A Population Health Guide for Primary Care Models - ImplementatIon and evaluatIon
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Implementation and Evaluation:
A Population Health Guide for
Primary Care Models
October 2012Care Continuum Alliance
701 Pennsylvania Ave. N.W., Suite 700
Washington, D.C. 20004-2694
(202) 737-5980
info@carecontinuumalliance.org
www.carecontinuumalliance.org
© Copyright 2012 by Care Continuum Alliance, Inc. All Rights Reserved. No part of the material protected by this
copyright notice may be reported or utilized in any form or by any means, electronic or mechanical, including
photocopying, recording or by any information storage and retrieval system, without written permission from the
copyright owner.
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 2Executive Summary
Why Was This Guide Developed?
This Implementation and Evaluation Guide (I&E Guide) was developed by the Care Continuum
Alliance to inform and guide the implementation of key components of population health and
specific strategies and suggestions for primary care-centered models to embed the components into
their practice. In addition, this Guide offers suggestions and resources on measuring the impact of
these efforts from both a cost and a quality perspective. The Guide also offers recommendations for
population health implementation for a variety of models and recognizes that models vary widely by
the resources available, the culture of the practice, organization or group of organizations working
together, and their level of health information technology sophistication. Ultimately, any health care
delivery model that is centered around primary care can benefit from the information delivered in
this Guide.
What Are the Goals of This Guide?
The goal of this Guide is to offer education and guidance on the development and measurement of
population health strategies embedded into the framework of a primary care-centered models. This
Guide focuses on the overall value of population health strategies for primary care and how these
strategies could be both implemented and measured based on the level of sophistication of the
model. This Guide is intended as a resource for primary care-centered models regardless of where
they are in the transformation process and offers suggestions and insight into specific tactics that can
be utilized by any practice at both the clinician level as well as the organization level.
Who Is This Guide For?
This Guide is for any health care entity working towards a patient-centered population health
model of care. It can also be useful for individual primary care and multispecialty practices that are
transforming into a model of care that is whole-patient, whole-population focused. Models that may
find the information and considerations in this Guide especially useful would include:
• Integrated delivery systems,
• Accountable care organizations,
• Patient-centered medical homes,
• Primary care practices,
• Multispecialty practices,
• Community health collaboratives,
• State health exchanges, and
• Large hospital systems.
At the end of this Guide is a reference section with tools and resources that offer additional detail
on several of the topics discussed within the Guide itself. In addition, we have included general
resources in this section that readers will also find useful.
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 3How to Use This Guide
As a resource and tool for primary care practices interested in implementing population health, this
Guide can be read in its entirety for an indepth overview of the value and benefits of population
health. Each section can also be a stand-alone resource on very specific pieces of population health,
including the value of the process, implementation, and evaluation. The following table lists specific
topics that each section covers.
Section Selected Topics Page
Number
Population Health What are the key components of population health? 9
Overview
As a clinician or practice manager, what are the 14
objectives and the benefits of population health?
What are the key benefits of population health for my 15
patients?
How can I implement population health based on my own 18
needs and resources?
Areas of Impact What kinds of impacts can population health have on my 19
practice or model of care?
What is the value proposition for each of the components 21
of population health?
What types of data should I consider if I am assessing the 24
health of my patient population?
Why should I go through the process of risk stratifying my 21
patient population?
What are some strategies that I can use to engage my 27
patients in their care?
Can population health help me to better coordinate the 28
care that patients receive?
What should I think about when I am trying to measure 33
savings of my population health efforts?
What is a comparison group, and why is it important in an 36
evaluation process?
What are leading and lagging indicators, and how will they 39
help me improve quality for my patients?
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 4Table of Contents
Foreword................................................................................................................................................6
Acknowledgments.................................................................................................................................7
Population Health Overview..................................................................................................................9
Best Practices Framework...............................................................................................................13
Areas of Impact......................................................................................................................................19
Impacts Model.................................................................................................................................19
The Value Proposition.....................................................................................................................21
Drivers of Change and Patient Engagement..................................................................................25
Care Coordination...........................................................................................................................28
Measuring Savings...........................................................................................................................33
Appendix: Special Topics..................................................................................................................... 43
Medicaid and Underserved Populations........................................... Release Date: December 2012
Oncology............................................................................................ Release Date: December 2012
Reference A – Health Information Technology Framework..................................................................44
Reference B – Population Health Management Program Evaluation...................................................46
Methodological Considerations
Reference C – Evaluation Study Design Considerations......................................................................54
Reference D – Methods to Define Outliers..........................................................................................55
Reference E – Evaluation Considerations for Small Populations..........................................................56
Reference F – Utilization Measures.......................................................................................................59
Reference G – Self Management Measures..........................................................................................61
Reference H – Medication Adherence Measures.................................................................................63
Reference I – Productivity Measure......................................................................................................74
Reference J – Selection Criteria Considerations...................................................................................76
Reference K – Additional Resources.....................................................................................................81
References..............................................................................................................................................82
Figures and Tables
Figure 1, Population Health Conceptual Framework......................................................................9
Figure 2, Population Health Process Model....................................................................................12
Figure 3, Population Health Impacts Model...................................................................................20
Figure 4, Population Levers for Change..........................................................................................26
Figure 5, Engagement Strategies Wheel........................................................................................27
Figure 6, PHM Impacts on Care Coordination...............................................................................29
Figure 7, Disease Progression Chart...............................................................................................39
Figure 8, Leading and Lagging Indicators......................................................................................42
Table 1, Population Health Objectives............................................................................................14
Table 2, Population Health Benefits................................................................................................15
Table 3, Population Health Components – Best Practice Implementation Levels
for Primary Care Clinicians........................................................................................................18
Table 4, Data Sources Value............................................................................................................24
Table 5, PHM Drivers of Change for Primary Care.........................................................................25
Table 6, Areas for Assessing Savings..............................................................................................35
Table 7, Comparison Group Options..............................................................................................37
Table 8, External Comparison Sources...........................................................................................38
Table 9, Utilization Measure Options..............................................................................................40
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 5Foreword
Amid the backdrop of ongoing political debate about its merits, health care reform and all that it
entails is quickly being implemented in every state. New models of care with primary care-based
population health at the center are coming into focus as they rapidly propagate through the health
care landscape.
