Utilization of Public Health Financing in Uganda's Primary Health Care Program
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Utilization of Public Health Financing in Uganda’s Primary Health Care Program
Mailing Address
PO Box 7404
Kampala, Uganda
Street Address
Ntinda Complex
2nd Floor, Block B, Plot 33
Ntinda Road
PO Box 7062
Kampala, Uganda
www.path.org
© 2021 PATH. All rights reserved.
Kisaame EK. Utilization of Public Health Financing in Uganda’s Primary Health Care Program.
Kampala, Uganda: PATH; 2021.
March 2021
iiContents
Objectives of the study ......................................................................................................................... 7
Data collection ....................................................................................................................................... 9
Key informant interviews ..................................................................................................................... 9
Data management and analysis .......................................................................................................... 9
Limitations of the study ...................................................................................................................... 10
PHC expenditure at local government and health care facility levels ........................................... 12
Performance in non-wage and development grants ....................................................................... 13
Adherence to PHC grant utilization guidelines ................................................................................ 15
Procurement using PHC funds .......................................................................................................... 16
Functionality of health unit management committees .................................................................... 18
Functionality of the village health teams .......................................................................................... 20
Utilization of other PHC resources (results-based financing)........................................................ 21
Annex 1. Detailed breakdown of primary health care grants to the local governments in the
study 29
ABBREVIATIONS .................................................................................................................................. 3
EXECUTIVE SUMMARY ........................................................................................................................ 4
INTRODUCTION ..................................................................................................................................... 6
Objectives of the study ............................................................................................................................ 7
APPROACH AND METHODOLOGY ..................................................................................................... 8
Data collection ......................................................................................................................................... 9
Key informant interviews ......................................................................................................................... 9
Data management and analysis ............................................................................................................. 9
Limitations of the study ......................................................................................................................... 10
1OVERVIEW OF HEALTH SECTOR EXPENDITURE .......................................................................... 11
PHC expenditure at local government and health care facility levels ................................................... 12
Performance in non-wage and development grants ............................................................................. 13
USE OF PHC FUNDS AT LOCAL GOVERNMENT AND FACILITY LEVELS ................................... 15
Adherence to PHC grant utilization guidelines...................................................................................... 15
Procurement using PHC funds.............................................................................................................. 16
Functionality of health unit management committees ........................................................................... 18
Functionality of the village health teams ............................................................................................... 20
Utilization of other PHC resources (results-based financing) ............................................................... 21
EFFECTS OF COVID-19 ON HEALTH SECTOR AND PHC EXPENDITURE .................................... 25
CONCLUSIONS AND RECOMMENDATIONS .................................................................................... 27
ANNEXES ............................................................................................................................................. 29
Annex 1. Detailed breakdown of primary health care grants among the local governments in the study
..................................................................................................................................................... 29
REFERENCES ..................................................................................................................................... 31
2Abbreviations
COVID-19 coronavirus disease 2019
DHT district health teams
EMHS essential medicines and health supplies
FY financial/fiscal year
HUMC health unit management committee
KII key informant interview
MoFPED Ministry of Finance, Planning and Economic Development
MoH Ministry of Health
PHC primary health care
RBF results-based financing
UGX Uganda shilling
VHT village health team
WHO World Health Organization
3Executive summary
Primary health care (PHC) provision around the world has been constrained by many challenges—
perhaps none greater than limited financing. Recognizing the gaps in health coverage, in 2019, the
World Health Organization recommended that countries increase spending on PHC by allocating at
least 1% more of their gross domestic product to PHC; this would enable the world to meet the health
coverage targets set out in the Sustainable Development Goals. However, the gap between basic
community health needs and PHC provision has persisted. In some cases, the gap has increased
despite increases in PHC resources—especially in low- and middle-income countries.
The limited financing that characterizes PHC provision in low- and middle-income countries like
Uganda suggests a need to effectively and efficiently utilize the limited resource available for PHC
coverage. Furthermore, effective utilization of resources (financial and otherwise) is at the heart of
many health systems strengthening initiatives in Uganda and the world over. However, there is limited
literature on the use of PHC funds in Uganda and the rest of the world. Most of the available PHC
financing literature focuses on the gaps in financing and the strategies to increase funding.
Against such a background, PATH commissioned a study to assess the trends in expenditure/use of
PHC finances in Uganda. The overall aim of the study was to examine the use of Uganda’s public
PHC funding at both national and subnational levels over a period of five years from fiscal year (FY)
2015/2016 to FY 2019/2020. The study specifically reviewed trends in the expenditure/use of PHC
finances at different levels of the health sector and how these have been affected by COVID-19. It
examined the limitations in utilization of PHC funds at the central and local government levels. It also
examined the functionality of oversight structures such as health unit management committees
(HUMCs).
The study examined expenditure patterns of PHC non-wage and development funds over the National
Development Plan II period. The focus was placed non-wage and development expenditure because
these are the PHC grants that are directly used to fund service delivery outputs. In addition, PHC
wage grants are paid directly into the respective bank accounts of the health workers on payroll.
The study employed an adaptation of the World Bank’s public expenditure review methodology,
focusing on the second of six questions under the public expenditure review: “How much was spent
and what it was spent on?” This involved analysis of the approved budgets and outturns for the health
sector. This was complemented with key informant interviews (KIIs) with actors in the Ministry of
Health (MoH); Ministry of Finance, Planning and Economic Development; district health offices; and
health facilities. KIIs at the subnational level were conducted in the districts of Arua, Kasese, Kisoro,
Mukono, and Tororo. These were purposively chosen on the basis of geographical representation,
high disease burdens, and their beneficiary status under any of the results-based financing (RBF)
projects being implemented in the country. RBF refers to the use of explicit performance-based
subsidies to encourage delivery of services by paying providers (government or development
partners) based on clearly defined quality outcomes. RBF in Uganda is delivered through Government
of Uganda and development partner–funded projects, which complement PHC financing.
