2021 Ready or Not: PROTECTING THE PUBLIC'S HEALTH FROM DISEASES, DISASTERS, AND BIOTERRORISM
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Ready or Not:
ISSUE REPORT
2021
PROTECTING THE PUBLIC’S HEALTH FROM
DISEASES, DISASTERS,
AND BIOTERRORISM
MARCH 2021
Acknowledgements
The National Health Security Preparedness Index (NHSPI) is a joint
Trust for America’s Health (TFAH) is a nonprofit, nonpartisan
initiative of the Robert Wood Johnson Foundation, the University
public health policy, research, and advocacy organization that
of Kentucky, and the University of Colorado. TFAH wishes to
promotes optimal health for every person and community and
recognize and thank Glen Mays and Michael Childress of the
makes the prevention of illness and injury a national priority.
NHSPI for their collaboration and expertise as well as the Robert
The Ready or Not report series is supported by generous Wood Johnson Foundation for its continued funding support.
grants from the Robert Wood Johnson Foundation, with
Ready or Not and the NHSPI are complementary projects that
additional support from The California Endowment, W.K.
work together to measure and improve the country’s health
Kellogg Foundation and The Kresge Foundation. Opinions
security and emergency preparedness. TFAH looks forward to a
in this report are TFAH’s and do not necessarily reflect the
continued partnership.
views of its funders.
TFAH BOARD OF DIRECTORS
Gail Christopher, D.N. Stephanie Mayfield Gibson, M.D. Eduardo Sanchez, M.D., MPH
Chair of the Board Director Chief Medical Office for Prevention
Executive Director U.S. COVID-19 Response Initiative American Heart Association
National Collaborative for Health Equity Resolve to Save Lives
Umair A. Shah, M.D., MPH
Former Senior Advisor and Vice President
Cynthia M. Harris, Ph.D. Secretary of the Health
W.K. Kellogg Foundation
Associate Dean for Public Health Washington State
David Fleming, M.D. Director and Professor
Vince Ventimiglia, JD
TFAH Distinguished Visiting Fellow and Vice Institute of Public Health
President
Chair, TFAH Board of Directors Florida A&M University
Collaborative Advocates
Robert T. Harris, M.D., FACP David Lakey, M.D. Leavitt Partners
Treasurer of the Board Chief Medical Officer and Vice Chancellor for
Senior Medical Director Health Affairs TRUST FOR AMERICA’S HEALTH
General Dynamics Information Technology The University of Texas System LEADERSHIP STAFF
Theodore Spencer, M.J. Octavio Martinez Jr., M.D., MPH, MBA, FAPA John Auerbach, MBA
Secretary of the Board Executive Director President and CEO
Co-Founder Hogg Foundation for Mental Health
J. Nadine Gracia, M.D., MSCE
Trust for America’s Health The University of Texas at Austin
Executive Vice President and Chief Operating Officer
John A. Rich, M.D., MPH
Co-Director of the Center for Nonviolence and
Social Justice
Drexel University School of Public Health
REPORT AUTHORS EXTERNAL REVIEWERS
Matt McKillop, MPP This report benefited from the insights and expertise of the following external reviewers. Although
Senior Health Policy Researcher and Analyst they have reviewed the report, neither they nor their organizations necessarily endorse its findings
or recommendations. TFAH is extremely grateful to these reviewers for their time and expertise.
Dara Alpert Lieberman, MPP
Director of Government Relations James Blumenstock Shelley A. Hearne, DrPH
Senior Vice President Deans Sommer and Klag Professor for Public
Rhea K. Farberman, APR
Pandemic Response and Recovery Health Advocacy
Director of Strategic Communications and Policy
Association of State and Territorial Health Director, Center for Public Health Advocacy
Research
Officers (ASTHO) Johns Hopkins University Bloomberg School of
Public Health
CONTRIBUTING AUTHOR Dr. Oxiris Barbot, M.D.
Adjunct Assistant Professor David Fleming, M.D.
Kendra May
Columbia University Mailman School of Public TFAH Distinguished Visiting Fellow and Vice
Consultant
Health and Senior Fellow for Public Health and Chair, TFAH Board of Directors
Social Justice at the JPB Foundation
Former New York City Health Commissioner
2 TFAH • tfah.org
Table of Contents Ready or Not
TABLE OF CONTENTS
Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
S
idebar: COVID-19 and Emergency Preparedness: Tragic Lessons . . . . . . . . . . . . . 6 2021
Interview: Earning Vaccine Confidence in Communities of Color . . . . . . . . . . . . . . 12
SECTION 1: A
SSESSING STATES’ PREPAREDNESS . . . . . . . . . . . . . . . . . . . . . . . . 15
Indicator 1: Nurse Licensure Compact . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Indicator 2: Hospital Participation in Healthcare Coalitions . . . . . . . . . . . . . . . . . . 18
Indicators 3 and 4: Accreditation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Indicator 5: Public Health Funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Indicator 6: Water System Safety . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Indicator 7: Access to Paid Time Off . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Indicator 8: Flu Vaccination Rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Indicator 9: Patient Safety in Hospitals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Indicator 10: Public Health Laboratory Surge Capacity . . . . . . . . . . . . . . . . . . . . . 32
Indicators Performance Matrix by State . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
SECTION 2: RECOMMENDATIONS FOR FEDERAL AND STATE POLICY ACTIONS . . . 36
P
riority Area 1: Provide Stable, Sufficient Funding for Domestic and Global Public
Health Security . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Priority Area 2: Prevent Outbreaks and Pandemics . . . . . . . . . . . . . . . . . . . . . . . . 39
P
riority Area 3: Build Resilient Communities and Promote Health Equity in
Preparedness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
P
riority Area 4: Ensure Effective Leadership, Coordination, and Workforce . . . . . . . 43
riority Area 5: Accelerate Development and Distribution of Medical
P
Countermeasures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Priority Area 6: Ready the Healthcare System to Respond and Recover . . . . . . . . 47
Priority Area 7: Prepare for Environmental Threats and Extreme Weather . . . . . . . . 49
APPENDIXES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Year in Review – 2020 Health Threats Incidents and Actions . . . . . . . . . . . . . . . . 50
Report Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
Endnotes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
Editor’s note: This report was being prepared during a presidential transition. We
have included comments in the report where we have noted action on TFAH policy
recommendations by the Biden administration.
