A New Hypothesis for Alzheimer's Disease: The Lipid Invasion Model
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Journal of Alzheimer’s Disease Reports 6 (2022) 129–161 129
DOI 10.3233/ADR-210299
IOS Press
Hypothesis
A New Hypothesis for Alzheimer’s Disease:
The Lipid Invasion Model
Jonathan D’Arcy Rudge∗
School of Biological Sciences, University of Reading, Reading, Berkshire, United Kingdom
Received 1 October 2021
Accepted 5 February 2022
Pre-press 11 March 2022
Published 25 March 2022
Abstract. This paper proposes a new hypothesis for Alzheimer’s disease (AD)—the lipid invasion model. It argues that AD
results from external influx of free fatty acids (FFAs) and lipid-rich lipoproteins into the brain, following disruption of the
blood-brain barrier (BBB). The lipid invasion model explains how the influx of albumin-bound FFAs via a disrupted BBB
induces bioenergetic changes and oxidative stress, stimulates microglia-driven neuroinflammation, and causes anterograde
amnesia. It also explains how the influx of external lipoproteins, which are much larger and more lipid-rich, especially more
cholesterol-rich, than those normally present in the brain, causes endosomal-lysosomal abnormalities and overproduction of
the peptide amyloid- (A). This leads to the formation of amyloid plaques and neurofibrillary tangles, the most well-known
hallmarks of AD. The lipid invasion model argues that a key role of the BBB is protecting the brain from external lipid access.
It shows how the BBB can be damaged by excess A, as well as by most other known risk factors for AD, including aging,
apolipoprotein E4 (APOE4), and lifestyle factors such as hypertension, smoking, obesity, diabetes, chronic sleep deprivation,
stress, and head injury. The lipid invasion model gives a new rationale for what we already know about AD, explaining its
many associated risk factors and neuropathologies, including some that are less well-accounted for in other explanations of
AD. It offers new insights and suggests new ways to prevent, detect, and treat this destructive disease and potentially other
neurodegenerative diseases.
Keywords: Alzheimer’s disease, anesthesia, anterograde amnesia, apolipoproteins, blood-brain barrier, cholesterol, ethanol,
lipids, lipoproteins, nonesterified fatty acids
INTRODUCTION called amyloid plaques and neurofibrillary tangles
(NFTs). While both plaques and NFTs are individu-
This introduction sets out the basic evidence for the ally seen in other forms of neurodegeneration [2–5],
lipid invasion model of Alzheimer’s disease (AD). their occurrence together is largely unique to AD.
AD is a neurodegenerative disorder first described AD has emerged as the most common dementia,
by the German physician Alois Alzheimer in 1907 accounting for over half of all such disorders, with
[1]. It is a cause of dementia characterized by the an especially high prevalence among over-85 year-
extensive death of brain cells and associated with two olds in the developed world [6]. Yet, in the century or
types of strongly-staining deposits within the brain, so since AD’s discovery, relatively limited progress
has been made in understanding its etiology or in
∗ Correspondence to: Jonathan D’Arcy Rudge, PhD, Paddock
developing effective treatments to stop its progression
Road, Caversham, Reading, Berks RG4 5BY, United Kingdom.
Tel.: +44 0 7799 033100; E-mail: j.rudge@reading.ac.uk.
[7–10].
ISSN 2542-4823 © 2022 – The authors. Published by IOS Press. This is an Open Access article distributed under the terms
of the Creative Commons Attribution-NonCommercial License (CC BY-NC 4.0).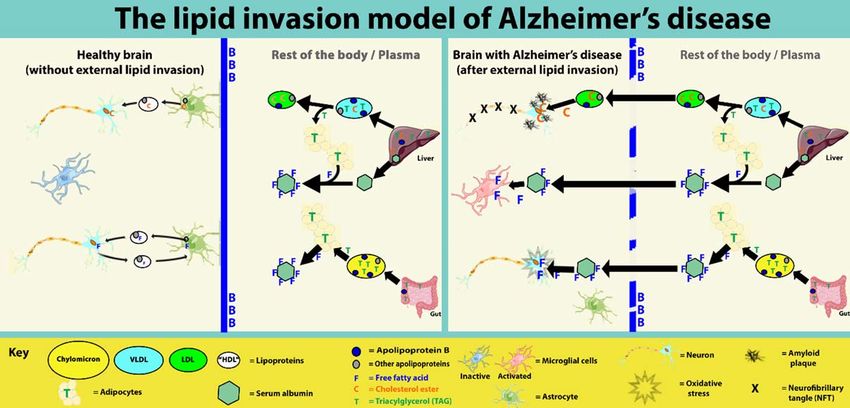
130 J.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease
There have been two major hypotheses so far as to the reverse direction to LRP1, P-glycoprotein,
what drives AD progression: the cholinergic hypoth- and PICALM), is found at significantly higher
esis and the amyloid cascade hypothesis. levels in cerebral endothelial cells in humans
with AD, as compared to those without AD [21].
The cholinergic hypothesis 5. Apolipoprotein E4 (APOE4), a well-established
inherited AD risk factor [22], is associated with
The cholinergic hypothesis, which emerged in the slower efflux of ApoE-A complexes, as com-
1980s, sought to explain the disease in terms of pared with other APOE isoforms, together with
reduced synthesis of acetylcholine within the brain impaired degradation and increased deposition
[11]. However, while substantial evidence points to and aggregation of A itself. This is thought
AD-associated deficits in the cholinergic projection to be a primary reason why A is more prone
system of the brain [11], treatments based on this to forming amyloid plaques in individuals pos-
model do not greatly slow disease progression [11, sessing APOE4, as compared to those with
12]. APOE2 and APOE3 [18, 23].
Any viable model of AD needs to take into account
The amyloid cascade hypothesis the importance of APP, A, and other proteolytic
products of APP, and the core evidence behind the
Since the 1990s the dominant model for explaining amyloid cascade hypothesis. However, the amyloid
AD has been the amyloid cascade hypothesis. This cascade hypothesis does not provide a comprehensive
postulates that amyloid- (A), a proteolytic prod- explanation of AD.
uct of amyloid- protein precursor (APP), is the
fundamental cause of the disease [13]. It is backed Problems with the amyloid cascade hypothesis
by a substantial body of evidence, not least the fact A is certainly a primary cause of neurodegenera-
that A is the main component of amyloid plaques tion in AD in many cases. However, there are several
[13]. aspects of AD which are not well-accounted by the
Key evidence of the important role of APP and amyloid cascade hypothesis. These are discussed in
A in AD includes: the Supplementary Material, and include:
1. Patients with inherited forms of the disease, col- 1. Poor correlation between amyloid plaque dis-
lectively referred to as familial AD (FAD), have tribution and disease progression.
a number of genes related to APP processing 2. Evidence that late-onset forms of AD (LOAD)
that are abnormal, leading to excess production do not always display elevated production of
of A [14]. A.