The study concludes that while spending at the central government level suffered from budget cuts,
as demonstrated by shortfalls in the funds released to them, local governments and health facilities
received most, if not all, of the funds in their approved budgets during the reference period.
It was also noted that while the MoH had issued Sector Guidelines for Budgeting and Utilizing PHC
grants to health facilities, the majority of actors at that level remained unaware of the guidelines or
had not yet started to use them. Thus, PHC budgeting and expenditure remained inconsistent at
facility level despite the existence of the Sector Grant and Budget Guidelines to Local Governments
4and the Primary Health Care Non-Wage Recurrent Grant and Budget Guidelines to Health Centre II,
III , IV, and General Hospitals.
It was noted that the PHC budgets and expenditure in FY 2019/2020 were not affected by the
economic disruptions that arose from the containment of COVID-19. In addition, local governments
received an additional Ugandan shilling (UGX) 165 million and regional referral hospitals received an
additional UGX 270 million to combat the spread of COVID-19. The pandemic, however, affected
access to PHC services, as many people could not travel to the health facilities during the lockdown.
The study noted several challenges in the spending of PHC resources. The key challenges included
the parallel planning, reporting, and accounting processes for RBF projects at the health facility level,
which likely constrained the effective and timely implementation of the mainstream PHC activities.
Additionally, the disbursement of RBF funds continued to be characterized by delays, which affected
the implementation of planned projects. On the other hand, it was also noted that while PHC funds
were disbursed by the tenth day of the quarter, receipt of the funds on facility accounts continued to
be characterized by slight delays. This likely arose from delays in warranting processes for the grant
transfers.
Finally, while the HUMCs played a significant role of representing communities in PHC resource
allocation and utilization decisions, limited training and limited awareness of their roles constrained
their effectiveness in exercising oversight over PHC expenditure. Along with the HUMCs, the village
health teams (VHTs) also played a significant role as the first points of call in Uganda’s health system.
However, the voluntary nature of this role limited their effectiveness, as the VHTs prioritized earning a
living.
Based on these conclusions, the study makes the following recommendations:
• The MoH should consider increasing awareness around the Sector Grant and Budget Guidelines
to Local Governments and Primary Health Care Non-Wage Recurrent Grant and Budget
Guidelines to Health Centre II, III , IV, and General Hospitals. The guidelines were found to be
comprehensive and could solve several procedural challenges experienced in spending PHC
resources.
• The MoH should consider publishing updated HUMC operational guidelines and conducting
regular training of the HUMC members in order to improve their oversight function at the health
facility level.
• The MoH, in collaboration with its RBF development partners, should consider streamlining RBF
planning, reporting, and accountability processes into the administrative processes for the
mainstream PHC funds to lessen the administrative burden placed on the health workers.
• Local government administrations should consider improving their effectiveness in warranting the
transfer of funds in order to minimize delays in receipt of PHC grants in health facility accounts. It
was found that while release of funds was timely (by the tenth day of the quarter), slight delays
continued to characterize the receipt of these funds in health facility accounts, with challenges
being noted in the warranting process.
• The MoH and its RBF partners should consider digitalizing the management of all RBF projects in
the country to minimize the delays in reimbursement. While RBF was reported to have improved
service delivery at health facilities, it was also reported that the process of claiming
reimbursements was characterized with bureaucratic delays.
• The MoH should consider designating a proportion of the PHC non-wage funding as allowances
for VHTs to facilitate their work. This is envisaged to go a long way in redeeming some of the time
that VHT members lose to earning a living—time that can be put to undertaking their health
promotion role.
5Introduction
Primary health care (PHC) has come to be known as the bedrock of health systems around the world
and as the foundation on which universal health coverage is built.1 It has been noted that countries
with strong PHC programs report better health outcomes.2 The World Health Organization (WHO)
defines PHC as:
a whole-of-society approach to health that aims to ensure the highest possible
level of health and well-being and their equitable distribution by focusing on
people’s needs and preferences (as individuals, families, and communities) as
early as possible along the continuum from health promotion and disease
prevention to treatment, rehabilitation and palliative care, and as close as
feasible to people’s everyday environment.
PHC provision around the world has been constrained by many challenges—perhaps none greater
than limited financing. Recognizing the gaps in health coverage, in 2019, WHO recommended3 that
countries increase spending on PHC by allocating at least 1% more of their gross domestic product to
PHC; this would enable the world to meet the health coverage targets set out in the Sustainable
Development Goals. However, the gap between basic community health needs and PHC provision
has persisted. In some cases, the gap has increased despite increases in PHC resources—especially
in the developing world.
Developing countries like Uganda already commit a large proportion of their health sector budgets to
PHC with the aim of improving health coverage. A study4 conducted by PATH in 2019 noted
increases in PHC funding over the five-year period that led up to the study year. In fiscal year (FY)
2018/2019, for example, PHC accounted for about 70% of the health sector funding when considered
collectively with the supply of emergency medicines and health supplies (EMHS). Nonetheless, the
health policy literature notes persistent financing gaps within PHC even considering the funding
increment.5
The persistent, and in some cases widening, gap between community PHC needs and the available
funding in low- and middle-income countries like Uganda suggests a need to effectively and efficiently
utilize the limited resources available to improve the coverage and quality of PHC. Furthermore,
effective utilization of resources (financial and otherwise) is at the heart of many health systems
strengthening initiatives in Uganda and the world over.6 However, there is limited literature on the use
of PHC funds in Uganda and the rest of the world. Most of the available PHC financing literature
focuses on the gaps in and strategies to increase financing.
