Two new inflammatory markers related to the CURB-65 score for disease severity in patients with community-acquired pneumonia: The hypersensitive ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Open Life Sciences 2021; 16: 84–91
Research Article
Bing Luo, Minjie Sun, Xingxing Huo, Yun Wang*
Two new inflammatory markers related to the CURB-65 score
for disease severity in patients with community-acquired
pneumonia: The hypersensitive C-reactive protein to albumin
ratio and fibrinogen to albumin ratio
https://doi.org/10.1515/biol-2021-0011 Keywords: community-acquired pneumonia, hypersen-
received October 16, 2020; accepted November 26, 2020 sitive C-reactive protein to albumin ratio, fibrinogen to
Abstract albumin ratio, CURB-65
Background ‒ The objective of this study was to inves-
tigate the relationship among hypersensitive C-reactive
protein to albumin ratio (CAR), fibrinogen to albumin ratio
(FAR), and the CURB-65 score for community-acquired 1 Introduction
pneumonia (CAP) severity.
Methods ‒ Clinical data and laboratory indicators of 82 Without timely and effective treatment, patients with
patients with CAP and 40 healthy subjects were retro- community-acquired pneumonia (CAP) are at an increased
spectively analysed. The relationship among CAR, FAR, risk for severe CAP, which may cause serious complica-
and the severity of CAP was then analysed. tions, significantly affecting patients' the quality of life and
Results ‒ CAR and FAR in patients with low-risk CAP even put their lives in danger [1]. Therefore, the ability to
were significantly higher than those in the normal control evaluate the severity of CAP and provide reasonable treat-
group (P < 0.05). CAR and FAR in patients with medium– ment is clinically significant. Most commonly, the CAP
high-risk CAP were further increased compared with those severity index scoring system has been used to assess
in patients with low-risk CAP (P < 0.05). CAR and FAR whether patients with CAP can be treated as outpatients
were positively correlated with hypersensitive C-reactive or inpatients [2], but the CURB-65 scoring system is also an
protein, neutrophil to lymphocyte ratio (NLR), platelet to important tool used to predict the severity of CAP [3].
lymphocyte ratio (PLR), and CURB-65 scores (P < 0.05). In However, these scoring systems require substantial time
the receiver operating characteristic curve for predicting and effort to collect multiple sets of patient data. There-
severe CAP, the area under the curve of combining four fore, various biomarkers have been studied to assess the
biomarkers (CAR + FAR + NLR + PLR) was the largest. CAR severity of CAP. Presently, the neutrophil to lymphocyte
was also an independent risk factor for severe CAP (OR = ratio (NLR), platelet to lymphocyte ratio (PLR), hypersen-
8.789, 95% CI: 1.543–50.064, P = 0.014). sitive C-reactive protein (hs-CRP), and fibrinogen (FIB)
Conclusions ‒ CAR and FAR may be used as the inflam- are the primary inflammation markers that have been
matory markers for CAP severity evaluation. studied in patients with CAP; of those, the NLR has
been shown to be an important marker of disease prog-
nosis and risk stratification in patients with CAP [4,5],
whereas NLR and PLR have also been shown to be
related to the severity of CAP [6]. However, the area
* Corresponding author: Yun Wang, Department of Hospital
under the curve (AUC) of the receiver operating character-
Infection Management, Anhui No. 2 Provincial People’s Hospital,
1868 Dangshan Road, Hefei, Anhui 230041, China, istic (ROC) curve of a single indicator that predicted severe
e-mail: ahs2y2008@126.com CAP was relatively small, and thus the combined evaluation
Bing Luo: Department of Clinical Laboratory, Anhui No. 2 Provincial of multiple markers may provide more valuable diagnostic
People’s Hospital, Hefei, Anhui 230041, China information.
