2017-21 DIABETES CARE ON THE CENTRAL COAST - Central Coast Local ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

DIABETES CARE ON
THE CENTRAL COAST
2017-21
HUNTER NEW ENGLAND
AND CENTRAL COAST
An Australian Government Initiative
Acknowledgements Diabetes Advisory Group Diabetes Plan Steering Group 50 participants in diabetes planning day including staff from Central Coast Local Health District, Hunter New England and Central Coast Primary Health Network, Yerin – Eleanor Duncan Aboriginal Health Centre, Diabetes NSW, Wyong Shire, NSW Health and consumers 104 staff who completed surveys regarding diabetes care on the Central Coast Six clients, some with carers for participating in interviews about their care experiences including how care could be improved. Abbreviations ABS Australian Bureau of Statistics ACI Agency for Clinical Innovation AIHW Australian Institute of Health and Welfare CDM Chronic Disease Management CHS Central Coast Community Health Survey CKD Chronic Kidney Disease Diabetes Ad Gp Diabetes Advisory Group ED Emergency Department HEAL Healthy Eating Active Living Int Care Integrated Care LHD Central Coast Local Health District MBS Medicare Benefits Schedule NRT Nicotine Replacement Therapy PHN Hunter New England Central Coast Primary Health Network PHU Public Health Unit RACGP Royal Australian College of General Practitioners SAPHaRI Secure Analytics for Population Health Research and Intelligence Yerin Yerin – Eleanor Duncan Aboriginal Health Centre

Contents
Executive Summary
1. Diabetes – A Case for Action
2. Diabetes on the Central Coast
2.1) Diabetes and diabetes risk factors in the Central Coast Community
2.2) Diabetes in Primary Care
2.3) Diabetes Secondary and Tertiary Care
3. Diabetes Service Profile on the Central Coast
3.1) Prevention services
3.2) Primary Care services
3.3) Secondary and Tertiary Care services
4. The Central Coast Approach to Diabetes Care
4.1) Central Coast Diabetes Model of Care
5. Central Coast Diabetes Plan
5.1) Priority Areas
5.2) Actions
Diabetes Care on the Central Coast 1
Foreword
This is the first Diabetes Plan and The Central Coast Regional The specialist services provided by
Model of Care for the Central Coast Leadership Executive the Central Coast Local Health
created in partnership between the Implementation Plan to Reduce District are challenged by
Central Coast Local Health District, Childhood Obesity and Promote increasing demands for their
the Hunter New England Central Healthy Eating and Active Living services, implementing
Coast Primary Health Network and reinforces the role of sectors improvements in technology in
Eleanor Duncan Aboriginal Health outside health to reduce the rates diabetes care, and the strategic
Services, with input from of overweight and obesity among imperative to support generalists
consumers. Central Coast residents. to work at the top of their scope of
practice – in order to maximise
The Central Coast Local Health For people with diabetes, much of health outcomes for all people with
District’s previous Diabetes Plans their care occurs in the community diabetes.
have guided the development of setting with their family doctor and
services for people with diabetes a range of other health Our three organisations are
on the Central Coast. These plans professionals. Work continues to committed to working together as
have set a strong foundation for ensure person-centred care, care one system to improve the health
this new population-based and coordination, and improved health and wellbeing of the Central Coast
collaborative approach to literacy and self-management community, and to provide person-
diabetes care. happens throughout the social and centred care for people with
health care system. This approach diabetes on the Central Coast. We
The new Diabetes Plan and Model requires strengthening of look forward to showing how this is
of Care are important to address relationships at a local or regional achieved over the next five years.
the increasing rate of diabetes on level, with specialists supporting
the Central Coast – about 10 per general practitioners and other
cent of adults living in the region generalist workers so all people
have diabetes, mostly type 2 with diabetes get the care they
diabetes. need, when they need it, in a place
Dr Andrew Montague
that feels safe to them. The
Lifestyle related risk factors, Chief Executive
Primary Health Network, Yerin –
including overweight and obesity, Central Coast Local Health District
Eleanor Duncan Aboriginal Health
are major contributors to the
Centre, the Local Health District,
prevalence of type 2 diabetes. The
general practitioners and other
Central Coast Local Health District’s
community-based workers are all
Health Promotion Unit and Eleanor
stakeholders in this work.
Duncan Aboriginal Health Services Richard Nankervis
have a range of programs in place Chief Executive Officer
in the community to increase Hunter New England and Central
physical activity levels, increase Coast Primary Health Network
fruit and vegetable consumption
and ultimately, reduce levels of
overweight and obesity in children
and adults.
Belinda Field
Chief Executive Officer
Yerin Aboriginal Health Services
2
Diabetes Care on the Central Coast 3

Executive Summary
Diabetes Care on the Central Coast The guiding principles behind this The vision for diabetes care on the
2017-21 outlines the Central Coast approach are: Central Coast is for the community,
Diabetes Model of Care and Central people with diabetes, their families
Coast Diabetes Plan to be • Prevention - health promotion and carers, and health professionals
implemented over the next five programs to reduce incidence of to work collaboratively to prevent
years. risk factors of diabetes and diabetes and achieve better health
proactive care to minimise the outcomes for people with diabetes.
Diabetes has become one of the impact of diabetes and prevent
most challenging problems for complications. The Diabetes Model of Care
public health. A global epidemic, • Person-centred care and identifies key responsibilities for
the prevalence of diabetes is supporting self-management people and workers in the
increasing and affecting on health throughout the life of a person community, primary care, and
care systems worldwide. with diabetes and their carer. secondary and tertiary care
settings. The Model of Care
• Access - diabetes care to be
In Australia, the prevalence of promotes person centred care with
provided as close to home as
types 1 and 2 diabetes has risen particular consideration for high
possible.
over the last three decades1. The risk groups including Aboriginal
number of people with type 2 • Coordination and integration of
and Torres Strait Islander people(s).
diabetes is growing, most likely due diabetes care across services,
to increases in overweight and settings, technology and sectors. The Diabetes Plan consists of 13
obesity rates, poor nutrition, lack of • Equity - with particular priority areas across the
physical activity and an ageing consideration for Aboriginal and community, primary care,
population – all risk factors for type Torres Strait Islander people and secondary and tertiary settings,
2 diabetes2. other marginalised people at including early detection of
higher risk. diabetes, specialist support for
On the Central Coast, around 10% primary care, and reducing the
• Effectiveness - evidence based
of adults live with either type 1 or 2 impact of diabetes among children,
care, best practice initiatives.
diabetes or high blood glucose3. older Australians, those with
• Quality improvement –
This rise in prevalence coupled with mental health issues, and
measurement of health
complications arising from late Aboriginal and Torres Strait
behaviours, treatments and
detection and suboptimal Islander people.
outcomes, and feedback to
management of diabetes are
providers and the community.
placing significant burdens on The Central Coast Local Health
primary, secondary and tertiary District, Hunter New England
care in the region. To address this Central Coast Primary Health
concern, a Central Coast-wide, Network and Yerin – Eleanor
whole-of-population and whole-of- Duncan Aboriginal Health Centre.
system approach is required. The (in consultation with the local
Central Coast Local Health District, community and key service
Hunter New England Central Coast providers) are committed to
Primary Health Network and Yerin working collaboratively to
– Eleanor Duncan Aboriginal Health implement the Central Coast
Centre. in consultation with other Diabetes Plan and Model of Care.
service providers and consumers
have developed a coordinated and
integrated approach to diabetes
care for the Central Coast.
