VACCINATION: ACHIEVEMENTS, CHALLENGES, PROSPECTS - NVTG
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

BULLETIN of the NETHERLANDS SOCIETY for TROPICAL MEDICINE and INTERNATIONAL HEALTH NO 04 / december 2019 - volume 57 VACCINATION: ACHIEVEMENTS, CHALLENGES, PROSPECTS
EDITORIAL
VACCINATION: ACHIEVEMENTS, CHALLENGES,
PROSPECTS
T
he history of vaccination announced that type 3 poliovirus has
is rich and full of success been eradicated worldwide. For polio to
stories. It all started in 1768 be fully eradicated, all three wild polio
when an English physi- strains (types 1, 2 and 3) need to stop
cian realised that prior infection with circulating. The three strains all cause
CONTENT cowpox rendered a person immune to the same horrible symptoms, including
smallpox. After several investigations paralysis and death, but are virologi-
REVIEWS and tests in human beings in the years cally distinct. Type 2 was eradicated
New developments in TB that followed, it was Edward Jenner, back in 2015; the last case of type 3
vaccine and correlate research another physician in England, who polio surfaced in northern Nigeria in
offer real hope for better TB observed that milkmaids were generally 2012 and the virus hasn't been seen
vaccines - 3 immune to smallpox. He postulated since. Today, only type 1 remains at
that pus in the blisters that milkmaids large — in Afghanistan and Pakistan.
Malaria vaccine development: developed from cowpox (a disease Enormous efforts are being made to
silver bullet or shot in the dark? similar to smallpox, but much less finally eradicate polio completely.
-6 virulent) protected them from smallpox.
In 1796, Jenner tested his hypothesis Many other diseases are being pre-
Overcoming the challenges in by inoculating an eight-year-old boy: he vented through routine vaccination pro-
achieving high immunization scraped pus from cowpox blisters on the grammes or through mass vaccination
coverage in low-income hands of a milkmaid who had caught in the event of outbreaks. But there is a
countries: the role of Gavi - 9 cowpox from a cow and inoculated whole series of conditions that deter-
the boy in both arms that same day. mine the success of such efforts. In this
The International Coordinating The boy developed a fever and some edition of MTb, you can read about vac-
Group on Vaccine Provision - 11 uneasiness, but no full-blown infection. cination surveillance in the Netherlands
The success of Jenner's discovery soon by our National Institute of Health and
CALL FOR ARTICLES - 13 spread around Europe, with small pox the Environment (RIVM) – illustrated
vaccination also being used for traders by the example of maternal pertussis
Monitoring of vaccine in their expeditions to the Americas (whooping cough) which was added
preventable diseases in the and the Far East. In 1980, following to the Dutch national immunisation
Netherlands - 14 an historic global campaign of sur- programme in December 2019. The
veillance and vaccination, the World media recently paid a lot of attention to
Vaccine hesitancy: a new kid on Health Assembly declared smallpox reluctance among the general public in
the block - 17 eradicated – the only infectious disease the Netherlands towards vaccination,
so far to achieve this distinction. showing that high coverage rates are
VIEWPOINT not to be taken for granted. Two articles
Vaccination: who is best Polio (poliomyelitis) is another conta- in this edition reflect on what it takes
equipped in the era of gious disease that could be eradicated, to safeguard high vaccination rates.
postmodern mistrust? - 18 as there is an effective and inexpensive
vaccine providing life-long immunity. Two other articles provide insight
IN MEMORIAM - 20 The Polio Eradication Initiative is a UN into global mechanisms to ensure
programme with the target of a polio- sustainable financing of vaccination
free world. Initially experts believed programmes (the case of GAVI) and
this could be achieved by the year reliable vaccine provision (the case of
2005, but that proved unrealistic. For ICG). The recent approval of an Ebola
a region or continent to be certified as vaccine (November 2019) made news
polio-free, there must be no detection headlines and several authors refer to it.
of wild poliovirus for three consecu- If you are interested in the latest on vac-
tive years as well as an appropriate cine development for TB and malaria,
surveillance system. Recently, polio we recommend the first two articles
got one step closer to becoming the of this edition. Enjoy the reading!
second human disease to be fully wiped
out. On 24 October 2019, World Polio Leon Bijlmakers, Jan Auke Dijkstra
Day, the World Health Organization
2 MT BULLETIN OF NVTG 2019 DECEMBER 04
REVIEW
New developments in TB vaccine and correlate
research offer real hope for better TB vaccines
Tuberculosis (TB) continues to tions (CMV, EBV) which can modu- Mycobacterium tuberculosis (Mtb) pro-
pose an enormous threat to global late immune responses. As a result tein, called Ag85A, which was expressed
health, with over one quarter of BCG vaccination has relatively little in a non-replicating viral vector (MVA)
the world’s population latently impact on global TB transmission and had been designed as a booster
infected, over 10 million new active patterns, which is a reason for TB vaccine for individuals that already have
TB cases each year, over 1.3 mil- vaccine researchers and developers been given BCG. Although the vaccine
lion annual deaths, and an ever- to promote TB vaccines that target was immunogenic and protective in cer-
rising frequency of multi-resistant adolescent TB. tain animal models of TB, it was unable
Mtb strains.[1] Classical intradermal to provide any additional protective
M.bovis Bacillus Calmette-Guerin DEVELOPING NEW TB VACCINES efficacy against TB when administered
(BCG) vaccination of neonates and Better TB vaccines could have sig- as a booster vaccine following BCG, in
young infants protects against nificant impact against TB, and pre- a large phase 2b study in infants.[4] This
severe forms of acute and early and post-exposure vaccination with disappointing result, which could have
TB disease, with over 80% protec- improved vaccines represents a cor- been due to the fact that the Ag85A
tive efficacy against TB meningitis, nerstone of the WHO End TB strategy antigen is insufficiently expressed by
which can be rapidly fatal. Unfor- which aims to end TB by 2035.[1] To Mtb bacteria in the lung,[5] spurred addi-
tunately, however, BCG vaccination discover and develop better TB vaccines, tional efforts to develop better vaccines.
