Università Campus Bio-Medico di Roma - IRIS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Università Campus Bio-Medico di Roma
Corso di dottorato di ricerca in
Scienze Biomediche Integrate e Bioetica
XXXIV ciclo a.a. 2018-2019
From the disease phenotype to the clinical actionable
information: the digital revolution of Parkinson’s disease.
Dott. Massimo Marano
Coordinatore Tutor
Prof Raffaele Antonelli Incalzi Prof. Prof Vincenzo Di Lazzaro
15 giugno 2022
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Index
• General background
1. An overview on PD epidemiology and pathophysiology
2. Pre-motor, motor, and non-motor aspects of the disease
3. Wearables in PD, history, and perspectives
4. A patient centered approach for an actionable information
• Specific introductions
1. The case of tremor
2. The case of dysphagia
3. The remote patient monitoring
• Aims of the study
• General methodology
• Clinical/epidemiological studies
§ The case of cardinal symptoms: tremor
§ The case of axial symptoms: dysphagia
• Remote monitoring studies
§ On demand monitoring and feasibility and post-hoc studies
• On the road to the continuous monitoring and final conclusions
• References
2
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Background and aims
An overview on Parkinson’s disease epidemiology and pathophysiology
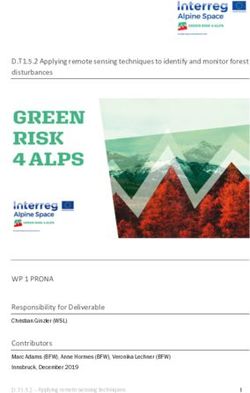
Parkinson’s disease (PD) is the second neurodegenerative disease in prevalence following
Alzheimer's disease. It is a leading cause of disability, counting nearly 8 million cases worldwide so
far, and is destined to count to 14 million cases in 2040 (Figure 1) [Dorsey et al., 2018]. In Italy, PD
counts 300-500 thousand cases with some uncertainties in numbers due to the fact that they are
obtained indirectly (drugs prescriptions, insurances, public health service data coding) [von
Campenhausen et a., 2005; Cicero CE et al., 2021].
Figure 1: the rise of Parkinson’s disease pandemic. Adapted by Dorsey et al., 2018.
PD is a neurodegenerative disease with a pathogenesis that is still largely unknown. From a brief
neurobiological perspective, the mitochondrial dysfunction with other concurring factors (figure 2)
3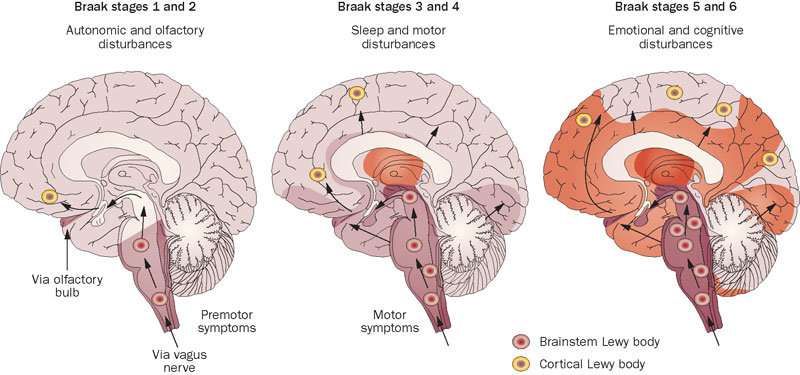
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. are likely to play a significant role together with the alpha-synuclein deposition and the Lewy body formation in generating the pathophysiological counterpart of the disease. Figure 2. Biological factors in the interplay of PD pathogenesis, adapted by Anthony et al., 2013. His clinical picture, intended as characterized by slowness of movement, rigidity and tremor, has been considered as caused by a dopaminergic dysfunction in the nigrostriatal pathway for decades. However, this seminal “reductionist” view of PD as a nigral pathology is currently substituted by a more “holistic” and systemic picture that postulate that several neurobiological systems (other than the dopaminergic one) justify the complex neurobiological and clinical picture of the disease (figure 3) (Anthony et al., 2013). Figure 3. From the reductionist to the holistic PD pathophysiology, adapted by Anthony et al., 2013. 4

Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Despite the PD pathogenesis is still controversial and the current causative role of the disease
pathological hallmarks is still debated, alpha-synuclein aggregates (figure 4a) in Lewy bodies.
Figure 4a. Alpha-synuclein aggregation in fibroblast from a PD of our series. The picture is
courtesy of Dr Casamassa and Dr Rosati (unpublished data).
This should happen according to the Braak’s hypothesis that broadly evolves with the clinical
picture (figure 4b).
Figure 4: schematic view of the Braak staging, adapted from Braak et al., 2003
5
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. The disease progresses along years in an ineluctable but variable and subjective fashion through the modified Hoehn and Yahr scale (ranging from score 1 to score 5) [Hoehn and Yahr, 1967; Goetz et al., 2004]. The latter resume the patient gross advancement in terms of motor disability (Figure 5). Figure 5: the modified Hoehn and Yahr staging. Adapted from PD workbook by We Move 2006. Motor, pre-motor and non-motor Parkinson’s disease PD patients exhibit a highly disabling and progressive motor phenomenology. Some clinical features, that we are going to discuss briefly in this chapter, made the disease suitable for a graphic representation since its early descriptions (figure 6). 6

Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Figure 6: the “Paralysie Agitante”, JM Charcot drawings on Parkinson’s disease posture and gait.
