16th Annual Nursing Symposium: Lessons from the Heart - April 7, 2017 - The Center for Continuing Professional Development
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The Center for Continuing Professional Development presents 16th Annual Nursing Symposium: Lessons from the Heart April 7, 2017 Mohegan Sun Pocono Wilkes-Barre, PA
16th Annual Nursing Symposium: Lessons from the Heart
April 7, 2017
Schedule
7:00 am Registration/Continental Breakfast
7:50 am Welcome and Introductions
8:00 am Patient Experience – What does it Mean to Nurses?
Dr. Venditti
9:00 am Demystifying 12 Lead EKG
Mr. Mullen, RN
10:00 am Nutrition Break
10:15 am Heart Failure – What’s New?
Dr. Qureshi
11:00 am Luncheon will be provided
12:00 pm Hot Topics in Cardiology (Lightening Round)
Broken Heart Syndrome
Ms. Reiner, BSN
Cardiac Testing: Why do they do which test?
Ms. Solomon, MS, ACSM-CEP
Funny Little Beats – Name that Rhythm!
Ms. Grudzinski-Cabelly, MSN
1:00 pm Nurses – Self Care
Dr. Maani-Fogelman
2:00 pm Nutrition Break
2:15 pm Palliative Care for the Cardiac Patient – Who and When?
Dr. Behm
3:15 pm Door Prizes/Evaluations/Adjournment
*Topics/Speakers are subject to change*
Faculty and Planning Committee Disclosure
As an accredited provider of continuing education for health professionals, Geisinger Health
System must ensure balance, independence, objectivity, and scientific rigor in each of its
educational activities. All persons in a position to control the educational content of a sponsored
activity (e.g. planners, presenters) must disclose to the audience any relevant financial
relationships that they have with commercial interests. Relevant financial relationships may
include such things as grants, research support, employment, consulting, stock ownership, or
speakers’ bureau membership. Any identified conflicts of interest must be resolved prior to the
activity.
The intent of this disclosure is not to prevent planners or presenters with financial relationships
from participating, but rather to provide learners with information on which they can make
informed judgments regarding the educational content. It remains for the audience to determine
whether an individual’s relationships influence the presentation with regard to exposition or
conclusion.
If you perceive commercial bias, please note it in the activity evaluations, notify onsite staff
persons, and/or call our anonymous toll free hotline at 1-877-557-7447.
The following persons in a position to control educational content of this activity have
disclosed no relevant financial relationships with commercial interests:
Bertrand Behm, MD John Mullen, RN
Cinde Bower Stout, RN, MHA Ataul Qureshi, MD
Stacey Grudzinski-Cabelly, MSN Amy Reiner, BSN
Judy Haines, BSN, RN, BC, CHFN Julie Solomon, MS, ACSM-CEP
Patricia Maani-Fogelman, DNP Denise Venditti, DNP, MHA, RN, NEA-BC, FACHE
Commercial Support
None
Objectives:
At the completion of this course, the participant should be able to:
• demonstrate self-care measurements to decrease stress effect of work in nursing
• define and describe the impact of Patient Care Experience and its effect on Health Care
Costs
• identify how and when Palliative Care is an appropriate intervention in the Cardiovascular
Patient
• describe changes in care of the Heart Failure Patients
• describe and identify 12 Lead EKG Patterns in STEMI
Accreditation
In support of improving patient care, Geisinger Health System is
jointly accredited by the Accreditation Council for Continuing
Medical Education (ACCME), the Accreditation Council for Pharmacy
Education (ACPE), and the American Nurses Credentialing Center
(ANCC), to provide continuing education for the healthcare team.
Designation Statement
Geisinger Health System designates this activity for 5.75 contact hours for nurses. Nurses should
only claim credit commensurate with the extent of their participation in the educational activity.
EXHIBITORS
Thank you to the following companies for their
generous support of this educational activity.
3M Infection Prevention Division
Abbvie
Amgen
Astellas Pharma
Invitae Genetics
Novartis
Thank you for attending today’s conference. You can use the link below to the
on-line evaluation form, which will also be e-mailed to you after the activity. If
you prefer to use your Smart Phone and/or device, you can click on the QR Code
below to access the evaluation form. Participants must submit an evaluation in
order for the activity to be thoroughly evaluated. Activities that are not
sufficiently evaluated may not be eligible for credit.
If you do not have the QR Reader on your phone, it is a free app you can
download.
Thank you.
https://go.geisinger.org/LessonsEval17
Certificates are no longer provided for registrants. Please follow the instructions
below how to access your credits.
Geisinger employees – you can locate your credits two different ways. You can
log into GOALS and click on the link My CME Transcript or you can log onto our
CPD Calendar and click the link entitled My Transcript.
Non-Geisinger participants – you can locate your credits by going to our CPD
Calendar: http://go.geisinger.org/MyTranscript and click on the My Transcript
link. You can select the date range that you want to view for your Transcript.
Any difficulties and/or questions, please contact the Center for Continuing
Professional Development at 570-271-6692.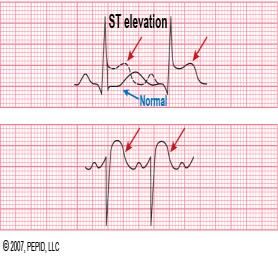
Patient Experience:
What does it mean to nurses?
April 7, 2017 Denise A. Venditti, DNP, MHA, RN, NEA-BC, FACHE
VP Patient Experience, Geisinger Health System
1
This presentation uses live polling on your smart phone:
http://davenditti.participoll.com/
2
Agenda
• What does Patient Experience mean to nurses?
• What do nurses mean to the Patient Experience?
• Understanding/appreciating your “sphere of influence”
• What will you do differently tomorrow?
3
1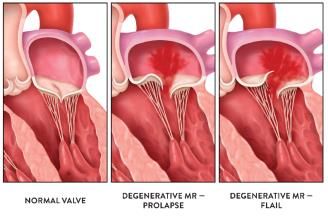
What does Patient
Experience mean
to nurses?