2. People with Down’s syndrome (DS) possess an 3. Questions about how so many diverse lifestyle
extra copy of chromosome 21, on which APP risk factors for AD (hypertension [24], obe-
resides. It is common for them to develop a form sity [25–27], diabetes [28], smoking [29], stress
of dementia largely indistinguishable from AD [30], sleep deprivation [31], and head injury
[15], if they survive into their 40s. [32]) can all promote AD by increasing A
3. There is substantial evidence, in postmortem levels.
human brains and animal and in vitro studies, 4. Lack of a convincing explanation why aging is
that amyloid plaque formation in AD is associ- the main risk factor for AD [33], specifically
ated with failure of mechanisms that normally why the normal functioning of a small number
clear A from the brain [16], including reduced of proteins should be so vulnerable to the aging
levels of expression and activity of a num- process, and result in a disease that affects such
ber of key proteins. These include low-density a large number of elderly people, while leaving
lipoprotein receptor-related protein-1 (LRP1), earlier age groups largely unaffected.
P-glycoprotein, and phosphatidylinositol bind-
ing clathrin assembly protein (PICALM) Viewing AD as a mechanical/structural disease
[17–20]. Most common diseases of aging involve some form
4. Postmortem studies show that receptor for of structural/mechanical damage, rather than changes
advanced glycation end products (RAGE), a in metabolic pathways, and the gradual accumula-
receptor that transports A into the brain (i.e., in tion of such damage explains why they only tend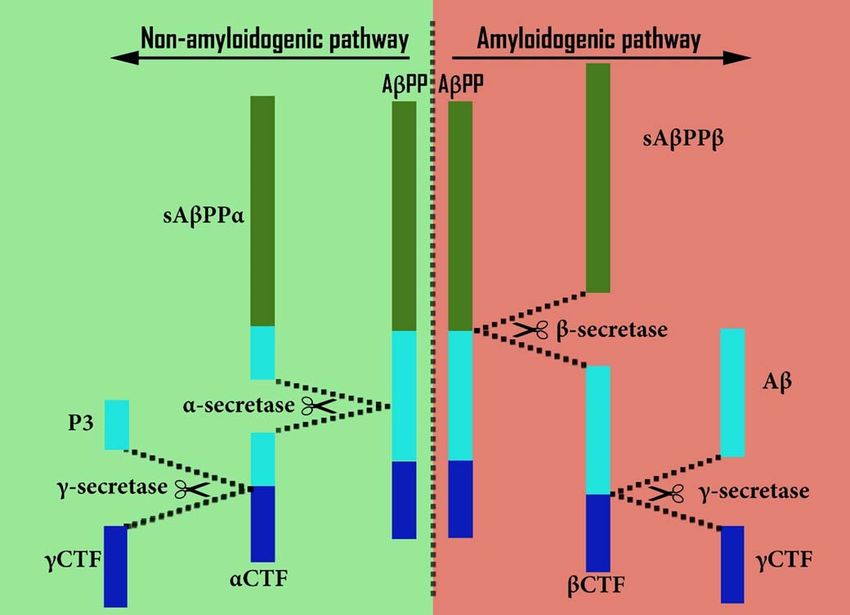
J.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease 131
to emerge in old age. For example: hemorrhagic tight junctions (TJs) and of BBB basement membrane
stroke and cardiovascular disease [34, 35], osteo- integrity [53–57].
porosis [36], cataracts and macular degeneration [37, Finally, the many risk factors for LOAD mentioned
38], hearing loss [39], osteoarthritis [40], and cancer previously, including aging, APOE4, hypertension,
(given that it typically involves progressive damage diabetes, lowered serum levels of sex hormones, dia-
to DNA) [41]. betes, obesity, smoking, chronic sleep deprivation,
The next sections outline how viewing AD also stress, and head injury, are also all associated with
as a structural damage-related disease could unlock vascular damage, including damage to the BBB [26,
an explanation for AD which is compatible with the 27, 58–68].
amyloid hypothesis as well as with all the above-
mentioned AD-associated risk factors. The role of Aβ in BBB disruption
Evidence of blood-brain barrier (BBB) From the above evidence, AD is strongly linked
disruption in AD with disruption of the BBB. So, what causes this
disruption, and how does it associate with A accu-
One extensively researched structural aspect of mulation?
AD is the BBB, and substantial evidence exists to There is, in fact, substantial experimental evi-
demonstrate an association of AD with BBB dam- dence of A itself directly damaging the BBB in
age/disruption [42–47]. humans, rodents, and other animals [46, 69–72].
This includes postmortem and imaging studies of Damage includes alterations in TJ protein distribu-
AD-affected brains [16], showing evidence of infil- tion and expression in brain endothelial cells [46,
tration into the brain of plasma-associated cells and 71–76], increases in matrix metalloproteinase expres-
proteins that should not be there, as well as cerebral sion [74, 77, 78], oxidative stress [76, 79], and
microbleeds, basement membrane thinning,and other possibly apoptosis [80–82] and dysregulation of cal-
direct evidence of neurovascular dysfunction. Simi- cium homoeostasis [46, 80]. Finally, there is further,
larly, many biofluid studies, looking at biomarkers of less direct, evidence that A can damage the BBB,
BBB disruption in live human subjects, have shown for example, in cases of cerebral amyloid angiopathy
a good correlation between such disruption and the (CAA) [74, 76, 77, 81, 83]. This is a disease of small
degree of AD progression. These are discussed in and medium blood vessels of the brain (or wider CNS)
more detail in the Supplementary Material. and meninges, caused (in the majority of cases) by
Some further support (although not conclusive A deposits in the blood vessel walls, and character-
proof) for BBB disruption in AD comes from the fact ized by micro-hemorrhages [84]. CAA shares many
that AD brains commonly stain for Evans Blue, which pathogenetic features with AD (especially in terms of
is normally substantially excluded by the BBB [44, the amyloidogenic pathway), with both diseases fre-
48–50]. Also, in the reverse direction, S100 calcium- quently co-occurring, such that around 80–90% of
binding protein B, normally only found only in the AD cases show some degree of CAA [83–87]. But
central nervous system (CNS) [51], has been shown to critically, it does not require plaque formation.
be present in blood plasma (i.e., outside of the brain) A can be found on either side of the BBB. This
in AD cases [52]. means that it can damage the BBB from both sides.
Further evidence, from a different perspective, of This, in turn, may help to explain evidence suggesting
an association of BBB disruption with AD, relates to that externally sourced A may be a major constituent
chronic traumatic encephalopathy (CTE). This pro- of amyloid plaques found within AD brains, having
gressive degenerative condition commonly affects passed through a compromised BBB [88], as men-
athletes (especially those who have participated in tioned in the Supplementary Material.
