Undetected sight loss in care homes: an evidence review - Jessica Watson and Sally-Marie Bamford International Longevity Centre - UK
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Undetected sight loss in
care homes:
an evidence review
Jessica Watson and Sally-Marie Bamford
International Longevity Centre - UK
July 2012
www.ilcuk.org.ukThe International Longevity Centre - UK (ILC-UK) is an independent, non-partisan think-tank dedicated to addressing issues of longevity, ageing and population change. It develops ideas, undertakes research and creates a forum for debate. The ILC-UK is a registered charity (no. 1080496) incorporated with limited liability in England and Wales (company no. 3798902). ILC–UK 11 Tufton Street London SW1P 3QB Tel: +44 (0) 20 7340 0440 www.ilcuk.org.uk This report was first published in July 2012 © ILC-UK 2012 Acknowledgements The authors would like to thank Thomas Pocklington Trust and particularly Sarah Buchanan for supporting this work. Thanks also go to all the contributors: in interview, at the focus group and in informal discussions (the full list is included in the Annex). It should be noted that all opinions expressed in this review are the authors’ and should not be considered representative of the contributors. Thanks to David Sinclair and Lyndsey Mitchell at ILC-UK for their assistance with the production of this review. ILC-UK would welcome any feedback on this publication. Please send your comments to Jessica Watson (jessicawatson@ilcuk.org.uk).
Table of Contents Executive Summary .................................................................................. 4 Introduction................................................................................................ 6 Background................................................................................................ 8 Legislation and regulation ...................................................................... 14 Issues and barriers ................................................................................. 19 Potential solutions .................................................................................. 25 Recommendations .................................................................................. 29 References ............................................................................................... 30 Annex........................................................................................................ 35
Executive Summary
Overview
This evidence review provides an overview of sight testing and sight loss in residential care
homes, including the legislative and regulatory context framing this issue. This review was
informed by desk research, informal stakeholder interviews and an expert stakeholder meeting to
discuss the potential solutions and recommendations.
Context
As we age, our eyesight naturally deteriorates. Of people aged 75 and over, one in five are living
with sight loss, and in the population aged over 90 this climbs to one in two. This is a problem that
will continue to increase as the population ages. Care home residents suffer from unusually high
rates of poor eyesight, with the RNIB estimating that as many as over half of older residents in
care homes have some form of sight loss. Furthermore it is argued up to 70% of sight loss may be
avoidable, with the chances of reduction significantly improved by early detection.
Poor eyesight can have significant repercussions for health and quality of life for residents, a
knock-on effect for other aspects of health and quality of life. As well as potential complications
from the eye condition itself, it can increase the risk of falls and contribute to depression and
isolation. There are significant associated costs with these health problems: for example, falls
directly relating to sight loss in the UK are estimated to cost £128m a year in medical costs alone.
Key issues and barriers
• Lack of awareness of sight loss and visual impairment, associated health problems and
symptoms at all levels, particularly residents, their families and care home staff and managers.
• Similarly, across these groups there is a lack of priority given to eye health, commonly seen
as an optional extra rather than an integral element of good health. This is particularly the case
for residents who have dementia. There is not enough connection with good eye health as a
contributing factor to a lower rate of falls, depression and isolation; and better quality of life.
• Eye health overlooked as a health indicator in assessment and checks of care home
residents; both internally as part of general health checks and externally through health
professional consultations and CQC assessments. While eye health is referenced in general
health outcomes, as a ‘silent’ health problem it is often missed off checks in practice.
• Reflecting the lack of explicit inclusion of eye health indicators, there is a limit on the time and
organisational practices for informal sight checking or assessing potential symptoms by
case home staff, exacerbated by low awareness of the issue.
• Training sessions and materials for care home staff on eye health and sight loss is available,
but there are limits in delivery of training owing to restricted time, staff turnover and other
practical barriers, such as shift working patterns.
4Recommendations
1. Create a national awareness campaign on the issue of sight loss in older people with
different cross-sections of stakeholders. Awareness of this issue should be increased through
education and guidance related to personal experiences for residents and their families, as well as
other health professionals such as GPs, nurses and occupational therapists working with the
residents
2. The Care Quality Commission should incorporate eye health indicators into their
assessment criteria for care homes and across the general health system. Priority given to
eye health by care inspectors will support additional time spent on this issue by care staff as well
as ensuring high quality standards.
3. Care home providers should be encouraged to add eye health and sight loss testing to
their key performance indicators.
4. Further research should be conducted to explore the impact of the General Ophthalmic
Services contract restrictions on domiciliary sight testing, specifically the need to pre-
notify appointments with individual patients and to examine the case for the contract to be
altered. Relaxation of restrictions on eye health professionals could enable ease in referring
residents for sight tests.
5. More qualitative research is required within care homes to ensure barriers to good eye
health practices for care home workers, managers and providers are understood. Once
barriers to good practice are identified, appropriate intervention and tailoring of existing
resources should be pursued. Training sessions for care home staff are considered to have
been very effective in improving awareness of eye health, but the coverage of these is patchy and
generally provided by the private or voluntary sector. More could be done through further
education of the staff and managers of the homes, but understanding the barriers to accessing this
information is crucial to its development.
5Introduction
This evidence review aims to give an overview of sight testing and sight loss in residential care
homes, including the legislative and regulatory context framing this issue. This review was
informed by desk research, informal stakeholder interviews and an expert stakeholder meeting to
discuss the potential solutions and recommendations. It covers the issues currently experienced
by residents of care homes with regard to sight testing and demonstrates the gaps in the formal
requirements of care homes and suggests areas where improvements can be made. In particular it
examines the current practices of informal vision checking and formal sight testing within the care
home, barriers in achieving effective and inclusive sight testing for care home residents, and
solutions to overcome these difficulties.
