will optimize the func-
underlying effect of this ownership category. tioning of care homes. This claim has been subjected to extensive
Throughout the synthesis, we incorporated these nuances by scrutiny and is not well supported by empirical evidence7–10,64. This
critically analyzing our results according to different model speci- review adds to this evidence base by systematically appraising and
fications and by considering other ownership types, such as multi- synthesizing the available research on how consequences of the
CA and PE-owned care homes. Understanding and analyzing COVID-19 pandemic in care homes varied by ownership type dur-
systematic variation across ownership groups is of immense policy ing the first wave of the pandemic. Although our results represent
relevance, given that the majority of care homes in many devel- multiple national settings, most of the included research was con-
oped countries are controlled by the FP sector. If social care mar- ducted in the US, likely owing in part to the public availability of the
kets facilitate the entry of providers that, on average, are associated national CMS dataset. Efforts are currently being made in the UK
with undesirable or risk-associated characteristics, this can, in the to create a similar type of systematic, live and linked dataset on care
958 Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/natagingNaTuRE AgIng Analysis
homes65, which is an important endeavor if the consequences of this Inclusion criteria. We assessed study eligibility based on four criteria. First,
pandemic are to be understood and addressed going forward. studies had to investigate variation in COVID-19 outbreaks, infection rates and/
or excess or COVID-19-related mortalities among residents or outcomes related to
Our findings should be interpreted in light of some caveats, PPE use and availability, staff shortages, preparedness and infection and mortality
most of which relate to characteristics of the included studies. First, among staff and visitors. We did not exclude studies based on how COVID-19
most studies were conducted in the US and Canada, and the results outcomes were operationalized (for example, if the infections were confirmed by
thus primarily relate to North America. Second, the majority of PCR test or by self-report and whether analyzed outcomes were dichotomized
or continuous), although these aspects were considered in our RoB assessments.
US studies relied on CMS data, whereas all the Canadian studies
Second, studies had to investigate variation in any of the above outcomes across
were conducted in Ontario using the same sample of long-term care ownership categories, which are conventionally operationalized as FP (that is,
facilities, which means that there is overlap in analyzed data across private care homes run for profit), NP (that is, registered not-FP care homes or
certain studies. Second, the body of included research was too het- charities) and ‘public’ (that is, municipal or local authority care homes). However,
erogeneous to be meaningfully meta-analyzed, and this review thus ‘ownership’ is not consistently operationalized and defined in the literature,
and terms such as FP, NP, ‘private’, CA and ‘public’ are rarely clearly defined. As
represents a critical appraisal and narrative synthesis conducted in the objective of this review is to appraise and synthesize research on ownership
line with synthesis without meta-analysis (SWiM) and COSMOS-E variation, we considered any definition or classification of ownership. The nuances
guidance66,67. Third, throughout our RoB assessments, we assumed of and potential for overlap between definitions are outlined in Supplementary
that the reporting of COVID-19 outcomes was not systematically Table 1. Third, studies had to employ an observational research design, including,
related to ownership. However, there is some suggestive evidence but not limited to, cross-sectional and cohort designs and secondary analyses of
registry data. Both published articles and unpublished manuscripts (for example,
of a longer turnaround period for resident test results among FP preprints and reports) were eligible for inclusion. Fourth, studies had to investigate
providers68, which, if generally true, may bias the effect of FP own- residential care homes for older people, including, but not limited to, long-term
ership toward the null due to under-reporting. Lastly, it is known care facilities, nursing homes and retirement homes.
that COVID-19 research is rapidly published69, which may expose
our results to publication bias in favor of articles that have been fast Data extraction. Descriptive information on citation details (author, title, journal)
tracked for reporting timely and significant outcomes. However, by and study characteristics (research design, analysis, sample details) were extracted
from all included articles. We also extracted detailed descriptive data (for example,
not restricting our studies to peer-reviewed research, we were able country, source and period of data coverage) and outcome and exposure variables
to also consider evidence presented in preprints and government (for example, definition, operationalization and cutoffs). All results relating to
reports in our synthesis. ownership variation across COVID-19-related outcomes and accompanying
This review presents a critical appraisal and synthesis of avail- interpretations were extracted for all studies. Results were extracted by A.M.B.-M.