Population health is a priority because of the financial and outcomes pressures inherent in reform.
Not only do providers need to concern themselves with patients who seek care, they also now must
engage whole populations in order to meet expectations. A population-driven, patient-centered
model of care can meet the needs of all consumers regardless of where those consumers are on the
continuum of health. With primary care at the center of a model surrounded by support that includes
a combination of health information technology, the care team and ancillary providers, diverse care
needs can be met, quality can be improved, and cost will be sustainably impacted.
Embedding population health into these new models and assessing its impact can be challenging for
models already in the midst of transformation in so many other ways. The Care Continuum Alliance
represents the population health industry and has developed the following Implementation and
Evaluation Guide as a resource for primary care-centered models that are transitioning to population
health.
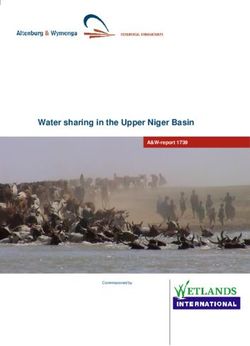
The foundation for the I&E Guide is the CCA Population Health Conceptual Framework (see Figure
1). The Conceptual Framework, released in 2010, outlines the key components necessary to deliver
population health to any defined population and in any setting. This Guide builds upon each of the
components in the framework, offering insight into the essential purpose of each component as well
as how to implement and evaluate a broad population health strategy. The Guide also incorporates
several years of Care Continuum Alliance efforts that explore appropriate program evaluation criteria
for population health management programs.
Many industry experts and partner organizations worked together to develop and offer comments
and feedback on the Guide, and we are grateful to all who supported this important work.
Jason Cooper, MS, and David Veroff, MPP
Co-Chairs, CCA Quality & Research Committee
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 6Acknowledgments
Quality & Research Committee Kelly Shreve, Capital Blue Cross
Co-Chairs: Earl Thompson, HealthFitness
Jason G. Cooper, MS Barry Zajac, MHSA, Blue Cross Blue Shield of
David Veroff, MPP, Health Dialog, Inc. Louisiana
Reviewers: EVALUATION DESIGN IMPACT
Jason G. Cooper, MS R. Allen Frommelt, PhD, Nurtur
Donald W. Fisher, PhD, CAE, American Medical Andre Gibrail, AxisMed Gestao Preventiva da
Group Association Saude S.A.
Helene Forte, RN, MS, PAHM, Aetna Gary Persinger, National Pharmaceutical Council,
Inc.
Sue Frechette, BSN, MS, MBA, Northfield
Associates LLC Tina Ross-Knapp, CCP, APS Healthcare, Inc.
Cindy Hochart, RN, MBA, PMP, Heartland Health David Veroff, MPP, Health Dialog, Inc.
Marcia Nielsen, PhD, MPH, Patient Centered Kimberly Westrich, National Pharmaceutical
Primary Care Collaborative Council, Inc.
Mary Jane Osmick, MD, American Specialty
Health DRIVERS OF PATIENT & PROVIDER CHANGE
David Veroff, MPP, Health Dialog, Inc. Felicia Brown, RN, Blue Cross Blue Shield
Association
Work Groups: Helene Forte, RN, MS, PAHM, Aetna
PHM PRIMARY CARE BEST PRACTICES Cynthia Hallam, RN, MBA, Blue Cross Blue Shield
FRAMEWORK of Louisiana
Mary Jane Osmick, MD, American Specialty Cindy Hochart, RN, MBA, PMP, Heartland Health
Health Tina Ross-Knapp, CCP, APS Healthcare, Inc.
Christobel E. Selecky, ZIA Healthcare Kelly Shreve, Capital Blue Cross
Consultants
Cindy Worrix, RN, CCP, Aetna
Susan Weber, RN, CCM, MHP, StayWell Health
Management
CARE COORDINATION MEASURES
Nancy Wilson-Ramon, IdealHealthIT
Marybeth Farquhar, PhD, MSN, RN, URAC
Betsy Farrell, RN, Aetna
VALUE PROPOSITION FRAMEWORK
Helene Forte, RN, MS, PAHM, Aetna
Felicia Brown, RN, Blue Cross Blue Shield
Association Andre Gibrail, AxisMed Gestao Preventiva da
Saude S.A.