Patient Experience Survey for Geisinger Nurses
Brief (7 questions), informal, voluntary, confidential survey (via Survey Monkey)
sent to licensed nurses all 10 hospitals and outpatient areas across
Geisinger Health system (came from Nurse Educators)
Survey was open for 10 days (March 10 – March 20, 2017)
325 total responses
Purpose: to better understand our (Geisinger) nurses’ perceptions about the
Patient Experience and hear specific examples/stories (not formal research)
5
Patient Experience Survey for Geisinger Nurses
Demographics - License Demographics - Age
RN – Full time 254 78% Age 20-29 80 25%
RN – Part time 38 11% Age 30-39 69 21%
RN - Flex 18 6%
Age 40-49 69 21%
LPN – Full time 12 4%
Age 50-59 68 21%
LPN – Part time 2 .62%
LPN - Retired 1 .31% Age 60+ 38 12%
TOTAL 325 100% TOTAL 324 100%
6
2
Patient Experience Survey for Geisinger Nurses
Demographics - # years in Nursing Demographics – Current Specialty
0-5 100 31% Critical Care 75 25%
6-10 63 20% ED 46 15%
11-15 35 11% OR 41 14%
16-20 19 6% Med-Surg 40 13%
21-25 24 7% Peds 23 8%
25+ 82 25% OB 41 6%
Total 323 100% Other 44 14%
Total 310 100%
7
As a nurse, please define what “Patient Experience” means to you?
Themes or key words:
8
Beryl Institute Definition of Patient Experience
9
3
Live Polling Question
Does your personal definition of Patient Experience include the
patient’s family?
A. Yes
B. No
10
Based on your recent interactions/observations with patients/families,
what aspect of the healthcare experience are they most dissatisfied with?
Themes or key words:
11
As a nurse, what specific actions do you take every day to create a
“great” patient experience?
Themes or key words:
12
4
Live Polling Question
Do you make a conscious effort to sit with your patients when having a
conversion with them?
A. Yes
B. No
C. There is rarely a chair available
13
What do nurses
mean to the Patient
Experience?
GALLUP Poll (December 2016) Honesty/Ethics in Professions
December 7-11, 2016
Source: http://www.gallup.com/poll/1654/Honesty-Ethics-Professions.aspx 15
5Rate different professions on warmth & competence
http://www.businessinsider.com/what-professions-are-most-respected-2016-12 16
In your current work environment, what position or role has the most
influence on the Patient Experience?
Role Responses
Nurses 210 68%
Team/everyone 35 11%
Physician 21 7%
Management/Administration 4 1%
Other responses 41 13%
Total 310 100%
17
In your current work environment, On a scale of 0 -10, please indicate how
much influence nurses have on the overall Patient Experience?
0 = no influence, 10 = significant influence
Nursing's Influence on the
Overall Patient Experience
46%
17%
15%
12%
5% 3%
0% 0% 1% 0% 1%
0 1 2 3 4 5 6 7 8 9 10
18
6But what do our patients say about our degree of influence?
Correlation is a statistical measurement of the
relationship between two variables. Possible
correlations range from +1 to –1. A zero correlation
indicates that there is no relationship between the
variables.
A correlation of –1 indicates a perfect negative
correlation, meaning that as one variable goes up,
the other goes down.
A correlation of +1 indicates a perfect positive
correlation, meaning that both variables move in
the same direction together.
19
HCAHPS Patient-Level Correlations
20
HCAHPS – Communication with Nurses
• During this hospital stay, how often did nurses treat you with
courtesy and respect?
• During this hospital stay, how often did nurses listen carefully to
you?
• During this hospital stay, how often did nurses explain things in
a way you could understand?
21
7Overall Hospital Rating
Recommend the hospital “Using any number from 0 to 10,
0.76 where 0 is the worst hospital possible
and 10 is the best hospital possible,
Communication with Nurses what number would you use to rate
0.64 this hospital during your stay?”
Pain Management
0.54
Responsiveness of Hospital staff
0.51
Communication with Doctors
0.50
22
Recommend the Hospital
Overall Hospital Rating “Would you recommend this hospital
0.76
to your friends and family?”
Communication with Nurses
0.57
Pain Management
0.48
Care Transition Measure
0.45
Communication with Doctors
0.45
23
Pain Management
Communication with Nurses
“During this hospital stay, how often was
your pain well controlled?”
0.56
During this hospital stay, how often dud the
Overall Hospital Rating hospital staff do everything they could to
0.54 help you with your pain?
Recommend the Hospital
0.48
Responsiveness of Hospital staff
0.48
Communication with Doctors
0.44
24
8Responsiveness of Hospital Staff
Communication with Nurses
“During this hospital stay, after you pressed
0.56
the call button, how often did you get help
as soon as you wanted it?”
Overall Hospital Rating
0.51
Pain Management
0.48
Recommend the Hospital
0.44
Communication with Doctors
0.36
25
Communication
with Doctors
Recommend the
Hospital
Pain
Management
With great
power….
.
Overall Hospital Responsiveness
Comes great
Rating of Hospital Staff
responsibility
Communication
about
Medications
26
Nursing Communication and Patient Safety
When patients were ask how well the nursing staff communicated, the
hospitals whose patients rated them the lowest (in the bottom 10%) for nursing
communication had on average 27% more overall patient safety events
compared to the highest rated (in the top 10%).
The following patient safety events were most related to nursing communication:
Post-op bloodstream infections were 77% higher in the lowest-rated hospitals.
Bed sores were 76% higher in the lowest-rated hospitals.
Catheter-related infections were 58% higher in the lowest-rated hospitals.
DVTs following surgery were 53% higher in the lowest-rated hospitals.
https://www.hospitals.healthgrades.com/CPM/assets/File/HealthGradesPatientSafetySatisfactionReport2012.pdf
27
9Understanding/appreciating
your “sphere of influence”
As a patient, what is most important to you when evaluating your own
health care experiences?
Themes or key words:
1) Staff attitude, respect, dignity, friendly, caring, privacy, personalized 134
2) Communication, listening, explanation, kept informed 113
3) Competence, skills, experience, knowledge, quality 61
4) Having enough time, timely care, access to care 36
5) Having enough staff or how many patients per nurse 5
As savvy, well-educated healthcare consumers, we (nurses) are fairly harsh
critics….
29
As a patient, what is most important to you when evaluating your own
health care experiences?
30
10What does Patient Experience mean to you?
“Treat the patient
as you would treat the person
whom you love the most”
31
Thank you for your attention today.
Thank you for all that you do, everyday.
33
11The Magical Pencil of
Cardiology
Or if you are a State Official: Tactical
12 Lead EKG Interpretation
Objectives
To identify acute ST elevations on a standard 12
lead EKG
To understand which myocardial wall is at risk
based on those changes
Understand the impact of specific MI’s and the
care involved in them
1Why bother ?
Differential of care- not all chest pain is created
equal
Time is Muscle remains a truism
Growing number of cath lab protocols
New equipment makes a 12 lead easy to obtain
Monitor the effectiveness of your interventions
Knowing what type of M.I. can alter your care
Do not forget the basics
M.O.N.A.