and independently validated by at least one other reviewer per study.
able evidence on ownership variation across COVID-19 outcomes
during the first wave of the pandemic. It reports evidence of mod- Risk-of-bias assessment. RoB was assessed using COSMOS-E guidance66. We
erate certainty that FP ownership was a risk factor for elevated employed this guidance rather than, for example, ROBINS-I for non-randomized
cumulative COVID-19 infections and deaths among care home intervention studies, as it is specifically designed for systematically reviewing
residents. Ownership and characteristics associated with FP care observational and correlational research. Specifically, we evaluated the following
home providers may thus present key regulatable factors that can bias domains: confounding, selection bias and information bias. In line with the
consistent recommendation to avoid quantitative scoring of risk domains66,74,
be addressed to improve health outcomes in vulnerable populations all RoB assessments were based on the qualitative subjective assessment of the
and reduce health disparities. reviewers. RoB assessments were conducted in blind duplicate by two reviewers,
and the final rating was decided through discussion and in consensus. All
Methods assessments were conducted with the focus of our review (variation in COVID-19
COVID-19-related research is published at a high frequency, and the time between outcomes across ownership) in mind, and assessments may thus not represent
submission and publication is substantially shorter than is typical for research more the RoB across other investigated associations and outcomes. The overall RoB
generally69, which makes it particularly important that this rapidly growing body of assessment for each study was based on the lowest assessment in any bias domain.
evidence is critically appraised and systematically synthesized regularly. To ensure We did not exclude studies based on RoB assessments.
that this review represents a recent and relevant synthesis of the available evidence
on the topic, it is being conducted as a living systematic review, ‘a systematic review Certainty of evidence. To assess the certainty of the evidence underlying each
that is continually updated, incorporating relevant new evidence as it becomes finding, we employed the GRADE approach, specifically recently published
available’ (refs. 70,71). Specifically, we plan to update our results every 6 months for guidance on the use of GRADE when assessing evidence on prognostic factors75,76.
2 years after initial publication. An update will entail (1) running the full search For this, a body of observational evidence starts with high certainty, and five
string for the updated time period and (2) forward and backward citation tracking domains are used to downgrade certainty: RoB (using COSMOS-E), imprecision,
of all included studies72. If inclusion of new evidence results in important changes inconsistency, indirectness and publication bias, as well as domains for upgrading
to the findings and conclusions, the publication may be updated to reflect these evidence. As the included body of evidence could not be meaningfully meta-
changes. If updated results do not change the main conclusions, we will instead analyzed (described in detail below), we did not conduct a statistical assessment
write a short report detailing the number of studies and characteristics of the of publication bias, such as testing asymmetry of funnel plots or the trim-and-fill
updated evidence. Updates will be published on the Open Science Framework25. method, as these tests would then only be conducted on a subset of included
This review is conducted and reported in accordance with PRISMA guidelines73 studies. To date, there are no guidelines on how to assess publication bias in
(see Supplementary Data 1 for a PRISMA checklist). systematic reviews without meta-analysis. Also, for observational studies, the
accuracy of such tests is unclear27. However, as this is the first iteration of a
Search strategy. Before developing our search strategy, we performed scoping review on a topic with rapidly emerging evidence, it may be prone to ‘lag bias’
searches using Google Scholar and preprint repositories to identify relevant (early publication of positive results)29, which will be explored in later updates
articles and performed citation searches on all identified articles. This preliminary of this review. In assessing publication bias in this iteration, we evaluated (1)
sample of includable studies was used to design our search strategy and to test whether there were serious concerns in the reporting of results and (2) whether
its specificity. The search strategy was piloted and adjusted until it retrieved all the direction of results consistently varied across peer-reviewed publications and
pre-identified studies. The full search strategy can be found in the Supplementary preprints or government reports across all outcomes.
