Understanding the positive outcomes of discharge planning interventions for older adults hospitalized following a fall: a realist synthesis - BMC ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Provencher et al. BMC Geriatrics (2021) 21:84
https://doi.org/10.1186/s12877-020-01980-3
RESEARCH ARTICLE Open Access
Understanding the positive outcomes of
discharge planning interventions for older
adults hospitalized following a fall: a realist
synthesis
Véronique Provencher1,2*, Monia D’Amours2, Matthew Menear3,4, Natasa Obradovic1,2, Nathalie Veillette5,
Marie-Josée Sirois6 and Marie-Jeanne Kergoat7
Abstract
Background: Older adults hospitalized following a fall often encounter preventable adverse events when transitioning
from hospital to home. Discharge planning interventions developed to prevent these events do not all produce the
expected effects to the same extent. This realist synthesis aimed to better understand when, where, for whom, why
and how the components of these interventions produce positive outcomes.
Methods: Nine indexed databases were searched to identify scientific papers and grey literature on discharge
planning interventions for older adults (65+) hospitalized following a fall. Manual searches were also conducted.
Documents were selected based on relevance and rigor. Two reviewers extracted and compiled data regarding
intervention components, contextual factors, underlying mechanisms and positive outcomes. Preliminary theories were
then formulated based on an iterative synthesis process.
Results: Twenty-one documents were included in the synthesis. Four Intervention-Context-Mechanism-Outcome
configurations were developed as preliminary theories, based on the following intervention components: 1) Increase
two-way communication between healthcare providers and patients/caregivers using a family-centered approach; 2)
Foster interprofessional communication within and across healthcare settings through both standardized and unofficial
information exchange; 3) Provide patients/caregivers with individually tailored fall prevention education; and 4)
Designate a coordinator to manage discharge planning. These components should be implemented from patient
admission to return home and be supported at the organizational level (contexts) to trigger knowledge, understanding
and trust of patients/caregivers, adjusted expectations, reduced family stress, and sustained engagement of families
and professionals (mechanisms). These optimal conditions improve patient satisfaction, recovery, functional status and
continuity of care, and reduce hospital readmissions and fall risk (outcomes).
(Continued on next page)
* Correspondence: veronique.provencher@usherbrooke.ca
1
School of Rehabilitation, Faculty of Medicine and Health Sciences, Université
de Sherbrooke, Sherbrooke, QC, Canada
2
Research Centre on Aging, Sherbrooke, QC, Canada
Full list of author information is available at the end of the article
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,
which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons
licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons
licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain
permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the
data made available in this article, unless otherwise stated in a credit line to the data.
Provencher et al. BMC Geriatrics (2021) 21:84 Page 2 of 18 (Continued from previous page) Conclusions: Since transitions are critical points with potential communication gaps, coordinated interventions are vital to support a safe return home for older adults hospitalized following a fall. Considering the organizational challenges, simple tools such as pictograms and drawings, combined with computer-based communication channels, may optimize discharge interventions based on frail patients’ needs, habits and values. Empirically testing our preliminary theories will help to develop effective interventions throughout the continuum of transitional care to enhance patients’ health and reduce the economic burden of avoidable care. Keywords: Discharge planning, Falls, Older adults, Transition of care, Review Background planning intervention components, contexts, mecha- Falls among older adults are a worldwide public health nisms and outcomes could lead to a more optimal de- concern, especially in the context of an aging population sign of interventions and improved outcomes for older [1]. According to the U.S. Centers for Disease Control adults and their families. and Prevention, falls are the leading cause of non-fatal The general research question was: How do the key injuries among older adults, and one in ten falls leads to components of discharge planning interventions target- a serious injury, such as a hip fracture or head injury, ing older adults hospitalized after a fall generate their which requires hospitalization [2]. In Canada, accidental outcomes, and for whom and in what circumstances are falls were the main cause (81%) of older adults being these components effective? Specifically, this study hospitalized for injury in 2019, which is a 9% increase aimed to: 1) Identify the key components of discharge over the previous year [3]. In the European Union, it is planning interventions for older adults hospitalized after estimated that each year almost two thirds (62%) of a fall and their outcomes; and 2) Develop preliminary older adults visiting emergency departments for fall- theories that improve our understanding of how these related injuries were admitted to hospital [4]. intervention components lead to different outcomes Older adults hospitalized for serious injuries due to a fall (mechanisms) and in what contexts (when, where and are exposed to significant risks of adverse events after dis- for whom) these components are effective. These pre- charge, such as a new fall, functional decline, hospital re- liminary theories will represent an important step to- admission, and emergency visits [5, 6]. Patients hospitalized wards recommendations for decision-makers and for a fall are more likely to be readmitted for a fall within clinicians on how to best design and implement dis- 30 days of discharge than non-fall patients (17.4% vs 3.8%) charge planning interventions for older adults hospital- [7]. Many older patients and their families were also dissat- ized following a fall. isfied with the hospitalization and discharge process [8, 9]. Recent studies reported that between one and two thirds of post-discharge adverse events could have been prevented Method [10–12], especially through comprehensive discharge plan- A realist synthesis was performed and reported in ac- ning [13]. The way the discharge is planned and carried out cordance with the standards issued by RAMESES (Real- can thus improve patients’ and families’ satisfaction with ist And Metanarrative Evidence Syntheses: Evolving the process [8, 9, 14–16] and their quality of life [16, 17]. Standards) [25, 26]. This method differs from systematic Many interventions have been developed to optimize reviews in that it not only examines the effectiveness of discharge planning for hospitalized older adults and interventions but also helps us to understand why and positive outcomes for them and their families after the how they produce the expected outcomes by making discharge home [18–24]. However, they do not all pro- their underlying assumptions and processes explicit [25, duce the expected effects to the same extent or in the 26]. In this synthesis, we relied on the work of Dalkin same way since they feature various intervention compo- and colleagues (2015) to conceptualize intervention nents that are delivered at different timepoints in the components as resources that are introduced into a con- healthcare continuum and in several healthcare settings text and that alter individuals’ reasoning and behaviors and target specific subgroups of older adults. Their effi- [27]. These changes in reasoning and behavior are then cacy may vary depending on the context in which they integral parts of the mechanisms that give rise to out- are implemented and because they generate their out- comes. Our realist approach will thus help us to produce comes through diverse mechanisms. The precise nature initial theories that explain how intervention compo- of these intervention components, how they work and in nents (I) provide resources that, when introduced into what circumstances has received little attention. A better certain contexts (C), activate mechanisms (M) that in understanding of the relationships between discharge turn generate various outcomes (O), i.e. preliminary

Provencher et al. BMC Geriatrics (2021) 21:84 Page 3 of 18
ICMO theories relevant to discharge planning for older feasible to focus our synthesis on the development of
adults hospitalized following a fall. preliminary program theories and to conduct work to
define more robust program theories as a later, sec-
Scoping the literature and focusing the review ond phase of the research.