4
The Central Coast Local Health The Hunter New England Central Yerin – Eleanor Duncan
District is committed to: Coast Primary Health Network is Aboriginal Health Centre is
committed to: committed to:
• providing specialist services
aligned to community need, • supporting general practices to • ensuring community
• working collaboratively with effectively manage diabetes, engagement to achieve best
primary care to support the • working collaboratively with health outcomes for the
provision of integrated and secondary and tertiary care, and Aboriginal and Torres Strait
effective diabetes care, and Islander community, and
• collecting and feeding back data
• developing health promotion to general practices to enhance • demonstrating high quality care
strategies leading to a decline in the culture of demonstrable for the Aboriginal and Torres
new cases of diabetes. improvement in patient care. Strait Islander community in the
primary care setting.
These are key elements of diabetes
care on the Central Coast that will
help improve health outcomes for
the Central Coast community as a
whole, and for people with
diabetes. There are more action
areas, and more detailed activities
to be found in the body of the plan.
The partnership between the three
organisations provides the forum
for monitoring the progress of the
plan, and tracking the health
outcomes we see for the future.
Diabetes Care on the Central Coast 5
1. Diabetes – A Case for Action
Diabetes represents one of the The prevalence of type 2 diabetes Risk of type 2 diabetes is greatly
most challenging public health increases with age, and is higher in increased if people display a
problems of the 21st century4. The the Aboriginal and Torres Strait number of modifiable lifestyle
disease and its associated Islander community. According to factors. These include high blood
complications contribute the Australian Institute of Health pressure, overweight or obesity,
significantly to mortality, morbidity, and Welfare5, in 2014-15 insufficient physical activity, poor
poor quality of life of sufferers and self-reported rates of diabetes diet and extra weight carried
carers, and the cost of health care3. among 65-74 year olds were three around the waist9. In approximately
times as high than for 45-54 years 58% of cases of type 2 diabetes the
In Australia, the prevalence of olds. The ageing population in condition can be delayed or
diabetes is rising, affecting around NSW is likely to influence these prevented by reducing weight,
1.2 million people in 2014-152. In rates; the population of 65+ increasing physical activity,
New South Wales in 2016, 8.9% of years old in the state has increased improving diet and stopping
people aged 16+ were told they over the past 20 years from 12% in smoking10. With this in mind, there
had diabetes or high blood glucose 1996 to an estimated 15.3% in 2016, is opportunity to promote healthy
levels, up from 6.5% in 20023. and is projected to increase even eating and active living across
more rapidly6. organisations on the Central Coast
Although rises are seen in both
to help reduce prevalence of the
types 1 and 2 diabetes, type 2 Appropriate management of disease. This is of particular
diabetes accounts for 85% of all diabetes is essential. If left relevance on the Central Coast,
cases. Cases like these are expected undiagnosed or poorly managed, where around 60% of adults are
to rise; within 20 years, the number type 2 diabetes can lead to currently overweight or obese3.
of people in Australia living with coronary artery disease, stroke,
type 2 diabetes may increase from kidney failure, limb amputation and To help reduce diabetes prevalence
an estimated 870,000 in 2014 to blindness2. There are more than and its consequent impact on
over 2.5 million2. 4,400 amputations every year as a Australian public health services
result of diabetes, of which 85% are and systems, health promotion is
preventable if diabetes is detected important. The Diabetes Model of
early and managed appropriately7. Care and Diabetes Plan aim to
address health promoting
Diabetes is a major cause of environments and education
chronic kidney disease (CKD). among communities and health
People receiving dialysis treatment professionals.
for CKD in Australia increased by
3% from 2013 to 20148. If CKD is
detected early and managed
appropriately, the otherwise
inevitable deterioration in kidney
function can be reduced by as
much as 50% and may even be
reversible8.
6
2. Diabetes on the Central Coast
2.1 Diabetes and diabetes risk factors
in the Central Coast Community
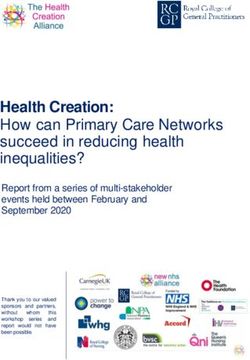
The NSW Population Health Survey (SAPHaRI) found, in the past seven
years, the percentage of persons on the Central Coast aged 16+ who were
told by a doctor or at hospital that they had diabetes or high blood glucose
levels to fluctuate around 9 to 10%3. In 2014, the estimated prevalence of
diabetes was 10.9% (7-14.7, 95% CI) and in 2016, it was 9.6% (6.9-12.3, 95%
CI). Trend lines from 2002-2016 show an overall increase in diabetes rates on
the Central Coast and in NSW, with rates on the Central Coast higher than in
NSW. (Figure 1).
Figure 1. Diabetes or high blood glucose rates for persons aged 16 years and over, Central Coast
Central Coast LHD, NSW, 2002-2016 NSW
Linear (Central Coast)
Linear (NSW)
12
10
8
PERCENT
6
4
2
0
15
10
12
14
16
05
07
09
11
13
02
04
06
08
03
20
20
20
20
20
20
20
20
20
20
20
20
20
20
20
Source: NSW Population Health Survey YEAR
(SAPHaRI). Centre for Epidemiology and
Evidence, NSW Ministry of Health
Diabetes Care on the Central Coast 7The Central Coast population has a The Central Coast Community For this report, we refer to the
high estimated population Health Survey (CHS) (Miles et al) prevalence of diabetes in Central
proportion of 16+ year olds with allows us to compare diabetes Coast adults as being 10%.
diabetes lifestyle risk factors. In rates in Gosford and Wyong. The
2016, 30.8% of 16+ year olds on the CHS (2014) estimated that 10.3% of The prevalence of type 2 diabetes
Central Coast were overweight, Central Coast adults (18+ years) increases with age, and the number
26.5% were obese, 60.2% did not had reported being told by a of people aged 65+ on the Central
do the recommended amount of doctor or at hospital that they had Coast is increasing. The ABS (2016)
physical activity, and 20.1% diabetes (approximately 26,000 estimated 20% of the Central Coast
smoked3. Over the last 10 years, people), with a slightly higher population was 65+ years old in
overweight and obesity rates have proportion of adults estimated with 2015, an increase from 18% in 20106.
increased, inadequate physical diabetes in Wyong (10.7%) than in
activity rates have levelled and Gosford (9.8%). This has increased
current smoker rates have from 7.9% in 2006. The study also
decreased. found diabetes lifestyle risk factors
higher in Wyong than Gosford
(Figure 2).