Minjie Sun: Department of Operating Room, Anhui No. 2 Provincial
C-reactive protein to albumin ratio (CAR) and fibri-
People’s Hospital, Hefei, Anhui 230041, China
Xingxing Huo: Department of Scientific Research Center,
nogen to albumin ratio (FAR) as the new inflammatory
The Traditional Chinese Medicine Hospital of Anhui province, markers have become useful indicators to predict the sys-
Hefei, Anhui 230020, China temic inflammatory response status. Specifically, CAR has
Open Access. © 2021 Bing Luo et al., published by De Gruyter. This work is licensed under the Creative Commons Attribution 4.0 International
License.Two markers related to the CURB-65 score for disease severity in patients with CAP 85
been widely used to evaluate the post operative survival 2.2 CAP severity index
rate of patients with pancreatic ductal adenocarcinoma,
the prognosis of survival and recurrence in patients with The CURB-65 score, which is an important tool used
oesophageal cancer, the activity of rheumatoid arthritis, to predict the severity of CAP, assigns different scores
and the severity of coronary heart disease [7–10]. Another to patients according to disturbance in consciousness,
new inflammatory marker, FAR, has shown utility in the blood urea nitrogen level, respiratory frequency, blood
evaluation of gastrointestinal stromal tumours, prognosis pressure, and patient age. The CURB-65 score was used
of resectable gastric cancer, and assessment of rheumatoid for the classification of CAP severity. The total score
arthritis activity [9,11,12]. Moreover, both CAR and FAR have ranges from 0 to 5: CURB-65 scores greater than or equal
been shown to be correlated with the activity level of to 0 and less than or equal to 1 indicate low risk; scores
rheumatoid arthritis [9]. However, the application of CAR equal to 2 indicate medium risk; scores greater than or
and FAR in the assessment of CAP severity has not been equal to 3 and less than or equal to 5 indicate high risk
reported in the literature. [3]. The CURB-65 score was used to assess the severity of
We assume that CAR and FAR might be two impor- CAP at the time of admission, after which the patients
tant markers that can be used to evaluate the severity of were divided into two groups based on the CURB-65
CAP. Therefore, this study intends to explore whether score: the low-risk CAP group included 42 patients with
CAR and FAR are associated with CAP's severity and com- CURB-65 scores greater than or equal to 0 and less than or
pare them with other known markers. equal to 1; the medium–high-risk CAP group included 40
patients with CURB-65 scores greater than or equal to 2
and less than or equal to 5.
2 Materials and methods
2.3 Clinical evaluation and laboratory data
2.1 Subjects
Clinical evaluation and laboratory data of all patients
A total of 82 patients with CAP who presented at Anhui included age, sex, leukocyte count (WBC), neutrophil
No. 2 Provincial People’s Hospital from January 2018 (N) count, lymphocyte (L) count, platelet (PLT) count,
to April 2019 were classified as the CAP group and D–dimer (D–D), hypersensitive C-reactive protein (hs-CRP),
were enrolled in this retrospective study. All patients albumin (ALB), and FIB. All patients fasted overnight
with CAP were diagnosed according to the American for 8–10 h after admission. Whole blood was collected
Thoracic Society/Infectious Disease Society of America's in the morning for testing according to the requirements
(2019) diagnostic standard [13]. The following patients of various test indicators. All operations were completed
were excluded from the study: patients who received other within 2 h in strict accordance with the standard oper-
treatment for 3 months, patients with CAP complicated by ating procedures of the instrument and the requirements
malignant tumours, other chronic diseases, infection or specified in the reagent manual (Sysmex automatic coa-
inflammatory diseases, systemic autoimmune diseases, and gulation analyser CS-5100, Japan; Sysmex automatic
cardiovascular and metabolic diseases. The normal con- blood cell analyser XN-1001, Japan; Hitachi automatic
trol group was composed of 40 healthy subjects matched biochemical analyser 008AS, Japan). CAR, FAR, NLR,
by age and sex in the physical examination centre. and PLR were calculated according to the results of indi-
vidual items.
Informed consent: Informed consent has been obtained
from all individuals included in this study.
Ethical approval: The research related to human use has 2.4 Statistical analysis
been complied with all the relevant national regulations,
institutional policies, and in accordance with the tenets SPSS21.0 (Version 21.0, Chicago, IL, USA) and MedCalc15.2.2
of the Helsinki Declaration and has been approved by the were used for the statistical analysis, the measurement data
ethics committee of Anhui No. 2 Provincial People’s were described by the mean (SD), and gender was shown as
Hospital (No. 2017-05). male (female). The Kolmogorov–Smirnov test was used to86 Bing Luo et al.
verify data normality, the chi-square test was used for 3.2 Clinical data and laboratory results of
counting data, independent sample t-test or one-way three groups of subjects
ANOVA was used for measurement data, and Pearson cor-
relation analysis was used for linear correlation analysis. The clinical data and laboratory results of 42 patients
Spearman correlation was used for rank correlation analysis. with low-risk CAP, 40 patients with medium–high-risk
The CURB-65 binary model (CURB-65 ≦ 1 and CURB-65 ≧ 2) CAP, and 40 healthy subjects were evaluated, and the
was used to analyse the relationship between laboratory results are presented in Table 2. Significant differences
parameters and CAP severity by logistic regression. The were observed in the results of all parameters among the
statistical level was set at 0.05. three groups except sex (P = 0.767) and age (P = 0.199).