Data 2. Our search string was implemented in the following databases: ABI/
INFORM Global, the Coronavirus Research Database, the Criminology Collection Data synthesis. Due to a high degree of heterogeneity among included studies
International (Criminal Justice Database and NCJRS Abstracts Database), the in terms of model specifications, operationalization of outcomes, inconsistent
International Bibliography of the Social Sciences, the Politics Collection (PAIS ownership categorization of the reference group and overlapping data, we did not
Index, Policy File Index, Political Science Database and Worldwide Political perform a statistical meta-analysis of included results. This decision was made
Science Abstracts), the Social Science Database, the Sociology Collection (Applied with attention to the pitfalls of employing statistical methods and assumptions
Social Science Index and Abstracts, Sociological Abstracts and Sociology Database) designed for the analysis of highly homogeneous data or randomized controlled
via ProQuest. We searched Embase, Global Health, Medline and PsycINFO via trials of interventions to observational and correlational research77. Our synthesis
Ovid. We also searched Web of Science and CINAHL. We implemented our search and reporting of findings was guided by SWiM guidelines67 and can be described
strategy on 3 November 2020 and on 6 May 2021 (see Supplementary Data 2 for as follows.
details). All search results were double screened by A.M.B.-M. and M.D.E. for the First, we narratively summarized key characteristics of included studies, such
first search iteration and A.M.B.-M. and B.V. for the second search iteration. as publication type, sample details, ownership categorization and data sources.
Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/nataging 959Analysis NaTuRE AgIng
Second, we assessed the RoB across all included studies. Third, using GRADE, 21. Rolland, Y. et al. Guidance for the prevention of the COVID-19 epidemic in
we assessed the certainty of evidence for each outcome across the full body of long-term care facilities: a short-term prospective study. J. Nutr. Health Aging
contributing studies. Fourth, we constructed harvest plots to graphically illustrate 24, 812–816 (2020).
the direction of effects across different outcomes and ownership categories with 22. Glasby, J., Zhang, Y., Bennett, M. R. & Hall, P. A lost decade? A renewed case
attention to model specifications, sample size and the RoB of contributing studies78. for adult social care reform in England. J. Soc. Policy 50, 406–437 (2020).
Harvest plots serve as a way to synthesize and describe heterogeneous bodies of 23. Bach-Mortensen, A. M. & Barlow, J. Outsourced austerity or improved
evidence that cannot be meaningfully synthesized meta-analytically. Lastly, we services? A systematic review and thematic synthesis of the experiences of
analyzed and examined the role or mediating factors associated with both FP social care providers and commissioners in quasi-markets. Soc. Sci. Med. 276,
ownership and COVID-19 outcomes79. 113844 (2021).
24. Oliver, D. David Oliver: let’s not forget care homes when COVID-19 is over.
Reporting Summary. Further information on research design is available in the BMJ 369, m1629 (2020).
Nature Research Reporting Summary linked to this article. 25. Bach-Mortensen, A., Verboom, B., Degli Esposti, M. Ownership and
COVID-19 in Care Homes for Older People: A Living Systematic Review of
Data availability Outbreaks, Infections, and Mortalities (OSF Home, 2021); https://osf.io/c8dq9/
As this is a systematic review, all data are already available in published articles and 26. Bui, D. P. et al. Association between CMS quality ratings and COVID-19
unpublished manuscripts. All data analyzed for this review are summarized in the outbreaks in nursing homes—West Virginia, March 17–June 11, 2020.
text or in the Supplementary Information. Morbidity and Mortality Weekly Report https://www.cdc.gov/mmwr/
volumes/69/wr/mm6937a5.htm (2020).
27. Rowan, P. et al. A Study of the COVID-19 Outbreak and Response in
Code availability Connecticut Long-Term Care Facilities (Mathematica, 2020); https://portal.ct.
Code used to create harvest plots is available upon reasonable request. gov/-/media/Coronavirus/20201001-Mathematica-final-report.pdf
28. Unruh, M. A., Yun, H., Zhang, Y., Braun, R. T. & Jung, H. Y. Nursing home
Received: 26 February 2021; Accepted: 2 August 2021; characteristics associated with COVID-19 deaths in Connecticut, New Jersey,
Published online: 7 October 2021 and New York. J. Am. Med. Dir. Assoc. 21, 1001–1003 (2020).