fails to protect consistently and research efforts were initiated in the
sufficiently against pulmonary TB mid-1990s, sponsored both by private USING DIVERSE APPROACHES
in adults, which is the main form of and public funding, particularly the ENHANCES CHANCE OF SUCCESS
contagious TB.[2] The reasons for this European Commission.[3] Discovery and Five approaches have been actively
deficiency are not fully understood evaluation of new candidate TB vaccines pursued in the last decade:[3]
but may involve waning of memory, initially focused on the preclinical and
interference by other infections early clinical space, from which emerged 1. Subunit vaccines which are based
such as Non Tuberculous Mycobac- a first candidate, namely MVA85A. on specific immunogenic com-
terial (NTM) or certain viral infec- This vaccine was based on a single ponents of the bacillus, such
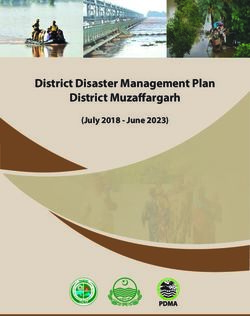
Figure 1: Global Clinical Development of TB vaccines. (Reproduced from TBVI, see: https://www.tbvi.eu/what-we-do/pipeline-of-vaccines/)
DECEMBER 04 2019 MT BULLETIN OF NVTG 3
REVIEW
as proteins, fusion proteins two years after infection. The final had remained IGRA positive after
and lipids, which are typically 3-year follow-up report was recently 24 months, representing a 45% VE
admixed with innate immu- reported. Encouragingly, the vaccine signal. This finding could suggest that
nity stimulating adjuvants; arm showed a 50% vaccine efficacy the immune system is able to eradi-
against developing TB, although a cate an already established infection
2. Virally vectored subunit vac- relatively limited number of cases from the human body once properly
cines in which the subunit was present in the control arm of this activated, in this case by revaccina-
component is typically expressed large phase 2B trial. Nevertheless, tion. This interesting and important
from a genetic insert encoding M72 has significant PoD VE, in the concept needs to be examined fur-
a selected Mtb antigen (such as absence of major adverse effects. ther, including novel animal models,
was the case for MVA85A); as it could focus research efforts on
This encouraging result needs follow Mtb eradication by vaccination.
3. Improving BCG, by inserting up for longer periods of time in order to
additional antigens or by genetic determine the longevity of the response,
manipulation of the BCG genome and to assess whether further boost- UNDERSTANDING
to improve its immunogenicity; ing would be required to maintain
or augment the VE. At this stage, the
THE IMMUNE
4. Attenuating Mtb by deleting mechanism of action of M72+AS01E MECHANISMS
essential virulence genes, thus
producing a safe and antigenically
is unknown. It could involve innate
immune driven responses, includ-
BEHIND THE
fully competent Mtb-like vaccine; ing trained innate immune memory PROTECTIVE
5. Alternative delivery routes using
of myeloid cells, and/or adaptive
immune responses (clear CD4+ T cell
EFFECT
existing vaccines, such as BCG, responses were induced by M72) or
for example via the mucosal route both.[3,7] Understanding the immune
(the lung) assuming that the mechanisms behind the protective NEW CLINICAL AND PROMISING
natural route of infection is the effect will be important in order to LATE PRECLINICAL APPROACHES
most relevant route of vaccine systematically improve and further There are, as already outlined in
delivery, inducing local immunity develop this or other similar vaccines. Figure 1, several candidate vaccines in
and immune (resident) memory. Besides determining the longevity of early stage clinical development. This
the protective effect, another relevant includes live vaccines such as recom-
RECENT SUCCESSES IN question is whether M72 also works well binant BCG and attenuated MTBVAC,
TB VACCINE DEVELOPMENT in non-Mtb infected persons, includ- other subunit vaccines such as H56,
Candidate vaccines from all five ing in BCG vaccinated individuals. and aerosol based delivery of BCG into
categories are being evaluated for Notwithstanding these questions, this the human lung.[7] In parallel, advanced
safety and immunogenicity in clinical landmark M72 trial result represents the preclinical evaluation models (usually in
phase 1/2 studies, and some already first promising signal for any new TB non-human primates (NHP)) are being
have been or are being evaluated in vaccine since a century, and now needs used to assess and compare additional
phase 2B/3 studies for vaccine effi- to be evaluated in large phase 3 trials in TB vaccine delivery routes and systems.
cacy (VE) using prevention of disease both infected and uninfected people. Some promising ones include: aerosol
(PoD) or prevention of infection (PoI) / pulmonary delivery of BCG in NHP,
as primary endpoints (Figure 1). A second promising result came from with excellent VE results;[9] intravenous
a BCG revaccination study.[8] In this delivery of BCG (with strong VE results;
Recently the results from two large stud- complex study design both a subunit Seder et al, unpublished), and Rhesus
ies were reported, with highly encourag- (H4/IC31) and a BCG revaccination monkey-CMV vectored multi-antigen
ing outcomes, strongly suggesting that arm were included in a setting in which subunit vaccines that are being tested
better TB vaccines indeed are possible. (sustained) PoI rather than PoD was in NHP models, again with striking
The most important results came from assessed. Infection was defined as VE effects.[10] In addition, combinato-
a study in which a subunit vaccine (cat- having developed a positive immune rial vaccines with heterologous prime/
egory 1 above), called M72 test (IGRA test) against Mtb specific boost-regimens can likely be har-
(a fusion protein consisting of 2 antigens. The most important result, nessed to further optimize protective
immunogenic Mtb antigens), was which had not been anticipated, was immunity induced by vaccination.
given together with a strong adjuvant, that although neither vaccine protected
called AS01E, to adults who were against infection (i.e. IGRA conversion THE IMPORTANCE OF
already latently (that is asymptom- from negative to positive) only BCG TB CORRELATES OF PROTECTION
atically) infected with Mtb.[6] Most Mtb revaccination protected significantly ‘Correlates’, often referred to as ‘bio-
infected people who will develop TB against sustained Mtb infection: in the markers’, are markers that correlate
in their lifetime will do so in the first BCG revaccination arm fewer persons with important biological or medical
4 MT BULLETIN OF NVTG 2019 DECEMBER 04
REVIEW
In-Vivo Expressed Mycobacterium Tuberculosis
outcomes, for example disease or protec- including multi-drug-resistant and Antigens Inducing Human T-Cell Responses
with Classical and Unconventional Cytokine
tion. Unfortunately, there are virtu- extensively drug resistant TB, and to Profiles. Scientific reports. 2016;6:37793.
ally no human correlates of protection help reach the End TB goal by 2035.[1] 6. Tait DR, Hatherill M, Van Der Meeren O et al. Final
analysis of a trial of M72/AS01E vaccine to prevent
against TB. This is a major bottleneck Tuberculosis. New England J Med, 29th October 2019.
7. Andersen P, Scriba TJ. Moving tuberculo-
delaying TB vaccine evaluation and sis vaccines from theory to practice. Nature
prioritisation, because such corre- Tom H.M. Ottenhoff, MD, PhD Reviews Immunology. 2019;19(9):550-62.
8. Nemes E, Geldenhuys H, Rozot V et al. Prevention
lates could help to identify protective Professor of Immunology, Head of Lab Dept of M. tuberculosis Infection with H4:IC31
Vaccine or BCG Revaccination. The New England
antigens, develop improved vaccines, of Infectious Diseases, Head of Immunology journal of medicine. 2018;379(2):138-49.
and allow the demonstration of immu- and Immunogenetics of Bacterial Infectious 9. Dijkman K, Sombroek CC, Vervenne RAW et al.
