We Can Do Better: Lessons Learned on Data Sharing in COVID-19 Pandemic Can Inform Future Outbreak Preparedness and Response
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Jonathan LoTempio, D’Andre Spencer, Rebecca Yarvitz, Arthur Delot Vilain, Eric Vilain, and
Emmanuèle Délot, “We Can Do Better: Lessons Learned on Data Sharing in COVID-19
Pandemic Can Inform Future Outbreak Preparedness and Response” Science & Diplomacy,
Vol. 9, No. 2 (June 2020). https://www.sciencediplomacy.org/article/2020/we-can-do-better-
lessons-learned-data-sharing-in-covid-19-pandemic-can-inform-future
This copy is for non-commercial use only. More articles, perspectives, editorials, and letters can be
found at www.sciencediplomacy.org. Science & Diplomacy is published by the Center for Science
Diplomacy of the American Association for the Advancement of Science (AAAS), the world’s largest
general scientific society.
We Can Do Better:
Lessons Learned on Data Sharing in COVID-19 Pandemic Can
Inform Future Outbreak Preparedness and Response
Jonathan LoTempio, D’Andre Spencer, Rebecca Yarvitz, Arthur Delot Vilain,
Eric Vilain, and Emmanuèle Délot
T he COVID-19 pandemic will remain a critical issue until a safe and
effective vaccine is in global use. A strong international network exists
for the systematic collection and sharing of influenza genome sequence data,
which has proven extensible to COVID-19.¹ However, the robust demographic
and clinical data needed to understand the progression of COVID-19 within
individuals and across populations are collected by an array of local, regional,
federal, and/or national agencies, with country-specific, often overlapping
mandates. The networks tasked with transmitting descriptive, disaggregated
data have not done so in a standardized manner; most data are made
available in variable, incompatible forms, and there is no central, global hub.
At the same time, data have been released and analyzed on Twitter, in blogs,
and by news outlets before undergoing scholarly peer review in the race to
learn about the emerging virus. Many journals have lowered their paywalls on
COVID-19 papers in accordance with WHO guidelines for sharing data in public
health emergencies. This has led to unprecedented access to knowledge for anyone,
Information about the authors can be found at the end of the article.
We Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
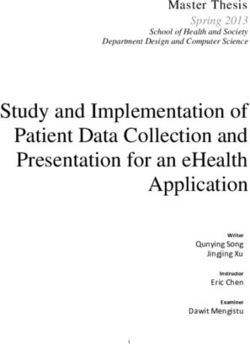
anywhere. Furthermore, in peer-reviewed journals, more papers that include the
term “coronavirus” have been published in just the past six months than in the
previous 70 years (Figure 1). Sorting through these papers to inform evidence-
based policy is daunting. This wealth of new knowledge can be a curse: scientists
and policymakers drown in the open sea of literature; unsure which papers are
life rafts and which are flotsam.
In short, there is a need for improved international data sharing policies to
support outbreak response. Previous successes and challenges in data sharing are
instructive. We probed the national-level reporting on cases between April 1 and
July 1, 2020 (evidence), efforts to share the pathogen’s genome sequence (science),
and existing tools for assessing and disseminating publications (policy). Based on
these observations, we suggest several structural improvements to the systems
that facilitate knowledge sharing.
Figure 1
Figure 1. Publications with the term “coronavirus” archived in PubMed over time. Since the start of the
pandemic, more papers have been published on coronaviruses than all previous years combined. This fact underscores
the need for expert guidance in combing through and making sense of the literature. The emergence of the two
previous human coronavirus outbreaks were followed by noticeable but much smaller increases in publications.
The term coronavirus was published for the first time in 1968 (see “News and Views” in Nature, vol. 220, no. 5168,
November 16, 1968, p. 650). PubMed indexes anterior reports of infections later demonstrated to be due to the same
type of virus, likely via the use of keywords (the early publications are not accessible online via PubMed). Due to
the size of the search query, the data underlying this figure were generated with Entrez Direct command line search.
Science & Diplomacy, June 2020 www.ScienceDiplomacy.org
We Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
Observations
Evidence: Heterogenous, internationally non-interoperable COVID-19 case reporting
We focused on the data reported by public health agencies of the fifteen
nations with the highest COVID-19 burden.² As of April 23, 2020, this list included
the United States (US), Spain, Italy, France, Germany, France, the United Kingdom
(UK), Turkey, Iran, China, Russia, Brazil, Belgium, Canada, the Netherlands, and
Switzerland, which represented ~75% of the reported global cases. Features of the
data reported by these agencies on April 23 can be examined in the Annex, along
with a table updated as of July 1, 2020.³
Many languages of data reports: The many tongues of the global village are
reflected in the ten unique de facto or national languages in these fifteen countries.
While summary data are reported in English by all nations except Iran, China,
Brazil, and Russia, more detailed reports, where available, are typically in official
languages. We used Google Translate to compare the official websites.
Heterogeneous data format: All fifteen agencies reported data in plain text, HTML,
or PDF; eleven offered an interactive web-based data dashboard; and seven had
comma-separated (CSV) data for download. Between April 1 and April 23, the US
agency added a CSV download function and the Turkish agency switched from a
CSV format to a Google product. None of these CSV files are compatible, and no
codebook was appended for decoding. There is little to no documentation which
records the locations where old data are archived or which URLs are stable. The
diversity of these fundamental methods of distribution presents great challenges
to accessing the data.
Data aggregation status: All agencies recorded cases and deaths of citizens due to
COVID-19, while only nine nations reported the number of tests conducted within
their borders. The number of tests performed can help shape evidence-based policy
by offering a crude estimate of infectivity.
Only eight agencies reported on age and sex, yet both variables are known to
have a strong predictive value on health outcomes. Age was reported categorically
with different, incompatible age groups across agencies, thus limiting research
potential.4,5 No agencies included socioeconomic status in their reports. Race/
ethnicity/ancestry was largely ignored, presented only by the US after April 17.
Science & Diplomacy, June 2020 www.ScienceDiplomacy.org
We Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
Clinical aspects of the disease, such as comorbidities, symptoms, or admission
to intensive care, were also unevenly reported. No agencies reported reinfection.