This review covers:
• the background to this issue
• the legislation and regulation related to sight testing in care homes
• the shortfalls of the legislative and regulatory framework
• the issues and barriers that occur in practice for involved parties
• potential solutions to these issues for respective involved parties
• recommendations for all parties to carry out these solutions, developed with expert
stakeholders in this field
This report aims to frame the context of issues relating to undetected visual impairment and sight
loss specifically for older people living in residential care homes, while acknowledging that there
are also other groups for whom this problem demands further attention. It should be noted that the
issues and barriers highlighted in this report are not exclusive to visual impairment and eye health.
For example, people experiencing hearing loss living in residential care homes may encounter
many of the same barriers to effective diagnosis and treatment of their sensory impairment. People
with learning disabilities (of whom around one in ten has some form of visual impairment (RNIB
website - Visual Impairment Learning Disability service)) also share many of the issues raised, with
some, such as communication difficulties, being particularly common for this group. Similarly, older
people living and being cared for in the community may receive worse eye care than those living in
a residential home, furthermore we also acknowledge the need for greater understanding into how
best to resolve the issue of poor eye health for people still living in their own homes.
Definitions and parameters
This review focuses exclusively on the issues facing older people living in residential care homes
(those providing personal or nursing care, see below), and not those still living at home and being
cared for in the community. This review concentrates on the situation in England, owing to the
differences in legislation and regulation compared to the rest of the UK. However, this review does
make reference to select examples of practice elsewhere in the UK.
This review takes a broad approach to eye health, for example, including eye conditions related to
forms of dementia and stroke. There is also a distinction to be drawn between sight testing, as
6formally conducted by an eye health practitioner, and sight checking as a process that can be
conducted by those with a lay understanding of sight loss and eye health (for example, simple
checks of the vision field by care home workers).
There are three different professions that operate under the umbrella term of ‘opticians’:
• optometrists, qualified to test sight, prescribe and dispense spectacles and other optical
appliances, and can detect signs of eye disease or abnormalities;
• ophthalmic medical practitioners (OMPs), qualified doctors with a specialism in eyes and eye
care, can detect and treat eye abnormalities and diseases and can also test sight and prescribe
like optometrists;
• dispensing opticians, who are not qualified to test sight or prescribe but are able to dispense
and fit spectacles and other optical appliances.
(Guidance and Audit Implementations Network, 2010).
Most commonly it is optometrists who conduct sight tests in care homes, but in order to avoid
confusion this report refers to ‘eye health professionals’ to cover all practitioners that conduct
testing and dispensing in care homes.
7Background
Demographic change
The UK population is ageing, with the numbers of people aged over 65 increasing by 1.7 million
from 1984 to 2009, and a projected 23% of the population will be aged over 65 by the year 2034
(ONS, 2011). This increase is particularly apparent in the oldest old, with the number of people
aged over 85 projected to be 5% of the population by 2035, 2.5 times the size of this group in 2010
(see Figure 1).
Figure 1: Population by age, UK, 1985, 2010 and 2035
Source: ONS, 2010a
As of September 2011 life expectancy at birth in the UK had reached its highest level on record, at
82.1 years for females and 78.1 years for males (ONS, 2011). However, healthy life expectancy
(the period of life that is free from poor health or a limiting illness or disability) is considerably
lower, at 70.5 years for females and 68.5 years for males (ONS, 2010). As the older population
lives longer, the UK will see a corresponding rise in the number of people living with chronic
diseases in long term poor health, as these diseases primarily affect older people (for example,
cardiovascular disease).
Age and eye health
There are an estimated two million people affected by sight loss in the UK, of which the vast
majority are older people (above working age) (Bosanquet and Mehta, 2008). Of people aged 75
and over, one in five are living with sight loss, and in the population aged over 90 this increases to
one in two (RNIB website). Age is a common driver for all forms of sight loss in the UK
(Bosanquet, 2010), with incidence of all kinds of conditions affecting sight increasing as we get
older, alongside normal changes in vision such as a need for increased light (Alzheimer’s Society,
2011; Percival, 2007). A review of studies examining sight problems in the older population found
8suggested rates of preventable sight loss (caused by cataracts or refractive error) in people aged
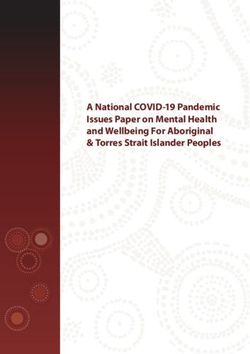
over 65 as high as 50-70% (Tate et al, 2006). Another study conducted by Evans and colleagues
(2004) examined the causes of sight loss in a sample group aged over 75. Of those suffering from
minor (defined as 6/18 on the Snellen scale1) sight loss (26% of a sample of 1742), refractive error
was the main cause of their poor sight. The causes of more severe sight loss were available for
76% of the remaining group, the breakdown of which is detailed in Figure 2.
Figure 2: Causes of severe visual impairment in sample group aged over 75
Adapted from Evans et al (2004)
Common causes of sight loss in older people
Refractive error describes both long and short sightedness. It causes blurring of vision and can
be corrected with glasses or contact lenses. Despite being one of the eye problems easiest to
remedy, it is often overlooked as a cause of sight loss (Bosanquet, 2010).
