Medical Trends Around the World 2016 - Mercer Marsh ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Medical Trends Around the World 2016


Introduction................................................................................................................................................ 2
1 High Medical Spend Continues: Is Lack of Action to Blame?......................................................... 4
2 The Rise in Non-communicable Disease Claims: the Impact of Lifestyle Choices........................ 8
3 The Burden of Risk: an Insurer’s Look at Rising Costs .................................................................15
4 The Rising Effect of Stress Is Evident .......................................................................................... 21
5 The Role of Government and/or Industry Associations Influencing Health................................ 29
6 Conclusion ................................................................................................................................... 30
About This Survey...................................................................................................................................... 31
Contents
1
Top Trends The results of Mercer Marsh Benefits (MMB)’s We’re grateful to the insurers that took the
second annual Medical Trends Around the World time and attention to respond to our survey.
1. Continuation survey are in. From February to May 2016, we Without these insights, we wouldn’t be able to
of high medical surveyed 180 insurers across 49 countries, produce such a comprehensive report. For a full
trend rate including almost 90 network affiliates of list of participating countries and the names of
multinational pools.1 insurers we’re able to disclose, please refer to
2. The rise in non-
the Appendix. (Note: Because the US is a very
communicable
Despite remaining stable, medical trend rates different healthcare market, we haven’t included
disease claims
continue to outpace local inflation and are on it in this report. For information on US trends,
and the impact of
average three times the general inflation rate. please consult Mercer’s National Survey of
lifestyle choices
They are driven by high healthcare spending in Employer-sponsored Health Plans.)
3. The burden of emerging markets and Western Europe. Several
risk: an insurer’s factors explain the growing costs: higher — often
look a rising costs lifestyle-related — risk factors; regulations that
transfer the burden of cost to private plans and,
4. The rising effect in some countries, foreign exchange rates.
of stress
It is no secret that an aging global population
5. The role of
will likely increase healthcare costs. But you can
government
optimize your health and well-being strategy
and/or industry
by keeping on top of these trends to manage
associations in
company spend while securing more rewarding
influencing health
futures for your business and your employees
around the world.
Introduction
Top Trends Shaping Employer-
sponsored Medical Plans
1
171 completed the full survey; 9 additional insurers provided medical trend data to support our findings.
About Mercer Marsh Benefits
Mercer Marsh Benefits (MMB) provides clients
with a single source for managing every aspect of
employee benefits. Located in 135 countries and
servicing clients in more than 150 countries, our
benefits professionals are deeply knowledgeable
about their local markets. Mercer and Marsh
have more than 75 years of experience in the
employee benefits brokerage and consulting
business, working with clients of all sizes.
In partnership with an integrated,
multidisciplinary team of nearly 300 professionals
advising multinational corporate headquarters,
we provide expert advice and coordinated
delivery of global and local solutions to help
our multinational clients leverage their buying
power. Blending technical knowledge with an
understanding of global business issues and
client-focused strategies, we have the expertise
and tools you need to help manage your cross-
border benefits and rewards programs.
In addition, our global health specialists
work extensively with more than 100 health
management and clinical resources around the
world. Together, our integrated global teams help
you enhance the physical and financial health of
your multinational workforce.
3
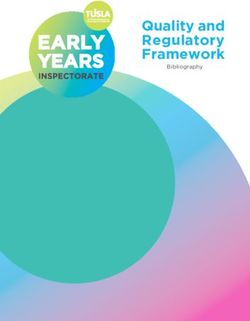
Insurers reported their actual 2015 and projected
2016 medical trend rates by responding to the
following question:
Based on your block of group or overall medical
insurance business, what actual medical trend rate
did you experience in 2015, and what rate are you
projecting for 2016? All aspects of healthcare including
hospitalization, outpatient, medications, maternity and
vision can be included in your assessment but where
possible, please exclude dental. The trend rate should
account for per person increases in cost due to medical
inflation, changes in utilization patterns and other
factors like changes in government regulation.
Seventy-three percent of countries (29 out of
40) who responded to this question still show a
medical trend rate double that of inflation, similar
to last year’s results. We should note that
1
inflation rates have generally been low and have
held steady according to our source data.2
However, we observed only moderate
fluctuations in medical trend rates, with most
only slightly higher than last year’s results.
High Medical Trend Rate
Continues: Is Lack of
Action to Blame? 2
S ources for inflation rates include:
• International Monetary Fund, World Economic Outlook Database, April 2016
Medical Trend Rates Continue to •
•
LA Economic Trends, April 2016 update
International Labour Organization, World Employment and Social Outlook, 2016
Outpace Inflation • European Commission, February 2016
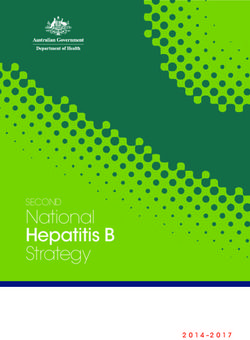
2015 medical 2016 projected 2015 medical 2016 projected
trend rate 2015 estimated medical trend 2016 forecast trend rate 2015 estimated medical trend 2016 forecast
experience* inflation† rate* inflation† experience* inflation† rate* inflation†
Global ‡ 9.9% 3.9% 9.8% 3.5% Spain 4.9% -0.5% 5.1% -0.4%
North America Sweden 5.5% 0.7% 5.7% 1.1%
Canada 6.3% 1.1% 6.0% 1.3% Switzerland 4.2% -1.1% 4.9% -0.6%
Asia (average) 10.3% 1.7% 11.5% 2.1% Turkey 10.1% 7.7% 11.8% 9.8%
China 10.3% 1.4% 11.5% 1.8% Ukraine 38.0% 48.7% 15.0% 15.1%
Hong Kong 7.5% 3.0% 7.7% 2.5% United Kingdom 5.9% 0.1% 6.4% 0.8%
India 9.7% 4.9% 8.5% 5.3% Latin America (average) 11.8% 6.7% 12.8% 8.0%
Indonesia 12.7% 6.4% 11.8% 4.3% Argentina 30.3% 28.1% 33.3% 33.7%
Malaysia 14.4% 2.1% 17.3% 3.1% Brazil 16.0% 9.0% 18.6% 8.7%
Philippines 9.4% 1.4% 10.0% 2.0% Chile 6.5% 4.3% 7.8% 4.1%
Singapore 9.9% -0.5% 9.9% 0.2% Colombia 8.1% 5.0% 9.0% 7.3%
South Korea 7.0% 0.7% 10.0% 1.3% Dominican Republic 4.6% 0.8% 6.0% 3.6%
Taiwan 8.7% -0.3% 10.1% 0.7% Mexico 10.5% 2.7% 11.0% 2.9%
Thailand 9.3% -0.9% 9.9% 0.2% Panama 10.8% 0.1% 10.5% 0.8%
Vietnam 14.3% 0.6% 19.3% 1.3% Peru 7.4% 3.5% 6.3% 3.1%
Europe, Middle East &
§
*The above medical trend rates reflect insurer survey results and may not be MMB’s view.