Accounting for each of these factors is of key importance to the professionals
looking to track, treat, cure, and prevent this disease.
Science: A robust system already exists for the rapid sharing of viral genome sequence data
The Bermuda Accord,6 outlined in 1996 at an International Human Genome
Project meeting, was a progenitor of rapid data release protocols, with the express
purpose of the betterment of society. This statement informed the HapMap data-
sharing policies, which still underpin human genomics today.7 In turn, HapMap
data-sharing policies inspired the founders of the 2006 Global Initiative on Sharing
Avian Influenza Data (GISAID).⁸ GISAID further required that data users not only
give credit to data submitters, but make maximum efforts to work with and include
them in joint analyses on viral sequence data, further tipping the scales in favor of
collaboration. This mandated sharing of not only data, but the benefits of research,
has resulted in a paradigm shift which helps to put contributors from higher or
lower resource settings on the same footing.
More than a decade and a name change since its conception, the nearly
invisible infrastructure of the Global Initiative on Sharing All Influenza Data (not
just avian influenza anymore), influences both research and actionable policy, from
the selection of yearly flu vaccines and the close monitoring of emerging strains
to the less tangible but equally important dimensions of diplomacy, including
conflict resolution and trust building.⁹ During the 2009 H1N1 pandemic, there
was only a 10-day period between the first human case identified in the US,10 and
the deposition of a full influenza genome sequence in GISAID11 The GISAID team
ensured that the repository was globally accessible by leveraging team members
across multiple time zones, allowing for round the clock work.12 Since then, the
system has dealt with both light and heavy flu seasons, accommodating the yearly
influx of data and demand for access to those data.
Through these efforts, GISAID has demonstrated that career advancement
and global cooperation are compatible, with little negative impact on researchers’
ability to make a name for themselves, a perennial concern in the open data
world. By changing the default from closely held data and few-author publications
to openness and rapid, multi-author publications, GISAID has helped influenza
research blossom.
GISAID has also shown remarkable robustness in the face of the COVID-19
pandemic. Since the first two SARS-CoV-2 genome sequence submissions on
January 10, 2020, more than 57,000 have followed (through July 1, 2020), deposited
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
from every continent except Antarctica and most countries.13 These files are
high-quality, deeply sequenced genomes with few errors, not just the results
of nasopharyngeal swab samples. For comparison, the National Center for
Biotechnology Information (NCBI, US National Institutes of Health) Genbank and
European Nucleotide Archive only contain ~10,000 SARS-CoV-2 sequences each.
The Chinese National Genomic Data Center’s Genbank links directly to GISAID.14
The GISAID epiCoV database includes metadata which are largely genomics-
focused: sequence of the virus in fasta (plain text) format; and sequencing platform
and analytic tools used to generate the sequence. Metadata are organized by
information about the virus clade, sample, institute, and submitter. These can
be further annotated with team member names, geographic location of sample,
sampling methodology, the age and sex of the case, and any treatment, if known.
However, filtering the database to only include sequences from patients of known
clinical status reduces the number to approximately 3,300. While each viral
sequence submission includes a unique identifier, detail on whether multiple
sequences from one individual are deposited is not readily available. Given the tens
of thousands of available sequences, the majority of the metadata in the database is
incomplete – just as with the public national dashboards described above.
Policy: an explosion of academic manuscripts underscores the need for curation and
summary
The products of academic research are key for informing the design of new
studies and policy. These products include two broad categories: preprints and
journal publications. Preprints have little or no review prior to being posted,
though ethical statements and declaration of competing interests are usually
required for the protection of human and/or animal subjects. Journal publications
undergo editorial review by the journal or platform, and typically peer review as
well, where professionals in the field are asked to assess the scientific and scholarly
merits of papers submitted to the journal.
In the 70 years between 1949 and 2019, approximately 14,000 papers referencing
coronavirus of any kind were published and indexed by PubMed, a database
maintained by NCBI (Figure 1). Since the beginning of 2020, approximately 17,000
more such papers have been archived.
Also, since the beginning of 2020, more than 6,000 manuscripts on
coronaviruses have been uploaded to bioRxiv and medRxiv, two leading preprint
servers. Recognizing the need to ensure open access to knowledge, the World
Health Organization (WHO) created a preprint repository, COVID-19 Open,15
which had ~50 papers as of July 1, 2020. If papers deposited to COVID-19 Open
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
cannot find suitable publication elsewhere, they will be archived by the WHO and
become citable as working papers.16
While it is encouraging that the global research community has turned its
attention to the COVID-19 crisis, and diverse opinions are important, not all papers
are of equal merit or should be used to guide hypothesis design or public policy.
Findability, however, does not ensure quality. The publish-or-perish culture of
academia is responsible for at least some of the failure of effective data sharing,
even though the requirements of funding agencies promote data deposition in
public repositories.17 Clinical and research data are often siloed, requiring further
efforts to join them.18 Predictably, early COVID-19 papers have been retracted
even from very high-profile journals,19 and reports of systemic quality issues
are emerging.20 The Retraction Watch blog has created a special list for retracted
COVID-19 publications.21
Discussion
The science-policy interface fosters a virtuous cycle where each field improves
the other, wherein access to clear and rigorous science is responsive enough to
inform policy yet stringent enough to advocate for the needs of the scientist. That
interface must be made more robust for research on outbreaks, whether measles
in the US, Ebola in the Democratic Republic of the Congo, or a novel swine flu in
China.
The global scope and global threat of pandemics underscores the need for a
transnational entity such as the WHO, which can convene experts and funders to
improve the infrastructure of outbreak response. The WHO is currently the only
global institution with the reach, trust, and power to bring together the parties
needed to build these resources and act as their arbiter. Here we propose two
discrete actions, informed by previous successes in the field, to improve the invisible
infrastructure of outbreak response. These improvements will directly advance
the Research Priorities (Objective 5) outlined in the 2019 WHO Coordinated Global
Research Roadmap R&D Blueprint.22
Research would benefit from centralized repositories of data, both for the scale
that they can achieve and for the inherent like-against-like comparisons that can be
made with harmonized data. At present, the data used for display on each national
dashboard are incomparable and their methodologies opaque. Closely linking the
case data that underpins dashboards to pathogen sequence data could facilitate
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
computational experiments and the ability to develop and test hypotheses.
