Use of a Metronome in Cardiopulmonary Resuscitation: A Simulation Study
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Use of a Metronome in
Cardiopulmonary Resuscitation:
A Simulation Study
Elise Zimmerman, MD, MSa, Naiomi Cohen, MDa, Vincenzo Maniaci, MDa, Barbara Pena, MDa, Juan Manuel Lozano, MD, MScb,
Marc Linares, MDa
Determine whether the use of a metronome improves chest compression rate and
OBJECTIVE: abstract
depth during cardiopulmonary resuscitation (CPR) on a pediatric manikin.
A prospective, simulation-based, crossover, randomized controlled trial was
METHODS:
conducted. Participants included pediatric residents, fellows, nurses, and medical students
who were randomly assigned to perform chest compressions on a pediatric manikin with and
without an audible metronome. Each participant performed 2 rounds of 2 minutes of chest
compressions separated by a 15-minute break.
RESULTS: A total of 155 participants performed 2 rounds of chest compressions (74 with the
metronome on during the first round and 81 with the metronome on during the second round
of CPR). There was a significant improvement in the mean percentage of compressions
delivered within an adequate rate (90–100 compressions per minute) with the metronome on
compared with off (72% vs 50%; mean difference [MD] 22%; 95% confidence interval [CI],
15% to 29%). No significant difference was noted in the mean percentage of compressions
within acceptable depth (38–51 mm) (72% vs 70%; MD 2%; 95% CI, 22% to 6%). The
metronome had a larger effect among medical students (73% vs 55%; MD 18%; 95% CI, 8% to
28%) and pediatric residents and fellows (84% vs 48%; MD 37%; 95% CI, 27% to 46%) but
not among pediatric nurses (46% vs 48%; MD 23%; 95% CI, 219% to 14%).
The rate of chest compressions during CPR can be optimized by the use of
CONCLUSIONS:
a metronome. These findings will help medical professionals comply with the American Heart
Association guidelines.
a
Department of Emergency Medicine, Nicklaus Children’s Hospital, Miami, Florida; and bDepartment of Medical WHAT’S KNOWN ON THIS SUBJECT: The
and Health Sciences Research, Florida International University Herbert Wertheim College of Medicine, Miami,
Florida frequency of cardiac arrest is significantly lower
in children than in adults, rendering the delivery
Dr Zimmerman conceptualized and designed the study, coordinated and supervised data collection,
carried out the initial analysis, and drafted the initial manuscript; Dr Cohen coordinated and of high-quality cardiopulmonary resuscitation
supervised data collection, carried out the initial analysis, and drafted the initial manuscript; more difficult. Metronome-based studies in
Drs Maniaci, Pena, and Linares carried out initial analysis and reviewed and revised the manuscript; adults showed improvement in adequate
Dr Lozano provided statistical advice on the study design, carried out initial analysis, and reviewed and
compression rate, with a detrimental effect on
revised the manuscript; and all authors approved the final manuscript as submitted.
the depth of chest compressions.
This trial has been registered at www.clinicaltrials.gov (identifier NCT02511470).
www.pediatrics.org/cgi/doi/10.1542/peds.2015-1858 WHAT THIS STUDY ADDS: This is the first
DOI: 10.1542/peds.2015-1858
pediatric study to confirm that the use of
a metronome during cardiopulmonary
Accepted for publication Aug 18, 2015
resuscitation significantly improves the delivery
Address correspondence to Elise Zimmerman, MD, MS, Department of Emergency Medicine,
Nicklaus Children’s Hospital, 3100 SW 62nd Ave, Miami, FL 33155. E-mail: elisezee@gmail.com
of adequate rate without affecting the
compression depth. This effect was more
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
prominent among medical students and
Copyright © 2015 by the American Academy of Pediatrics
pediatric residents and fellows than nurses.