An initial scoping of the literature on discharge plan-
ning interventions for older adults carried out by the Searching process and selection of documents
research team in 2016–2017 led to the identification To identify articles or reports that could be helpful to de-
of several intervention components common across scribe the discharge planning intervention components
discharge planning interventions. Recognizing the and develop initial program theories, we conducted
need to better understand how and why these compo- searches in nine databases (MEDLINE, CINAHL, Ageline,
nents worked, the research team pursued a realist SCOPUS, ProQuest Dissertations & Theses, EBM Re-
synthesis approach and invited several stakeholders to views, Health Star, Nursing & Allied Health Database,
participate. The research team defined the scope of Health Management Database) as well as the grey litera-
the realist synthesis with input from partners within ture, including library catalogs (BANQ, Santécom,
the Quebec Ministry of Health and Social Services re- CUBIQ, Germain [IUGM catalog] and other resources
sponsible for older adult care policies. There was a (BDSP [public health data bank], Google, Google Scholar
shared interest in focusing the review on interven- and Social Care Online). Manual searches in reference
tions that could not only reduce rates of lists of selected articles were also conducted. This search
hospitalization, but also improve the satisfaction of strategy was developed in partnership with an experienced
older adults. Given their increased risk of adverse librarian and verified by a second one. Although a set of
outcomes, we decided to focus the synthesis on the natural and controlled keywords was targeted (Table 1)
population of older adults hospitalized after a fall. based on three main concepts (population: older adults;
This choice led to the need to verify the relevance of interventions / follow-up; outcomes / effects), the search
the previously identified intervention components to strategy was flexible enough to allow for an iterative
this specific population. Finally, based on our initial process involving searching for evidence-based data, as
literature review, we judged it more appropriate and recommended for realist syntheses [28].
Table 1 Database search strategy based on three concepts
CONCEPTS KEYWORDS
1 Population: older adults + [fall-related] older adult*
elder*
senior*
old* people
geriatric patient*
older patient*
aged[MESH]
AND
[accidental fall*]
[hip fracture*]
2 Interventions / follow-up transition of care / transitional care
continuity of patient care
discharge planning
patient discharge
hospital discharge
return to home / returning home
post discharge + follow up / support
3 Outcomes / effects length of stay in hospital
readmission to hospital
emergency visit
admission to an institution
fall
mortality
functional decline
cost
health care utilization
patient health status
patient satisfaction
carer satisfaction
quality of life
well-being
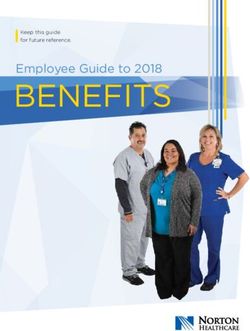
Provencher et al. BMC Geriatrics (2021) 21:84 Page 4 of 18 Selection and appraisal of documents the theory); and 2) rigor (validity and credibility of The selection of documents to be included in the realist the methods used). The ‘relevance’ criterion was ap- synthesis was carried out by a single reviewer following plied throughout the selection process whereas the a three-step process: 1) title screening; 2) abstract ‘rigor’ criterion was used during the full-text screen- screening; and 3) full-text screening. Documents were ing process. Documents were relevant if they con- considered eligible if the population of interest was older tributed information about the contexts, mechanisms adults (65 years and older) that had been hospitalized or outcomes of discharge planning intervention com- following a fall. ponents. One reviewer examined all relevant empir- They were also eligible if they described any discharge ical articles using the Mixed Methods Appraisal Tool planning intervention or components of these interven- (MMAT) [29], a valid and reliable tool suitable for differ- tions. We excluded studies that described interventions ent types of empirical studies (qualitative, quantitative, implemented exclusively post-discharge, in emergency mixed) to ensure that selected documents met minimal departments, or in palliative care (as our focus was the criteria for rigor. No articles were excluded from the real- process of discharge planning for hospitalized older ist synthesis based on the rigor. The principal investigator adults). Documents not reporting outcomes (e.g. proto- supervised the complete process to ensure adequate selec- cols, abstracts of posters) were excluded. Reverse citation tion of relevant documents. searches to capture studies related to these protocols or abstracts were done when it was relevant, but none were Data extraction found. Consistent with realist methods, we did not ex- With respect to data extraction, one reviewer extracted clude studies based on their research design and a wide information on data sources (year of publication, authors, variety of design types were eligible for inclusion in the study type), population characteristics (diagnosis, comor- synthesis (e.g. clinical trials, observational studies, quali- bidity/frailty, presence of cognitive deficits) and healthcare tative studies, etc.). However, we did exclude any docu- settings (acute, post-acute, community). To understand ments published in languages other than English or evidence-based effects of intervention components in a French. In order to consider evidence consistent with specific context, the reviewer then extracted and compiled current healthcare contexts and circumstances, we only the data in a table using a classification based on key con- included documents published in the past decade. As cepts of a realist synthesis, namely intervention compo- the initial database searches were conducted in 2018 and nents (I), contextual factors (C), underlying mechanisms then updated in 2020, articles published before 2008 (M) and outcomes (O). Extracting data based on these were excluded. concepts enabled the research team to then synthesize the In addition to these criteria, we used an assess- information in order to develop Intervention-Context- ment grid to select documents based on two other Mechanism-Outcome (ICMO) configurations [25–27, criteria: 1) relevance (contribution to development of 30–33] that reflect our preliminary theories. Fig. 1 Iterative process used to develop the ICMOs

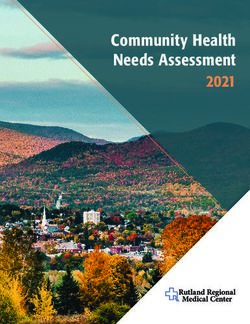