View this report online at www.tfah.org/report-details/readyornot2021
MARCH 2021
Ready or Not Executive Summary
EXECUTIVE SUMMARY
2021 The past year, 2020, will long be remembered as the year more
than 2 million people lost their lives due to a global pandemic. Not
since the 1918 influenza pandemic has a single event so urgently
demonstrated the criticality of a strong public health system. This
Ready or Not report has tracked the country’s level of public health
emergency preparedness since 2003. For nearly two decades, it has
asked the fundamental question: “are we ready?” Unfortunately, the
COVID-19 crisis has provided a clear answer: an emphatic “no.”
The COVID-19 crisis has illuminated In addition, the pandemic has once
the urgent need for federal, state, local, again demonstrated and exacerbated
tribal, and territorial leaders to take the impact of structural racism, both
aggressive steps to shore up the nation’s historic and current, on the health and
preparedness for all types of emergency well-being of communities of color and
events. The pandemic put a spotlight Tribal Nations. Acknowledging the
on a public health system hollowed- lingering health impacts of slavery and
out by years of insufficient funding. the treatment of native peoples and
Health departments were overstretched, addressing current day racist policies,
responding to the pandemic with systems, and attitudes must be part
archaic technologies1 and with of building the nation’s resilience.
overworked staff who faced threats In short, equity is not separate from
and retribution.2 These gaps were preparedness. Ensuring an equitable
all the more critical in 2020 because opportunity for the health and well-
the federal government failed to take being of all residents before a disaster
an evidence based, leadership role in creates more resilient communities
the pandemic response, with many during an emergency. Equity must be an
decisions being left to states that would explicit and foundational principle in all
ordinarily be federally coordinated. emergency planning. Achieving equity
It also demonstrated the harm that in all facets of emergency response
can be done when science and public requires including equity accountability
health expertise are stifled by political metrics in emergency preparation and
interference and misinformation. management.
MARCH 2021
Foundational capabilities are necessary
throughout the public health system, “A powerful aspect of this report is its long history objectively
from the Centers for Disease Control measuring states’ preparedness. This year’s recommendations
and Prevention (CDC) to state,
local, tribal, and territorial health are almost identical to past years. Had the nation paid more
departments, including:3 attention to pandemic threats and TFAH’s commonsense and
l H
ealth monitoring and assessment, consistent recommendations, this country would be in a very
comprising surveillance,
different place today.”
epidemiology, and laboratory capacity;
Shelley A. Hearne, DrPH
l A
ll-hazards preparedness and response;
Johns Hopkins University Bloomberg School of Public Health
l P
olicy development and support;
l P
ublic communications;
It is also important to note that the threats. They are not tailored to an
l C
ommunity outreach and partnership infusion of COVID-19 emergency assessment of a given state’s response to
development; funding was onetime funding—critical the COVID-19 pandemic, as widescale
to the pandemic response but not political, funding, economic, and social
l O
rganizational and administrative
a solution to the system’s longtime factors all influenced the virus impact
competencies (i.e., leadership,
underinvestment. and local responses. A state may do well
governance, and health equity); and
in terms of its ranking in this report but
This report is designed to give
l A
ccountability and performance poorly in its response to the COVID-19
policymakers at all levels of government
management.4 pandemic—and vice versa. While no
actionable data and recommendations
state has been spared, what seems to
Today, only half of Americans are with which they can target policies
have mattered most in the pandemic
protected by a comprehensive local and spending to strengthen their
response is a state’s socioeconomic and
public health system.5 The Public jurisdiction’s emergency preparedness.
racial profile, as well as the adherence
Health Leadership Forum estimates The report’s 10 key public health
of elected leaders and residents to
a $4.5 billion annual shortfall in preparedness indicators give state
evidence-based public health guidelines.
the spending necessary to meet officials benchmarks for progress, point
The pandemic has illustrated that
the infrastructure needs of public out gaps within their states all-hazards
robust and sustained funding, elected
health agencies nationwide.6 This preparedness, and provide data to
officials’ leadership, and federal-state
shortfall was on display throughout compare states’ performance against
coordination and planning are key to
the COVID-19 pandemic, as decades like jurisdictions. These data points,
protecting Americans’ health security.
of chronic underfunding hindered or ones similar to them, have been the
Moreover, there is no substitute at the
communications, disease surveillance, focus of this report for over a decade
state or local level for a strong federal
contact tracing, vaccine delivery, and and are meant to measure readiness
response.
other key health department activities. for a broad set of health security
TFAH • tfah.org 5
COVID-19 AND EMERGENCY PREPAREDNESS: TRAGIC LESSONS
TFAH’s Ready or Not: Protecting the
Public’s Health from Diseases, Disasters
and Bioterrorism report has tracked the
nation’s readiness to respond to a public
health emergency for nearly two decades.
During that time, no event highlighted
the critical importance of this report’s
purpose—measuring and promoting
readiness to safeguard Americans’ health
during an emergency—to the degree the
COVID-19 crisis has.
The COVID-19 pandemic is an on-
the-ground, real-time measure of the
nation’s public health emergency
response system—a test the federal
government failed according to most
public health experts. An October
2020 report by Columbia University
Earth Institute’s National Center for
Disaster Preparedness estimated that
the federal government’s inadequate
pandemic response led to between
130,000 and 210,00 avoidable
deaths. The report submits that if
the United States had implemented
sufficient testing, earlier lockdowns, a accreditation, (4) public health funding, Importance of Federal Leadership
national mask-wearing mandate, and (5) access to paid time off, (6) flu Government at multiple levels shares
provided federal guidance on social vaccination rates (as a proxy for a responsibility for emergency planning
distancing, over 200,000 lives could community’s vaccination infrastructure and response. Under this tiered
have been saved.7 and receptivity), and (7) laboratory structure, when an event requires a
With a possible single exception (water surge capacity. TFAH will continue to larger response than a local entity
system safety), all of the readiness measure states on these indicators, as can provide, government from the tier
indicators measured annually by this they play a central role in the standing- above it—typically a tribal, territorial
Ready or Not report played a role in ready, public health protection capacity or state agency—provides assistance.
