QUALITY TIME: THE VALUE OF GETTING IT RIGHT - NOCA WEBINAR 2021 #NOCA2021 - Cloud Object ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

NOCA WEBINAR 2021
QUALITY TIME:
THE VALUE OF GETTING IT RIGHT
2ND FEBRUARY 2021 • 14:00 - 16:00
@noca_irl #NOCA2021
In association with RCSI Charter Week
GENERAL INFORMATION
VENUE
This year’s event will take place virtually.
Pre-registration is essential at https://rcsi.eventsair.com/charter-meeting-2021/noca2021
TWITTER
We welcome you to Tweet about the conference using the details below
@noca_irl #NOCA2021
CPD
The Conference has been awarded the following credits:
RCSI: 3 PCS credits, 2 CNMEU credits
NMBI: tbc
A CPD cert will be issued to you electronically within a month of the conference
In association with RCSI Charter Week
2 @noca_irl #NOCA2021
A MESSAGE FROM OUR CLINICAL DIRECTOR
AND EXECUTIVE DIRECTOR
Dear Colleagues
You are all very welcome to our annual conference which
celebrates and promotes the importance of quality
improvement through national clinical audit.
It is difficult to find the words to summarise the past year.
The impact of a global pandemic has affected us all in many
ways but it’s fair to say the biggest impact has been on our front
line colleagues.
To each and every one of you, we want to say thank you and
it is our privilege to support you in improving the care and
outcomes for your patients.
Like every other organisation, NOCA too was impacted by
DR BRIAN CREEDON COLLETTE TULLY
COVID 19 and a number of projects were deferred. However,
CLINICAL DIRECTOR EXECUTIVE DIRECTOR
on the positive side, we have truly transformed into a virtual
NOCA NOCA
organisation being able to continue our day to day work
as well as host meetings, training, strategy workshops and
now our annual conference virtually. But we are all looking everyone who has supported NOCA in becoming the
forward to the day when we can meet again. recognised and trusted body in Ireland to drive quality
Some key successes to highlight this year include: improvement through national clinical audit. Over the next 5
years, NOCA will continue to provide high quality and timely
• Transfer of the National Paediatric Mortality Register (NPMR) data across the healthcare system, expand our audit portfolio
from Childrens Health Ireland at Temple Street to NOCA and collaborate with other national partners to minimise the
• Publication of the first national report for the Irish burden of data collection.
National Audit of Stroke (INAS) We would like thank everyone who has contributed to
• First successful HRB Grant for INAS in collaboration with our annual conference event - speakers, sponsors, RCSI,
RCSI attendees. A special thank you to everyone who entered our
Quality Improvement Champion Award this year. Inspirational
• Published the first in a series of rapid learning COVID 19
commitment to improving care for your patients even in the
reports summarising the impact on activity and care from
most difficult of times.
the IHFD
Finally, we would like to thank everyone who makes these
• Irish National Orthopaedic Register (INOR) went live in
audits happen; the NOCA Team, a power house of expertise
the first private hospital site, Blackrock Clinic
and commitment, the NOCA Board, HSE, RCSI, Department
• First Major Trauma Audit Paediatric Report of Health and most importantly our clinical leads, audit
• Commencement of our first new audit feasibility study in committee members, public patient representatives and the
the management of deteriorating patients audit teams in each hospital who have continued to collect
and use national clinical audit data to drive improvement for
• Fast tracked the implementation of the national critical
their patients.
care Bed Information System (BIS) for critical care beds
to support the management of care during COVID 19. The We look forward to the year ahead with the launch of our
BIS, led by the Irish National ICU Audit Team and Brid new strategy and returning to a new way of working post
Moran, our Information Manager, is providing twice daily COVID 19. Until then, stay safe.
updates on COVID 19 patients in ICU as well as supporting Regards
hospitals and the ambulance service with bed availability
information.
In 2021, we will publish the first national reports for the
INOR, Irish Heart Attack Audit (IHAA) and Irish National ICU
Paediatric audit.
Dr Brian Creedon Collette Tully
We are also currently working on our new 5-year strategy. Clinical Director Executive Director
As our current strategy concludes, we would like to thank NOCA NOCA
3 @noca_irl #NOCA2021
AGENDA
NOCA WEBINAR 2021
QUALITY TIME: THE VALUE OF GETTING IT RIGHT
2ND FEBRUARY 2021
TIME SPEAKER PRESENTATION
Mr Kenneth Mealy,
14:00 Welcome Address
NOCA Chair
Moderator: Dr Philip Crowley, National Director, National Quality Improvement Team (NQIT), HSE
Prof Pat O’Mahony,
Chair of HIQA and
14:15 - 14:45 Keynote: Quality assures best outcomes
Director Clinical Research
Development Ireland
Dr Joan Power,
14:45 - 15:05 Consultant Haematologist, Quality improvement – shifting the paradigm
Irish Blood Transfusion Service
Dr Rory Dwyer,
Clinical Lead,
15:05 - 15:25 COVID19: how ICU responded
Irish National ICU Audit,
NOCA
Dr Brian Creedon,
15:25 - 15:40 Clinical Director, NOCA reflections and looking to the future
NOCA
Collette Tully,
15:40 - 16:00 Executive Director, NOCA Quality Improvement Champion Award & Closing address
NOCA
4 @noca_irl #NOCA2021
CONFERENCE SPEAKER, CHAIR AND
MODERATOR BIOGRAPHIES
Dr Brian Creedon
Clinical Director, NOCA
Dr Brian Creedon has practiced as a Consultant Palliative Medicine Physician in the South East
for 10 years. He has served in a number of leadership roles, both regionally and nationally,
including Chairman of the Irish Palliative Medicine Consultants Association and president of
the Waterford Clinical Society. His primary place of work is University Hospital Waterford
@CreedonBrian which is a designated National Cancer Centre and university teaching hospital. He has an
ongoing active commitment to medical education and has held teaching positions with 4
medical schools and currently serves as a Senior Clinical Lecturer with both University College
Cork and the Royal College of Surgeons in Ireland. Brian is passionate about service user/
patient driven quality improvement and patient involvement in service development through
co-design. He recently chaired a working group to produce a National Review of Clinical
Audit for the Irish healthcare system. Aligned with this interest, he is the Clinical Director for
the National Office of Clinical Audit (NOCA) which has led the inception of over 15 national
clinical audits to improve patient outcomes. Brian was appointed the National Clinical Lead for
Palliative Care in Ireland in 2018 and leads the national clinical programme for palliative care
determining best models of care, supported by evidence based guidelines and efficient use
of resources. For over a decade Brian has pioneered the development of national outcomes
measures for palliative care and, having secured a Senior Fellowship supported by Atlantic
Philanthropies, has led with his colleague, Dr Mike Lucey, the implementation of the Australian
conceived Palliative Care Outcome Collaboration throughout Ireland as a clinical tool and
quality improvement method. In his “spare” time, Brian is an avid climber/adventurer.