contact sports, such as boxing, soccer, rugby and A recent theory, based on studies in mice and
American football) and others with a history of brain humans [88, 89], has proposed that A-related BBB
trauma, especially concussion [53]. CTE typically damage results from external assault by excessive
shows many similarities with AD [53]. These include numbers of A-containing lipoproteins, which might
severe memory deficits, large-scale neuronal loss, be expected from a diet high in saturated fats and
extensive NFTs, and, frequently in advanced cases, cholesterol. Among other evidence, this is based on
diffuse amyloid plaques [53]. Crucially, CTE is char- the fact that A is a regulatory protein involved
acterized by BBB disruption, including disruption of in lipoprotein formation, primarily of triacyl glyc-132 J.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease
eride (TAG)-enriched lipoproteins originating from Evidence of a role for lipids in AD
absorptive enterocytes [90]. Building on this, since A growing body of research supports this associa-
these lipoproteins will also contain high levels of tion between AD and lipids:
A, it is possible that they may contribute to cere-
bral amyloid plaque formation, as well as to BBB 1. As mentioned above, one of the biggest risk fac-
damage [88]. tors for AD, after aging, is having the E4 isoform
The above evidence suggests that A might have of apolipoprotein E (i.e., APOE4) [22], which
a dual role in AD progression, firstly, by damaging is a major component in lipoprotein transport of
the BBB from either side, and secondly, by causing lipids within the body. Similarly, as mentioned
neurodegeneration in the brain, in the form of amy- earlier, one of the other biggest AD risk factors,
loid plaques or as individual molecules or oligomers, A, has been identified as a regulatory com-
including triggering NFTs, as described in the amy- ponent of chylomicrons, a class of lipoprotein
loid hypothesis. which serves to transport TAGs and other lipids
But, as explained above, BBB disruption may from the intestine to the liver [93, 94]. Thus,
result from any one or more of the AD-associated risk two of the most important risk factors for AD
factors, allowing A into the brain to cause neurode- (after aging) both have important roles in lipid
generation. This includes A, alone or with others of transport.
these risk factors, but does not require it. 2. Genes for another apolipoprotein, apolipopro-
tein J (also known as clusterin), and for the
ABCA7 (ATP-binding cassette sub-family A
The lipid factor identified by Alois Alzheimer member 7) protein, involved in lipid homoeosta-
sis, have also been identified as susceptibility
A damaged BBB will clearly not just enable A loci for AD [95–97].
to enter the brain. Many other molecules and larger 3. Elevated serum levels of cholesterol, triglyc-
structures will also be allowed through. This could erides, and apolipoprotein B (ApoB) have all
explain an additional feature of AD, which was iden- been associated with higher risk of getting AD
tified by Alois Alzheimer in his original research. [98–100]. So, taken together, lipids, lipid trans-
In describing the first diagnosed case of AD, port, and homoeostasis all play an important
Alzheimer makes frequent reference to “adipose sac- role in AD progression.
cules”, “lipoid granules”, and similar lipid-based 4. There is also substantial experimental data
aggregations within both glial and neuronal cells, pointing to the direct involvement of choles-
as well as to amyloid plaques, NFTs, and gen- terol in A formation [101, 102], not least
eral brain degeneration [1, 91]. Lipids are a class the high levels of cholesterol and other lipids
of biomolecules that do not dissolve (or not eas- found within amyloid plaques [103, 104]. Also,
ily) in water. They include fatty acids, glycerolipids, NFTs occur extensively in Niemann Pick type C
glycerophospholipids, and sphingolipids, as well as (NPC), another disease associated with demen-
cholesterol and other sterols. (See the Lipid Maps tia, which is caused by internal cholesterol
database for a comprehensive list [92]). Descrip- accumulation within cells [105]. Substantially
tions of these lipid aggregations appear almost as elevated levels of cholesterol are found in NFT-
frequently in Alzheimer’s writings as do the refer- bearing neurons in both NPC and AD [106].
ences to what have become known as amyloid plaques 5. Finally, brains of those who have died from,
and NFTs. or with, AD contain unexpectedly high lev-
Likewise, colleagues of Alzheimer, describing this els of albumin [107–109] (which transports
and other AD cases, refer to “abundant deposits of free fatty acids (FFAs) within the blood-
fatty substances and pigments”, and “major accumu- stream) and ApoB (another major component of
lation of lipoid products in the ganglion cells, glia lipoprotein-mediated lipid transport). ApoB is
and vasculature” [91]. found, along with A, within amyloid plaques,
It is clear from Alzheimer’s writings that he and also in NFTs [110–112].
regarded “this degree of lipid degeneration”, as he
described it, to be as much a hallmark of the disease Substantial levels of these lipid transport proteins,
we now call AD as the associated plaques and NFTs albumin and ApoB, should not be found within the
[91]. brain compartment in normal circumstances, as theyJ.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease 133
are both generally, but not conclusively, believed albumin [114]. Within the brain compartment, sep-
to only be expressed outside of it, and should be arated from its external blood supply by the BBB,
excluded from entering it by the BBB [113–119]. lipoproteins tend to be relatively small and lipid-poor
This suggests that the “lipid degeneration” that [117], and there is little evidence of non-lipoprotein
Alois Alzheimer referred to may have its origins out- FFA transport [126].
side the brain, and results from some kind of external The main reason for these differences in lipid trans-
lipid incursion through damaged portions of the BBB. port on each side of the BBB lies in differences
in availability of key transport proteins—principally,
The unexpected role of cholesterol and FFAs apolipoproteins, which determine the size and lipid
content of lipoproteins, and serum albumin, the main
So, which of these invading lipids are most likely to non-lipoprotein FFA transporter. It is this differ-
cause AD? For several reasons, cholesterol and FFAs ence which underlies the lipid invasion model, as
are the most likely candidates. This is partly because explained in the next section.
of their large numbers as a proportion of readily avail-
able plasma lipids [120], but mainly because their The lipid invasion model
presence in excess numbers within the brain could
explain a number of brain-associated anomalies seen The differing lipid transport systems explain the
in AD, including plaques, NFTs, lipid accumulation, apparent paradox, referred to above, whereby exter-
neuroinflammation, and bioenergetic changes. nal lipids, especially FFAs and cholesterol-rich
At first sight this second assertion makes little lipoproteins, which are so necessary for the nor-
sense, because cholesterol and FFAs are essential to mal functioning and survival of brain cells, may
the survival of the brain, and pose no danger, in nor- start to pose a threat to their normal functioning and
mal quantities, to it. So how does damage to the BBB survival, if they break through the BBB. These exter-
turn such lipids into a threat? To explain this, it is nal lipids are (for the most part) transported in a
helpful to understand the important role of BBB in different way to what is normally seen within the
respect of lipids. brain compartment [114, 117, 118, 122, 127], and
their flow is often much less tightly controlled [118,
The BBB: a barrier between two different lipid 126, 128], so brain cells exposed to them become
systems vulnerable. Neurons and inflammatory microglial
cells, especially, become overloaded and overstim-
It would appear from its unique architecture that ulated. This is explained in more detail in later
the BBB’s main purpose is to exclude certain cells sections.
and molecules from the brain compartment (meaning Over time, this lipid invasion will result in various
the brain parenchyma and interstitial fluids) and the forms of lipid-associated brain pathology. In the case
wider CNS. This architecture is described in detail in of invading FFAs this will take three main forms:
the Supplementary Material. 1) changes in brain bioenergetics, oxidative stress,
Because of its architecture, the BBB is known to lipid peroxidation, and mitochondrial damage result-
substantially prevent lipids passing through it, cer- ing from excess FFA accumulation within neurons;
tainly those that remain bound to, or within, their 2) neuroinflammation; 3) anterograde amnesia (AA)
normal transport partners [121–124]. resulting from tonic inhibition and disruption of neu-
In addition, there are different lipid transport sys- rogenesis. These are all characteristics that have been
tems either side of the BBB, as will be explained associated with AD [129–131].