9.1% 4.1% 7.8% 2.5%
Africa (average) †
Sources for inflation rates include:
• International Monetary Fund, World Economic Outlook Database, April 2016
Denmark 2.0% 0.5% 3.8% 0.8%
• LA Economic Trends, April 2016 update
Egypt 14.8% 11.0% 16.6% 9.6% • International Labour Organization, World Employment and Social Outlook, 2016
France 2.0% 0.1% 1.8% 0.4% • European Commission, February 2016
‡
Average of 40 participating countries with an acceptable number of responses
Greece 5.7% -1.1% 5.1% 0.02% §
A lthough we received insufficient responses for Middle East, in general, medical inflation there remains high and
Ireland 9.7% -0.03% 5.3% 0.9% consistent with previous two years. Utilization trends show bias toward secondary healthcare facilities, which is often
further compounded by overutilization and overprescribing, so this trend is set to continue. As a result, within medical
Italy 2.3% 0.1% 2.9% 0.2% insurance market we are seeing increased emphasis on risk control, either through proactive health management
Latvia 10.8% 0.2% 9.1% 0.5% (wellness initiatives) or managed care approaches. The market, however, is not advanced in these approaches and, as
such, we do not foresee this having significant impact on cost in short term.
Lithuania 22.3% -0.7% 17.3% 0.6% ||
Stated values due mainly to increase of deductible.
Netherlands 2.5%|| 0.2% 2.5%|| 0.3%
Norway 7.6% 2.2% 6.9% 2.8%
Poland 10.1% -0.9% 7.8% -0.2%
Portugal 2.9% 0.5% 4.0% 0.7%
Romania 5.1% -0.6% 5.7% -0.4%
Russia 15.8% 15.5% 17.8% 8.4%
5
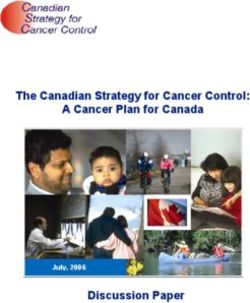
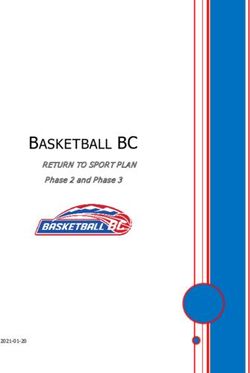
Medical Trend 0% 5% 10% 15% 20% 25%
Rates: Inpatient China
7.3%
11.9% 9.3% 12.8%
vs. Outpatient 7.2%
Hong Kong 6.1% 5.7% 8.7%
11.2%
Indonesia 12.8% 11.0% 11.8%
13.6%
Malaysia 14.5% 15.2% 18.1%
10%
Philippines 10.5% 10.0% 11.5%
11.3%
Singapore 7.8% 6.8% 10.3%
7.5%
South Korea 13.5% 10.0% 14.5%
11%
Taiwan 8.1% 8.9% 13.7%
7.7% 9.3%
Thailand 9.0% 9.2%
17.2%
Vietnam 12.1% 17.2% 22.1%
2015 inpatient medical 2015 outpatient medical 2016 projected inpatient 2016 projected outpatient
trend rate trend rate medical trend rate medical trend rate
Insurers in Asia provided medical trend rates for trend. Comparing our results to last year’s,
inpatient and outpatient coverages separately, one may say little to no change is a step in the
as is the norm in most countries across this right direction; however, the trend may reveal
region. The data are relatively similar to last year’s the extent to which employers are leading and
findings, with the greatest changes reflected in influencing employees regarding taking control
South Korea, Thailand and Vietnam (which have of their health.
experienced increased rates due to the high
prevalence of respiratory conditions in conjunction On a positive note, 13 countries (mostly in Europe,
with infectious diseases and new regulation for as evidenced by the regional average) suggest
accessing healthcare. For example, in Vietnam, the that medical trend rates will decrease next year.
Ministry of Health has recently issued a change to Such a decrease may indicate that this year’s
public hospital services that will increase charges moderate change is a sign that health- and well-
and potentially drive up costs by 30%.3) being-related actions being taken by employers
and employees could have an impact, though the
The current year’s data confirm that medical rates realization of these benefits will take time.
continue to outpace inflation, which is a long-term
3
ospital fees to increase by 30%, Viet Nam News, 15 February 2016, available at
H
6 http://vietnamnews.vn/society/282320/hospital-fees-to-increase-by-30-next-month.html.For information on This trend is not unlike our findings in the US.
US health trends, The 2015 Mercer US National Survey of Employer-
refer to Mercer’s sponsored Health Plans was completed in mid-2015
National Survey with the participation of 2,486 employers. When
of Employer- reviewing the results for the average per-
sponsored Health employee cost of health benefits, the actual cost
Plans 2015 report. growth for 2015 and the projected cost growth
for 2016 remain moderate overall. Overall results
reflect a 3.8% increase in 2015, nearly unchanged
from 2014’s increase of 3.9%. Whereas large
employers held the increase to 2.9%, small
employers saw cost rise 5.9%.
After years of increases of around 6%, cost
growth dipped to nearly 2% in 2013 and now
seems to be settling at a new plateau of around
4%. Although health benefit cost increases
are still outpacing CPI and growth in workers’
earnings, the gap is smaller than in past years.
Employers are predicting that costs will rise by
4.3% in 2016. That number reflects the changes
they intend to make this year to medical plan
offerings and plan design or contribution
strategy. We asked them how much costs would
rise in their largest medical plan if they made no
changes, and the average estimated increase
before changes was 6.3%. This is the lowest
underlying trend we’ve seen in a long time,
which has typically been closer to 8% or 9%. Of
course, general inflation is also very low — in fact,
it dipped below zero in 2015. In that context, a
6% underlying trend in health benefit cost still
represents a significant real increase in costs.
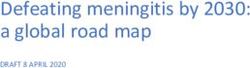
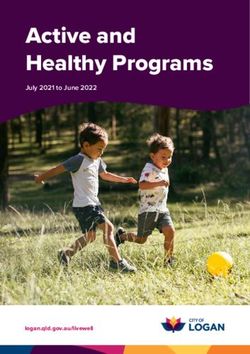
7Based on (dollar) 0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
amount claimed, 56%
52%
what were the top Cancer 53%
three causes of 64%
82%
claims cost in
53%
2015 based on your 59%
Diseases of the circulatory system 41%
book of group or 73%
68%
overall business?
29%
46%
Gastrointestinal diseases 25%
9%
9%
27%
46%
Respiratory conditions 15%
18%
27%
23%
4%
Osteomuscular diseases 43%
2
0%
9%
18%
14%
Obstetrics and pregnancy 16%
27%
27%
15%
18%
Endocrine and metabolic diseases 8%
27%
23%
15%
Rise in Non- Accidents, conditions derived from violence
18%
16%
18%
communicable Disease 5%
Claims: the Impact
15%
23%
Infectious diseases 9%
of Lifestyle Choices 36%
5%
10%
Claims for Lifestyle-related Illnesses Other (not classified in above groups)
4%
18%
Continue to Increase 0%
5%
Global Asia Europe M iddle East/ Latin America
Africa (MEA) (LATAM)Although retrospective claims costs represent Gastrointestinal health concerns also have of outpatient procedures, behind circulatory
just one data point in understanding a emerged into the top three claims categories and gastrointestinal conditions. Cardiovascular
population’s health profile and are heavily globally. The prevalence of infectious diseases conditions, cancer and respiratory diseases in Asia
influenced by the scope of coverage, cost of in emerging markets, the rise in liver diseases can be associated with exposure to polluted air,
treatment and other factors, they do provide an and diagnosis of inflammatory bowel disease are solid fuels used at home and infectious respiratory
indication of key health risks and opportunities just a few issues that could be attributed to the diseases including tuberculosis. Tobacco use is
to promote preventive care. Employers seeking increase in gastrointestinal infections and claims. also high, with the 2015 World Health Organization
to rely on such data to inform wellness initiatives reporting that, in some countries, more than 50%
should also consider other data sources, such In Asia, inpatient claims for gastrointestinal of adult males are smokers.
as annual medical examination anonymized conditions are trending higher than are
aggregated results, health risk assessments and circulatory claims. Cancer is now fourth in terms
employee surveys.