Against such a background, PATH commissioned a study to assess the expenditure/utilization of PHC
financing in Uganda. The study focused on different levels of health service delivery in five selected
districts that represent the major regions of Uganda. Findings from this study are envisaged to
contribute to the growing body of available literature on PHC financing and expenditure in Uganda.
The study is also envisaged to provide policy evidence to strengthen advocacy efforts on PHC
financing and expenditure— especially as the country moves into another phase of implementing the
new National Development Plan II, the Health Sector Development Plan, and the universal health
coverage agenda.
Additionally, the study is expected to contribute evidence on how COVID-19 has affected overall
health sector financing and the provision of PHC in Uganda. The study was conducted when Uganda,
along with the rest of the world, was battling to contain COVID-19 and to recover from the devastation
caused by the pandemic. Pandemics such as COVID-19 are often accompanied by economic shocks
that place unpredictable pressures on already limited resource envelopes in developing countries
such as Uganda. The health sector in Uganda was and continues to be at the forefront of efforts to
contain the spread of the pandemic in the country. Country efforts to combat the pandemic were
financed via supplementary budgets mainly from grants and additional borrowing from the country’s
development partners.
6Objectives of the study
The overall aim of the study was to examine the use of Uganda’s public PHC funding at both national
and subnational levels. The study objectives were to:
1. Review the expenditure/utilization trends of PHC finances at different levels of the health sector
and how these have been affected by COVID-19.
2. Examine the limitations in the utilization of PHC funds at central and local government levels.
3. Examine the functionality of oversight structures, such as health unit management committees
(HUMCs) and expanded district health teams.
7Approach and methodology
PATH focused its analysis of trends in the use of PHC public funding on recurrent non-wage functions
and development (capital) expenditure at both the national (central) and subnational (local
government) levels. The scope of the study was limited to funding from the Government of Uganda
and development partners over the five-year period from FY 2015/2016 to FY 2019/2020.
PATH used the following criteria to select study districts at the local government level: The study team
purposively sampled the study districts to ensure regional representation. In order to maintain
consistency in its PHC analyses, PATH took efforts to maintain three of the districts—Mukono, Arua,
Kisoro—that were part of the PHC financing study that PATH conducted in 2019. PATH also
purposively selected study districts with a high burden of disease. PATH added the criterion of
implementation of results-based financing (RBF) projects to ensure that all PHC financing (including
co-funding arrangements between the Government of Uganda and its development partners) were
represented in the study. Following these criteria, the districts of Arua, Kasese, Kisoro, Mukono, and
Tororo were selected for data collection (see Table 1 for details).
Table 1. Purposive sampling criteria used to select study districts.
Subregion District Rationale/characteristics considered
Eastern Tororo ⎯ High disease burden.
⎯ Results-based financing beneficiary district (currently
part of Uganda Reproductive, Maternal and Child
Health Improvement Project).
⎯ Border district to Kenya.
Central Mukono ⎯ Combination of urban and rural characteristics.
⎯ Taken as a proxy for Uganda’s capital given its
proximity to the capital.
⎯ Results-based financing beneficiary district (Uganda
Reproductive, Maternal and Child Health
Improvement Project).
South-Western Kisoro ⎯ Hard-to-reach areas due to a mountainous terrain.
⎯ Border district to Rwanda.
⎯ Results-based financing beneficiary district (Uganda
Reproductive, Maternal and Child Health
Improvement Project).
West Nile Arua ⎯ Refugee hosting dynamics.
⎯ Results-based financing beneficiary district
(Establishing a Financial Mechanism for Strategic
Purchasing of Health Services in Uganda).
Western Kasese ⎯ Border district with the Democratic Republic of the
Congo.
⎯ Hard-to-reach areas due to a mountainous terrain
⎯ Results-based financing beneficiary district (currently
Uganda Reproductive, Maternal and Child Health
Improvement Project).
8Data collection
PATH used two approaches to collect data: key informant interviews (KIIs) and review of available
documents.a These approaches generated financial, statistical, and graphical data as well as other
information for analysis.
Key informant interviews
PATH conducted KIIs with key actors at both the central and local government levels. At the central
government level, the study team held KIIs with key actors in the Ministry of Finance, Planning and
Economic Development (MoFPED), the Ministry of Health (MoH), and civil society organizations that
were undertaking PHC activities. At the local government level, the study team held KIIs with key
actors in the district health departments as well as coordinators of the village health teams (VHTs) to
obtain views from the district administration.
The study team also conducted interviews at health facilities—at three levels of care (health center II,
health center III, and health center IV) that make up the health subdistrict. The health subdistrict was
considered because Uganda runs a referral-based system of care, in which the bulk of PHC services
are delivered in the health subdistrict. Four health facilities were purposively selected to represent the
three levels of care as well as the private, not-for-profit facilities, which also receive PHC funding from
the government. Additionally, facilities were purposively selected to reflect both urban and rural
settings in the district. In Arua, one of the facilities was selected because it was in a refugee camp.
The study team undertook KIIs with health unit in-charges and the chairperson of the HUMC, or
another member of the HUMC in the chairperson’s absence. In addition, the study team conducted
exit interviews of patients at health facilities to obtain the views of the users of PHC services. A
breakdown of the interviews undertaken is presented in Table 2.
Table 2. Key informant interviews undertaken in the districts.