Prevention of tuberculosis infection and dis-
nogenicity and potential VE at an early Diseases Group, Leiden University Medical ease by local BCG in repeatedly exposed rhesus
stage. Correlates would thus facilitate Center, Leiden, the Netherlands. macaques. Nature Medicine. 2019;25(2):255-62.
10. Hansen SG, Zak DE, Xu G et al. Prevention of
the selection and prioritisation of can- t.h.m.ottenhoff@lumc.nl tuberculosis in rhesus macaques by a cytomegalovirus-
based vaccine. Nature Medicine. 2018;24(2):130-43.
didate TB vaccines for human clinical 11. Zak DE, Penn-Nicholson A, Scriba TJ et al. A blood
RNA signature for tuberculosis disease risk: a prospec-
efficacy testing, and help reduce the tive cohort study. Lancet 2016;387(10035):2312-22.
protracted time scale, large size, and REFERENCES 12. Fletcher HA, Snowden MA, Landry B et al. T-cell activa-
tion is an immune correlate of risk in BCG vaccinated
expense of human efficacy trials, thus 1. WHO. Global Tuberculosis Report. 2019. infants. Nature Communications. 2016;7:11290.
2. Ottenhoff TH, Kaufmann SH. Vaccines against 13. Sloot R, Schim van der Loeff MF, van Zwet EW et
significantly facilitating TB vaccine tuberculosis: where are we and where do we need al. Biomarkers can identify pulmonary Tuberculosis
development. In addition, correlates to go? PLoS pathogens. 2012;8(5):e1002607. in HIV-infected drug users months prior to clini-
3. Kaufmann SHE, Dockrell HM, Drager N et al. cal diagnosis. EBioMedicine. 2015;2(2):172-9.
could help guide preclinical animal TBVAC2020: Advancing Tuberculosis Vaccines 14. Suliman S, Luabeya AKK, Geldenhuys H et al. Dose
from Discovery to Clinical Development. Optimization of H56:IC31 Vaccine for Tuberculosis-
studies and thus help minimize use of Frontiers in immunology. 2017;8:1203. endemic populations. A double-blind, placebo-
animals. Samples from well-defined 4. Tameris MD, Hatherill M, Landry BS et al. controlled, dose-selection trial. American J Respirat
Safety and efficacy of MVA85A, a new tubercu- Critical Care Medicine. 2019;199(2):220-31.
human cohorts with various Mtb losis vaccine, in infants previously vaccinated 15. Penn-Nicholson A, Hraha T, Thompson EG
with BCG: a randomised, placebo-controlled et al. Correction: Discovery and validation of
exposure or infection states, including phase 2b trial. Lancet 2013;381(9871):1021-8. a prognostic proteomic signature for tubercu-
long-term resisters (either resisting 5. Coppola M, van Meijgaarden KE, Franken KL et losis progression: A prospective cohort study.
al. New Genome-Wide Algorithm Identifies Novel PLoS Medicine. 2019;16(7):e1002880.
natural infection induced IGRA conver-
sion or resisting TB progression once
infected), samples from future con-
trolled human mycobacterial challenge SHUTTERSTOCK.COM
models, and – particularly important
– from individuals from trials with TB
vaccines demonstrating protective VE
will be essential for accelerating cor-
relate discovery, testing and validation.
In addition, correlates of risk for
progressing from asymptomatic
(latent) infection towards TB disease
would be extremely useful, e.g. in
stratifying individuals in observational
and clinical intervention studies,
including (therapeutic) vaccination
and drug studies. Several first signa-
tures were reported a few years ago
[11-13]
, and some of these are currently
being further refined (e.g. [14,15]).
Although beyond the scope of this short
review, it is clear that correlate discovery
and evaluation is a second major priority
in the field of TB vaccine development.
CONCLUDING FUTURE OUTLOOK
In very recent years, TB vaccine research
and TB correlate discovery have wit-
nessed significant breakthroughs. This
provides real hope for effective, life-
saving TB vaccines, which are much
needed to control the TB endemic,
DECEMBER 04 2019 MT BULLETIN OF NVTG 5
REVIEW
Malaria vaccine development: silver bullet or shot in
the dark?
D
espite encouraging reduc- RTS,S AS01 (MOSQUIRIX TM) vaccine candidates. The first trials of
tions in the global burden Development of RTS,S started in the RTS,S in African (Gambian) adults were
of malaria in the early 21st late 1980s, following the discovery conducted around the millennium,
century, progress has since that immune responses against P. but efficacy against naturally-acquired
stagnated, particularly in the most Falciparum Circumsporozoite Protein infection proved somewhat disappoint-
heavily affected areas of sub-Sa- (CSP) play an important role in pro- ing, protecting against only about 34%
haran Africa. Implementation of an tection against infection. CSP is the of infections. Despite this setback, over
effective malaria vaccine is con- most abundant protein on the surface the next decade further testing was
sidered essential to bolster existing of sporozoites, the infectious form conducted in children and finally in
tools (e.g., effective case manage- of the parasite transmitted by mos- infants, initially in Mozambique and
ment, intermittent presumptive quitoes to people. The RTS,S vaccine subsequently in pivotal phase-3 trials
treatment, seasonal malaria che- consists of recombinant (synthetically in several counties across sub-Saharan
moprevention, and vector manage- produced) sections of CSP, fused and Africa. RTS,S has consistently demon-
ment) and underpin control, or even combined with recombinant hepatitis B strated a good safety and tolerability
perhaps for eradication of malaria. surface antigen (HBsAg). The addi- profile, but at ~18-36% protection against
Ideally, a malaria vaccine would be tion of HBsAg helps to strengthen the episodes of clinical malaria, efficacy
integrated into the World Health immune response against CSP, but remains well below the target threshold
Organization’s (WHO) Expanded also induces potent immunity against of 75% set by the WHO.[1,2] Protection
Programme of Immunisation, ben- hepatitis B virus. RTS,S is adminis- against severe malaria is lower still (1%
efitting from the programme’s ex- tered in a strong adjuvant, AS01, to to 32%). A partial explanation for this
isting management and logistics in further boost immune responses. relatively disappointing efficacy against
order to effectively target those at naturally-acquired malaria infection
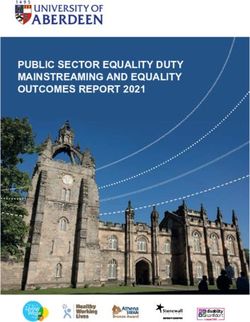
greatest risk for malaria, i.e. infants Figure 1 summarises the developmental may be that the vaccine only protects
and children. history of RTS,S, illustrating just how well against circulating P. falciparum
So where are we currently in terms long such processes can take. Initial strains that genetically resemble the
of malaria vaccine development – clinical testing was conducted in trials vaccine.[3] Moreover, protection is of
do we have a silver bullet in hand, in malaria-naïve U.S. adult volunteers in relatively short duration, waning within
or is it still just a ‘shot’ (of vac- the mid-90s, demonstrating safety and 3 years of initial immunisation. Indeed,
cine) in the dark? After presenting protection against Controlled Human it has been suggested that RTS,S may
some background, we will discuss Malaria Infections (CHMI). Such even cause a rebound-effect, whereby
the current developmental status studies, in which subjects are deliber- susceptibility to malaria is increased in
and prospects of three promising ately infected with laboratory-cultured the long term compared to unvaccinated
examples of vaccines that target malaria parasites under highly con- subjects, at least in high-transmission
Plasmodium falciparum, the most trolled conditions, have proven them- areas, due to slower induction of
severe strain of malaria parasites selves an invaluable tool for advancing naturally-acquired immunity in vaccin-
globally. the clinical development of promising ees.[4] In an attempt to overcome waning
Figure 1: Developmental history of RTS,S AS01 (MosquirixTM) vaccine.