Dr Philip Crowley
National Director, HSE National Quality Improvement Team
Dr Philip Crowley is the National Director for Quality Improvement in the HSE. He is a graduate
of the Advanced Training Programme in Healthcare Delivery Improvement, Intermountain
Healthcare Salt Lake City Utah. He leads a national team that supports the health service
in improving care through the application of a framework for improving quality. He is a
@crowley_philip doctor who works part-time as a GP. He worked for five years in Nicaragua, trained in public
@NationalQI health in Newcastle Upon Tyne and worked for 6 years as Deputy Chief Medical Officer in the
Department of Health. He has been in his current post for since 2015 and has worked in the
HSE since 2011.
Dr Rory Dwyer
Clinical Lead, Irish National ICU Audit
Dr Rory Dwyer is the Clinical Lead for the National ICU Audit. He is a Consultant in ICU and
Anaesthesia in Beaumont Hospital, Dublin and Senior Lecturer in the RCSI Department of
Anaesthesia. He is currently President of the Intensive Care Society of Ireland. He has
previously been Chairman of the Training Committee of the College of Anaesthetists and the
Clinical Lead for Transport of Critically Ill Adults.
Mr. Kenneth Mealy, MD FRCSI
Consultant General Surgeon Wexford General Hospital and Clinical Director Liver Transplant
and HPB Unit, St Vincent’s University Hospital, Dublin. Chair of the Forum of Irish Medical
Postgraduate Training Bodies, Co-Lead of the National Clinical Programme in Surgery and
Past President of RCSI.
5 @noca_irl #NOCA2021
CONFERENCE SPEAKER, CHAIR AND
MODERATOR BIOGRAPHIES
Prof Pat O’Mahony, MVM, MBA, C Dir
Chief Executive at Mapat Management Consultants
Pat provides strategic management consultancy to selected clients. Pat is also Executive
Chairman of Muir PT, which is planning to provide Proton Therapy services on the island of
Ireland, Chairman of the Board of the Health Information and Quality Authority (HIQA) and
Chairman of the Board of the Irish Medicines Verification Organisation (IMVO).
Pat previously served as CEO at Clinical Research Development Ireland, the clinical and
translational research partnership of the universities in Ireland from 2017 to 2019, Deputy
Secretary General and Head of Governance and Performance at the Department of Health in
Dublin for 15 months, prior to which Pat was Chief Executive of the Health Products Regulatory
Authority from 2002 to 2015.
Having spent a number of years in private clinical practice and as technical manager in the
pharmaceutical industry in Ireland and the UK, Pat worked in public health and was Director of
Consumer Protection at the Food Safety Authority of Ireland.
Pat has previously served on a variety of public and private sector boards including the
European Medicines Agency (EMA), where he served as Chairman from 2007 to 2011, the Food
Safety Authority of Ireland, the National Patient Safety Advisory Group and was vice Chair of
the International Coalition of Medicines Regulatory Authorities. Pat was appointed Adjunct
Professor at UCD in 2017.
Dr Joan Power, MB FRCPI, FFPath
Medical graduate UCC. Currently Consultant Haematologist Munster Regional Transfusion
Centre, IBTS. Medical Director Therapeutic Apheresis Service, Senior Clinical Lecturer UCC. Board
member Faculty of Pathology, RCPI Councillor, Chair FPath Scientific Meetings Committee. As
Clinical Lead Advisor for Transfusion she set up the National Transfusion Advisory Group (NTAG).
Following her identification of the Hepatitis C contamination of BTSB anti-D Immunoglobulin in
1994, she was National Co-ordinator for the Hepatitis C Programmes to 1997. She contributed to
European Commission specialist committees on HCV and development of Quality framework
standards prior to introduction of European Directives.
She is committed to the application of Quality and Clinical Governance frameworks to
Health Service delivery and led the Munster Centre in accreditation to ISO, Clinical Pathology
accreditation prior to European Directive Transposition into Irish Statutory Instruments.
She was awarded the UCC Medical Faculty Gold Medal in 2002 for outstanding contribution
to Medicine in Society.
Ms Collette Tully
Executive Director, NOCA
Collette Tully was appointed the NOCA Executive Director in June 2016. Prior to this, Collette
was the Operations Manager for Medical Validation Ireland, a consortium of the main Medical
and Dental Training Bodies in Ireland, working on international projects. Collette worked for a
number of years as a management consultant with Deloitte Ireland, where she was responsible
@noca_irl for change programmes across multiple sectors including banking, health insurance and
the public sector. Collette also has significant international experience working with the
Department for Education England, BHP Billiton Australia and JP Morgan London. Collette is
a qualified accountant with the Chartered Institute of Management Accountancy (CIMA) and
Association of Project Management (APM) certified.
6 @noca_irl #NOCA2021
NOCA QUALITY IMPROVEMENT CHAMPION
AWARD - 2021 SUBMISSIONS
Alphabetical order by title. Submissions will be made available through our website.
Submission Title Organisation Project Team Lead/s
1. Accelerated Community University Hospital Orthogeriatric & Nur Atikah Mhd Asri,
Discharge Careplan Limerick Orthopaedic team; Pamela Hickey,
Trauma Ward Stephen White
2. Audit of facial pressure injuries Beaumont Hospital/ Natalie McEvoy, Natalie McEvoy
in COVID-19 staff RCSI Prof Zena Moore,
Prof Declan Patton,
Prof Ger Curley,
Dr Pinar Avsar,
Prof Tom O’Connor,
Dr Agelica Budri,
Dr Linda Nugent,
Simone Walsh,
Linda McEvoy,
Sinead Connolly,
Dr Jennifer Clarke
3. Development of a Virtual OA St Vincent’s University Vanessa Cuddy, Vanessa Cuddy,
Knee Clinic In SVUH Hospital Aoife Caffrey, Aoife Caffrey
Paul Curtin
4. Diagnosing the presence of Connolly Hospital Lisa Donaghy Lisa Donaghy
Atrial Fibrillation and other Dr Eamon Dolan
cardiac abnormalities in patients Dr Marie O’Connor
who present with Acute Stroke Dr. Avril Beirne,
and TIA in Connolly Hospital Dr. Patricia Guilfoyle and
using 72 hour Holter Monitors the Cardiac Diagnostics
Department
5. Enhancing Patient Visibility and St James’s Hospital Covid-19 ward Bernie Waterhouse,
Safety on a COVID Ward nursing staff Anthony Galvin,
Christopher Soraghan
6. Fast track pathway for Beaumont Hospital Department of Caroline Treanor,
degenerative cervical Neurosurgery and Warren Lenehan
myelopathy Physiotherapy
7. Getting the balance right for The National Maternity Dr Anna Curley, Dr Anna Curley
families: managing low blood Hospital Dr Ibrahim Dafalla,
sugars in newborn infants in a Dr Sarah Kasha,
maternity setting Avril Kearney,
Hilda Wall
8. Improving IHFD Hip Fracture Mater Misericordiae MMUH Hip Fracture Mary Mullen,
Standard 1 - patient’s admission University Hospital Governance Committee Dr Sandra O’ Malley,
times to bed Keith Synnott,
Dr Vinny Raminah,
Prof Joe Duggan,
Dr Liz Callaly,
Ruth Buckley,
Karen Fitzpatrick
7 @noca_irl #NOCA2021
NOCA QUALITY IMPROVEMENT CHAMPION
AWARD - 2021 SUBMISSIONS
Alphabetical order by title. Submissions will be made available through our website.