Downloaded from www.aappublications.org/news by guest on October 19, 2021
PEDIATRICS Volume 136, number 5, November 2015 ARTICLEDespite recent advances in both clinical and animal 100 000 person-years, compared with
resuscitation, such as defibrillation investigations.8,9 Kern et al7 126.52 per 100 000 person-years
technology, survival from cardiac evaluated metronome guidance for adults. To our knowledge no
arrest remains poor.1,2 Without of both chest compressions and study to date has evaluated pediatric
prompt care the chance of survival ventilation on adults, both before and practitioners in performing high-
falls dramatically within minutes after endotracheal intubation. The quality CPR in the setting of
of arrest onset.3 Matos et al3 found combined tone and voice prompt audio metronome use. The low frequency
that survival outcomes in the first guidance they used was effective at of pediatric cardiac arrests compared
15 minutes are linear and decline maintaining the target chest with adults is the basis of our study.
rapidly, highlighting the importance compression rate and avoiding the We report a study of CPR by pediatric
of immediate return of spontaneous common problem of hyperventilation care providers on a pediatric manikin
circulation. Pediatric survival to during CPR by professional rescuers with and without a metronome.
discharge rate after in-hospital (ie, emergency medical technicians). We hypothesized that the use of
cardiac arrests is .25%; in Some studies have suggested that a metronome would improve chest
comparison, 5% to 10% survive rescuer fatigue may decrease the compression rate and depth during
after out-of-hospital cardiac arrests.4 quality of CPR even after 1 minute CPR.
Poor-quality cardiopulmonary of chest compressions, and the rescuer
resuscitation (CPR) has been cited may not recognize this decrease in
as a contributing factor to this dismal performance.6 Jäntti et al8 were able METHODS
to show that participants perceive
statistic on outcomes.4 Optimizing Selection of Participants
more exhaustion when given chest
the CPR technique improves
compressions without metronome A total of 155 participants were
resuscitation success. It is well
guidance, but the measured recruited for this study. Participants
known that immediate delivery
compression depth did not decrease included residents, fellows, and
of high-quality CPR increases
during the 10-minute scenario. They nurses specializing in pediatrics and
survival rates. The key elements of
mentioned that this effect might be medical students rotating in
high-quality CPR are to push hard,
the result of the experience of the pediatrics, who voluntarily
push fast, allow full chest recoil
participants (ICU nurses and members participated from January to July
between compressions, avoid
of the cardiac arrest team). A number 2014. Recruitment took place through
excessive ventilations, minimize
of studies suggest that human factors e-mails, flyers, and directly during
interruptions, avoid preshock pause,
contribute to poor CPR quality, which conferences. Eligibility criteria
resume CPR immediately after shock, includes difficulty in performing CPR included health professionals with
and rotate compressor role every during stressful and chaotic cardiac a minimum of basic life support
2 minutes.5 Therefore, each minute is arrest conditions, the lack of internal training according to the 2010 AHA
critical to achieving both survival and sense of chest compression rate and guidelines and capable of performing
favorable neurologic outcomes.3,6 At depth, rescuer fatigue, and infrequent chest compressions. Verbal consent
the completion of a CPR course, health CPR recertification.1,6 One possible was obtained and demographic data
care professionals are examined and solution to these problems is were collected from the participants,
given a provider card that indicates measuring the quality of resuscitation including time since last CPR training,
course completion. It is assumed by use of an audible metronome professional background, and gender.
that when properly trained health during CPR to better train our
care professionals perform CPR, the pediatric health care providers. Study Design and Setting
American Heart Association (AHA)
Inadequate chest compression rate A prospective, simulation-based,
standards are being met.