Provencher et al. BMC Geriatrics (2021) 21:84 Page 5 of 18 Fig. 2 Document selection flowchart, OAH: older adults hospitalized, ED: emergency department, int: intervention Analysis and formulation of preliminary program theories and mechanisms, these aspects were enhanced and Two reviewers and the principal investigator then clarified with complementary sources of data regard- analyzed and synthesized the extracted data as fol- ing discharge planning for older adults. Full-text lows: 1) the information gathered was organized by assessed for eligibility documents pertaining to hos- intervention component (I); 2) for each intervention pitalizations for hip fracture (round 2) and in gen- component, we identified recurring patterns of asso- eral (round 3) were thus included if they ciated outcomes; 3) we examined relationships be- documented mechanisms and contexts and were ap- tween underlying mechanisms (M) (i.e. resources, plicable to fall situations. reasoning and behaviors) and specific outcomes (O); Regular team meetings were held throughout the and 4) we explored the contextual factors (C) that process to discuss emerging ICMO configurations and influenced the expression of M-O relationships. Fig. 1 produce iteratively revised versions. Synthesis of the shows the iterative process we used to develop the evidence led to the development of the main prelim- ICMOs. Data from articles specifically related to inary theories resulting from the analysis process. older adults hospitalized after a fall were first ana- Knowledge users (decision-makers, clinicians) were lyzed (round 1). The central place of communica- consulted during this process to ensure that the pre- tion, education and coordination in components of liminary theories formulated were clinically relevant. discharge planning interventions was highlighted and these became the foundation for developing the pre- Results liminary program theories (ICMOs). As there were Figure 2 shows the flowchart for the selection of docu- few articles on discharge planning for older adults ments. Out of 8809 records identified (8794 through hospitalized after a fall that documented contexts database searches after duplicates were removed and

Table 2 Synthesis of each Intervention-Context-Mechanism-Outcome (ICMO) configuration
INTERVENTION COMPONENTS (I) CONTEXTS (C) MECHANISMS (M) OUTCOMES (O)
ICMO-1: Two-way communication between healthcare providers and patients/caregivers
Provide patients and families with individually When For patients ↑ patients’ and families’
tailored, complete and repeated information [34] Throughout the discharge planning process ↑ understanding of how to balance risks safely [38] satisfaction [37, 41]
Regarding: - from admission [37, 43] to post-discharge (home) [37] For patients and families ↑ patients’ recovery [38,
health conditions, symptoms, how they evolve and - frequently [35] Communication on recovery time and ↑ knowledge of the illness/ injury [36] and how to 40]
how to manage them [9, 34] risk management manage it [9] ↑ patients’ functional
healthcare planning [9, 35–38] - before discharge [38, 41] ↑ adjustment of expectations regarding recovery [41] status [38, 40]
information seeking [9] For whom ↑ self-confidence, sense of control [38] and feeling of
Provencher et al. BMC Geriatrics
Using: Some intrinsic characteristics may compromise being prepared [37]
verbal and written communication [34] (adapted to communication [38, 44] ↓ stress and frustration [9, 34–36]
each patient) [39] - advanced age [38, 44] ↓ confusion and tension between family members
simple language [40] - high degree of frailty [38, 44] [37]
Involve patients and families in healthcare and - living alone [38] For healthcare providers
discharge planning [9, 35, 36, 38, 41] ↑ ability to address questions that patients do not
Improve knowledge and understanding of families’ know how to ask [41, 45]
(2021) 21:84
concerns, barriers and expectations to recovery [34, 41,
42]
Have a comprehensive picture of the situation [9, 39]
ICMO-2: Interprofessional communication within and across healthcare settings
Interprofessional communication and information When ↑ knowledge and understanding of healthcare ↑ quality of care [9, 34, 39]
sharing Throughout the healthcare continuum [9, 39] providers regarding patients’ situations, and their own ↓ hospital readmissions
accurate and effective [9, 36, 38–40, 45, 46] Between different healthcare settings [39] respective roles, tasks and responsibilities [9, 34, 46] [9, 35]
By using/doing: Where ↓ redundancies, overlap, delays, inaccuracies, ↑ identification of
standardized routine for information exchange [9, In a supportive organizational and management incompleteness, uncertainties regarding what has patients at risk of falls [47]
47] context (local and national levels) [44, 47] been done [34]
verbal and timely non formal communication [9] ↓ losses of information across care settings [39]
regular multidisciplinary meetings [9, 43, 47] ↓ anxiety and frustration experienced by healthcare
complete handovers documenting fall risk [36, 46, providers [39]
47] ↓ time spent gathering information on patients [9]
Web-based information system [9, 35, 39]
(interoperable across care settings and available to
all healthcare providers throughout the continuum
of care) [39]
clear boundaries for care (tasks and responsibilities)
between all healthcare providers [35, 40]
ICMO-3: Patient/caregiver individually tailored education on fall prevention
Patients’ and caregivers’ education and training When For patients and caregivers ↓ fall risk [49, 50]
should: Before discharge [36, 49, 50] ↑ awareness of fall prevention [37] ↓ negative psychological
Target real needs of patients at home [37, 48, 49] Reinforced education by follow up phone call post ↑ recognition of near-falls [49] impacts on caregivers
Teach possible prevention strategies and exercises to discharge [49] For patients (burden) [37]
foster recovery [37, 38, 48, 49] For whom ↑ knowledge of prevention strategies [42, 48] ↑ safety in the care
Encourage and motivate patients to use these Optimal in cognitively healthy patients [42, 48, 49] ↑ confidence and motivation to use them [42, 48] provided by caregivers at
strategies and do the exercises [42, 48] If patients cognitively impaired: caregivers’ education is For caregivers home [36]
Provide families with written educational material [48] essential [48] ↑ knowledge of the illness/ injury makes them more ↑ continuity for patients in
Caregivers’ education and training should also: resilient when providing care (↑ flexibility and abilities) transition from hospital to