Steven Burch, RPh, PhD, GlaxoSmithKline
Garry Goddette, RPh, MBA, Alere
Sue Frechette, BSN, MS, MBA, Northfield
Associates LLC Diane M. Hedler, RN, MS, CHIE, Kaiser
Permanente
R. Allen Frommelt, PhD, Nurtur
Cindy Hochart, RN, MBA, PMP, Heartland Health
Thomas L. Knabel, MD, Ingenix Inc.
Suzanne Janczak, Health Integrated, Inc.
Jennifer Pitts, PhD, Edington Associates
Peter J. Kapolas, RN, MBA, CPHQ, Healthways
Tatiana Shnaiden, MD, ActiveHealth
Management, Inc. Erik Lesneski, AllOne Health
Cynthia O’Neill, URAC
Mary Jane Osmick, MD, American Specialty
Health
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 7Urvashi Patel, PhD, Horizon Blue Cross Blue Medicaid and Underserved Populations
Shield of New Jersey
Jason G. Cooper, MS
Gary Persinger, National Pharmaceutical Council,
R. Allen Frommelt, PhD, Nurtur
Inc.
Carl Garrett, Centene Corporation
Lisa Saheba, MPH, URAC
Toni Miller, CareSource Management Group
Chris Tourville, RN, MSHM, FAHM, Cigna
Arnold Ari Wegh, ActiveHealth Management,
Inc. SPECIAL TOPICS – SHARED DECISION-MAKING
Jason G. Cooper, MS
TOTAL COST SAVINGS Andrea Fong, Health Dialog
David Aronoff, Nurtur Natalie Heidrich, Ethicon Endo-Surgery
Jean Ann Cherry, BSN, MBA, OptumHealth Paul C. Mendelowitz, MD, MPH, ActiveHealth
Natalie Heidrich, Ethicon Endo-Surgery Management, Inc.
Cindy Hochart, RN, MBA, PMP, Heartland Health Julie Slezak, MS, Silverlink Communications
Iver Juster, MD, ActiveHealth Management, Inc. Arnold Ari Wegh, ActiveHealth Management,
Inc.
Diana Potts, APS Healthcare, Inc.
Carrie Wolbert, APS Healthcare, Inc.
Julie Slezak, MS, Silverlink Communications
David Veroff, MPP, Health Dialog, Inc.
SPECIAL TOPICS – ONCOLOGY
Courtney Cantrell, RN, Aetna
Jason G. Cooper, MS
R. Allen Frommelt, PhD, Nurtur
Jody Garey, PharmD, US Oncology
Deb Harrison, US Oncology
Jad Hayes, MS, ASA, MAAA, McKesson
Specialty Health
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 8Population Health Overview
The Care Continuum Alliance has developed As mentioned, there are two specific models
frameworks to illustrate, both conceptually or frameworks used in this Guide that will be
and operationally, the process and activities referenced: the Population Health Conceptual
associated with population health. These Framework (Figure 1), which will be referred
frameworks have been developed as a guide to as the “Conceptual Framework”, and the
for care delivery models seeking to integrate Population Health Process Model (Figure 2),
and implement population health strategies, which will be referred to as the “Process Model.”
components, and processes. The population The intent of the Conceptual Framework is to
health framework can be embedded into a identify the general components of population
primary care integrated system in a variety health and how they relate to one another.
of different ways. For example, primary care- The Conceptual Framework depicts the
centered delivery models such as integrated identification, assessment and stratification of
delivery systems and accountable care patients. The core of the model (central blue
organizations, as well as in patient-centered box) includes the continuum of care, as well
medical home practices, can adopt the as patient-centered interventions. The patient
processes and key components outlined in these is central in the model, and is surrounded by
frameworks to assess their own capabilities and various overlapping sources of influence on of his
to guide the development of expanded and or her health. This can include, but is not limited
integrated care delivery models. to, organizational interventions,
Figure 1. Population Health Conceptual Framework
Patient & Provider
Primary Care
Care Continuum Alliance 9provider interventions and family and interventions in a continuous cycle of quality
community resources. Operational measures are improvement and improved patient experience.
represented as are the core outcome domains.
Finally, the cycle of quality improvement In addition, this process can offer information
based on process learnings and outcomes is that will be extremely helpful in a clinician’s
prominently depicted by the large curved green efforts to engage with patients in the patient’s
arrows. plan of care. It is becoming increasingly evident
that effective enrollment and engagement is key
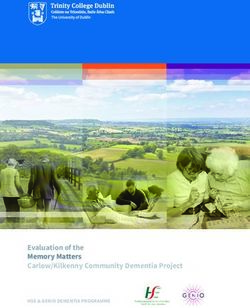
The intent of the Population Health Process to impacting the health of a patient population.