Age-related macular degeneration (AMD) affects central vision and the ability to see fine detail.
There are two main types; wet (10-15% of all AMD cases) and dry, which is more common. Wet
AMD is more treatable, but requires early intervention in order to be effective. There is no
treatment for dry AMD (RNIB Eye Conditions website).
Cataract is the clouding of the lens. Alongside the effects of normal ageing of the eye, common
causes of cataract include diabetes, a trauma and some medications or surgery for other eye
problems (RNIB Eye Conditions website). Cataracts develop quite slowly, but are usually easily
treatable with a minor operation.
Glaucoma is the name given to a group of eye conditions that affect the optic nerve. It can be
caused by raised eye pressure or by weakness in the optic nerve. There are a number of different
types which present with different symptoms, all of which are treatable. Some kinds of glaucoma
do not have obvious symptoms for a long period, but still cause damage to vision (RNIB Eye
Conditions website).
1
The Snellen scale is used to measure visual acuity (clearness of vision). It is measured using a Snellen test, which consists of rows of letters
decreasing in size that are read from a certain distance away. The first number refers to the distance in metres at which the chart is read, and the
second number refers to the size of letters that can be read without assistance. Normal visual acuity is 6/6.
9Diabetic eye disease can take a number of forms, the most serious of which is diabetic
retinopathy, a condition affecting the blood vessels in the retina, which affects 40% of people with
type 1 diabetes and 20% of those with type 2 diabetes (RNIB Eye Conditions website). Rates of
diabetic retinopathy in the over 65s have doubled since 1990-91 (Bunce and Wormald, 2006).
While screening for diabetic retinopathy is at a very high standard in the UK, a key issue in this
area is the high number of undiagnosed people living with diabetes (up to half a million: Diabetes
UK, 2010) who will be unable to access this screening programme (and other health support).
Sight loss can also occur after a stroke, particularly one affecting the right side of the brain (RNIB
Eye Conditions website). The issues potentially arising from vision loss after a stroke are varied,
including visual field loss and eye muscle problems, making it difficult to focus. Some of these
issues may improve over time and others may be permanent.
Different forms of dementia can also affect sight independent of other sight conditions. The
problems it can cause are varied and range from impairments in visual contrast sensitivity, depth
perception, motion perception and colour discrimination (Kéri et al, 1999). Difficulties in
visuoperception have been reported for Alzheimer’s disease, dementia related to Parkinson’s
disease, Lewy body dementia and vascular dementia (if damage is on or near the visual pathway)
(Alzheimer’s Society, 2011).
Of these eye conditions, AMD and glaucoma have both increased since 1990-91 and diabetic
retinopathy has doubled (Bunce and Wormald, 2006). Rising levels of diabetes and stroke related
to unhealthy lifestyles (NHS Information Centre, 2010) may have a future influence on the burden
of poor eye health. Two thirds of the sight loss in older people is caused by refractive error and
cataracts, both of which can be diagnosed through a sight test and are for the most part easily
corrected or treated with glasses or surgery (RNIB website). There are also some treatment
options for the other major eye health problems, particularly with early intervention, so it is vital that
older people avoid long periods without sight testing to aid the potential for prevention.
Care homes
The landscape of residential care (in an institution as opposed to care provided at home) in the UK
is one of variety, with a mix of state, private and voluntary sector homes that provide different
levels of care. The term ‘care home’ covers two distinct levels of care provided in residential
homes; personal care and nursing care. Personal care covers assistance with tasks such as
washing, eating and dressing residents, whereas care homes that provide nursing care are
designed for people who are frailer and have greater health needs, be they mental or physical
(First Stop Care Advice website). Homes providing nursing care will have a registered nurse on
duty all the time. There are also other residential arrangements in place for older people, such as
retirement villages and sheltered housing, but the care offered by such schemes is not at the same
level as is currently provided in care homes. A crucial difference between care homes and others
types of residential settings for older people is the transfer of responsibility for health to the care
home staff. The vast majority of homes offering residential care are run by private companies or
voluntary organisations, with only 11% under the control of local authorities (CQC, 2011, p. 30).
As the numbers of older people rise, so will the number of people in need of care. Currently there
are around 400,000 older people living in care homes across the UK, of which 376,250 are in
10England (across 10,331 care homes) (British Geriatrics Society, 2011). Projections for the future
need for 24-hour care for people aged 80 years or over in England and Wales suggest increases
of 82% from 2010 to 2030 with a demand for 630,000 care-home places by 2030 (Jagger et al,
2011).
Dementia
Population ageing in the UK will herald an increase in the number of people with dementia.
Dementia directly affects over 750,000 people in the UK and it is estimated that this number will
increase to over one million by 2025 (Alzheimer’s Society, 2007). This number may in fact
represent an underestimate, given that diagnosis rates are lower in the UK than in many other
European countries. Diagnosis levels in the UK are estimated at almost 40 per cent, although the
number masks significant regional variations (Alzheimer’s Society, 2011).
Dementia represents a huge challenge not only for individuals and families, but also for our health
and social care system and its workforce. More than one-third of people with dementia live in care
homes and dementia is the strongest determinant for entry into residential care for people over 65.
At least two-thirds of all people living in care homes have a form of dementia (Alzheimer’s Society,
2007). Care homes are now ‘front-line’ dementia providers, particularly during the severe stages of
the disease. People with dementia who live in care homes have among the most complex health
and social care needs of any group in UK society (Heath and Sturdy, 2009). A report from the
Alzheimer’s Society in 2007, entitled Home from Home, highlighted that while some care homes
are providing good-quality care to people living with dementia, many homes are still not providing
the level of person-centred care people with dementia deserve.