and depth are common during CPR crossover, randomized controlled trial
Very high compression rates may even among skilled health care was conducted and approved by the
compromise coronary blood flow providers.1,10 This finding may be Western Institutional Review Board,
due to a significant shortening of more prominent in the pediatric an independent institutional review
the diastolic period, when the setting because of the infrequent board. Participants were randomly
majority of coronary flow occurs. occurrence of cardiac arrests in assigned into 2 CPR rounds by
Too slow a rate delivers too few comparison with adults. Most of the a Microsoft Excel 2010 random
compressions per minute to achieve recommendations for pediatric CPR generator program. The simulation
optimal resuscitation hemodynamics are extrapolated from adult studies. clinical educator used the Excel
and outcomes.1,7 The notion of chest Atkins et al11 found the incidence of software to create a random list of
compression–only CPR (without out-of-hospital nontraumatic cardiac numbers used for the allocation of
ventilations) has gained support from arrest in pediatrics to be 8.04 per participants. One round consisted
Downloaded from www.aappublications.org/news by guest on October 19, 2021
906 ZIMMERMAN et alof chest compressions with an level meter (Amprobe, Everett, WA) the metronome would increase this
audible metronome and the other of to ensure that the noise level percentage to 70% (a relative
chest compressions without an (measured in decibels) was similar improvement of about 25%),
audible metronome that sounded at for each scenario. Video recording a sample of 152 participants was
a rate of 100 times per minute. A of each participant was obtained for used (a = 0.05, paired 2-tailed test,
monitor–defibrillator (Lifepak 15 feedback purposes only. power 80%).
from Physiocontrol, Redmond, WA) Data were collected in the simulation Descriptive data are given as means
with a built-in CPR metronome was laboratory and emergency department with SD or as proportions and 95%
used; it was set to “pediatric with setting with the equipment setup confidence intervals (CIs). Because
airway setting” for this study. The being identical in both locations. this was a crossover trial, a formal
metronome was placed ∼8 feet from Resusci Anne Wireless SkillReporter test for a treatment by period
the participants. The participants software with a personal computer interaction was conducted to assess
were blinded to the specific purpose skill reporting system (Laerdal whether the results had been affected
of the study; they were told that Medical AS, Stavanger, Norway) was by order or carryover effect. Given
they would be participating in an used to record the data for each that no interactions were observed
educational study about CPR training. participant. The manikin wirelessly (data not shown, available upon
Study investigators were not blinded transmitted the information to the request), the analysis was based on
to the study, but all measurements computer and captured data estimates of the within-subject
were collected directly by the including rate, depth, hand position difference in the average of the
software, so investigators had no (hands compressing the sternum), percentage of compressions that were
impact on the data collected. release time (chest fully released within an adequate rate (90–110 per
Participants were informed that back to resting position), and minute) or depth (38–51 mm) with
a metronome would be used downstroke/upstroke ratio and without the metronome.
randomly during 1 of their CPR (amount of time compressing vs Accordingly, differences equal to
sessions, and the rate and depth of decompressing, optimal ratio 0 indicate that there were no changes
chest compressions would be 1.00 [50%/50%]). This information with the metronome, positive values
assessed according to the Pediatric allowed us to determine whether that the metronome improves the
Advanced Life Support (PALS) 2010 the time interval between 2 outcomes and negative values the
AHA guidelines. No participants were compressions matched that of an opposite. 95% CI and P values,
excluded or lost after randomization. adequate rate (90–110 per minute; obtained via t test, were calculated
shorter and longer intervals to determine whether the differences
Methods and Measurements indicated compression rates that observed were statistically
Each participant performed 2 rounds were too fast and too slow, significant. Statistical software used
of 2 minutes of chest compressions respectively) and whether every was SPSS Statistics version 21 (IBM
separated by a 15-minute break to compression was within adequate SPSS Statistics, IBM Corporation).