However, the files behind these dashboards are incompatible with each other. The
WHO global dashboard is also incompatible with country dashboards, and does
not disaggregate the data by sex or age, important risk factors. There is a lack of
transparency in the methods used for collection and aggregation, which would
help transition these dashboards to research and policy resources.
For most researchers, these possibilities are presently limited by a lack of
access to the relevant datasets, which is unproductive and undemocratic, and
which furthermore stifles innovation and discovery. One model for expanding
access to fine-grained case report data (the sort usually sequestered in medical
records) is the Medical Information Mart for Intensive Care (MIMIC-III) database
at the Massachusetts Institute of Technology.23 Another is the European Union’s
COVID-19 data portal, which links virus and host genome, protein, expression,
and biochemistry data, but leaves out clinical and case data.24 Adopting a system
of credit sharing similar to GISAID’s would ensure that regardless of resource
setting, data depositors are incentivized and recognized.
The centralization of outbreak data would have positive effects for policy-
and decision-makers as they address local and global problems. With access to
comparable global data, they can make better-informed decisions. However,
they also need access to curated summaries of the literature written on the data,
which will provide context and clues to which studies are superlative and should
be used as a basis for action. Compendia of this sort will inform best practices
for international consideration on policy for measures to flatten curves or open
economies.
The removal of paywalls to promote access is not a new concept. There is a
strong history of advocacy for broad access to knowledge, whether in recent
commitments25 to open access in public health emergencies or the Findable
Accessible Interoperable Reusable (FAIR) Data Principles from 2016,26 the Budapest,27
Bethesda,28 and Berlin29 statements on open access publishing and knowledge from
the early years of the millennium, or the creation of the preprint arXiv in 1991.30
However, access without guidance can lead to chaos, and potentially a source of
misinformation in the public sphere.
During the pandemic, these previously inward-facing resources have
experienced increased interest and scrutiny from journalists and the general
public. Creating a platform where data produced in the laboratory, field, and
clinic face in to researchers and with summary, dashboard-like information facing
out to decisionmakers will improve the quality and utility of those data across
fields. Sharing credit more equally between depositors and users or analysts will
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
incentivize participation. Curating compendia for non-scientists will help bring
the fields together; when they are paired with rapid peer review, the gap between
new ideas and consumption by non-scientists across all fields is narrowed. Taken
together, these data repositories and resources for high-quality summaries of
impactful papers will help stimulate effective exchange at the science-policy
interface.
Recommendations
Pandemics, as global problems, require harmonization across local contexts.
Through better exchange of information at the science-policy interface, their
human and economic price can be mitigated.
Broadly, we advocate that the WHO, under the auspices of Research Priority
Objective 5,31 should take a lead role in fostering systems that aggregate case
report data for outbreaks, modeling them after GISAID’s. We further advocate
for the creation of metareview panels for papers related to the disease that would
assemble and summarize strong research papers and preprints.
First, we propose a central repository for data from outbreaks, what that
repository should contain, how to manage and perpetuate it, and possible
limitations (Evidence & Science). Second, we explore the possibility for metareview
and the creation of compendia of high-quality papers and summaries of those
papers designed for a broad audience (Policy).
A. Evidence & Science: Joint repository for case report and pathogen sequence data
Present assessment: National-level dashboards cataloguing the spread of COVID
are dynamic. In our initial survey (April 23, 2020), dashboards presented limited
data, but as of July 1, the data and visualizations were generally more mature and
of higher quality.
Publicly available data on COVID-19 require harmonization across sex, age,
location, and disease severity. These data are of paramount importance in design
of clinical trials and dosage levels for vaccines and therapeutics,32 the formation
of basic hypotheses,33 and policy elaboration and implementation.34 Without a
standard minimum amount of information included and a unified repository for
these data, researchers cannot assess the biological and demographic factors that
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
affect health outcomes. The data are (largely) findable, but they are not accessible,
interoperable, or reusable.
Infrastructure need: There is no single place to go for robust data on cases and
the pathogen sequence. The resources that do exist are largely for expert scientists,
but the need exists to span disciplines. This lack of infrastructure hinders our
understanding of and our ability to respond to outbreaks. A repository, or set
of repositories, with case reports and pathogen genome sequence data with an
outward-facing dashboard designed for use by non-experts, and controlled access
to the underlying data for researchers is needed.
Informed execution: The WHO Global Research Roadmap for COVID-19 provides
an excellent, comprehensive of the research needs for this outbreak with an eye
towards generalizable methodology, but little space is devoted to the mechanisms
of data sharing.35
Rather than call on the WHO to build these platforms themselves, we suggest
that it convenes stakeholders, who will themselves build consensus on the necessary
data to be deposited into any repository and find funders to ensure stability of the
resource, as is the case with GISAID. Stakeholders’ openness to ideas in less formal
encounters, specifically at World Economic Forum meetings, were instrumental to
building GISAID – this light-touch approach should be replicated and built upon
by the WHO to build out similar systems for all outbreaks.
The stakeholders’ group should look to the genomics community and the
NCBI Database of Genotypes and Phenotypes (dbGaP), a repository for personally
sensitive or identifiable data.36 While often not user-friendly for submitters or
accessors, it has helped to advance the state of the controlled access data sharing
in genomics where some aspects of the data are individualized and identifiable.
There, scientists eligible for an eRA Commons37 account may submit a project
description to a Data Access Committee to access the data. eRA Commons is the
United States National Institutes of Health investigator portal. This certification
system is used to ensure a high bar of access for dbGaP and like resources. Similar
controlled-access systems maintained by the European Bioinformatics Institute
(EBI) and Chinese National Genomic Data Center also serve this purpose. Results
of the parties convened could be reported with the same mechanism as the Global
Research Roadmap and decision-makers could begin to form the public-private
partnerships needed to address the agreed-upon gaps, needs, and challenges.