jurisdictions’ COVID-19 response. that every state needs. When a state’s response resources
Seven were relevant to the effort to The pandemic has also spotlighted a are not enough to meet demands
control the pandemic and save lives: number of issues not currently measured during an emergency, the federal
(1) nurse licensure compact (allowing by the report but critical and dramatically government provides support. For a
jurisdictions to borrow medical apparent if absent during a health public health emergency as significant
personnel when they need to surge emergency: federal and state political and contagious as COVID-19, clear
capacity), (2) hospital participation leadership, interagency coordination, communication and strong leadership
in healthcare coalitions, (3) public consistent and well-executed public and coordination by the federal
health and emergency management communications, and health equity. government are essential, elements
6 TFAH • tfah.org
that were lacking during the initial Overcoming the Legacy of Racism l Developing a White House led strategy
months of the pandemic response. The legacy of slavery, genocide, focused on addressing the root
Instead, inconsistent messages and centuries of racism, combined causes of disease and on promoting
between federal agencies and the White with current day interpersonal and health equity.
House; lack of centralized coordination, structural racism, is at the root of the l Creating a social determinants of
such as for procurement of personal disproportionate impact COVID-19 has health line item at the Centers for
protective equipment (PPE); and had on communities of color and Tribal Disease Control and Prevention
political interference with guidance from Nations. These systemic inequities, in (CDC), authorized and fully funded
scientific agencies—all led to confusion access to healthcare, housing, education, by Congress, with sufficient funding
and contradictory policies among states transportation, and employment, existed to guarantee grant-funded efforts
and weakened the emergency response. before the pandemic and have been throughout the nation.
TFAH has made a number of policy exacerbated by it. Health inequities due l Requiring all agencies to collect,
recommendations designed to ensure to disadvantages experienced by racial, disaggregate, and report health
robust and nonpartisan federal ethnic, or other population groups are data in such a way that the impact
leadership during future public health preventable differences in the burden of of health conditions, policies, or
emergencies, including: disease, injury, and health emergencies interventions on specific population
and to opportunities to achieve good groups are known, including health
l Create a White House Health
health.8 Addressing issues at the status data by race, ethnicity, sexual
Security Directorate, including senior
root of health inequity is imperative to orientation, gender identity, primary
advisors to the president with public
ensuring all people, regardless of their language, and disability status.
health expertise on health security
race or ethnicity or where they live, have
issues. This directorate would The tragedy of the COVID-19
the opportunity for good health and are
oversee the national biodefense pandemic, including over 500,000
protected during a health emergency.
strategy and all interagency deaths in the United States (as this
emergency responses. TFAH has called on the administration publication was being prepared) and
l Ensure full transparency and and Congress to make advancing unprecedented harm to the economic
consistency in federal messaging health equity and eliminating health security of millions of American
from the White House, CDC, ASPR, disparities a national priority by: families, will forever be a painful
FDA, and National Institutes of Health l Ensuring that all COVID-19 response reminder of the critical importance
(NIH) concerning public health issues actions prioritize advancing health of pre-event public health emergency
to ensure message clarity, avoid equity, including access to COVID-19 preparations, investments in public
confusion, and build trust. testing and vaccinations. health infrastructure, and evidence-
l Ensure that federal public health l Creating a Truth, Racial Healing, and based policy and communications. The
officials are fully empowered to make Transformation Commission, and pandemic has undeniably demonstrated
decisions based on science and provide funding to communities to begin that historical discrimination coupled
without undue political influence. the process of acknowledging a history with current-day racism impacts a
Efforts to infuse politics into public of racism and working to dismantle the community’s health status and ability
health decision-making puts the myth of hierarchy based on race. to weather a disaster. The COVID-19
public’s health at risk. crisis has also painfully reinforced
l E xpanding funding for initiatives
that national leadership must be
l HHS should strengthen leadership serving communities that have been
grounded in science and committed
by working with states and suppliers marginalized by disinvestment, and
to addressing structural racism, both
to ensure adequate stockpiling ensure that federal funding supports
of which are imperative to saving lives
and distribution of medical processes that meaningfully engage
during an emergency.
countermeasures and ancillary the most affected communities in
emergency response products, such the planning and implementation of
as personnel protective equipment. such initiatives.
TFAH • tfah.org 7
This edition of the Ready or Not series other areas—such as paid time off for compared with last year, while eight fell
finds that states have made progress workers and hospital patient safety—has behind. Three states improved by one
in most of the report’s measured stalled. In this 2021 report, Trust for tier, six states dropped one tier, and two
areas, especially rates of seasonal flu America’s Health (TFAH) found that dropped two tiers.
vaccination. However, improvement in three states improved their standing
TABLE 1: Top-Priority Indicators of State Public Health Preparedness
INDICATORS
1 Incident Management: Adoption of the Nurse Licensure Compact. 6 Water Security: Percentage of the population that used a community
water system that failed to meet all applicable health-based standards.
2 Cross-Sector Community Collaboration: Percentage of hospitals 7 Workforce Resiliency and Infection Control: Percentage of employed
participating in healthcare coalitions. population that used paid time off.
3 Institutional Quality: Accreditation by the Public Health 8 Countermeasure Utilization: Percentage of people ages 6 months or
Accreditation Board. older who received a seasonal flu vaccination.
4 Institutional Quality: Accreditation by the Emergency Management 9 Patient Safety: Percentage of hospitals with a top-quality ranking (“A”
Accreditation Program. grade) on the Leapfrog Hospital Safety Grade.
5 Institutional Quality: Size of the state public health budget 10 Health Security Surveillance: The public health laboratory has a plan
compared with the past year. for a six- to eight-week surge in testing capacity.
Notes: The National Council of State Boards of Nursing organizes the Nurse Licensure Compact. The federal Hospital Preparedness Program of the U.S.
Office of the Assistant Secretary for Preparedness and Response supports healthcare coalitions. The U.S. Environmental Protection Agency assesses commu-
nity water systems. Paid time off includes sick leave, vacation time, or holidays, among other types of leave. The Leapfrog Group is an independent nonprofit
organization. TFAH drew every indicator, and some categorical descriptions, from the National Health Security Preparedness Index, with one exception: pub-
lic health funding. See “Appendix A: Methodology” for a description of TFAH’s funding data-collection process, including its definition.