Cover patients’ medical condition, signs of [37, 38] home [37]
complications, physical care requirements, medication,
Page 6 of 18
etc. (be prepared for “afterwards”) [37, 38]Table 2 Synthesis of each Intervention-Context-Mechanism-Outcome (ICMO) configuration (Continued)
INTERVENTION COMPONENTS (I) CONTEXTS (C) MECHANISMS (M) OUTCOMES (O)
ICMO-4: Discharge planning coordination
Designation of 1 pivotal healthcare provider When ↑ stability and consistency through coordinator’s ↑ quality (continuity) of
(coordinator) to manage discharge planning [35, 38, Throughout the discharge planning process - from regular contacts with patients, families and care [34, 39, 48, 53]
39, 50]: admission to discharge [35, 36, 40, 51] - post-discharge professionals [34, 39] ↑ patients’ quality of life
Acting as the single regular contact point for patients (home) [36] ↑ trust [39] (physical, psychological
[35] For whom ↑ identification, anticipation and alleviation of barriers and social needs met) [48]
Coordinating a comprehensive intervention adapted Older patients’ multiple comorbidities and medical experienced by patients [34, 35] ↑ patients’ satisfaction [52]
to patients [50] complexities require extensive coordination as many ↑ communication and information sharing among
Provencher et al. BMC Geriatrics
Tools to facilitate coordination: healthcare providers are involved [35, 36, 41, 50, 53] healthcare providers and settings [53]
Interdisciplinary worksheet to record all the barriers to ↑ identification and prioritization of patients’ needs
a safe return home identified by all the healthcare [48]
providers [51] ↑ personal engagement from each healthcare
Web-based information system to integrate provider and families over care [34]
information from different providers and care settings
[35, 50, 52]
(2021) 21:84
Page 7 of 18Provencher et al. BMC Geriatrics (2021) 21:84 Page 8 of 18 Fig. 3 ICMO-1: Two-way communication between healthcare providers and patients/caregivers 15 through manual searches), the full text of 48 was ICMO-1: two-way communication between healthcare assessed for final eligibility. Only seven documented providers and patients/caregivers contexts and mechanisms of interventions aimed at Key findings optimizing discharge planning for older adults hospi- The first ICMO (Figure 3) can be synthesized as follows: talized after a fall. Fourteen other documents related increase two-way communication between healthcare to older adults hospitalized for a hip fracture (n = 7) providers and families (patients and caregivers) regard- or hospitalized in general (n = 7) were added to enrich ing the patient’s health status, care provided and care our understanding of contexts and mechanisms. Thus, planning, and address barriers experienced by families a total of 21 documents were included in the (I), when occurring early in the process (upon admis- synthesis. sion) (C), trigger a better patients’ understanding of how Additional file 1 presents the descriptive of the se- to manage risks safely, caregivers’ knowledge of the ill- lected documents. Comprising 20 scientific papers and ness/injury and how to handle it, and families’ realistic one research report, the studies used different research expectations regarding recovery, self-confidence and strategies to investigate discharge planning. There were self-efficacy (M), which produce an improvement of pa- two Randomized Control Trials (RCT), four other quan- tient satisfaction, recovery and functional status (O). titative studies, two mixed-methods processes, seven qualitative studies, one using both qualitative methods Intervention components and a literature review, and five literature reviews. The Communication between healthcare providers and fam- latter were international (n = 5) while the others were ilies (patients and caregivers) regarding the patient’s conducted in different countries from almost every con- health status, care provided and care planning is one of tinent (North America 7, Europe 4, Oceania 3, South the core components of these interventions (or sug- America 1, Asia 1). More than half the papers (57%; n = gested interventions to address gaps) to improve dis- 12) were published between 2010 and 2014, nearly one charge planning for hospitalized older adults. Several third (29%; n = 6) since 2015, and 14% (n = 3) before studies report patients’ and caregivers’ frustration with 2010. communication during healthcare delivery [35, 36] as This realist synthesis led us to develop four ICMOs to they often feel they have not received enough or appro- better understand how and why the intervention compo- priate information from healthcare providers [9, 35, 37, nents designed to improve discharge planning for older 38]. In their literature review of best practices for hos- adults hospitalized following a fall might generate posi- pital discharge planning for frail older people, Bauer tive outcomes: 1) two-way communication between et al. [38] emphasized that the lack of communication healthcare providers and patients/caregivers; 2) interpro- between healthcare providers and patients/families was fessional communication within and across healthcare one of the main barriers to an effective discharge settings; 3) patient/caregiver individually tailored educa- process. tion on fall prevention; and 4) discharge planning coord- Healthcare providers should give patients individually ination. Table 2 synthesizes the content of the four tailored, comprehensive, adequate and repeated informa- ICMOs. tion [34]. They should advise patients and caregivers
Provencher et al. BMC Geriatrics (2021) 21:84 Page 9 of 18
how to manage the formers’ health conditions and Some intrinsic characteristics may also have an impact
symptoms and how to seek help [9], and they should on communication. For example, with advanced age
provide families with written information [9, 34]. The (85+) and a high degree of frailty, communication effi-
way information is shared should be adapted to each pa- cacy may be compromised [34, 43]. As the oldest old,
tient [39]. Being informed should mean receiving not frailest patients and those who live alone are more likely
only information but also feedback, advice or reassur- not to be informed, not remember being informed or be
ance from healthcare providers about the patient’s pro- unable to understand the information provided and then
gress (after hip fracture, etc.) [34]. take undue risks [34], adequate communication is par-
Families should also be included in planning care ticularly important in this context.