Figure 2. Diabetes and risk factors, persons aged 18 years and over, Gosford, Wyong and
Central Coast, 2014
60 Source: Central
Coast Local Health
District. Central
Coast Community
Health Survey:
50
Analysis of
Telephone Survey
2014.
Community Health
40
Survey smoking data
inconsistences due
to rounding
PERCENT
30
20
10
0
diabetes overweight obese inadequate current high blood
p.activity smoker pressure
Gosford 9.8 34 21.8 45 14.2 28.5
Wyong 10.7 33.1 29.9 49.5 14.5 31.9
Central Coast 10.3 33.8 25.7 46.7 14.7 29.7
82.2 Diabetes in Primary Care
The Hunter New England Central
Coast Primary Health Network
(PHN) offers practice support and
development to general practices
on the Central Coast. This includes
use of the practice data extraction
and analysis tool PEN/PATCAT. In
2016, 61 (57%) Central Coast
practices had data agreements
with the PHN to use this tool. For
those practices who provide
aggregated de-identified clinical
data using PEN/PATCAT, quarterly
reports are produced and provided
to general practices, benchmarking
where possible - activity with peer
group-comprising general practices
in the same remoteness area (as
identified by ABS – RA1, 2 etc). The
tool also allows for the analysis of
data to assist with population This cohort of patients includes Key observations
health and services planning. those coded as having diabetes
and those indicated by the PEN/ • From this population, 11% of
The data following is based on PATCAT tool who are likely to have people have diabetes, which is
aggregate data from 51 (48%) diabetes. Those likely to have similar to that estimated for the
practices on the Central Coast that diabetes have glycated Central Coast population
provided data extracted from PEN/ haemoglobin (HbA1c) >=6.5 or, • For people with diabetes,
PATCAT in the 6-month period to HbA1c recorded AND on an anti- the measure of blood sugar
the end of February 2017 (for more diabetic medication or, fasting control over the last 3 months,
data see Appendix 1). More than blood glucose (FBG) >7. HbA1c, was 7% or less for 56%
95% of the data summarised was of people, >7% for 29% of
provided in the January-February people, and was not recorded
2017 period. The data is for active for 15% of people
patients 18 years and over only.
• For people with diabetes,
Active patients are defined by The
31% had high blood pressure.
Royal Australian College of General
Blood pressure was not recorded
Practitioners (RACGP) and includes
for 7% of people
those patients who have visited a
• For people with diabetes,
general practice three or more
65% were overweight or obese
times within the last two years.
and for 25% of people BMI was
not available
Diabetes Care on the Central Coast 9Table 1: Summary data provided by General Practices in the Central Coast relating to
diabetes, PEN/PATCAT extracts, 6 months to Feb 2017
Gosford Wyong Central Coast
Number of general practices 57 50 107
Practices who have provided data 23 28 51
Total active patients 99394 108721 208115
Total patients with diabetes* 10482 12352 22834
Total patients with diabetes (%) 10.5 11.4 11.0
Total patients with Diabetes Type 1 (%) ** 8.4 7.3 7.7
Total patients with Diabetes Type 2 (%) 71.0 76.1 74.4
Total patients with Diabetes Other (%) 20.6 16.5 17.9
Total patients with diabetes, HbA1c > 7 (%) 28.7 29.8 29.3
Total patients with diabetes, HbA1c > 8 (%) 14.0 15.3 14.7
Total patients with diabetes, HbA1c not recorded in last 12 months (%) 16.9 13.1 14.8
Total patients with diabetes, with high blood pressure 29.1 32.7 31.1
(>140 over 90) (%)
Total patients with diabetes, blood pressure not recorded (%) 7.0 7.1 7.1
Total patients with diabetes, overweight (%) 21.6 22.1 21.8
Total patients with diabetes, obese (includes morbidly obese) (%) 39.6 46.8 43.5
Total patients with diabetes, BMI not available (%) 27.2 22.7 24.7
Total ATSI patients (%) 2.1 6.1 4.2
Total ATSI patients with diabetes (%) 9.5 7.6 8.5
* Unless otherwise specified, the term
‘patients with diabetes’ in this table refers
to the combined group of patients coded as
having diabetes and indicated as likely to
have diabetes
** Denominator for rates of diabetes types
includes patients with both Type 1 and Type
2 diabetes
10Medicare data
Medicare data gives limited ten activities completed over a 12
knowledge of activity due to a month period and a full eye check
limited number of diabetes-specific every 24 months for diabetic
Medicare Benefits Schedule (MBS) patients which can be claimed
item numbers (see Appendix 2 for every 12 months.
MBS item details). MBS items 701-
707 can be claimed for health Data in Figure 3 and 4 may indicate
assessments for seven specified an increase in service counts and
target groups, including patients practitioners performing health
aged 40-49 years who are at risk assessments. It may also indicate
of developing diabetes as assessed no increase in the number of
by the Type 2 Diabetes Risk annual cycles of care being
Assessment Tool. MBS item 715 performed and no increase in the
can be claimed for health numbers of practitioners
assessments for Aboriginal people. performing an annual cycle of care.
The diabetes annual cycle includes
2012
2013
Figure 3. Number of Medicare item health assessments and annual diabetes cycle of care, 2014
Central Coast, 2012-15 2015
12,000
10,000
8,000
Service Count
6,000
4,000
2,000
0
701 703 705 707 715 annual cycle
of care
Source: Australian Government Department
Medicare item
of Health, Medicare Benefits Schedule Data
Diabetes Care on the Central Coast 112012
2013
Figure 4. Number of GPs claiming Medicare health assessment and annual cycle of care, 2014
Central Coast, 2012-15 2015
250
200
Number of GPs’
150
100
50
0
701 703 705 707 715 annual cycle
of care
Source: Australian Government Department
of Health, Medicare Benefits Schedule Data Medicare item
122.3 Diabetes in Secondary and Tertiary care
Hospitalisations where diabetes is the main cause
There were 742 hospitalisations due to diabetes (main reason for
admission) among Central Coast residents in 2015-163. This represents a rate
of hospitalisation per 100,000 population per year of 225 for males (432
admissions) and 162 for females (310 admissions). The same rates for NSW
in 2015-16 were 168 per 100,000 for males and 133 per 100,000 for females.