EMA – European Medicines Agency; GSK – GlaxoSmithKline; WRAIR – Walter Reed Army Institute of Research.
6 MT BULLETIN OF NVTG 2019 DECEMBER 04
REVIEW
immunity, a subset of participants in these trials are whether it is feasible and were first pioneered for malaria by
the phase 3 trials were administered a logistically to target vaccine recipients Ruth and Victor Nussenzweig in the
booster dose at 20 months after initial for a booster dose, and whether the 1960s and ‘70s.[6] Sporozoites can be
immunisation; over 3-4 years of follow- marginally increased (but still extremely attenuated by radiation, genetic modifi-
up, protection was indeed poorer in low) risk of cerebral malaria and menin- cation, or concomitant administration of
subjects who did not receive a booster. gitis in children and a slight increase in chemoprophylaxis. The objective in all
Importantly, protection is also relatively all-cause mortality in girls as observed cases is to ensure that these inoculated
poorer in areas of high transmission, in RTS,S recipients in the phase 3 sporozoites abort their development
and in infants as compared to children.[2] studies represent genuine associations before themselves becoming pathogenic
or merely chance post-hoc findings.[5] blood-stage parasites; in the process
Based on these results, in 2015 (some they are exposed to the immune system,
30 years since its first development) ATTENUATED WHOLE inducing protective immune responses
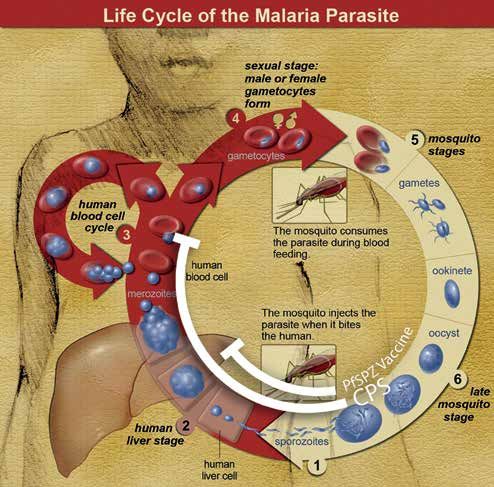
RTS,S nevertheless received regulatory SPOROZOITE-BASED VACCINES against subsequent infections (Figure 2).
approval from the European Medicines In an attempt to improve upon the
Agency – the first malaria vaccine ever protection induced by RTS,S, other In a landmark study, researchers at
to do so. Before taking a decision on researchers have been developing Radboud UMC (Nijmegen) pioneered
whether to recommend the widescale second-generation vaccines consisting a highly efficacious form of immunisa-
implementation of RTS,S, however, of attenuated live sporozoites. Live- tion known as ChemoProphylaxis-with-
WHO has requested further large-scale attenuated vaccines are widely used Sporozoites (CPS), whereby subjects
post-licensure trials. These commenced against other diseases (e.g., measles, are inoculated with infectious sporo-
earlier this year in Ghana, Kenya and yellow fever and BCG for TBC) , are zoites by mosquito bites whilst tak-
Malawi and will last until 2024. Some believed to induce stronger, broader ing anti-malarial prophylaxis (usually
issues that remain to be resolved in and longer-lasting immune responses, chloroquine or mefloquine) to kill any
parasites emerging from the liver
into the blood-stream.[7] Alongside
colleagues from Leiden UMC and
Erasmus MC (Rotterdam), they have
advanced this concept in a series
of successful CHMI studies. This
immunisation strategy, although
not practically implementable
on a large scale in resource-poor
settings, remains the most potent
known method for inducing
immunity against malaria.[8]
The success of CPS has led to
resurgent interest in the potential
of attenuated whole-sporozoite vac-
cines. An important player in this
field has been the U.S. biotech start-
up Sanaria Inc., which pioneered a
method to purify live aseptic P. falci-
parum sporozoites (PfSPZ) from the
salivary glands of laboratory-reared
mosquitoes and cryopreserve these
in vials stored in liquid nitrogen.
These can be shipped all over the
world, thawed and administered
intravenously by needle & syringe.
This has helped to accelerate global
vaccine development by allowing
clinical trials to be conducted where
they are most relevant, in resource-
Figure 2: Life cycle of malaria parasites. Attenuated live sporozoites (white semicircles) abort their development poor settings in sub-Saharan
before becoming pathogenic blood-stage parasites, in the process allowing the host to develop protective immune
Africa. Indeed, Sanaria’s PfSPZ
responses against subsequent infections. Irradiated sporozoites (e.g., PfSPZ Vaccine) arrest early during liver-
stage development. In ChemoProphylaxis-with-Sporozoites (CPS), sporozoites complete liver-stage development Vaccine, consisting of radiation-
but fail to multiply within red blood cells due to concomitant chemoprophylaxis. (Modified from Wikimedia attenuated sporozoites, has over
Commons. Original source: National Institutes of Health.)
DECEMBER 04 2019 MT BULLETIN OF NVTG 7
REVIEW
the past decade undergone testing in this vaccine induced antibodies with
African adults, children and infants potent ability to inhibit invasion.[11] Matthew B.B. McCall, MD, PhD, DTMH
in amongst others Tanzania, Kenya, Clinical parasitologist, Department of
Mali, Gabon and Equatorial Guinee.[9] In parallel with the clinical development Medical Microbiology, Radboudumc,
of these vaccine strategies, state-of-the- Nijmegen, the Netherlands.