(current and follow-up) and discharge [9, 34–36, 38, 39,
41]. By engaging patients and their caregivers in discus- Mechanisms
sions that recognize their perceptions of future risk, their Being well informed (i.e. provided with suitable informa-
concerns and the barriers to recovery they encounter or tion) improves patient understanding regarding how to
worry about, healthcare providers will know the right in- balance risk safely [34] and increases caregiver knowledge
formation to share with them [34, 41]. For example, of the illness/injury [37] and how to manage it [9]. This
many patients may experience a fear of falling when dis- greater knowledge will reduce families’ stress and frustra-
charged home after a fall or hip fracture [34, 37, 41, 42]. tion [9, 35–37] and increase patients’ and caregivers’ self-
In these cases, some advice from healthcare providers confidence and self-efficacy [34], sense of control, self-
could be perceived as threatening their safety [34] and care and symptom management after hospitalization [9].
patients may avoid participating in activities that they To enhance their self-efficacy, patients need to acknow-
could in fact do [41]. To ensure responsive interactions, ledge their progress and achievements [34]. When pro-
it is crucial to have a better understanding of families’ vided with adequate information, family members will be
concerns [34]. able to achieve a balance between making progress and
For fall-related hip fractures, some authors emphasize potential dangers versus the use of protective strategies
the importance of addressing patients’ expectations re- and following professionals’ instructions [34]. Conversely,
garding recovery [42] and conducting a comprehensive a lack of information may cause anxiety and frustration,
assessment to develop a customized discharge plan [45]. and make caregivers feel unprepared for discharge, which
Healthcare providers may use a preoperative classifica- worsens their relationship with the patient [38]. Written
tion system to assess patients and produce a more ex- information minimizes confusion and tension between
haustive, personalized recovery timeline for their family members [34].
patients [42]. Consulting relatives may also give them a Giving patients incomplete information leads to un-
more comprehensive view of the situation as family realistic expectations about recovery that are at odds
members may provide valuable information about the with their lived experiences and makes them less en-
patient’s health [9, 39]. gaged in their own recovery [42]. An information gap
When talking with families, healthcare providers may also leave people with emotional struggles and mis-
should use lay (non-technical) language and take the understandings, which induce them to take unnecessary
families’ views into consideration; otherwise, the latter risks [34]. Patients will adjust their expectations for their
may feel powerless and vulnerable [40]. recovery based on the information received [42].
A better understanding by healthcare providers of pa-
tients’ experiences may further improve their capacity to
Context address questions that patients do not know enough to
Many studies on discharge planning, including literature ask, which increases the likelihood that the information
reviews, maintain that communication between health- patients receive is accurate and applicable to their specific
care providers and families is important throughout the condition [42, 44], and ensures appropriate and complete
discharge planning process, upon admission of patients discharge instructions [41] and transitions [36].
to hospital [40] or within the next 24 to 48 h at most
[38], and should be frequent [36]. A discussion on ex- Outcomes
pected versus realistic recovery time and how to manage All the mechanisms discussed above, triggered by better
risk should take place before the discharge home [34, communication between healthcare providers and fam-
42]. The most effective communication interventions ilies, ultimately improve patient satisfaction [42], recov-
started at an early stage and continued during the hos- ery, functional status and independence [34, 41]. A
pital stay and post-discharge phase [38]. According to negative gap between expectations and reality results in
some studies, the biggest communication gap occurs patient dissatisfaction and disengagement [42]. In hip
during the transition from hospital to home [34, 40]. fracture studies, most patients were not satisfied withProvencher et al. BMC Geriatrics (2021) 21:84 Page 10 of 18
Fig. 4 ICMO-2: Interprofessional communication within and across healthcare settings
the information from healthcare providers regarding healthcare specialties and complex recoveries require
their surgery, the recovery process or their own progress various care settings; this means that the accuracy and
[42]. Patients were dissatisfied because they took longer effectiveness of information sharing between different
to recover than expected, they were not informed about healthcare providers are of the utmost importance [9,
which activities could help their recovery or the occur- 36, 38–40, 45, 46]. In practice, however, this interprofes-
rence of unexpected post-operative complications, and sional communication is often lacking or interrupted
they did not recover as well as expected [42]. In a review [40, 46], especially between hospital and community
of discharge planning, Bauer et al. [38] noted that care- healthcare providers [38, 40].