There will be 2 types of pain
Lead placement can make all the difference
The 12 lead is not a treatment
Calm, attentive bedside manner
General Principals
Limited types of M.I’s make your life easier
1) anterior wall
2) posterior wall
3) lateral wall
4) inferior wall
2Learn ST elevations first
Why ST elevations ?
ST elevations are never normal
Although T wave changes first it returns to
normal quickly
ST elevations hang around after the pain is gone
Need at least 2mm ( 2 blocks up ) elevation to
be clinically significant. For now
3You can do it
Take your time, be systematic- do not guess
The pencil becomes the resultant electrical
vector
Let the pencil point out the wall
Sometimes there will be a “note to self “
And now the process
Limb leads
Start with the pencil flat on your chest pointing
from the right shoulder towards the left- this is
Lead 1
Now rotate the pencil until it points towards the
left leg- this is Lead 2
Continue rotating the pencil limb to limb ending
with AVF pointing straight down
What wall is the pencil point on?
V leads
Place the point of the pencil on your chest, like
you have been shot with an arrow
V1- 4th intercostal right sternal border then on
around to V6- 5th intercostal mid axillary line
What wall does the pencil point stick in?
4Things that make you go hmmm
What about the posterior wall ?
No direct lead, infer from reciprocal changes
ST depressions are ‘ripples’ from another wall
ST depressions throughout the precordium =
ripples from the posterior wall
For now the only ST depressions to worry about
Special situations
RV infarct
1) can be seen with a right sided EKG
2) can be inferred from an IMI with
hypotension
3)only MI where volume is your friend
a) Starlings law
5Special situations
Septal M.I.
1) special subset of anterior M.I.
2) ST elevation in V2-V3
3) possible because it has it’s own artery
4) endangers the main wiring harness of the
heart
Special situations
Pacemakers
1) make the 12 lead non-diagnostic
2) can use a magnet to inhibit the pacer
3) you’ll have to rely on the story/ history
6Special situations
Pericarditis
1) SSCP not relieved with morphine or
nitrates
2) pain relieved with position, deep breath
and NSAID’s
3) piddling ST elevations everywhere
The Pencil Method
Go lead to lead and look for ST elevations
If there is an elevation, write down the lead #
After all the leads are reviewed, use the pencil to
tell you what wall(s) are involved
Remember, AVR is a garbage lead
2mm elevations in contiguous leads and you are
on to something
Practice session
Take your time, do not jump ahead
All things in the fullness of time
Not all ekg’s are abnormal
7Let’s play
89
10
Silence in the audience please
11What will bite you
Anterior M.I.- pukers code, loss of pump, AV
blocks
Inferior M.I.- puke on a good day, ectopy and
congestive failure
VT-VF in the first 24-48 hrs non- predictive of
mortality or morbidity
12Questions?
13MitraClip- A New Way to Fix MR
Amy Reiner MSN, RN, CCRN
Clinical Nurse Educator
CVT-ICU, CVT-SCU, eICU
1
Mitral Regurgitation
MR is the most common type of heart
valve disease, affecting nearly 1 in
10 people aged 75 years and
older— approximately 4 million
people in the U.S. alone.
This progressive condition occurs
when the flaps of the heart’s mitral
valve do not close completely,
causing blood to flow backward into
the left atrium of the heart. This
requires the heart to work harder
and may raise the risk of irregular
heartbeats, stroke, and heart
failure, which can be life-
threatening.
2
MITRACLIP: What is it
MitraClip is a new way to fix MR. It is the world’s first transcatheter mitral valve
repair therapy. It provides a proven treatment option for select patients with
significant degenerative MR who are too high-risk for open-heart surgery and
do not have other treatment options available to them.
It was first implanted in 2003 in trials and in 2013 was the first FDA
commercially approved alternative to mitral valve regurgitation surgery.
3
1INDICATIONS
The MitraClip® NT Clip Delivery System is indicated for the percutaneous
reduction of significant symptomatic mitral regurgitation (MR ≥ 3+) due to
primary abnormality of the mitral apparatus [degenerative MR] in patients
who have been determined to be at prohibitive risk for mitral valve surgery by
a heart team, which includes a cardiac surgeon experienced in mitral valve
surgery and a cardiologist experienced in mitral valve disease, and in whom
existing comorbidities would not preclude the expected benefit from reduction
of the mitral regurgitation.
4
CONTRAINDICATIONS
The MitraClip® NT Clip Delivery System is contraindicated in patients with the
following conditions:
• Patients who cannot tolerate procedural anticoagulation or post procedural
anti-platelet regimen
• Active endocarditis of the mitral valve
• Rheumatic mitral valve disease
• Evidence of intracardiac, inferior vena cava (IVC) or femoral venous
thrombus
5
RELATIVE CONTRAINDICATIONS
• Porcelain aorta or extensively calcified ascending aorta.
• Frailty (assessed by in-person cardiac surgeon consultation)
• Hostile chest
• Severe liver disease / cirrhosis (MELD Score >12)
• Severe pulmonary hypertension (systolic pulmonary artery pressure >2/3 systemic pressure)
• Unusual extenuating circumstance, such as right ventricular dysfunction with severe tricuspid
regurgitation, chemotherapy for malignancy, major bleeding diathesis, immobility, AIDS, severe
dementia, high risk of aspiration, internal mammary artery (IMA) at high risk of injury, etc.
6
2HOW DO THEY DO IT?!!!!!!
They insert the catheter in
the femoral vein and thread
it through the vena cava to
the right atrium. They then
push through the septum to
the left atrium
7
8
The device is then
placed by
inserting through
the valve.
9
310
Once through the valve the top
of the clip is lowered and the
leaflets are pinched
between. This narrows the
opening thus reducing the
regurgitation of blood. The
implanting provider will have
a TEE done to ensure good
placement prior to removing
the implementation device.
Up to 3 clips may be place
depending on the anatomy
and need
11
The MitraClip can
be repositioned if
needed prior to the
removal of the
deploying device
12
4The MitraClip will
eventually be
covered with fibrous
tissue bridge.