29. Brown, K. et al. Association between nursing home crowding and COVID-19
infection and mortality in Ontario, Canada. JAMA Intern. Med. 181,
References 229–236 (2020).
1. Oliver, D. David Oliver: let’s be open and honest about COVID-19 deaths in
30. Bowblis, J. & Applebaum, R. Prevalence of COVID-19 in Ohio nursing
care homes. BMJ 369, m2334 (2020).
homes: what’s quality got to do with it? J. Aging Soc. Policy https://doi.org/10.
2. Burki, T. England and Wales see 20 000 excess deaths in care homes. Lancet
1080/08959420.2020.1824542 (2020).
395, 1602 (2020).
31. McGarry, B. E., Grabowski, D. C. & Barnett, M. L. Severe staffing and
3. Comas-Herrera, A. et al. Mortality associated with COVID-19 in care homes:
personal protective equipment shortages faced by nursing homes during the
international evidence. LTCcovid.org, International Long-Term Care Policy
COVID-19 pandemic. Health Aff. 39, 1812–1821 (2020).
Network, CPEC-LSE (1 February 2021).
32. Morciano, M., Stokes, J., Kontopantelis, E., Hall, I. & Turner, A. J. Excess
4. Iacobucci, G. COVID-19: lack of PPE in care homes is risking spread of
mortality for care home residents during the first 23 weeks of the COVID-19
virus, leaders warn. BMJ 368, m1280 (2020).
5. Schuss, D. G. COVID-19’s deadly lesson: time to revamp long-term care. pandemic in England: a national cohort study. BMC Med. 19, 71 (2021).
Health Affairs (17 November 2020). 33. Braun, R. T. et al. Comparative performance of private equity-owned US
6. Le Grand, J. Quasi-markets and social policy. Econ. J. 101, nursing homes during the COVID-19 pandemic. JAMA Netw. Open 3,
1256–1267 (1991). e2026702 (2020).
7. Barron, D. N. & West, E. The quasi-market for adult residential care in the 34. Gandhi, A., Song, Y. & Upadrashta, P. Have private equity owned nursing
UK: do for-profit, not-for-profit or public sector residential care and nursing homes fared worse under COVID-19? Preprint at SSRN https://doi.
homes provide better quality care? Soc. Sci. Med. 179, 137–146 (2017). org/10.2139/ssrn.3682892 (2020).
8. Bach-Mortensen, A. M. & Montgomery, P. Does sector matter for the quality 35. Xu, H., Intrator, O. & Bowblis, J. R. Shortages of staff in nursing homes
of care services? A secondary analysis of social care services regulated by the during the COVID-19 pandemic: what are the driving factors? J. Am. Med.
Care Inspectorate in Scotland. BMJ Open 9, e022975 (2019). Dir. Assoc. 21, 1371–1377 (2020).
9. Ronald, L. A., McGregor, M. J., Harrington, C., Pollock, A. & Lexchin, J. 36. Gibson, D. M. & Greene, J. State actions and shortages of personal
Observational evidence of for-profit delivery and inferior nursing home protective equipment and staff in U.S. nursing homes. J. Am. Geriatr. Soc. 68,
care: when is there enough evidence for policy change? PLoS Med. 13, 2721–2726 (2020).
e1001995 (2016). 37. Li, Y., Cen, X., Cai, X. & Temkin-Greener, H. Racial and ethnic disparities in
10. Comondore, V. R. et al. Quality of care in for-profit and not-for- COVID-19 infections and deaths across U.S. nursing homes. J. Am. Geriatr.
profit nursing homes: systematic review and meta-analysis. BMJ 339, Soc. 68, 2454–2461 (2020).