The data show that “we” remain in control of Asia Cost of Claims: Inpatient vs. Outpatient
the solution. Diseases of the circulatory system 0% 10% 20% 30% 40% 50% 60% 70%
have risen to be the leading cause of claims cost 46%
Cancer
16%
in Asia and the Middle East/Africa, surpassing 46%
Gastrointestinal diseases
even cancer. Gastrointestinal disease is now 34%
41%
ranked third highest in claims cost globally. Diseases of the circulatory system
41%
Cardiovascular health concerns can often be Respiratory conditions 32%
55%
attributed to health choices made by each Infectious diseases 23%
21%
person, and as such, there are actions that the Accidents, conditions derived from violence 16%
11%
collective “we” — employees and employers — can 13%
Disease of the sense organs
take to help control these issues, with the proper 2%
Endocrine and metabolic diseases 11%
access to information to live healthier lives. 18%
Obstetrics and pregnancy 11%
4%
Only in Latin America did the top three causes Genitourinary conditions 7%
9%
of claims costs remain unchanged, with cancer, Blood diseases 5%
2%
diseases of the circulatory system and obstetrics
Osteomuscular diseases 5%
ranking highest respectively. This rise in the 11%
2%
amount of medical spend on cardiovascular Mental conditions
0%
disease is particularly concerning in emerging Skin diseases 2%
13%
markets, suggesting earlier onset of lifestyle- Congenital anomalies 2%
0%
related diseases. 2%
Other (not classified in above groups)
11%
0%
Neurological conditions
2%
Inpatient Outpatient
9Based on 0% 10% 20% 30% 40% 50% 60% 70%
(frequency) 43%
66%
incidence of claims, Respiratory conditions 23%
what were the top 45%
64%
three causes of
40%
claims in 2015 43%
Diseases of the circulatory system 35%
based on your 64%
36%
book of group or
overall business? 38%
43%
Gastrointestinal diseases 40%
36%
23%
31%
14%
Osteomuscular diseases 46%
9%
27%
26%
38%
Infectious diseases 15%
27%
32%
21%
21%
Cancer 21%
18%
23%
15%
16%
Obstetrics and pregnancy 10%
27%
27%
15%
11%
Other (not classified in other groups) 20%
0%
14%
14%
16%
Endocrine and metabolic diseases 8%
36%
23%
12%
5%
Accidents, conditions derived from violence 19%
9%
9%
10 Global Asia Europe M iddle East/ Latin America
Africa (MEA) (LATAM)Lower Frequency of Cancer Claims
Asia Frequency of Claims: Inpatient vs. Outpatient
The survey revealed little change in the top three 0% 10% 20% 30% 40% 50% 60% 70%
most frequent causes of claims, except that the 41%
Gastrointestinal diseases
30%
amount of claims related to cancer has lowered
39%
Respiratory conditions
in comparison to our results from last year. This 64%
could be due to changes in how carriers manage Infectious diseases
34%
25%
claims in terms of treatment arrangements Cancer
29%
11%
with health vendors. The survey also confirmed
25%
Diseases of the circulatory system
the continued high frequency of respiratory 34%
16%
conditions in growth markets. Obstetrics and pregnancy 5%
Endocrine and metabolic diseases 14%
13%
Given the continued rise of cardiovascular 11%
Genitourinary conditions
illness, employers should expect to see a 11%
9%
correlation between absenteeism rates and Disease of the sense organs
5%
lowered productivity. As well as the direct cost Other (not classified in above groups)
9%
9%
of unplanned absence, such illness results in an Accidents, conditions derived from violence
7%
11%
associated reduction in productivity of 36.6% in 5%
Skin diseases
the US and 31.6% in Europe.4 13%
Blood diseases 4%
2%
As observed previously, the survey also showed a Osteomuscular diseases 4%
14%
rise in gastrointestinal conditions in Asia. 2%
Mental conditions
2%
Neurological conditions 0%
2%
Inpatient Outpatient
4
S ociety for Human Resource Management (in conjunction with Kronos). Total Financial Impact of Absences across the United States, China, Australia, Europe, India and Mexico, 2014.
110% 20% 40% 60% 80% 100%
To what extent 30% 44% 17% 7% 2%
Increased non-communicable disease (e.g., heart Global
do you think the d isease, cancers, stroke, chronic respiratory
25%
32%
39%
54%
24%
9%
10%
3% 2%
2%
Asia
Europe
d iseases, diabetes, Alzheimer’s disease, mental illness
following will and kidney diseases) 36%
45%
41%
46%
14%
9%
9%
MEA
LATAM
increase employer- Increased communicable disease (e.g., malaria, lower 6% 17% 21% 33% 23% Global
7% 38% 27% 28% Asia
sponsored respiratory, HIV/AIDS, tuberculosis, measles, h epatitis
1% 5% 13% 39% 42% Europe
B, other outbreaks of infection such as E bola, dengue 27% 9% 28% 18% 18% MEA
healthcare costs fever, Zika and chikungunya) 9% 14% 36% 27% 14% LATAM
in your country 4% 16% 29% 36% 15% Global
4% 28% 32% 36% Asia
over the next Increased accidents/violence 5% 6% 25% 35% 29% Europe
46% 27% 27% MEA
three years? 9% 41% 41% 9% LATAM
9% 33% 40% 14% 4% Global
Increased workplace and/or personal-related 5% 38% 43% 12% 2% Asia
11% 31% 38% 14% 6% Europe
stress/pressure 9% 27% 55% 9% MEA
9% 36% 32% 18% 5% LATAM
14% 37% 30% 16% 3% Global
11% 46% 34% 7% 2% Asia
Aging 14% 35% 27% 19% 5% Europe
9% 9% 36% 37% 9% MEA
27% 27% 28% 18% LATAM
9% 33% 37% 18% 3% Global
7% 41% 41% 11% Asia
Rising employee expectations 11% 23% 39% 20% 7% Europe
9% 64% 9% 18% MEA
5% 36% 36% 23% LATAM
18% 36% 32% 12% 2% Global
Availability and access to new medical 11% 41% 34% 11% 3% Asia
15% 38% 32% 14% 1% Europe
technologies, providers 18% 37% 27% 18% MEA
50% 23% 23% 4% LATAM
18% 22% 39% 17% 4% Global
21% 32% 34% 9% 4% Asia
Changes to health provider fee guides/schedules 14% 11% 43% 26% 6% Europe
18% 27% 37% 18% MEA
23% 32% 36% 9% LATAM
15% 28% 26% 21% 10% Global
Changes to public/government social security s chemes 11% 29% 36% 21% 3% Asia
19% 23% 20% 22% 16% Europe
and/or health reform/legislation 36% 28% 18% 18% MEA
18% 41% 23% 18% LATAM
4% 13% 36% 31% 16% Global
4% 29% 46% 18% 3% Asia
Environment factors (e.g., air pollution) 1% 4% 30% 38% 27% Europe
18% 9% 36% 37% MEA
9% 14% 32% 36% 9% LATAM
Expansion of coverage (e.g., higher benefit 12% 37% 27% 19% 5% Global
14% 48% 29% 7% 2% Asia
levels, reduction of exclusions, expansion of 8% 22% 32% 29% 9% Europe
covered services) 9% 82% 9% MEA
23% 36% 18% 18% 5% LATAM
7% 18% 38% 25% 12% Global
All forms of medical plan fraud and abuse (Initiated by 9% 23% 48% 16% 4% Asia
4% 8% 34% 31% 23% Europe
users, doctors and/or health vendors) 18% 46% 18% 18% MEA
9% 27% 41% 23% LATAM
Very large extent Large extent Some extent Modest extent No extent at all
12Lifestyle-related Conditions and Other Non-communicable Disease Conditions
to Continue to Drive Cost
Not surprisingly, increased incidence of non- organizations seek to redesign the benefits
communicable diseases (for example, heart strategy to make it more cost-effective,
disease, cancers, stroke, chronic respiratory analyzing the level of employee contributions
diseases, diabetes, Alzheimer’s disease, mental according to local resources and market needs.