avoid participant fatigue. Chest depth (38–51 mm). Then we
compressions were performed on determined, for every participant, RESULTS
a Resusci Anne pediatric torso the percentage of compressions
simulator manikin (Laerdal Medical that were within adequate rate and A total of 155 participants were
AS, Stavanger, Norway) placed on depth. Finally, we obtained the mean included in the study (medical
a board on a standard hospital bed of the percentage of compressions students rotating in pediatrics, n = 55;
and mattress and adjusted to the within adequate rate and depth with pediatric nurses, n = 33; and pediatric
participant’s comfort level. In and without the metronome, which residents and pediatric fellows,
addition, a step stool was provided to were the primary outcomes. n = 67). There were varying levels of
those participants who chose to use basic and advanced life support
one. Participants were also advised to Primary Data Analysis training, most obtained within the
take off any items (eg, ID badge, We calculated sample size by using previous 12 months. See Table 1 for
stethoscope, watch) that may data provided by Buléon et al12 in participant characteristics.
interfere with delivery of high-quality a crossover study involving medical Of the 155 participants, 74 were
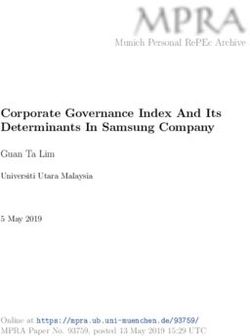
chest compressions. All participants students performing CPR on randomly assigned to have the
conducted chest compressions on the a manikin with and without metronome on during the first round
same manikin. To simulate a more a CPRmeter. Fifty-six percent of of CPR, and the remaining 81
accurate cardiac arrest environment, compressions were in the appropriate participants had the metronome on
background “crowd noise” was used range without the use of during the second round. All
and measured with an SM-10 sound a metronome. Assuming that use of participants completed the 2 rounds
Downloaded from www.aappublications.org/news by guest on October 19, 2021
PEDIATRICS Volume 136, number 5, November 2015 907TABLE 1 Characteristics of Study Exploratory subgroup analyses were of CPR as early as the third minute
Participants (n = 155) performed on adequate compression of continuous chest compressions.
Characteristic N (%) rate by training level (Table 2). When These outcomes support the
Level of training and background we compared the percentage pediatric advanced life support
Medical student rotating in 55 (36) of adequate compression rate by concept of “push-as-fast-as-you-can”
pediatrics training level, we noted that the to emphasize organization of care
Pediatric residents and fellows 67 (43)
metronome had a significant effect around 2-minute periods of
Pediatric nurse 33 (21)
Women 87 (56) among medical students rotating uninterrupted CPR.16
Men 68 (44) in pediatrics (73% vs 55%; MD 18%; There have been metronome-based
CPR training 95% CI, 8% to 28%) and pediatric studies illustrating improvement of
BLS only 30 (19) residents and pediatric fellows
BLS and PALS 125 (81) adequate compression rate, but,
(84% vs 48%; MD 37%; 95% CI,
Time (mo) since last CPR training unlike our study, they demonstrated
,6 35 (23) 27% to 46%) but not for pediatric
a negative impact on the depth of
6–12 80 (52) nurses (46% vs 48%; MD 23%;
chest compressions.18,19 Our study
.12 40 (26) 95% CI, 219% to 14%).
focused on rate-only feedback from
BLS, basic life support; PALS, pediatric advanced life
support. a metronome because it is easily
DISCUSSION
accessible as part of the defibrillator
To our knowledge, this is the first machine on code carts and the
of chest compressions (Fig 1). Mean pediatric manikin-based simulation defibrillators in the resuscitation
levels of environment background study assessing pediatric practitioners room. The actual cause of suboptimal
crowd noise during rounds with the performing chest compressions with chest compression depth with
metronome on and off were almost and without a metronome. Our results metronome guidance is unknown.
identical (67.9 dB vs 67.5 dB; mean illustrate how metronome guidance However, it has been hypothesized
difference [MD] 0.4 dB; 95% CI, 20.01 improves the delivery of chest that various factors could contribute
compressions at an adequate rate but to shallower compressions, including
to 0.7).