13
POTENTIAL COMPLICATIONS AND ADVERSE EFFECTS
Allergic reaction Failure to deliver MitraClip® NT to the intended site
Aneurysm or pseudo-aneurysm Failure to retrieve MitraClip® NT System components
Arrhythmias Hematoma
Atrial septal defect requiring intervention Hypotension/hypertension
Arterio-venous fistula Infection
Bleeding Injury to mitral valve complicating or preventing later surgical repair
Cardiac arrest MitraClip® NT erosion, migration or malposition
Cardiac perforation MitraClip® NT Device thrombosis
Cardiac tamponade/Pericardial Effusion MitraClip® NT System component(s) embolization
Chordal entanglement/rupture Mitral stenosis
Death Myocardial infarction
Deep venous thrombus (DVT) Pulmonary congestion
Dislodgement of previously implanted devices Pulmonary thrombo-embolism
Dizziness Single leaflet device attachment (SLDA)
Dyskinesia Stroke or transient ischemic attack (TIA)
Dyspnea Vascular trauma, dissection or occlusion or Vessel spasm
Emboli (air, thrombus, MitraClip® NT Device) Vessel perforation or laceration
Emergency cardiac surgery Worsening heart failure
Endocarditis Worsening mitral regurgitation
Esophageal irritation or Esophageal perforation or stricture
14
15
516
17
References
18
6Cardiac Stress Testing
Choosing the best Modality
Julie Solomon, MS
Case Manager, Cardiology Imaging Program
Geisinger Medical Center
Indications for Stress Testing
Evaluation for symptoms
Angina, chest pain, DOE
Evaluation of drug therapy for CAD patients
Evaluation for arrhythmias
Exercise capacity assessment
Prognosis/risk stratification
Exercise prescription, cardiac rehab
Evaluation of perioperative risk for non-cardiac
surgery
Absolute Contraindications
for Stress Testing
Acute CHF
Unstable angina
Severe HTN (>200/100)
Symptomatic severe AS
Suspected aortic dissection
Recent systemic or pulmonary embolus
Recent MI (within 2 weeks)
Recent CVA or TIA (within 4 weeks)
1Absolute Contraindications cont.
High grade carotid disease
Acute myocarditis
Left Main disease >50%
Significant change in resting EKG
Populations for Testing
Anyone 8 years or older
Ambulatory patients
Treadmill Stress test
Exercise Echocardiogram
Nuclear Stress SPECT
Metabolic (mV02) Stress test
Populations cont.
Non-ambulatory patients
Dobutamine Stress Echocardiogram
Pharmacologic Nuclear SPECT
Lexiscan or Dobutamine
Advanced Imaging tests
Calcium Score
Cardiac CT
Cardiac MRI
Cardiac Stress MRI
2Treadmill Stress test
EKG analysis
Arrhythmia analysis
Symptom evaluation
Exercise capacity
Blood pressure
response
Heart rate response
Comparison to norms
for age/gender
Exercise Echocardiogram
Resting and Stress
Echocardiogram
analysis
EF, wall motion and
valvular anatomy
EKG analysis
Arrhythmia analysis
Symptom evaluation
Exercise capacity
BP/HR response
Exercise Echocardiogram cont.
Rest and stress images are compared side by
side
Normal response is for myocardial contractility to
increase with stress
Ischemic response causes hypokinesis, akinesis,
or dyskinesis of the segments
3Relative Contraindications for
Exercise Echo
LBBB
Ventricular paced rhythm
Advanced Heart Block
Myocardial Stress SPECT
Rest and Stress
SPECT analysis
EF, wall motion
Uses technetium (Tc)-
99m sestamibi
EKG analysis
Arrhythmia analysis
Symptom evaluation
Exercise capacity
BP/HR response
Myocardial Stress SPECT cont.
Perfusion defects that are present during
exercise but not at rest indicate myocardial
ischemia (reversible)
Perfusion defects that are present at rest and
during exercise suggest previous MI (fixed)
4Metabolic (mV02 max) test
Used for:
Congenital heart
abnormalities
Risk stratification for
heart transplant/CHF
Risk stratification for
pre-op lung resection
Differentiate between
cardiovascular and
pulmonary limitations
Metabolic (mV02 max) test cont.
12 Lead EKG hook-up
Ramping treadmill protocol
Screens for cardiac or pulmonary limitations to
stress
Obtains V02max, measured METs, Anaerobic
Threshold (AT), Breathing Reserve, Respiratory
Exchange Ratio (RER), SP02, VO2/HR
RER >1.09 represents maximal aerobic effort
Dobutamine Stress Echocardiogram
Resting and Stress
Echocardiogram
analysis
EF, wall motion and
valvular anatomy
EKG analysis
Arrhythmia analysis
Blood pressure
response
Heart rate response
5DSE Protocol
Dobutamine infused over an 18 minute protocol
5 mcg/kg/min to 50 mcg/kg/min
An adrenergic agent that increases myocardial
oxygen demand by increasing myocardial
contractility, HR, and BP
Echo images obtained each stage
Atropine given for additional HR response (up to
2 mg)
Lopressor given for reversal, HTN, abnormal
EKG, symptoms
Relative Contraindication for DSE
LBBB
Ventricular paced rhythm
Advanced Heart Block
History of paroxysmal A-fib, not on current
anticoagulation therapy
History of closed angle glaucoma
Pharmacologic Myocardial Stress
SPECT
Rest and Stress
SPECT analysis
EF, wall motion
EKG analysis
Arrhythmia analysis
Blood pressure response
Preferred for LBBB or
ventricular paced rhythm
6Pharmacologic SPECT cont.
Agents used
Lexiscan – a coronary vasodilator, causes a rapid
increase in coronary blood flow for short duration
Can cause bronchospasm, SA and AV nodal block, sinus
bradycardia
Common side effects include SOB, headache, flushing, chest
pain, dizziness, nausea, abdominal pain
Aminophylline to reverse side effects
Dobutamine – andrenergic agent, increases
contractility, HR, BP
Contraindications for Lexiscan
Advanced heart block or SA node dysfunction,
without functioning pacemaker
Theophylline therapy – inhibits Lexiscan
Caffeine use within 24 hrs. – inhibits Lexiscan
Dipyridamole therapy – increases the activity of
Lexiscan (Aggrenox, Tegretol)
Severe or uncontrolled asthma/COPD – can
substitute Dobutamine protocol if appropriate
Calcium Score only
Screening for CAD
Asymptomatic patients
Strong family history of CAD
Detection of coronary calcium in the coronary
arteries
Findings expressed as Calcium Score
Not covered by insurance
$200 out of pocket expense
Offered at GMC, GWV, Grays Woods
7Cardiac CT
Calcium Score
Detection of coronary atherosclerosis
Visualize heart anatomy
Etiology of cardiomyopathy
Offered at GMC, GWV, Grays Woods
Findings of CAD 50% » invasive Cath
Contraindications
GFR 20, patient age >65
Images of Cardiac CT
Cardiac MRI
Myocardial viability early after MI (Cardiac Stress MRI
Ischemic evaluation
Ideal for:
morbidly obese patients (BMI >40)
patients with history of limited quality studies
patients with low EF or resting WMA on Echo
Offered at GMC
Contraindications
Pacemaker or other implantable devices
Severe claustrophobia
GFRQuestions?