illness and kidney diseases) is still projected to be Many interventions are not possible without
the leading cause of higher healthcare costs over the combined efforts of employers, employees,
the next three years. carriers, governments and health providers.
Increasing employer health plan costs can be A few notable changes from last year’s
attributed to three main causes: findings include:
1. Changes in many social security systems over • In Asia, we observed an increase related to the
the past few years imply a greater transfer of expected rise in incidence of communicable
the burden of cost to employers. diseases such as malaria, lower respiratory
disorders, HIV/AIDS, tuberculosis, measles, and
2. The increase in non-communicable diseases hepatitis B.
in an aging workforce drives the utilization of
new, more expensive technologies. • Latin American insurers consistently indicated
increased availability of and access to new
3. The pressure of attracting and retaining medical technologies and providers.
diverse and competitive talent compels
companies to offer enticing health benefits • Increased workplace and/or personal-related
packages. stress/pressure is now more evident across all
markets as a potential concern.
This requires consideration of accountable
models under which employees take more • On average, globally, insurers noted a growing
responsibility for their health. Sharing the risk trend toward the expansion of coverage (for
with employees and empowering them to make example, higher benefit levels, reduction of
consumption and prevention decisions are exclusions, expansion of covered services).
important elements employers consider when
defining a health and wellness strategy. Many
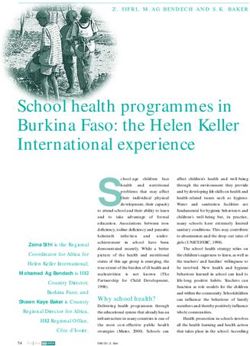
13Select the top 0% 20% 40% 60% 80% 100%
three risk factors 82%
80%
you believe Metabolic risk: high blood pressure,
78%
high cholesterol, high blood glucose
influence employer- 100%
91%
sponsored group
medical costs Dietary risk: high carbohydrates
71%
64%
the most. consumption, low fiber and vegetables, 71%
overweight/obesity, physical inactivity 64%
86%
39%
Emotional/mental risks: stress, 29%
51%
sleeping disorders 27%
23%
39%
Occupational risk: work-related risks, 43%
39%
ergonomics, occupational carcinogens 36%
27%
29%
3
Tobacco smoke: smoking, 21%
28%
secondhand smoke 45%
41%
18%
Environmental risk: urban 39%
indoor/outdoor air pollution, ozone, 9%
water sanitation, climate change 9%
5%
11%
Childhood and maternal under-nutrition 9%
11%
including maternity-care-related risks
The Burden of Risk:
18%
14%
an Insurer’s Look at 7%
6%
Rising Costs Alcohol and drug abuse 9%
0%
9%
Metabolic Risk, Poor Diet Trends Traffic, violence and safety: includes
4%
9%
Continue and Are Expected sexual abuse and intimate partner 1%
to Increase violence, unsafe sex 0%
5%
Global Asia Europe M iddle East/ Latin America
Africa (MEA) (LATAM)Global Asia Europe MEA LATAM
1 Metabolic risk Metabolic risk Metabolic risk Metabolic risk Metabolic risk
2 Dietary risk Dietary risk Dietary risk Dietary risk Dietary risk
3 Emotional/mental risks: Environmental risk: urban Emotional/mental risks Tobacco smoke Tobacco smoke
stress, sleeping disorders indoor/outdoor air pollution,
ozone, water sanitation,
climate change
4 Occupational risk: work- Occupational risk Occupational risk Occupational risk Occupational risk
related risks, ergonomics,
occupational carcinogens
5 Tobacco smoke: smoking, Emotional/mental risks Tobacco smoke Emotional/mental risks Emotional/mental risks
second-
hand smoke
This year’s survey also asked insurers to provide Offering a comprehensive medical plan to Emotional and mental health risks (such as stress
their perspective on the rising costs of healthcare. employees is no guarantee of optimal health or sleeping disorders) and occupational risks also
outcomes in the working population. Prevention ranked in the top five cost-influencers in each
Consistently across the world, metabolic risks and health risk management now play an region. Our fourth trend, “The Rise of Stress Is
such as high blood pressure, high cholesterol, important role in the administration of the health Evident,” will explore this area in more detail.
obesity/overweight and high blood glucose and benefits strategies. Wellness and prevention
were among the top three influencers of group programs that promote behavioral change and As we consider the top risk factors influencing
medical costs, followed by dietary risk (defined develop a culture of health will be the focus of group medical costs, we also asked insurers to
as high carbohydrate consumption, low fiber and high-performing organizations in the next few name the top components of cost under their
vegetable consumption, and physical inactivity). years in order to have in place the productivity book of group or overall business.
These data are supported by the belief that non- and health resources necessary to support
communicable diseases will increase healthcare business needs.5
costs to employers to a very large extent over
the next three years, along with the rising cost of
claims relating to circulatory system issues and
diabetes and its complications.
5
rossmeier J, Fabius R, Flynn J, Noeldner S, Fabius D, Goetzel R, Anderson D. “Linking Workplace Health Promotion Best Practices and Organizational Financial Performance: Tracking Market Performance of Companies With Highest Scores on
G
the HERO Scorecard,” Journal of Occupational and Environmental Medicine, Volume 58, Issue 1 (2016), pp. 16–23. 15In 2015, what were
the top three
components of 1%
cost under your 10%
book of group or
overall business?
33% 11%
13%
18% 14%
Hospital, Outpatient Outpatient Inpatient fees Inpatient Lab tests / Outpatient fees
surgery room, fees medicines medicines, diagnostics (specialists)
inpatient room, (physicians) materials,
inpatient prostheses,
equipment supplies
rental expenses
16Globally, the survey results pointed to hospital
and inpatient fees as the top components of
cost; however, in emerging markets, the higher-
ranked components included outpatient services
and medicines.
A closer look at the sources of cost reveals that
57% correspond to inpatient services and 43% to
outpatient services. Cost-management efforts
might focus on fees paid to clinical staff (32%)
or hospital rent fees (33%), and opportunities
remain to negotiate prices for medicines,
equipment and new technologies. Consumer-
driven programs aim to empower users to make
more informed choices, such as using closed
networks or leveraging referral programs based
on quality and cost-effectiveness. For example,
centers of excellence for specialized services,
including back surgery, cardiovascular conditions,
maternity (promoting natural birth) and cancer,
could be helpful in redirecting patients to
institutions where services are provided on the
basis of superior health outcomes, evidence-
based practices and cost-effectiveness.