Figure 5 shows the Central Coast rates for persons with diabetes as a
principal diagnosis were above the state average.
Figure 5. Diabetes as a principal diagnosis, hospitalisations, Central Coast LHD, NSW
2010-11 to 2015-16
250 Central Coast
NSW
200
Rate per 100,000 population
150
100
50
0
2010-11 2011-12 2012-13 2013-14 2014-15 2015-16
Source: NSW Combined Admitted Patient Epidemiology Data and ABS population estimates (SAPHaRI).
Centre for Epidemiology and Evidence, NSW Ministry of Health. Accessed 4.9.17
Diabetes Care on the Central Coast 13Amputations due to diabetes
From 2012 to 2016, among Central Coast residents and due to diabetes, there were on average, per year:
• 11 below knee amputations
• 62 toe/foot/ankle amputations, and
• 6 above knee amputations.
The rates of amputations were about 16%, 16%, and 37% higher than the state average for below knee, toe/foot/ankle,
and above knee amputations respectively (though not statistically significantly different, as some of these numbers
are relatively small).
Figure 6. Amputations due to diabetes, hospitalisations by site of amputation: Below the
knee, Comparison by LHD, NSW, 2013-16
5
Rate per 100,000 population
4.5
4
3.5
3
2.5
2
1.5
1
0.5
0
s
t
ey
t
ee
ey
W
s
ey
ey
W
en
d
W
ey
as
as
ain
HD
an
NS
NS
dn
NS
dn
dg
dn
dn
dn
av
Co
Co
nt
gl
lL
lh
Sy
Sy
Sy
Sy
bi
Sy
n
En
rn
rn
ou
rth
al
Al
oa
m
er
he
r
rn
te
rn
rn
n
M
nt
ru
w
rth
No
Sh
er
es
e
te
te
ut
Ne
Ce
ue
ur
st
rth
No
W
es
es
ra
So
id
Ea
M
Bl
W
W
er
No
ar
M
an
h
nt
w
h
ut
Illa
Hu
ut
pe
So
So
Ne
Figure 7. Amputations due to diabetes, hospitalisations by site of amputation: Toe/foot/
ankle, Comparison by LHD, NSW 2013-2016
20
Rate per 100,000 population
18
16
14
12
10
8
6
4
2
0
s
t
ey
t
ee
ey
W
s
ey
ey
W
en
d
W
ey
as
as
ain
HD
an
NS
NS
dn
NS
dn
dg
dn
dn
dn
av
Co
Co
nt
gl
lL
lh
Sy
Sy
Sy
Sy
bi
Sy
n
En
rn
rn
ou
rth
al
Al
oa
m
er
he
r
rn
te
rn
rn
n
M
nt
ru
w
rth
No
Sh
er
es
e
te
te
ut
Ne
Ce
ue
ur
st
rth
No
W
es
es
ra
So
id
Ea
M
Bl
W
W
er
No
ar
M
an
h
nt
w
h
ut
Illa
Hu
ut
pe
So
So
Ne
Source: NSW Combined Admitted Patient Epidemiology Data and ABS population estimates (SAPHaRI).
Centre for Epidemiology and Evidence, NSW Ministry of Health. Accessed 4.9.17
143. Diabetes Service Profile on the Central Coast
3.1 Prevention services
There are many organisations on Healthy Eating Active Living: the Other organisations involved in and
the Central Coast that implement health promotion service has a supporting health promotion
strategies to address the lifestyle strong commitment to promoting initiatives include PHN, Yerin –
risk factors for diabetes and other healthy eating and active living Eleanor Duncan Aboriginal Health
chronic diseases. Examples include across the Central Coast Centre, CC Council, NSW
implementing health promotion community. There is enhanced Department of Education and
policies and practices in the focus on achieving the NSW Communities, Broken Bay Diocese
workplace (no smoking worksite Premier’s Priority (2015) of Catholic Education Commission,
and Nicotine Replacement Therapy reducing overweight and obesity Association of Independent
(NRT) for those attempting to quit, rates in children by 5% over 10 Schools, NSW Ministry of Health,
healthy food at staff cafeteria), years. The Central Coast Healthy Office of Preventive Health, Healthy
providing structural support for Eating & Active Living (HEAL) Kids Association, CC Primary
good health (Council shared Delivery Plan also addresses adult School Principals and teachers,
pathways) and running programs overweight and obesity at a local Central Coast School Education
that encourage good health level and supports the NSW HEAL Region, early childhood education
(exercise classes for older adults). Strategy 2013-2018. Key actions and care services, TAFE NSW, Early
include: Childhood Training and Resource
The Central Coast Local Health Centre, WorkCover (Gosford), NSW
District (LHD) Health Promotion • Develop, implement and Business Chamber (CC), Local
Service is a key service using a evaluate a Central Coast HEAL Chambers of Commerce, private
population health approach and Delivery Plan that engages and gyms and pools, walking groups,
working in partnership with others mobilises relevant stakeholders Cancer Council NSW, Heart
to improve the health of the across sectors. Foundation NSW, Diabetes NSW.
Central Coast community. • Continue the tailored local
delivery of state-wide programs
Work led by the Health Promotion
and supporting strategies that
Service to address chronic disease
promote healthy eating and
risk factors includes:
active living for children and
adults, such as Munch and Move,
Live Life Well at School, Go4Fun
and referral to the Get Healthy
Service.
• Continue advocacy for health
promoting environments by
working with planning agencies
to ensure population health is
prioritised.
• Integrate and emphasise
physical activity in all
appropriate projects.
Diabetes Care on the Central Coast 153.2 Primary Care services
General Practices
In 2016 the Central Coast had an estimated population of 333,11912. There were approximately 447 GPs,
with a total full service equivalent (37.5 working hours per week) of 281 across 106 general practices (PHN).
In 2015, the rate of supply of general practitioners in Australia was 114 per 100,00013 based on full-time
equivalent defined as working 40 hours per week. Central Coast has less than the national average of GPs
per 100,000 population.
In 2016 there were approximately 228 Practice Nurses on the Central Coast working in 73 general practices
(PHN).