Submission Title Organisation Project Team Lead/s
9. Introduction of Beta D-Glucan Mater Misericordiae Dr Breda Lynch, Dr Breda Lynch
Testing University Hospital Dominic Gilmore,
Fiona Hegarty,
Nuala Scanlon,
Leah Colclough,
Louise O’Sullivan,
Assumpta Killarney
10. ISBAR3 Children’s Health Warren O’Brien Warren O’Brien
Ireland Crumlin
11. Medication Request and Public Health Virginia Pye, Virginia Pye
Administration Record for Public Nursing Service, Ina Crowley,
Health Nursing Community Healthcare Sinead Lawlor,
Organisations, HSE Breda Horgan,
Olivia Byrne,
Margaret Nally,
Marie Therese Buckley,
Fiona O’Connor Power,
Dr David Hanlon,
Muriel Pate,
Eileen Whelan,
Clare MacGahann,
Lisa Marry
12. Prostate Biopsy Infection Rates Mater Misericordiae Dr Jack Power, Dr Jack Power,
in the Mater Hospital Radiology University Hospital Dr Carmel Cronin, Dr Carmel Cronin,
Department Dr Barry Hutchinson, Prof John Murray
Dr Daragh Murphy,
Kiaran O’Malley,
Dr Margaret Hannan
Catherine McGarvey,
Nisha Soman,
Prof John Murray
13. Reducing Hospital Acquired Incorporated Emma Cullen Gill Emma Cullen Gill
Pressure Ulcers using Plan, Do, Orthopaedic Hospital,
Study, Act (PDSA) Quality Cycle Clontarf
14. Striking back against stroke Connolly Hospital Lisa Donaghy, Lisa Donaghy
Laura Morrison,
Julie Prendergast,
Dr Eamon Dolan
Dr Marie O’Connor
Dr Avril Beirne,
Dr Patricia Guilfoyle
8 @noca_irl #NOCA2021
NOCA QUALITY IMPROVEMENT CHAMPION
AWARD - 2021 SUBMISSIONS
Alphabetical order by title. Submissions will be made available through our website.
Submission Title Organisation Project Team Lead/s
15. UHW OA Knee Pathway University Hospital Siobhan Corcoran, Siobhan Corcoran
Waterford, UHW Professor May Cleary,
Orthopaedic Terence Murphy,
Dept, South East Damian Rice,
Community Healthcare Pauline Kirwan,
Physiotherapy, South Anne-Marie Tully
East Community
Healthcare Dietetics.
16. Utilization of Lean Six Sigma Mater Misericordiae James W Ryan, James W Ryan,
Tools for Quality Improvement in University Hospital Sine Gilchriest, Sine Gilchriest,
Interventional Radiology Leo P Lawler, Leo P Lawler
Sean Paul Teeling,
Anita Little,
Mark Glynn,
Lisa Comerford,
Megan Power-Foley,
Tony Geoghegan,
John G Murray
9 @noca_irl #NOCA2021
SPONSORS/EXHIBITORS As usual, the NOCA webinar takes place as part of RCSI Charter Week. This year, instead of sponsorship for the individual events, sponsorship is at the RCSI charter week level. NOCA will receive a percentage of the funding raised through Charter Week sponsorship and any such funding will be used to print patient diaries for NOCA audits that collect patient diary information. We would like to thank the following sponsors of RCSI Charter week: 10 @noca_irl #NOCA2021
NOCA AT A GLANCE
NOCA was established in 2012 to create sustainable clinical audit programmes at national level. NOCA enables
those who manage and deliver healthcare to improve the quality of care through national clinical audit. NOCA
is funded by the Health Service Executive Quality Improvement Team, governed by an independent voluntary
board and operationally supported by the Royal College of Surgeons in Ireland.
NOCA GOVERNANCE BOARD ATTENDANCE 2020
Representative Name Jan May Jun Sept Nov Total
2020 2020 2020 2020 2020 2020
Faculty of Paediatrics A Prof Michael Barrett ✓ ✓ ✓ ✓ 7 4/5
Joint Faculty of Intensive Care Medicine of Ireland Dr John Bates ✓ ✓ ✓ ✓ ✓ 5/5
NOCA Clinical Director Dr Brian Creedon ✓ ✓ ✓ ✓ ✓ 5/5
HSE Quality Improvement Division Dr Philip Crowley ✓ ✓ ✓ ✓ ✓ 5/5
Public Patient Interest Representative Brigid Doherty ✓ ✓ ✓ ✓ ✓ 5/5
Prof Francis
Royal College of Physicians of Ireland ✓ ✓ ✓ ✓ ✓ 5/5
Finucane
Office of Nursing and Midwifery Services Director Dr Anne Gallen 7 ✓ ✓ 7 ✓ 3/5
Irish Institute for Trauma and Orthopaedic Surgery Mr Paddy Kenny 7 ✓ 7 ✓ ✓ 3/5
Dr Brian Kinirons/
College of Anaesthesiologists of Ireland ✓ 7 ✓ 7 ✓ 3/5
Prof Gerry Fitzpatrick
Irish Committee for Emergency Medicine Training Dr Gerard McCarthy ✓ ✓ ✓ ✓ ✓ 5/5
Chair Mr Ken Mealy ✓ ✓ ✓ ✓ Chair 5/5
Dr Deirdre
Faculty of Public Health Medicine ✓ ✓ ✓ ✓ ✓ 5/5
Mulholland
Consultant Histopathologist,
Prof Conor O’Keane Chair Chair Chair Chair ✓ 5/5
Mater Misericordiae University Hospital
Public Patient Interest Representative Iryna Pokhilo ✓ 7 ✓ ✓ ✓ 4/5
Dr Niall Sheehy/
Dean, Faculty of Radiologists ✓ ✓ 7 7 ✓ 3/5
Dr Peter Kavanagh
Independent Hospitals Association of Ireland Dr Carmel Sheridan 7 ✓ ✓ 7 ✓ 3/5
Royal College of Surgeons in Ireland Prof Sean Tierney ✓ ✓ 7 ✓ 7 3/5
NOCA Executive Director Collette Tully ✓ ✓ ✓ ✓ ✓ 5/5
3 Attended
7 Did not attend
11 @noca_irl #NOCA2021CLINICAL AUDIT PORTFOLIO
Bed Information
System (ICU BIS)
12 @noca_irl #NOCA2021ICU BED INFORMATION SYSTEM (ICU-BIS)
PROJECT TO IDENTIFY
SPARE INTENSIVE CARE
BEDS ACCELERATED
BY PANDEMIC
New technology allows doctors
to see which hospitals have
available beds in ICUs
www.irishtimes.com
“It became clear in early March 2020 that a key determinant for care of patients with COVID-19 was
ICU capacity. NOCA prioritised the rapid development of a project that we had been working on for
some time. This was a web-based display of ICU bed occupancy and availability across the acute
hospitals – the NOCA ICU Bed Information System (ICU-BIS)”
Dr Rory Dwyer Clinical Lead for National ICU-BIS.
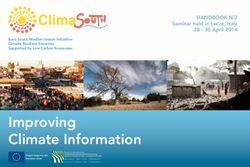
WHAT IS A BED INFORMATION SYSTEM?