170% 20% 40% 60% 80% 100%
To what extent does 46% 7% 15% 32% Global
your organization Coinsurance 39%
59%
4% 10%
9% 20%
47%
12% Asia
Europe
27% 18% 36% 19% MEA
perform the 45% 5% 14% 36% LATAM
60% 12% 15% 13% Global
following to help 54% 16% 18% 12% Asia
Deductibles/excesses 60% 13% 12% 15% Europe
manage plan 46% 36% 18% MEA
77% 5% 9% 9% LATAM
member health and/ 72% 7% 10% 11% Global
61% 7% 9% 23% Asia
or contain medical Negotiated rates with health providers
64%
78%
18%
6% 10%
18%
6% Europe
MEA
costs for employer- 82% 5% 9% 4% LATAM
61% 14% 14% 11% Global
sponsored medical Negotiated packaged/bundled pricing for 46%
69%
9% 25%
14% 9%
20%
8%
Asia
Europe
specific procedures
insurance? 55%
77%
18% 27%
23%
MEA
LATAM
67% 12% 11% 10% Global
Pre-authorization including assessment of 59% 9% 11% 21% Asia
61% 15% 16% 8% Europe
reasonableness of procedure/supply cost 91% 9% MEA
91% 9% LATAM
Pre-authorization including assessment of medical 53% 12% 21% 14% Global
43% 14% 18% 25% Asia
appropriateness of treatment undertaken and a
ctive 47% 10% 29% 14% Europe
82% 18% MEA
involvement in determination of treatment 77% 9% 14% LATAM
40% 14% 23% 23% Global
Access to a nurse or other clinician via telephone, 29% 11% 30% 30% Asia
49% 15% 19% 17% Europe
chat or email 27% 9% 18% 46% MEA
45% 18% 23% 14% LATAM
66% 11% 15% 8% Global
52% 14% 20% 14% Asia
Preferred provider networks 73% 7% 15% 5% Europe
46% 27% 18% 9% MEA
82% 9% 5% 4% LATAM
48% 9% 25% 18% Global
29% 11% 30% 30% Asia
Second-opinion services 56% 9% 23% 12% Europe
46% 9% 18% 27% MEA
68% 5% 27% LATAM
30% 14% 26% 30% Global
30% 7% 31% 32% Asia
Centers of excellence 29% 18% 26% 27% Europe
18% 18% 27% 37% MEA
36% 18% 18% 28% LATAM
11% 7% 21% 61% Global
13% 2% 28% 57% Asia
Support for medical tourism 9% 10% 16% 65% Europe
18% 18% 64% MEA
9% 14% 23% 54% LATAM
39% 20% 27% 14% Global
Education in order to make plan members smarter 52% 16% 18% 14% Asia
28% 21% 34% 17% Europe
consumers of healthcare 46% 27% 27% MEA
41% 23% 27% 9% LATAM
28% 15% 20% 37% Global
Provision of medical clinics near or onsite to 25% 9% 21% 45% Asia
28% 17% 15% 40% Europe
sponsoring employer sites 18% 46% 27% 9% MEA
45% 9% 32% 14% LATAM
23% 8% 27% 42% Global
Influencing government around legislative c
hanges/ 14% 7% 38% 41% Asia
28% 9% 21% 42% Europe
health reform 9% 9% 27% 55% MEA
27% 5% 23% 45% LATAM
This is an active part of We are experimenting and/or We are currently We have no plans to invest in
18 our current plan have developed plans to initiate considering this this area
management approach this within the next 24 monthsInsurers Are Expanding Their Role to Support Cost-containment
In many of the following categories, we see an To help understand best practices in this
increase in insurer action beyond the common area, employers can use the HERO Health
deductible and co-insurance approaches. For and Well-Being Best Practices Scorecard,
example, the survey revealed a much greater an online survey tool designed by the Health
percentage of insurers offering negotiated Enhancement Research Organization (HERO©) in
packaged/bundled pricing for specific collaboration with Mercer. Data collected from
procedures and an increase in preauthorization organizations that complete the International
practice and second-opinion services. More Scorecard (released in early 2016) will help
insurers are also taking a more active approach build country-specific normative databases to
to influencing government around legislative further the industry’s understanding of best-
changes/health reform. practice approaches to workplace health and
well-being around the world. This in turn will aid
Although insurers are taking these actions to organizations in strategic planning, program
control costs, employers should recognize that evaluation/design and gap analysis.
these strategies are not addressing employee
lifestyle choices. Employers can address the gap
by creating a work environment that supports
health and by educating individuals on the
importance of making healthy choices.
190% 20% 40% 60% 80% 100%
To what extent
44% 31% 11% 8% 6% Global
do plan members 20% 45% 18% 14% 3% Asia
Basic infrastructure for human health — safe water
covered under supply, sanitation, clean air
63% 18% 6% 6% 7% Europe
9% 55% 27% 9% MEA
your medical
59% 32% 9% LATAM
insurance plans
24% 46% 17% 8% 5%
have high-quality Global
14% 57% 16% 9% 4% Asia
and comprehensive Healthy food options 34% 39% 11% 7% 9% Europe
access to the 64% 27% 9% MEA
23% 36% 36% 5% LATAM
following, without
significant barriers 27% 37% 20% 11% 5% Global
A trained general clinician such as a family physician or 16% 45% 25% 12% 2% Asia
such as poor nurse to provide continuity, treat minor c
onditions and 37% 34% 20% 5% 4% Europe
environmental oversee all medical care 9% 36% 9% 46% MEA
conditions, a large 27% 27% 18% 9% 19% LATAM
out-of-pocket 37% 42% 19% 2% Global
cost, or treatment Medically-necessary specialist care, surgery
20% 54% 21% 5% Asia
49% 30% 20% 1% Europe
waiting list? and hospitalization
9% 73% 18% MEA
54% 41% 5% LATAM
39% 41% 16% 3% 1% Global
4
20% 50% 25% 3% 2% Asia
Lab tests and other diagnostics delivered out
45% 38% 15% 1%1% Europe
of hospital
27% 46% 9% 18% MEA
68% 27% 5% LATAM
29% 40% 15% 10% 6% Global
14% 48% 20% 13% 5% Asia
Safe, non-fraudulent medications delivered out
35% 39% 11% 6% 9% Europe
of hospital
9% 37% 18% 27% 9% MEA
50% 23% 18% 9% LATAM
21% 20% 30% 23% 6% Global
7% 14% 43% 27% 9% Asia
The Rising Effect of
Counseling and treatment for mental
29% 25% 21% 18% 7% Europe
health conditions
9% 18% 36% 37% MEA
Stress Is Evident 27% 18% 23% 32% LATAM
32% 39% 18% 10% 1% Global
13% 46% 27% 14%
Employers Must Recognize the
Asia
Maternity care including pre- and post delivery
36% 35% 19% 9% 1% Europe
d iagnostics and supplements
Need for Appropriate Mental 27% 46% 9% 18% MEA
Health Coverage 68% 32% LATAM
Very large extent Large extent Some extent Modest extent No extent at allAs trend three and our survey results indicated,
mental health (for example, stress-related issues)
and occupational risks were consistently viewed
as top contributors to cost. Several of our survey
questions attempted to gather information that
may reveal progress in these areas.