Table 2. General Practice’s in Gosford, Wyong and Central Coast, 2016
Central
Gosford Wyong Coast
General Practices 54 52 106
GP total 237 210 447
GP full service equivalent 163.5 117.5 281
GP FSE per 100,000 population 94 73.8
Registrar 29 12 41
Source: Estimates from HNECC PHN ChilliDB workforce data, Nov 2016
Note: GP hours are missing from two practices in Gosford and seven in Wyong so number FSE hours and FSE per 100,000 would be higher, provided by
HNECC PHN
Preliminary GP and Registrar numbers only. Headcounts only, does not account for GPs or Registrars who may work in more than one general practice
Allied Health Services
Allied Health information was most recently collated by Central Coast Medicare Local in mid-2015 and should be
used with caution. Allied Health professionals employed at LHD and Gosford Private Hospital are not included here.
Data gives an indication of relative workforces in 2015.
Table 3: Allied Health professionals in private practice and service in Gosford, Wyong and Central Coast, 2015
Central
Health Professionals /Services Gosford Wyong Coast
Podiatrists 41 38 79
Pharmacies 36 37 73
Pharmacists 63 58 121
Diabetes Educators 3
Dietitians 26
Exercise physiologists 29
Source: Information from CC Medicare Local collected in mid-2015 and no longer updated
16Yerin – Eleanor Duncan Aboriginal Hunter New England Central Coast Primary Health Network
Health Centre
The PHN is a not-for-profit • PENCAT feedback to practices;
Yerin – Eleanor Duncan Aboriginal organisation funded by the summary of practice activity and
Health Centre. (Yerin) is a Commonwealth Government to patient outcomes provided to
community controlled integrated improve the efficiency and practices to assist with
primary health care service located effectiveness of the primary health identifying areas of need
at Wyong and Gosford on the NSW care system. • Hunter Alliance Diabetes
Central Coast, Darkinyung country. Integration Project; high risk
Yerin – Eleanor Duncan Aboriginal The PHN works in collaboration
diabetes patients attend a case
Health Centre is the only with its partners and stakeholders
conference at the GP practice
community controlled Aboriginal to deliver better health outcomes.
with at least a GP, practice nurse,
Health Service on the Central Diabetes management forms part
endocrinologist and diabetes
Coast. Services provided in relation of this vision. Key initiatives
educator in attendance.
to diabetes include: currently in place that support
Education for GPs and practice
diabetes management and care
nurses also takes place. Six and
• clinical services by GPs, practice coordination include:
12 month outcomes are
nurses and Aboriginal health
favourable and a similar project
practitioners, • HealthPathways; an online
is being considered for piloting
health information portal for GPs
• a Medical Outreach Indigenous on the Central Coast.
and other primary health
Chronic Disease Program which
clinicians
comprises of monthly services
including a visiting • Patient Info; a website with
endocrinologist, diabetes trusted health information likely
educator, podiatrist and dietitian, to be helpful for patients with
diagnosed conditions
• an optometrist visiting one other
day a fortnight, • Practice Support and
Development; this team provides
• an Integrated Team Care service
direct support to general
that assists clients with chronic
practices in areas such as
health issues to receive the
Practice Management,
health care they need, such as
Education/Professional
organising doctors’
Development, Digital Health,
appointments, transport to and
Quality Improvement/
from appointments, following up
Accreditation, Chronic Disease
with clients on their health plan,
Management, Preventative
etc.
Health, Workforce Support,
Immunisation, Practice data
extraction and analysis
• Better health care planning for
our region
• Practice data analysis; collective
de-identified practice data
analysed to assist with
identifying area needs, service
gaps and enhance service
provision
Diabetes Care on the Central Coast 173.3 Secondary and Tertiary Care services
Members of the LHD diabetes specialist team include:
• 1.5 FTE LHD endocrinologists, approximately 50% of time diabetes related
• 7 FTE LHD diabetes educators
• 2.2 FTE LHD dieticians diabetes related
• 8.2 FTE LHD podiatrists, approximately 90% of time diabetes-related
In total there are seven endocrinologists working publicly and/or privately on the Central Coast.
Private allied health professionals have been included under Primary Care Services.
A summary of LHD services available for diabetes clients is presented in Table 4.
Table 4. Diabetes services available for diabetes clients
Diabetes services Endo D Ed Diet SW Pod
Inpatient services x x x X x
Paediatric Outpatient Appointments Paed Endo x x x
Paediatric Diabetes Clinic Paed Endo X X x
Team T1 Adolescent Insulin Adj and CHO Count x x
Paediatric School visits x
Antenatal Endocrine Clinic x x x
GDM Group X x
Antenatal Insulin Stabilisation Program x
Young Persons Transition Clinic X X X x
Insulin Stabilisation Program x
Type 1 Group x x
Type 2 Group x x
Adult Outpatients Appointments x x x x
DM Outpatient Clinic; DEd and Diet x x
DM Outpatient Clinic; Diet only x
T1 Insulin Pump Clinic x x x x
Continuous Glucose Monitoring Service Clinic x x
Complications Clinic x x x x
Foot Wound Clinic x
Diabetes Foot Assessment Clinic x
High Risk Foot Clinic x
48 hr follow up x
Home Visits x
External Education x
Staff Diabetes Education x
National Aborigines and Islanders Day x x x x x
Observance Committee (NAIDOC)
18Additional diabetes related
LHD services
Nunyara Aboriginal Health Unit
provides a range of health services
for Aboriginal and Torres Strait
Islander people. The Chronic Care
Manager and CNS Chronic Care for
Aboriginal People implement the
Chronic Care program which
includes but is not limited to
following up patients who have
been admitted to hospital and
identified as having one or more
chronic disease/s, and coordinating
an annual NAIDOC celebration
including an extensive health
check.
The Chronic Care self-management
program consists of community
voluntary leaders running the
Stanford Better Health
Management Program at various
Central Coast locations for
community members with chronic
disease/s.
Ongoing and Complex Care
supports a CNS2 within Diabetes
for Chronic Disease Management
(CDM). Diabetes is one of five of
the targeted diagnostic areas for
the selection of CDM patients.
These complex patients may be
offered case management or
coaching within the work of care
coordination and complex care.
Diabetes Care on the Central Coast 194. The Central Coast Approach to Diabetes Care
The vision for diabetes care on the The LHD, PHN and Yerin – Eleanor A proposed Diabetes Model of
Central Coast is for the community, Duncan Aboriginal Health Centre in Care to be adopted and a Diabetes
consumers and health professionals consultation with other service Plan to be implemented over the
to work collaboratively to prevent providers and consumers have next five years have been
diabetes and achieve better health worked collaboratively to develop a developed. Both the model and
outcomes for those with diabetes. coordinated and integrated plan range from diabetes
approach to diabetes care. The prevention through to
The incidence of diabetes and planning process identified service management of complications in
diabetes risk factors is high and gaps and opportunities, and the community through to the
increasing. A Central Coast wide, consumer and community needs. tertiary setting.
whole-of-population and whole-of- The Australian National Diabetes
care approach is required to Strategy 2016-202014 was used as
address this concern. a framework to develop this local
plan. Other regional, state and
international approaches have also
been considered15-20.