With regards to sight loss, dementia poses some very specific and significant challenges for all
actors in the care home environment. The majority of people living with dementia in the UK are
aged over 65, and of these 1 in 7 is living with significant sight loss. In the general population, after
age 75 the chance of a person having both sight loss and dementia is 2.5% (Dementia and Sight
loss Interest Group). Different forms of dementia can also affect sight not limited to loss of visual
field and/ or acuity, but also linked to difficulties in carrying out practical activities (Alzheimer’s
Society, 2011). The National Institute for Health and Clinical Excellence (NICE) has published
guidance providing details of the recommendations and advice for treating patients with dementia.
While the guidance includes aims to promote and maintain the independence of people with
dementia, including environmental modifications, maintaining good vision is not included (NICE,
2006).
Alzheimer’s disease and other forms of dementia affect an individual’s ability to communicate and
particularly in the middle to late stages of the disease they may not be cognisant of their own
health or social care needs. Therefore, for those with dementia, recognising or even expressing
concern about their own respective eye health will be extremely difficult. This in turn represents a
challenge to care home workers and managers, as they may not receive the same verbal or
physical cues of sight loss compared to other residents without dementia. Some research has
highlighted that a diagnosis of dementia can lead to a perception of a resident being ‘difficult’
rather than an awareness that they are displaying sight loss symptoms (Oddy, 2003). This
11situation is further hampered by low levels of awareness and understanding of how to respond to
residents with dementia and their specific health and social care needs.
Eye health of care home residents
People who live in residential care have historically been an under-researched group.
Compounded by the ‘silent’ nature of undetected sight loss and visual impairment, it is extremely
difficult to identify an exact number of just how many care home residents are affected by this
issue. While there has not been specific research conducted into the total numbers of people living
in care homes with undetected sight loss, the documented high risk levels for older people suggest
that the number who are could conceivably be very high. The RNIB estimate that as many as over
half of older residents in care homes have some form of sight loss (RNIB, 2010). Additionally,
existing research examining sight loss among adults who are cared for has found that people living
in care homes are up to five times more likely to experience sight loss than someone cared for at
home (Mitchell et al, 1997). Turpin (2011) suggests three possibilities for these high levels of visual
problems in care homes; a higher likelihood of visually impaired people to be admitted to care
homes (although co-morbidity issues may be a stronger contributing factor, see Evans, 2008);
difficulty in accessing eye care services; and that care home residents’ co-morbidities mean that
eye care interventions are overlooked or thought unnecessary.
Other data can inform this picture; for example, out of 1.75 million people who could benefit from a
domiciliary sight test provided at no cost to them by the NHS, only 418,000 tests (UK total;
346,500 in England) were performed in 2008/9 (these figures include people who are cared for in
the community as well as those in residential care homes) (FODO, 2010). The review of UK sight
loss prevalence conducted by Tate and colleagues (2006), which suggested rates of undetected
sight loss of up to 70%, found that few studies included care home residents; though taking into
account high risk factors, the problem is likely to be far greater in this group. There is potentially a
very high number of people living in care homes with varying stages of deteriorating sight, without
the knowledge of or ability to raise this issue with care home workers, who are equally unaware of
this problem.2
Evidence supporting intervention
Sight loss comes with an enormous financial cost. The cost to society of people who are blind or
have sight loss has been estimated to between £4.1 billion and £8.8 billion a year (including
people who have sight loss but do not report it) (Ethical Strategies, 2003). The RNIB has estimated
that half of this cost is avoidable through increasing regular sight tests and early detection,
projecting savings of £2 - £4.1billion annually through these measures (Bosanquet, 2010). In
response to this issue, the UK Vision Strategy has a strategy outcome entirely dedicated to
“Eliminating avoidable sight loss and delivering excellent support for people with sight loss” (UK
Vision Strategy, 2008). A report by Access Economics (2009) commissioned by the RNIB ran a
cost benefit analysis of various areas for improvement in eye care. Running a campaign
encouraging people aged over 60 to have regular sight tests has a potential cost effectiveness
ratio of £24,200 per Disability Adjusted Life Year (in comparison to not running the campaign).
2
It should be noted that there are many examples of excellent practice of sight testing in care homes. This report does not aim to reduce the
laudable outcomes of these examples, but to highlight the importance of this practice being repeated across the country.
12A lack of detection of sight loss can also lead to a higher level of falls. The rate of falls for older
people with sight loss is 1.7 times that of people without eye problems (Legood et al, 2002). A joint
policy statement from the British Geriatrics Society and the College of Optometrists (2010) calls
attention to the impact of falls and their associated pathologies, and the related benefits of
improving vision for people at a higher risk of falling, of which care home residents are a key
group. With one in three over 65s falling every year, falls are the most frequent and serious
accident affecting this group (Age UK website, 2010). Over a 12-month period the medical cost of
falls among people with sight loss is estimated at £269 million, and falls that are directly related to
having sight loss at £128 million (Scuffham et al, 2002).
In addition to the physical health benefits of maintaining good eye health, there are also mental
health benefits of preventing sight loss. The relative risk of depression is 3.5 times higher in people
who experience sight loss, compared to those who do not (Access Economics for RNIB, 2009).
The prevalence of depression in people in residential care is thought to be around 40%, and rates
of depression are generally higher for older rather than younger people (10-15% for over 65s
compared to 9% in younger age groups) (SCIE website). Furthermore it has been argued sight
loss has been found to be a key contributory factor to suicide in older people (RNIB Cymru, 2011).