101
2
3
4
5
6
*&!%$#@!
(HEALTHCARE BURNOUT)
I KNOW IT WHEN I SEE IT…
Patricia Maani-Fogelman, DNP
Department of Thoracic/Pulmonary Medicine
Pulmonary-Palliative Clinic
Director, GMC Nursing Grand Rounds
National Faculty, American Association of Colleges of Nursing (AACN) ELNEC Project
Associate Professor of Nursing, Columbia University
SELF ASSESSMENT
Ask yourself the following:
• Have you become cynical or critical at work?
• Do you drag yourself to work and/or have trouble getting started once
you arrive?
• Have you become irritable/impatient with co-workers, patients, families?
• Do you lack the energy to be consistently productive?
• Do you lack satisfaction from your achievements?
• Do you feel disillusioned about your job?
• Are you using food, drugs or alcohol to feel better (or to simply not feel?)
• Have your sleep habits or appetite changed?
• Are you troubled by unexplained headaches, backaches or other
physical complaints?
1BACKGROUND DATA
• 2007/American J Resp and CCM: 24% ICU nurses and 14% general
nurses tested positive for symptoms of post-traumatic stress
disorder.
• Nursing long been considered one of the most stressful professions
(National Institute for Occupational Safety and Health at the Centers
for Disease Control and Prevention, 2012.)
• Nurses and researchers say it comes down to organizational
problems in hospitals worldwide: cuts in staffing, wages, insufficient
resources, poor managerial support, lack of empowerment, lack of
gratitude, etc.
• Highly bureaucratic setting: top-down organizations that do not seek
out clinicians' solutions for problem-solving in patient care.
STRESS
• Stress contributes to outcomes that threaten
organizational success:
• Physical injuries at work
• Absenteeism
• Turnover
• Reduced productivity
• Diminished job satisfaction
• Low morale
• Burnout.
Job stress is believed to account for approximately 50% of all
workplace absences and for as much as 40% of employee turnover.
Roberts R, Grubb PL, Grosch JW. Alleviating job stress in nurses: approaches to reducing job stress in nurses. Medscape 2012 Jun:
http://www.medscape.com/viewarticle/765974
STRESS RELATED OUTCOMES
• Considerable losses to industry:
• Employers losing up to $60 billion per year.
• Significant financial costs associated with job stress also
are absorbed by the US economy.
• Econometric analyses show that healthcare expenditures
have increased nearly 50% for workers who perceive their
jobs as stressful and nearly 200% for those who report high
levels of job stress and depression.
• Per national estimates, the total cost of job stress incurred
by the US economy ranges from $250-$300 billion annually.
Roberts R, Grubb PL, Grosch JW. Alleviating job stress in nurses: approaches to reducing job stress in nurses.
Medscape 2012 Jun: http://www.medscape.com/viewarticle/765974
2BURNOUT & PATIENT EXPERIENCE
• Patients cared for on units that the nurses felt had:
• Adequate staff
• Good administrative support for nursing care
• Good relations between doctors and nurses
were more 2x likely as other patients to report high
satisfaction w/their care
• These nurses reported significantly lower burnout
• The level of nurse burnout on hospital units directly affects
patient satisfaction.
Vahey DC, Aiken LH, Sloane DM, Clarke SP, Vargas D. Nurse Burnout and Patient Satisfaction. Medical care. 2004;42(2 Suppl):II57-II66.
doi:10.1097/01.mlr.0000109126.50398.5a.
CAUSES
• Lack of control:
• inability to influence decisions that affect your job (schedule,
assignments or workload, lack of the resources.)
• Unclear job expectations:
• If you're unclear about the degree of authority you have or what
your supervisor or others expect from you, you're not likely to
feel comfortable at work.
• Dysfunctional workplace dynamics:
• work with a bully? Feeling undermined or micromanaged?
• Mismatch in values:
• your values differ from the way your employer’s values.
CAUSES
• Poor job fit: does the job fit your interests and skills?
• If not, it might become stressful over time.
• Extremes of activity: monotony vs chaos
• constant energy required for both…can be exhausting.
• Lack of social support
• those who feel isolated at work (or in personal life) may feel
more stress
• Work-life imbalance
• work consumes so much time, you lack energy to spend time
with your family and friends.
3CAUSES
• Hospitals think of nurses as a cost to be cut and not as a revenue
stream.
• Cynda Rushton, Professor of Nursing and Bioethics @Johns Hopkins
Berman Institute of Bioethics and School of Nursing:
"There is a mindset among some administrators that nurses are easily
replaceable commodities — a nurse is a nurse is a nurse.“
• Nearly 20% new RNs leave within the first year for the same job
elsewhere, or a different job in a different organization.
• Thus, organizations aren't investing enough in their nursing staff.
Kovner CT, Brewer CS, Fatehi, F, Jun, J. What Does Nurse Turnover Rate Mean and What Is the Rate? Policy, Politics, & Nursing Practice; Vol 15, Issue 3-4, 2014.
BURNING OUT
• Seems to have little to do with hours worked or the ability to balance personal life
with work:
the factor predictive of higher risk was practicing a specialty that offered
front-line access to care (CCM, family medicine, ER Medicine)
• A significant proportion of doctors feel trapped:
• thwarted by the limited time they are allowed to spend with patients
• stymied by ever-changing rules set by insurers/payers on what we can
prescribe or offer as treatment
• frustrated that any gains in efficiency offered by EMR are soon offset by
numerous, newly devised administrative tasks that must also be completed on
the computer.
• In this setting, “doctors are losing their inspiration, and that is a very frightening
thing.”
From: Shanafelt TD, Boone S, Tan L, et al. Burnout and Satisfaction With Work-Life Balance Among US Physicians Relative to the General US Population. Arch
Intern Med. 2012;172(18):1377-1385. doi:10.1001/archinternmed.2012.3199.
BURN OUT
• Constellation of: emotional exhaustion, detachment
and a low sense of accomplishment – is widespread
among medical students and doctors-in-training.