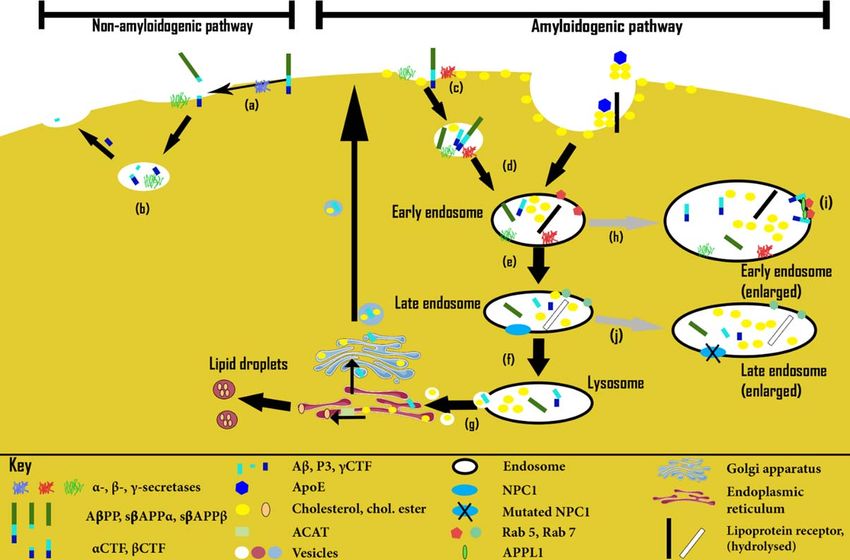
in much more detail below, with major differences in Other characteristics of AD, such as changes in
the types of lipoprotein transporters employed. These endosomal-lysosomal pathway disruption, cerebral
assemblies transport cholesterol, fatty acids (FAs), amyloidosis and NFT formation can also be explained
and other lipid classes, all of them water-insoluble, by lipid influx in the form of external lipopro-
within blood plasma and other extracellular watery teins. With the exception of high-density lipoprotein
fluids. (HDL), these plasma lipoproteins are typically much
In the blood plasma compartment, such lipopro- larger than CNS lipoproteins, and therefore much
teins tend to be relatively large and contain large richer in cholesterol, which has also been linked with
quantities of lipids [125], and there is also abundant AD [102, 132, 133], particularly in connection with
non-lipoprotein transport of FFAs, mostly bound to amyloidosis and NFTs.134 J.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease
The lipid invasion model argues that failure of the neuroinflammation, tonic inhibition, and neurode-
BBB allows lipids in the plasma compartment to enter generation. However, unlike AD, ARBD does not
the brain compartment and cause various forms of involve exposure of the brain to external FAs and,
damage, including AD, because these lipids are trans- even more importantly, cholesterol-rich lipoproteins.
ported, stored, and regulated in very different ways This explains why the amyloid plaques, NFTs, and
to resident lipids. endosomal-lysosomal abnormalities seen in AD are
not seen in ARBD [139], while some other features
How the lipid invasion model fits in with other of AD, including neuroinflammation and (somewhat
lipid- and BBB-based explanations of AD limited) neurodegeneration and inhibition of neuro-
genesis, are seen in ARBD [140–144].
Numerous articles have shown an association There is also extensive evidence that the detrimen-
between BBB dysfunction and AD, many of them tal effects observed in the brain from chronic alcohol
suggesting some form of causal link [43, 134, 135]. exposure are the result not only of neurodegeneration
Likewise, many articles have shown an association resulting from neuroinflammation, but also (judged
between lipids and AD [91, 136, 137]. A few of these from what is seen in rodent models) of reduced lev-
have suggested that some form of lipid dysfunction els of neurogenesis [140, 141, 143, 145], similar to
may have a role in AD progression [136, 137]. But what is seen in AD.
it appears that only one group of researchers (from These similarities and differences yield important
Curtin University of Technology, Perth, Australia, insights into the etiology of AD, which reinforce
subsequently referred to as “the Curtin explanation”), the model, particularly increases in neuroinflamma-
have sought to explain AD in a way that can be said tion, neurogenetic inhibition, and AA, all mediated
to link these two aspects together [138]. This has by FFAs. A more detailed discussion of this evidence
already been referred to earlier, and links dietary fats appears in the Supplementary Material.
(specifically saturated FAs and cholesterol) with BBB Following the above outline of the lipid invasion
dysfunction and amyloid plaque formation, providing model, the next section provides a more detailed
a compelling explanation for the presence of ApoB explanation and justification.
within these plaques [93, 94, 111, 138].
However, this explanation is largely limited to TECHNICAL EVIDENCE AND MORE
plaque formation and does not include a more gen- DETAILED EXPLANATION OF THE LIPID
eral role for external lipids in AD progression, in INVASION MODEL
terms of cerebral amyloidosis, NFT formation, AA,
and the other AD-associated pathologies mentioned This section first looks at differences in lipid
earlier. Therefore, by explaining the origins of AD in metabolism between the brain and plasma compart-
terms both of BBB disruption and subsequent exter- ments of the body and the importance of this to
nal lipid invasion, and in showing how all aspects of the model. Then the many ways in which the BBB
disease progression are primarily driven by such lipid becomes damaged will be explained. Finally, the con-
incursions, the lipid invasion model provides a new sequences for the brain compartment of the lipid
approach to understanding AD. incursions that result from such BBB disruption will
be examined. This includes changes to brain ener-
Similarities between AD and alcohol-associated getics, neuroinflammation, neurodegeneration, AA,
brain damage endosomal-lysosomal disorder, lipid accumulations,
amyloid plaques, and NFTs.
An additional reason for identifying BBB dam-
age and subsequent lipid influx as the driver of AD Differences between lipid metabolism on either
is the similarity between the overall structural pat- side of the BBB
tern of neurodegeneration seen in AD and that seen
in alcohol-related brain damage (ARBD), resulting There are many differences in lipid metabolism
from chronic exposure of the brain to ethanol. either side of the BBB. This is most apparent in the
Ethanol passes relatively easily through the BBB. case of FAs and cholesterol. (Here, FAs denote all
Once in the brain compartment, as will be explained fatty acids, including esterified FAs such as TAGs, as
in later sections, it will have some of the same well as FFAs, which are not esterified.) Because these
overall effects as overexposure to FFAs, namely differences in metabolism and transport are so criticalJ.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease 135
to the lipid invasion model, accounting for many of At first sight, this would appear to invalidate the
the pathological hallmarks observed in AD, they are claim by the lipid invasion model that invading FFAs
explained in detail below. from the plasma compartment, entering the brain
through a disrupted BBB, cause many of the patholo-
gies seen in AD. Why are such pathologies not seen
Fatty acid metabolism even when the BBB is not disrupted? This question
For efficient transport within plasma, the vast is addressed in the next section.
majority of FAs, being highly hydrophobic, must FAs and the brain. Despite this evidence of external
travel within lipoproteins, or must be bound to the plasma-originating FFAs entering the brain compart-
protein serum albumin, to improve solubility [114, ment, it is clear that, almost uniquely among organs,
127]. the brain in humans and other animals does not rely on
Immediately after eating, dietary FAs are bound FAs (certainly in albumin-bound FFA form) as a pri-
to glycerol as TAGs and then transported within the mary energy source [156, 160]. This is despite the fact
class of lipoproteins known as chylomicrons. These that the brain has a high energy requirement, and other
chylomicrons constitute a major proportion of the organs with high energy needs, such as the heart and
plasma transport pool [127, 146]. At the same time, kidney, preferentially oxidize FAs [156, 161], reflect-
high blood glucose levels associated with satiety lead ing the wide availability of FFAs in the bloodstream,
to hepatic neogenesis of FFAs and glycerol, with and the fact that they provide about twice the energy
the resulting TAGs being transported in the blood content of glucose and similar sugars [162]. Instead,
within very low-density lipoproteins (VLDLs) [127, during the fasting state when glucose availability is
146]. During subsequent plasma transport most of the low, the liver will typically transform such plasma
TAGs within chylomicrons and VLDLs are taken up FFAs into much smaller ketone bodies, which, hav-
by tissues, principally adipocytes and muscle cells ing been transported through the BBB, are used in
[147, 148]. preference to FFAs as an energy source by the brain
The chylomicrons and VLDLs are relatively large [163–165].