Improving sight can also improve personal and social factors for older people, leading to an
increased quality of life, enabling them to be more active and engaged. Research conducted by
the Alzheimer’s Society demonstrated that ‘the availability of activities and opportunities for
occupation is a major determinant of quality of life’, and not having enough to do was a major issue
for care home residents (Healthcare at Home, 2011). Some studies have suggested that the
percentage of time spent on ‘constructive activity’ in care homes could be as low as 3% (Ballard et
al, 2001). Cook et al (2005) also found that despite being in a larger community than an older
person living alone at home, sight loss can still cause feelings of isolation for people living in
residential care.
The implications of improving vision in care homes are not limited to improving the quality of life
and potential health of the residents. Additionally, an awareness and correction of sight problems,
such as glasses or improving contrast and lighting, can cut down the time needed for staff to carry
out tasks such as hand-feeding residents and could also reduce or help minimise the risk of certain
forms of challenging behaviour.
13Legislation and Regulation
Sight testing in England
Sight testing in England and Wales is carried out under the General Ophthalmic Services contract
(GOS), which describes the relationship between the NHS and eye professionals and the required
actions of the eye professionals in testing sight and prescribing further correction or treatment.
Under the GOS, sight tests are carried out in order to both check the health and functioning of the
eye, and to provide prescriptions for glasses or contact lenses if necessary (General Ophthalmic
Services Contract Regulations, 2008). Under the Health and Social Care Act (2012) primary eye
health services including budgets for GOS sight test are to be managed by the NHS
Commissioning Board, previously managed by Primary Care Trusts.
Certain members of the population are entitled to free eye tests, paid for by the NHS. This
includes, but is not limited to: people over the age of 60, people with glaucoma and diabetes (or
are aged 40+ with an immediate relative with glaucoma or have been advised by an
ophthalmologist of being at risk of glaucoma), people who are below a certain threshold to qualify
for subsidised tests based on socio-economic status (NHS choices website). This last group may
also qualify for vouchers towards the cost of glasses. Free eye tests are conducted by eye health
professionals who claim back the NHS charge from the GOS budget. However, the GOS
payments are restricted to sight tests that fall within the recommended frequencies agreed by the
Department of Health, the Association of Optometrists and the Federation of Ophthalmic and
Dispensing Opticians (FODO). The current guidelines recommend sight tests once every two
years for adults aged between 16-70 years and annually for: people aged over 70; people with
diabetes; or people aged over 40 with a family history of glaucoma or with ocular hypertension and
are not in a monitoring scheme (Primary Ophthalmic Services Regulations, 2008). However, an
eye practitioner may claim for a GOS sight test at a shorter interval if there is a clinical reason for
doing so, for example, if the patient has a pathology that is likely to worsen. This reason must be
indicated on the request for reimbursement. In the year to the end of March 2009 16.5 million sight
tests were carried out in England, of which 5.2 million were private and the remainder were NHS
funded (FODO, 2010).
Sight testing is provided by eye professionals who conduct testing either at a practice or through
mobile or domiciliary testing for people who are unable to leave their homes. Not all eye
professionals conduct domiciliary testing, and specialist equipment is required by those that do.
People who live full-time in a residential care home qualify for domiciliary testing as long as the
home is their main place of residence and they are “unable to leave the home unaccompanied
because of physical or mental illness or disability” (NHS Choices website). Those who qualify for
domiciliary testing also receive their eye tests free on the NHS. When carrying out eye testing in a
domiciliary setting, eye professionals must notify the patients to be tested and provide notice
(previously to PCTs, now under the Health and Social Care Act (2012) to the NHS Commissioning
Board, which will be established October 2012) of their visit (48 hours’ notice for one or two
patients and three weeks for three or more patients) (General Ophthalmic Services Contract
Regulations, 2008). This notice period permits monitoring as to whether that patient is eligible for
14another sight test. This process was designed to prevent tests being performed unnecessarily and
charges claimed for by multiple eye health practitioners.
Representative bodies of the eye health professionals have responded to the complex
requirements of a domiciliary sight test and the variety of issues that a patient confined to their
residence may experience by producing a code of practice for domiciliary testing. The practice
guidelines reinforce the entitlement of people receiving domiciliary testing to the standards
experienced by those receiving eye tests at the eye professional’s practice (for example, being
treated as an individual and not having to participate in group testing). The guidelines also
highlight issues such as communication where special attention may be needed for this group
(ABDO et al, 2009).
Care homes
The essential standards of quality and safety for care homes consist of 28 regulations (and
associated outcomes) that are set out in two pieces of legislation: the Health and Social Care Act
2008 (Regulated Activities) Regulations 2010 and the Care Quality Commission (Registration)
Regulations 2009.
Under the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 a registered
individual at the care home (or other service provider) is responsible for residents’ health. These
regulations stipulate (among other areas) that care provision (including medical treatment) should
be adapted to meet each resident’s individual needs, that the resident should have their privacy,
dignity and independence respected, with their views taken into account in their service delivery,
and that the care home should work with other providers to ensure the appropriate health and
social care support for the resident (Regulations 9, 17 and 24 respectively). These regulations
form the basis of how the health of residents is managed in care homes. While they do not
specifically mention eye health, a precedent is set for how it should be managed within the broader
remit of health and social care provision by the care home.
Within the regulatory framework relating to care homes there are few specific mentions of sight
testing, with eye health being covered more generally under regulations relating to general health.