Adapted from Walusinski 2018.
The early identification of motor signs is the key to reaching the clinical diagnosis. This should be
coupled with a genuine non-motor and pre-motor signs and symptoms characterization according to
the known clinical diagnostic criteria by UK Brain Bank and the MDS consensus [Postuma et al.,
2015]. Clinical picture should be coupled with nuclear imaging (figure 7) and with a punctual
analysis of red flags signs that let the clinician address his diagnostic suspect toward atypical
parkinsonism more than PD [Postuma et al., 2015].
Non-motor symptoms (table 1) have a leading role in both the pre-motor phase, when they could
grossly predict the disease onset and phenotypes, and the overt phase when they have a significant
detrimental effect over the patient's quality of life.
7
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Table 1. Examples of non-motor manifestations of PD listed by categories.
Psychiatric Gastrointestinal Autonomic Cognitive Other
Depression Stypsis Sweating Mild cognitive Insomnia
impairment
Anxiety Abnormal gastric Sialorrhea Late dementia Excessive
emptying daytime
sleepiness
Apathy Orthostatic REM sleep
hypotension behavior
disorders
Hallucinations Nocturia and Fatigue
urinary
symptoms
Compulsive Anosmia
behavior
Pain
Cardinal motor features such as bradykinesia, rigidity, resting tremor and postural instability/gait
dysfunction are combined in attributing the core motor phenotype to the disease. All of them, with a
special mention for bradykinesia/rigidity/tremor, exhibit a significant improvement by the
dopaminergic medications - i.e., L-DOPA and related medications.
A general view of PD clinical pre-motor, motor and non-motor progression is depicted in figure 7.
8
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Figure 7. Pre-motor, motor and non-motor progression of PD over a 40 years span, adapted by
Kalia & Lang 2015.
Broadly, L-DOPA, coupled with DOPA-decarboxylase-inhibitors (DDCI), can trigger the quiescent
dopaminergic network after being metabolized to dopamine by astrocytes in the brain and - despite
L-DOPA is not the former neither the latter medication that has been found as effective in PD - after
more the 50 years since its discovery L-DOPA is still the gold standard for treating the disease
[Hauser, 2009] (figure 8).
Figure 8: a brief overview of pharmacological therapy and trials in Parkinson’s disease. Adapted
from Bloem et al., 2021.
9
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. However, the chronic use of L-DOPA, together with the supersensitization of the dopaminergic neurons lead to the development of motor fluctuations with motor and non-motor “OFF” states and dyskinesias during the “ON” medication states. This reduces the therapeutic L-DOPA window and represents a serious detrimental factor for patient quality of life (figure 9). Figure 9. Motor fluctuations in the progression of PD. Physicians who are involved in PD care and research need to score the disease motor and non-motor features with tools and rating scales in order to monitor the disease progression. This is possible with the Hoehn and Yahr scale (modified) and, more commonly, with the Unified Parkinson’s Disease Rating Scale, its modified MDS endorsed version and other non-motor and quality of life questionnaires able to identify all the aspects of the disease burden (MDS Task force on Rating Scales in PD, 2003). The MDS-UPDRS part III and the UPDRS 3 rank all the PD motor symptoms. These scales are both subjectively assessed by the clinician and attribute a subscale score and a total score to the patient that are currently used in the validation process of new clinimetric technologies (figure 10). 10
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Figure 10a. A wearable sensor system to detect bradykinesia and its correlation with the UPDRS
score adapted from Mentzel et al., 2016.
The latter are aimed at improving the objective assessment of the disease and are projected to a
more ecologic patient view, moving from laboratories to the subject house the observation point and
will match with the possibility of stream the brain patient activity through new devices (figure 10b).
Figure 10b. Intraoperative recordings performed by our research team in collaboration with Prof
Brow and Dr Torrecillos shows the brain activity (subthalamic nucleus) of a PD patient during
surgery and how this could be interrupted by artifacts. The possibility of obtaining data by new
closed devices will let us to explore the brain without the occurrence of such artifacts and the
possibility of streaming the brain activity of patients “live”.
11Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. Wearables in PD, history and perspectives - toward the remote patient monitoring “To measure is to know, if you cannot measure it, you cannot improve it” (WT Kelvin). The need of symptom measurement has always featured the modern neurology since the time of Jean Martin Charcot observations (Figure 11). Figure 11. The Charcot’s myographic curves, acquired with a tambur like mechanism by a multiple sclerosis patient and a PD patient Figure adapted from Lanska et al., 2001. Patient symptom objective measurement has made a long road before reaching a tangible clinical reliability. For instance, it was the end of the 19th century when researchers such as Braune and Fisher investigated wearable systems to study the human gait (Baker 2006). 12
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Figure 12. The Braune and Fisher subject wearing the experimental suite made up Geissler tubes
strapped to his body. Adapted from Baker 2006.
For instance, the current available technologies for analyzing the human gait are expensive and far
to be portable - just imagine a computerized gait analysis system that requires force platforms,
systems of cameras for the optometric control and surface electromyography to allow a control on
muscle activities (Whittle 1996, figure 13).
Figure 13. representation of modern gait analysis. Adapted by Whittle 1996 and other anonymous
sources.
13Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. Hence, to match the need of patients and clinicians to own an accessible monitoring system it is necessary to adopt smaller and wearable technologies. Indeed, the use of wearable devices such as inertial motion units (IMUs), that can catch movement dynamic features, is spreading in research and clinical neurology. However, the use of multiple sensors is generally limited to supervised “in lab” experiments. To such regard, supervised vs unsupervised assessments differ in terms of several characteristics. Ecologic monitoring is considered a more trustable kind of patient monitoring able to provide more real information about dynamic patient conditions (e.g. gait features) with some limitations further discussed (Warmerdam et al., 2020 - figure 14). Figure 14. Supervised vs unsupervised monitoring. 14
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Moving to the patient environment is a “to-do” in the list of the clinical neurologist activity. Hence,
using mobile technologies and wearable sensors is going to be necessary. Among trustable wearable
technologies, smartphones (embedded with powerful single IMU sensors or single sensor) are on
the rise. Indeed, they are already perfectly merged with any human environment. Smartphones seem
to be perfect tools to move from a supervised active testing (which imposes a strict behavioral
control of the tested subject) to a passive unsupervised testing (which is totally ecologic but might
be confounded by contextual factors).
Smartphones are able to capture motion information similarly to those detected by conventional
motion capture systems and “in lab” wearables (Tchelet et al., 2019). They can provide a wireless
transmission of data to the server and through apps or offline machine learning it is possible to use
modern algorithms to summarize and extract all the chosen features with (e.g., data labeling) or
without human intervention. This led to clinical event prediction thanks to the concept that are at
the basis of the actionable information logics (Little et al., 2021; Figure 15).
Figure 15. Smartphones embedded sensors and workflow towards their clinical utility. Adapted by
Little et al., 2021.
15Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. A patient centered approach for the actionable information As depicted in the previous paragraphs, PD is a heterogeneous disease with some fixed features (e.g. cardinal motor symptoms) acting with a pivotal role with respect to the other highly variable conditions (e.g. non-motor manifestations, progression rates, variable disease phenotypes, clinical response to therapies). Nevertheless, doctors need to find objective markers for staging the disease and rating symptoms - these markers might not match the patient's feelings, expectations or the real burden of a specific symptom in a patient's life creating a gap between the actors of the PD care: the patient, the caregiver and any other healthcare team member. Figure 16. The gap between PD patients and doctors and the need of a patient centered approach, adapted from Bhidayasiri et al., 2020. 16
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
In a survey by Mathur and colleagues (2017) performed on 492 PD subjects, authors found that
patients are interested in monitoring their symptoms (87%) and letting the clinician know about
their disease pattern by a monitoring system (in 97% it was very or moderately important). Subjects
thought that disease monitoring would help clinician and patients to improve disease knowledge,
therapy, communication and disease copying. In another survey performed in the UK by Deane et
al. in 2014 on 600 PD patients, the large part was concerned about the neuropsychiatric burden of
the disease and symptoms like gait troubles and tremor. Questionnaires, rating scales and evaluating
tools (as performed at any technological level, i.e., digitally or paper and pencil) should provide
actionable information according to the “actionable information logistics”. This emerges from two
concepts: a) the actionable information and b) information logistics. Both, in clinical neurology,
cannot exist without a deep knowledge of the disease given by the study of the patient phenotype by
clinical epidemiological observations.
Actionable information means having the necessary information immediately available in order to
deal with the situation at hand. Information Logistics addresses the supply of information to patients
and clinicians. Its goal is the efficient delivery of information tailored to the patient and doctor’s
needs. Information logistics provides several concepts, methods, and technologies to optimize
content creation along the information value chain and delivery in accordance with user needs.
Information-on-demand services are typical features of information logistics, as they have to fulfill
user needs with respect to content, location, time and quality. Actionable information logistics
addresses patient-centered design of information logistics: the clinician and the patient actively
design, develops and monitors processes necessary for delivery and presentation of information
tailored to individual user needs.
Hence, to obtain actionable clinical information by mobile technologies and wearable devices such
as smartphones in PD, it is necessary to rely on the patient centered outcome (figure 17).
17Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. Figure 17. Examples of clinical actionable information. adapted by Ghoraani et al. 2021 Another clear example of this is the possibility of detecting a specific symptom (i.e. freezing of gait) with a sensor to allow an automated correction through a prompt delivered therapy as in the experiment of Zoetwei and colleagues (DeFOG trial; Zoetewei et al 2021, figure 17b) 18
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Figure 17b adapted by Zoetwei et al. 2021. The patient experiences the symptom and train the
algorithm to detect the incipient risk of freezing and to activate an auditory cue.
In the following chapters we will go through disease phenotyping focusing on some specific disease
aspects.
The first PD feature in our analysis will be the tremor. It is the most pictorial and famous PD
symptom. Its presence fosters the former PD definition as the “shaking palsy” together with
bradykinesia (the slowness and reduced amplitude of movement that was interpreted as a “palsy”).
It is more typical of an early disease stage but could present at any time and being even the most
bothersome aspect. The second aspect is dysphagia. It is one of the most dangerous PD
complications and, although it has been considered for a long time a hallmark of a late disease
stage, it could present since the diagnosis with all the implications that will be discussed later in the
text. The third and last point will be the gait. This will not be analyzed by an epidemiological point
of view but in the light of a remote patient monitoring analysis.
19Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. Tremor: a pictorial L-DOPA responsive cardinal motor symptom Tremor has been defined as a rhythmic and oscillatory involuntary movement with varied phenomenology, which can be classified based on several parameters, such as body parts, frequency and activation state (Louis, 2019). The latest consensus classification by the Movement Disorders Society (MDS) classifies tremor using a two-axis approach based on clinical features and etiology, which are then subclassified into multiple subcategories. Within the category of clinical feature axis and its subcategory of tremor characteristics, tremor is subclassified based on activation characteristics into rest tremor (RT) and action tremor (AT) [Bhatia et al., 2018]. The RT has been defined as a tremor in a body part that is not voluntarily activated, assessed when the patient is attempting to relax and is given adequate opportunity to relax the affected body part. Whereas the MDS classification of RT is a singular definition, AT is further subdivided into postural tremor, kinetic tremor and isometric tremor. AT has been defined as a tremor occurring in a body part while voluntarily maintaining a position against gravity (postural tremor), during any voluntary movement (kinetic tremor), or during muscle contraction against a rigid stationary object (isometric tremor) [Bhatia et al., 2018]. Although RT is one of the cardinal features of Parkinson’s Disease (PD), PD patients are also observed to have postural tremor, kinetic tremor or both [Pasquini et al., 2018; Luo et al., 2019]. In addition to being one of the most visual symptoms of PD, tremor is also ranked as one of the most troubling symptoms by PD patients [Heusinkveld et al., 2018]. Moreover, tremor impairs several physical and psychological quality of life domains in PD patients, like essential tremor patients as assessed with the Quality of Life in Essential Tremor (QUEST) questionnaire [Tröster et al., 2005]. Importantly, presence of tremor is also used to classify PD into tremor- dominant (TD), indeterminate (IND) and postural instability and gait difficulty (PIGD) subtypes [Stebbings et al., 2013], which have been linked with different rates of disease progression [Rajput et al., 2009]. Specifically, a total of 8 and 11 tremor items from Unified Parkinson Disease Rating Scale (UPDRS) or MDS-UPDRS scales are used to calculate tremor score, which is then used in 20
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
conjunction with the postural instability/gait difficulty (PIGD) score, for computing these subtypes
[Stebbings et al., 2013]. Despite such significance of tremor in PD, descriptions of prevalence of
basic tremor types (RT, postural tremor, kinetic tremor) and relationship of RT with AT in PD are
currently limited [Rajput et a., 1991; Pasquini et al., 2018; Hughes et al., 1993; Louis et al., 2001;
Gigante et al., 2015], as summarized in Table 2.
Table 2: Summary of previous studies reporting tremor prevalence
Table 2 legend: Not reported (NR), Unified Parkinson Disease Rating Scale (UPDRS), Washington
Heights-Inwood Genetic Study of ET (WHIGET), Parkinson's Disease Society Brain Bank (PDSB).
The study by Pasquini et. al. used the Parkinson Progression Marker Initiative (PPMI) data and also
reported on prevalence of difference tremor types at 2-years follow-up as following: any tremor
83.9%, rest tremor 67.9%, postural tremor 49.5%, and kinetic tremor 46.8%.
With the progression through disease stages, patients experience the appearance of axial symptoms
and levodopa unresponsive disturbances. This ranges from posture and postural reflex
abnormalities, freezing of gait, speech and swallowing disturbances.
The disease is not lethal itself, but some motor and non-motor features could trigger early stage
phenomena leading to the patient death - e.g. dysphagia & aspiration pneumonia, dysautonomia &
cardiac rhythm abnormalities & arrhythmia.
21Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. Dysphagia: a subtle L-DOPA non-responsive axial symptom Dysphagia – the dysfunction of the swallowing process – is one of the most feared complications in Parkinson's disease (PD) and a significant prognostic factor for poor outcomes [Fabbri et al., 2019]. Since its high prevalence during the course of PD (i.e., up to 80%) [Suttrup and Warnecke, 2016] dysphagia is assessed as part of the MDS Unified Parkinson's Disease Rating Scale (MDS- UPDRS). Known clinical predictors of dysphagia are Hoehn and Yahr stage > 3, disease duration, a relevant weight loss or a body mass index (BMI) < 20 kg/m2, the presence of drooling or sialorrhea and dementia [Suttrup and Warnecke, 2016; Troche et al., 2016]. Although dysphagia is mainly listed among late PD motor features, some data suggest that it may occur earlier and probably under-recognized and under-referred to swallowing specialists for a definite evaluation. Dysphagia has complex pathophysiology and data on its potential predictors in PD are limited, including the role of non-motor symptoms, such as sleep, and of dopamine replacement therapy [Suttrup and Warnecke, 2016]. At present, there is an unmet need for updated data on dysphagia occurrence and its risk factors in PD patients, despite clinicians' increasing awareness. Remote monitoring and the pandemic On March 9th, 2020, the Italian government imposed a national lockdown, due to Coronavirus disease 2019 (COVID-19) outbreak. Such restrictions also aimed to protect fragile people with chronic diseases, a population that is particularly at risk of SARS-CoV-2 complications. However, these patients often needed a tight follow-up and therapies to be tailored from time-to-time. In the last few years, mobile technologies have been extensively explored in patient management. However, this has not changed current clinical practices [Sim et al., 2019]. At the time of this study, despite a lot had been already done on wearables, the data available for remote patient monitoring (RPM) in a real-life cohort of PD patients were scarce, such as the application of data coming from 22
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
wearables on the clinical routine - the latter is basic need for the identification of a digital actionable
information. Hence studies on the feasibility of RPM with smartphone applications are necessary to
better understand the significance of patient ecological tracking on our daily life as PD healthcare
providers.