District HUMCs In-charges Patients VHT DHOs Row
coordinators totals
Arua 4 4 11 1 1 21
Kasese 5 4 10 1 1 21
Kisoro 4 4 11 1 1 21
Mukono 4 4 10 1 1 20
Tororo 3 4 8 1 1 17
Column totals 20 20 50 5 5 100
Note: DHO, district health officer; HUMC, health unit management committee; VHT, village health team.
Data management and analysis
The study team analyzed both qualitative and quantitative data. The management and analysis of the
quantitative data were done using Microsoft Excel. Qualitative data obtained from the KIIs were
transcribed (verbatim) in Microsoft Word documents to form the interview transcripts. The interview
transcripts were entered into ATLAS.ti to form a hermeneutic unit (qualitative database) that was used
for analysis. In ATLAS.ti, the qualitative data were analyzed along content themes that were
developed from the reviewed literature.
a
The documents reviewed for the study are provided in the reference list of this study report.
9Limitations of the study
The study was undertaken in the middle of the COVID-19 pandemic. As a result, the study team faced
a lot of constraints in collecting data, especially the absence of key informants. Many of the targeted
respondents were among the first responders and also part of the various task forces convened to
combat the pandemic. To mitigate this challenge, the study team replaced these respondents with
other actors in the same entities so as not to derail the study. In addition, the study team faced
challenges in accessing budget outturn (expenditure) data and other information at local government
and facility levels due to the limited availability of approved expenditure reports. The team therefore
sought to obtain data from MoFPED; however, these data were also limited because the local
governments were only added to the program budgeting system in FY 2018/2019. Therefore, while
the reference period for the study was the five-year period from FY 2015/2016 to FY 2019/2020, the
analysis was affected by missing data in some instances.
10Overview of health sector expenditure
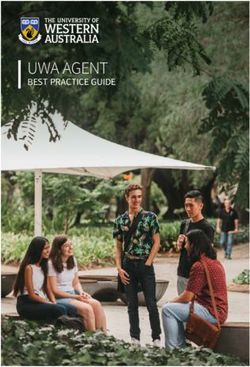
Over the reference period of the study, the health sector budget increased from Ugandan shilling
(UGX) 1.271 trillion in FY 2015/2016 to UGX 2.589 trillion in FY 2019/2020. However, over the same
period, it was noted that the sector persistently received and subsequently spent less than what had
been appropriated by the Parliament of Uganda. See Figure 1 for details; note that “released” funds
represent the actual public funds received by the government spending entities.
Figure 1. Health sector budget performance patterns and trends (in billion UGX).*
3,000
2,500
2,000
1,500
1,000
500
-
Spent
Spent
Spent
Spent
Spent
Released
Released
Released
Released
Released
Approved
Approved
Approved
Approved
Approved
FY 2015/16 FY 2016/17 FY 2017/18 FY 2018/19 FY 2019/20
Other NRH (Naguru, Kawempe & Kiruddu) Kampala Capital City Authority
Local Governments Regional Referral Hospitals
Uganda Virus Research Institute (UVRI) Butabika Hospital
Mulago Hospital Complex Uganda Blood Transfusion Service (UBTS)
Health Service Commission National Medical Stores
Uganda Heart Institute Uganda Cancer Institute
Source: Computations from the Annual Health Sector Performance Reports over the years.
Note: FY, fiscal year; National Referral Hospital; UGX, Ugandan shilling.
* Outturn data for FY 2015/2016 were missing in that fiscal year’s Annual Health Sector Performance Report.
It was noted that there was no discrepancy between what the local governments received and spent
compared to what was appropriated. Among the government entities that made up the health sector,
the MoH was the most affected by the challenge of receiving less funds than what was appropriated.
This trend was mostly attributed to revenue shortfalls for the Government of Uganda budget lines and
delayed disbursement of funds from development partners for the externally financed budget lines.
For instance, in FY 2016/2017, the health sector received about 66% of the funds appropriated to it,
with the MoH receiving only 36% of the funds it had been appropriated. The FY 2016/2017 Annual
Health Sector Performance Report attributed these shortfalls to low disbursements from the MoH’s
key development partners, namely Gavi, the Vaccine Alliance and the Global Fund to Fight AIDS,
Tuberculosis and Malaria.
It is notable that the challenge of budget cuts (i.e., releases of funds less than budgeted amounts) in
the Government of Uganda budget lines is not unique to the health sector. These cuts mostly arise
from shortfalls in domestic revenue collection, which compel the Government of Uganda to cut back
11on its planned spending if additional revenue is not raised through borrowing. However, it was noted
that this expenditure trend persisted across the reference period of the study when the health sector
benefited from revised budgets that were higher than their approved budgets, mostly due to
supplementary funding to deal with health emergencies. Despite this, the health sector still ended up
receiving less funds than what was budgeted. Most of the funds the sector received were spent—on
average, between 98% and 100% absorption/consumption.
PHC expenditure at local government and health care facility levels
Further scrutiny of the sector budgets over the reference period revealed that the disruptions arising
from budget cuts mostly affected central government entities of the health sector. Local governments,
which only receive PHC funds, either registered supplementary budget releases or received more
than 97% of their budgeted funds. In FY 2016/2017, several local government votes received
supplementary funding (extra funds), which resulted in 101% and 97% of these transferred/released
funds being spent. In FY 2018/2019 and FY 2019/2020, local governments received 99.6% and
97.0% of their budgets respectively (see Figure 2 for details).
Figure 2. Performance in releases/transfer of PHC grants to local governments.
600,000
UGX in Millions
500,000
400,000
300,000
200,000
100,000
-
Approved Total Approved Total Approved Total
Budget Releases Budget Releases Budget Releases
FY 2016/17 FY 2018/19 FY 2019/20
Source: Computations from Ministry of Finance, Planning and Economic Development data.