An electronic system which automatically
populates a view of patient admissions, level of
care and discharges to critical care units nationally.
ADMISSIONS BIS DISCHARGES
As the health system reorganised itself to cope with the coming tsunami, NOCA put other projects on hold to fast-track the
development of ICU-BIS. NOCA recognised that this could play a central role in monitoring and responding to COVID pressures
on ICU capacity. The team worked late at night and at weekends to design the configuration of the system, working with our
IT partners in DMF Systems to implement and test the software design, communicate with the hospitals, the HSE and the
Department of Health and to train staff in the hospitals to use the system. On March 26th 2020, the system went live in 26
hospitals just as ICU bed occupancy with COVID patients was starting to increase exponentially. By April 4th, the Paediatric
and Private hospitals were on-board.
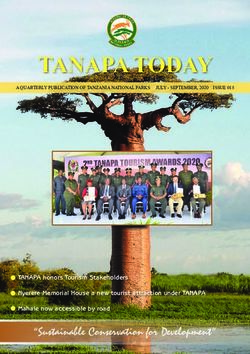
13 @noca_irl #NOCA2021ICU BIS provides a real-time overview of ICU bed occupancy and bed availability nationally. This allows monitoring of trends
and of spare capacity in ICU. It also provides data on individual hospital ICU bed occupancy and bed availability. This provides
visibility of hospitals who are approaching the limits of their capacity, to trigger transfers of patients to other hospitals with
spare capacity.
National ICU Bed Information System
National Status (All critical care units & off-unit occupancy figures)
Open/Staffed Occupied Invasively Cleared for Reserved/ Available Closed Bed Last Updated
Beds Beds ventilated (n) Discharge Assigned Beds
21/05/2020
409 292 115 47 25 107 78 10:56:54
ICU-BIS allows identification of hospitals with spare capacity also.
Hospital Unit Total Open/ Occupied Invasively Ready for Reserved Available Last Updated
No. Beds Staffed Beds ventilated Discharge Beds Beds
Beds (n)
21/05/2020
BEAUMONT ICU 12 10 5 5 - - 5 08:25:04
21/05/2020
HDU 8 8 6 1 3 - 2 08:25:32
On March 30th Connolly Hospital experienced a surge of critically ill patients with COVID-19 arriving to the Emergency
Department, similar to those described by clinicians in Italy and London. Using ICU-BIS, they identified neighbouring hospitals
with spare capacity and after contacting ICU Consultants in these hospitals, arranged the transfer of four patients to these
hospitals. Two of these transfers were undertaken by the Critical Care Retrieval Service MICAS service who also use ICU BIS
to identify need and plan their service.
More recently in the 3rd surge, the ICU-BIS has again played a pivotal role in identifying hospitals who are approaching the
limits of their capacity, and triggering transfers of patients to other hospitals with spare capacity.
ICU-BIS also provides a real-time display of COVID-19 cases and activity in ICU. This is the most up-to-date and accurate
measure of the number of critically ill patients with COVID-19.
This data is used by the Department of Health to monitor trends in COVID-19 numbers in ICU and ICU bed availability and
provides the data quoted in the media for ICU beds.
National ICU Bed Information System
National Current COVID Status
Admissions of Confirmed-COVID Confirmed-COVID Confirmed-COVID COVID-confirmed Suspected Suspected COVID Last Updated
COVID-confirmed cases under care cases invasively deaths under patients COVID cases cases invasively
patients in last of ICU team; ventilated (n) care of ICU team discharged to under care of ICU ventilated (n)
24hrs (8am-8am) in-Unit or in last 24hrs ward in last 24hrs team;
off-Unit (n) (8am-8am) (n) (8am-8am) (n) in-Unit or
off-Unit (n)
21/05/2020
2 52 36 0 2 21 7 10:56:54
Government decisions about restrictions on activity are based on predictions from ‘modelling’ experts on likely patterns in
COVID infection rates and the ability of the health system, especially ICU beds, to cope with patient numbers. NOCA data both
from the ICU-BIS and Irish National ICU Audit data has been a central part of the data they are using to make these predictions.
As part of the ICU-BIS project, NOCA undertook a detailed census of ICU potential bed capacity at different levels of ‘surge’ in
COVID-19 patient numbers and this has been enthusiastically welcomed by planners in the HSE and Department of Health also.
The HSE is currently planning an expansion in ICU bed capacity to cope with what is expected to be an ongoing requirement
for ICU beds by COVID-19 patients. A return to normal hospital activity will mean a return to normal baseline requirement
for ICU beds by non-COVID-19 patients and this will require increased ICU capacity. NOCA data on COVID-19 activity and on
baseline non-COVID-19 activity is central to planning this.
14 @noca_irl #NOCA2021PRESS RELEASE: FRIDAY 18 DECEMBER 2020:
Minister for Health announces plan to expand critical care capacity to 446 beds
The Minister for Health, Stephen Donnelly TD, has today announced a strategic multi-year plan to expand adult
critical care capacity from 255 beds to 446 beds.
Work on Phase One of the plan has already begun and will see 321 adult critical care beds in place by the end
of 2021, compared to 255 at the start of this year. This will be funded by €52 million allocated in Budget 2021.
This funding will also allow for education and training initiatives to increase the critical care workforce and for
investment in critical care retrieval services.
These developments have been achieved by a small team in NOCA who put their personal lives on hold to complete the
ICU-BIS project in time for the 1st surge in COVID-19 activity. Brid Moran is our IT expert; her other expertise is in patience in
dealing with vague specifications from the clinical lead and regular changes in design requests. Fionnuala Treanor is Audit
Manager for ICU-BIS and she and Mary Baggot have been indefatigable in the design of the system and in liaising with the
hospitals to set up and maintain daily data entry into the BIS. Paul Dempsey joined the team in October 2020 to help support
and maintain daily data entry into the ICU-BIS. Fionnola Kelly has provided data analysis. Collette Tully, NOCA Executive
Director, immediately recognised the importance of the project and sanctioned the redirection of NOCA resources to ICU-BIS.
Our partners in DMF Systems, especially software engineers Miguel Bueno and Giulio Iannella, with the Managing Director,
Declan Fitzgerald put other projects on hold and worked late and at weekends to implement all our requests – and changes
of requests as we responded to requests from those using the data. HSE Office of the Chief Information Officer (HSE OCIO),
Hannah Stern, deftly channelled all the varied requests through the HSE to enable us get the system live, all while delivering in
an ever changing fast-paced situation. The Tech Platforms and operations team in the HSE also played their part in enhancing
the infrastructure to meet growing usage demands. Full support was received from Martina Burns HSE OCIO, Ciaran Browne
and Liam Woods in HSE Acute Operations and Philip Crowley in HSE Quality Improvement Team. These have all combined to
make a significant contribution to the health service response to this national emergency.
ICU-BIS NATIONAL IMPLEMENTATION TEAM (NIT)
Dr Rory Dwyer Mary, Brid & Fionnuala (NOCA) Paul (NOCA) Miguel, Declan, Giulio (DMF)
Team supported by NOCA & HSE, ICU Project Board and ICU Governance Committee
FUTURE PLANS 2021:
The plan was to integrate with the technology used by NOCA to audit ICUs. While the COVID-19 pandemic
accelerated the project, the plan is to fully automate the ICU-BIS technology in the future, when there’s a bit less
pressure on the system.