Source: National Health Security Preparedness Index 9
The Ready or Not report groups states a greater share of its hospitals receive that received an “A” rating—one of
and the District of Columbia into one high marks on patient safety. Montana, the highest in the nation—rose by
of three tiers (high, middle, low) based which elevated from the low tier to the slightly less than the national average.
on their performances across the 10 middle tier, increased its public health Other steps it could take to improve
indicators. This year, 20 states and funding level in fiscal year 2020. And its standing include joining the Nurse
the District of Columbia scored in the Rhode Island, which rose from the Licensure Compact or increasing its
high-performance tier, 15 placed in the middle tier to the high tier, did so by below-average share of residents who
middle-performance tier, and 15 were dramatically increasing its community take paid time off from work.
in the low-performance tier (see Table drinking-water security.
Five states fell from the high tier to the
2). (See “Appendix A: Methodology”
Two states fell from the high tier to the middle tier: Alabama, Illinois, Iowa,
for more information on the scoring
low tier: Missouri and Pennsylvania. New Jersey, and Tennessee. These
process.)
Missouri cut its public health funding in states did not experience significant
Three states showed notable FY 2020 and saw an increase in the share backsliding overall, but they lost ground,
improvement, moving up a tier: of its residents that used a community as a number of other states took greater
Georgia, Montana, and Rhode Island. water system with one or more health- steps that increased their standing.
Georgia, which rose from the middle based violations. Its flu vaccination
One state fell from the middle tier to
tier to the high tier, improved its rate ticked up marginally, but by less
the low tier: Arizona. Arizona’s below-
standing by achieving accreditation than the nation as a whole. Likewise,
average flu vaccination rate rose, but by
by the Emergency Management Pennsylvania also cut its public health
less than the nation overall, so its overall
Accreditation Program and by having funding level, and its share of hospitals
standing fell back.
8 TFAH • tfah.org
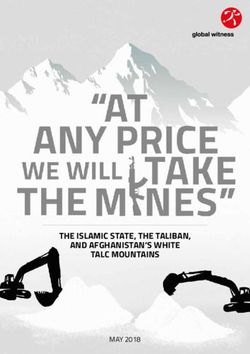
TABLE 2: State Public Health Emergency Preparedness
State performance, by scoring tier, 2020
Performance Number of
States
Tier States
CO, CT, DC, DE, GA, ID, KS, MA, MD, ME, MS,
High Tier 20 states and DC
NC, NE, NM, OK, RI, UT, VA, VT, WA, WI
AL, CA, FL, IA, IL, KY, LA, MI, MN, MT, ND, NJ,
Middle Tier 15 states
OR, TN, TX
AK, AR, AZ, HI, IN, MO, NH, NV, NY, OH, PA,
Low Tier 15 states
SC, SD, WV, WY
Note: See “Appendix A: Methodology” for scoring details. Complete data were not available for U.S.
territories.
TFAH’s Analysis Found: during an emergency. What’s more,
A majority of states have made every state had public health laboratories
preparations to expand healthcare that had plans for how to manage a
and public health capabilities in an large influx of testing needs. States had
emergency, often through collaboration. a plan to surge public health laboratory
Thirty-four states participated in the capacity for six to eight weeks as necessary
Nurse Licensure Compact, up from 26 during overlapping emergencies or large
in 2017,10 with Indiana and New Jersey outbreaks, an increase of six states since
being the most recent adopters.11 The 2017.
compact allows registered nurses and Most states are accredited in the
licensed practical or vocational nurses areas of public health, emergency
to practice in multiple jurisdictions management, or both. As of December
with a single license. In an emergency, 2020, the Public Health Accreditation
this enables health officials to quickly Board (PHAB) or the Emergency
increase their staffing levels. For example, Management Accreditation Program
nurses may cross state lines to work at (EMAP) accredited 42 states and the
evacuation sites or other healthcare District of Columbia; 29 states and the
facilities. In addition, hospitals in most District of Columbia were accredited
states have a high degree of participation by both groups, a net increase of
in healthcare coalitions. On average, 89 one since November 2019. (EMAP
percent of hospitals were in a coalition, has now accredited Delaware and
and 17 states and the District of Columbia Georgia; Maryland transitioned from
had universal participation, meaning being accredited by both bodies to the
every hospital in the jurisdiction was PHAB only, with the EMAP providing
part of a coalition. Such coalitions bring conditional accreditation.) Eight states
hospitals and other healthcare facilities (Alaska, Hawaii, Indiana, New Hampshire,
together with emergency management South Dakota, Texas, West Virginia, and
and public health officials to plan for and Wyoming) were not accredited by either
respond to incidents or events requiring group. Both programs help ensure that
extraordinary action. This increases the necessary emergency prevention and
likelihood that providers serve patients response systems are in place and staffed
in a coordinated and efficient manner by qualified personnel.
TFAH • tfah.org 9
Seasonal flu vaccination rates, while still Most residents who received their
too low, have risen significantly. The household water through a community
seasonal flu vaccination rate among water system had access to safe water. On
Americans ages 6 months or older rose average, just 5 percent of state residents
from 42 percent during the 2017–2018 used a community water system in 2019
season to 52 percent during the 2019– (latest available data) that did not meet
2020 season.12 However, Healthy People all applicable health-based standards,
2030, a set of federal 10-year objectives down slightly from 7 percent in 2018.
and benchmarks for improving the Water systems with such violations
health of all Americans by 2030, set increase the chances of water-based
a seasonal influenza vaccination-rate emergencies in which contaminated
target of 70 percent annually.13 water supplies place the public at risk.