givers’ greater involvement in care planning (fostered by A standardized routine for exchanging information is
good communication) contributed to greater satisfaction advocated [9, 47], and a variety of communication chan-
with the process. nels are required (structured and unstructured, formal
and informal). Multidisciplinary meetings should be
ICMO-2: Interprofessional communication within and held on a regular basis (which varies between differ-
across healthcare settings ent settings and according to foreseeable length of
Key findings stay) to discuss treatment goals, the patient’s progress
ICMO-2 (Fig. 4) can be summarized as follows: interpro- and discharge plan, and to standardize interprofes-
fessional communication and information sharing within sional communication [9, 43, 47]. Accurate and
and across different healthcare settings through both complete standardized handovers documenting fall
standardized and unofficial information exchange (I), if risk would improve the quality of the transfer of in-
supported by a favorable organizational and manage- formation [36, 46, 47], which could be measured by
ment context (C), trigger an improvement in healthcare the ISBAR (Identify, Situation, Background, Assess-
providers’ knowledge and understanding of the patient’s ment and Recommendation) quality score (/5) [47].
situation and their respective roles and responsibilities, However, patient handover documents or discharge
and less redundancies, delays and loss of information in summaries are often absent, incomplete or inaccurate,
patient handovers (M), which enhance the quality of which leads to a communication gap between differ-
care and identification of patients at risk of falls, and de- ent healthcare settings or between acute and commu-
creases the risk of hospital readmission (O). nity healthcare providers [38, 40, 46].
It is practical to use a Web-based information system
Intervention components (or electronic health record) to facilitate exchanges re-
In addition to communication with families, it is crucial garding key patient information during handovers [9, 35,
to promote interprofessional communication and infor- 39], as long as it is interoperable across care settings and
mation sharing regarding the patient’s health status, care available to all healthcare providers throughout the con-
provided and care planning throughout the healthcare tinuum of care [39]. Clear boundaries pertaining to the
continuum and between different healthcare settings. As roles and responsibilities of each provider of patient care
most hospitalized older patients have comorbidities, must be established among all healthcare providers, as
multiple concurrent diseases are addressed by numerous they are often an area of misunderstanding [35, 40]. ForProvencher et al. BMC Geriatrics (2021) 21:84 Page 11 of 18
example, in their review, Carroll and Dowling [40] re- about patients’ health condition, medical history and
ported that in two hospitals, the majority of nurses did medication [9].
not complete the discharge plan as they thought it was
the case manager’s responsibility to do so. When inter- Outcomes
viewing healthcare providers involved in care transitions Healthcare providers’ greater knowledge and under-
of older patients hospitalized for hip fracture, Toscan standing of the patient’s situation and of what has been
et al. [35] found that these professionals could not done by their counterparts in other fields, resulting from
clearly describe the limits of their own responsibilities in appropriate interprofessional communication, will im-
the patient discharge care plan, nor those of other pro- prove the quality of transitional care received by older
fessionals within and across different care settings. adults hospitalized following a fall [9, 35, 39] and de-
Verbal and timely informal communication between crease their risk of further hospitalization [9, 36]. Con-
healthcare providers is also important throughout the versely, unnecessary hospitalizations and increased
process [9]. mortality and dependency are outcomes that result from
a paucity of communication between healthcare pro-
Context viders [53]. It has been found that standardized commu-
Interprofessional communication should take place in a nication between healthcare providers and improved
favorable organizational and management context. It is quality of discharge information led to better identifica-
difficult for healthcare providers to change their fall pre- tion of older patients at risk of falls [47].
vention practices if the organization and the healthcare
system (government and policymakers) do not support ICMO-3: patient/caregiver individually tailored education
their efforts to communicate better [43, 47]. Optimized on fall prevention
communication between different healthcare providers Key findings
can only be achieved when there is strong, early engage- The third ICMO (Fig. 5) can be outlined as follows: pro-
ment at the local and national organizational levels [47]. viding older adults and their families with targeted fall
However, healthcare providers have reported that they prevention education and teaching, reinforcing and mo-
often feel they are the only ones making an effort to tivating patients to use these prevention strategies (I),
change practices [47]. when done before discharge (C), triggers an improved
awareness regarding fall prevention, recognition of near-
Mechanisms falls more easily and knowledge of and motivation to use
Optimized interprofessional communication and infor- prevention strategies (M), which will reduce the risk of
mation exchange increase healthcare team members’ falls post-discharge and negative psychological impacts
knowledge and understanding of the patient’s situ- on caregivers, and ensure a better transition from hos-
ation and their respective tasks, roles and responsibil- pital to home for patients (O).
ities (“who does what”) [9, 35, 46]. It is widely
recognized that poor interprofessional communication Intervention components
generates redundancies, overlaps, delays, inaccuracies, Next to communication, education encompasses another
incompleteness, uncertainties regarding what has been important group of intervention components used to
done versus what has to be done [35], and losses of optimize discharge planning for hospitalized older
information during transitions across care settings adults. These intervention strategies mainly involve fall
[39], which leaves healthcare providers feeling anxious prevention education tailored to the older adult [37, 48,
and frustrated. Using an appropriate information sys- 49]. For example, advocating a behavior change model
tem reduces the time spent gathering information of education, Hill et al. [48] reported positive outcomes
Fig. 5 ICMO-3: Patient/caregiver individually tailored education on fall preventionProvencher et al. BMC Geriatrics (2021) 21:84 Page 12 of 18
with an intervention comprising an initial training ses- education interventions for patients and caregivers
sion (during which a video was viewed and written ma- should take place at the hospital, prior to discharge [37,
terial was given to the patient) followed by individual 48, 49]. One such intervention includes a follow-up call
tailored in-person discussion sessions. In these individ- two weeks post-discharge to reinforce the education pre-
ual sessions, the patient could discuss issues with the viously provided at the hospital [48].