• Nearly half of these aspiring doctors end up
becoming burned out over the course of their
schooling
• Many lose or have a loss in their sense of empathy for
others and may succumb to unprofessional behavior.
http://www.nytimes.com/2008/10/31/health/chen10-30.html?em
4BURN OUT
• Dyrbye et al (2006) @ Mayo Clinic:
• nearly half of the 545 medical students surveyed suffered from
burnout
• Scope of research was then expanded nationally:
• Responses from 2,248 medical students at seven medical
schools across the country revealed (again) nearly half of
the students surveyed met the criteria for burnout.
• A more ominous finding:
11 percent of all the students surveyed also reported having
suicidal thoughts in the past year.
NURSING DEFICIT
Bureau of Labor Statistics’ Employment Projections 2012:
• Registered Nursing (RN) is listed among the top
occupations in terms of job growth through 2022.
• RN workforce is expected to grow from 2.71 million
in 2012 to 3.24 million in 2022, an increase of
526,800 or 19%.
• 525,000 replacements nurses will be needed in the
workforce to meet the number of job openings for
nurses (due to growth/replacements) to 1.05 million
by 2022.
ARE WE PREPARED?
• US Registered Nurse Workforce Report Card & Shortage Forecast
(Jan 2012, Am J Med Qual):
• Shortage of registered nurses is projected to spread across the
country between 2009 and 2030.
• State-by-state analysis: RN shortage will be most intense in
the South and West.
• IOM (Oct 2010), The Future of Nursing:
• increase number of baccalaureate-prepared nurses in workforce
to 80% and double the population of nurses with doctoral
degrees.
current nursing workforce falls far short of these
recommendations with only 55% of registered nurses prepared at
the baccalaureate or graduate degree level.
5HOW TO HANDLE BURNOUT
• Manage the stressors that contribute to job burnout:
• identify what's fueling your feelings burnout to help develop a
plan to address the issues.
• Evaluate your options and discuss specific concerns with your
supervisor:
• Work together to change expectations or reach compromises
or solutions.
• Job share, telecommuting or flex time options
• Would it help to establish a mentoring relationship?
• What are the options for continuing education/professional
development?
HOW TO HANDLE BURNOUT
Adjust your attitude:
• If you've become cynical, consider ways to
improve your outlook.
• Rediscover enjoyable aspects of your work.
• Recognize co-workers for valuable contributions
or a job well-done.
• Take short breaks throughout the day.
• Spend time away from work doing things you
enjoy.
HOW TO HANDLE BURNOUT
Seek support:
• Reaching out to co-workers, friends or loved ones,
support and collaboration
helps us cope w/job stress and feelings of
burnout.
• Employee Assistance Program (EAP)
• Unit based debriefing after complex cases,
traumas, loss of long term patients or difficult
pt/family/team dynamics
6TREATMENT: WHAT CAN HELP US
• Without decreasing the total hours worked or the number of
patients we must see, hospital Systems might:
• Restructure clinics so that we spend more time with patients and less
time on the phone getting authorization from insurers or in front of a
computer completing administrative tasks.
“If people work in an environment where they believe there is
meaning, they will put up with a lot. It goes beyond the significant
personal consequences for an individual provider. It affects whom
patients can see when they are sick, the quality of care they receive
and their safety.”
PREVENTION: NURSING SCHOOL
• Recognize the potential for and early signs of burnout, which is a
gradual process (not all personalities are prone to it); instructors should
watch for potential warning signs:
• the feeling of being underappreciated for a job well done
• unclear job demands
• Insufficient sleep
• taking on too many projects without help
• lack of close relationships
• high achieving/”Type A” personalities
• need to control everything constantly
• a pessimistic view of themselves.
• Teach resiliency and self-care: Educators have a responsibility to
help nurses understand ways to keep themselves physically and
emotionally healthy and to recognize the signs and symptoms of
burnout.
• 'Nurses, heal thyselves' should no longer be status quo.
PREVENTION: FOR HOSPITALS
• Create a positive work environment for nurses: nurses must be
able to express themselves in a professional manner about
their workload and work environment — and actually have
their issues heard.
• Hospitals should have an open door policy and listen when
there are serious concerns.
• Hospitals should put policies in place to limit nurse-to-patient
ratios.
• Address staffing concerns immediately:
• Consider new grad or agency hires in severe situations
• Understand that when nurses know their patients have safe
staffing, there is less stress coming home with them.
7PREVENTION: FOR NURSES
• Take regular breaks: Adopt a daily ritual to help with stress.
• Journal, exercise/yoga/meditation, reading: find whatever trips your
trigger to chill out and relax and put it in your ritual, do it each day.
• Disconnect from technology for 10 to 15 minutes.
• During the technology break, do some deep breathing, sit outside and
focus on nothing but nature, or meditate and think about your mantra.
• Seek out support: We need outlets to channel their thoughts,
feelings and emotions. Remember that you have an employee
assistance program to confidentially.
http://www.beckershospitalreview.com/human-capital-and-risk/7-ways-hospitals-nurses-and-nursing-schools-can-combat-nurse-
burnout.html; Accessed 03.01.17
PREVENTION
On-boarding interview:
• As part of the credentialing process, physicians participate in an initial
interview with a therapist.
• The embedding strategy offers a nonthreatening opportunity to establish
a relationship between the new physician and the mental health
professional.
• The therapist initiates a discussion about health and self-care practices,
invites the physician to consider his or her professional development and
future goals, and encourages the physician to tap into resources to
support growth and development.
• Self-care is presented not as an option but as a best practice, therefore
normalizing and integrating the personal with the professional.
HEART MATH INSTITUTE
WWW.HEARTMATH.ORG
• Research and develop reliable, scientifically based tools to bridge the
connection between heart/mind and deepen people’s connection with the
hearts of others.
• This empowers people to greatly reduce stress, increase resilience and
unlock their natural intuitive guidance for making better choices.
• User-friendly mental and emotional self-regulation tools and techniques
provide benefits in the moment and over sustained periods.
• Enable people everywhere to break through to greater levels of personal
balance, creativity, intuitive insight and fulfillment.
• Training and education programs worldwide, among diverse cultures:
major corporations, government and social-service agencies, military,
schools and universities, hospitals and health-care professionals and law
enforcement agencies.
8HELPFUL STRATEGIES
• Helpful strategies include:
• changing the work assignment or shift
• recommending time off or reducing overtime hours
• encouraging attendance at a conference
• becoming involved in a project of interest.
• Nurses in high stress areas can also benefit from
stress reducers such as meditation or heart math.
• In serious cases, the nurse may need to be referred
to an employee assistance program.