In 2019, only 55 percent of employed state Based on its policy research and
residents, on average, used paid time off, analysis, consultation with experts,
the same percentage as in 2018. Those and review of progress and gaps in
without paid leave are more likely to work federal and state preparedness—with
when they are sick and risk spreading a particular focus on the preparation
infection. In the past, the absence of gaps and shortfalls identified by
dedicated paid sick leave has been linked the COVID-19 pandemic—TFAH is
to or has exacerbated some infectious recommending policy action in seven
disease outbreaks.14 This became priority areas:
particularly relevant during the COVID-
1. P
rovide stable, sufficient funding
19 pandemic, as isolation and quarantine
for domestic and global public
were important tools for controlling the
health security.
outbreak. The Families First Coronavirus
Response Act helped address this issue 2. Strengthen policies and systems to
during the early stages of the pandemic for prevent and respond to outbreaks
employers with fewer than 500 employees and pandemics.
and certain public employers, temporarily
3. B
uild resilient communities and
requiring employees to be paid up to 80
promote health equity generally and
hours of sick leave benefits under certain
in preparedness.
conditions.15 In January 2021, the Biden
administration economic stimulus package 4. E
nsure effective public health
proposal included extending paid sick leadership, coordination, and
leave to over 100 million U.S. workers. workforce.
Only 31 percent of hospitals, on 5. A
ccelerate development and
average, earned a top-quality patient distribution, including last-
safety grade, up slightly from 30 mile distribution, of medical
percent in 2019. Hospital safety scores countermeasures.
measure performance on such issues as
6. S
trengthen the healthcare system’s
healthcare-associated infection rates,
ability to respond to and recovery
intensive-care capacity, and an overall
from health emergencies.
culture of error prevention. In January
2021, the Biden administration’s 7. P
repare for environmental threats
economic aid package included and extreme weather.
extending paid sick leave to over 100
million U.S. workers.
10 TFAH • tfah.orgReport Purpose and Methodology
TFAH’s annual Ready or Not report series Foundation, the University of Kentucky,
tracks states’ readiness for public health and the University of Colorado. (See
emergencies based on 10 key indicators “Appendix A: Methodology” for a
that collectively provide a checklist of detailed description of how TFAH
top-priority issues and action items for selected and scored the indicators.)
states and localities to continuously
While state placements in Ready or
address. By gathering together timely
Not and the NHSPI largely align,
data on all 50 states and the District
there are some important differences.
of Columbia, the report assists states
The two projects have somewhat
in benchmarking their performance
different purposes and are meant to be
against comparable jurisdictions.
complementary, rather than duplicative.
TFAH completed this research after
With more than 100 indicators, the
consultation with a diverse group of
Index paints a broad picture of national
subject-matter experts and practitioners.
health security, allowing users to zoom
out and holistically understand the
Ready or Not and the National Health
extent of both individual states’ and the
Security Preparedness Index
entire nation’s preparedness for large-
The indicators included in this report scale public health threats. In slight
were drawn from, and identified in contrast, Ready or Not, with its focus on
partnership with, the National Health 10 select indicators, focuses attention on
Security Preparedness Index (NHSPI),16 state performances on a subset of the
with one exception: a measure of state Index and spotlights important areas
public health funding-level trends, for stakeholders to prioritize. TFAH
which reflects how well-resourced key and the NHSPI work together to help
agencies are to prepare and respond federal, state, and local officials use data
to emergencies. The NHSPI is a joint and findings from each project to make
initiative of the Robert Wood Johnson Americans safer and healthier.
TFAH • tfah.org 11Earning Vaccine Confidence in Communities of Color
Interview with Claude A. Jacob, Dr.PH(c), MPH, the chief public
health officer at the Cambridge, Massachusetts, Public Health
Department, and Maria Lemus, the executive director of Visión y
Compromiso, about barriers—both historic and contemporary—
to COVID-19 vaccinations within communities of color. This
interview was conducted in December 2020.
TFAH: As this report is being finalized, voice on COVID-19. Given this finding,
the United States is nearing a time when we plan to work closely with our hospitals,
many Americans, particularly those ambulatory sites, and healthcare
at the highest risk of infection or the providers to help spread the message.
most serious impact if infected, can be
Ms. Lemus: There are many barriers.
vaccinated. What are the barriers to high
The ones I’m most concerned about are
rates of vaccination in communities of
myths and misinformation, including
color and among Tribal nations?
crazy social media propaganda, fear of
Dr. Jacob: We are fortunate in adverse reactions, and problems with
Cambridge. Flu vaccine participation is vaccine accessibility. High rates of the
strong and childhood vaccine compliance uninsured among some populations
is also very high, which we view as rough groups and misconceptions about who is
proxies for COVID-19 vaccine acceptance. at risk are additional concerns.
That being said, there is a long and
TFAH: The pace of COVID-19 vaccines
sordid history of abuse and mistreatment
development has been quicker than
of these communities by the U.S.
many people expected. In some
government and healthcare system. That
communities this may mean that
many Black and Brown people continue
the vaccine will be available before
to feel deep mistrust of the healthcare
communications programs about
system is understandable. All of us in
the vaccine’s safety and availability
healthcare and public health must
have fully taken root. What do those
understand that this mistrust goes back
responsible for vaccine distribution
to slavery for Black Americans and the
need to do when distributing the vaccine
genocide perpetuated against indigenous
under these circumstances?
people that lasted for centuries.
Dr. Jacob: First of all, we need to
We have strong relationships with
celebrate the news that, so far,
community organizations, leaders in the
two vaccines have received FDA
faith community, and others who are well
emergency use authorization. That
known and trusted among communities
two vaccines were developed, tested,
of color, and we will partner with them
and manufactured in less than 12
to overcome these barriers to vaccine
months is a breathtaking achievement.
uptake. Recent national and state surveys
While we can’t let down our guard on
have told us that Americans view their
physical distancing, wearing masks,
personal physician as the most trusted
12 TFAH • tfah.organd continuing to practice good hand
hygiene, the COVID-19 vaccine marks
a watershed moment in the pandemic.
We now see the light at the end of
the tunnel. At the same time, it’s
understandable that people have many
questions and deep concerns given how
quickly the vaccine was developed and
approved. For communities of color, the
concern over safety comes with a long-
standing, entrenched, and well-placed
mistrust of the healthcare system.