We will focus on the analysis of the gait and postural transition for several reasons. First, gait
impairment is a major determinant of PD patient quality of life; then, gait features are able to confer
to a patient a determinate phenotype class. Last, but not least, gait issues are intimately related to
the risk of falling - indeed falls are dramatic events in any patient life especially for subjects with
PD.
Falls are leading causes of morbidity and poor quality of life, particularly in Parkinson’s disease
(PD) [Fasano et al., 2017]. About 35–90% of PD patients experience a fall during the course of the
disease and 70% of them will fall again — constituting a milestone in disease progression [Fasano
et al., 2017; Van der Mark et al., 2014].
Different PD fall risk factors have been identified — such as inaccurate stepping or disease severity
[Zampogna et al., 2020]. Fall prevention is of the utmost importance and new technologies — as
wearable sensors — offer the chance to augment the ability to detect and track the fall risk [Fasano
et al., 2017; Zampogna et al., 2020]. The use of sensors has been applied mainly in controlled
laboratory settings, so far. Inertial sensors have been used in different neurological disorders to
objectively assess static and dynamic balance, but the large amount of data that they are able to
provide are not commonly applied in routine clinical practice [Zampogna et al., 2020].
Coronavirus disease-2019 (COVID-19) posed a great challenge on neurological patients [Fearon et
al., 2021] and the restrictive measures to limit the spread of the infection had the unexpected twist
of accelerating the use of digital health, remote patient monitoring strategies, teleneurology, and
even remote rehabilitation programs [Motolese et al., 2020; Isernia et al., 2021]. In this regard,
sensors had already been proved to be a robust tool in identifying the various kinematic risk factors
23Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. for falling [Zampogna et al., 2020]; therefore, wearables and sensors embedded in smartphones may be helpful to stratify the risk of falling of PD patients. Aims The present study is going to present some of the research activity conducted in the last 3 years by the movement disorder research team of Campus Bio-Medico of Rome aimed at disease phenotyping and remote patient monitoring. Those 2 activities are strictly connected between each other since the former is required to provide the correct data selection and interpretation that could be obtained by wearable patient monitoring. General methodology Epidemiological studies (study 1 and 2) are both retrospective longitudinal studies performed on large databases obtained by cooperative international studies which are further presented below. The PPMI, BioFIND and PDBP are multi-center, observational studies, designed to accelerate research in PD, especially biomarkers discovery, through collection of clinical, biospecimen and other relevant data, such as imaging, by making the data available to researchers in an open-access manner through their respective portals. The PPMI is an international, longitudinal study of early- stage PD patients (n = 423), recruited within 6 months from initial diagnosis and not on dopaminergic treatment, and healthy controls (n = 196). The BioFIND is a cross-sectional study of moderate to advanced stage PD patients (n = 118) on dopaminergic treatment and healthy controls (n = 88). The PDBP is a longitudinal study of primarily early to advanced stages PD patients (n = 882), with most patients on dopaminergic treatment and healthy controls (n = 549), in addition to patients with other related clinical diagnosis (n = 168, e.g., atypical parkinsonian disorder, essential tremor). A summary of relevant demographics and clinical features of these three cohorts is presented in Table 3 while more details have been described in the respective cohorts elsewhere [PPMI, 2011; Kang et al., 2016; Rosenthal et al., 2016]. 24
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Table 3: Summary of relevant demographics and clinical features of the PPMI, BioFIND and PDBP
cohorts.
Table 3 legend: Parkinson Progression Marker Initiative (PPMI), The Fox Investigation for New
Discovery of Biomarkers (BioFIND) and Parkinson's Disease Biomarkers Program (PDBP). * this
value was taken from original description of the PDBP cohort for 449 Parkinson’s disease subjects.
Study 3 is a prospective longitudinal study performed remotely on a sample of patients recruited at
the Movement disorders clinic of the Policlinico Campus Bio-Medico of Rome. This study has been
further implemented by a post hoc analysis focused on gait monitoring and falls. The last study,
study 4, has been developed following study 3 and is focused on the continuous remote movement
monitoring.
In all the presented studies, variables have been expressed as means and standard deviation (parametric
data), median (interquartile ranges, IQR) or and frequencies (%) (non-parametric data), and differences
across groups were tested with the student’s t or the Wilcoxon or the chi-squared test respectively. The
Kolmogorov-Smirnov test was adopted to investigate the data distribution. The association between
variables was investigated through univariate and multivariate logistic regressions, after controlling for
multicollinearity. Odds ratios (OR) were reported together with their 95% confidence intervals (95%
CI). A p < 0.05 was adopted for statistical significance. Statistical analysis was performed through the
JMP-14 software (SAS institute Inc.).
25Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. Clinical epidemiological studies The case of cardinal symptoms: tremor in Parkinson’s disease (Study 1 by Gupta and Marano et al., 2020) In this study, we specifically aimed to describe the prevalence of basic tremor types, and the relationship of RT with AT in three large cohorts of PD patients, including the Parkinson Progression Marker Initiative (PPMI) [PPMI, 2011], The Fox Investigation for New Discovery of Biomarkers (BioFIND) [Kang et al., 2016], and the Parkinson’s Disease Biomarkers Program (PDBP) [Rosenthal et al., 2016]. We chose to compare the PPMI, BioFIND and PDPB cohorts of PD patients for this study for the following reasons: large number of PD patients in each cohort; subjects recruited in each cohort by movement disorders specialists; data available on open-access basis; and, a wide range of severity of disease, ranging from drug-naïve PD patients in the PPMI cohort, moderately advanced PD patients on dopaminergic treatment (with MDS-UPDRS captured in on-state on baseline visit and off-state in follow-up visit) in the BioFIND cohort, and all stages of PD severity in cohort with majority being on dopaminergic treatment (with MDS-UPDRS irrespective of off-state or on-state) in the PDBP cohort. Baseline visit data of the PD patients (n = 423 for PPMI, n = 118 for BioFIND, n = 873 for PDBP) were accessed as of January 22, 2020 from the PPMI (https://www.ppmi-info.org) and Accelerating Medicine Partnership in Parkinson’s Disease (AMP PD) databases (https://amp-pd.org/). For the BioFIND cohort, the MDS-UPDRS part III data from baseline visit (on-state) were used by default for all calculations, while the follow-up visit data (off-state; 14 days after the baseline visit) were used for comparison separately. 26
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
The three basic tremor types, specifically, RT, postural tremor, and kinetic tremor were captured by
value of >= 1 on items 3.17 (rest tremor amplitude), 3.15 (postural tremor of the hands), and 3.16
(kinetic tremor of hands), respectively, from part III (motor) of the MDS-UPDRS in all three
cohorts. For the purpose of this study, we defined AT to include both postural and kinetic, rather
than postural or kinetic tremor, as former approach yields higher specificity and avoids false
positives, given that re-emergent rest tremor can be frequently mistaken as postural tremor [Dirkx et
al., 2016]. We also defined RT severity (range 0–80) by adding five sub-items of RT (3.17) and
then multiplying the sum with item 3.18 (constancy of rest tremor) (3.18) from part III (motor) of
the MDS-UPDRS. We also assessed the perception of tremor by patients using item 2.10 (Over the
past week, have you usually had shaking or tremor?) from part II of the MDS-UPDRS.
We first analyzed the average prevalence of RT (irrespective of postural or kinetic tremor), pure RT
(with neither postural tremor or kinetic tremor), AT (irrespective of RT), pure AT (with no RT),
postural tremor (irrespective of RT or kinetic tremor), pure postural tremor (with neither RT or
kinetic tremor), kinetic tremor (irrespective of RT or postural tremor), pure kinetic tremor (with
neither RT or postural tremor), no tremor (neither RT, postural tremor or kinetic tremor), any
tremor (any of three basic tremor types) and all tremor (all three basic tremor types), and
distribution of perception of tremor across baseline data of the three cohorts and in each individual
cohort. We then tested the hypothesis that prevalence RT and AT are not independent of each other,
such that the severity of RT would be higher in PD patients with AT versus without AT, in
individual cohorts. Finally, we also compared the prevalence of RT, AT, postural tremor, kinetic
tremor, any tremor and all tremor in off-state and on-state in the BioFIND cohort.
The average prevalence of RT and pure RT was 58.2% and 14.5 %, respectively. In contrast, the
average prevalence of AT and pure AT were 36.6% and 9.6%, respectively. The average prevalence
of postural tremor and pure postural tremor was 49.7% and 4.0 %, respectively. The average
prevalence of kinetic tremor and pure kinetic tremor was 52.3% and 8.1 %, respectively. The
27Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. average proportions of patients with no tremor, any tremor and all tremors were 19.9%, 79.9%, and 26.9%, respectively. Figure 18 provides a summary of these results using a diagram. Figure 18: Average prevalence of different tremor types and their combinations across baseline data of the PPMI, BioFIND and PDBP cohorts. Figure 1 legend. Parkinson Progression Marker Initiative (PPMI), The Fox Investigation for New Discovery of Biomarkers (BioFIND) and Parkinson's Disease Biomarkers Program (PDBP). Size of the circles are not indicative of the prevalence magnitude. Table 4 summarizes these results in each individual cohort. 28
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Table 4: Distribution of prevalence of different types and combinations of tremor in baseline data of
each of three cohorts.
Table 4 legend: Parkinson Progression Marker Initiative (PPMI), Fox Investigation for New
Discovery of Biomarkers (BioFIND), Parkinson's Disease Biomarkers Program (PDBP).
As for average perception of tremor by the patient over the past week, 19.5% of the patients
reported having no tremor, while 52.8%, 21.4%, 5.3% and 1.0%, reported having slight, mild,
moderate and severe tremor, respectively. Table 4 summarizes these results in each individual
cohort.
Table 5: Distribution of perception of tremor in each of three cohorts.
29Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. Table 5 legend: Movement Disorders Society Unified Parkinson’s Disease Rating Scale (MDS- UPDRS) item 2.10. Conversely, on average 79.5% patients reported having any shaking or tremor (subtle, mild, moderate or severe) over the past week. We also found that patients with RT versus without RT consistently had a significantly higher (Chi- square test) proportion of AT in the PPMI (40.0% versus 30.1%, OR 1.55, CI 1.00–2.40, p = 0.049), in the baseline visit of the BioFIND study (48.0% versus 40.0%, OR 3.04, CI 1.31–7.05, p = 0.008,) and PDBP (49.9% versus 21.0%, OR 3.75, CI 2.78–5.06, p = 0.000) cohorts, respectively. In multivariate logistic regression analysis adjusting for age, gender, and disease duration (not included for the PDBP cohort), the presence of RT was consistently associated with higher odds (p < 0.05) of having AT in the baseline data of the PPMI, BioFIND and PDBP cohorts (supplementary table 1). Male gender was also associated with higher odds of AT in the PPMI and PDBP cohort, but not in the BioFIND cohort (table 6). Table 6. Multivariate logistic regression analysis of prevalence of action tremor and rest tremor, adjusting for age, gender, disease duration. Data are reported as OR (95% CI); *p
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Variable Baseline PPMI Baseline BioFIND Baseline PDBP data
data data
Rest tremor 1.72 (1.09 – 2.73)* 3.15 (1.30 – 7.62)* 3.77 (2.79 –
5.10)***
Male gender 1.69 (1.09 – 2.61)* 1.87 (0.80 – 4.36) 1.87 (1.05 – 1.94)*
Disease duration 1.00 (0.97 – 1.02) 0.99 (0.98 – 1.00) NA
(months)
Age 0.98 (0.96 – 1.00) 0.94 (0.88 – 1.01) 1.01 (0.99 – 1.03)
Based on these observations, we postulated that PD patients might develop AT after RT becomes
severe, or conversely, PD patients with AT would have higher severity of RT compared to patients
without AT. In support of this hypothesis, we found that the severity of RT was significantly higher
(Student’s t-test) in patients with AT than patients without AT in the PPMI (5.7 ± 5.4 versus 3.9 ±
3.3, p = 0.000), BioFIND (6.4 ± 6.3versus 3.8 ± 4.4, p = 0.000) and PDBP (6.4 ± 6.6 versus 3.7 ±
4.4, p = 0.000) cohorts, respectively.
In the BioFIND cohort (in which patients were examined in on-state on baseline visit and off-state
in second visit), we found that the prevalence of RT, AT, postural tremor, kinetic tremor, and
proportion of patients with any tremor and all tremor were significantly (p < 0.05, Chi-square test)
higher in off-state in follow-up visit, compared to on-state in the baseline visit (Figure 19).
31Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. Figure 19: Changes in different tremor types and their combinations from off-state to on-state in the BioFIND cohort. Figure 19 legend. Fox Investigation for New Discovery of Biomarkers (BioFIND). On-state data were obtained from the baseline visit; off-state data were obtained by the follow-up visit (14 days after the baseline). *p
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
BioFIND and PDBP cohorts, although RT has the highest prevalence (58.2%) in PD, AT can also
be present in a sizable number (36.2%) of PD patients, which is in line with similar literature [Louis
et al., 2001; Gigante et al., 2015; Louis et al., 2003]. In comparison, a large majority (79.5%) of the
patients self-reported having tremor. Our study results also indicate all tremor types are reduced by
dopaminergic treatment, which is consistent with the traditionally held view on the influence of
levodopa and dopamine agonist on tremor in PD [Tedeschi et al., 1990; Elble et al., 2002].
We also found that the PD patients with RT had significantly higher prevalence of AT in all three
cohorts. Moreover, we found that the patients with AT, compared to patients without AT, had more
severe RT in all three cohorts, similar to findings reported in previous studies [Louis et al., 2001;
Gigante et al., 2015]. These findings together demonstrate that AT could be a part of broader tremor
syndrome of PD. Furthermore, these findings are supported by functional neuroimaging and
electrophysiology studies demonstrating cross-interactions between basal ganglia and
cerebellothalamic circuitry in mediating tremor in PD [Dirkx et al., 2016; Muthuraman et al., 2018].
The presence of re-emergent RT or a comorbid alternative tremor disorder (such as essential
tremor) could, at least in part, explain these findings. It is worth noting that MDS-UPDRS scale
does not distinguish between postural tremor and re-emergent rest tremor mimicking postural
tremor, and such distinction can only definitely be made with electrophysiological analysis [Dirkx
et al., 2016].
One of the limitations of our study was that the data used for defining prevalence of different types
of tremors were collected by multiple investigators in the PPMI, BioFIND and PDBP cohorts.