Reminiscent of RTS,S however, protec- art technologies such as genetically- matthew.mccall@radboudumc.nl
tion in African populations, particularly attenuated parasite strains and passive
infants, appears to be somewhat poorer immunisation with recombinant mono- Prof. Robert W. Sauerwein, MD, PhD
than in malaria-naïve adult volunteers clonal antibodies are making inroads
Clinical parasitologist, Department of
exposed to CHMI in Europe and the in the P. falciparum vaccine field, with Medical Microbiology, Radboudumc,
U.S. Potential explanations, including significant contributions from research- Nijmegen, the Netherlands.
immaturity of young children’s immune ers in the Netherlands, and offer great
systems, immunosuppressive effects of promise for the future. Moreover, vac-
prior malaria exposure and/or helminth cines against the world’s second most REFERENCES
co-infections, and parasite strain diver- dangerous malaria parasite, P. vivax, 1. Rts S Clinical Trials Partnership. Efficacy and safety
of RTS,S/AS01 malaria vaccine with or without
sity, remain to be elucidated. Despite are also starting to be developed. a booster dose in infants and children in Africa:
these set-backs, PfSPZ Vaccine is set to final results of a phase 3, individually randomised,
controlled trial. Lancet. 2015;386(9988):31-45.
undergo large-scale testing in a phase 3 Malaria vaccine development’s slow 2. Moorthy VS, Newman RD, Okwo-Bele
J-M. Malaria vaccine technology road-
trial in Equatorial Guinee later this year. track record, and particularly the rela- map. Lancet. 2013;382(9906):1700-1.
tively disappointing efficacy of candidate 3. Neafsey DE, Juraska M, Bedford T et al. Genetic
diversity and protective efficacy of the RTS,S/AS01
TRANSMISSION-BLOCKING VACCINES vaccines in naturally-exposed popula- malaria vaccine. N Engl J Med. 2015;373(21):2025-37.
4. Olotu A, Fegan G, Wambua J et al. Seven-Year Efficacy
Vaccines targeting gametocytes (the tions, should of course caution against of RTS,S/AS01 malaria vaccine among young African
parasite forms taken up by mosquitoes hubris. In parallel with empirical children. N Engl J Med. 2016;374(26):2519-29.
5. Guerra Mendoza Y, Garric E et al. Safety profile
to complete malaria’s life cycle) can vaccine development, the field needs to of the RTS,S/AS01 malaria vaccine in infants and
children: additional data from a phase III random-
help to reduce transmission. Although develop a better understanding of funda- ized controlled trial in sub-Saharan Africa. Hum
such a vaccine would not directly mental obstacles to malaria immunity, Vaccin Immunother. 2019;15(10):2386-98.
6. Nussenzweig RS, Vanderberg J, Most H et al.
benefit its recipient, it could reduce including strain-diversity – currently a Protective immunity produced by the injec-
tion of x-irradiated sporozoites of plasmodium
cases of malaria in the community major area of research focus at amongst berghei. Nature. 1967;216(5111):160-2.
and indirectly even the recipient’s others Radboud UMC. That said, ratio- 7. Roestenberg M, McCall M, Hopman J et al. Protection
against a malaria challenge by sporozoite inocu-
own chances of re-infection. Such an nal approaches and dedicated effort have lation. N Engl J Med. 2009;361(5):468-77.
8. Sauerwein RW, Bijker EM, Richie TL. Empowering
altruistic vaccine could conceivably already advanced malaria vaccine devel- malaria vaccination by drug administration.
be added to a multi-component vac- opment well beyond a proverbial shot in Curr Opin Immunol. 2010;22(3):367-73.
9. Richie TL, Billingsley PF, Sim BKL et al. Progress with
cine that also induces direct protec- the dark. Several shiny-looking bullets Plasmodium falciparum sporozoite (PfSPZ)-based
malaria vaccines. Vaccine. 2015;33(52):7452-61.
tion against infection or disease. look set to be added to our anti-malarial 10. Singh SK, Roeffen W, Andersen G et al. A Plasmodium
arsenal and with concerted research falciparum 48/45 single epitope R0.6C subunit
protein elicits high levels of transmission block-
Several candidate vaccines induce one will yet be crafted of true ‘silver’. ing antibodies. Vaccine. 2015;33(16):1981-6.
11. Payne RO, Silk SE, Elias SC et al. Human vac-
potent transmission-blocking immunity cination against RH5 induces neutralizing anti-
in animal models and are currently malarial antibodies that inhibit RH5 invasion
complex interactions. JCI Insight. 2017;2(21).
undergoing clinical development. A
WHO-INT
leading example is Pfs48/45, a game-
tocyte protein shown by researchers at
Radboud UMC to form a critical link
in mosquito-transmission. A recom-
binant vaccine, R0.6C, based on
this protein is set to undergo testing
here in first-in-human clinical tri-
als in 2020, including assessment of
transmission-blocking activity.[10]
PERSPECTIVES
After years of largely unsuccessful
attempts, exciting progress is now
also being made towards a blood-stage
malaria vaccine, based on reticulocyte-
binding protein homolog 5 (RH5) that
plays an essential role in the inva-
sion of erythrocytes by P. falciparum
merozoites. A first phase 1 trial of
8 MT BULLETIN OF NVTG 2019 DECEMBER 04REVIEW
Overcoming the challenges in achieving high
immunization coverage in low-income countries:
the role of Gavi
W
hen Ebola hit West major investment from pharma developing countries. But even though
Africa for the first time ceutical companies. a highly effective vaccine had been
just five years ago, it available in wealthy countries since
was a little known, but Its ability to clear these two hurdles 1982, only a minority of low-income
much feared lethal disease. With no is in part due to the work of Gavi, the countries had so far introduced it. At the
cure or vaccine available it could kill Vaccine Alliance based in Geneva, same time, global coverage of routine
over 50% of people infected.[1] This, which seeks to increase access to new immunization was also plateauing,
and the fact that people were unfa- and underused vaccines in low-income with more than 30 million children
miliar with the disease and the way it countries. At the end of the West in the world’s poorest countries not
spread, is why the disease was able to African outbreak, Gavi sent a signal being fully immunized even with the
sweep across the region infecting more to the market that it would be there to basic vaccines. Gavi’s strategy was
than 28,600 people and killing 11,300 purchase vaccines by committing to to bring together key players at the
of them. Upon the recommendation make up to USD 345 million available global and local level – country govern-
of the European Medicines Agency’s for Ebola vaccines. Then this particular ments, UN agencies, and civil society
scientific committee to recommend vaccine was made available through organizations – to address the major
the approval of conditional market an Advance Purchase Commitment mismatch between the people who had
authorization for the world’s first agreement signed between Gavi and the access to vaccines and the people who
Ebola vaccine (in October 2019), which vaccine manufacturer, Merck, in 2016. could benefit from them the most. By
has been successfully deployed as an Gavi offered a USD 5 million pre-paid harnessing the financial resources and
investigational product to fight the now commitment to Merck in exchange for expertise of these different partners,
waning outbreak in the Democratic doses of the vaccine once it was licensed, Gavi aimed to increase the affordability
Republic of the Congo, the World Health under the condition that Merck would and accessibility of life-saving vaccines.