Communication will be pivotal
in educating everyone, especially
communities of color, about the safety
and importance of this vaccine. To
start, we need to have communities
of color and physicians of color at the
TFAH: A woeful history of mistreatment speak to these injustices; they must
decision-making table to inform and
of people of color by government and denounce them and support remedies.
ensure a vaccine rollout that is equitable
the healthcare system is at the root of They need to give real-time examples
for all members of our community.
much of the lack of trust in the COVID- of the efforts being made to engage
Messaging around the vaccine also
19 vaccine within those communities with and empower communities and
needs to be informed by, and tested
but there are other barriers to vaccine to correct past wrongs. Only then will
with, communities of color to make
access. What are they and how can they government be able to be heard and
sure that these communication efforts
be overcome? only by using trusted messengers and
resonate. We have a superb opportunity
community navigators.
to work with those on the front line Ms. Lemus: The understandable
of this pandemic, especially doctors, distrust of government is going to It’s also important to remember that
nurses, and physicians’ assistants, be a huge barrier to the vaccine. A the reasons for distrust of government
to help amplify the message in core specific example for my community is within underrepresented communities
communities. By all accounts, frontline the Bracero Program, which between is not only about historical legacies;
medical workers are the most trusted 1942 and 1964, based on a series of it is based on current-day events and
source of health information and they bilateral agreements between the U.S. climates. However, it can be corrected.
are the first to be vaccinated, starting and Mexican governments, brought My organization, Visión y Compromiso,
this past December. We should use their nearly 4.6 million Mexican citizens has as its mission providing leadership-
voices of trust and reason to speak to to work on U.S. farms, railroads, and development and capacity-building
communities of color about the safety factories. Those workers experienced opportunities for promotores and
and critical importance of getting this racial and wage discrimination and were community health workers in over
vaccine. forced to live and work in substandard 4,000 communities. These community-
conditions. More recently, there based promotores will have a critical role
Ms. Lemus: It will be imperative to
have been allegations of unnecessary to play in reducing vaccine hesitancy
share data about the vaccine without
hysterectomies being performed in ICE in communities of color. Messaging to
jargon and to have trusted messengers
detention centers. convince people to be vaccinated has to
deliver the information. I heard a quote
feature their heroes, their community
recently in response to the question, The only way to overcome these
leaders, their voices.
“Do you know what’s in Tylenol?”: “No, histories will be to first acknowledge
but I trust it will help me.” them. Leaders must acknowledge and
TFAH • tfah.org 13Dr. Jacob: Communities of color have TFAH: What is the importance of where uptake in your community? What
historically had difficulty accessing the COVID-19 vaccine is available in resources do you need to be successful?
healthcare. Lack of transportation, your community?
Dr. Jacob: Local public health has
work schedules, childcare needs, and
Ms. Lemus: Where the vaccine will be an important role and responsibility
competing financial interests—such as
available is another critical issue. The in educating communities about the
paying rent and bills—pose significant
credibility, location, hours, accessibility, safety and importance of the COVID-19
barriers to healthcare, as do other social
relationship to community, their vaccine, as it does with all vaccinations.
determinants of health, such as poverty
staff, and emissaries are important to Once the vaccine is made available
and lack of education. Even with the
individual and families’ decision to be to the general public, the Cambridge
Affordable Care Act—which greatly
vaccinated. Promotores are important Public Health Department, through its
expanded access to health insurance
also in gathering information to partnership with city agencies and the
for everyone—Hispanic, Black, and
contribute to the vaccine distribution private sector, will be ready to provide
some Asian communities have lower
and administration, planning vaccines to residents. Throughout the
insurance coverage rates than any other
implementation, and communications. pandemic, our department has worked
population. Many of them remain
Community-based organizations hand in hand with city partners, especially
uninsured altogether.
must be included in all planning and first-responders, to provide testing and
The cost of the vaccine is being covered execution; they are a big part of the flu shots, and we will rely on this strong,
by the federal government through solution. Partnering with community- successful relationship to provide the
tax dollars, but providers can charge based organizations allows local officials COVID vaccine. It is critically important
to administer the vaccine, if they to scale means and resources. to note that we could not do our work
choose. We need to do everything without strong financial support. Our city
Dr. Jacob: As I have already
we can and work with providers to manager, Louis A. DePasquale, and the
mentioned, the Cambridge Public
eliminate fees they may charge in the Cambridge City Council have provided
Health Department has had enormous
interest of overcoming this public financial resources to fight this pandemic
success with COVID-19 testing and flu
health emergency. When it is available, and keep our residents and those who
vaccinations by bringing these services
we need to bring the vaccine to the work in Cambridge safe. They have long
to people in the communities where
public rather than making people been committed to the important work
they live and work. We have taken
come to the vaccine. In Cambridge, of the public health department, which
a traditional grassroots approach—
the public health department, through is enhanced by the Cambridge Health
going door to door in harder-hit
its partnership with the city’s first- Alliance led by Dr. Assaad Sayah, who is
neighborhoods and providing
responders and others, have made the commissioner of public health for the
information in eight languages—to build
free COVID-19 testing available to all city of Cambridge.
trust and understanding. We need to
residents (regardless of symptoms) Dr. Claude A. Jacob is the chief public health
use this same approach with the COVID-
since July 2020. Starting in November officer for the City of Cambridge, Massachusetts.
19 vaccine and build on these robust He served as the president of the National
2020, this “no-barrier,” city-funded
community linkages, which are anchored Association of City and County Health Officials in
testing program expanded to seven
to the long-standing relationships that we 2016–2017.
days a week (from two days/week) and
have with partners on the ground. Maria Lemus is the executive director of Visión
from two neighborhood sites to four.
y Compromiso, headquartered in San Francisco,
These testing sites are geographically TFAH: As the chief public health California. Visión y Compromiso provides
dispersed, and all but one are located in officer for the city of Cambridge, leadership, advocacy, and capacity-development
neighborhoods with disproportionately Massachusetts, what is your training to community health workers.
high rates of new COVID-19 infections. department’s role in increasing vaccine
14 TFAH • tfah.orgSECTI O N 1:
Assessing State Preparedness Ready or Not
SECTION 1: ASSESSING STATE PREPAREDNESS
Every state needs to be prepared to respond to a variety of 2021
potential public health emergencies; such readiness requires
understanding an individual state’s preparedness strengths, risks,
and vulnerabilities. To help states assess their readiness, and to
highlight a checklist of top-priority concerns and action areas,
this report examines a set of 10 select indicators. The indicators,
used consistently year to year, draw heavily from the National
Health Security Preparedness Index (NHSPI), a joint initiative
of the Robert Wood Johnson Foundation, the University of
Kentucky, and the University of Colorado. They capture core
elements of emergency preparedness.