381–384 (2009). 38. Gopal, R., Han, X. & Yaraghi, N. Compress the curve: a cross-sectional study
11. Hillmer, M. P., Wodchis, W. P., Gill, S. S., Anderson, G. M. & Rochon, P. A. of variations in COVID-19 infections across California nursing homes. BMJ
Nursing home profit status and quality of care: is there any evidence of an Open 11, e042804 (2021).
association? Med. Care Res. Rev. 62, 139–166 (2005). 39. Shallcross, L. et al. Risk factors associated with SARS-CoV-2 infection and
12. Stolt, R., Blomqvist, P. & Winblad, U. Privatization of social services: quality outbreaks in long term care facilities in England: a national survey. Lancet
differences in Swedish elderly care. Soc. Sci. Med. 72, 560–567 (2011). Healthy Longev. 2, e129–e142 (2021).
13. Harrington, C., Olney, B., Carrillo, H. & Kang, T. Nurse staffing and 40. Ryskina, K. L., Yun, H., Wang, H., Chen, A. T. & Jung, H. Y. Characteristics
deficiencies in the largest for-profit nursing home chains and chains owned of nursing homes by COVID-19 cases among staff: March to August 2020. J.
by private equity companies. Health Serv. Res. 47, 106–128 (2012). Am. Med. Dir. Assoc. 22, 960–965 (2021).
14. Grabowski, D. C., Feng, Z., Hirth, R., Rahman, M. & Mor, V. Effect of 41. Chen, M. K., Chevalier, J. A. & Long, E. F. Nursing home staff networks and
nursing home ownership on the quality of post-acute care: an instrumental COVID-19. Proc. Natl Acad. Sci. USA 118, e2015455118 (2020).
variables approach. J. Health Econ. 32, 12–21 (2013). 42. Interim Final Rule Updating Requirements for Notification of Confirmed and
15. Gupta, A., Howell, S. T., Yannelis, C. & Gupta, A. Does private equity Suspected COVID-19 Cases Among Residents and Staff in Nursing Homes
investment in healthcare benefit patients? Evidence from nursing homes. (Centers for Medicaid and Medicare Services, 2020).
Preprint at SSRN https://doi.org/10.2139/ssrn.3785329 (2021). 43. Shen, K. Relationship between nursing home COVID-19 outbreaks and staff
16. Harrington, C., Woolhandler, S., Mullan, J., Carrillo, H. & Himmelstein, D. U. neighborhood characteristics. Preprint at medRxiv https://doi.
Does investor ownership of nursing homes compromise the quality of care? org/10.1101/2020.09.10.20192203 (2020).
Am. J. Public Health 91, 1452–1455 (2001). 44. Weech-Maldonado, R., Lord, J., Davlyatov, G., Ghiasi, A. & Orewa, G.
17. O’Neill, D. COVID-19 in care homes: the many determinants of this perfect High-minority nursing homes disproportionately affected by COVID-19
storm. BMJ 369, m2096 (2020). deaths. Front. Public Health 9, 606364 (2021).
18. Booth, R. COVID-19 outbreaks up to 20 times more likely in large care 45. Chatterjee, P., Kelly, S., Qi, M. & Werner, R. M. Characteristics and quality of
homes, study finds. The Guardian (14 July 2020). US nursing homes reporting cases of coronavirus disease 2019 (COVID-19).
19. Goldstein, M., Silver-Greenberg, J. & Gebeloff, R. Push for profits leaves JAMA Netw. Open 3, e2016930 (2020).
nursing homes struggling to provide care during coronavirus pandemic. The 46. Li, Y., Fang, F. & He, M. Exploring the N95 and surgical mask supply in U.S.
New York Times (7 May 2020). nursing homes during COVID-19. J. Appl. Gerontol. 40, 257–262 (2020).
20. Li, Y., Temkin-Greener, H., Gao, S. & Cai, X. COVID-19 infections and 47. Stall, N. M., Jones, A., Brown, K. A., Rochon, P. A. & Costa, A. P. For-profit
deaths among Connecticut nursing home residents: facility correlates. J. Am. long-term care homes and the risk of COVID-19 outbreaks and resident
Geriatr. Soc. 68, 1899–1906 (2020). deaths. CMAJ 192, E946–E955 (2020).
960 Nature Aging | VOL 1 | October 2021 | 948–961 | www.nature.com/natagingYou can also read