has no effect on the depth. These multitasking, rescuer fatigue, and
There was a statistically significant findings are in accordance with rescuer distraction (concentrating on
improvement in the mean percentage several adult studies showing similar rate management rather than
of compressions delivered within an results.8,13 Our study focused on CPR maximal effort).18–20 The effect of
adequate rate with the metronome with only chest compressions rather greater compression depth is
on compared with the metronome off than the addition of ventilation, associated with increased coronary
(72% vs 50%; MD 22%; 95% CI, 15% leading to a shorter delay to chest perfusion pressure, higher success
to 29%) (Table 2). This difference was compressions. Initiating chest of defibrillation, increased cardiac
explained by a decrease in the mean compressions early is of utmost output, and improved clinical
percentage of compressions that were importance, as emphasized by the outcomes.21,22 A compression depth
too fast (21% vs 39%; MD 218%; changes in the traditional of 5 cm is more effective than 4 cm
95% CI, 224% to 212%). The total airway–breathing–circulation
in children and adults. The most
number of compressions during 2 sequence to the current
recent AHA guidelines recommend
circulation–airway–breathing
minutes was lower with the a compression depth of $5 cm in
metronome on than with the sequence put forth in the 2010
children and adults, in hopes to
resuscitation guidelines.14–16 These
metronome off (210.6 vs 221.9; eliminate confusion when ranges
guidelines are supported by Kern
MD 211.3 compressions; 95% CI, of depth are provided.16 The overall
et al,9 who demonstrated that only
215.8 to 26.8). No statistically quality of CPR is highly dependent
chest compressions in early cardiac
significant difference was noted when on multiple factors, but most
arrest provides reasonable
we compared the mean percentage of importantly on rate and depth.
circulation, does not compromise
compressions within acceptable depth Therefore, devices that combine
survival, and is associated with
(72% vs 70%; MD 2%; 95% CI, 22% successful outcomes. In addition,
audible feedback on both rate and
to 6%) or the mean compression depth may improve CPR quality.18
in an attempt to minimize the
depth (43.8 mm vs 44.0 mm; effect of rescuer fatigue, we In our study the level of background
MD 20.2 mm; 95% CI, 21.0 to 0.6). selected a 2-minute time limit for noise was controlled for and
Metronome guidance had no effect compressions. Furthermore, the therefore similar in each group.
on percentage of good hand position, importance of rescuer fatigue The direct impact of background
percentage of adequate release, was highlighted by Hong et al17 to noise could not be assessed because
or mean downstroke/upstroke ratio. substantially diminish the quality the actual noise level in a pediatric
Downloaded from www.aappublications.org/news by guest on October 19, 2021
908 ZIMMERMAN et alguidance on subgroups. The
subgroups analyzed were not
prespecified and were conducted for
exploratory purposes only, to generate
hypotheses for future research.
Metronome guidance increased the
percentage of adequate compression
rate for medical students rotating in
pediatrics and pediatric residents and
fellows but not for pediatric nurses.
This difference could be attributed
to the level of training. Audible
metronome guidance helped improve
the percentage of compressions
delivered at an adequate rate despite
the length of time since participants
completed their last CPR training.