4.1 Central Coast Diabetes Model of Care
The proposed Central Coast The model promotes:
Diabetes Model of Care (graphic
follows) provides a framework for a • Consumer centred care with • Secondary and tertiary setting;
coordinated and integrated particular consideration for diabetes specialists provide care
approach to diabetes prevention Aboriginal and Torres Strait and for complex diabetes and
and management to achieve better other marginalised people to support to primay care
health outcomes for our reduce inequalities in care. providers.
community. The model includes • Community setting; prevention • Further development and
key elements of care in the and health promotion to implementation of this Model of
community, primary care, and improve the health of the whole Care falls within the scope of this
secondary and tertiary care community and may focus on plan.
settings and acknowledges that identified target groups. • This model acknowledges that
care overlaps between settings. • Primary care setting; general there is variability among
practice has the central role in practitioners and a need for
diabetes identification and some flexibility; some GPs may
management. Specialists assist wish to extend their role into
with complex diabetes and more complex care, others may
provide health professional need greater support for their
education updates. Primary patients.
Health Network provide regional
and practice specific data
analysis and support practice
development.
20Diabetes
Model of Care
Community Setting
1. Prevention and Health Promotion
a. Building healthy public policy
b. Supportive environments
c. Promoting healthy lifestyle
d. Partnership and planning with services,
organisations, consumers and communities
2. Consumer and community
engagement: Across all settings
3. Reduction of health inequalities:
Primary Care Setting
Target Aboriginal & Torres Strait
4. Primary Care: General health and wellbeing Islander people and other
marginalised people
5. Primary Care relating specifically to
diabetes: “The Necessary Nine”
Secondary & Tertiary
a. Screening
Care Setting
b. Prevention
c. Regular reviews / surveillance 7. Complex Care: “The Super Seven”
d. Prescribing a. In-patient care
e. Insulin b. Insulin pumps
f. Patient & carer self-management c. End stage renal
education d. High risk foot
g. Cardiovascular e. Children/ adolescents
h. Housebound / care homes f. Pregnancy
i. Outcomes / audit g. Type 1 / rare / complex / unstable
6. Specialist support for Primary Care
Adapted from: Leicestershire Clinical Commissioning Groups
Diabetes Care on the Central Coast 215. Central Coast Diabetes Plan
The Central Coast Diabetes Plan
Priority Areas
(pp 23-40) identifies 13 priority
areas across the community, All Settings
primary care, secondary and 1 Enhance consumer involvement
tertiary settings.
2 Align workforce capacity with community need
Priority areas across all settings 3 Further develop and enhance utility of information and
include enhanced consumer communication technology
involvement, aligning workforce
capacity with community need, Community Setting
and use of information and 4 Promote healthy eating and active living across the Central Coast
communication technology. These
Primary Care Setting
are essential for coordinated,
integrated and best practice 5 Maximise the early detection of diabetes
diabetes care. 6 Strengthen primary care management of diabetes and local care
pathways
Prevention and health promotion
priority areas include promoting 7 Implement a consistent approach to patients diabetes education and
healthy living and active living in self-management
the community.
8 Strengthen and expand specialist support for Primary Care
Early detection and optimal 9 Reduce the impact of diabetes among Aboriginal and Torres Strait
diabetes management takes place Islander people
predominantly in general practice
Secondary and Tertiary Care Setting
with support from diabetes
specialists. Priority actions focus on 10 Further develop and enhance diabetes services to better outcomes
early detection, self-management, for people with newly diagnosed or complex diabetes
marginalised and priority groups, 11 Reduce the impact of diabetes among Aboriginal and Torres Strait
and best practice diabetes Islander people
management.
12 Reduce the impact of pre-existing and gestational diabetes in
Enhanced services are provided by pregnancy
the diabetes specialist team to 13 Reduce the impact of diabetes among children with diabetes, older
manage complex diabetes, support Australians, and those with mental health and wellbeing issues
general practices to manage
complex patients and to provide
education updates to health
professionals.
225.2 Actions
All Settings
LHD, PHN and Yerin – Eleanor Duncan Aboriginal Health Centre will work collaboratively to provide evidence-based,
comprehensive, accessible, efficient and coordinated diabetes prevention and management services for all people on
the Central Coast reflective of community need.
Key Priority Area 1: Enhance consumer involvement
Service
Actions Performance Indicators Responsible Timeframe
1.1 Engage existing avenues for Meetings with:
consumer involvement in identifying
CCLHD Community Diabetes Mar 2017,
gaps, health planning and service
Engagement Committee Advisory Group ongoing
delivery including PHN and LHD
Clinical Councils, PHN Central Coast CCLHD Clinical Council Jul 2017
Community Advisory Committee, HNECCPHN Clinical Council Oct 2017
LHD Consumer and Community
HNECCPHN Community Aug 2017
Engagement Committee, PHN and
Engagement Committee
LHD Collaboration Unit GP Panel,
Yerin – Eleanor Duncan Aboriginal CC GP Collaboration Unit Ongoing
Health Centre’s men’s and women’s – GP Panel
groups.
Yerin – Eleanor Duncan Aboriginal Ongoing
Health Centre’s men’s and
women’s groups
1.2 Identify and implement best (a) Consumer(s) on Diabetes Diabetes Jun 2017, ongoing
consumer feedback mechanisms for Advisory Group Advisory Group
diabetes services and programs
(b) ACI Patient Journey LHD Public Oct 2017
including but not limited to:
– Diabetes Education Centre Health/Int Care
(a) consumers on Diabetes
(b) Existing service evaluation/ Ongoing
Advisory Group
feedback Service managers
(b) feedback from people attending in each
diabetes services organisation
(c) CCLHD survey and report, Oct 2017
(c) survey LHD employees with with recommendations LHD Public
diabetes and those with family / Health/Int Care/
friends with diabetes Yerin – Eleanor
Duncan Aboriginal
Health Centre
Diabetes Care on the Central Coast 23Key Priority Area 2: Align workforce capacity with community need
Service
Actions Performance Indicators Responsible Timeframe
2.1 Analysis of service use data, Population need identified and LHD Planning/ 2017-18
population health data, best reported Public Health/
practice guidelines to define/ Performance,
estimate community need. PHN, Yerin –
Eleanor Duncan
Aboriginal Health
Centre
2.2 Determine workforce capacity, Workforce capacity report LHD Workforce/ 2017-18
and how they relate to the Central Planning/Public
Coast population’s needs – across Health, Diabetes
LHD, PHN, General Practice and Services, Yerin –
Yerin – Eleanor Duncan Aboriginal Eleanor Duncan
Health Centre’s range of health Aboriginal Health
workers Centre, PHN
2.3 Identify areas of need and Workforce analysis report and Workforce/ 2018
actions required for the Central recommendations Planning/Public
Coast health workforce, including Health/Diabetes
but not limited to diabetes Services, PHN,
education for health workers in Yerin – Eleanor
hospital and community settings; Duncan Aboriginal
clinical care options for people with Health Centre
type 1 and type 2 diabetes, and
higher risk populations. Identify the
types of skills, and workforce
required to deliver the Diabetes
Model of Care for the Central Coast
population.