Model is to help improve our understanding
of the essential and detailed elements of Risk Stratification
population health. This Process Model outlines The next step in the population health process
the process flow associated with delivering is to stratify patients into meaningful categories
the key components of population health, for patient-centered intervention targeting, using
beginning with monitoring the population and information collected in the health assessments.
identifying patients who are appropriate for an This process yields information that the system
activity or intervention. It also includes a health can use to divide the patient population into
assessment stage, followed by risk stratification, different levels to ensure ROI based on resources
the application of engagement strategies, allowed. Stratification should include categories
the availability of multiple communication that represent the continuum of care in the
and delivery modalities, patient-centered patient population. While some organizations
interventions across the care continuum use complicated and proprietary mathematical
and the process of evaluating the impact of algorithms to predict risk, others use a simple
these efforts in multiple domains. Finally, it count of risks to classify individuals. It is not
includes a feedback loop that reflects the need our intent to prescribe how risk stratification
to incorporate process and quality-related should be conducted, rather to emphasize the
improvements based on learnings from the importance of having some type of stratification
impact evaluation. The sections below provide in place to help align patients with appropriate
a detailed description of the components of the intervention approaches, thereby maximizing the
Process Model. health improvement impact of care. This process
is designed to aid both the organizations and
Health Assessment clinicians by helping them focus appropriate
The Health Assessment section of the Process resources on those patients and segments of the
Model represents the effort to assess the health population with greatest need. Furthermore, the
of a specific population (i.e., patient panel, care team will be better equipped to identify
diabetic population, etc.). This assessment opportunities to impact a patient’s health either
typically “triangulates” by drawing on available by addressing gaps in care or by offering new
types of information, including self-reported evidence-based interventions determined by a
health questionnaires, health insurance claims, new diagnosis or newly discovered risk factor.
laboratory and pharmacy data and clinician-
documented information. Analytics and the Patient-Centered Interventions
ability to combine and analyze this data is a key Whenever possible, the components of
part of this process. It also is important to point population health can and should be offered
out that, while there is an initial assessment, through a variety of communications and
repeated measures over time are necessary to interventions in order to maximize the clinician’s
demonstrate changes in health status of patients resources and reach and to accommodate
and populations over time. This monitoring of the preferences and technological abilities of
results in a continuous feedback loop for the patients with the ultimate goal of increased
care team facilitates documenting the progress patient engagement and support for self
of any population-based care over time, management. For example, some patients,
establishing new baselines and adjusting care perhaps those with low risk, may prefer to
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 10receive everything through the mail, while the conceptualization of the overall strategy
others might want to participate through an and specific intervention approaches. Careful
on-line program geared toward education and consideration of the chain of effects that will
information sharing. Some interventions are eventually lead to the ultimate goal or outcome,
best delivered directly by the provider during and inclusion of those outcomes in the impact
a standard office visit, while other interventions evaluation framework, can help clinicians to
and care plans may be offered through a identify the components needed to impact
combination of intervention modalities. The those outcomes. Additionally, because there are
Process Model includes social media as a many that contribute to the financial impact of
delivery modality to reflect the increasing an intervention, explicitly outlining the predicted
popularity and promise of this type of health short-, intermediate- and long-term outcomes
education and support. Matching intervention can help primary care-centered models
modalities to the preferences of patients likely understand the full range of impacts and the
will lead to an increased level of participation expected time frame for ultimately generating
and engagement, and ultimately to improved cost savings. Finally, a well-constructed
patient health. conceptual outcomes framework can help with
interpretation of outcomes and shed light on
Impact Evaluation the practical implications of evaluation findings.
To maximize the health impact of a patient- Demonstrating that short- and moderate-
centered intervention or activity, it is important term outcomes are occurring as expected can
to consider the environment of patients and, provide early evidence to clinicians that efforts
whenever possible, to employ interventions are benefitting patients. Conversely, if early
designed to create a supportive environment outcomes are contrary to expectations, early
and organizational culture for patients. The link in reporting allows for midcourse corrections to the
the outcomes framework between environment activities.
and the actual tailored interventions represents
the implicit hypothesis that population health Quality Improvement Process
will impact psychosocial variables that will then Lastly, Quality Improvement Process is also
drive changes in health behaviors, including represented in the both the Conceptual
self-management and the use of screening and Framework and the Process Model. The cycle
preventive services. Improvements in these of quality improvement includes changes to
behaviors will, in turn, have a positive impact on both interventions and processes (including
patient health and clinical outcomes. In addition, assessment, stratification and engagement/
the Impact Evaluation section of the Process enrollment strategies) based on process
Model represents the ultimate impact on service learnings from operational measures, as well
utilization, provider and patient satisfaction, and as outcomes. This process also highlights the
financial outcomes derived from improvements patient's voice through data collection that will
in health behaviors, health and clinical outcomes lead to an enhanced patient experience.
and productivity.
Health information technologies (HIT) continue
Outlining a framework for an intervention’s to increase in their importance to population
associated outcomes can have several practical health. CCA developed the HIT Framework to
applications. It can help systematize the help identify the key components necessary
design and implementation, as well as the to fully operationalize population health.
evaluation processes. Whether the evaluation Reference A includes a full discussion of the HIT
framework is created before or parallel to Framework, first released in Volume 5 of the
the intervention deployment, it can help with Outcomes Guidelines Report.