As a result there is not one pathway to sight testing in a care home. Sight testing can be pursued
by the care home (acting on a resident’s request, or otherwise) or can be set up through contact
from eye professionals asking to complete sight tests in the home. While much of this will be
domiciliary testing, some residents may be able to travel to a practice premises in order to receive
testing, which requires some coordination of their medical records and accompaniment by a care
home worker. Some care homes will have policies in place to frame their sight testing procedures,
and others are purely reactionary to requests from residents. The visiting eye professionals will
vary from those from smaller, local practices to one of the larger optometry companies that
specialises in sight testing in care homes across the country. Nationally, there is no standard
procedure for the management of sight testing for care home residents, with the exception of the
precedent set by legislation that healthcare should be patient-focussed and patient-managed.
Prior to the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 and the Care
Quality Commission (Registration) Regulations 2009 quality of care was standardised by the
National Minimum Standards for Care Homes for Older People, produced by the Department of
15Health (2003), now superceded. Sight testing was specifically mentioned in the standards, which
stipulated that when new residents are admitted care homes undertake a full assessment of their
health and personal needs, including: ‘sight, hearing and communication’ (Standard 3.3). This
assessment was designed to provide the basis of the care plan each resident receives, to be
updated at least once a month to reflect ‘changing needs and current objectives for health and
personal care’ (Standard 7.4). In addition, access to sight tests and appropriate aids, according to
need, were specifically mentioned in Standard 8, which covers health and healthcare provision.
There was also a requirement for staff to aim to ‘maximise [the] service user’s capacity’ (Standard
8.1).
The Care Quality Commission (CQC) is the body responsible for the regulation and assessment of
all providers of health and social care in England, including care homes and their performance in
providing care. They run inspections of homes and provide guidance for good quality care. The
CQC has recently undertaken a review of its care assessment practice, and are now using
registration and inspection procedures for care providers in line with the standards of quality and
safety which came into effect in 2010 (CQC, 2010a). These new guidelines are designed to be
more generic and focus on the end outcome of the care provided, rather than detailed descriptions
of the provisions that should be made (Stakeholder interview).
The Wales Council for the Blind and the Care Standards Inspectorate for Wales (the equivalent of
the Care Quality Commission in England) published supplementary guidance relating to sight loss
for the Minimum Standards to advise inspectors who were interpreting them (WCB and CSIW,
2003). This guidance expanded on the existing regulations with detailed instructions for ensuring
standards were met in relation to sight loss. For example, the advice for Standard 8.1 suggested
that a service user’s capacity can be optimised by ‘maximising the sight by proper medical
treatment’ (WCB and CSIW, 2003, p. 8). No such supplementary guidance is currently used for
care homes in England under the current regulations.
Other organisations have produced guidance for care home workers to supplement the minimal
information provided by legislation and regulation. The RNIB has provided a guide for care home
workers to highlight the need to detect and support sight loss in residential homes. Their guidance
for detection includes a list of key signs to be aware of, such as falls, walking into doorways and
furniture, difficulty recognising people and so on. The guide then suggests that a sight test should
be arranged if two or more key indicators from this list apply to a resident, and suggests support
mechanisms such as environmental adjustments (RNIB, 2010). Other guidance and training
comes directly from eye professionals themselves, for example, Health Call Optical, a large
nationwide group of optometrists specialising in domiciliary eye testing, run training sessions for
care home workers to increase awareness of the signs of sight loss (Stakeholder interview).
Additional materials have been developed by the third sector, such as the My Home Life bulletin
and poster for care homes (My Home Life, 2011).
Wider policy context
Improving eye health
In 2008 the UK Vision Strategy was launched as an initiative by Vision 2020 UK, lead by RNIB to
draw together the variety of groups that work in eye health with common goals. It was developed
16as a response to the resolution from the World Health Assembly Resolution 2003 to reduce
avoidable blindness by the year 2020 (UK Vision Strategy, 2008). The strategy has three key
outcomes:
1. Improving the eye health of the people in the UK
2. Eliminating avoidable sight loss and delivering excellent support for people with sight loss
3. Inclusion, participation and independence for people with sight loss
(UK Vision Strategy, 2008)
The aims for these areas include raising awareness and understanding of eye health in the public
and among service providers, including health and social care practitioners. It also aims to ensure
‘the early detection of sight loss and prevention where possible’.
Recently, the need to improve eye health has been included in national public health planning. In
the Public Health White Paper ‘Healthy Lives, Healthy people’, the Department of Health drew
attention to avoidable sight loss with in the inclusion of an eye health indicator in the Health
Outcomes framework (Department of Health, 2012). The Department of Health also produced the
Commissioning Toolkit for Community-based Eye Care service in 2007, promoting a message of
developing eye health provision away from hospital-based services (Department of Health, 2007).
Recent progress has also been made on improving eye care service provision, with the
establishment of model pathways for cataracts, glaucoma, AMD and low vision (Bosanquet and
Mehta, 2008).
Care
In November 2010 the coalition Government announced its Vision for Adult Social Care, setting
three core values. The Government wants to develop social care which gives people the freedom
to choose services and shifts power from the centre. They want social care to be fair in terms of
funding and they emphasised the need to move towards a shared responsibility for care between
the individual and the state (Department of Health, 2010b).
