VITAMIN A SUPPLEMENTATION AND DEWORMING CAMPAIGN 2020 - Borno State Primary Health Care Development Agency - 20 January 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

VITAMIN A SUPPLEMENTATION AND
DEWORMING CAMPAIGN 2020
Borno State Primary Health Care Development Agency – 20 January 2021
BACKGROUND INFORMATION
Borno State has been the epicenter of the Boko Haram conflict in Northeast Nigeria
since 2009 with attendant serious humanitarian crises. According to the 2020 Humanitarian
Needs Overview (HNO), an estimated 7 million people need humanitarian assistance in 2020,
with more than 1.8 million being Internally Displaced Persons (IDPs). The conflict had badly
affected normal livelihood activities, including agriculture, which has come to a complete halt
in many locations. Access to food is a huge problem; even when available, increasing prices
also meant that most of the IDP population in these areas, already deprived of their means of
survival, are not able to afford proper daily meals. Sections of populations are also completely
cut off from access to food and other basic amenities. The Cadre Harmonisé conducted in
October 2019 indicated decrease in food consumption and livelihood opportunities in Borno,
Adamawa and Yobe (BAY) states, with about 2.7 million people in the states being in the
critical phases (3 to 5) of food insecurity in October to December 2019, with expected increase
to 3.6 million from January to March 2020 if the ongoing humanitarian assistance is not
sustained. Additionally, the recent onset of convid-19 pandemic with the movement
restrictions imposed by Government have led to increase in challenges at household level,
especially, with regards to feeding and nutrition status of children (including deficiency
diseases), thereby aggravating already dire situation nutrition situation in Borno State.
INTRODUCTION
Vitamin A supplementation is a global health strategy to eliminate vitamin A deficiency and
its tragic consequences. Since vitamin A can be stored in the body for a few months, two high
dose supplements per year are all that is required for young children. Vitamin A is essential
for the functioning of the immune system and the healthy growth and development of
children, and is usually acquired through a healthy diet. However, it is estimated that, globally,
190 million children under five years of age are affected by vitamin A deficiency. These
children suffer an increased risk of visual impairment (night blindness), illness and death from
childhood infections such as measles and those causing diarrhea. Estimated Contribution of
VAD to child mortality in Sub-Saharan Africa is illustrated in Figure 1 below.
Provision of vitamin A supplements every four to six months is an inexpensive, quick, and effective way to improve vitamin A status and reduce child morbidity and mortality in the long term. In areas where vitamin A deficiency is a public health problem, routine vitamin A supplementation is recommended in infants and children 6-59 months of age as a public health intervention, and has been shown to reduce the risk of all-cause mortality by 24%. Comprehensive control of vitamin A deficiency should include strategies for dietary improvement and food fortification as well. More than 836 million children are at risk of parasitic worm infections worldwide. Soil transmission infections can lead to anemia, malnutrition, impaired mental and physical and cognitive development, and reduced school participation. Vitamin A supplements are given from the age of 6 months; deworming tablets are given from the age of 1 year. Research has shown that there is a clinical link between worm infection and reduced vitamin A levels. Roundworms live in the gut and need vitamin A to grow. Worm infestations contribute to vitamin A deficiency; deworming reduces anaemia, anaemia is also associated with increased vitamin A deficiency. Therefore, worm infestations and vitamin A deficiency both have serious health repercussions for a growing child and therefore both should be prioritized. Routine Vitamin A supplementation in Borno is very low; the last mass Vitamin A supplementation and deworming (during MNCHW) was conducted in November 2019. Onset of convid-19 with its attendant restrictions imposed by Government

have led to increase in challenges in households, especially, with regards to feeding and
nutrition status of children (including deficiency diseases).
The demographic information includes:
1. Total No of LGAs in Borno – 27
2. No of Implemented LGAs in Borno – 23
3. Total No of Wards in Borno– 311
4. No of Implemented Wards – 145
5. Total Population of Borno State – 6,629,190 (based on 2006 Nat. Provisional Results
with the State-specific Growthrate).
6. Children 6- 11 months = 132,584
7. Children 12-23 months = 265,168
8. Children 24 -59 months =795,503
9. Children 12 – 59 months = 1,060,671
10. Children 6-59 months = 1,193,255
PLANNING MEETING.
In preparation for the VAS and Deworming Campaign, an advocacy visits to the
Commissioner of Health, led by the Executive Director and Director PHC Borno SPHCDA
with Nutrition Team of SPHCDA and UNICEF.