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 11Figure 2 – Population Health Process Model
Population Monitoring / Identification
Health Assessment 1
HRA Medical Claims Lab Data Other
Incentives & Rewards
Incentive Reward
Risk Stratification2
Enrollment/ Participation
Healthy Health/Emotional Chronic Illness End Of Life Engagement Outcomes
Risk
Quality Improvements Based on Process Learnings and Outcomes
Enrollment / Engagement Strategies
Communication and Intervention Delivery Modalities1,2
Mail E-mail Telephone Internet/Intranet Social Media Face-to-Face Visits
Patient-Centered Interventions1
Health Continuum
• Program Referrals (External/Internal)
Organizational Interventions
Culture/Enviornment • Integrated/Coordinated Components
Health Promotion, Health Risk Care Coordination/ Disease/
Wellness, Management Advocacy Case Management
Preventive Services
Tailored Interventions2
Operational Measures Impact Evaluation
Program Outcomes
Health Status and
Clinical Outcomes
Psychosocial
Drivers Health Behaviors
Quality of Productivity
Self-Management
Life
Satisfaction
Patient/Provider
Screening /Preventive
Services
Service Utilization
Financial Outcomes
Time frame for Impact
1 Represents example components for each essential element. Does not necessarily reflect the universe of components.
2 Communication may utilize one or more touch points within the delivery system.
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 12Best Practices Framework staff may implement population health in a very
different way. The best practices framework
Population health is a framework that can section has been developed to help each model
be implemented in a variety of settings and and practice understand the various options
for many different populations. In addition, available for implementing population health
the strategy can be implemented in varying and specifically at a tactical level what those
degrees or levels based on resources, options look like.
technology sophistication and the practice’s
current stage of transformation. Even basic The section begins with detail on the basic
differences in practices will very likely play a objectives and benefits of each population
role in how population health is implemented. health component for the organization as well as
For example, a small practice of primary care for the clinician, and for the patient. Following
physicians, who have an electronic health these grids is a framework that offers steps to
record and disease registry in place as well as a population health implementation at a tactical
care coordinator, may be able to implement a level specifically for the clinician. Additional
population health strategy at a very high level, frameworks will be added for the other levels at
while a rural, integrated delivery system with a later date.
few technology resources in place and limited
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 13Table 1. Population Health Objectives
Mary Jane Osmick, MD
Population Health Domain Organization Clinician Patient
Patient Population Identification Use eligibility/administrative data to push Become aware of all patients in managed Link self to medical home and organization
updated ”population list” to clinicians population
Health Assessment Assess customer base demographics, values Use validated tools to assess patient health • Increase awareness of health risks and
and special needs risks, preferences, activation and values within conditions
defined patient panel • Increase understanding of health risks and
conditions
Risk Stratification • Identify cost drivers, at-risk individuals in • Prioritize at-risk patients and intervene to • Understand condition severity
patient population decrease both acute and long-term risks • Understand how behaviors affect risks and
• Prioritize at-risk patients for clinicians • Offer appropriate patient support based conditions
• Identify and offer tailored interventions on risk and segment
for segments
Engagement • Support engagement of patient Offer patient-specific care plans and ancillary • Participate in defining customized care plan
population interventions based on identified patient • Receive information and support tools to
• Help patients access care and needs, preferences, activation, values, become activated in care
interventions appropriately capabilities
Patient-Centered Interventions Direct resources toward the areas of greatest Assure every at-risk patient receives timely Learn how to implement self-care plan to
population risk and opportunities for health care and has access to resources to help improve/stabilize health
improvement manage acute and chronic health needs
Impact Evaluation • Use analytics to understand and improve • Access ”scorecard” to understand and Improve health risks and control of conditions
population health interventions impact improve performance relative to others
• Push “scorecard” to individual clinicians • Identify areas for care improvement
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 14Table 2. Population Health Benefits
Population Health Domain Organization Clinician Patient
Patient Population Identification Understands make-up of assigned population Focuses defined resources on identified Has medical home and trusted organization
patients
Health Assessment Drives organizational strategy and allocation Defines and directs staff/ancillary resources • Creates individual patient base line
of resources to support identified population required to meet needs of identified • Provides opportunity for more meaningful
individuals clinician encounters
Risk Stratification • Identifies cost drivers, patients at risk • Provides more efficient encounter for • Provides appropriate level of care based on
• Helps define interventions required to patients/clinicians condition severity
support population and segments • Enables proactive interventions to maximize • Offers resources specific to identified needs
outcomes and P4P payments
Engagement • Reduces out-of-network utilization Enhances practice efficiency (seeing patients • Provides customized care experience
• Promotes outcomes-driven use of the appropriately) while being comfortable that • Promotes partnership with clinician
system the entire patient population’s needs are
being met
Patient-Centered Interventions • Optimizes population engagement • Enhances practice efficiency (seeing • Promotes improved likelihood of patient/
consistent with preferences, values patients appropriately) while being family participation in care plan
• Focuses resources on appropriate comfortable that the entire patient • Promotes improved adherence to evidence-
population cohorts population’s needs are being met based interventions
• Optimizes outcomes and P4P payments
Impact Evaluation • Identifies improvement opportunities • Improves health of clinician population • Provides feedback, motivation
• Identifies savings opportunities • Increases revenue through quality and P4P • Promotes self-care management
payments
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 15Various primary care-centered models are In Table 3, the six population health components
likely to implement population health and its are arrayed across the page from left to right:
individual components in a variety of ways. How, 1. Identification,
as well as how completely, the components are
2. Health Assessment,
implemented will depend largely on the specific
characteristics of the health care practice 3. Risk Stratification,
or organization, the resources available to 4. Engagement,
support the effort, and the collaborations and
5. Patient-centered Interventions, and
partnerships that exist within the matrix of the
organization. Although implementations may 6. Impact Evaluation.