Organization formally announced its make a stockpile of investigational doses
prequalification in mid-November. In available for outbreak response as well SUSTAINABILITY GOAL
less than half a decade, Ebola has gone as some regulatory requirements. It is The most important partners within this
from being nearly a death sentence these doses that have helped protect over Alliance are the implementing countries
to a vaccine-preventable disease. 254,000 people against Ebola in DRC.[2] themselves. A cornerstone of the Gavi
approach is that the organization works
The significance of this is two-fold. This type of novel approach is indica- together with governments to build sys-
Firstly, national regulatory bodies tive of the unique way that Gavi takes tems that they can sustainably finance
can now choose to expedite their own on the challenges that exist in increas- well into the future, independently of
approval for the ing access to vaccines. Since 2000, Gavi support. The Gavi model requires
vaccine, just the Vaccine Alliance has been help- all countries, no matter how poor, to
five years after ing protect some of the world’s most contribute some proportion of the cost of
the West Africa vulnerable children against deadly the vaccines that they introduce through
outbreak, whereas and debilitating diseases by leverag- Gavi. As a country’s economy grows, as
the whole process ing innovative partnerships, technolo- measured by their gross national income
can normally take gies, and financing mechanisms. per capita, so too does the proportion
well over a decade. that they pay, until it reaches a point
And secondly, it is GAVI’S INCEPTION of transition where the government
a vaccine against In the late 1990s, new and under- has five years to fully fund its vaccine
a disease that used vaccines were not reaching those programmes. So far, 15 countries have
predominantly people most in need of them because transitioned out of Gavi support, with
impacts some of new vaccines were made in low volume three more expected by the end of 2020.
the poorest com- for high priced markets and therefore,
munities in the most vaccines were simply not avail- THE MARKET SHAPING GOAL
world: the type able at prices that their countries could Addressing the affordability side
of vaccine that afford. For example, in 2000, hepatitis involves leveraging predictability
would not tradi- B infections were killing more than of demand and economies of scale
tionally attract 900,000 people a year, the majority in to secure lower vaccine prices. Gavi
DECEMBER 04 2019 MT BULLETIN OF NVTG 9REVIEW
purchases vaccines for half of the IMPACT sub-nationally. This approach aims to
world’s children and secures long-term Since 2000, Gavi has helped protect reach an additional 300 million children
funding from donors, helping create the more than 760 million children with by 2025, saving up to 8 million more
visibility of demand and reducing the vaccines against a range of diseases, lives. But also built into this plan is an
risk of investment for manufacturers. and in doing so has prevented more understanding that many of the greatest
This helps to incentivize manufacturers than 13 million deaths. Coverage with global health challenges we will face are
to sustainably produce vaccines at prices the most basic vaccines has increased those that we cannot plan for. Climate
that these countries can afford. And it from 59% to 81% in Gavi-supported change, antimicrobial resistance, and
works. As of 2018, it cost only USD 27 countries.[4] This has paid dividends not emerging infectious diseases pose an
to immunize a child with a full course just in terms of lives saved but also in ever-evolving risk. As the threats to
of basic vaccines in a Gavi-eligible terms of helping to boost economies. our health become increasingly global-
country, compared to USD 1,300 in In a Gavi-supported country, every dol- ized and increasingly unpredictable,
the US. It has helped to build healthier lar invested in vaccines yields USD 54 the Vaccine Alliance provides a valu-
vaccine markets serving low-income in wider societal benefits,[5] and since able opportunity to get a multitude of
countries: the number of manufactur- 2000 this has translated into more than stakeholders around the same table.
ers who supply Gavi with affordable USD 150 billion in economic gains. All This has already enabled Gavi to help
vaccines has grown from five in 2000 this makes vaccines one of the most protect an entire generation of children.
to seventeen today, now that there is cost-effective public health interventions Efficiency, innovation and collaboration
a viable developing country market. ever. At the same time, vaccines bring will be the names of the game going for-
us closer to the goal of Universal Health ward, to help us make further progress,
Coverage, by acting as a platform that protect the next generation, and ensure
EVERY DOLLAR helps to strengthen primary health care, that by 2030 no one is left behind.
INVESTED IN because vaccines don’t deliver them-
selves. With vaccination comes infra-
VACCINES YIELDS structure, supply chains, cold storage Seth Berkley, MD
USD 54 IN WIDER facilities, trained health care workers,
community outreach, data services, dis-
Epidemiologist and CEO of Gavi,
the Vaccine Alliance.
SOCIETAL BENEFITS ease surveillance, and much more. So, sberkley@gavi.org
when communities get access to vaccina-
tion it puts these people on the map, and
THE SYSTEMS GOAL it is often not long before they also get REFERENCES
Yet accessibility to vaccines relies not access to a host of other critical services. 1. Kucharski A, Edmunds J. Case fatality rates
for Ebola virus disease in West Africa. Lancet
just on the affordability of the vac- 2014; 384(9950):1260. Available from: https://
cines themselves, but on having strong GAVI 5.0 doi.org/10.1016/S0140-6736(14)61706-2
2. World Health Organization. Ebola virus dis-
systems in place to deliver them. This is Ultimately, Gavi is built on the phi- ease Democratic Republic of the Congo: exter-
nal situation report 68/2019. https://www.who.
where local and private sector part- losophy that no-one should die of a int/publications-detail/ebola-virus-disease-
ners play a crucial role in the work of vaccine-preventable disease, regard democratic-republic-of-congo-external-situation-
report-68-2019. [Accessed November 26, 2019].
the Alliance. Worldwide, 19.4 million less of wealth, geography or gender. 3. World Health Organization. Immunization Coverage.
https://www.who.int/news-room/fact-sheets/detail/
children are still missing out on some Yet every year 1.5 million people still immunization-coverage [Accessed October 27, 2019].
vaccines: many of them in remote rural do.[6] Reaching those still missing out 4. World Health Organization. Immunization,
vaccines, and biologicals. https://www.who.
communities, urban slums, displaced will prove increasingly challenging, int/immunization/monitoring_surveillance/
data/en/ [Accessed October 27, 2019].
communities or areas of conflict.[3] Gavi as population growth, rapid urbaniza- 5. ImmunizationEconomics.org. Decade of Vaccine
works with the private sector to harness tion and climate change continuously Economics: return on investment. http://immunizatio-
neconomics.org/dove-roi [Accessed October 27, 2019].
new technologies that can address these move the goalposts. As will the unprec- 6. World Health Organization. Immunization. https://
www.who.int/news-room/facts-in-pictures/detail/
bottlenecks. In Rwanda and Ghana, for edented migration we are seeing with immunization [Accessed October 27, 2019].