Planning meeting was held between the State and partners on 2nd and 4th of December 2020
at the Conference Hall, Borno State Primary Health Care Development Agency. These
meetings were held for proper planning and coordination of the campaign.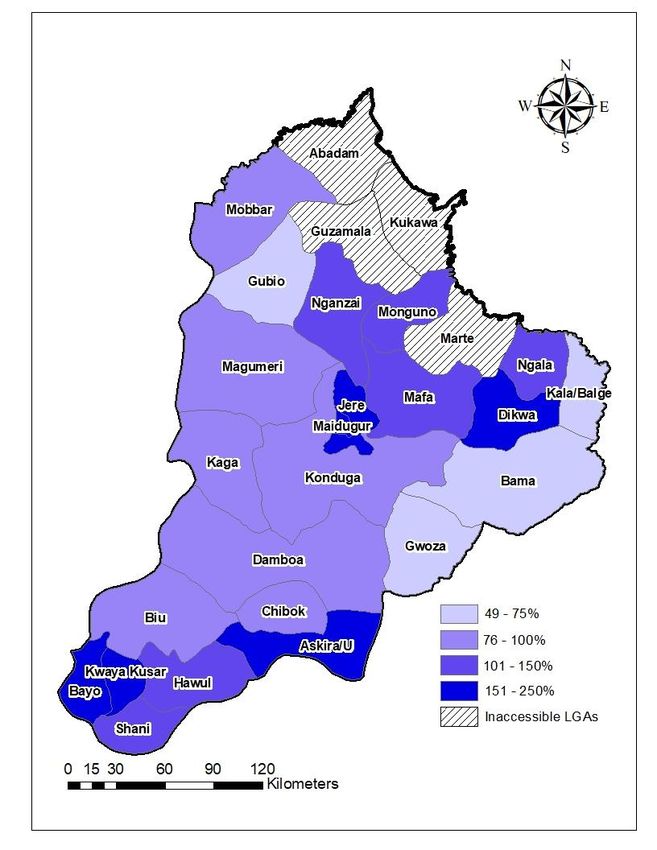
Cross section of Participants during Planning Meeting
During these meetings, there was a presentation on the Micro plan for the campaign, a
consensus by all that the campaign will be in two Batches and It will be House to House using
the Community structure (community nutrition mobilizers) in order to achieved maximum
coverage. Partners were asked to inform their field workers about the VAS and Deworming
Campaign so they can contribute in strengthening the supervisory activities and report back
any challenges encountered.
At the end of the Meetings, the following commitments were by Partners:
S/N PARTNERS COMMITMENTS
1 State (SOML) 1. Production and Airing of radio jingles
2. Procurement of;
❖ 3,000 Face Mask
❖ 413 Hand Sanitizer
❖ 9,695 tins of Deworming Tablets
❖ 6,000 Scissors
❖ 1 CNT Polythene (Dispensing Envelop)
❖ 1000 packs of SP Tablets
2 UNICEF 1. Vitamin A (100,000IU)
2. Vitamin A (200,000IU)
3. Albendazole
4. Funding for:
❖ Planning meeting and training at LGA Level
❖ State Supervisors in 12 LGAs
❖ LGA Team Supervision in 23 LGAs
❖ Transportation of commodities from State to
LGAs
❖ Printing of Data Tools
3 INTERSOS 1. Production and Airing of radio jingles
2. Procurement of;
❖ 500 Face Mask
❖ 400 Hand Sanitizer
❖ 150 Hand Towel
4 SCI 1. Production and Airing of radio jingles
2. Procurement of;
❖ 5000 Face Mask
❖ 1500 Soap
5 PUI Procurement of 120 Hand Sanitizer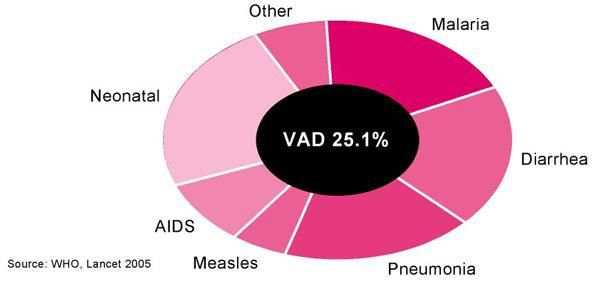
6 ACF 1. Procurement of;
❖ 200 Face Mask
❖ 12 Hand Sanitizer
7 All Partners Supportive Supervision at LGA Level.
LOGISTICS AND COMMODITY DISTRIBUTION
Commodities for the VAS and Deworming Campaign were successfully distributed in 23
LGAs. The point of collection was the Central Medical Store from the 3rd through to the 7th
of December, 2020. Nutrition Focal Persons were responsible for collection in order to ensure
that the commodities were evenly distributed among the LGAs before implementation. The
total commodities distributed include:
S/N COMMODITIES QUANTITY
1 Albendazole (400mg) 9,794
2 Vitamin A (blue) 2342 tins
3 Vitamin A (red) 2314 tins
4 Towel 1,312 pieces
5 Scissors 4,000 pieces
PPE
1 Face Mask 8,700 pieces
2 Hand Sanitizer 533 (500ml)
12 (200ml)
400 (100ml)DATA TOOLS
1 Vitamin A Tally sheet 20,000
2 Deworming Tally Sheet 20,000
5 Ward Summary sheet 1,500
6 LGA Summary sheet 30
TRAINING
A one-day sensitization/training for CNMs and VCMs supervisors at LGA level by the LGA
team (DPHC, NFP, LIO, M&E, CCO, MCH Coordinator, HE) in order to ensure quality
step-down training for the CNMS and VCMs and also to ensure effective implementation of
the VAS and Deworming campaign.