vary widely based on how organizations learn
and grow, best practices will certainly emerge Each of the six components are broken down
over time. One can assume that organizations into five “Population Health Best Practice
will take a phased-in approach, and demonstrate Levels” (from Level I at the bottom through
iterative improvement as they become more Level V at the top). In each of the five cells under
sophisticated in defining their own delivery the six population health components, a brief
model and responding to the need to produce description of the clinician function at each level
favorable outcomes. is presented. The goal of presenting Levels I to V
is to demonstrate progression towards clinician
In Table 3, we present a clinician-specific best practice in each of the six components.
framework which highlights how the role Moving upward in any of the six components
of the clinician must change based on (from Level I to V) demonstrates enhanced
the components of population health. (In integration among clinicians, improved data
subsequent publications, the framework will be access and connective technology, use of valid
expanded and also focus on the changing role of measurement and decision-support tools – all of
organizations, as well as the patient.) which strengthen the medical home model.
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 16Each of the five best-practice levels is described knowledge of other practitioner interventions
below: becomes easier. In addition, at this level all
clinicians and facilities identify the concept
Level I represents (mostly) a “manual” system,
•
and need for a patient medical home, and
with no or rudimentary connection to wider
are working with each other and technology
systems of care. Here, the clinician (or group
to make this happen. Often in this level,
of clinicians) works individually with a patient,
text-based, non-searchable documents exist,
generally becoming aware of need only
disallowing true integration of longitudinal
when the patient presents for care. At this
patient data. Clinicians may begin to
level, the clinician tends to be reactive, and
communicate with patients electronically in
“waits” for individuals to identify themselves
a secure and HIPAA-compliant environment.
with specific health care needs. Information
Clinicians begin to receive outcomes data
is limited to what is shared between patient
from the larger health care system, and
and clinician at point of care and is refreshed
performance targets are set. Clinicians may
as the patient presents to the clinician time
have ability to share personal health records
over time. The clinician is required to function
with patients.
as the integrator of information – patient and
practice-specific. Longitudinal patient data is • Level V is characterized by the existence
difficult to identify. of valid, frequently refreshed data and
information represented in a dashboard-
Level II demonstrates that clinician and staff
•
type format to enhance the patient-clinician
have an awareness of the patient population,
relationship. At a high level, infrastructure,
but may lack connectivity. The clinician
information, and incentives are all aligned
continues in “manual mode”, although some
and in place for fully-coordinated patient
functions may be accomplished electronically
care across applicable care settings. More
(i.e., billing). They may identify and focus on
specifically, decision support tools flag
specific diagnoses (such as diabetes, etc.) and
opportunities for error reduction/patient
individual complex patients who frequently
safety, enhanced outcomes, etc. Here, there
present for care.
is full viewing of all medical information in a
• Level III begins the transition toward HIPAA- compliant way for all clinicians and
population health, as the practice shifts patients. Patients decide what and how much
to electronic venues for some patient information they choose to have available. In
interactions. A registry of specific health addition, two-way ongoing communication
conditions and risks may be available to the occurs through all available electronic and
clinician and staff. Proactive outreach to face-to-face modalities. Peer support is
individuals identified with high risk become available for patients who choose this method
possible to prevent avoidable hospitalizations of self-management. A team that supports
and ED visits. At this level the clinician is still the patient population is also clearly identified
reactive, but this is the earliest form of an at this level. Finally, a patient/family/support
automatic “push" of patient information to the structure is in full collaboration with the
clinician. clinician and coordinated care team (who have
Level IV includes the assumption that
• all the patient information needed to play
electronic connectivity exists within the their role).
practice with some ability to connect to
the larger system of care. In this setting,
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 17Table 3. Population Health Components - Best Practice Implementation Levels for Primary Care Clinicians
1 2 3 4 5 6
Patient Population Health Assessment Risk Stratification Engagement Patient-centered Impact Evaluation
Identification Interventions
Clinician receives Clinician auto-notified Valid tools auto- stratify “Medical home”; Clinician/Patient Real-time feedback;
Level V real-time, patient & of new or conflicting patients & population clinician monitors, collaborative care plan; outcomes meet &
population specific data info requiring resolution across all clinicians; optimizes care plan & 1°, 2°, 3° prevention exceed patient , peer,
at point of care gaps flagged for action care team across all focus; coordinated team population goals
settings
PHM Best Practice Level
Patient information Patient health, values, Stratification lists Clinician engages with Clinician aware of & Clinician receives
Level IV available from all preferences assessed; available based on patient in “medical responds to patient patient outcome info;
clinicians - ID, risks, clinician receives info claims, HA, labs, home,” coordinates needs/preferences performance goals set
condition control for consideration screening info across connected focus on 1°, 2°, 3° in peer organization
settings prevention
Clinician registry – key Clinician evaluates New health risks Clinician engages with Clinician focuses on Clinician unaware of
Level III diagnoses, tests, Hx, health risks based identified through patient focusing on 1°, 2°, 3° prevention; patient outcome unless
and condition control on year-over-year health assessments and both past and newly strategies for risks directly involved in care
comparing assessments via registry lists identified risks identified
Clinician has patient list Clinician asks patients Risk based on “frequent Clinician engages with Intervention based on Clinician unaware of
Level II with diagnoses for baseline health flier” status & clinician patient episodically at current patient need patient outcome unless
assessment; assesses lists with diagnoses patient presentation and known health risk(s) directly involved in care
patient at the visit
Clinician identifies Clinician assesses Clinician aware of high- Clinician engages with Intervention based on Clinician unaware of
patient through direct patient at the visit risk patients based on patient episodically at current patient need patient outcome unless
Level I interaction and hard- “frequent flier” status patient presentation and known health risk(s) directly involved in care
copy records
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 18Areas of Impact
Once embedded in a primary care-centered The relationship between the patient and the
model of care, the process of delivering clinician can have a strong impact on patient
population health as outlined in the Conceptual engagement in the care process, as well as on
Framework and Process Model (see pages 9 the patient’s treatment adherence, engagement
and 12) can impact that model in a variety of in tailored population health interventions, self
different ways. The Population Health Impacts management, and a healthy lifestyle.