Based on states’ standing across the 10 indicators (see “Appendix
A: Methodology” for scoring details), TFAH placed states into
three performance tiers: high, middle, and low. (See Table 3.)
TABLE 3: State Public Health Emergency Preparedness
State performance, by scoring tier, 2020
Performance Number of
States
Tier States
CO, CT, DC, DE, GA, ID, KS, MA, MD, ME, MS,
High Tier 20 states and DC
NC, NE, NM, OK, RI, UT, VA, VT, WA, WI
AL, CA, FL, IA, IL, KY, LA, MI, MN, MT, ND, NJ,
Middle Tier 15 states
OR, TN, TX
AK, AR, AZ, HI, IN, MO, NH, NV, NY, OH, PA,
Low Tier 15 states
SC, SD, WV, WY
Note: See “Appendix A: Methodology” for scoring details. Complete data were not available for U.S.
territories.
Importantly, the implications of and administrators. Moreover, some
this assessment, and responsibility indicators are under the direct control
for continuously improving, extend of federal and state lawmakers, whereas
beyond any one state or local agency. improvement in other indicators
Such improvement typically requires requires multisector, statewide efforts,
MARCH 2021
sustained engagement and coordination including by residents.
by a broad range of policymakers
TFAH • tfah.org 15INDICATOR 1: ADOPTION Workforce shortages can impair a state’s in nurses from other member states,
ability to effectively manage disasters without harmful delays, or to send
OF NURSE LICENSURE
or disease outbreaks, potentially nurses to other member states that
COMPACT resulting in poorer health outcomes for were experiencing acute shortages. For
those affected. This reality was starkly example, New Jersey, which experienced
KEY FINDING: 34 states illuminated by the COVID-19 pandemic one of the most severe outbreaks in
as healthcare capacity in some parts of spring 2020, began implementing the
participate in the Nurse the country was overwhelmed by the NLC, immediately qualifying out-of-
Licensure Compact. number of people needing care. In state nurses with a multistate license
an event like a pandemic, the ability to practice.17 “I think the COVID-19
to quickly surge qualified medical outbreak is going to cause the states
personnel by bringing healthcare that are not in the compact now to
workers from out of state is a key really take a second look at it,” says NLC
component of healthcare readiness. Director Jim Puente. “If the NLC was
expanded to all 50 states, none of the
This indicator examines whether states
guesswork with emergency orders would
have adopted legislation to participate
be necessary because nurses could travel
in the Nurse Licensure Compact
to other states where they are needed.
(NLC). Launched in 2000 by the
No applications, fees, or background
National Council of State Boards of
checks would be necessary.”
Nursing, the NLC permits registered
nurses and licensed practical nurses As of December 2020, 34 states had
to practice with a single multistate adopted the NLC, with Indiana and New
license—physically or remotely—in any Jersey being the most recent adopters.18
state that has joined the compact. The This was a net increase of two since 2019
NLC provides standing reciprocity, with and eight since 2017. Toni Herron, the
no requirement that an emergency be education compliance officer of the
formally declared. Indiana State Board of Nursing, which
joined the compact on July 1, 2020,
Throughout much of 2020, the COVID-
said that the NLC “presents innovative
19 pandemic placed extraordinary
ways for our Indiana nurses to improve
pressure on hospitals across the country
both access to care for patients, while
as surging infections sent admissions
simultaneously reducing the regulatory
soaring. States that were members of
burden on licensees.” 19
the NLC were well positioned to bring
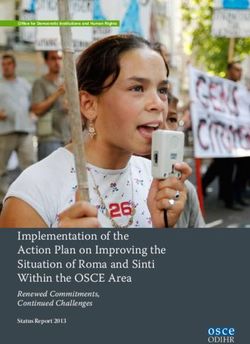
16 TFAH • tfah.orgTABLE 4: 34 States Participate in the Nurse Licensure Compact
Participants and nonparticipants, 2020
Participants Nonparticipants
Alabama Louisiana North Dakota Alaska Nevada
Arizona Maine Oklahoma California New York
Arkansas Maryland South Carolina Connecticut Ohio
Colorado Mississippi South Dakota District of Columbia Oregon
Delaware Missouri Tennessee Hawaii Pennsylvania
Florida Montana Texas Illinois Rhode Island
Georgia Nebraska Utah Massachusetts Vermont
Idaho New Hampshire Virginia Michigan Washington
Indiana New Jersey West Virginia Minnesota
Iowa New Mexico Wisconsin
Kansas North Carolina Wyoming
Kentucky
Note: Indiana and New Jersey joined the NLC in 2020.
Source: National Council of State Boards of Nursing.20
TFAH • tfah.org 17INDICATOR 2: HOSPITAL The federal Hospital Preparedness information about available beds and
Program (HPP), which is managed ICU capacity, and training healthcare
PARTICIPATION IN by the HHS Office of the Assistant workers on PPE use, treatments,
HEALTHCARE COALITIONS Secretary for Preparedness and and testing guidelines.25 During a
Response, provides cooperative pandemic, coordination across a region
agreements to states, localities, is essential to alleviate pressure on any
KEY FINDING: Widespread
and territories to develop regional single facility, to promote cooperation
hospital participation in coalitions of healthcare organizations and information sharing for supplies
healthcare coalitions was that collaborate to prepare for, and and bed availability, and to facilitate
in many cases respond to, medical training of healthcare personnel.26
common in 2017*; only surge events.21 Coalitions prepare The extent to which healthcare systems
four states (California, New members with critical tools, including leveraged the resources of their
medical equipment and supplies, coalitions during the pandemic is a
Hampshire, Ohio, and South
real-time information, enhanced subject that requires further research.