Data deposition: Support for centralized data sharing is growing and has a long
history in genomics38 where it has improved the quality and scope of research. In
our proposal for outbreak data sharing, it is reasonable to expect state agency data
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
depositions to come first, with researchers incentivized to deposit data thereafter,
either at the time of publication or as a stipulation of funding.
Long-term support: This repository will require commitment to digital and
human infrastructure that will take time to build, but which will have numerous
long-term benefits and improve scientific study at all levels. GISAID, born of
a public-private partnership, has been supported by numerous public entities.
In 2010, the German Federal Republic took over housing the resource. The US,
European Union, and China all support their federal data repositories, which
are open for global use. A model that leverages governments, philanthropy and,
potentially, commercial sector users will be key for the long-term sustainability of
future endeavors.
Limitations of centralized data repositories
Privacy. The need to maintain essential liberties while enacting short-term,
explicitly temporary restrictions proportionate with the risk to society is essential.39
It has been argued that COVID-19 provides an ideal case to test exceptions to
existing data protection frameworks, including GDPR (General Data Protection
Regulation).40 To this end, multiple tiers of access to a central repository could serve
the greatest number of people while also modeling responsible privacy by design
solutions, where proactively and transparently through all phases of engineering,
measures are in place to protect the privacy and sensitivity of data is the default.41
Hypothesis formation and evidence-based policy in the current pandemic
rely on the accurate reporting of sex, age, and location data, which impact disease
severity and control. To be useful in real time, one tier of data on these key aspects
of the disease must face the public, while another tier of data remains private and
available to researchers while reflecting local privacy laws. One dilemma is that
the US HIPAA standard,42 which considers precise location and age after year 89 as
personally identifying information. This information is critical to understanding
this disease, yet reporting those data widely is irreconcilable with the current
framework in the US. Furthermore, the heterogenous rule of law and standards
of privacy across all nations will require rigorous debate over how to balance
individual and collective needs. Where combined mobile device-based geospatial
location data and contact tracing fits into this schema is unresolved, and warrants
study in the bioethics and legal communities.43
Equity. Health care systems are functionally different44 in high-, middle-, and
low-income countries - we have seen this firsthand in our work in genetic medicine
and infectious disease outbreaks in Central Africa.45 The use of and access to clinic
and hospital settings, where data on epidemics are collected, varies with resources
but also cultural norms. Infrastructure must be operable in low-resource settings
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
with incentives for local participation to ensure that data from low-resource
environments are accurately collected.
Interoperable data collection may also not be a high priority for staff focused
on patient care in clinics. Our experience in clinical team science46 shows us that
the more comprehensive the form, the less all fields are used. International data
interoperability has another fundamental dilemma: harmonize data in English, or
leave data in language with concepts useful to its generators, but more challenging
to use by its aggregators? Here, we err towards equitability of language use, trusting
that, with constant dialogue between the WHO and its regional and country
offices, data will be human- or machine-processable and thus, interoperable.
Accuracy. Data collection can be hindered by agencies with overlapping
mandates. For example, the Italian agency responsible for disaster mitigation
documents different aspects of the pandemic than the Ministry of Health.47 This
redundancy likely improves robustness but hampers data tracking for observers.
Furthermore, faultlessly incorrect or intentionally misleading data are as
detrimental as missing or incompatible data. This belies the need for post hoc data
cleanup.
Our experience in coordinating large, multi-sited consortia (in English,
French, and Spanish) has shown the need to strike a balance between easy-to-
report , easy-to-collect, and easy-to-use data.48,49 Furthermore, our experience
designing prescriptive templates to report disease-specific, standardized metrics,
which ensure high-fidelity responses but require extensive training and practice,
inform our recommendation to strike a balance between more and less open-
ended responses in reporting cases.50 Creating new formats for data reporting is
inherently a community activity, but remember that a camel is a horse designed
by committee. Stakeholders must keep accuracy and utility at the forefront of their
discussions. Once again, the WHO should provide leadership and guidance in
constructing these much-needed data formats.
B. Policy: Transparency at the science-policy interface through expert curation
Present assessment: The viral growth of papers begs for comparison to be drawn
to the outbreak. We would not suggest flattening this curve, as research and analysis
of an outbreak that touches every corner of the earth are important. However, for
scientists and policymakers alike, there is a need to sort the meritorious from the
mere musings. Rather than more avenues for preprint publications, there is a need
for curated libraries of science.
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
For maximum utility across fields, the glut of papers and preprints cannot
simply be archived. High-quality items must be preserved and promoted with their
systematic high-level expert summaries in a central hub. Those with preliminary,
exploratory, or statistically underpowered findings must be handled carefully,
and excluded where appropriate. Summary and archival of critical papers will
serve policymakers and non-experts by bringing more arcane research to light.
Rapid and centralized curation will help to stem the spread of misinformation and
misunderstanding.
Infrastructure need: An endeavor of this ilk would require mobilizing wide-
ranging expertise to assess the relevance of publications or preprints. One such
strategy has been devised by a team at Johns Hopkins University who are offering
metareview through their 2019 Novel Coronavirus Research Compendium (NCRC),
which aims to provide “accurate, relevant information for global public health
action by clinicians, public health practitioners, and policy makers.”51 Drawing
upon PubMed and the preprint servers medRxiv, bioRxiv, and the Social Science
Research Archive, as well as a suggestion box, they search for papers that best
advance the state of COVID-19 knowledge to highlight and summarize.
On June 29, 2020, an initiative from MIT and UC Berkeley with a diverse
editorial board of global experts launched a new journal, Rapid Reviews: COVID-19,
“to combat misinformation in COVID-19.”52 “Promising” manuscripts identified in
preprint archives by UC Berkeley’s COVIDScholar artificial intelligence tools will
be subjected to expert review in a matter of days, and published with accompanying
commentary. This model has the potential to revolutionize peer review as we know
it and may become a model for all fields of research.
Such initiatives must be encouraged and globally funded, to ensure their
independence and representativeness of high-quality research from across the
world. For increased preparedness for the next pandemic, vetted compendia of the
available literature should also be created for other viruses (e.g. Ebola, Zika), and
other successive outbreaks. These metareviews should be housed in a central hub
with easy access and promoted to policymakers.