RESILIENCY TRAINING
• The daily demands of a complicated medical practice challenge
providers to concentrate on the task before them, yet be able to
recover rapidly and confront new problems and situations.
• Resiliency when confronted by adversity is supported by a holistic
approach to improved overall health and well-being
• Resiliency training teaches providers to strategically incorporate into
their lifestyles:
• Nutrition
• Exercise
• Self-reflection
• Mutually supportive relationships
• Good health practices.
http://www.medscape.com/viewarticle/782514_5
MARTIN SELIGMAN, PHD
DIRECTOR, PENN RESILIENCE PROGRAM
UNIVERSITY OF PENNSYLVANIA
• US Army: Master Resilience Training/Ready and Resilient Mission
• 1.1 million people where trauma is more common and more severe
than in any corporate setting
• Struggles with depression, PTSD, burnout ?learned helplessness
• Program aims to teach the [psychological] skills to stop the
downward spiral that can follow repeated losses/perceived failures
• $145 million initiative: Comprehensive Soldier Fitness (CSF), consists
of:
• test for psychological fitness
• self-improvement courses available following the test
• “master resilience training” (MRT) for drill sergeants, based on
PERMA: positive emotion, engagement, relationships, meaning,
and accomplishment—the building blocks of resilience and
growth.
9RACHEL REMEN, MD
CLINICAL PROFESSOR OF FAMILY & COMMUNITY MEDICINE
UCSF SCHOOL OF MEDICINE
FOUNDER/DIRECTOR, THE INSTITUTE FOR THE STUDY OF HEALTH AND
ILLNESS
• “The Healer’s Art” -- medical students learn how to offer stronger
emotional support to their patients, their colleagues, and
themselves.
• “The Healer’s Art” has spread to 47 medical schools, including
institutions in Slovenia, Israel, and Sri Lanka.
• As part of the class, students write their own versions of the
Hippocratic oath:
Challenge: If you wrote your own Hippocratic Oath, what
would it say?
MEANING IN MEDICINE
• Developed ~1990 by Rachel Remen, MD:
• Physician-to-physician facilitated dialogues
• Speak openly about personal experiences in the everyday
practice of medicine that remind participants of why they
became doctors and encourage them to see their colleagues
as people.
• The conversations serve an important purpose:
• Enhance trust, goodwill, and collaboration among the
physicians
• A "win" for everyone -- the individual physician, the
patients, and the healthcare system in which they function.
DR. REMEN
• Since 1992, the Institute has provided education and support for
health professionals to bring their hearts into their work and are
dedicated to practicing a medicine of service, human connection
and compassionate healing.
• For Physicians: Remembering the Heart of Medicine (online
community) accessed via http://theheartofmedicine.org/
• Courses to date have reached into the lives of thousands of
physicians, medical educators, medical students, nurses and
others in the healing professions:
• helping them to hold to their values, humanity, excellence, and
renew their commitment to themselves, to their patients and to
medicine.
10DR. REMEN: THE HEALER’S ART
• Innovative discovery model curriculum in values clarification
and professionalism for first and second year medical students
• Offered annually at 70+ US medical schools as well as medical
schools around the world.
• Physicians and nurses are looking for ways to connect with
each other and find their place of truth in the changing arena
of medicine:
• ISHI helps clinicians initiate Finding Meaning groups:
• Finding Meaning in Medicine for Physicians
• Finding Meaning in Nursing for Nurses
• Finding Meaning in Service for other Healthcare Professionals
JAMES GORDON, MD
DIRECTOR, CENTER FOR MIND-BODY MEDICINE
GEORGETOWN UNIVERSITY
• Works with practicing physicians but program has broader
application for nursing as well!
• Program has an enduring theme: “Physicians, heal each other.”
• The heart of the work is about self-care as foundation for
being with & caring for others.
• Physicians must open up and “shed the armor of detachment”
if they are to serve their patients and feel personally fulfilled.
• Participants work together in small groups: learn meditation,
techniques for self-expression with the goals understanding the
personal struggles they’ll face in school and over their careers.
JAMES GORDON, MD
DIRECTOR, CENTER FOR MIND-BODY MEDICINE
GEORGETOWN UNIVERSITY
• Crucial to the program is bearing witness to each
other as they move through challenges and pain.
• Result: Increase in the compassion that medical
students feel for each other.
• Presently used at 18+ medical schools nationally.
“Our groups hold out a hope of community to people
who may feel isolated and unfulfilled in their hospitals
and clinics and private offices.”
11A SOFTER APPROACH
• Code Lavender
• a code the hospital staff can call for themselves when they are being
overloaded by stress and traumatic events on a particular work day.
• When triggered, the staff member gets a chaplain consult, reiki
treatment, some down time and a lavender ribbon on their arm to tell
everyone they are having a rough day.
• Code lavender started by Earl Bakken at North Hawaii Community
Hospital in Waimea in 2008 and has been reported on most recently
in the Cleveland Clinic System.
• Meditation
• Alternative therapies: physical stress reduction
DEATH & DYING
• Our over-exposure to death and dying can often be a trigger for worsening
burnout: major cause of occupational stress
• As part of a reflective process, allowing for healing and acceptance, consider
the following:
“Before we leave the room, could we just take a moment to stop as a
group and honor this person that was in the bed?
Before they came here, they had a life, and they had family. They were
loved, and they loved other people.
[Let's] take that time to recognize that right now, and also take the time
to honor and recognize the efforts we put in to try to save them, and
do that in such a way in silence so that we can each have our own
voice.”
http://www.acphospitalist.org/archives/2016/01/q-and-a-the-pause.htm
COMPASSION = HEALING
• Compassion doesn’t require more time, just
more attention.
• 40 seconds of compassionate communication
from us could reduce patient anxiety.
• “Our power to heal is far less limited than our
power to cure. Healing is not a relationship
between an expert and a problem … it is a
relationship between human beings”
12• If we develop our courage and generosity to listen
when there are no clear answers, and to bear witness
to losses, patient and provider satisfaction rises
reducing burnout for us, reassurance/comfort to
the patient.
• Taking care of ourselves allows us to take better care
of others.
• Do not lose yourself in the work of service to others.
BLESSING OF THE HANDS
BE KIND TO ONE AND OTHER
Thank You.
13Integrating Palliative Care into a
Comprehensive Advanced Heart Failure
Care Model
16th Annual Nursing Symposium: Lessons
from the Heart
Bertrand Behm, MD
Geisinger Health System
April, 2017
Financial Dislosure
No relevant financial conflicts to disclose
Stages of Heart Failure
Krum H, Abraham WT. Lancet (2009) 373: 941-
965
1The Burden of Advanced Heart Failure (AHF)
More then one million Americans affected
$ 32 Billion estimated cost
• One in 9 deaths in 2009 included heart failure as
contributing cause.