Model (Figure 3) offers a high level overview of
the purpose, value and clinician-related impact An important feature of population health is that
of each of the components of population health. it can have positive impact on both the patient
Following the model are four subsections that and the clinician. As depicted in the model,
specifically discuss the impact of population impacts on the clinician include, but are not
health on 1) primary care, 2) drivers of change limited to, more comprehensive understanding
and patient engagement, 3) care coordination, of patient health risks, more efficient and
and 4) measuring savings. effective use of resources, better quality care,
increased overall satisfaction, and ultimately,
Impacts Model more positive patient outcomes. These patient
outcomes include, but are not limited to, better
The Population Health Impacts Model represents awareness and self-efficacy (psychosocial
the primary elements of the Conceptual impacts), improved health behaviors, enhanced
Framework (health risk assessment, risk health status and quality of life, and more
stratification, engagement, patient-centered appropriate service utilization.
interventions, and impact evaluation). In
addition, the model represents the purpose, A final feature of the Impacts Model is the
value proposition, and clinician impact for each quality improvement process that can be
of these areas, as well as the patient impact in facilitated by the ongoing evaluation of impact.
several important domains. Information from the impact evaluation can
be used to enhance and refine the health
Like the Conceptual Framework, the Population assessment process, risk stratification, the
Health Impacts Model includes patient-centered intervention process and content of the
interventions as the core, and the patient is interventions, and ultimately, the relationship
central. But unlike the Conceptual Framework, between the patient and clinician.
the patient is not alone in the center of the
model. Here, the patient-clinician interaction is More detailed information about the value
central. Health assessment and risk stratification proposition for each of the Model components
give the clinician important information that can be found in the sections that follow.
brings richness and value to the patient- For further discussion on self management
clinician conversation. The patient-centered measures see Reference G, and for medication
interventions give the clinician valuable tools adherence measures see Reference H.
to offer patients across the health continuum.
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 19Figure 3. Population Health Impacts Model
Jennifer Pitts, PhD
Health Assessment
Clinician Impact
• C omprehensive understanding of patient
Purpose Value Proposition
health/risk
• C
ollects important information • P
rovides a comprehensive view of • E nhanced care plan
about patient health risks and health health status and individual risks in • S tronger patient engagement
behaviors clinician’s practice panel communication
• Increased clinician work satisfaction
Risk Stratification
Value Proposition Clinician Impact
Continuous Quality Improvement
Purpose
• Improves clinician understanding of uality Indicators
Q
• S
tratify patients into meaningful
how to guide and support patient • Efficient and effective use of resources
categories for personalized
efforts to maintain health and/or • Quality of the care plan for individual
intervention targeting
reduce risks patients
Engagement in Patient-
Centered Interventions PATIENT- clinician INTERACTION
• Optimal use of time with patient
Health Promotion • Targeted communication and education Disease Management
Preventive Services • Quality of communication Case Management
• Engage in shared decision-making
Population Health Across the Health Continuum
Value Proposition
Purpose Clinician Impact
• A
ssure every at risk patient receives
• P
rovide resources for patients across • Improved patient health status
timely care and has access to resources
the health continuum to support the • Improved patient health management
to help manage acute and chronic
needs of the entire patient population • Improved quality and cost outcomes
health needs
Impact Evaluation
Patient Outcomes
Clinician Impact
Healthy Behaviors Quality of Life Service Utilization • Better understanding
Psychosocial Drivers of opportunity to
• S
elf-Management Clinical/Health Status Improved • In- and Out-patient
• Awareness enhance patient care
• S
creening & • Health Status communication and Visits • Knowledge to self
• Readiness
Prevention • BMI, BP, Labs relationship with • E R Visits assess and improve as
• Self-efficacy
• Treatment Adherence clinician • P harmacy a clinician
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 20The Value Proposition in that particular band of the continuum. For
example, providing nutrition education to all
Sue Frechette, BSN, MS, MBA, R. Allen Frommelt, patients may promote behavior change for
PhD, Thomas L. Knabel, MD, Tatiana Shnaiden, MD,
Kelly Shreve, Earl Thompson, and Barry Zajac, MHSA some. However, targeting specific patients
who are at-risk for diabetes and/or are obese
As health care continues to transform,
based on their risk status would be more
population health is often designated as a key
impactful.
part of the process. The Conceptual Framework
identifies the six core component to the •
At the organization level, risk stratification
process of delivering population health. This yields information that can be used to
section reviews the value proposition for each effectively and efficiently allocate resources
component as well as the ultimate impact of and lead to the greatest health impact.
population health overall. Without a clear picture of the risk of a patient
population, decisions regarding what type
Health Assessment Value and to whom an intervention should be
delivered can be imprecise and unfocused.