example, fleets of autonomous drones a record 70 million displaced people
are now being routinely used to avoid recorded last year. That is why Gavi’s
stockouts by delivering vaccines to new strategy, its fifth, covering strategic
communities across both countries period from 2021-2025, called Gavi 5.0, SO FAR,
when supplies are low or when there
is unexpected demand. Developed by
is prioritizing communities with zero
dose children (children not received
15 COUNTRIES
California-based technology company any routine vaccine doses) who have HAVE
Zipline, and with support from the UPS
Foundation and Gavi, these networks
historically missed out on vaccines. It
also recognizes the need to put gender
TRANSITIONED
are supporting millions of people, more at the centre of our programmatic OUT OF GAVI
increasing the reach of health services
and reducing waste at the same time.
planning, to ensure that communities
are engaged and to offer tailored support
SUPPORT
not just at the national level but also
10 MT BULLETIN OF NVTG 2019 DECEMBER 04REVIEW
The International Coordinating Group on Vaccine
Provision
V
accines are commodities BACKGROUND to pre-finance the purchase of vac-
for which ordinary market Triggered by an outbreak of cerebro- cines, vaccine-related supplies, and
mechanisms do not apply. spinal meningococcal meningitis antibiotics. Countries were expected to
Their development includ- in in 1996 in West-Africa, the ICG reimburse the cost of vaccines drawn
ing clinical testing, the production was established as the International from the ICG stockpiles that were kept
process, their shelf lives, and their Coordinating Group on Vaccine Provision by manufacturers in their warehouses
often very limited supplier base, in for Epidemic Meningococcal Disease. to enable replenishment. In 2002,
combination with unpredictable The outbreak affected primarily the Gavi Alliance (see the article on
disease outbreaks and epidemics, Nigeria and Burkina Faso, with a total GAVI elsewhere in this edition) started
regularly lead to vaccine shortages. of 152,813 confirmed cases and 15,783 providing financial support, initially
It is good to realise that vaccines registered deaths. The actual incidence for the procurement of YF vaccine, later
are a public good and access needs was probably considerably higher. also of Meningitis vaccines (2008) and
to be equitable. From a public OCV (2013). At Gavi’s request, the ICG
health point of view, national Since its establishment, the ICG has stopped the reimbursement require-
health authorities and interna- undergone several changes. In 2001 ment for Gavi support-eligible countries
tional development partners need to Yellow Fever (YF) vaccine was added in 2015. A year later, Gavi decided that
ensure steady supplies and the effi- to its mandate, followed by Oral investments in emergency vaccine
cient and fair distribution of scarce Cholera Vaccine (OCV) in 2013. The stockpiles would no longer be time-
vaccines to places where they are ICG has three guiding principles:[1] bound and that non-Gavi-supported
needed most. With new vaccines • Equity: distribution of vaccines countries were also eligible to access
entering the market and many parts based on public health priorities; vaccines from the stockpiles, in the
of the world in civil or military tur- • Rapid and timely access: deliv- understanding that they would ensure
moil, where outbreaks and epidem- ery of vaccines within a defined replenishment, with Gavi covering the
ics thrive, reliable mechanisms for timeframe to control outbreaks; financial risk in case they failed to do so.
vaccine supply chain management • Independence: decisions made
are of paramount importance. independently of political or The supply division of UNICEF plays a
Vaccination is a main pillar in economic influences, with the sole key role in this process, as it procures
emergency responses and dis- goal of improving public health. all the vaccines for the ICG stock-
ease outbreak management while piles.[2] The revolving funds are now
the vaccine market has gradu- Initially the ICG used a revolving fund dormant, leaving the Gavi Alliance
ally become more complex. Ample
supply is not a given anymore, e.g.
only one manufacturer remains for
the yellow fever vaccine. Ordinary
lead times may be up to two years,
shelf lives differ between different
types of vaccines, and supply chain
requirements have become more
differentiated. Modern vaccines
are very complicated in terms of
production and quality control. As
always, politics reign in this field
as well, necessitating a fair public
health approach which strives for
equity and efficiency.
This article describes the role of The
International Coordinating Group
on Vaccine Provision (ICG) in ensur-
ing that scarce vaccines are avail-
able where they are needed as part
of disease control.
SHUTTERSTOCK.COM / BY JOA SOUZA
DECEMBER 04 2019 MT BULLETIN OF NVTG 11REVIEW
as the sole funding source for these financing, replenishment, monitoring, left the border area in DRC exposed to
stockpiles. Gavi also provides fund- and reporting. In 2015, discussions further spread of the epidemic. The
ing to support the operational costs started about an ICG mechanism for a criteria used during decision-making
of emergency immunization cam- future Ebola vaccine.[3] An ICG Ebola differ among the three stockpiles
paigns in Gavi-eligible countries. expert group is not in place though. because each outbreak has its own
peculiarities. These criteria are publicly
available. [4,5,6] The balance between
responding to single outbreaks and
Country request 1 SUBMISSION
considering the global epidemic
context is and remains delicate. When
Request WHO ICG secretariat 2 CIRCULATION working in epidemic or outbreak set-
more
information tings, public health experts should
IFRC, MSF, UNICEF, WHO 3 DECISION IN 48H be aware of ICG’s existence and its
modus operandi so they can act and
ICG 4 APPROVAL
advise in an appropriate manner.
THE GLOBAL DISEASE
UNICEF SD 5 PROCUREMENT CONTROL CONTEXT
The occurrence of and response to
Manufacturers 6 PACKING AND SHIPMENT
disease outbreaks need to be seen in
the context of global disease control
Vaccines in country 7 ARRIVAL
strategies. In many cases outbreaks are
Payment / Funding 8 PAYMENT / REIMBURSMENT the consequence of insufficient cover-
age of routine immunisation systems
and failure to compensate for that
with effective special immunization
Figure 1: The ICG mechanism (Adapted from: http://www.who.int/csr/disease/icg/qa/en/). activities, including campaigns. While
ministries of health with the support
of various partners usually implement
The ICG Executive sub-Group is consti- The full ICG meets physically twice a control programmes for meningitis, YF
tuted by its 4 founding members: WHO, year as well as through remote digital and cholera through routine preventive
UNICEF-Headquarters, Médecins Sans conferencing in the event of an emer- and reactive immunisation, it is the ICG
Frontières (MSF), and the International gency request. The ICG Secretariat that coordinates the management of
Federation of Red Cross (IFRC). Other based at WHO-HQ plays a central and the three vaccine stockpiles, especially
stakeholders, such as UNICEF’s Supply coordinating role in the entire ICG in emergency outbreak situations.