Compared to last year’s data on this topic, our
survey revealed some improvements in terms of
increased access to the above categories for
employees. Specifically, Latin America and
Europe both confirmed more accessibility to
safe, non-fraudulent medications delivered out
of hospitals. And in response to the belief that
emotional and mental health will contribute
significantly to healthcare costs, all regional
data indicate a small but growing trend to cover
more counseling and treatment for mental health
conditions. The European Agency for Safety and
Health at Work believes strongly in awareness
and understanding of work-related stress and
has even created an e-guide for managing these
issues in the workplace.6
6
European Agency for Safety and Health at Work. E-guide to managing stress and psychological risks, available at https://osha.europa.eu/en/tools-and-publications/e-guide-managing-stress-and-psychosocial-risks.
210% 20% 40% 60% 80% 100%
To what extent 11% 16% 29% 24% 20% Global
Vaccines recommended by local government health
does your standard authorities but not covered by public health s ystem/
7%
10%
16%
16% 25%
45%
21%
23%
28%
9% Asia
Europe
employer- social security 18%
18%
9%
23% 18%
55%
23%
18%
18%
MEA
LATAM
sponsored medical 16% 18% 30% 18% 18% Global
13% 23% 36% 16% 12% Asia
plan cover the Annual or periodic health check-ups not covered by
21% 13% 29% 16% 21% Europe
public health system/social security 9% 18% 18% 37% 18% MEA
following? 14% 23% 27% 18% 18% LATAM
6% 4% 29% 26% 35% Global
Biometrics performed onsite or near to an 2%4% 34% 30% 30% Asia
6% 1% 28% 21% 44% Europe
employer’s site 27% 27% 18% 28% MEA
18% 5% 27% 32% 18% LATAM
12% 15% 32% 20% 21% Global
7% 18% 30% 27% 18% Asia
Health risk assessment 13% 15% 32% 16% 24% Europe
9% 46% 18% 27% MEA
27% 9% 28% 18% 18% LATAM
7% 8% 22% 23% 40% Global
4% 5% 25% 25% 41% Asia
Personalized health coaching 5% 5% 23% 21% 46% Europe
9% 18% 18% 55% MEA
18% 23% 18% 27% 14% LATAM
12% 9% 26% 24% 29% Global
Access to preventive lifestyle programs like weight loss 9% 7% 32% 27% 25% Asia
13% 7% 25% 19% 36% Europe
or smoking cessation programs 18% 9% 27% 46% MEA
18% 18% 23% 36% 5% LATAM
8% 14% 25% 22% 31% Global
Case and disease management programs like 2% 16% 32% 27% 23% Asia
9% 9% 19% 22% 41% Europe
d iabetes or asthma management programs 27% 27% 18% 28% MEA
23% 23% 27% 9% 18% LATAM
7% 10% 24% 25% 34% Global
Access to personal counseling (e.g., employee 5% 7% 23% 29% 36% Asia
10% 10% 26% 20% 34% Europe
a ssistance plan) 9% 18% 36% 37% MEA
5% 13% 18% 32% 32% LATAM
12% 20% 23% 22% 23% Global
Wellness and health literature (e.g., health n
ewsletter, 13% 34% 27% 16% 10% Asia
10% 9% 21% 26% 34% Europe
website, health talks) 18% 18% 37% 27% MEA
18% 27% 23% 14% 18% LATAM
6% 12% 27% 21% 34% Global
9% 16% 28% 20% 27% Asia
Health fairs 1% 9% 29% 16% 45% Europe
9% 9% 46% 36% MEA
18% 18% 27% 23% 14% LATAM
5% 11% 24% 21% 39% Global
4% 11% 29% 19% 37% Asia
Onsite clinic in the client’s facility 4% 13% 21% 20% 42% Europe
18% 18% 18% 9% 37% MEA
9% 27% 37% 27% LATAM
7% 9% 25% 18% 41% Global
Access to maternity counselling/ 2% 9% 27% 19% 43% Asia
6% 6% 24% 15% 49% Europe
management programs 9% 27% 46% 18% MEA
23% 23% 23% 13% 18% LATAM
Very large extent Large extent Some extent Modest extent No extent at all
22Standard Employer-sponsored Medical
Plan Design Remains Largely Unchanged
Many of the approaches commonly offered in
plans today have been in place for some time.
Our survey data suggest that some approaches
(for example, providing wellness and health
literature) are offered slightly less than they
were in the past. That said, we recognize the
importance of providing health-awareness and
behavior-change support through in-house
specialists and specialty vendors. The lack of
large changes to employer-sponsored plan
design reported by the participating insurers may
be attributed to the growing number of experts
and third parties being used by employers to
support more proactive health management.
230% 20% 40% 60% 80% 100%
To what extent do
14% 22% 35% 21% 8% Global
you see employers Creating or expanding wellness programs
19% 25% 43% 11% 2% Asia
10% 21% 35% 23% 11%
engaging in the 45% 46% 9%
Europe
MEA
following to improve 18% 9% 36% 32% 5% LATAM
plan member health 6% 16% 29% 30% 19% Global
Creating or expanding onsite clinical services (e.g.,
and/or contain onsite medical facilities)
5% 18% 32% 29% 16% Asia
4% 14% 33% 27% 22% Europe
healthcare costs? 27% 18% 9% 46% MEA
9% 18% 18% 41% 14% LATAM
6% 22% 38% 25% 9% Global
Requiring employees to pay a portion of the premium or
5% 27% 32% 23% 13% Asia
raising their portion
4% 19% 44% 23% 10% Europe
9% 9% 46% 36% MEA
14% 27% 27% 27% 5% LATAM
16% 23% 33% 17% 11% Global
Requiring employees to pay a portion of claims 16% 20% 34% 17% 13% Asia
(e.g., coinsurance, deductibles) or raising 16% 23% 33% 17% 11% Europe
their portion 9% 18% 46% 18% 9% MEA
18% 32% 27% 14% 9% LATAM
16% 26% 28% 15% 15% Global
16% 30% 32% 11% 11% Asia
Placing monetary or frequency caps/limits on
13% 26% 23% 17% 21% Europe
covered services
36% 18% 28% 9% 9% MEA
9% 23% 36% 23% 9% LATAM
7% 25% 35% 19% 14% Global
5% 29% 32% 23% 11% Asia
Reducing coverage or increasing employee 8% 26% 36% 14% 16% Europe
contributions for dependent coverage 18% 27% 37% 18% MEA
5% 27% 36% 23% 9% LATAM
8% 22% 29% 20% 21% Global
5% 30% 34% 13% 18% Asia
Adding additional controls on use of specialists 13% 19% 26% 17% 25% Europe
9% 18% 36% 28% 9% MEA
and s elect other services, e.g., gate keepers,
18% 23% 36% 23% LATAM
referral requirements, pre-authorizations
5% 21% 33% 27% 14% Global
4% 23% 32% 25% 16% Asia
6% 19% 36% 29% 10% Europe
18% 27% 28% 9% 18% MEA
Implementing flexible benefit programs
23% 18% 41% 18% LATAM
4% 9% 20% 27% 40% Global
2% 9% 25% 29% 35% Asia
9% 9% 21% 27% 34% Europe
Implementing flexible benefit programs
18% 36% 46% MEA
5% 9% 13% 73% LATAM
Very large extent Large extent Some extent Modest extent No extent at all
24Cost-containment Ideas Are in Need of an
Innovative Approach
Employers seem to be operating on a “status quo”
approach, continuing to explore traditional ways
to increase employee accountability through
consumer-driven choices, requiring employees to
pay a portion of claims and/or premiums that they
may not have in the past.