However, these data are considered valid as the clinical examination for recording presence of
tremor were done as part of the standardized MDS-UPDRS by trained movement disorders
specialists in all three of these studies conducted at internationally recognized movement disorders
centers. Another limitation was that we could not include isometric tremor in defining AT, which
was unavoidable since the MDS-UPDRS scale does not capture isometric tremor. It is also worth
noting that MDS-UPDRS does not capture postural and kinetic tremor in lower limbs or head,
33Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano, discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022. La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca, a condizione che ne venga citata la fonte. unlike RT, which is captured in upper limbs, lower limbs and lip/jaw. Another key limitation of average prevalence reported across the three cohort was that patients in these different cohorts had wide ranges of disease duration and dopaminergic medications status. Specifically, the patients in PPMI study were early disease and drug naïve, compared to BioFiND, where patients were moderate to advanced stage and all on dopaminergic medications, and PDBP, where patients had intermediate disease duration and nearly 90% were on medications. To partially address this limitation, we have reported respective prevalence in individual cohorts, and reported changes in prevalence of tremor from off-state and on-state state in the BioFIND cohort. The presence of RT is not mandatory for a diagnosis of PD, which is supported by our data demonstrating absence of any tremor and presence of pure AT in nearly one-fifth and one-tenth of all patients across the PPMI, BioFIND and PPMI cohorts. These observations have implications in clinical practice and research enrollment, where the presence of patients either without tremor or with multiple tremor subtypes potentially lead to diagnostic delay, ambiguity and uncertainty. For example, different patterns of basic tremor types have been shown to improve differential diagnosis of PD from essential tremor. All together, these results provide further evidence that PD tremor is highly heterogeneous and its correct phenotypic classification in PD will be essential in optimizing diagnostic, therapeutic and prognostic approaches. The case of axial symptoms: dysphagia (study 2, by Marano et al., 2020) Parkinson progression markers initiative (PPMI) is an international multi-center and longitudinal observational study of PD patients diagnosed within 2 years before the enrollment, who are not taking PD medication at study entry, followed on a yearly basis [PPMI, 2011]. Here, we aimed to investigate the prevalence of swallowing impairment and find potential predictors in early PD patients, exploring the Parkinson's disease progression markers initiative (PPMI) database. 34
Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
We stratified PD patients (n = 422) and healthy controls (HC, n = 194) using the MDS-UPDRS part
II item 2.3 (“chewing and swallowing problems” in the past week) and the Scales for outcomes in
Parkinson's disease – autonomic (SCOPA-AUT) question 1 (“difficulty swallowing or choking” in
the past month). Subjects who scored at least 1 point at both scales were classified as reporting
swallowing dys- function (dysphagia, PD-Dy or HC-Dy). Scales description and case distributions
are reported in Tables 7 and 8.
Table 7. MDS-UPDRS II, Item 2.3 and SCOPA-AUT question 1 descriptions and grouping.
MDS-UPDRS II, Description SCOPA-AUT, Description Group
Item 2.3 – question 1 (“In the
“chewing and past month, have you
swallowing” had difficulty
swallowing or have
you choked?”)
0 (Normal) “no problems” 0 “Never” PD-
NDy
1 (Slight) “I am aware of slowness in 1 “Sometimes” PD-
my chewing or increased Dy
effort at swallowing, but I
do not choke or need to
have my food specially
prepared”
2 (Mild) “I need to have my pills cut 2 “Regularly”
or my food specially
prepared because of
chewing or swallowing
problems, but I have not
choked over the past week”
3 (Moderate) “I choked at least once in 3 “Often”
the past week”
4 (Severe) “Because of chewing and - -
swallowing problems, I
need a feeding tube”
35Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
Table 8. Distribution of MDS-UPDRS item 2.3 and SCOPA-AUT question 1 scores across groups.
Data are reported as raw number (%).
PD-Dy PD-NDy p-
(n=44) (n=378) value
MDS-UPDRS II, item 0 (normal) 0 367 (97)Tesi di dottorato in Scienze biomediche integrate e bioetica, di Massimo Marano,
discussa presso l’Università Campus Bio-Medico di Roma in data 15/06/2022.
La disseminazione e la riproduzione di questo documento sono consentite per scopi di didattica e ricerca,
a condizione che ne venga citata la fonte.
part I non-motor symptom burden, MDS- UPDRS part I item 1.7 nighttime sleep disturbances,
MDS-UPDRS part III motor score, Montreal cognitive assessment scores or MoCA, PPMI
psychometric battery, Geriatric depression scale score or GDS, Epworth Sleepiness Scale or ESS
score, REM sleep behavior Disorder Questionnaire score or RBDQ and Unified Pennsylvania Smell
Identification Test score or UPSIT, and nuclear imaging or [123I]FP-CIT uptake.
Groups were also compared for the presence of “depression” based on Geriatric depression scale
(GDS) score of ≥6, “moderate to severe insomnia” based on MDS UPDRS item 1.7 “sleep
problems” ≥ 3, “excessive daytime sleepiness” (EDS) based on ESS score ≥ 9 [Johns, 1991] and
“possible RBD” to patients with RBDQ ≥6 [Stiasny-Kolster et al., 2015]. After excluding baseline
PD-Dy patients, we calculated the incidence and prevalence of dysphagia during the three years of
follow-up and, in order to identify possible baseline predictors, we arbitrarily chose the
development of dysphagia at year 3 as the main outcome of the analysis. Also, the subsequent use
of dopamine replacement therapy at year 1 (DRT, a major confounding factor) was included in the
analysis. Data used in the preparation of this article were obtained from the Parkinson's Progression
Markers Initiative (PPMI) database (www.ppmi-info.org/ data). For up-to-date information on the
study, visit www.ppmi-info. org.
The baseline prevalence of dysphagia was 10.4% (44 out of 422) in PD patients, compared to 0.5%
(1 out of 194) in HC subjects (p < .01). Dysphagia presented an incidence of 12.8% at year 1
(prevalence 16.9%), 9.9% at year 2 (prevalence 17.6%), 6.4% at year 3 (prevalence 19.1%) in PD.
The comparison between PD-Dy and PD-NDy at baseline showed significant differences in BMI,
MDS-UPDRS I, GDS, RBDQ, ESS and [123I]FP-CIT uptake in caudate (Table 9).
37You can also read