The Care Quality Commission have published a special review of the provision of healthcare in
care homes, focusing on whether people in care homes have equal access to services from the
NHS, have choice and control over their health care and if the care they receive preserves their
dignity and promotes good standards of safety (CQC, 2012). This review assessed the poorest
achieving areas, consulted with local care homes and asked care home workers and managers to
feedback on the areas where they required more prescriptive notes and signposting to best
practice. Among the requested areas for these additional notes are incontinence care, and
medication regulation. Vision and sight loss were not one of the areas where additional notes were
requested by the trialed care homes (Stakeholder interview). This review also looked at how a
person’s healthcare needs were identified, including examining case files for indications of
assessment of various areas, including foot care/podiatry/chiropody, dental health, but not for
vision or eye health (CQC, 2012).
Older people
Policy makers have developed specific strategies to address the unique health problems and
issues in accessing health and social care equitably that older people face. In 2001 the NHS
17introduced the National Service Framework for Older People (NSF), a ten year plan for improving
services for older people, particularly looking at creating national standards and preventing
disparities in the level of care received (Department of Health, 2001). This strategy supports the
idea of joined up care and interaction between different elements of the health and social care
system in order to achieve the best possible health and to give older people the maximum amount
of independence and quality of life. Questions have been raised over the lack of attention given to
sight loss in the NSF document or follow-up progress reports, where there are only brief mentions
of the role of sight loss as a risk factor for falls (Bosanquet and Mehta, 2008).
This sentiment of ensuring a higher quality of life in older age has been echoed by the Care
Quality Commission’s position statement and action plan for older people, including people with
dementia (2010b). It too picks up on the need for joined-up care, having identified issues with
patients passing between different services and a lack of coordination. As well as providing a basic
standard of care quality, it is also highlighted that care homes should be places to promote
independence and a good quality of life: ‘”Look at the culture in the (care) home, helping people to
enjoy life rather than just waiting for them to die.”’ (CQC, 2010b, p.6). To this end, the plan also
supports the personalisation of care and places emphasis on the choice of older people and
people with dementia about their care options.
In addition to the positive effects of improving quality of life for residents, research has also gone
into the potential of preventative health measures to improve the efficiency of services. The role of
prevention both as a tool for delaying or reversing deterioration, and for increasing the potential
and independence in functioning of older people has been explored by the Department of Health
(2010a). While still supporting the view that people should be given as much independence as
possible for as long as possible, this research also highlights the costs of a higher level of
dependency in this group, particularly in the context of an ageing population. Falls are an area that
is particularly highlighted in this report, with recommendations to focus on the causes of an
individual fall in order to prevent further (and potentially more serious) falls occurring. ‘Joined-up’
care and building effective working relationship between different providers of health and social
care is recommended, as in other reports.
Equality
The Equality Act (2010) supercedes much of the previous legislation related to discrimination and
presents a standard for all marginalised groups. Under the Act, discrimination law related to age,
disability, gender reassignment, marriage or civil partnership, race, religion or belief, sex and
sexual orientation is drawn together into one document. The Equality Act prohibits any
discrimination, either direct or indirect, based on any or all of these characteristics, when providing
services (among other areas). There are exceptions permitted in the Act in order to allow for, for
example, differential sight test entitlements based on age.
18Issues and barriers
The regulation of health provision for care home residents covers a broad remit of health, including
sight. However, there are limitations on the performance of these regulations, evidenced by the
numbers of people not receiving sight tests they are entitled to (FODO, 2010) and through informal
reports of under-testing from consultation with stakeholders, including optometrists. There are a
number of barriers to pursuing better eye health and sight testing for the different parties involved:
the individuals themselves, families and carers, care home staff, care home managers, eye health
practitioners and professionals from the wider health community. There are additional issues at the
regulatory and guidance level.
Residents
At an individual level, a lack of awareness of eye health and sight problems is a key issue. In an
RNIB survey, 60% of a sample aged over 60 who had not had an eye test in the previous two
years stated that the main reason was that they were not having any sight problems (RNIB, 2007).
Given the incidence of sight problems at this age, it is likely that at least some of these people are
experiencing sight problems, or are in need of a new prescription for their existing corrective aids,
but are unaware of this. There is also a fatalistic assumption among many older people that sight
will inevitably decline with age and that this process is irreversible. Therefore they are unlikely to
recognise, accept or communicate that sight loss is a problem. A positive attitude to preventative
health (as opposed to attributing change to a normal ageing process) has been shown to have a
positive association with the uptake of eye checks (Iliffe et al, 2009). Older people may feel that a
slight impediment in their sight is an insignificant health problem compared to other health
problems they or their contemporaries are experiencing. Additionally, it has been reported that
care home residents are reluctant to agree to intervention, particularly surgical procedures
(Fletcher et al, 2009).Research has found that while many older people (aged over 60) understood
the benefit of a sight test as a tool for early detection of eye disease (RNIB, 2007; McLaughlin and
Edwards, 2010), this did not translate into seeking sight tests for themselves (RNIB, 2007).
Considering the strong emphasis on patient-focused care and the promotion of independence for
older people, combatting the perception of a lack of need or inevitable deterioration will rely heavily
on increasing the patient’s awareness and interest in their own eye health.
In addition to residents potentially being unaware of their sight problems, some may be aware of a
change but unable to communicate it to others. As mentioned above, dementia is a key issue in
this area. For some in the middle to later stages of the disease in particular, communication can be
very difficult, either in alerting someone to issues that they are aware of with their sight or their
general level of communication such that the external signs of sight problems which could be
picked up by people around them, will go unnoticed. While there are best practice guidelines
issued by representative bodies for testing sight in people with dementia and navigating these
communication difficulties (College of Optometrists Ethics and Guidance, 2011), this relies on the
sight issue being highlighted in order to book a sight test.