But we are still not observing any increase in
coverages for mental health or other more
modern issues (such as benefits focused on
gender, ethnicity, cultural, generational or
sexual-orientation health concerns).
250% 20% 40% 60% 80% 100%
To what extent
17% 22% 36% 17% 8% Global
are you seeing 18% 20% 43% 14% 5% Asia
Preventive care 15% 28% 27% 19% 11% Europe
employers seeking 18% 9% 36% 28% 9% MEA
23% 14% 41% 18% 4% LATAM
to expand coverage
under their insured 12%
11%
21%
27%
26%
27%
21%
28%
20%
7%
Global
Asia
Primary care, e.g., coverage for treatment by a
medical plan for family doctor
14% 20% 26% 14% 26% Europe
18% 9% 36% 28% 9% MEA
the following? 9% 18% 18% 27% 28% LATAM
9% 9% 28% 26% 28% Global
4% 9% 37% 32% 18% Asia
Same- or opposite-gender domestic partner 9% 9% 21% 25% 36% Europe
27% 27% 46% MEA
27% 14% 27% 18% 14% LATAM
2% 6% 22% 23% 47% Global
2% 4% 23% 32% 39% Asia
Infertility 8% 20% 17% 55% Europe
36% 27% 37% MEA
9% 9% 14% 23% 45% LATAM
2% 1% 15% 17% 65% Global
Family planning assistance for same-gendercouples 4% 2% 18% 21% 55% Asia
1% 11% 13% 75% Europe
(e.g., surrogacy) 27% 27% 46% MEA
5% 9% 23% 63% LATAM
4% 15% 30% 33% 18% Global
4% 5% 30% 47% 14% Asia
Mental health 5% 20% 33% 22% 20% Europe
27% 46% 27% MEA
5% 27% 18% 36% 14% LATAM
15% 27% 27% 16% 15% Global
9% 38% 34% 12% 7% Asia
Prenatal and maternity care 11% 21% 26% 20% 22% Europe
27% 36% 28% 9% MEA
37% 18% 18% 18% 9% LATAM
5% 9% 21% 22% 43% Global
4% 12% 27% 32% 25% Asia
HIV/AIDS 3% 4% 14% 17% 62% Europe
18% 27% 9% 46% MEA
18% 14% 32% 23% 13% LATAM
5% 15% 26% 23% 31% Global
4% 12% 32% 27% 25% Asia
Women’s care program 4% 19% 20% 20% 37% Europe
18% 18% 37% 27% MEA
14% 9% 36% 23% 18% LATAM
12%1% 17% 70% Global
18% 14% 68% Asia
Gender reassignment procedure 1% 8% 16% 75% Europe
9% 9% 18% 64% MEA
18% 23% 59% LATAM
Very large extent Large extent Some extent Modest extent No extent at all
26We acknowledge the importance of diversity in
benefit design; employers are under increased
scrutiny to define and uphold standards that
sustain a healthy and tolerant environment, and
diversity promotes increased performance and
productivity. In our experience, organizations are
interested in implementing adequate benefits,
but employers should consider expanding
benefits offerings to address the concerns of the
increasingly diverse workforce in order to attract
and retain key talent. This likely means straying
from common market practice.
Occupational risks can be largely contained and
influenced by corporate leaders. We see the
most potential here to influence downstream
medical conditions that stem from occupational
risks, namely stress-management and wellness
programs designed with a preventative
strategy. The role of the work environment in
employee health and wellbeing should not be
underestimated. The burden of cost will continue
to affect employers through lost productivity
and the lower performance levels of an
unhealthy workforce.
27To what extent do 0% 10% 20% 30% 40% 50%
government(s) or 8%
25%
professional bodies Global 37%
23%
control the cost 7%
and quality of 4%
25%
Asia 41%
medical care 27%
4%
(e.g. treatment
9%
protocols)? 28%
Europe 38%
19%
8%
0%
18%
Middle East/Africa (MEA) 18%
27%
36%
14%
14%
Latin America (LATAM) 41%
32%
0%
5
Very large extent Large extent Some extent Modest extent No extent at all
Insurers reported an increase in organizations In Latin America, government control has been
considering or attempting to influence healthcare used to increase coverage or transfer more of
legislative change and reform. As we noted earlier, the healthcare burden to employer-sponsored
insurers continue to voice concerns about how plans, causing uncertainty in expectations about
changes to public/government social security future costs. Social security systems in this
schemes and/or health reform could affect the region are also transferring costs by reducing the
overall cost of healthcare. integration of services between private plans and
The Role of Government social security, or by preventing access to social
and/or Industry Compared to last year’s data, the responses to
this year’s survey suggest more consistently
security until private-plan coverage options are
exhausted. Employers are looking for alternative
Associations in that governments or professional bodies will paths that provide more predictable benefits
Influencing Health evidently have “some control” over the cost and
quality of medical care. This is particularly true
costs, including through the addition of choice.
in Latin America and Europe, whereas in the
Insurers and Employers Can Play a
Middle East, government is not seen as much
Role in Health Reform of a player in healthcare.In the US, for example, controlling health benefit
cost growth has taken on new urgency in recent Do you track and report paid claims by ICD10 or another diagnostic category? If your response is “no,”
years as employers have ramped up cost-saving which classification system do you use?
measures in anticipation of the excise or
0% 5% 10% 15% 20%
“Cadillac” tax, one of the Affordable Care Act’s
7%
(ACA’s) final provisions.7 Originally slated to 11%
ICD9 8%
go into effect in 2018, in December 2015 the 0%
0%
government announced that implementation Global Use of ICD 10
2%
would be delayed until 2020. Still, employer actions 5%
Current Procedural Terminology category 0%
to reduce their exposure to the 40% excise tax 0% Yes No
0% 63% 37%
helped hold growth in health benefits cost per
employee to just 3.8% in 2015, for a third straight 3%
2%
year of increases below 4%. Enrollment in high- Local government catalog 1%
0%
14%
deductible, consumer-directed health plans,
which grown steadily during this period, reached 3%
4%
a milestone 25% of all covered employees in 2015 Local social security catalog 4%
0%
as the percentage of large employers offering 0%
these lower-cost plans jumped from 48% to 59%. 1%
0%
National Insurance Association catalog 1%
0%
What Can Be Done With the Data 0%
15%
14%
Global data-tracking tools used by the survey Your own catalog 18%
9%
respondents have remained largely the same 5%
as last year, with more than half of all insurers 5%
4%
surveyed tracking the diagnoses of paid claims Other classification system 6%
9%
using the International Classification of Disease 0%
version 10 (ICD10). 2%
0%
None used 4%
9%
0%
Global Asia Europe M iddle East/ Latin America
Africa (MEA) (LATAM)
7
For information on US trends, refer to Mercer’s National Survey of Employer-sponsored Health Plans 2015 report.
29General Conclusions
The results of the survey reflected that most
governments today are not providing adequate
healthcare systems to cope with growing demand.