educator, and a phone call 2 weeks post-discharge rein-
forced what was learned. This intervention educated pa-
Mechanisms
tients on fall prevention strategies as well as barriers and
Education on fall prevention raises awareness in older
facilitators to using these strategies, fostered patients’ be-
people and their families [37] and contributes to a better
lief that they could use these strategies successfully, and
recognition of near-falls, which is well known to be critical
provided cues for action. In their study, Sims-Gould
for preventing falls [49]. For patients, education gives
et al. [42] noted that it was important for healthcare pro-
them greater knowledge, confidence and motivation to en-
viders to not only teach patients how to do the exercises
gage in fall prevention strategies [42, 48]. For caregivers,
but also motivate them not to abandon their exercise
greater knowledge of the illness/injury helps them take
program [42].
care of patients with more resilience, i.e. perform their
Different tools are used to assess and raise hospitalized
caregiving role with increased flexibility rather than a rigid
patients’ awareness of the risk of falling. One study used
mindset [37] and with more proficiency [38]. Caregivers,
home floor plans drawn by patients, combined with indi-
on the other hand, often mentioned that they were not
vidual interviews with them, to identify potential fall
prepared for “post-hospitalization” [37] and this feeling of
hazards at home and develop a tailored education pro-
being unprepared made them anxious and frustrated [38].
gram targeting home and behavior modifications (e.g. re-
ducing clutter, wearing appropriate footwear, adequate
lighting) [49]. Outcomes
Some authors agree that healthcare providers should By raising awareness and better recognition of near-falls,
also provide caregivers with fall prevention [37, 38, 49] targeted fall prevention education for older adults and
and health education [37]. As this is not always done, their families reduces the risk of falls [48, 49]. For ex-
caregivers stress their need for more education concern- ample, participants in an intervention group (education
ing the patient’s medical condition and prognosis, signs on fall prevention strategies including a training video,
of complications, physical care requirements, medica- written material and individual in-person discussions be-
tions, and other specific care demands [38]. fore discharge and follow-up phone call post-discharge)
lowered their rate of falls to 5.4/1000 patients during the
Context month post-discharge compared to 18.7 for the control
Several studies have been conducted with cognitively in- group [48]. These participants were also more likely to
tact patients [42, 48, 49]. However, with cognitively im- plan how to resume to functional activities safely and to
paired patients, educational material and strategies complete other targeted behaviors such as their home
should be adapted and caregivers’ input be included in exercise program [48].
the education process so that they can both acquire Educating caregivers reportedly leads to greater safety
skills regarding how to handle daily impacts of major in the care they provide to their family members at
neurocognitive disorders [38]. Most authors agree that home [37], less negative psychological impact on
Fig. 6 ICMO-4: Discharge planning coordinationProvencher et al. BMC Geriatrics (2021) 21:84 Page 13 of 18
themselves and more continuity in patients’ transition Context
from hospital to home [38]. Many studies agree that integration and coordination of
healthcare should take place throughout the process,
ICMO-4: discharge planning coordination from patient admission to discharge home [35, 36, 40,
Key findings 51], and during the follow-up process [36]. However, in
The last ICMO (Fig. 6) is related to coordination and in- many healthcare systems, providers still lack the time
tegration of healthcare services and can be synthesized and resources to coordinate the care and discharge of
as follows: the designation of a coordinator (pivotal older patients effectively [35, 53].
healthcare provider) to manage patient care and act as Because of multiple comorbidities and medical com-
the single contact point for the patient (I), throughout plexities, older patients require more extensive healthcare
the continuum of care and, more importantly, for pa- coordination because of the larger number of profes-
tients with comorbidities who have a large number of sionals working with them [35, 36, 41, 50, 53]. For ex-
health professionals working with them (C), triggers en- ample, patients with a hip fracture need surgical, geriatric,
hanced staff stability and consistency of the information rehabilitation and psychosocial services to be integrated
provided, trusting relationship between patients, families [36]. When a patient transitions from one healthcare set-
and professionals, and communication, information ting to another, the healthcare teams responsible for dis-
sharing and identification of patient needs (M), which charge are often not the same [35], which poses a
improves patient satisfaction and the continuity of care challenge when trying to coordinate services.
and reduces the risk of hospital readmission and func-
tional decline of the patient (O). Mechanisms
Staff stability and consistency of the information pro-
Intervention components vided in the healthcare delivered are reinforced when
Communication and education strategies cannot achieve the coordinator provides a single regular contact point
their goal if they are not well integrated and coordinated for patients, families and professionals [35, 39]. Relation-
[40, 50, 53]; in fact, they are crucial components of inte- ships of trust are established between team members,
grated and coordinated healthcare services [35, 50]. external providers, patients and families [39]. Coordin-
One key component of a coordinated system is the ation and integration help healthcare providers to iden-
designation of a pivotal healthcare provider to manage tify, anticipate and alleviate barriers experienced by
the care to be provided to older adults hospitalized fol- patients [35, 36] and help the multidisciplinary team to
lowing a fall [35, 38, 39]. This designated healthcare pro- make a more appropriate use of resources [53]. Inte-
vider can act as the single contact point for patients grated information systems would improve communica-
[35], coordinate comprehensive and customized inter- tion and information sharing between healthcare
ventions for this frail population [50], and address the providers and healthcare settings [52]. Without integra-
needs of families with input from a multidisciplinary tion and coordination, the size of the healthcare team
team [38]. A systematic review of the literature on osteo- may grow with the complexity of older patients’ medical
porosis care in orthopedic environments revealed that needs and lessen the personal engagement of each
65% of the healthcare systems analyzed included a dedi- healthcare provider and the family in providing care
cated coordinator who acted as the link between the [35]. A lack of integration and coordination of health-
orthopedic team, osteoporosis and fall services, the pa- care may also lead to poor communication between
tient and the primary care physician [50]. The assigned healthcare providers, and less awareness and inappropri-
coordinator may be called a system coordinator [35], ate prioritization of patients’ needs [53].
discharge coordinator [38] or case manager [39, 50].