Note: FY, fiscal year; PHC, primary health care; UGX, Ugandan shilling.
In the KIIs, respondents from local government administrations and health facilities attributed the high
level of expenditure performance at the local government level mostly to the insufficiency of the PHC
funds. As a result, these funds are often quickly spent and used up before health needs are met. At
times, local government PHC funds require supplementary allocations in the case of emergencies.
Comments from the respondents included the following:
Now how can you have unspent PHC money? We are
already getting little money. Now how can you fail to
spend it? The money is little, so by the time it comes you
already have a number of debts here and there. Then
how can you fail to spend the money?
12– District health officer
[There are] no balances apart from the money we leave
to maintain the account, because if they give us 5 million
shillings and a few cents, we use most of the money for
activities and the rest to secure the account and for bank
charges.
– Health facility in-charge
At health facility level, the high level of expenditure performance was reported to be similar across the
public and the private, not-for-profit health facilities. It was also similar across all levels of care
assessed (health center II, health center III, and health center IV).
Performance in non-wage and development grants
The study sought to assess performance in the PHC non-wage and development grants across the
reference period. Local governments receive a recurrent non-wage grant to fund the day-to-day
running of their health departments and the health facilities. In addition, they receive a PHC
development grant for the maintenance of health infrastructure and, in subcounties without a health
center III, for the upgrading of health center II facilities into health center III facilities. In selected local
governments, the PHC transitional development grant funds hospital rehabilitation and other specified
capital investments.
Over the study period, the study sites demonstrated high levels of budget performance in PHC non-
wage and development grants, with most the budgeted funds released to the local governments (see
Figure 3).
Figure 3. Performance in PHC grants to local governments.*
140,000
UGX in Millions
120,000
100,000
80,000
60,000
40,000
20,000
-
Budget Releases Budget Releases Budget Releases Budget Releases
FY 2016/17 FY 2017/18 FY 2018/19 FY 2019/20
Transitional Development Non-Wage Development
Source: Computations from Ministry of Finance, Planning and Economic Development data.
13Note: FY, fiscal year; PHC, primary health care; UGX, Ugandan shilling.
* FY 2016/2017 and 2017/2018 reflect no development funding because local governments did not receive PHC
development grants.
It was noted that the PHC transitional development grant accounted for most, if not all, discrepancies
between the amounts budgeted and the amounts received by local governments. In FY 2018/2019
and FY 2019/2020, local governments received 45% and 70% of the budgeted transitional
development grants respectively. These performance levels could be attributed to revenue shortfalls
and procurement delays.
Among the study districts, only Tororo district and Arua district budgeted for PHC transitional
development grants in FY 2019/2020. However, while the other study districts received all of their
budgeted amounts across all of their budgeted funds, Arua did not receive any of its budgeted PHC
transitional development grant (see Table 3 for details).
Table 3. PHC grants transfer performance in fiscal year 2019/2020 (in UGX).
PHC Non-Wage PHC Development Transitional Development Grant
Local Government Approved Total Approved Total Approved Total
Budget Releases Budget Releases Budget Releases
Arua District 701,701,135 702,180,975 162,348,223 162,348,223 213,165,330 -
Arua Municipality 46,151,129 46,151,151 6,012,897 6,012,897 - -
Kasese District 971,256,400 969,537,590 1,134,543,803 1,134,543,80 - -
3
Kasese Municipality 44,709,783 47,360,050 12,025,794 12,025,794 - -
Kisoro District 583,862,464 579,482,278 602,311,301 602,311,301 - -
Kisoro Municipality 54,530,859 54,530,885 500,092,049 500,092,049 - -
Mukono District 340,500,257 339,261,725 78,167,663 78,167,663 - -
Mukono 35,306,647 35,306,663 12,025,794 12,025,794 - -
Municipality
Tororo District 806,277,232 807,202,850 614,337,095 614,337,095 250,000,000 250,000,000
Tororo Municipality 59,652,476 59,652,504 18,038,691 18,038,691 - -
Grand Total 3,643,948,382 3,640,666,67 3,139,903,311 3,139,903,31 463,165,330 250,000,000
1 1
Source: Computations from Ministry of Finance, Planning and Economic Development data.
Note: PHC, primary health care; UGX, Ugandan shilling.
The PHC expenditure was noted to be similar across the years (See Annex 1) as well as across
districts and municipalities (municipalities receive their funding independent of the districts where they
are located). Over the course of FY 2019/2020, utilization of development grants was reported to
have improved relative to previous years. This was mostly attributed to a reform instituted by the
MoFPED to transfer all development grants to local governments by the end of the third quarter. This
ensured that local governments had a whole quarter in which to spend the funds, which minimized the
unspent balances that arose from procurement delays in previous years when some development
funding was transferred in the final quarter of the fiscal year.
While the timeliness of the disbursement of funds has greatly improved and is now predictable,
timeliness in the receipt of grants remains a challenge. In 2014, the MoFPED instituted a reform to
disburse funds by the tenth day of every quarter. However, the literature on public expenditure
indicates that government spending entities are still receiving funds late due to delays in warranting
and in submission of relevant supporting documents.7
14Use of PHC funds at local government and facility levels
The study sought to assess the processes through which PHC funds are used at both local
government and health facility levels. In particular, the study team undertook consultations with
various actors at these levels with regard to procurement, use of MoH guidelines, and the oversight
roles of actors such as the HUMCs. This section delves into the findings from these consultations.