15 @noca_irl #NOCA2021IRISH HEART ATTACK Clinical Lead: Dr Ronan Margey
Audit Manager: Joan McCormack
AUDIT (IHAA)
OVERVIEW THE AIM OF THE PROGRAMME WAS TO ENSURE
In 2012, the National Clinical Programme for Acute Coronary THAT ALL PATIENTS WITH ACS NATIONALLY
Syndrome (ACS) published an ACS Model of Care https:// ARE MANAGED ACCORDING TO THE OPTIMAL
www.hse.ie/eng/services/publications/clinical-strate- REPERFUSION SERVICE PROTOCOL.
gy-and-programmes/acute-coronary-syndrome-prog-moc.
pdf. The aim of the programme was to ensure that all patients
with ACS nationally are managed according to the Optimal
Reperfusion Service protocol. PARTICIPATING HOSPITALS
• Beaumont Hospital
In order to assure the ACS programme, a performance • Cork University Hospital
monitoring mechanism, known as Heartbeat, was established • Letterkenny University Hospital
to facilitate improvement in care of ACS patients and so • Mater Misericordiae University Hospital
reduce mortality and morbidity through a focus on evidenced • St James’s Hospital
based indicators of care in hospitals across the country. In • St Vincent’s University Hospital
2019, governance of Heartbeat was transferred to NOCA with • Tallaght University Hospital
a view to establishing the Irish Heart Attack Audit. The audit • University Hospital Galway
is clinically led, collecting high quality data on ACS patients • University Hospital Limerick
admitted to Primary Percutaneous Intervention Centres in • University Hospital Waterford
Ireland for the purpose of healthcare quality improvement.
KEY ACHIEVEMENTS IN 2020
In 2020, Dr Ronan Margey, Consultant Interventional Cardiologist, was appointed as Clinical Lead of the IHAA. Under the
Governance Board of NOCA, an Irish Heart Attack Audit Governance Committee has been convened and an inaugural meeting
was held virtually on 9th July 2020. Its membership comprises clinical experts, Public and Patient Interest representatives, the
Healthcare Pricing Office, senior accountable healthcare management, and research and specialist bodies
Dr Sean Fleming, Consultant Cardiologist has been appointed as Chairperson of the Heart Attack Audit Governance Committee.
16 @noca_irl #NOCA2021AIM AND OBJECTIVES
AIM: TO CONDUCT AUDIT OF ACUTE CORONARY SYNDROME (ACS) CARE.
OBJECTIVES
> To integrate the existing Heartbeat audit of STEMI into a National Acute Coronary Syndrome Audit within NOCA
that encompasses STEMI, NSTEMI, and unstable angina hospital admissions
> To evolve and develop the current Heartbeat dataset to match data collection international best practice standards
for ACS audit (Swedeheart SCAAR; NCDR MI-PCI Registry; UK MI National Audit Project datasets)
> To maintain a database of all in-patients with an ACS in Ireland to drive continuous quality improvement to deliver
the best patient outcomes
> Support the collection of high quality data on all in-patient ACS admissions in Ireland to permit local and national
reporting of outcomes
> Disseminate the outputs from the data in a timely manner to all relevant stakeholders
> Benchmark ACS care and outcomes against national and international standards
> Support / promote use of ACS data for quality improvement initiatives at local and national level
To develop appropriate risk adjusted modelling of outcomes to facilitate national, regional hospital group, and
> individual hospital level and physician level quality improvement and to develop patient reported outcomes
measures for ACS
> Provide data to support and inform National Policy for ACS and related conditions.
PLANS FOR 2021
• Publish a 2017 – 2019 national report
• Engage with key stakeholders such as the National Ambulance Service and the Out of Hospital Cardiac Arrest
• Register to develop data sharing agreements
• Publish a COVID impact report
• Establish a data validation reporting process to support data quality in all participating hospitals.
• Commence data collection in University Hospital Waterford
17 @noca_irl #NOCA2021IRISH HIP FRACTURE Clinical Orthopaedic Lead: Mr Conor Hurson
Clinical Geriatric Lead: Dr Emer Ahern
DATABASE (IHFD) Audit Manager: Louise Brent
OVERVIEW
The IHFD is a clinically led, web-based audit which measures of the BPT. NOCA engages the hospitals and hospital groups
the care and outcomes of patients with hip fractures. on a continuous basis using the quarterly reports which have
The IHFD grew out of a collaboration between the Irish been further augmented during 2020 to include Statistical
Gerontological Society (IGS) and the Irish Institute for Trauma Process Control (SPC) charts. Each hospital, through the
and Orthopaedic Surgery (IITOS). Since 2013, the IHFD has formation of a hospital hip fracture governance committee
been under the management and governance of NOCA. Hip (HFGC), is encouraged to use these reports for continuous
fractures are an ideal condition to measure as they serve as a quality improvement.
marker condition for how well a trauma service is functioning
and how well older patients are cared for in acute hospitals.
The IHFD has matured as a robust national clinical audit and
as a consequence hip fracture has become the first condition
to have an associated best practice tariff (BPT) in the Health
Service Executive. The BPT is a monetary payment linked to
the standard of care. Cases receiving the optimum standard
of care defined by the Irish Hip Fracture Standards (IHFS) are
awarded the BPT. In 2019, €548,000 was paid to the hospitals
representing 15% of all hip fracture cases; an increase from
7% in 2018. The engagement of the hospitals with the BPT is
intended to drive a reduction in the variation of care across
the standards. This money is to be used by the local hip
fracture governance committee to improve the quality of
patient care in the trauma service.
In 2020, a new IHFS was introduced measuring ‘the
percentage of patients mobilised on the day of or after
surgery’ (IHFS 7). In 2021, this new standard will become part
IRISH HIP FRACTURE STANDARDS (IHFS)
The Irish Hip Fracture Database measures key clinical steps in the care of hip fracture patients.