(typically within a range of 100–1000 nm and The most likely reason why the brain does not
30–80 nm, respectively [127, 146]) and lipid-rich by use whole FFAs extensively for its energy needs
virtue of their association with ApoB isoforms. Such is that ATP generation from FFAs requires sub-
lipoprotein-mediated FA transport appears to allow stantially more oxygen than from alternative energy
only very restricted access to the postnatal brain substrates such as glucose, lactate, butyrate, and
compartment across the BBB. This is partly because ketone bodies [156]. As a consequence, such FFA
ApoB is (according to current orthodoxy) synthe- usage would increase the risk of brain hypoxia,
sized only in the liver and in enterocytes, but not as well as generating higher levels of oxidative
in the CNS [115, 127]. But more importantly, it is stress, thus proving toxic to neurons [128, 156,
because of the architecture of the BBB, mentioned 162, 166]. Another possible reason is that the
earlier and detailed in the Supplementary Material rate of ATP generation from FFAs is slower than
[117, 149–151]. This substantially excludes larger from the other mentioned energy substrates, mean-
lipoproteins, with only much smaller, less lipid-rich, ing that FFAs may not be able to yield ATP fast
HDL appearing to cross the BBB in any quantity enough (or flexibly enough) for rapidly firing neu-
[118]. rons, especially under conditions of sustained activity
During the fasting state, adipocytes release stored [156].
FFAs directly back into the bloodstream, with the What happens to those FFAs that make it across
majority being subsequently bound to serum albu- the BBB from the plasma compartment into the brain
min [114, 127]. Because serum albumin is created compartment? As explained in detail in the Supple-
almost exclusively in the liver [114, 152, 153] and mentary Material, the evidence strongly suggests that
cannot pass readily through the BBB [113, 154, 155], the vast majority will be taken up by astrocytes.
it has until recently been assumed that albumin-bound Typically, these will be sequestrated within lipid
FFAs must also be largely excluded from the brain, droplets inside the host astrocyte, with most being
in the same way as external lipoprotein-associated converted into ketone bodies or the much shorter
FAs. More recent findings suggest that more FFAs FFA butyrate, and used as fuel, either by the host
are taken up by the brain compartment through the astrocyte or by local neurons and other neighboring
BBB than originally envisaged [156–159]. brain cells [128]. Others of these FFAs will be trans-136 J.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease ported onwards in esterified form (mainly as TAGs or Cholesterol metabolism either side of the BBB phospholipids) within lipoproteins, for use by other Numerous studies in humans and other higher neighboring cells. Certainly, given that albumin trans- animals have shown that, except in very early port is no longer available to these extravasated FFAs, fetal development, almost all cholesterol in the and given the absence of any obvious alternatives to CNS is of local origin, relying on endogenous de albumin in the CNS [156, 167–169], some form of novo biosynthesis rather than external, lipoprotein- lipoprotein-mediated transport seems the most likely mediated provision [117, 122, 150, 151]. This appears alternative. to be true for a wide range of animals, including birds However, there are important differences between and mammals, with much of cholesterol production lipoprotein transport in the CNS, and lipoprotein for neuronal consumption being delegated to local transport in the plasma compartment. These differ- astrocytes [117, 122, 174]. ences have critical implications if the BBB becomes Moreover, cholesterol turnover in the mature CNS disrupted and are explained in more detail in the next is very low, typically only around 5% of the turnover section. seen in the rest of the body [122, 150, 151]. A major Lipoprotein transport of lipids inside and outside reason for this is that a large proportion of such the brain/CNS. In contrast to what is seen in plasma, cholesterol remains locked up within the insulating the principal apolipoproteins expressed in the CNS myelin sheath that permanently encases the axons of (including Apo E, D, and J [117, 170]) associate into many neurons, particularly within the white matter lipoprotein particles that are relatively small (typi- of the brain [124]. Much of this myelination takes cally less than 20 nm) and contain modest amounts place early in organismal development [175]. Any of lipids [127, 168, 171]. Such CNS lipoprotein parti- remaining freely circulating cholesterol within the cles tend to resemble HDL [117, 146, 168, 171] much brain is kept at low levels by various mechanisms, more than the larger ApoB-associated lipoproteins including removal across the BBB in the form of that predominate outside the CNS. 24S-hydroxycholesterol [122, 176]. Furthermore, astrocytes are known to be a principal In the rest of the body (and thus on the other source of many of these CNS-originating apolipopro- side of the BBB), a large proportion of cholesterol teins, particularly Apo E and J [117, 171, 172], and is either of dietary origin or else the result of neo- lipoproteins have been isolated from the conditioned genesis in the liver [127, 146]. From there much of medium of astrocytic cultures [170]. They can then be it is transported in the same large, lipid-rich, ApoB- assembled into HDL-like (or even smaller) lipopro- containing lipoproteins (i.e., chylomicrons, VLDLs, teins within the astrocyte body, and secreted into and low-density lipoproteins (LDLs)) that also trans- the interstitial fluid of the brain compartment, for port dietary and liver-derived FAs [115, 127, 146], onward transport and uptake by neurons and glial albeit chylomicrons typically contain relatively little cells [173]. cholesterol. For this reason, as well as the properties From this description, it would appear that FA of the BBB itself (as explained in the Supplemen- transport and metabolism in the CNS is very different tary Material), much cholesterol of non-CNS origin from that seen in the rest of the body. In particular, is unable to cross the BBB [117, 150, 151, 177]. there appears to be little, if any, non-lipoprotein FA By contrast, within the brain compartment and transport in the CNS and, on average, CNS lipopro- wider CNS, cholesterol is transported within the teins are much smaller than their plasma equivalents. same HDL-like lipoproteins. As stated, such lipopro- In many respects, FA transport seems more tightly teins tend to be small, compared to many of their controlled in the brain compartment than outside it plasma counterparts, typically containing only mod- [118, 126, 128]. Certainly, it is hard to see how such est amounts of cholesterol and other lipids [127]. differences could be maintained without a BBB that is substantially intact. Overall differences in lipid transport either side Major differences either side of the BBB are also of the BBB seen in cholesterol transport and regulation, as out- Overall, it is clear that, from birth onwards, in lined in the next section. Later sections will explain humans and other animals [178], the BBB separates the implications such differences in lipid organization two compartments, the brain/CNS and external sys- will have, as predicted by the lipid invasion model, temic/plasma compartments, with very different lipid when the BBB becomes disrupted, and how this all systems [122, 179]. Compared to the rest of the body, relates to AD. the mature CNS compartment is distinguished by
J.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease 137
a much lower circulation of lipids, with apparently metallopeptidases (MMPs) and basement membrane
restricted external lipid supplementation and a set of (BM) proteins drive changes in BM thickness, among
lipoproteins that are noticeably smaller and less lipid- other BBB-associated alterations [59, 74, 78, 184,
rich. Much of this difference can be accounted for by 186, 189, 205–207]. In many cases more than one
the BBB (which substantially prevents lipoproteins such mechanism may be involved, some of which
crossing from one compartment into another), and by may interact. For instance, APOE4-associated BBB
the fact that ApoB and albumin (or their functional breakdown has been shown to be driven by activation
equivalents) are not (according to current orthodoxy) of a pro-inflammatory pathway in pericytes, acting
produced in the brain compartment. on MMP9, which cleave TJ, as well as BM proteins
Given that this distinction appears to have first [182, 195, 208]. Similarly, some AD risk factors such
emerged comparatively early in vertebrate evolution as smoking and sleep deprivation have been shown
[180, 181], it seems plausible that serious disruption to damage the BBB by causing inflammation, which
to the BBB will have lipid-related consequences. This in turn causes reductions in expression of TJ proteins
can be inferred from the fact that the mature brain or redistribution of such proteins around endothelial
compartment has evolved for so long to function in an cells [191, 192, 194, 209].