About half of the patients who develop heart failure
die within 5 years of diagnosis.
Crude prevalence 6.6 million in 2010 with ~670,000
newly diagnosed annually
Centers for Disease Control and Prevention. (2014) Division for Heart Disease and Stroke Prevention. Data Fact Sheet.
Retrieved August 15, 2014, from CDC website:
http://www.cdc.gov/DHDSP/data_statistics/fact_sheets/fs_heart_failure.htm
Magnitude of the problem
■ Projected increase of an additional 3 million by 2030
■ One in 9 deaths has HF mentioned on the death
certificate
■ One in five die within one year of diagnosis
■ Hospital discharges increased about 10% in last
decade to ~1.1M
■ Incremental health care spending of 39.2B
■ Most expensive DRG
AHA, Circ: Heart Disease and Stroke
Statistics 2012 update
Prevalence of heart failure by sex and age (National
Health and Nutrition Examination Survey: 2007–
2010).
Source: National Center for Health Statistics and
National Heart, Lung, and Blood Institute.
2Burden of Disease
Symptom Cancer COPD HF
Pain 35-96% 34-77% 41-78%
Fatigue 32-90% 68-80% 69-82%
Dyspnea 10-70% 90-95% 60-88%
Depression 3-77% 37-71% 9-56%
Insomnia 9-69% 55-65% 36-48%
Solano et al. J Pain Sympt Man 2006;31 :58-69
AHF patients desire …
Good communication about the nature of the disease
Better care coordination
More comprehensible information
Having an adequate care plan and health service
availability
Having options for less aggressive treatment with a focus
on QoL
Low et al J Card Fail 2011; 17: 231-251
3Palliative Care Definition
“…is applicable early in the course of illness, in conjunction with
other therapies that are intended to prolong life, … and
includes those investigations needed to better understand and
manage distressing clinical complications.”
World Health Organization, WHO Definition of Palliative Care, Updated 2002. Retrieved July 15, 2014,
from WHO website: http : //www.who.int/cancer/palliative/definition/en/
Palliative care
Interdisciplinary care that aims to relieve suffering and
improve quality of life for patients with serious illness and
their families
It is provided at the same time with other disease directed
therapies
Overview of Palliative Care in the US
Began as hospice grassroots movement in 1970s
1982 introduction of federal Medicare Hospice Benefit
Broader palliative care movement emerged in 1990s
2004 National Consensus Project for Quality Palliative
Care
2008 ABMS approval of palliative medicine as a bona fide
subspecialty
4Integrating Palliative Care Into Disease Trajectory
Guideline Recommendations for Palliative Care in
AHF
2013 ACC/AHA Guidelines for Treatment of Heart Failure
“Patient and family education…about the role of palliative and
hospice care services with re- evaluation for changing clinical
status is recommended for heart failure patients”
J Am Coll Cardiol. 2013;62(16):e147-e239.
Guideline Recommendations for Palliative Care in
AHF
HRS Expert Consensus Statement on the Management of
(CIEDs) in Patients Nearing End of Life or Requesting
Withdrawal of Therapy
Referral to palliative care occurs at the time of
“progression of cardiac disease, including repeated
hospitalizations for heart failure and/or arrhythmias”
Heart Rhythm 2010; 7(7) 1008-1026
5Challenges to initiate a palliative medicine referral
• Unpredictable heart failure trajectory
• Concern over “destroying hope”
• Not familiar with principles and practice of palliative
medicine
• Conflicting conceptualization of palliative medicine as a
system of care delivery as opposed to a philosophy of
care
Hupvey, JE, Penrod, J, Fogg, J. Heart Failure and Palliative Care: Implications in practice. J Palliat
Med 2009;12:531-536
Challenges to initiate palliative medicine referral
• Misperception by cardiologists of PC: Reluctance of
cardiologists to “hand over” patient, denial of death
• PC: Lack of HF knowledge (stopping meds,)
“cancer focus”
• Patient reluctance to accept palliative care
• System wide lack of coordination of services, confusion
over the role of advance practice heart failure nurse
specialists
Selman et al. Pall Med 2007;21:385-90
What are the benefits of palliative care for advanced
heart failure patients ?
1. Clinical Quality
2. Patient and Family Preferences
3. Complexity of HF Trajectory
4. Financial Imperative
61. Clinical Quality
Recognition of the need for better quality care for anyone
dealing with a serious and complex illness
2. Patient and Family Preferences
There is a concordance of patient and family wishes
• Pain and symptom control
• Avoid inappropriate prolongation of the dying
process
• Maximize function
• Achieve a sense of control
• Relieve burdens on family
• Strengthen relationships with loved ones
Singer et al. JAMA 1999;281(2):163-168.
Caldwell PH, Arthur HM, Demers C. Can J Cardiol 2007; 23(10): 791-796
What unfortunately Happens …
Based on National Data on the Experience of
Dying in 5 Tertiary Care Teaching Hospitals:
Objective was to improve end-of-life decision making for
seriously ill patients
9105 adults hospitalized with one or more of nine life-
threatening diagnoses
6-month mortality rate of 47 %
38 percent of patients who died spent at least 10 days in
an intensive care unit
7What unfortunately happens…
% of 5176 patients reporting moderate to severe
pain between days 8-12 of hospitalization:
Illness % of patients reporting
pain
Colon Cancer 60%
Liver Failure 60%
Lung Cancer 57%
MOSF + Cancer 53%
MOSF + Sepsis 52%
COPD 44%
CHF 43%
Desbiens & Wu. JAGS 2000;48:S183-186.
End-of-Life Care in Heart Failure Patients
In the last 6 months of life:
80% of patients hospitalized
Average days in hospital: 20
Average days in ICU: 4.6
Costs rising: $36,216
Readmissions common
36% die within one year of HF-related hospitalization
Unroe et al. Arch Int Med 2011;171:196-203
Curtis et al. Arch Intern Med 2008;168:2481-88
Palliative Care Effects on Clinical Outcomes
Comparing Hospice and Nonhospice
Patient Survival Among Patients Who
Die Within a Three-Year Window
Connor et al. J Pain Symptom Manage, 33 (2007) 33:
Survival curve for patients with CHF. 238–246
8You can also read

















