Division (Copenhagen), Agence de mechanism. It also does price nego-
Médecine Préventive (AMP), Centre tiations through its constituency and 1. CHOLERA
for Disease Control, manufacturers, network, and evaluates interventions In 2013, WHO established the Global
international NGOs, technical agen- and standard protocols for managing Oral Cholera Vaccine (OCV) stock-
cies, financial partners and country vaccine-preventable diseases. Its infor- pile, and the Global Task Force on
representatives (two from countries mality and flexibility is a key strength. Cholera Control (GTFCC) launched a
in the African meningitis belt, plus a Vaccines are allocated based on techni- renewed strategy for cholera control in
third country) support various activities cal and public health criteria without which OCV plays an important role.
of the ICG mechanism, e.g. decision- political or financial considerations. [7]
Many countries are now integrating
making, forecasting of vaccine require- The ICG mechanism is depicted in the use of OCV within their cholera
ments, procurement, and deployment. Figure 1. It aims at delivering vaccines control programs. As of May 2018, over
The ICG Executive sub-Group reviews within a time span of a maximum of 25 million doses had been adminis-
requests not only from countries but 10 days after receipt of the request. tered in 19 countries – of which 41%
also from international organisa- in humanitarian situations, 38% for
tions that act swiftly in the event of Recent major outbreaks – yellow fever outbreaks, and 21 % for endemic areas.
disease outbreaks such as MSF. It can in DR Congo and Angola, cholera in
do so within 48 hours after receipt by Yemen and the Horn of Africa – have 2. YELLOW FEVER
its secretariat of a formal request. confirmed the need for effective man- The Yellow Fever Initiative was launched
agement and distribution of vaccines in 2006 as a joint collaboration of WHO
Standard operating procedures for of which the supply can be unreliable. and UNICEF. In 2016, a new more
emergency stockpiles of meningitis In 2017 for example, the ICG had to specific and comprehensive strategic
and YF vaccine (but not for OCV) are in prevent Angola from procuring large approach towards the Elimination
place for vaccine applications, release, quantities of YF-vaccine that would have of Yellow fever Epidemics (EYE) was
12 MT BULLETIN OF NVTG 2019 DECEMBER 04REVIEW
vaccines/Briefing_OCV_stockpile.pdf?ua=1
developed.[8] It involves a mechanism supply for some time, undermining the 7. https://www.who.int/cholera/task_force/en/
8. https://www.who.int/csr/disease/yellowfev/
that automatically replenishes the emer- smooth implementation of the global eye-strategy-and-global-agendas/en/
gency stockpile to ensure that 6 million polio eradication strategy, it remains 9. Burki T. Ebola virus vaccine receives prequali-
fication. Lancet 2019; 394(10212):1893.
doses are available at all times. The ICG to be seen whether industry can meet https://www.thelancet.com/journals/lan-
cet/article/PIIS0140-6736(19)32905-8/
remains responsible for rapid and inde- the future demand for Ebola vaccine. fulltext?dgcid=raven_jbs_etoc_email
pendent decision-making on the alloca-
tion of YF vaccines during emergencies. CONCLUSION
Since infectious agents can spread faster
3. MENINGITIS than ever after an outbreak, even from
There is no single strategy that com- very remote areas, vaccine-preventable
bines prevention, routine immunisation, disease control is of global public health
and emergency responses for meningi- importance. Both management and
tis. At present the supply of serogroup financing of vaccine development and
A meningococcal conjugate vaccine supply need to be secured through
(MenAfriVac) is adequate and afford- close coordination of all stakeholders:
able, which has helped substantially
to reduce the number and severity of
meningitis outbreaks in countries of
national authorities, international health
organisations, international and national
NGOs, and the vaccine manufacturing
CALL
the African meningitis belt. However,
meningitis outbreaks are now domi-
nated by other meningococcal sero-
industry. The ICG, with its secretariat
based in WHO headquarters, plays a
key role in monitoring and guiding
FOR
groups, for which conjugate vaccine
supplies are insufficient and expensive.
vaccine provision. Its mandate and
capacity need to be safeguarded, free
from any (geo)political interference.
ARTICLES
4. EBOLA While comprehensive and adequate
The recent approval of an Ebola vaccine mechanisms are in place for the three Following a request from
following outbreaks in West-Africa vaccines discussed above that fall within several NVTG working parties
and the eastern part of the Democratic ICG’s mandate, the recent approval of earlier this year, we hereby
Republic of Congo (DRC) shows that an Ebola vaccine shows that there is call for contributions to next
there is political will and funding to political will and funding to develop year's editions of MTb. The
develop new vaccines in a much shorter new vaccines in a much shorter time Editorial Board is planning to
time that ever before. An important that ever before. It is opportune to now cover the following themes:
milestone in 2015 were the trials in also safeguard the provision of Ebola
which more than 16,000 volunteers in vaccine. The ICG could fulfil that role. • Disease modelling
Africa, Europe and the United States
received the rVSV-ZEBOV vaccine. The Acknowledgement: This article is for a sub- • Mental health
vaccine was found to be safe and to stantial part based on the report of an eval-
offer protection against the Ebola virus. uation of the ICG in 2017 by a team from • Orphan diseases
Following further testing during Ebola HERA-Belgium, of which the author was a
outbreaks in DRC/Equateur province member. The author acknowledges the con- • Global Health education
(in May-July 2018) and DRC/North Kivu tributions of fellow team members Dr. Josef
province (still ongoing) and consulta- Decosas, Leen Jille and Marieke Devillé. • Support to church affiliated
tions by the Strategic Advisory Group of hospitals in sub-Saharan
Experts on Immunization (SAGE), the Africa: past and present
Ebola vaccine was formally approved Henri van den Hombergh, MD, MPH
and licensed by WHO in November Public Health consultant, the Netherlands. We would be pleased to receive
2019, just before this paper went to your contributions – in relation
hvdhombe@gmail.com
press.[9] It means that the vaccine can to these themes or any other
now widely be used, rather than under topic – in the form of an article,
certain restrictions (‘expanded access’ REFERENCES news from the working party
or what is also known as ‘compassion- 1. World Health Organization: Review of the in which you are involved, a
International Coordinating Group on Vaccine
ate use’). Ringfencing vaccination in Provision, 2006-2016. WHO Geneva, 2016
letter from the field, a personal
combination with early case detection 2. www.https://www.unicef.org/supply/ viewpoint, or an ethical dilemma
3. International Coordinating Group for Ebola
and widespread vaccination of health Vaccine, 1st Meeting, 11 December 2015 – WHO that you have come across.
Headquarters, Geneva, Switzerland
staff working in outbreak situations will 4. Meningitis guidelines: http://apps.who.int/
certainly boost demand. Considering iris/bitstream/10665/154595/1/WHO_HSE_ The Editorial Board
GAR_ERI_2010.4_Rev1_eng.pdf?ua=1
the experience with bivalent polio 5. Yellow fever guidelines: http://www.who.int/csr/
disease/icg/ICG-request-form-EN.pdf?ua=1
vaccine, which was in short global 6. OCV guidelines: http://www.who.int/cholera/
DECEMBER 04 2019 MT BULLETIN OF NVTG 13You can also read