environment low in circulating lipids compared with However, this is an area of intensive research, and
the rest of the body. And, given the relative volumes of many details remain to be determined.
the two compartments, it seems likely the brain com-
partment will be the most vulnerable to lipid incursion BBB disruption as a biomarker for AD
if no longer substantially isolated from the rest of the Having outlined the various mechanisms by which
body by the BBB. the BBB may be disrupted by most risk factors for
Above the evidence for BBB disruption in AD AD, it is important to clarify further why such BBB
(from postmortem, biofluid and imaging studies, and disruption is relevant to AD. This is because, as well
CTE) was provided. However, this still leaves the as being directly associated with FAD and LOAD
question of how the disruption occurs, and how this (as inferred from postmortem, biofluid and imaging
relates to the many identified AD risk factors. This is studies, and from CTE, as outlined earlier), BBB
explained in the next section. breakdown has been shown to be an early biomarker
of human cognitive decline, irrespective of A reac-
The causes of BBB disruption in the lipid tivity and APOE status [210]. And there is plenty of
invasion model reason to believe this is not a coincidence. Recent
studies suggest that, perhaps because of zonal differ-
Understanding how the BBB becomes disrupted in ences in BBB composition and other properties (as
AD is central to the lipid invasion model. It largely shown in mice and postmortem human brains [211,
explains why AD has all the risk factors it has, and 212]), the aging brain is especially prone to BBB
why the disease is so much more common in old age. damage in the hippocampal and wider medial tempo-
As stated earlier, almost all the major identified ral lobe regions. These regions are, of course, known
risk factors for AD (aging, A, APOE4, head injury, to be particularly associated with memory formation
hypertension, diabetes, obesity, smoking, lowered and cognition. Such zonal differences of the BBB,
sex hormones, sleep deprivation, and stress) have may reflect differences in the properties of pericytes
been shown to also be causally associated with the within the BBB [63, 210]. Whatever the reason, it
structural and functional disruption of the BBB. How- suggests that these brain regions will be subject to
ever, each one of the mentioned risk factors causes the greater levels of lipid invasion than other, less affected
BBB disruption via different mechanisms. regions. Further research is needed into such zonal
These mechanisms are detailed in the Supplemen- differences to establish a more complete, and more
tary Material, and include reduced junctional strength quantitative picture.
between BBB endothelial cells (especially TJs) [27,
45, 65, 76, 82, 182–190], inflammation and oxida- Aging, AD, and BBB disruption
tive stress [191–194], lowered pericyte numbers and Collectively, these facts provide a simple rea-
activity levels [135, 195–201], impaired astrocyte son, according to the model, why LOAD incidence
activity [189, 202, 203], and chronic dysregulated is closely correlated with age. Not only is the
neogenesis [82, 185, 189, 204]. In addition, alter- wear and tear of aging itself directly associated
ations in expression levels and activity of matrix with loss of BBB integrity, but so are most of the138 J.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease
risk factors—including diabetes/obesity, hyperten- BBB disruption (as described in the Supplementary
sion, smoking, stress, sleep deprivation, and declining Material).
sex hormones—whose cumulative effects on the In the case of LOAD, APOE4 may be viewed as just
BBB may reasonably be expected to build up with one of a number of AD risk factors that contribute to
age for those affected. BBB dysfunction, as outlined earlier in this section.
Similarly, the above account suggests a plausible But it could also be that the same mechanisms by
explanation for why inherited forms of AD (i.e., FAD) which APOE4 is believed to aggravate A-mediated
occur earlier but much less commonly than non- BBB damage in FAD (as outlined in the previous
inherited forms (i.e., LOAD). This is because FAD is paragraph), also act on physiologically normal lev-
the product of excess A production, resulting from els of A to cause similar BBB damage, albeit at a
rare genetic mutations, but commencing relatively lower rate than seen in FAD. Taken together with the
early in life [213]. By contrast, LOAD is the prod- BBB-disrupting mechanisms that APOE4 is associ-
uct of many factors, the majority of whose effects ated with (as detailed in the Supplementary Material),
can be expected to result in equivalent cumulative this suggests that APOE4 may be much more dam-
levels of damage only later in life, with a mean age aging to the BBB than other LOAD-associated risk
of onset around 20 years later than that of inherited factors. Certainly, according to the model, this would
forms [213]. seem to provide an obvious reason, why homozy-
gous carriers of APOE4 have a two- to five-increased
Wider implications of the different mechanisms risk of developing LOAD, compared to non-APOE4
of BBB disruption in FAD and LOAD carriers, and with a substantially earlier age of onset
In both FAD and LOAD, the resulting AD- [22].
associated neuropathology is explained by the model
in terms of the resulting invasion of external lipids Curtin explanation of BBB disruption in AD
through the disrupted BBB. Except that in FAD, As mentioned previously, there is possibly a further
earlier A-driven BBB disruption means that this means by which high levels of A may contribute to
invasion occurs much sooner than in LOAD, and, BBB damage, but in a different way to that described
according to the model, it is this earlier external above; one that is relevant to both FAD and LOAD,
lipid invasion, and not so much the direct actions and yet wholly consistent with the lipid invasion
of A on the brain, that primarily explain the ear- model. This is when A-mediated disruption of the
lier AD onset and progression typically seen in BBB originates from outside the brain, the A being
FAD. As mentioned above, it is these invading lipids transported within triglyceride-rich lipoproteins, as
that primarily drive the changes to brain energetics, explained in detail in the Supplementary Material.
neuroinflammation, neurodegeneration, AA, amy- However, such disruption is not a requirement of the
loid plaques, and NFTs seen in AD, rather than raised model.