In agreement with Handley and
Handley’s24 study regarding an
audible feedback system, our study
suggests that incorporating an audible
metronome in monitors, defibrillators
FIGURE 1
Participant flowchart. and automated external defibrillator
devices, in both hospital and
community settings, could lead to
cardiac arrest case is unknown. You measuring the noise level in pediatric improved performance and delivery
et al23 mentioned that in certain cardiac arrest cases might be helpful of high-quality CPR during pediatric
community environments noise levels to determine the impact of noise resuscitation attempts. Not only can
measured to be .70 dB were found level on quality of CPR. metronome guidance help with rate
to cause irritation and hearing Additional analysis allowed us to control of chest compressions, as
impairment. Additional studies compare the effect of metronome demonstrated in our study, it can
also help with ventilation rate
(hyperventilation is a common
TABLE 2 Outcome Variables With and Without Metronome Guidance (n = 155) problem during actual cardiac arrest
Metronome Difference (95% CI) P resuscitation efforts).20
On Off The AHA recommends periodic
Percentage of compressions with adequate 72 (38) 50 (43) 22 (15 to 29) ,.001 assessment of rescuer knowledge
rate and skills, although optimal timing
Percentage of compressions within 72 (39) 70 (41) 2 (22 to 6) .29 and methods for these are not
acceptable depth known.16 We recommend that
Total number of compressions 210.6 (31.2) 221.9 (32.7) 211.3 (215.8 to 26.8) ,.001
metronome guidance be
Compression rate per min 106.6 (17.5) 112.0 (17.1) 25.4 (28.1 to 22.7) ,.001
Percentage of compression rate too fast 21 (36) 39 (45) 218 (224 to 212) ,.001 incorporated into CPR training,
Percentage of compression rate too slow 8 (24) 11 (27) 22 (26 to 2) .32 the rate of which could be easily
Mean compression depth (mm) 43.8 (10.8) 44.0 (11.3) 20.2 (210 to 0 6) .63 adjusted to comply with the frequent
Percentage of compressions too shallow 28 (39) 30 (40) 22 (26 to 2) .31 guideline updates. Furthermore,
Percentage of compression with correct 90 (25) 92 (23) 22 (25 to 2) .32
we agree with the AHA
hand position
Percentage of compressions adequate 83 (32) 82 (32) 1 (23 to 4) .78 recommendations and suggest an
release increased need for more frequent
Noise level (dB) 68 (4) 68 (4) 0.4 (20.01 to 0.7) .05 CPR training with the use of
Downstroke upstroke ratio 90 (18) 89 (17) 2 (21 to 4) .2 refresher courses. This training is
Percentage of ACR, medical students 73 (39) 55 (44) 18 (8 to 28) .001
especially necessary for medical
rotating in pediatrics
Percentage of ACR, pediatric residents and 84 (30) 48 (43) 37 (27 to 46) ,.001 professionals working within the
pediatric fellows pediatric population because of the
Percentage of ACR, pediatric nurses 46 (41) 48 (44) 23 (219 to 14) .75 low number of cardiac arrest events
Data are presented in means (SDs) unless otherwise indicated. ACR, adequate compression rate. among children. Studies have shown
Downloaded from www.aappublications.org/news by guest on October 19, 2021
PEDIATRICS Volume 136, number 5, November 2015 909that as one goes without CPR training account. Fourth, no formal trials assessing the effect of
refresher courses, the quality of CPR feedback was obtained on how a metronome in delivering
performance deteriorates in as little participants felt about the audible compressions at an adequate rate
as 3 months.20 Because of the low metronome and whether it affected and depth in real-life pediatric
frequency of pediatric codes, we believe the quality of their chest cardiac arrest cases.
there should be more frequent pediatric compressions. Finally, participant
code simulations or refresher courses fatigue was not assessed, which is
during pediatric residency and important especially with the ACKNOWLEDGMENTS
pediatric fellowship training. ongoing changes in CPR guidelines Nicklaus Children’s Hospital, formerly
There are several limitations to our (ie, the number of chest Miami Children’s Hospital Human
study. First, the actual environment compressions and compression Patient Simulation Program
in which the study was performed depth). Many of these limitations Department, provided the equipment
might be artificial. Although we could affect future studies and used to collect the data. The authors
attempted to simulate as close to should be taken into consideration thank the simulation clinical educator,
a medical resuscitation when additional research is Beth Ann Ramey, RN, and the
environment as possible with conducted. simulation technicians, Zeshan Khan
background noise, the actual noise and Jason Cheleotis, for their support
and stress level of being in a real and dedication to this study. We also
CONCLUSIONS thank all the participants who
resuscitation setting could not be
simulated. Second, code situations It is well known that prompt volunteered and made this study
with real-life cases were not used response to cardiac arrest and possible.