Adherence to PHC grant utilization guidelines
Budgeting and expenditure at the local government and health facility levels are guided by the MoH’s
Sector Grant and Budget Guidelines to Local Governments. Over the reference period for this study,
the MoH had not produced health facility–level guidelines since 2003, which provide comprehensive
guidance on the utilization of and accountability in PHC non-wage and development grants
transferred to health center II, health center III, and health center IV facilities, as well as general
hospitals. As a result, there was a lot of inconsistency in how PHC funds were used at the facility
level. The MoH resumed the publication of guidelines for health facilities’ utilization of PHC funds with
the FY 2020/2021 guidelines. This was a result of policy recommendations made by PATH in its 2019
study and other studies5 that recommended the same.
The study assessed awareness of and adherence to the guidelines among district health officers,
health facility in-charges, and VHT coordinators. The study team worked under the assumption that
the guidelines had been used during the budgeting for FY 2020/2021. The study team also assumed
the guidelines were being used for expenditures since data collection took place in August—midway
through the first quarter of FY 2020/2021.
The study findings showed that district health offices/departments were fully using the health
guidelines. In contrast, the majority of the health facility in-charges, members of the HUMCs, and VHT
coordinators who were consulted either were not aware of the guidelines or were aware but had not
received a copy of the guidelines. Furthermore, even in instances where in-charges reported being
aware of the guidelines, their facility budgets were inconsistent with the provisions of the guidelines.
For instance, while the guidelines allocate 30% of the PHC recurrent non-wage grant toward outreach
activities, most facilities reported allocating between 40% and 50% to outreach programs; they
claimed that this was based on the allocations on the guidelines. Furthermore, inconsistencies were
noted between the allocation patterns of the public and the private, not-for-profit facilities. Comments
from respondents included the following:
The 50% goes for medicine; that is, NMS [National
Medical Stores]. The remaining 50% is divided into two:
30% for top up of salaries for staff while 20% for
maintaining the facility. They know that our collection may
not be enough to undertake all our activities.
– Respondent from private, not-for-profit organization
The PHC grant has its own way of expenditure; the
money comes with directions on how it should be spent—
15for example, 40% for outreaches, 30% for management,
and 30% for transport and support services. So this
money is spent in line with the above stipulation as per
the MoH guidelines.
– Health center III in-charge
The persistent inconsistency across facilities implies that the MoH’s guidelines were not disseminated
to the health facilities. There is therefore a need to widely circulate the guidelines to ensure service
provision is consistent across the country. This dissemination ought to also extend to the HUMCs,
which oversee expenditures at the health facility level. Consultations with the HUMCs revealed that
they were not aware of the new guidelines.
Procurement using PHC funds
Procurement is a significant part of expenditure of public funds, such as the PHC recurrent non-wage
and development grants. Over the years, procurement delays have been cited as a major challenge
to the effective utilization of PHC and other public funds in Uganda. It is worth pointing out that the
Primary Health Care Non-Wage Recurrent Grant and Budget Guidelines to Health Centre II, III, IV,
and General Hospitals provide a comprehensive guide to procurement processes at both local
government and health facility levels.
The guidelines state that health departments are expected to be familiar with the procurement
procedures laid out in the guidelines, since the departments have had the guidelines for several
years. The health facilities, on the other hand, are envisaged to have implementation gaps since they
have not had guidelines to refer to for several years.
At the departmental level of local governments, the district is expected to have an approved
procurement plan that is incorporated in the local government procurement plan. Procurement is
expected to be undertaken in adherence to the Public Procurement and Disposal of Public Assets
Authority regulations. In addition, it is expected that the signing of contracts for construction under the
PHC development grants is witnessed by the HUMC or hospital board of the affected facility.
Consistent with the grant utilization guidelines, all KII respondents at local governments and health
facilities reported that they had functional procurement committees in place. These work with the
procurement departments and the user departments (the departments that undertake the purchase to
contracting) to advertise, scrutinize bids, and award contracts in conformity with Public Procurement
and Disposal of Assets Authority regulations. A respondent reported:
We have the procurement committee, and on that
committee, we have the Chief Administrative Officer who
sends the budget to the procurement committee with
items for procurement. The procurement department then
organizes the bid documents and advertises. After
advertising, the procurement committee seats and
awards the contract. Now the head of department is the
vote controller, and also plays a role of supervision, and
16writes the technical report that is used to pay the
contractors.
– District health officer
Procurement committees were also reported to be in existence at the local government level with
varying degrees of functionality. Facilities that benefited from RBF reported that the existence of
procurement committees was a prerequisite for the receipt and use of RBF funds. These facility
procurement committees were reported to handle procurements that do not exceed UGX 1 million.
Thus, procurement using PHC development funding is undertaken at the local government
administrative level and procurement using the PHC recurrent non-wage grant is undertaken at the
health facility level. As a respondent explained:
Now let me tell you, every facility that is implementing
RBF has what we call a procurement committee. And at
facility level, they are able to discuss and procure
commodities which don’t go above 1 million. So
commodities which go above 1 million, we use the district
procurement officer with a plan. We have a procurement
officer at this level through, which all these go through.
– District health officer
KIIs with the HUMCs and health facility in-charges also confirmed the existence of functional
procurement committees. However, while the majority of the HUMCs reported having functional
procurement committees or subcommittees, in some of the facilities, the HUMCs reported having
limited involvement in the procurement and disposal of assets. Health facilities reported that they did
not have the mandate to dispose of Government of Uganda assets. Disposal of assets, such as
expired or soon-to-expire medicine, is done in collaboration with the district health department and
National Medical Stores. A respondent reported:
For disposal of assets, first of all, the health facility
doesn’t have a mandate of disposing—it is the district
[that has this mandate]. Therefore, when the district
officials…come to register those assets to be disposed of,
obviously they interact with the health in-charge and the
HUMC members who tell them which items are no longer
in use and can’t be used again at the facility.