A levels. Whatever the cause of BBB disruption (includ-
ing A-mediated damage), the model argues that the
The role of APOE4 in BBB disruption and in AD consequences for the brain, resulting from external
According to the model, APOE4 can be expected lipid invasion, will be the same, thus explaining why
to have a potential role in both FAD and LOAD. In so many disparate risk factors (aging, A, APOE4,
the case of FAD, it is known to reduce A clearance hypertension, diabetes, lowered sex hormone levels,
from the brain [18, 23], to impair A degradation obesity, smoking, stress, sleep deprivation, and head
[214], and to increase A deposition and aggrega- injury) are associated with the same disease, i.e., AD.
tion [215]. Such increased deposition is evident not The next three main sections explain how, accord-
just within amyloid plaques but also within cerebral ing to the model, this external lipid invasion of the
blood vessels [214, 216], where postmortem studies brain results in the collection of neuropathologies that
in humans and animals show that it is associated with characterize AD.
increased prevalence of CAA, BBB dysfunction, and
other consequences leading to impaired blood vessel AD-relevant consequences of FFA influx to the
integrity [214, 216–220]. Therefore, in FAD, APOE4 brain
contributes to BBB disruption both indirectly, by
promoting A-mediated disruption, and directly, via This section and the next principally focus on
other mechanisms associated with APOE4-mediated the consequences of external FFA influx in termsJ.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease 139
of changes to brain energetics, increased neuroin- hypometabolism, all these above-mentioned changes
flammation, neurodegeneration, AA, and inhibition are seen in AD [166, 230–233].
of neurogenesis. Then the effects of exposure Finally, recent evidence of non-mitochondrial
to excessive levels of cholesterol within certain oxidative phosphorylation within the myelin sheath,
externally-derived lipoproteins is explained. involving subunits of electron transport chain com-
plexes and of F1F0-ATP synthase [234], suggests that
FFA-mediated changes to brain bioenergetics this sheath may also be highly vulnerable to oxidative
and oxidative stress stress, as a result of exposure of these electron trans-
External fatty acid ingress into the brain will sub- port chain elements to intact FFAs [235], i.e., in much
stantially alter local brain bioenergetics, which are the same way as described for neuronal mitochondria.
normally characterized by glucose/lactate-dominated White matter loss is, of course, widely associated with
energy metabolism [221, 222]. In its place, accord- AD, its occurrence coinciding with, and often pre-
ing to the model, such bioenergetics will be pushed ceding, the appearance of other AD markers [236].
in the direction of ketone metabolism, a shift that It may be that this exposure to invading FFAs pro-
has been widely reported in AD [223, 224]. How- vides a primary explanation for such progressive local
ever, this differs from other accounts of glucose demyelination in AD.
hypometabolism in AD. These tend to focus on Having shown how, according to the model, exter-
age-related faulty mitochondrial bioenergetics, accu- nal FFA invasion disrupts normal brain bioenergetics
mulation of A within mitochondria coupled with in a similar ketogenetic direction as seen in AD, the
oxidative stress, and other such factors [224], all driv- next section shows how external FFAs can also trigger
ing a shift from glucose-driven bioenergetics towards the neuroinflammation (defined as inflammation of
a ketogenic/-oxidation pathway. According to the the brain and other nervous tissue) seen in the disease.
lipid invasion model it is, in many ways, the other way
round. FFA-mediated neuroinflammation
The underlying mechanism behind this bioener- In order to appreciate how FFAs might cause neu-
getic shift, and its implications, is explained in more roinflammation in AD (with accompanying damage
detail in the Supplementary Material. Put simply, it to the brain), as predicted by the lipid invasion model,
is argued that invading external FFAs will mainly be it is useful to understand firstly how such neuroin-
taken up by astrocytes, most being converted into flammation is driven by exposure to excess ethanol
ketone bodies and used to meet neuronal energy needs in ARDB.
rather than those of the host astrocyte. The resulting Extensive research (principally in rodents, but
increase in ketone availability will tend to inhibit gly- echoed by findings in plasma and in postmortem
colysis and drive a local bioenergetic shift towards brains of human alcoholics) has established that
ketone metabolism. neuroinflammation is an important cause of ethanol-
Nevertheless, some of the invading FFAs in inter- induced neurodegeneration [145, 237–239], and that
stitial fluids will be taken up by neurons, which microglia are central agents of such inflammation
have very limited capacities for -oxidation or lipid [145, 237, 240, 241]. This central role is perhaps
sequestration [128, 156, 225, 226], leaving neu- unsurprising, given that the “immune-privileged” sta-
ronal mitochondria directly exposed to these FFAs. tus conferred on the brain compartment by the BBB
Such FFA exposure has been shown to have vari- leaves microglia as the primary immune cell [242,
ous negative consequences for affected mitochondria, 243], a role not seen as a rule in macrophages in the
including interfering with electron transport, col- rest of the body. Their ability to perform this role
lapsing the electrochemical proton gradient and seems to depend in large part on being abnormally
uncoupling oxidative phosphorylation [156, 227, sensitive to a wide range of ligands [243–245], and
228]. As well as leading to a reduction in the rate this, in turn, helps to explain why chronic ethanol,
of ATP production and in the calcium ion retention largely unobstructed by the BBB, causes such exten-
capacity of these mitochondria [156, 228], these FFA- sive inflammatory damage to the brain compartment
associated deficits will also lead to increased reactive over time [246]. Additionally, the mechanism through
oxygen species production, lipid peroxidation, and which this occurs suggests that FFAs, provided they
oxidative stress, opening of the mitochondrial per- could pass through the BBB in quantity, would have
meability transition pore and release of pro-apoptotic similar inflammatory effects, since both are known to
factors [156, 227–229]. Together with glucose powerfully activate the same critical receptor.140 J.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease
Ethanol activation of microglia [246] is accom- the very specific areas of atrophy seen in both diseases
panied by upregulation of the transcription factor and the failure to recover, particularly in the case of
NF-κB [247, 248] and other macromolecules known AD. Again, the ethanol-induced mechanisms thought
to be involved in inflammation and in the immune to underlie such inhibition in ARBD will most likely
response. The evidence (at least in mice) suggests also be triggered by exposure to FFAs—another key
that toll-like receptors, particularly toll-like receptor prediction of the lipid invasion model of AD. The
4 (TLR4, a receptor that binds bacterial lipopolysac- sections below explain this in much greater detail.
charide), are central to such activation and the
FFA-mediated neurodegeneration and AA
subsequent neuroinflammation [248, 249].
In the previous section, it was shown how ethanol
If TLR4 is central to ethanol-induced neuroin-
and FFAs induce neuroinflammation by similar
flammation, then there seems every reason to think
mechanisms. The same can also be said of neurode-
that FFAs entering the brain compartment would
generation, with many of the insights gained about
have similar neuroinflammatory effects. Saturated
ethanol-induced neurodegeneration also being appli-
(but not, apparently, unsaturated) FAs are known to
cable to AD.
activate TLR4 in macrophages, leading, in turn, to
Much of ethanol-mediated neurodegeneration has
activation of NF-κB and the other pro-inflammatory
been linked (at least in rats) to inhibition of neuroge-
molecules just mentioned [250, 251]. And TLR4 acti-
nesis [142, 239], with many studies suggesting that
vation in adipocytes by saturated FAs (and perhaps
neurogenetic deficits are almost as important a fac-
by some unsaturated FAs) is an essential step in lipid-
tor as neuroinflammation in such degeneration [239].