Pressure
4 48 Ulcers
to Zero
IHFS 1: IHFS 2: IHFS 3: IHFS 4: IHFS 5: IHFS 6:
Be admitted to an Receive Not develop Be seen by a Receive a Receive a
orthopaedic ward surgery within a pressure geriatrician bone health specialist
within 4 hours 48 hours ulcer assessment falls assessment
18 @noca_irl #NOCA2021HIGHLIGHTS
On November 10th 2020, The IHFD National Report 2019 was launched:
The main highlights from this report are:
> Excellent data coverage nationally - 99%
> 25% of patients were admitted to an orthopaedic ward or theatre from
the ED within four hours, compared with only 17% of patients in 2018
> A geriatrician reviewed 82% of patients at some point during their
acute hospital stay; an improvement of 13% from 2018
> In 2019, a bone health assessment was carried out on 94% of patients
nationally (compared with 84% in 2018)
> Prior to discharge, 84% of patients nationally had a specialist falls
assessment in 2019 compared with only 70% in 2018
> In 2019, €548,000 was paid to the hospitals for BPT; an increase from
€278,000 in 2018
RECOMMENDATIONS
The recommendations coming from this report are summarised as follows:
1. Introduce a new IHFS for early 7. Increase engagement with PPI
mobilisation – measuring how representatives to:
many patients were mobilised by a • raise awareness of topics such as falls
physiotherapist on the day after their prevention and frailty
surgery. • create resources for patients
• create opportunities for engagement
around patient issues
2. Develop workshops to create a learning 8. The Health Service Executive (HSE),
culture for quality improvement using the National Office for Trauma Services in
audit data. collaboration with the Clinical Programme
for Trauma and Orthopaedic Surgery, will:
• continue to implement a national hip
fracture bypass for all hospitals
• improve patient care pathways for hip
fracture
3. Support hospitals to collect high levels of 9. Hospital Hip Fracture Governance
data until at least 2022, as they recover Committees should continue to meet
from COVID-19. regularly and use the audit data to
measure and improve their service
4. Implement processes for the collection of 10. Focus on increasing compliance with the
data of the patient’s recovery after they IHFS to attain the BPT.
leave hospital.
IHFS
5. Develop a research group for the IHFD, 11. Develop and resource a multidisciplinary
including Public and Patient Interest (PPI) orthogeriatric service
representatives.
6. Conduct an organisational audit to look 12. Prioritise the discharge of patients directly
at resources, governance and quality home from hospital where possible.
improvement at hospital level in 2020.
19 @noca_irl #NOCA2021IRISH NATIONAL AUDIT Clinical Lead: Professor Joe Harbison
Audit Manager: Joan McCormack
OF STROKE (INAS)
OVERVIEW
In 2019, the National Stroke Register (NSR), which was first developed in 2012, came under
the governance of NOCA and evolved into the Irish National Audit of Stroke (INAS). The INAS
Governance Committee ensures that all relevant stakeholders are represented, in order to verify
that outputs of the audit findings are interpreted appropriately. INAS is a clinically led audit and
in collaboration with the Hospital In-Patient Enquiry’s (HIPE’s) existing information system and
the addition of a stroke-specific data entry system, is collecting high quality data on all patients
with stroke in Irish hospitals for the purpose of healthcare quality improvement. The audit is live
in all 25 hospitals that admit acute stroke patients.
In 2020, NOCA published the first Irish National Audit of Stroke National Report 2019.
“Stroke remains the third leading cause of death in Ireland and Western Europe, and the leading cause of
severe, adult-onset physical disability. This report will benefit stroke services in Ireland to review quality
and allow for improvements across acute stroke care. This audit points to the need for investment in more
designated stroke unit beds to meet our key performance indicators (KPIs). It also highlights the need for
patients to go to hospital as soon as possible when experiencing stroke symptoms. ‘Time is brain’ ”.
Professor Joe Harbison, Clinical Lead, Irish National Audit of Stroke.
HIGHLIGHTS
EMERGENCY CARE STROKE UNIT CARE
Treatment of acute stroke is time dependent, > 71% of patients were admitted to a stroke unit
> but less than one-half of cases (49%) of patients
arrived at hospital within 3 hours from onset of > The median length of stay in a stroke unit was
8 days
stroke symptoms
> 67% of patients had a swallow screen performed
> 66% of patients were seen by a doctor within 1
hour of arrival at hospital
> 22% of patients had a mood screen performed.
> 44% of CT scans were performed within 1 hour of
arrival at hospital OUTCOMES
> The median time between arrival at hospital and
72% of patients with ischaemic stroke and
treatment with thrombolysis 56 minutes
> 62% of patients with haemorrhagic stroke had
Thrombolysis is the breakdown of blood clots disabilities on discharge
formed in blood vessels using medication. It
> can only be given within 4.5-hours of onset of > 51% of patients with a stroke were discharged
home
stroke symptoms. In 2019, 10.6% of patients
with ischaemic stroke had treatment with 5% of patients with a stroke were discharged
thrombolysis home with Early Supported Discharge (ESD) -
Thrombectomy (EVT) is a procedure where
> stroke specific rehabilitation in the home setting.
8% of patients with a stroke were discharged to
large clots can be removed from arteries in the
long term care
> brain. In 2019, 9% of patients with a stroke had
a thrombectomy. The rate of thrombectomy in
Europe is 2%.
> Mortality rate for ischaemic stroke mortality is
9% and 31% in haemorrhagic stroke.
20 @noca_irl #NOCA2021THE HEALTH AND SOCIAL CARE PROFESSIONAL(HSCP) DATASET
The HSCP dataset was developed by the NSP in collaboration with the professional bodies
for physiotherapy, occupational therapy, and speech and language therapy. The data
represents additional rehabilitation information from 1,604 physiotherapy cases, 1,194
occupational therapy cases and 993 speech and language therapy cases in 17 participating
hospitals. It is not a representation of rehabilitation for all patients with stroke.
Within the HSCP dataset More than 50% of Approximately 50%
Physiotherapists, Occupational patients did not of their patient groups
therapists and Speech and receive sufficient required follow-up
language therapists reported that: therapy. therapy on discharge.
RECOMMENDATIONS PUBLIC AND PATIENT
INTEREST
RECOMMENDATIONS FOR NOCA
‘The recommendations from the Irish
All hospitals providing acute stroke National Audit of Stroke Report,
care should fully participate in the Irish if implemented, will lead to much
National Audit of Stroke. better outcomes for all those who
will require dedicated stroke care in
Complete an organisational audit of
stroke units to review the availability Ireland. As a patient representative I very
and accessibility of stroke unit beds, the much welcome the recommendations and
availability of the appropriate number of the clear emphasis on acting FAST for better
trained stroke staff, and accessibility to outcomes and less disability’
diagnostic tests and investigations.
Martin Quinn, Patient and Public Interest
Complete an audit of Early Representative, Irish Heart Foundation
Supported Discharge services nationally. Stroke Survivor & Advocate.
INAS Governance Committee Member
“The data collated in INAS and the
RECOMMENDATIONS FOR THE NATIONAL CLINICAL
resultant recommendations will
PROGRAMME FOR STROKE
inform better stroke service
Develop a stroke awareness planning and provision in Ireland.
campaign. The information generated by audits
such as this one are vital given the future
Pilot a large vessel occlusion predicted increase in the prevalence of stroke
ambulance bypass to the endovascular and consequentially, in the numbers of stroke
thrombectomy stroke centres in Dublin
survivors needing both acute and longer
and Cork.
term community based healthcare services.
I believe that in order to improve services
RECOMMENDATIONS FOR HOSPITAL MANAGERS,
and outcomes for stroke survivors we need to
CLINICIANS, AND AUDIT COORDINATORS
listen to, collaborate and learn from the patient
Improve the level of swallow experience. The value placed on this is evident
screening for patients with a stroke. in the inclusion of PPI representatives such as
myself in national audits.”
Marcia Ward, Patient and Public Interest
All stroke services should have access
Representative. Neuropsychologist.
to a clinical neuro/psychologist as part
Headway Ireland
of a specialist multidisciplinary team
INAS Governance Committee Member
providing care to patients with a stroke.