– Health unit management committee member
17Districts also reported having comprehensive procurement plans that were developed in consultation
with actors at all levels. Procurement at the health facility level is undertaken in line with annual work
plan budgets, with the HUMCs inspecting and approving the purchases. Items such EMHS are
procured on a quarterly basis. As a respondent noted:
We have a procurement plan that we worked on together
with the Joint Medical Store that supports the district in
the supply of drugs, and that procurement plan [was]
done in collaboration with the facility in-charges for health
centers II, III, IV, and hospitals. The health centers, they
come seat together and say for us we shall meet a, b, c
per quarter as per the work plans and they are sent to the
ministry. They plan for the year, but they keep on
requesting per quarter, because what they require varies
and this depends on their consumption rate.
– District health officer
The current study’s findings revealed that challenges continue to plague procurement of EMHS and
their effective delivery. PATH’s 2019 study on PHC financing in Uganda revealed major funding gaps
in both credit line and non-credit line commodities of the EMHS.b The study estimated that in FY
2018/2019, credit and non-credit line commodities had funding gaps of about 42% and 22%
respectively.
The funding gaps for EMHS heighten the need for effective and efficient use of the limited resources
available. However, while the health facilities’ requisition systems for EMHS have been reported to
function effectively, discrepancies between what was requisitioned and what was delivered have also
been reported.5 Discrepancies have been reported both in the quantities delivered and in the
composition of the delivery. In some instances, health facilities have been reported to receive
consignments meant for other health facilities. In addition, the available literature points to a lack of
feedback and responsiveness from the National Medical Stores when such discrepancies are
reported. Such system challenges ought to be rectified for health facilities to effectively and efficiently
use their credit lines for EMHS.
Functionality of health unit management committees
The HUMCs undertake an important role of exercising oversight on the utilization of PHC resources at
health facilities.
Composition of HUMCS: It was observed that the Sector Grant and Budget Guidelines to Local
Governments outlined the functions of the HUMC in the use of PHC resources. However, the
guidelines did not comprehensively delineate the composition of the HUMCs. The HUMC guidelines
that were published in 2003 are outdated and have not been accessed by many of the current health
b
Credit-line commodities are essential medicines and health supplies that are entirely funded by the Government of Uganda and have budget
ceilings/expenditure limits, which are solely controlled by the health facilities. On the other hand, non-credit line commodities are co-funded by the
Government of Uganda and its development partners. The quantification and budget control functions are under the MoH.
18facility staff and HUMC members. It was observed that the composition of HUMCs varied greatly,
including the gender compositions of these committees.
The 2003 HUMC guidelines called for a minimum of four members, including a chairperson, the
facility in-charge (secretary of the HUMC), a teacher in the zone where the facility is located, and a
representative from each parish that the health facility serves. Thus, the number of members of
HUMCs varies depending on the number of parishes served by the given health facility. Across the
facilities visited, the composition of the HUMCs ranged from three members (contravening the
minimum number required) to nine members. The HUMC guidelines were silent on the gender
distributions of the membership, and it was noted that all the HUMCs included in the KIIs were male
dominated.
Meeting frequency: Meetings are essential to the effective functionality of the HUMCs. They
enhance accountability by ensuring that decisions are not made by the chairpersons and in-charges
alone. HUMCs are required to meet at least quarterly, as per the HUMC guidelines of 2003. Indeed,
the majority of the HUMC members interviewed for this study reported that they met quarterly.
However, there were a few cases in which the HUMCs reported that their meetings were infrequent;
these HUMCs depended on the in-charge convening them and the availability of PHC resources to
fund the allowances of the members. As one respondent commented:
We are supposed to meet quarterly but because of the
PHC, we meet when funds are available, because you
cannot tell people to meet and then tell them to go
without transport, as you know our people.
– Health unit management committee member in
Kisoro
Understanding of their roles: Knowledge plays an important part in the effective delivery of any role.
When HUMC members asked about whether they were oriented to their roles, the study team
received mixed reports: some HUMC members reported having been oriented and other HUMC
members even within the same districts reported not being oriented. Orientations were conducted by
various actors, including the chief administrative officer of the district, the district health officers, and
staff of nongovernmental organizations. As a respondent said regarding training of HUMC members:
It’s supposed to be so, but you find that the subcounty
has limited resources for training those people…but there
are some other partners like World Vision or Plan
International that train. Like just of recent it was Plan
International who took us for training on management of a
facility.
– Health unit management committee member in
Tororo
19It is important to orient HUMC members to their roles in order for them to be effective in exercising
oversight over PHC expenditure at the facility level. There were reports of the HUMCs being highly
influenced by the facility in-charge in undertaking their duties, which blurs the lines of accountability
and constrains the oversight. The knowledge acquired through orientations will empower the HUMC
members to provide oversight.
Functionality of the village health teams
In Uganda’s referral-based health system, the VHTs play an important role of being the first
responders. They play a significant role in promoting health, sensitizing communities, and creating
awareness on disease prevention. The VHTs therefore significantly contribute to the decongesting of
Uganda’s health center II facilities by providing basic diagnostics and first aid, as evidenced by the
following comment:
[The] government established them [VHTs] as health
center I. First of all, they help us in mobilizing in the
communities. At the same time, they help in community
sensitization, especially on healthy practices at
household level as far as PHC is concerned, like having
sanitary facilities at household level, proper use of treated
mosquito nets, and then access of health services at the
right time and from the right place. And they help us
reach out to the communities. Occasionally, they are our
entry points to the community: like under PHC, we have
health camps. We engage them to mobilize, like I said.
And also, they demonstrate…those practices that need to
be demonstrated to the communities before they can
adopt them.