for the study. Instead, the proper delivery of high-quality
compressions were performed on chest compressions increases
a pediatric manikin, so patient meaningful survival in patients. ABBREVIATIONS
outcomes were not measured. Our data indicate that the use of a
AHA: American Heart Association
Third, participants were asked only metronome improves the accuracy
CI: confidence interval
to perform chest compressions, of the rate of compressions
CPR: cardiopulmonary
and therefore the importance of delivered to a pediatric manikin.
resuscitation
pauses for ventilation and tracheal These data are encouraging and
MD: mean difference
intubations was not taken into support the need for future clinical
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Abella BSMP, Sandbo N, Vassilatos P, Investigators. Duration of on the quality of chest compressions.
et al. Chest compression rates during cardiopulmonary resuscitation and Resuscitation. 1998;37(3):149–152
cardiopulmonary resuscitation are illness category impact survival and
7. Kern KB, Stickney RE, Gallison L, Smith
suboptimal: a prospective study during neurologic outcomes for in-hospital
RE. Metronome improves compression
in-hospital cardiac arrest. Circulation. pediatric cardiac arrests. Circulation.
2013;127(4):442–451 and ventilation rates during CPR on
2005;111(4):428–434
a manikin in a randomized trial.
2. Milander MM, Hiscok PS, Sanders AB, 4. Topjian AA, Berg RA, Nadkarni VM. Resuscitation. 2010;81(2):206–210
Kern KB, Berg RA, Ewy GA. Chest Pediatric cardiopulmonary resuscitation:
compression and ventilation rates advances in science, techniques, and 8. Jäntti H, Silfvast T, Turpeinen A, Kiviniemi
during cardiopulmonary resuscitation: outcomes. Pediatrics. 2008;122(5): V, Uusaro A. Influence of chest
the effects of audible tone guidance. 1086–1098 compression rate guidance on the
Acad Emerg Med. 1995;2(8):708–713 5. Al-Shamsi M, Al-Qurashi W, de Caen A, quality of cardiopulmonary resuscitation
Bhanji F. Pediatric basic and advanced life performed on manikins. Resuscitation.
3. Matos RI, Watson RS, Nadkarni VM, et al;
support: an update on practice and 2009;80(4):453–457
American Heart Association’s Get With
The Guidelines–Resuscitation (Formerly education. Oman Med J. 2012;27(6):450–454 9. Kern KB, Hilwig RW, Berg RA, Ewy GA.
the National Registry of 6. Ochoa FJ, Ramalle-Gómara E, Lisa V, Efficacy of chest compression-only BLS
Cardiopulmonary Resuscitation) Saralegui I. The effect of rescuer fatigue CPR in the presence of an occluded
Downloaded from www.aappublications.org/news by guest on October 19, 2021
910 ZIMMERMAN et alairway. Resuscitation. 1998;39(3): emergency cardiovascular care. dispatcher-assisted compression-only
179–188 Circulation. 2010;122(18 suppl 3): cardiopulmonary resuscitation by an
10. Dine CJ, Gersh RE, Leary M, Riegel BJ, S862–S875 untrained layperson: a randomised
Bellini LM, Abella BS. Improving 15. Kleinman ME, Chameides L, Schexnayder controlled simulation study using
cardiopulmonary resuscitation quality SM, et al. Part 14: pediatric advanced life a manikin. Emerg Med J. 2013;30(8):
and resuscitation training by combining support: 2010 American Heart Association 657–661
audiovisual feedback and debriefing. Crit guidelines for cardiopulmonary 20. Abella BS. The importance of
Care Med. 2008;36(10):2817–2822 resuscitation and emergency cardiopulmonary resuscitation quality.