21 @noca_irl #NOCA2021IRISH NATIONAL ICU AUDIT Clinical Lead: Dr Rory Dwyer
Audit Manager: Mary Baggot
(INICUA-ADULT)
OBJECTIVES
> Measure quality of care in ICU by benchmarking outcomes
> Use audit data to drive improvements in quality of care
> Measure activity to guide the configuration of Critical Care nationally
> Provide Data to support the Hospital In-Patient Enquiry (HIPE) and Activity Based Funding (ABF)
> Audit healthcare-associated infection (HCAI)
> Audit organ donation and potential organ donors
> Develop an ICU bed information system (BIS)
> Develop a National Database for ICU Audit data
> Provide comprehensive national audit coverage of critical care activity.
WHAT INFORMATION IS COLLECTED
Age & Gender Pre-ICU admission data
Pre-existing medical Source of admission to
conditions hospital and to ICU
Clinical diagnoses
Children in adult ICUs
including infection
Physiological Organ support provided
details during ICU stay
Interventions such as
ventilation, invasive Organ donation
monitoring, dialysis, nutrition
IMPLEMENTATION STATUS NATIONAL REPORTS
Irish National ICU Audit (adult) is currently live in 21 adult The Irish National ICU Audit Annual Reports 2017 and
hospitals, encompassing 25 Critical Care Units including 2018 presented 58% and 70% respectively of all critical
three specialist Units. Audit implementation is scheduled in care activity in Health Service Executive (HSE) funded
a further five adult hospitals during 2021. hospitals during those years.
22 @noca_irl #NOCA2021IRISH NATIONAL ICU AUDIT ANNUAL REPORT 2019
managers who support them, at the 90% bed occupancy rate (88% in
national structures for administration of 2018). There were several indicators
the health service, and at the users of of shortage of ICU bed availability
intensive care services in the Republic including high NEWS scores on
of Ireland (ROI). discharge from a number of Units
(suggesting early discharge). Several
This is a condensed version of the usual
Units did not achieve the targets
INICUA Annual Report to provide key
of 50% of ICU admissions within 1
data to support the planning of ICU
hour of a decision to admit and 80%
expansion due to take place in 2021 and
within 4 hours. Conversely, delayed
subsequently.
discharge from ICU was common, with
Nationally, there were no major changes 4.6% of bed days occupied by patients
in findings compared to 2018. Units who had been cleared for discharge >
varied widely in volumes and case-mix, 8 hours.
reflecting the heterogeneity of the
Despite the pressures on ICUs, the
Units included. Children < 16 years
overall national risk-adjusted mortality
were rarely admitted to adult ICUs
rate was at the expected level and
except in University Hospital Galway
no individual Units were outliers
This Report is a comprehensive overview and Beaumont Hospital Neurosurgical
for mortality. There were outlier
of activity and outcomes of 88% of ICU. A new report on obstetric patients
data for quality indicators which
critical care provided in HSE-funded showed 147 admissions of patients
indicated shortages of ICU beds in
hospitals in 2019. The Report includes currently or recently pregnant to ICU.
some Units e.g. delayed admission
four hospitals not previously audited, Patients were very ill on admission, with (Cork University Hospital GICU and St
Cork University Hospital, Letterkenny higher scores for illness severity and James’s Hospital GICU). The hospitals
University Hospital, South Tipperary requirements for organ support than the have responded to these outlier
General Hospital and University Hospital UK. Fifty four percent of Irish patients findings with actions to expand ICU bed
Kerry. The report is consistent with data required invasive ventilation versus 41% capacity.
from 2018, with no major changes in in the UK. The larger referral centres
activity or outcomes. In summary, Irish ICUs are very busy but
were particularly under pressure with
are managing to provide high-quality
The report is aimed at the very ill patients and high occupancy
care with good outcomes. However,
multidisciplinary teams (MDTs) caring levels.
there is little reserve capacity in the
for patients in ICU, at the hospital Units were very busy with an overall system.
“You might like to know that the Audit data and reporting was very useful in our pre-Budget discussions
to help give a sense of what under-capacity means in terms of patient care. In terms of the detail,
the funding is to provide 321 beds by end 2021 - this includes permanently retaining the 40 funded
temporarily this year plus a further 26 adult beds”.
Celeste O’Callaghan, Director, Primary and Acute Integrated Policy, Department of Health
PUBLIC AND PATIENT INTEREST
“Information derived from the NOCA ICU audit proved invaluable during this pandemic and further emphasised the urgent
need to increase ICU capacity permanently. At the heart of this audit is the desire to improve services and outcomes for all
ICU patients. I encourage others to consider becoming a PPI representative, in order to advocate for patients and be a voice
for positive change.” Barbara Egan, Public and Patient Involvement Representative
“Understanding and appreciation of ICU has been transformed by COVID-19. Staff have shown unparalleled heroic bravery,
and we are eternally grateful. NOCA reports a deficit in optimum infrastructure. Provision of this will lead to Improving
patient outcomes, staff safety, morale and effectiveness in a post COVID world. NOCA supports this improvement by
continued effective statistics to inform decision makers”. Damien Nee, Public and Patient Involvement Representative
23 @noca_irl #NOCA2021IRISH NATIONAL ICU AUDIT Clinical Lead: Dr Martina Healy
Audit Manager: Fionnuala Treanor
(INICUA-PAEDIATRIC)
OVERVIEW NOCA works with the Paediatric
Intensive Care Audit Network (PICANet)
The Paediatric Intensive Care Audit in the UK for data validation, data
Network (PICANet) was established in analysis, and the generation of reports.
2001 in the UK.
PICANet produce annual reports and
PICANet was established to develop and the report relates to data collected
maintain a secure and confidential high and events in the previous three-year
quality clinical database of paediatric period e.g. 2020 report relates to events
intensive care activity across the UK, occurring in the 3-year period (January
Wales, Northern Ireland (NI) and ROI in 2017-December 2019). The report
order to: provides data on five key metrics for
• Identify best clinical practice Paediatric Intensive Care services: case Summary Report with a focus on the
• Monitor supply and demand ascertainment, retrieval mobilisation two PICUs at CHI at Crumlin and CHI at
• Monitor and review outcomes of times, number of qualified nurses per Temple Street.
treatment episodes bed, emergency readmissions within 48
• Facilitate healthcare planning and hours and mortality in PICU. At the start of 2020, the plan was to
quantify resource requirements produce the first Irish National ICU
• Study the epidemiology of critical PICANet has also expanded its data Audit Annual Report for paediatrics.
illness in children https://www. collection to include the referral The report would incorporate data from
picanet.org.uk/ and transport of children who need 2015-2019. Figures and tables would
paediatric intensive care. This enables be taken from the PICANet Annual &
The PICUs at CHI at Crumlin and CHI
us to compare and audit important Summary Reports and data reproduced
at Temple Street have been submitting
aspects of care for these children. by NOCA.
anonymised data to PICANet since
2009 and 2010, respectively. There are In 2018, the Irish National ICU Audit However, with the impact of COVID-19,
32 PICUs and 12 specialist transport produced its first Annual report for data originally planned to be released
organisations currently submitting data 2017 data. In this report, a chapter from PICANet in July was not received
to PICANet. was included on the PICANet 2018: until December 2020.