induced type 2 diabetes mellitus [250, 252], which
Here too, TLR4, and other ethanol-sensitive toll-like
is now thought to be substantially inflammatory in
receptors, are likely to have an important inhibitory
nature [252–254]. In support of this, knockdown
role [264, 265], diminishing proliferation of adult
or ablation of TLR4 has been shown to inhibit
neuronal progenitor cells and restricting neuronal dif-
both FFA-induced and ethanol-induced inflamma-
ferentiation. Such inhibition would obviously be most
tion [248, 250–252], as well as protecting against
apparent in the main adult neurogenic niches, i.e.,
FA-induced diabetes.
the subgranular and subventricular zones (SGZ and
Given how responsive microglia are to patholog-
SVZ), which provide new neurons and glial cells to
ical stimuli [255–258], one could reasonably expect
(respectively) the hippocampus and the olfactory bulb
activation by both ethanol and FFAs to result in
[266]. This could explain deficiencies in learning and
far more vigorous inflammatory activity than seen
olfaction common to both AD and ARBD [267–274],
in other parts of the body. And, while the relative
given that such receptors should also be sensitive to
affinities of ethanol and FFAs for TLR4 have yet
FFAs, as explained in the previous section.
to be determined, the fact that saturated fatty acyl
In addition, current evidence indicates that the
groups are known (at least from animal studies) to
overall level of neurodegeneration in both cases is
be crucial to TLR4 recognition of lipopolysaccharide
determined almost as much by the relentlessness of
(TLR4’s principal pathogenic ligand) [259] suggests
the ethanol assault as by the concentrations involved
that FFAs should have a substantially higher affin-
[140, 142, 239]. Thus, one can reasonably infer that
ity than ethanol for TLR4. Thus, the relatively low
constant exposure of the brain compartment to plasma
levels of FFAs seen in human plasma (generally
levels of FFAs is likely to overwhelm the brain’s
agreed to fall within an average range of 0.3–0.6
capacity to recover, especially in the elderly. Such
mM [260, 261]) should be sufficient to generate a
a conclusion is further supported by evidence that
steady level of neuroinflammation, following major
inhibition of neurogenesis, by both ethanol and FFAs,
BBB damage, especially if they are accompanied by
does not need to rely on the TLR4 receptor alone, and
pathogen-associated lipopolysaccharide, as seen in
may, in fact, depend more on GABAergic effects.
ethanol-induced liver injury [262]. So it may be FFAs,
The relevance of this to the lipid invasion model is
rather than TLR4 stimulation by amyloid [263], that
explained in the next section.
are the primary driver of microglial-based neuroin-
flammation in LOAD. GABAergic effects
Whatever the case, oxidative stress and neuroin-
flammation are not the only drivers of neurodegenera- Recent research (in postmortem rodent and human
tion, either in ARBD or AD. Another important factor brains) has indicated a possible role for the inhibitory
is inhibition of neurogenesis, which can account for neurotransmitter gamma-aminobutyric acid (GABA)J.D. Rudge / Lipid Invasion Model of Alzheimer’s Disease 141
in the development of AD [275–277], with a num- the fact that the vast majority of anesthetic agents
ber of possible mechanisms being suggested. One are known to cause AA, at concentrations well
such mechanism, GABA-induced tonic inhibition below those needed for clinical anesthesia [287, 293,
within the hippocampus, provides an obvious expla- 294]. Such low-level anesthesia-induced AA is now
nation of why AD is characteristically associated with known to involve extrasynaptic GABAARs [293,
AA. However, the proposed source of this excess 294], whose subunit composition (including either
GABA within hippocampal-resident reactive astro- ␣5 or δ subunits) gives them sufficient sensitivity to
cytes, does not have much support in the literature, respond to low levels of ambient GABA [295]. It is the
either for AD or ARBD. resulting low-level inhibitory currents, collectively
The lipid invasion model provides an alternative termed “tonic inhibition”, which are associated with
mechanism, extending beyond tonic inhibition. This AA [296–298]. (By contrast lower-affinity synap-
mechanism accounts for the coexistence of AA tic GABAARs, with different subunit compositions,
in AD and ARBD, as well as other similarities, respond only to the higher concentrations of GABA
including the similar patterns of neurodegeneration released within their associated synapses, with the
within the two major neurogenic niches, i.e., the resulting phasic inhibition causing the other, later,
SGZ and SVZ, as outlined in the previous sec- anesthetic effects [287, 294, 299], including anal-
tion. Underlying this common mechanism is the gesia, immobility, and unconsciousness.) In support
proven affinity of ethanol, and very likely affinity of this, pharmacological and genetic knockdown of
of FFAs, for GABAA receptors (GABAARs), as extrasynaptic ␣5- and δ-containing GABAARs in
well as the recently-discovered role of high-affinity mice has been shown to improve performance on
extrasynaptic GABAARs in both tonic inhibition learning and memory tasks [300–302], possibly by
and anesthesia-associated amnesia. This mechanism lowering the threshold for long-term potentiation
is explained more fully in the next section. [303–305].
The reason for this is that GABAARs have
FFAs as anesthetics
associated ion channels, which become permeable
From the 1950s onward, Samson and Dahl, and
to chloride (and, to a lesser extent, HCO3 ) ions,
other groups, showed that injection of FFAs induced
in response to GABA ligation [306–308]. Upon
light general anesthesia in a range of mammals
such activation, chloride ions flow through these
[278–281]. Anesthetic potency increases with FFA
GABAAR channels in a direction determined by
chain length, and thus hydrophobicity, up to an unde-
their electrochemical gradient. Since mature neurons
termined cut-off, in line with the well-established
maintain an excess of chloride ions externally, the
Meyer-Overton correlation [278, 279, 282, 283].
normal response to GABA binding is therefore for
Such potencies fall within the low millimolar range
these negative ions to flow in through the GABAAR
(expressed both as moles per liter and moles per
channels, increasing the negative membrane poten-
kilogram of body weight) and show similar poten-
tial and thereby hyperpolarizing (i.e. inhibiting) the
cies to structurally comparable 1-alcohols (including
affected neuron [307, 309]. Tonic inhibition is the
ethanol) [284], as well as to alkanes [285] and alde-
extrasynaptic form of this [310, 311]. The majority
hydes [286]. All of which suggests that plasma levels
of anesthetic agents (including those that are only
of FFAs may be only an order of magnitude or so less
weakly anesthetic, such as ethanol) are known to
than general anesthetic potency levels.
enhance this GABA binding, acting primarily as pos-
Given the general correlation between hydropho-
itive allosteric modulators [312, 313]. Accordingly,
bicity and anesthetic potency first described (inde-
they tend to inhibit normal activity in mature neurons
pendently) by Meyer and Overton [287], it would
of the CNS [312, 314, 315], resulting in the vari-
perhaps be surprising if FFAs did not show similar
ous anesthetic effects, among the earliest of which is
anesthetic potencies to structurally very similar fatty
AA—the form of amnesia primarily associated with
alcohols/alkanols [287–290]. Nor, given the estab-
AD, at least in its early stages.
lished anesthetic properties of various steroids [291,
292], should it be a surprise that other lipids might
Extrasynaptic GABAARs and neurogenesis
display similar properties.
However, recent research has shown that the same
Anesthesia, AA, and extrasynaptic GABAARs high-affinity extrasynaptic GABAARs that mediate
The immediate significance of lipids’ anesthetic tonic inhibition in mature neurons [295, 316] also
properties to dementia, in terms of the model, lies in play a significant role in neurogenesis and neuronalYou can also read