11. Atkins DL, Everson-Stewart S, Sears GK, cardiovascular care. Circulation. 2010; Curr Opin Crit Care. 2013;19(3):175–180
et al; Resuscitation Outcomes 122(18 suppl 3):S876–S908 21. Yun SW, Lee BK, Jeung KW, et al. The
Consortium Investigators. Epidemiology 16. Hazinski MF, Chameides L, Hemphill R, effect of inclined step stool on the
and outcomes from out-of-hospital Samson RA, Schexnayder SM, Sinz E, eds. quality of chest compression during in-
cardiac arrest in children: the Highlights of the 2010 American Heart hospital cardiopulmonary resuscitation.
Resuscitation Outcomes Consortium Association guidelines for CPR and ECC. Am J Emerg Med. 2014;32(8):851–855
Epistry-Cardiac Arrest. Circulation. 2009; 2010. Available at: www.heart.org/idc/ 22. Kramer-Johansen J, Myklebust H, Wik L,
119(11):1484–1491 groups/heart-public/@wcm/@ecc/ et al. Quality of out-of-hospital
12. Buléon C, Parienti JJ, Halbout L, et al. documents/downloadable/ucm_317350.pdf cardiopulmonary resuscitation with
Improvement in chest compression 17. Hong MY, Tsou JY, Tsao PC, et al. Push- real time automated feedback:
quality using a feedback device fast recommendation on performing a prospective interventional study.
(CPRmeter): a simulation randomized cardiopulmonary resuscitation causes Resuscitation. 2006;71(3):283–292
crossover study. Am J Emerg Med. excessive chest compression rates, 23. You JS, Chung SP, Chang CH, et al. Effects of
2013;31(10):1457–1461 a manikin model. Am J Emerg Med. 2014; flashlight guidance on chest compression
13. Paal P, Pircher I, Baur T, et al. Mobile 32(12):1455–1459 performance in cardiopulmonary
phone-assisted basic life support 18. Oh JH, Lee SJ, Kim SE, Lee KJ, Choe JW, resuscitation in a noisy environment.
augmented with a metronome. J Emerg Kim CW. Effects of audio tone guidance Emerg Med J. 2013;30(8):628–632
Med. 2012;43(3):472–477 on performance of CPR in simulated 24. Handley AJ, Handley SA. Improving CPR
14. Berg MD, Schexnayder SM, Chameides cardiac arrest with an advanced airway. performance using an audible
L, et al. Part 13: pediatric basic life Resuscitation. 2008;79(2):273–277 feedback system suitable for
support: 2010 American Heart 19. Park SO, Hong CK, Shin DH, Lee JH, incorporation into an automated
Association guidelines for Hwang SY. Efficacy of metronome sound external defibrillator. Resuscitation.
cardiopulmonary resuscitation and guidance via a phone speaker during 2003;57(1):57–62
Downloaded from www.aappublications.org/news by guest on October 19, 2021
PEDIATRICS Volume 136, number 5, November 2015 911Use of a Metronome in Cardiopulmonary Resuscitation: A Simulation Study
Elise Zimmerman, Naiomi Cohen, Vincenzo Maniaci, Barbara Pena, Juan Manuel
Lozano and Marc Linares
Pediatrics 2015;136;905
DOI: 10.1542/peds.2015-1858 originally published online October 12, 2015;
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/136/5/905
References This article cites 23 articles, 8 of which you can access for free at:
http://pediatrics.aappublications.org/content/136/5/905#BIBL
Subspecialty Collections This article, along with others on similar topics, appears in the
following collection(s):
Emergency Medicine
http://www.aappublications.org/cgi/collection/emergency_medicine_
sub
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on October 19, 2021Use of a Metronome in Cardiopulmonary Resuscitation: A Simulation Study
Elise Zimmerman, Naiomi Cohen, Vincenzo Maniaci, Barbara Pena, Juan Manuel
Lozano and Marc Linares
Pediatrics 2015;136;905
DOI: 10.1542/peds.2015-1858 originally published online October 12, 2015;
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/136/5/905
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2015
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
Downloaded from www.aappublications.org/news by guest on October 19, 2021You can also read