Leverage expertise: Peer review relies on volunteer time from specialists in the
field of the manuscript under review. Reviewers are contacted by editors on a
case by case basis. For metareview and compendia, a more permanent group of
volunteers or paid staff would be beneficial, activated as needed during outbreaks.
These reviewers could be tapped and vetted by permanent staff, and offered
compensation for their time, to ensure that even early- or mid-career academics
could contribute. If reviewers had conflicts of interest, they would recuse
themselves as usual.
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
Paradigm shift: Like peer review, curating and summarizing literature for
a WHO-mediated compendium must become part of the job of the expert. This
laborious, but significant, change at the science-policy interface will help increase
the utility of open access knowledge. This work needs to be recognized by
university promotion and tenure committees to ensure that experts tapped to do
so can spend the necessary time and resources on this activity.
Conclusions
It is one thing to contemplate the needs of the world, and another entirely
to know the world as it is - especially in a pandemic. COVID-19 has exposed
the strengths and weaknesses of the many national and global systems of
data sharing.53 When the doubling time of new papers is as fast as that of new
cases of a virulent infection, it is not enough to have open access – guides and
way finders are needed. As such, we propose solutions for better scientific data
collection and dissemination. However, data availability only tells part of the
story: resources must be effectively mobilized in order for policymakers to design
the best responses.54 Many governments responded to the pandemic threat with
protectionist action: by April 1, 2020, 68 jurisdictions had adopted export controls
on everything from personal protective equipment to testing reagents and soap.55
We must work together to craft policy based in evidence, rather than protectionist
fear if we are to win against COVID-19. While we have proposed solutions for data
sharing in outbreaks and pandemics, a similar reflective analysis must be made
by trade and policy experts. Efforts for data sharing and global policy design must
be examined to improve flow of information and resources at the science-policy
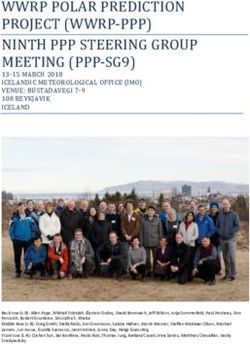
interface (Figure 2). SD
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
Figure 2
Figure 2. Graphic representation of the science-policy interface. Top and bottom text denotes flow of information
as it cycles the scientific and diplomatic processes. In green, data inform the creation of new knowledge, which
generates new data and improves old data. In blue, cooperation and transparency in decision-making combined
with a barrier-free environment improve conditions to make better policy. These colors meet at the science-policy
interface where facets of science and policy come together to inform each other, supporting an environment for
evidence-based policy. In the COVID-19 pandemic, the flow of information across this interface broke down. In
this manuscript, we describe structural improvements to the points illustrated by equilibrium arrows A and B.
Formalized structures at these points will improve science and policy, while providing opportunity to ameliorate
information flow at the science-policy interface. We call on the World Health Organization to act as convener to
ensure effective, broad, and stakeholder-focused resources are created.
At equilibrium arrows A, we propose the construction of a tiered-access data repository to promote the flow of
information to scientists and policy decisionmakers. Tiered-access will provide scientists with granular, identifiable
data while also giving policymakers important high-level data. Some part of these data should be made open-
access to promote transparency, while adhering to privacy by design.
At equilibrium arrows B, we propose the creation of metareview panels responsible for both the assessment of
published literature and preprints, as well as the summary of those meritorious studies for non-science audiences.
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
About the authors
Jonathan LoTempio, BS, is a PhD candidate in the George Washington University Genomics and
Bioinformatics program. His dissertation research is conducted at Children’s National Hospital in Eric
Vilain’s laboratory. He previously served as a Scientific Program Analyst at the National Human Genome
Research Institute and as a member of the Fast-Track Action Committee on Mapping Microbiomes of the
United States Office of Science and Technology Policy.
D’Andre Spencer, MPH, is an epidemiologist who specializes in global health threats specifically in
underserved communities. He is a staff scientist at the Center for Genetic Medicine Research at Children’s
National Hospital where his work focuses on capacity building in health and genetic research in the
Democratic Republic of the Congo and developing database infrastructure for multi-center translational
research.
Rebecca Yarvitz is an international trade analyst in Washington, DC. She holds a BA in International
Relations from the Elliott School of International Affairs of the George Washington University.
Arthur Delot Vilain is an independent high-school student with a focus on history, environmental sciences,
and civil rights and social justice issues.
Eric Vilain, M.D., Ph.D., investigates questions at the intersection of science and society. He is the Director
of the Center for Genetic Medicine Research at Children’s National Hospital, the Chair of the Department
of Genomics and Precision Medicine at George Washington University, and the director of the CNRS
International Research Laboratory “Epigenetics, Data, Politics”. He is an advisor to the International
Olympic Committee Medical Commission and Past President of the International Academy of Sex Research.
Emmanuèle Délot, PhD, is a researcher and educator in developmental genetics and genomics. She is
a professor at the George Washington University, and on the faculty at Children’s National Hospital.
She serves as the founding executive coordinator for the Disorders/Differences of Sex Development
Translational Research Network.
Acknowledgements
We would like to acknowledge and express gratitude for the thoughtful comments and
suggestions from the external reviewers and the Science & Diplomacy editorial board.
This work was supported by the A. James Clark Distinguished Professor of Molecular
Medicine Endowment to Professor Eric Vilain, MD, PhD, A. James Clark Professor,
Children’s National Hospital.