Carolina) reported 70 percent communication systems, and exercises
On average, 89 percent of hospitals
and training for healthcare personnel.22
or less of their hospitals in states belonged to a healthcare
A healthcare coalition must contain a
participated in coalitions coalition in 2017, with universal
minimum of two acute-care hospitals,
participation, meaning every hospital
supported by the HHS Hospital emergency medical services, emergency
in the state was part of a coalition, in 17
management, and public health
Preparedness Program. states (Alaska, Colorado, Connecticut,
agencies.23 Healthcare coalitions
Delaware, Hawaii, Louisiana,
invest in local capacity to prepare
Minnesota, Mississippi, Nevada, North
for and respond to events, reducing
Dakota, Oregon, Rhode Island, South
jurisdictions’ reliance on federal
Dakota, Utah, Vermont, Virginia,
medical assets during disasters.
and Washington) and the District of
Broad and meaningful participation by Columbia. (See Table 5.) However,
hospitals in healthcare coalitions means some states, such as Ohio (25 percent)
that when disaster strikes, systems are and New Hampshire (47 percent)
in place to coordinate the response, lagged behind.
freeing hospitals to focus on clinical
The pandemic exposed major gaps in
care. In the past, healthcare coalitions
healthcare preparedness, mentioned
have assisted in patient transfer,
in TFAH’s 2020 report, including
evacuations, and information sharing
coordinating surge capacity across
in events such as Hurricane Harvey
the healthcare system;27 building and
in 2017.24 More recently, the COVID-
maintaining preparedness for high-
19 pandemic presented the most
consequence infectious diseases;28
intense, widespread, and prolonged
preparedness of facilities that serve
test of U.S. hospital systems in a
people at higher risk, such as long-term
century, threatening at several points
care facilities; and lack of training and
to overwhelm facilities’ capacities.
preparedness for events in healthcare.29
Healthcare coalitions performed
Experts have also identified additional
roles such as facilitating the transport
gaps, such as pediatric surge capacity,30
of equipment and supplies, sharing
burn capacity and other specialty
18 TFAH • tfah.orgcare needed for emerging threats, *This summary reflects the latest available
and ongoing stress on the healthcare data (2017). Because these data are no
system’s ability to provide emergency longer being updated, TFAH will consider
care. While healthcare coalitions replacing this measure in future assessments.
can help address some of these
vulnerabilities, systemwide approaches
to preparedness are needed.
TABLE 5: Widespread Participation of Hospitals in
Healthcare Coalitions
Percent of hospitals participating in healthcare coalitions, 2017
States Percent of Participating Hospitals
AK, CO, CT, DC, DE, HI, LA, MN, MS, NV, ND,
100%
OR, RI, SD, UT, VT, VA, WA
ID, WI 98%
GA, WV 97%
KS 96%
AL, NE, NC, OK 95%
ME 94%
KY 93%
WY 92%
TN 91%
MI 90%
MD 89%
IL 88%
MO 87%
NY, PA 86%
MT 83%
MA, NJ 82%
AR 81%
IA, TX 80%
IN 75%
FL 73%
AZ 72%
NM 71%
CA 70%
SC 56%
NH 47%
OH 25%
Note: This indicator measures participation by hospitals in healthcare coalitions supported through the
federal Hospital Preparedness Program of the Office of the Assistant Secretary for Preparedness and
Response. The latest available data is from 2017.
Source: NHSPI analysis of data from the Office of the Assistant Secretary for Preparedness and
Response, U.S. Department of Health and Human Services.31
TFAH • tfah.org 19INDICATORS 3 AND 4: The Public Health Accreditation Board threats. The priority capabilities that
(PHAB), a nonprofit organization that the PHAB and the EMAP test include
ACCREDITATION administers the national public health identification, investigation, and
accreditation program, advances quality mitigation of health hazards; a robust
KEY FINDING: Most states are within public health departments by and competent workforce; incident,
providing a framework and a set of resource, and logistics management;
accredited by one or both of
evidence-based standards against which and communications and community-
two well-regarded bodies—the they can measure their performance. engagement plans.35,36 States sometimes
Among standards with direct relevance aim to meet applicable standards but do
Public Health Accreditation
to emergency preparedness are not pursue accreditation.
Board and the Emergency assurances of laboratory, epidemiologic,
As of December 2020, 29 states and the
Management Accreditation and environmental expertise to
District of Columbia were accredited
investigate and contain serious
Program—but eight are not by both the PHAB and the EMAP—a
public health problems, policies, and
net increase of one (Delaware and
accredited by either. procedures for urgent communications
Georgia are now accredited by the
and maintenance of an all-hazards
EMAP; Maryland transitioned from
emergency operations plan.32 Through
being accredited by both bodies to the
the process of accreditation, health
PHAB only, with the EMAP providing
departments identify their strengths
conditional accreditation) since
and weaknesses, increase their
November 2019. Nevada is once again
accountability and transparency, and
accredited by the EMAP, alongside an
improve their management processes,
additional 12 states that have received
which all promote continuous quality
accreditation from one or the other.
improvement.33
(See Table 6.) “Over the last eighteen
Emergency management, as defined months we have worked diligently
by the Emergency Management to review our processes, plans, and
Accreditation Program (EMAP), relationships,” said the director of
encompasses all organizations in a Delaware’s Emergency Management
given jurisdiction with emergency or Agency, A.J. Schall. “Over that time,
disaster functions, which may include we learned a tremendous amount and
prevention, mitigation, preparedness, modernized procedures.”37
response, and recovery. The EMAP
Just eight states (Alaska, Hawaii,
helps applicants ensure—through
Indiana, New Hampshire, South Dakota,
self-assessment, documentation, and
Texas, West Virginia, and Wyoming)
peer review—that they meet national
received no accreditation from either
standards for emergency response
body. A state without an accreditation
capabilities.34
has not necessarily been denied
The PHAB and the EMAP each provide accreditation; the state may not have
important mechanisms for improving pursued accreditation. This analysis
evaluation and accountability. includes state-level accreditations
Accreditation by these entities only, it does not include accredited
demonstrates that a state’s public local or tribal health departments. In
health and emergency management some instances, local public health
systems are capable of effectively departments have an accreditation in
responding to a range of health states that do not.
20 TFAH • tfah.orgYou can also read