Assessing the health of a patient benefits the
For example, if a practice finds through a risk
primary care-centered model for both the
stratification process that its patient panel
clinician as well as the organization by enhancing
consists of a high percentage of healthy
the available knowledge of the overall health of
people and people at low health/emotional
a patient and/or a group of patients. There are
risk, then resources could be allocated for
many types of data and data sources available
interventions that focus on prevention and
for this process, each adding its own value to
wellness. However, if risk stratification reveals
the assessment. Table 4 identifies both the data
a higher percentage of patients with chronic
source and the value of each.
illness, then the practice may decide to invest
resources in chronic care and complex case
Bringing together individual level data from
management.
multiple sources provides value to the primary
care team. For example, an ACO affiliated with
Engagement Value
a payer could understand how accessing claims
data would be relatively easy, while an ACO in Engagement requires an alignment of personal
the Boston area—where there are a relatively and program goals in the overall context of
large number of smaller payers—would see that intrinsic motivation and is different from a
same process as requiring a greater investment. patient’s general participation. Two relevant uses
An ACO affiliated with a hospital system that from Merriam-Webster’s dictionary apply here:
has implemented and enjoys a high adoption (1) emotional involvement or commitment and (2)
rate of electronic health records (EHRs) would the state of being in gear.1 In short, engagement
make different investment decisions than one is (1) a psychological state which (2) manifests
that doesn’t, and the presence of an advanced in positive behavior change. As such, it consists
regional health exchange would also affect that of self-determined participation in intervention-
decision. directed activities in alignment with patient goals
to which the patient is dedicated. Engaging
Risk Stratification Value patients in their own health improvement
from a clinician perspective includes patients
Risk stratifying a patient population offers two
and families engaging with their primary care
key values:
practice to improve health care delivery and
•
For the individual clinician, risk stratification patients and families engaging in the health of
gives the information they need to match their communities. Engagement requires several
patients to the most appropriate intervention. psychological and environmental conditions that
This matching depends on where the patient must be present to some degree. The seven
lands on a stratification continuum and the precursors to positive behavior change are listed
nature of the factors that place the patient on the next page.
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 21The value of engagement from a patient Patient-Centered Interventions
perspective is in having the capability to make The value of having a broad range of
behavior change, maintain recommended organizational and tailored population health
behavior, or self manage health. From the interventions is the ability to provide the best
clinician and organization perspective, the (or most appropriate) intervention from the
perceived value is having realistic expectations right source and delivered in the right way
of the largest superset of the patient population for each patient, depending upon where they
that could be impacted by an intervention, are on the health continuum, as well as to
thereby improving health and lowering overall enable a measurable change in behavior with
cost. corresponding measurable change in health
status (or outcome). Tailored interventions will
Patients and their primary care team are partners vary based on both the availability of those
in patient-centered models of care. Population interventions and the current reimbursement
health management requires both prevention model. In addition, the most appropriate
and treatment of disease and a focus on wellness interventions can only be determined once
and quality of life. The primary care practice the health of the patient population has been
engages with the patient to support improved assessed and stratified by risk. Clinicians may
health behaviors (e.g., medication management, initially focus on patients in the higher risk
glucose monitoring, etc.) and self-management categories but ultimately will deliver a broad
of chronic conditions. range of patient-centered interventions to all
patients. The lack of ability and information
Engagement begins with a clear understanding necessary to tailor interventions based on risk
by the care team of the patient’s health and and patient need could result in ineffective
behavior change goals which are documented and inefficient use of limited health care
in the patient's care plan. Engagement can then resources. In addition, resources could be used
be measured by assessing specific behavior unnecessarily, resulting in an increase in health
changes through self or other administered care consumption without improvement in either
assessment. There are several standardized tools health or cost. Examples of high-risk tailored
available to accomplish this, including the Patient interventions would include:
Activation Measure. In addition, an indirect
• For the patient with congestive heart failure
measure can be taken by monitoring behavioral
(CHF) at high risk for ER use:
progress toward the goals required. Examples
of indirect or process measures include: • CHF clinics (typically sponsored by
regular communication on progress, refills hospitals)
of medications, office visits, activity logging, • Home care visits
appropriate screenings performed, etc.
• Home monitoring equipment (BP, HR,
weight)
• Case and chronic care management
• Caregiver and community engagement
• For patients with diabetes:
• Diabetic educators/nutritionists
Clinician Checklist: Precursors to Behavior Change
• Medication management
Sense of necessity for change.
Willingness to experience anxiety or difficulty. • Self management programs (Several
Awareness of the problem. national programs are being adopted by
Confronting the problem. hospitals.)
Effort toward change. • Diabetes support groups
Hoping for a positive change.
Social support for change.2
Care Continuum Alliance • Implementation and Evaluation: A Population Health Guide for Primary Care Models 22You can also read