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al Endnotes 1. GISAID, “Genomic Epidemiology of hCoV-19,” www.gisaid.org/epiflu-applications/next-hcov-19-app/ 2. For Iran, reports from the Islamic Republic News Agency were used in lieu of information from a public health agency. 3. Johns Hopkins University and Medicine, “COVID-19 Map,” Coronavirus Resource Center (2020), https://coronavirus.jhu. edu/map.html 4. R. H. H. Groenwold, O. H. Klungel, D. G. Altman, Y. Van Der Graaf, A. W. Hoes, and K. G. M. Moons, “Adjustment for continuous confounders: An example of how to prevent residual confounding,” Canadian Medical Association Journal vol. 185, no. 5 (2013): 401–406. 5. Further analysis of these demographic considerations can be found in K. M. Kocher, A. Délot-Vilain, D. Spencer, J. LoTempio, and E. C. Délot, “Paucity and disparity of publicly available sex-disaggregated data for the COVID-19 epidemic hamper evidence-based decision-making,” medRxiv, www.medrxiv.org/content/10.1101/2020.04.29.20083709v1 6. R. Cook-Deegan and A. L. McGuire, “Moving beyond Bermuda: Sharing data to build a medical information commons,” Genome Research vol. 27, no. 6 (2017): 897–901. 7. “NIH Genomic Data Sharing Policy,” https://grants.nih.gov/grants/guide/notice-files/not-od-14-124.html 8. P. Bogner, I. Capua, N. J. Cox, and D. J. Lipman, “A global initiative on sharing avian flu data” Nature vol. 442, no. 7106 (2006): 981. 9. S. Elbe and G. Buckland-Merrett, “Data, disease and diplomacy: GISAID’s innovative contribution to global health,” Global Challenges vol. 1, no. 1 (2017): 33–46. 10. Center for Disease Control, “2009 H1N1 Pandemic Timeline” www.cdc.gov/flu/pandemic-resources/2009-pandemic- timeline.html 11. Elbe and Buckland-Merrett, “Data, disease and diplomacy.” 12. L. Schnirring, “Pandemic reveals strengths of new flu database,” Center for Infectious Disease Research and Policy, www. cidrap.umn.edu/news-perspective/2009/06/pandemic-reveals-strengths-new-flu-database 13. GISAID, “Genomic Epidemiology of hCoV-19,” www.gisaid.org/epiflu-applications/next-hcov-19-app/ 14. National Center for Biotechnology Information, “GenBank Overview,” www.ncbi.nlm.nih.gov/genbank/; EMBL-EBI, “European Nucleotide Archive,” https://www.ebi.ac.uk/ena; NGDC-China, “National Genomics Data Center,” https://bigd. big.ac.cn/databases. 15. V. Moorthy, A. M. H. Restrepo, M. P. Preziosi, and S. Swaminathan, “Data sharing for novel coronavirus (COVID-19),” Bulletin of the World Health Organization vol. 98, no. 3 (2020): 150. 16. Ibid. 17. “Data management - H2020 Online Manual,” https://ec.europa.eu/research/participants/docs/h2020-funding-guide/ cross-cutting-issues/open-access-data-management/data-management_en.htm; “Dissemination and Sharing of Research Results | NSF - National Science Foundation,” https://www.nsf.gov/bfa/dias/policy/dmp.jsp; “NIH Sharing Policies and Related Guidance on NIH-Funded Research Resources | grants.nih.gov.” https://grants.nih.gov/policy/sharing.htm. 18. C. V. Cosgriff, D. K. Ebner, and L. A. Celi, “Data sharing in the era of COVID-19,” The Lancet Digital Health, vol. 2, no. 5 (2020): e224. 19. C. Piller, “Who’s to blame? These three scientists are at the heart of the Surgisphere COVID-19 scandal,” Science Magazine, June 8, 2020, www.sciencemag.org/news/2020/06/whos-blame-these-three-scientists-are-heart-surgisphere- covid-19-scandal 20. E. Xiao, “Red Flags Raised Over Chinese Research Published in Global Journals” Wall Street Journal, July 5, 2020, www. wsj.com/articles/chinese-research-papers-raise-doubts-fueling-global-questions-about-scientific-integrity-11593939600 21. Retraction Watch, “Retracted coronavirus (COVID-19) papers,” https://retractionwatch.com/retracted-coronavirus- covid-19-papers/ 22. World Health Organization, in collaboration with the Global Research Collaboration for Infectious Disease Preparedness and Response, “A coordinated Global Research Roadmap” Global Research Forum on COVID-19 (February 11-12, 2020) www.who.int/blueprint/priority-diseases/key-action/Roadmap-version-FINAL-for-WEB.pdf?ua=1 23. Cosgriff, Ebner, and Celi, “Data sharing in the era of COVID-19.” 24. “COVID-19 Data Portal,” www.covid19dataportal.org/about 25. “Statement on data sharing in public health emergencies,” February 1, 2016, https://wellcome.ac.uk/press-release/ statement-data-sharing-public-health-emergencies; “Sharing research findings and data relevant to the Ebola outbreak in the Democratic Republic of Congo,” May 22, 2018, https://wellcome.ac.uk/press-release/sharing-research-findings- and-data-relevant-ebola-outbreak-democratic-republic-congo; “Coronavirus (COVID-19): sharing research data,” January 31, 2020, https://wellcome.ac.uk/coronavirus-covid-19/open-data Science & Diplomacy, June 2020 www.ScienceDiplomacy.org
We Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al 26. M. D. Wilkinson et al., “Comment: The FAIR Guiding Principles for scientific data management and stewardship,” Scientific Data vol. 3, no. 1 (2016): 1–9. 27. “Budapest Open Access Initiative,” https://www.budapestopenaccessinitiative.org/read. 28. “Bethesda Statement on Open Access Publishing,” http://legacy.earlham.edu/~peters/fos/bethesda.htm 29. “Berlin Declaration on Open Access to Knowledge in the Sciences and Humanities,” https://openaccess.mpg.de/Berlin- Declaration 30. P. Ginsparg, “It was twenty years ago today ...,” August 14, 2011, http://arxiv.org/abs/1108.2700 31. WHO, “A coordinated Global Research Roadmap.” 32. C. Tannenbaum and D. Day, “Age and sex in drug development and testing for adults,” Pharmacological Research, vol. 121 (2017): 83–93; S. Feldman, W. Ammar, K. Lo, E. Trepman, M. Van Zuylen, and O. Etzioni, “Quantifying Sex Bias in Clinical Studies at Scale with Automated Data Extraction,” Journal of the American Medical Association Network Open vol. 2, no. 7 (2019): e196700–e196700.; S. L. Klein and A. Pekosz, “Sex-based Biology and the Rational Design of Influenza Vaccination Strategies,” The Journal of Infectious Diseases vol. 209 suppl. 3 (2014): S114–S119. 33. H. Li et al., “SARS-CoV-2 and viral sepsis: observations and hypotheses,” Lancet vol. 395, no. 10235 (2020): P1517-1520; R. Verity et al., “Estimates of the severity of coronavirus disease 2019: a model-based analysis,” The Lancet Infectious Diseases vol. 20, no. 6 (2020): 669–677. 34. E. W. Colglazier, “Response to the COVID-19 Pandemic: Catastrophic Failures of the Science-Policy Interface,” Science & Diplomacy vol. 9, no. 1 (March 2020) https://sciencediplomacy.org/editorial/2020/response-covid-19-pandemic- catastrophic-failures-science-policy-interface 35. WHO, “A coordinated Global Research Roadmap.” 36. M. D. Mailman et al., “The NCBI dbGaP database of genotypes and phenotypes,” Nature Genetics vol. 39, no. 10 (2007): 1181–1186. 37. “Overview of eRA Commons,” https://era.nih.gov/help-tutorials/era-commons/overview.htm?q=commons/index.htm 38. Cook-Deegan and McGuire, “Moving beyond Bermuda”; “GenBank Overview”; EMBL-EBI, “European Nucleotide Archive.” 39. American Civil Liberties Union, “Maintaining Civil Liberties Protections in Response to the H1N1 Flu,” www.aclu.org/ other/maintaining-civil-liberties-protections-response-h1n1-flu?redirect=technology-and-liberty/maintaining-civil- liberties-protections-response-h1n1-flu 40. S. McLennan, L. A. Celi, and A. Buyx, “COVID-19: Putting the General Data Protection Regulation to the Test,” Journal of Medical Internet Research Public Health and Surveillance vol. 6, no. 2 (2020): e19279. 41. The 32nd International Conference of Data Protection and Privacy Commissioners, “Resolution on Privacy by Design,” 2010. 42. Mailman et al., “The NCBI dbGaP database.” 43. A. Hern, “France urges Apple and Google to ease privacy rules on contact tracing,” The Guardian, April 21, 2020, www.theguardian.com/world/2020/apr/21/france-apple-google-privacy-contact-tracing-coronavirus; T. Bradshaw, “2bn phones cannot use Google and Apple contact-tracing tech,” Financial Times, April 19, 2020, www.ft.com/ content/271c7739-af14-4e77-a2a1-0842cf61a90f; Apple and Google, “Privacy-Preserving Contact Tracing,” www.apple. com/covid19/contacttracing 44. Norwegian Refugee Council, “Just three ventilators to cope with Covid-19 in Central African Republic,” March 31, 2020, www.nrc.no/news/2020/march/just-three-ventilators-to-cope-with-covid-19-in-central-african-republic/; R. Maclean and S. Marks, “10 African Countries Have No Ventilators. That’s Only Part of the Problem” New York Times, April 18, 2020, www.nytimes.com/2020/04/18/world/africa/africa-coronavirus-ventilators.html 45. J. D. Kelly et al., “Neurological, Cognitive, and Psychological Findings Among Survivors of Ebola Virus Disease From the 1995 Ebola Outbreak in Kikwit, Democratic Republic of Congo: A Cross-sectional Study,” Clinical Infectious Diseases vol. 68, no. 8 (2019): 1388–1393; N. A. Hoff et al., “Evolution of a Disease Surveillance System: An Increase in Reporting of Human Monkeypox Disease in the Democratic Republic of the Congo, 2001–2013,” International Journal of Tropical Disease and Health vol. 68, no. 8 (2017): 1388–1393. 46. E. C. Délot et al., “Genetics of Disorders of Sex Development: The DSD-TRN Experience,” Endocrinology and Metabolism Clinics of North America vol. 46, no. 2 (2017): 519–537. 47. Dipartimento della Protezione Civile, “COVID-19 Italia - Monitoraggio situazione,” https://github.com/pcm-dpc/ COVID-19. 48. Kelly et al., “Neurological, Cognitive, and Psychological Findings”; Hoff et al., “Evolution of a Disease Surveillance System”; Délot et al., “Genetics of Disorders of Sex Development.” 49. P. Speiser et al., “SAT-LB050 Congenital Adrenal Hyperplasia Newborn Screening Protocols Differ Widely in the US: A Survey by the Differences/Disorders of Sex Development Translational Research Network (DSD-TRN),” Journal of the Endocrine Society vol. 3, suppl. 1 (2019); E. Stulberg et al., “An assessment of US microbiome research,” Nature Microbiology vol. 1, no. 1 (2016): 1–7. Science & Diplomacy, June 2020 www.ScienceDiplomacy.org
We Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
50. E. C. Délot et al., “Genetics of Disorders of Sex Development”; E. Stulberg et al., “An assessment of US microbiome
research.”
51. “2019 Novel Coronavirus Research Compendium (NCRC),” https://ncrc.jhsph.edu/
52. The MIT Press, “The MIT Press and UC Berkeley Launch Rapid Reviews: COVID-19,” MIT News, June 29, 2020, https://
mitpress.mit.edu/blog/mit-press-and-uc-berkeley-launch-rapid-reviews-covid-19
53. Colglazier, “Response to the COVID-19 Pandemic.”
54. R. Azevêdo and T. A. Ghebreyesus, “Joint Statement,” World Trade Organization News, April 20, 2020. www.wto.org/
english/news_e/news20_e/igo_14apr20_e.htm
55. A. Beattie, “Can this mad, global scramble for protective gear be avoided in future?,” Financial Times, April 20,
2020, www.ft.com/content/8a473d3a-3a2f-46c1-b1da-f555d50a8c92; Global Trade Alert, “Latest State Acts,”www.