Insurers are doing what they can to control costs,
but employers must also do their part. Unless
employers act to address certain endemic health
concerns in their workforces, they face lowered
levels of productivity and performance.
The role of the employer must continue to
evolve. Organizations worldwide must attempt to
influence government provision of appropriate
healthcare services and fill the gaps by offering
employer-sponsored health improvement
programs and changing the work environment in
support of health and well-being. Designing benefit
offerings that address individual needs, provide
portability, and offer access to transparent
healthcare are challenges faced by many
employers as they endeavor to attract, retain and
6
maintain a healthy, high-performing workforce.
Conclusion
Change Is on the HorizonInsurers from
Region Country Region Country
49 countries
Asia China Europe Belgium
participated in this
Hong Kong Denmark
year’s survey.
India France
Indonesia Greece
Malaysia Hungary
Philippines Ireland
Singapore Italy
South Korea Latvia
Taiwan Lithuania
Thailand Netherlands
Vietnam Norway
Americas Argentina Poland
Brazil Portugal
Canada Romania
Chile Russia
Colombia Serbia
Dominican Republic Spain
Mexico Sweden
Panama Switzerland
Peru Turkey
Middle East & Africa Egypt Ukraine
Burkina Faso United Kingdom
Ghana
Malawi
Mali
Qatar
Saudi Arabia
About This Survey
Appendix
31The following Country Insurance company Country Insurance company
insurers agreed Africa Metropolitan Health Insurance Ghana Limited Hong Kong Manulife (International) Limited
to having their Africa Metropolitan Malawi Hong Kong MassMutual Asia Ltd
names published Argentina Grupo Sancor Seguros Hong Kong Sun Life Hong Kong Limited
as participants Argentina MEDIFE A.C. Hungary Vienna Life Vienna Insurance Group Biztosító Zrt.
in the survey, Belgium AXA Belgium Indonesia Aetna
whereas 81 insurers Belgium DKV Belgium SA/NV Indonesia PT Asuransi Reliance Indonesia
participated on a Brazil Allianz Saúde Indonesia PT FWD Life Indonesia
confidential basis. Brazil Care Plus Medicina Assistencial LTDA Ireland Laya Healthcare
Brazil SulAmérica Seguros SA Italy Reale Mutua di Assicurazioni
Canada Green Shield Canada Latvia BTA Baltic Insurance Company AAS
Canada Sun Life Assurance Company of Canada Lithuania Gjensidige
Chile Chilena Consolidada Malaysia AIA Bhd
China 友邦保险有限公司上海分公司 (American International Malaysia TOKIO MARINE INSURANS BERHAD
Assurance Company Limited, Shanghai Branch) Norway Gjensidige Forsikring
China Generali China Life Insurance Company, Ltd. Norway If Skadeforsikring NUF
China MHS China (Shanghai) Enterprise Services Co., Ltd. Norway Storebrand Helseforsikring AS
China Ping An Annuity Insurance Company, Shanghai Branch Norway Vertikal Helseassistanse AS
Colombia Allianz Seguros Panama MAPFRE PANAMÁ
Colombia AXA COLPATRIA Medicina Prepagada Panama Pan-American Life Insurance Group
Denmark Codan Peru Rimac S.A. EPS
Denmark Dansk Sundhedssikring A/S Philippines Avega Managed Care, Inc.
Denmark Mølholm Forsikring A/S Philippines MEDICARD PHILIPPINES INC.
Denmark Skandia Philippines The Philippine American Life and General Insurance Company
Greece Allianz Hellas SA Philippines United Coconut Planters Life Assurance Corporation
Greece Generali Hellas Poland Compensa TU SA Vienna Insurance Group
Greece International Life Poland LMG Försäkrings AB
Greece MetLife Poland PZU Życie S.A.
Hong Kong Aetna Global Benefits (Asia Pacific) Limited [in Hong Kong: Portugal Allianz Portugal
Starr International Insurance (Asia) Ltd.]
Portugal Companhia de Seguros Tranquilidade
Hong Kong Assicurazioni Generali S.p.A. Hong Kong Branch
Portugal Generali-Companhia de Seguros, S.A.
Hong Kong AXA Hong Kong
Portugal Groupama Seguros S.A.
Hong Kong Blue Cross (Asia-Pacific) Insurance Limited
Portugal Multicare — Seguros de Saúde, S. A
Hong Kong Bupa (Asia) Limited
Portugal VICTORIA Seguros
Hong Kong Federal Insurance Company
Russia Allianz Life
Hong Kong Liberty International Insurance Limited
Russia Ingosstrakh Insurance Company
32Country Insurance company
About Mercer Marsh Benefits
Russia OJSC Alfa Strakhovanie
The Mercer Marsh Benefits network is a combination of
Russia RESO-GARANTIA
Mercer and Marsh local offices around the world, plus country
Russia VTB Insurance
correspondents who have been selected based on specific
Saudi Arabia Allianz Saudi Fransi Cooperative Insurance Company
criteria. Through our locally established businesses, we have
Singapore Aetna International Singapore
a unique common platform that allows us to serve clients with
Singapore Aviva Ltd.
global consistency and locally unique solutions.
Singapore AXA Life Insurance Singapore Pte Ltd / AXA Insurance
Singapore Pte Ltd
Mercer and Marsh are two of the Marsh & McLennan
Sweden Euro Accident Health & Care Insurance AB
Companies, together with Guy Carpenter and Oliver Wyman.
Sweden Länsförsäkringar
Sweden Skandia
This information is not intended to be taken as advice
Switzerland Helsana Versicherungen AG regarding any individual situation and should not be relied
Switzerland Sanitas upon as such. Statements concerning tax, accounting and/
Switzerland Sympany or legal matters are general observations based solely on our
Taiwan China Life Insurance Co., Ltd experience as insurance brokers and risk consultants and
Taiwan Fubon Life Insurance Co., Ltd should not be relied on as legal, tax or accounting advice. You
Taiwan Nan Shan Life Insurance Co., Ltd
should contact your legal, accounting, tax and other advisors
regarding specific coverage and other issues. The information
Taiwan Shin Kong Life Insurance Company
contained in this publication is based on sources we believe
Thailand Krungthai-AXA Life Insurance Public Company Limited
are reliable, but we make no representation or warranty
Thailand Tokio Marine Life Insurance (Thailand) PCL
as to its accuracy. All insurance coverage is subject to the
Ukraine AXA Insurance (Ukraine)
terms, conditions and exclusions of the applicable individual
Ukraine The European Insurance Alliance, Private Joint Stock policies. Marsh and Mercer cannot provide any assurance that
Company
insurance can be obtained for any particular client or for any
Ukraine INGO Ukraine particular risk. Marsh and Mercer make no representations or
Ukraine JSIC "Illichivske" warranties, expressed or implied, concerning the application
Ukraine PROVIDNA, Ins. Co. Ukraine of policy wordings or the financial condition or solvency of
Ukraine PZU Ukraine insurers or reinsurers.
United Kingdom Aviva Health UK Limited
United Kingdom AXA PPP Healthcare
United Kingdom Cigna UK HealthCare Benefits
United Kingdom VitalityHealth
Vietnam Bao Viet Saigon Insurance
Vietnam Petro Vietnam Insurance Corporation
33For further information, please contact your local Mercer Marsh Benefits office. Copyright 2016 Mercer LLC. All rights reserved. 21525-MB
You can also read