Some samples of older people surveyed on eye health have stated that the cost or fear of the cost
of the test and glasses is a barrier to seeking sight testing (RNIB, 2007; RNIB Cymru, 2011). The
vast majority of people living in care homes (that is, all residents who are unable to leave the care
19home owing to their health) are eligible for free tests, meaning that theoretically this is an even
smaller issue for this group than for the general population. However, some concerns have been
raised over the cost of glasses and other corrective aids, as there is only limited financial support
available from the NHS. Even those who are eligible for financial support for acquiring glasses
(those with low incomes) are not always aware of that fact (RNIB, 2007). However, analysis has
found that economic status is not significantly associated with take-up of eye examinations (Iliffe et
al, 2009).
While patient-centred healthcare is a positive outcome of recent health regulation, there are limits
to what can be achieved in the way of choice for care home residents in their sight tests. Their
preferred eye professional may not conduct domiciliary testing, or they may have moved from the
area covered by that particular provider. The guidelines on the GOS contracts issued by the
representative bodies of the eye professions suggest that there has historically been some
contention between eye health professionals and PCTs over practitioners refusing to conduct
domiciliary sight testing based on distance to travel (Association of British Dispensing Opticians et
al, 2008, p.3), particularly if another contractor able to perform domiciliary testing is situated closer.
These practical boundaries impose limits on the choice of provider for residents in care homes.
These limits may have a detrimental effect on the care home residents: being unable to use their
previous eye professional, they lose interest in sight testing or are not comfortable with switching
to a new practitioner. In this way a resident’s lack of empowerment about their own health choices
could be a barrier to eye health.
Families and carers
Families and carers of care home residents are potentially a useful group to highlight sight
problems and advocate testing, not having the conflicting responsibilities or time restrictions of a
care home worker. However, they are subject to many of the same issues that the residents
themselves face, namely a lack of awareness and knowledge of eye health and the benefits of
regular sight testing. They too may see sight loss as an inevitable part of the ageing process, be
unaware of the role a sight test plays in early detection of eye disease and other conditions or, like
the residents themselves, fear the cost of testing and glasses. Interviews with stakeholders
suggest that many do not think of sight loss as a problem; given the other, potentially multiple,
health issues the resident may be experiencing which have more pronounced symptoms, vision
problems are not on their priority list. There is a perception that measures designed to improve the
quality of life of dementia patients will not be effective, and therefore should not be attempted
(Alzheimer’s Society, 2007). As a result, families may feel that glasses and other interventions are
a waste of money.
However, a resident without a support network may actually be subject to an increased risk of
undetected sight loss without these potential advocates present to notice signs of impaired vision
and raise the issue of sight testing on their behalf. Indeed, some materials encourage family or
carers being present during sight tests for their additional knowledge of the patient’s history and
health needs, particularly if a patient is suffering from advanced dementia (College of
Optometrists, 2011).
20Care home staff
Stakeholders suggested that some care home staff were concerned about raising the issue of
potential sight loss in residents as the staff felt it detracted from the promotion of a culture of
independence for residents. Eye health is, relatively speaking, an open healthcare market
(Bosanquet, 2010), with patients given a variety of choice of eye health practitioners both for their
sight tests and separately for their prescribed glasses and contact lenses. While this level of
independence can be positive and promotes patient-centred care, it also means that there is
greater pressure on the patient to pursue sight testing and vision correction, which as referenced
above, is an unlikely course of action for many residents. Restrictions in the GOS contract
protecting the patient’s right to choose who provides their sight testing or whether they receive
testing at all add to this issue. As a result, fewer people are receiving sight testing than could
benefit from it, particularly domiciliary testing (FODO, 2010). This becomes more complex still
when responsibility for health is transferred as the person enters a care home. While the aim
across regulation of care homes to maintain the independence of a person as they transition into
residential care is laudable, it leaves the residents potentially uninformed about the much higher
risks they face of sight loss.
Much of what exists in the current regulations, best practice guidelines and material from the
voluntary sector refers to care options and environmental improvements for previously detected
poor sight or vision problems: suggesting that if a resident wears glasses when they enter the care
home their needs will be taken into account. The professional guidelines issued by the Care
Quality Commission on their essential standards mention vision only in the context of notifying the
CQC of severe injuries (CQC, 2010). However, there is little that addresses the issue of
undetected or worsening vision problems that are not an emergency for residents.
Care home staff are potentially best placed to detect the signs and behaviours that point to vision
problems, and to recommend sight testing for residents, as they will have the most contact with the
residents and receive training as part of their role. However, as a workforce they are generally
overstretched despite working extremely hard, with many responsibilities and tasks needing to be
completed. As a result (although this will not be the case in all care homes), eye health and sight
problems may not be on their list of priorities as they are not perceived to be a serious threat to the
health of their residents. They may have little awareness of the problems associated with
deteriorating sight, and the potential for treatment and adjustment for many eye conditions, or its
role in other conditions on which they have received training, such as dementia. This is due to a
number of factors: insufficient or infrequent education or training on sight loss and how to
recognise it; a primary concern with other health problems of their residents; inability to
communicate or understand communications effectively with residents in order to establish the
possibility of sight loss (particularly those with mental health problems, see above); lack of interest
in or importance given to sight loss prevention (for example, for advanced onset dementia patients
where there may not be a perceived improvement to be made in their quality of life). Equally, a
care home worker may be fully aware of the issues and signs of sight loss, but be restricted in the
time available to highlight problems with a resident. Additionally, as mentioned above, there is a
problem of confidence in raising the issue of potential sight loss in relation to providing a resident
with independence and control over their own health.
21You can also read