globaltradealert.org/latest/state-acts/page_513
Annex
Superscript Country Link
a United States https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html
b United States https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html
c United States https://www.cdc.gov/mmwr/volumes/69/wr/mm6912e2.htm?s_cid=mm6912e2_w
d United States https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
e Spain https://covid19.isciii.es/
f Spain https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/
EnfermedadesTransmisibles/Documents/INFORMES/Informes%20COVID-19/Informe%
20n%C2%BA%2021.%20Situaci%C3%B3n%20de%20COVID-19%20en%20Espa%
C3%B1a%20a%206%20de%20abril%20de%202020.pdf
g Italy https://www.epicentro.iss.it/en/coronavirus/bollettino/Infografica_15aprile%20ENG.
pdf
h Italy https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-
COVID-19_16-aprile-2020.pdf
i France https://www.data.gouv.fr/fr/datasets/donnees-des-urgences-hospitalieres-et-de-sos-
medecins-relatives-a-lepidemie-de-covid-19/
j France https://www.data.gouv.fr/fr/datasets/donnees-hospitalieres-relatives-a-lepidemie-de
covid-19/
k France https://geodes.santepubliquefrance.fr/#c=indicator&view=map2
l Germany https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Fallzahlen.html
m Germany https://experience.arcgis.com/experience/478220a4c454480e823b17327b2bf1d4
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al
n Germany https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus
Situationsberichte/2020-04-17-en.pdf?__blob=publicationFile
o United Kingdom https://coronavirus.data.gov.uk/
p Turkey https://covid19.tubitak.gov.tr/turkiyede-durum
q Iran https://en.irna.ir/news/83753345/Coronavirus-death-toll-reaches-4-869-in-Iran
r China weekly.chinacdc.cn/news/TrackingtheEpidemic.htm#NHCApril01
s China http://www.nhc.gov.cn/xcs/yqtb/202004/9ffacd69bc67476eb83a2776b8d8c70c.shtml
t Russia https://covid19.rosminzdrav.ru/
u Brazil https://covid.saude.gov.br/
v Belgium https://covid-19.sciensano.be/sites/default/files/Covid19/Derni%c3%a8re%20mise%20
%c3%a0%20jour%20de%20la%20situation%20%c3%a9pid%c3%a9miologique.pdf
w Belgium https://epistat.wiv-isp.be/Covid/
x Belgium https://datastudio.google.com/embed/u/0/reporting/c14a5cfc-cab7-4812-848c-
0369173148ab/page/tpRKB
y Canada https://www.canada.ca/content/dam/phac-aspc/documents/services/diseases/2019-
novel-coronavirus-infection/surv-covid19-epi-update-eng.pdf
z Canada https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-
infection.html#a1
alpha Netherlands https://www.rivm.nl/documenten/epidemiologische-situatie-covid-19-in-nederland-16-
april-2020
beta Netherlands https://app.powerbi.com/
These are countries with the highest overall case counts on April 23, 2020 as collated by the Johns Hopkins University Center
for System Science and Engineering. Each national public health website was queried on April 1, April 13, April 17, and April
23. As all websites reported the number of cases, a column was not created to document this metric in the table. In column
9, Severity, ICU stands for intensive care unit, the most common delineation of severe or critical cases. The Italian health
ministry used a scale from asymptomatic to critical instead of hospitalization. Citations within the table document the URL
accessed to find the information.
Superscript Country Link
a United States https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html
b United States https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html
c United States https://www.cdc.gov/mmwr/volumes/69/wr/mm6912e2.htm?s_cid=mm6912e2_w
d United States https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
e Brazil https://covid.saude.gov.br/
f Russia https://covid19.rosminzdrav.ru/
Science & Diplomacy, June 2020 www.ScienceDiplomacy.orgWe Can Do Better: Lessons Learned on Data Sharing in COVID-19... Jonathan LoTempio et al g India https://www.icmr.gov.in/ h India http://https://www.mohfw.gov.in/ i United Kingdom https://coronavirus.data.gov.uk/ j Peru https://www.gob.pe/coronavirus k Peru https://covid19.minsa.gob.pe/sala_situacional.asp l Chile https://www.minsal.cl/nuevo-coronavirus-2019-ncov/casos-confirmados-en-chile- covid-19/ m Spain https://covid19.isciii.es/ n Spain https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/ EnfermedadesTransmisibles/Documents/INFORMES/Informes\%20COVID-19/Informe\ %20n\%C2\%BA\%2021.\%20Situaci\%C3\%B3n\%20de\%20COVID-19\%20en\%20Espa\ %C3\%B1a\%20a\%206\%20de\20abril\%20de\%202020.pdf o Italy https://www.epicentro.iss.it/en/coronavirus/bollettino/Infografica_15 aprile\%20ENG.pdf p Italy https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata- COVID-19_16-aprile-2020.pdf q Iran https://en.irna.ir/news/83753345/Coronavirus-death-toll-reaches-4-869-in-Iran r Mexico https://coronavirus.gob.mx/contacto/ s Pakistan http://covid.gov.pk/ t France https://www.data.gouv.fr/fr/datasets/donnees-des-urgences-hospitalieres-et-de-sos- medecins-relatives-a-lepidemie-de-covid-19/ u France https://www.data.gouv.fr/fr/datasets/donnees-hospitalieres-relatives-a-lepidemie -de-covid-19/ v France https://geodes.santepubliquefrance.fr/#c=indicator&view=map2 w Turkey https://covid19.tubitak.gov.tr/turkiyede-durum x Germany https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Fallzahlen.htm y Germany https://experience.arcgis.com/experience/478220a4c454480e823b17327b2bf1d4 z Germany https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte /2020-04-17-en.pdf?__blob=publicationFile Nations were selected by their overall case count as collated by the Johns Hopkins University Center for System Science and Engineering on July 1, 2020. Each national public health website was queried on July 1 and July 2 in the process of assembling this table. As all sites reported counts of cases, a column was not created to document this metric in the table. In column 9, Severity, ICU stands for intensive care unit, the most common delineation of severe or critical cases. The Italian health ministry used a scale from asymptomatic - critical instead of hospitalization. Citations within the table document the URL accessed to find the information. Note: all hyperlinks on both tables were verified and active at the time of submission, but may have expired since. Science & Diplomacy, June 2020 www.ScienceDiplomacy.org
You can also read