Training of CNMs and VCMs SupervisorsThere was also a step-down training at ward level by the CNMs and VCMs supervisors
between 5th to 6th December, 2020 for the CNMS and VCMs, across the 23 implementing
LGAs
JINGLES AND AIRING
Radio jingles was aired on BRTV and Peace Fm for ten days, from 7th to 11th and 14th to 18th
of December 2020. The jingles were aired in English and three other local languages
(Kanuri, Hausa and Fulfulde) to help in reaching more audience in creating awareness about
the campaign.
The message was about the importance and benefit of Vitamin A and Deworming tablet,
Eligible children and the Implementing LGAs.
IMPLEMENTATION
The VAS Campaign was implemented in Community house-to-house and supported by
Community Nutrition Mobilizers (CNMs), Volunteer Community Mobilisers (VCMs) in 23
LGAs of Borno State in two batches from 7th to 11th December and 14th to 18th December
2020.
Adhering to the Covid-19 IPC Measures, the community workers visited house to house
to target children 6 – 59 months for supplementation.
1. Vitamin A Supplementation (children 6 – 11 Months and 12 – 59 Months)
2. Deworming to children (12 – 23 Months and 24 – 59 Months)Community Nutrition Mobilizers administering Vitamin A to a Child
Batch 1 (7th to 11th December 2020).
Batch 2 (14th to 18th December 2020).
Batch 1 Batch 2
1 Askira Uba Bama
2 Bayo Dikwa
3 Biu Kala – Balge
4 Chibok Magumeri
5 Damboa Mobbar
6 Gwoza Monguno
7 Gubio Ngala
8 Hawul Nganzai
9 Jere
10 Kaga
11 Konduga
12 Kwaya Kusar
13 MMC
14 Mafa
15 Shani
RESULT
Children 6 – 11 months and 12 – 59 months targeted with vitamin A were 132,584 and
1,060,671 respectively, while deworming (12 – 23 months) and (24- 59 months) targeted
were 265,168 and 696,896.
A coverage of 107% children were reached with Vitamin A (6 – 59 months) while 92%
children were reached with deworming tablet.Below is the graphical representation of the coverage
Children reached with Vitamin A
200%
180%
160%
140%
120%
100%
80%
60%
40%
20%
0%
6 - 11 Months 12-59 Months 6 - 59 Months
Target Coverage
Children reached with Deworming Tablet
120%
100%
80%
60%
40%
20%
0%
12 - 23 Months 24-59 Months 12 - 59 Months
Target CoverageCoverage of Vitamin A (6 -59 months) in various LGAs
Coverage of Deworming (12 -59 months) in various LGAs
SUCCESS
1. Community involvement and ownership helped in reaching high number of
children.
2. Supervision by State, LGA team and Partners contribute in strengthening the
supervisory activities.
3. Radio jingles in local languages helped in reaching more audience in creating
awareness at the community level.
4. Effective coordination between partners and the Government
CHALLENGES
1. Implementation on the 14th of December 2020 was not feasible in Kala Balge due
to delay in transportation of commodities.
2. Late Sending of Call – in Data due to poor network.
3. Insecurity
4. Covid – 19 Pandemic
SWOT ANALYSIS
STRENGTH
1. Support from Partners
2. Engagement of CNM, VCM & other community structure etc.
3. Planning meeting at State and LGA for pre-implementation
4. A new, innovative service for house-to-house supplementation
5. Daily debriefing at LGA level
6. Commitment of LGA program officers and other support teamWEAKNESSES
1. Insecurity in some LGAs/wards
2. The terrain of some LGAs/wards are hard to reach
3. Lack of State level training of State supervisors and LGA program officers
4. No network coverage in some LGAs and wards across the State.
5. Poor micro plan at LGA level
6. Insufficient hand sanitizers
OPPORTUNITY
1. Financial support from State (SOML) and Partners
2. Deployment of state supervisors to 12 selected LGAs in state by UNICEF
3. Supply of commodities by partners
THREATS
1. No Implementation in 4 Inaccessible LGAs
2. Insecurity
RECOMMENDATION
1. Conduct state level training of state supervisor & LGA program officers
2. Planning meeting at State & LGA level with all relevant sectors for adequate
support for implementation
3. Appropriate development of micro plan at LGA/ward level for effective
implementation4. Engagement of addition personnel to cover all the settlement in densely populated area e.g. Maiduguri and Jere LGA 5. Develop standardized security clearance document for transportation of commodities & supplies from state to LGA/ward 6. Adequate supplies of all commodities (e.g Hand Sanitizers) 7. Deployment of state supervisor at least one per LGA for pre and implementation support 8. Priorities data management and timely reporting at State, LGA and ward level 9. Ensure adequate document of activity in HMIS reporting tools at HF by facility worker 10. Contingency plan for inaccessible or facially inaccessible area e.g. Abadam, Marte, Guzamala and Kukawa in next implementation 11. Timely use of UNHAS for transportation of commodities to hard-to-reach LGAs
You can also read

















