Different tools are used to optimize the coordination Outcomes
of transitional care. For example, Dedhia et al. [51] used By reinforcing the stability of staff and consistency of the
an interdisciplinary worksheet to record all the barriers information provided in the delivery of care, the coord-
to the patient’s safe return home identified by each of ination and integration of healthcare services for older
the different professionals part of the Safe STEPS (Safe adults hospitalized after a fall enhance the quality and
and Successful Transition of Elderly Patients Study) Inter- continuity of care provided to patients [35, 39, 52, 53].
vention Program. In addition to facilitating communica- According to Khatib et al. [53], if patient needs are not
tion between healthcare providers, an information system properly identified and prioritized, the healthcare pro-
or electronic medical records would also help to achieve vided will be fragmented and of lower quality. Quality
integration of patient information from different health- healthcare contributes to a better quality of life for pa-
care providers and settings [35, 50, 52] but this remains a tients as their physical, psychological and social needs
challenge for many healthcare systems [52]. will be met [53].Provencher et al. BMC Geriatrics (2021) 21:84 Page 14 of 18
Using an interdisciplinary team worksheet coordinated their presence may not always be helpful: 13% of older
by a case manager skilled in discharge planning, Dedhia adults who received assistance with one or more activity
et al. [51] found an increase in the proportion of patients of daily living reported that this aid was only somewhat
with high-quality transitions home (patient satisfaction or not at all reliable [57]. Patients and caregivers may
measured by Coleman’s Care Transition Measures) from not share the same opinion regarding which treatment
68% before the intervention to 89% after, and a lower option is best and thus be inclined to make different de-
rate of readmission (22 to 14%). cisions [58]. Family involvement in planning care is
often valued but healthcare providers must be vigilant
Discussion regarding potentially problematic situations [58].
This realist synthesis sheds light on contexts and under-
lying mechanisms of the outcomes of intervention com- ICMO-2: Interprofessional communication within and
ponents aimed at optimizing discharge planning for across healthcare settings
older adults (65+) hospitalized following a fall. Four Since discharge information from one care setting be-
ICMOs were developed and grouped into three highly comes admission information for another [39], a key
interrelated domains of discharge planning: communica- element of interprofessional communication is to make
tion, education and coordination. sure that the shared information is understood correctly
by the recipient. Mansah [59] highlights the importance
ICMO-1: two-way communication between healthcare of communication in care transitions for the older adults
providers and patients/caregivers and discusses the theory of “planned communication”,
The first ICMO emphasizes the importance of not only which takes into consideration the receiver of the mes-
informing families but also involving them in care and sage during the transition.
discharge planning. In this patient-centered approach, Defining clear boundaries for the roles and responsi-
making joint decisions with families is often suggested. bilities of the different healthcare providers involved in
Healthcare providers should offer possible options, not discharge planning for older adults has been targeted as
impose a decision. A balance should be achieved be- an important step in optimizing interprofessional com-
tween informing and deciding with families without dis- munication [9, 35, 40, 46]. Clarifying roles so that they
empowering them. Offering patient-adapted options to are complementary is important but challenging. Dupli-
guide informed decision-making is relevant but may be cation of some interventions at different times and in
ethically difficult to do. Communication should be a various settings can be beneficial if done at the right
two-way street as healthcare providers should give time and in the right context to prevent service gaps.
enough information to foster dialogue with patients and However, a flexible approach is needed to keep in mind
caregivers. Because it would be relevant to have families what is best for the patient.
generate answers by themselves and target interventions
acceptable to them, it is important for healthcare pro- ICMO-3: patient/caregiver individually tailored education
viders to offer options. However, the literature does not on fall prevention
shed any light on exactly how to operationalize families’ While some hospitalized patients fear falling when thinking
integration in making decisions about discharge plan- about their discharge home [34, 36, 37, 47, 60], many older
ning. Authors agree that communication should begin adults do not worry about it (believing that fall prevention
upon patient admission but more research is needed to is for others), even if they were hospitalized following a fall
determine specifically what should be said (information [61]. According to Meyer et al. [61], fall prevention is not a
to provide and questions to ask to elicit informative an- priority for older patients admitted to hospital after a fall if
swers from families) and when, as patients’ perceptions they have another acute medical condition, which becomes
and needs can change depending on when the informa- the priority for them. These situations pose a challenge as
tion is shared [54, 55]. they increase the difficulty of making evidence-based fall
Family members play a central role in communication prevention strategies relevant and a priority for older adults
as they provide information about the patient’s health, [61]. It is crucial to educate patients on the possible severity
habits and values, ask for appropriate health services and of the consequences (including death) of a possible fall,
support the patient with self-care [9, 39]. However, some while highlighting what can be done to minimize the conse-
may feel burdened and pressured to take on extensive quences, with few changes in their daily lives.
responsibility for the patient [9]. As argued by Funk The theory of planned communication [59] can also
[56], to prevent family members from feeling that the be applied to education since the way information is
whole burden lies on their shoulders, they should be taught and the content of the message should be
supported during the transition and provided with tools adapted to the recipients’ characteristics or specific
to navigate in the system. Despite relatives’ essential role, needs. An example of adaptation is using pictogramsYou can also read