2.4 Explore options to increase (a) private providers included (a) PHN, LHD 2018
access to diabetes services in the in HealthPathways
community, e.g. community health,
(b) roles of private providers (b) PHN
community pharmacies, private
identified and supported
allied health providers.
24Key Priority Area 3: Further develop and enhance utility of information and communication technology
Service
Actions Performance Indicators Responsible Timeframe
3.1 Fully utilise existing information Strategies implemented and
and communication systems such as activity monitored
eMR, CHOC, ComCare, Argus, MHR
and PENCAT to deliver better clinical
and operational performance and
support improved patient outcomes
and experience
(a) Develop ComCare to receive and (a) ComCare receives electronic (a) External TBA
send messages directly from and to faxes. Receiving and sending out provider/LHD
primary care via secure messaging Argus messages in development. ComCare
(Argus)
(b) ComCare to use patient (b) Exists for new patients. (b) Ongoing
demographic data from eMR Else manual updates
(c) Enable patients notes to be (c) Functionality now in place (c) LHD ComCare/ July 2017
shared between CHOC, ComCare eMR support
and eMR teams
(d) Investigate the possibility to (d) Assess functionality of Audit 4, (d) LHD Diabetes 2018
enable interface between Audit 4 connectivity services
and CHOC, ComCare and eMR
(e) eMR referral to Diabetes (e) Feasible. For consideration. (e) LHD ComCare/ Dec 2017
Educator (via ComCare) eMR teams
(f) Pilot GPs sending health (f) Feasible. In progress. (f) LHD Int Care 2018
summaries directly to ED
(g) Investigate the possibility for the (g) Functional requirements (g) LHD Diabetes 2018/19
Citrix platform to enable software to be determined. services, NSW
changes rather than making changes Health State wide
to individual computers. service desk
(h) Discharge summaries from (h) Update from Obstetrix (h) LHD Dec 2017
maternity to GPs eMaternity
(i) Discharge summaries from (i) Update from relevant working (i) LHD eMR team 2019
hospital to residential aged care group
facilities
(j) Promote use of My Health (j) Request update from PHN (j) PHN 2018
Records
(k) SMS to patients for (i) (k) (i) Feasible. (k) LHD ComCare/ k.i) 2018
appointment reminders and (ii) For implementation. eMR teams
capacity to respond
(k) (ii) Assess feasibility k.ii) 2019
Diabetes Care on the Central Coast 25Service
Actions Performance Indicators Responsible Timeframe
3.2 Investigation and investment Emerging technologies LHD IT, PHN
into emerging technologies identified and implemented
including but not limited to (a) 3D
(a) For review (a) LHD Podiatry 2020
scanning and printing for diabetes
wound orthoses, (b) electronic (b) patient portal – not yet (b) LHD ComCare 2020/21
appointment system for patients, available
(c) e-referrals (Argus), (d) (c) feasible – review business (c) LHD 2018
telehealth (e) use of apps (f) social model
media. Modifications also required
(d) feasibility on Central Coast, (d) PHN 2018/19
to better support Model of Care.
MBS item nos
(e) assess functionality of apps (e) LHD Diabetes 2019
Services
26Community Setting
A population approach is used to prevent people developing type 2 diabetes. Programs are aimed at targeted
populations rather than individuals and are delivered in partnership with other services, organisations and
communities. Working in partnership ensures that health promotion practices are embedded into other settings,
other professionals are up skilled in health promotion and programs are subsequently more sustainable. There is
enhanced focus on achieving the NSW Premier’s Priority (2015) of reducing overweight and obesity rates in children
by 5% over 10 years.
Key Priority Area 4: Promote healthy eating and active living
Service
Actions Performance Indicators Responsible Timeframe
4.1 With Dept. Premier and Cabinet, Sub-committee had first meeting LHD Health 2017 - 2025
lead on the development of a June 2017. Promotion, Dept.
whole-of-government regional Premier and
Cross-agency action plan
approach to address childhood Cabinet
completed and agreed upon at
overweight and obesity on the
June 2017 meeting. For annual
Central Coast. Establish Central
progress report to NSW Health.
Coast Regional Leadership
Executive Sub-committee for cross-
agency collaboration on reducing
obesity and promoting healthy
eating and active living. Develop
cross-agency action plan to address
childhood overweight and obesity
in the region
4.2 Enhanced focus on tailored local LHD Health Ongoing
delivery of state-wide programs Promotion reports
promoting healthy eating and on each of these
active living in early childcare programs
settings, schools, community sports, quarterly to NSW
workplaces and community settings Health
(a) foster healthy habits in children (a) Support provided to, and
and young people at school ‘uptake measures’ for 79 primary
schools, 29 high schools
(b) provide a supportive (b) Measures of capacity for 127
environment for healthy eating, early childhood education and
physical activity and reducing small care services
screen recreation for children in
early childcare settings
(c) increase referrals to Get Healthy (c) Annual report provided to LHD
Service and Go4Fun for Get Healthy Service (including
tailored Type 2 Diabetes
Prevention program and Get
Healthy in Pregnancy) including
number of referrals, weight loss
and waist circumference. Target
for 2017-18, 383 referrals by Health
Professionals; target for 2017-18
Go4Fun to deliver 12 programs
Diabetes Care on the Central Coast 27Service
Actions Performance Indicators Responsible Timeframe
4.3 Advocate for health promoting Develop planning strategies LHD Health Ongoing
environments and provide for safe walking, cycling, public Promotion/Public
submissions to planning agencies transport and chilled water Health Unit
and development processes to stations
ensure population health is
Implement healthier food and
prioritised. Promote environments
drink policy initiative for staff and LHD 2017, ongoing
that support healthy eating and
visitors in NSW Health facilities.
active living.
28Primary Care Setting
Around one in five adults with diabetes do not know they have the condition21. If left undiagnosed or poorly
managed, diabetes can lead to coronary artery disease, stroke, kidney failure, limb amputations and blindness. Early
detection and optimal management of diabetes can improve access to necessary care and reduce complications,
improving quality of life among people with diabetes and reduce the escalating burden on health resources. General
practice has the central role in type 2 diabetes management across the spectrum, from identifying those at risk right
through to caring for patients at the end of life2, and is supported by specialty services.