PLANS Despite the setbacks, work is continuing on the first stand-alone Irish National ICU Audit Annual
Report for paediatrics. The report will incorporate data collected by the two PICUs for the reporting
FOR 2021 period 2016-2019. Once this report is published, analysis of the 2020 data will begin.
UPDATE ON RECOMMENDATION FROM 2017 ANNUAL REPORT
RECOMMENDATION 1 MEETING IN NOVEMBER 2019
In November 2019, The National Clinical Programme for Critical Care & National Clinical Programme for Paediatrics
launched Model of Care for Paediatric Critical Care in the College of Anaesthesiologists of Ireland. It sets out clearly the
requirements to establish safe, effective care for all our critically ill children requiring Critical Care Medicine in the ROI.
These requirements align with the recommendations outlined in our INICUA Annual report 2017.
RECOMMENDATION 2
NOCA strive to improve data quality and use the data to advocate for change at a national level. NOCA also want to
increase public and patient involvement (PPI) in their audits. Currently, nominations are sought for a PPI to sit on the
Irish National ICU Audit Governance Committee from paediatrics.
RECOMMENDATION 3
With the expansion of the INICUA for adults nationally, the audit is able to capture in more detail the number of children
who are cared for in adult critical care. This information will be included in the 2020 annual report and is critical to the
health service for future planning of paediatric bed capacity and transport services.
24 @noca_irl #NOCA2021IRISH NATIONAL ORTHOPAEDIC
Clinical Lead: Mr Paddy Kenny,
Mr David Moore and Mr James Cashman
REGISTER (INOR) Audit Manager: Suzanne Rowley
Audit Assistant Manager: Deborah McDaniel
OVERVIEW AIMS & OBJECTIVES
The Irish National Orthopaedic The primary objective of INOR is to
Register (INOR) aims to improve the provide information that is designed
quality of services and care provided to help improve the quality of care and
to patients having elective hip and clinical outcomes of joint replacement
knee replacement surgery. By using recipients. The introduction of a
patient scoring systems and recording National Arthroplasty Register will
on implant performance and patient enable early detection of failing devices,
outcomes, INOR aims to monitor the procedures, institutions or surgeons to
safety of implants and support hospitals limit the impact for future patients.
should an implant recall occur. Implementation of INOR will increase
patient safety, confidence and overall
experience while reducing surgical
THE PRIMARY OBJECTIVE revision and providing orthopaedic
OF INOR IS TO PROVIDE surgeons the opportunity to participate
INFORMATION THAT IS and contribute to measurable clinical
DESIGNED TO HELP IMPROVE audit. Unlike other International
Arthroplasty Registers, who collate
THE QUALITY OF CARE the data retrospectively, INOR data
AND CLINICAL OUTCOMES collection is real-time and is entered
OF JOINT REPLACEMENT electronically at the point of care by
RECIPIENTS. the nurses, doctors and patients into a
bespoke secure web application.
KEY ACHIEVEMENTS 2020
INOR is currently live in eight out of 12 • Kilcreene Orthopaedic Hospital normal figures in September. Further
of our public elective sites nationally. • Our Lady’s Hospital, Navan implementations were impeded by
This accounts for 80% of our national • Merlin Park University Hospital access to hospitals due to COVID-19.
public coverage. It includes the • Cappagh National Our first private hospital, Blackrock
following Orthopaedic Hospital Clinic went live in November 2020.
• South Infirmary Victoria • University Hospital Kerry INOR commenced the development
University Hospital In April 2020, elective arthroplasty of their reporting strategy and a
• Midland Regional Hospital surgery was significantly impacted glance at of the first national report
Tullamore by COVID-19, with a reduction of 95%. was presented at the IITOS meeting
• Croom Orthopaedic Hospital This only started to show a return to in November 2020
PLANS FOR 2021 (dependent on COVID-19 impact)
> Implementation of Tallaght University Hospital (Q1 2021)
> Complete the implementation of all elective public hospitals (if local resource available)
> Implementation of 2 nd and subsequent Private Hospitals
> Hospital Reports (January 2021)
> INOR First National Report (Q2-3 2021)
> Plan for the inclusion of Non Elective sites in INOR
> INOR Reporting Dashboards.
25 @noca_irl #NOCA2021MAJOR TRAUMA AUDIT Clinical Lead: Professor Conor Deasy
Audit Manager: Louise Brent
(MTA)
OVERVIEW
The Major Trauma Audit (MTA) was established by NOCA in National Report 2017, a focus was put on older persons
2013. This audit focuses on care of the more severely injured who suffer major trauma and highlighted the issues around
trauma patients in our healthcare system. The methodological identifying major trauma in older persons, equity of access
approach for the MTA is provided by the Trauma Audit & to care and priority and poorer outcomes. In the forthcoming
Research Network (TARN). In 2016, the MTA became the MTA National Report, an analysis of paediatric major trauma
first national clinical audit endorsed by the National Clinical will be presented focusing on data from 2014-2019. This will
Effectiveness Committee (NCEC) and mandated by the provide the first clear description of the epidemiology of
Minister for Health. Since 2016, all 26 eligible hospitals have paediatric major trauma patients, main mechanisms of injury,
been participating in the audit and data have been collected locations of injury, care processes and outcomes.
on more than 25,000 trauma patients to date. The audit has By focusing on sub-group analysis for MTA patients, the
been reporting at hospital level since 2017. integrated trauma system of the future will be a system that
The MTA National Reports have created a burning platform for can meet the needs of a diverse major trauma population.
the need to change the Irish trauma system. The Department
of Health published a report entitled A Trauma System for
Ireland: Report of the Trauma Steering Group in 2018 and
following that publication, the MTA has been providing data to
support the reconfiguration. The report highlighted the need
for two Major Trauma Centres in Ireland, one in the south in
Cork University Hospital and the second one in Dublin, the site
of which is yet to be announced. The ability of MTA to provide
reliable and robust data that can support the development
of this new system is key. MTA can measure activity, access
to care, standards of care, processes and outcomes. The MTA
will continue to monitor the impact of the evolving service to
inform healthcare commissioners, stakeholders and society.
The maturity of the MTA now lends itself to further analysis
of subgroups of the major trauma population. In the MTA
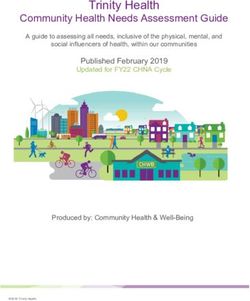
TRAUMA SYSTEM
MTC
ISS
TU
LIU/LEH
STEP 1 STEP 2 STEP 3 STEP 4 STEP 5 STEP 6 STEP 7 STEP 8
INCIDENT PRE-HOSPITAL PATIENT MAJOR TRAUMA RECEPTION PATIENT REHABILITATION DISCHARGE
RESPONDERS PATHWAY CENTRE (MTC) BY A TRAUMA TREATMENT IN FROM
ASSESSMENT TRAUMA UNIT (TU) TEAM HOSPITAL HOSPITAL
LOCAL INJURY
UNIT (LIU) / LOCAL
EMERGENCY
HOSPITAL (LEH)
26 @noca_irl #NOCA2021You can also read