– Village health team coordinator
In the country’s effort to combat the spread of the COVID-19 pandemic, VHTs have played an
important role in creating awareness about the virus and the standard procedures put in place to
minimize the spread of the virus. For example, a respondent note:
Their role as VHTS is very critical; for example, the first
alerts we got of people passing through porous borders
was through them. Everybody identified with
abnormalities is reported immediately and we were
picking them. So their systems are the ones which have
helped us safeguard our district from intruders and
20maybe infection from across borders. So the role in
COVID-19 vigilance has been critical and has helped us.
– Village health team coordinator in a border district
Challenges faced: While the VHTs operate voluntarily and are only paid a modest allowance, their
coordination function is meant to be facilitated through the funding for PHC. However, the VHT
coordinators interviewed in this study reported that their funding was meager and unpredictable based
on activities. While some of the districts have established proportions to be allocated to these
coordination functions under the RBF projects, these have not been adhered to, mostly due to the
inadequacy of PHC funding. A KII respondent noted:
For sure, in terms of percentages, I can’t lie to you.
Because even as the board controller in my department,
I’m supposed to be allocated 15%, but I don’t see even 2
or 1%. My other colleague who is supposed to be given
8% gets 2%, but you are only allocated an activity and
under that activity you realize the only person you can
mobilize is the VHT. There is no clear budget or
proportion given to them… they are only given
allowances based on the activities they’re engaged in and
that also depends on the implementing partners.
– Village health team coordinator
Utilization of other PHC resources (results-based financing)
The provision of PHC in Uganda, along with other developing countries, is constrained by well-
documented financing challenges.8 Over the last 17 years, RBF projects have been implemented in
the health sector to complement the limited PHC resources available.9 The main feature of RBF is the
payment for results attained, as per the health facility’s performance improvement plan.
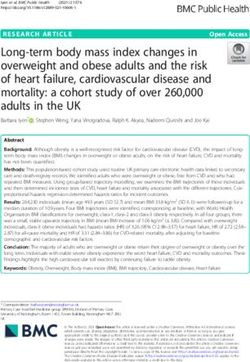
RBF has significantly improved the financing for PHC in Uganda. For instance, in FY 2018/2019, the
Kasese district received a total payout of UGX 2.965 billion for its facilities that implemented RBF; this
was funded by Enabel, a Belgian development agency. In FY 2017/2018, the facilities that
implemented RBF in the district received a total payout of UGX 3.131 billion from Enabel. These
resources were significantly higher than the sum of the PHC non-wage and development grants that
the district received in that year.10 Several other districts in the Rwenzori and West Nile Region have
benefited from this kind of funding, as illustrated in Figure 4.
21Figure 4. Fiscal year 2018/2019 results-based financing payouts by Enabel.
3,500
2,965
3,000
Pay-outs in Million UGX
2,500
2,000
1,500
1,116
792 905
1,000 671 727
513 518 599
481
500 363
202
48 49
0
Source: Rwenzori Center for Research and Advocacy, 2019.
Note: UGX, Ugandan shilling.
Similar payouts have been received around the country: RBF currently covers over three quarters of
the districts in Uganda.
Use of RBF: There are strict guidelines for the use of RBF funds that are separate from the Sector
Grant and Budget Guidelines to Local Governments. Beneficiary facilities must develop a
performance improvement plan that includes all RBF activities that it will undertake. Thus, while the
funding is complementary, it comes with parallel utilization, reporting, and accounting procedures,
which place additional administrative requirements on the health facility staff. As a respondent
reported:
Every quarter, we fill monthly invoices according to our
performance per month. Then, after calculating our
performance output, we convert it into monetary value.
So, at the end of the quarter, we come up with a quarterly
invoice, which we send to the Ministry of Health through
the district RBF focal person. Then, from the district RBF
focal person, she organizes a DHT (district health team)
to come and to audit what we did in that quarter. So, they
look at the self-assessment we did as a facility, whether it
rhymes with what the DHT has seen. So, when the DHT
is done, they make a report to the Ministry of Health RBF
unit. Then the MoH decides and sends external auditors
to come and counter-check what the DHT did. Now, after
approving the invoices, the money is sent according to
how we performed.
22– Health center III in-charge
Considering that the RBF activities are highly incentivized, and the funding is significantly higher than
the PHC non-wage grant allocations, there are indications that the RBF administrative requirements
are prioritized ahead of the PHC administrative requirements. As one respondent noted:
… Off that money, we calculate the 40% and we share as
staff then the 60%. We look at our performance
improvement plan of that quarter to see what we need to
buy; then the procurement committee sits and they plan
how to procure.
– Health center III in-charge
Benefits of RBF: Health facilities that implemented RBF projects reported that several benefits arose
from the implementation of the RBF projects. For example, with regard to health outcomes, RBF
incentivizes results, which leads to improved health outcomes, especially in reproductive, child,
maternal, and adolescent health. RBF complements allowance payments to health workers, which are
usually limited under the mainstream PHC grants. A respondent noted:
Our maternal services have greatly improved with RBF.
We managed to construct a ward for the pregnant
mothers, and our newborn care has therefore improved.
Another thing is that staff motivation has increased, so
now they work harder so as to benefit from the funds.
– Health center II in-charge
Challenges in implementation: Due to the additional administrative requirements placed on the
health facility workers, several KII respondents reported delays in the disbursement of the RBF funds:
The major challenge is the inability of the center to meet
and beat the timelines that are set according to our
guidelines; for example, now we are in the first quarter of
a new financial year but we are just receiving third-
quarter RBF facilitation for the last financial year. That
has been a great source of demoralization and has
affected the perception of the program among the staff.
23You can also read