Key Priority Area 5: Maximise the early detection of diabetes
Service
Actions Performance Indicators Responsible Timeframe
5.1 Address risk factors for disease, (c) Annual report provided to LHD LHD Health 2017, ongoing
in the whole population and for for Get Healthy Service including Promotion
people with diabetes by extended referrals and weight loss and waist
promotion of Get Healthy Service circumference. Target for 2017-18,
utilisation to health professionals 383 referrals by Health
Professionals
5.2 Promote strategies aimed at
screening and early detection of
people at risk of developing
diabetes
(a) implementation, evaluation and (a) ‘Over 40? Check Your Risk!’ LHD Health 2017-18
review the diabetes prevention implemented Promotion/Public
campaign, ‘Over 40? Check Your Health, PHN, Yerin
# hits on Health Promotion Check
Risk!’ (a program that includes – Eleanor Duncan
Your Risk site
education about diabetes risk Aboriginal Health
factors and the promotion of # Health Assessments (MBS) via Centre 2018
diabetes screening by GPs) PENCAT/MBS
(b) Assess feasibility of trial to Review with recommendations
LHD Public
undertake BSL on every patient to (b) Brief report on feasibility, 2018-19
Health/Health
ED or admitted to hospital, expected outcomes and Promotion
including impact for services recommendations
providing follow-up and benefits LHD Diabetes
Advisory Group
Diabetes Care on the Central Coast 29Key Priority Area 6: Strengthen primary care management and local care pathways
Service
Actions Performance Indicators Responsible Timeframe
6.1 Build on the Diabetes Model of GP and practice nurse education – Diabetes Advisory May18 ongoing
Care (from this plan) to consolidate annual forum Group, PHN
roles and responsibilities of primary
Range of HealthPathways exist PHN Ongoing
care providers, and implement
for diabetes care
strategies to support primary care
Number of times accessed,
providers. Including education for
unique users
general practitioners and practice
nurses, use of care guidelines Review of pathways every 2 years PHN Ongoing
(HealthPathways), referral pathways Develop mechanisms to monitor PHN/Diabetes 2019-20
and options to access diabetes referrals, specialist feedback and Advisory Group
specialist advice and transition GP feedback, appropriateness
services.
6.2 Support quality improvement
processes in general practice,
including mechanisms for primary
care providers to use their clinical
data to compare with peers and
care guidelines.
(a) PHN practice support team to (a) Number of practices receiving PHN Annually
provide clinical data feedback to clinical feedback report
GPs % of GPs/patients achieving care PHN Annually
guidelines
(b) PHN assisting/ training GPs to (b) Number of practices using PHN Annually
use clinical software to generate recall/reminders
recalls and reminders, pro-actively Number of practices prioritising PHN Annually
manage people with complex issues complex cases
30Key Priority Area 7: Implement a consistent approach to diabetes education and self-management
Service
Actions Performance Indicators Responsible Timeframe
7.1 Continue to implement and Number of Stanford program LHD Chronic Care Annually
promote the various health self- attendees with diabetes Self Management
management and support
Get Healthy Service Diabetes – LHD Health Annually
programs offered on the Central
activity report Promotion
Coast including but not limited to
the Stanford Better Health LHD Diabetes and Nutrition LHD Diabetes Annually
Management program offered by education Services/Nutrition
LHD and run by community Services
volunteers, Get Healthy Service Other peer support programs, LHD,PHN,Yerin – Annually
Diabetes offered by NSW Health, including Diabetes NSW Eleanor Duncan
peer support programs run by volunteers and community led Aboriginal Health
Diabetes NSW volunteers, Aunty groups Centre, Diabetes
Jean’s Chronic Disease Outreach NSW, CC Primary
Program run by CCPC, Integrated Care
Team Care program run by Yerin –
Diabetes Advisory
Eleanor Duncan Aboriginal Health
Group
Centre, and web-based patient
education and self-management
programs, e.g. patientinfo
7.2 Ensure education is provided to (a) Survey general practices and PHN 2017
patients and their carer (where private allied health providers re
applicable) in a form that is roles, perceived needs
accessible and relevant to individual
(b) Survey community nurses as LHD, PHN 2017
goals. Review the capacity of
above
community nurses, practice nurses,
Aboriginal Health workers/ (c) Incorporate these findings into Diabetes Services, 2018
Practitioners and GPs and what delivery of diabetes education on PHN
roles they have in providing and Central Coast
reinforcing diabetes education and
key messages, including people
newly diagnosed and after hours
services.
Consider redistributing some
aspects of diabetes education to
different roles. This may assist
credentialed diabetes educators
taking on expanded roles in
diabetes management, e.g. insulin
stabilisation.
Diabetes Care on the Central Coast 31Key Priority Area 8: Strengthen and expand specialist support for Primary Care
Service
Actions Performance Indicators Responsible Timeframe
8.1 Provide education and support (a) Needs assessment of general PHN 2018
for general practice to deliver the practice in relation to ‘Necessary
Model of Care. Nine’ functions within the Model of
Care
(b) Content and locality targeted PHN, LHD, Yerin – 2017-18 and
education and specialist support Eleanor Duncan ongoing
(diabetes educators, Aboriginal Health
endocrinologists) Centre
8.2 Develop mechanisms for GPs to
access specialist support for their
patients and carers
(a) telephone advice for immediate (a) Implementation/promotion LHD, PHN Oct 2017
issues of telephone advice
(b) review GP needs for outpatient (b,c) LHD Outpatient clinic options LHD 2018
clinic support in terms of timeliness to be informed by GP needs
and nature of consultations as part assessment (10.3)
of needs assessment (10.3)
(c) incorporate GP needs into types
and timing of outpatient clinics
(d) GP, endocrinologist, diabetes (d) Trial with 3 practices on LHD, PHN, Yerin – 2018/19
educator shared consultation in the Central Coast (10.1) Eleanor Duncan
general practice setting (Hunter Aboriginal Health
(e) Monitor appropriateness 2018
model) (10.1) Centre
of referrals
LHD, PHN
8.3 Develop strategies to support Business case for case PHN 2018
GPs caring for young people with conferencing/telehealth
Type 1 diabetes. Involves GP,
Service model developed PHN, LHD 2018-19
paediatric endocrinologist,
and trialled
paediatrician, endocrinologist,
diabetes educator, practice nurse. Monitor person, carer, health PHN 2018-19
Consider shared care arrangements, worker experience of care
telehealth, case conferencing,
integrated care model (13.1)
32You can also read