The NLR, PLR, D–D, hs-CRP, CAR, FIB, and FAR were all
elevated in patients with low-risk CAP and medium–high-
risk CAP, whereas PLT, L, and ALB were decreased, and
WBC and N were significantly increased in patients with
3 Results medium–high-risk CAP compared with the normal control
group. In addition, the differences in WBC, N, L, NLR, PLR,
3.1 Clinical data and laboratory results of D–D, hs-CRP, CAR, FAR, and ALB were statistically signifi-
study groups cant between the low-risk CAP group and medium–high-
risk CAP group (P < 0.05) (Table 2).
The hospital records of 82 patients with CAP and 40
gender- and age-matched healthy control subjects were
assessed. The clinical data and laboratory results of the
3.3 ROC curve of NLR, PLR, CAR, FAR, and
two groups of subjects are presented in Table 1. Signifi-
cant differences were observed in 14 parameters between combining four biomarkers (CAR + FAR +
the two groups but not gender (P = 0.585) and age (P = NLR + PLR) for predicting severity in
0.239). Patients with CAP had elevated levels of WBC, N, patients with CAP
NLR, PLR, D–D, hs-CRP, CAR, FIB, and FAR, whereas
their levels of L, PLT, and ALB tended to be decreased The prediction efficacy of NLR, PLR, CAR, FAR, and com-
(Table 1). bining four biomarkers (CAR + FAR + NLR + PLR) for
Table 1: Clinical data and laboratory results of study groups, mean (SD)
Parameters Control group (N = 40) CAP group (N = 82) t/χ2 P-value
Gender: male (female) 25 (15) 47 (35) 0.299 0.585
Age: year, mean (SD) 75.93 (8.69) 78.00 (9.29) 1.183 0.239
WBC (109 L−1) 6.51 (1.69) 8.83 (4.69) 3.988Two markers related to the CURB-65 score for disease severity in patients with CAP 87
Table 2: Clinical data and laboratory results of three groups of subjects, mean (SD)
Parameters Control group Low-risk CAP group Medium–high-risk CAP F/χ2 P-value
(N = 40) (N = 42) group (N = 40)
Gender: male (female) 25 (15) 23 (19) 24 (16) 0.531 0.767
Age: year, mean (SD) 75.93 (8.69) 76.67 (7.97) 79.40 (10.42) 1.099 0.199
WBC (109 L−1) 6.51 (1.69) 7.35 (4.10) 10.38 (4.81)*# 11.65788 Bing Luo et al.
Table 3: AUC analysis results of ROC curve of NLR, PLR, CAR, and a collinearity problem between hs-CRP and CAR with
FAR for predicting severe in patients with CAP variance inflation factor equal to 12.511, and thus hs-CRP
was excluded from the regression model. The updated
Laboratory AUC Standard P-value 95% CI results are presented in Table 6. Multivariate logistic
indicators error
regression analysis showed that high CAR was an inde-
NLR 0.786 0.051Two markers related to the CURB-65 score for disease severity in patients with CAP 89
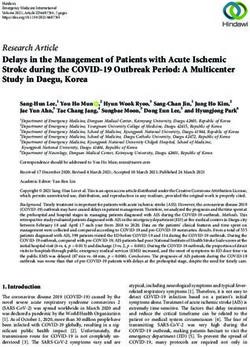
Figure 2: Correlation analysis of CAR with NLR, PLR, and hs-CRP in patients with CAP, CAR, and NLR (a); CAR and PLR (b); and CAR and
hs-CRP (c).
patients with CAP are consumed in the anti-infection Table 6: Multivariate logistic regression analysis of risk factors for
immunity response [16]. Therefore, NLR and PLR are con- severe CAP
sidered to be representative of the inflammatory status
[17,18]. It has been reported that NLR and PLR may be Index B Wald χ2 OR OR 95% CI P-value
alternative markers of CAP-related inflammation [19–21]. WBC −1.067 1.188 0.344 0.051–2.343 0.344
Moreover, NLR and PLR have been shown to be predictors (109 L−1)
of CAP severity [6]. As shown in this study, NLR and PLR N (109 L−1) 1.067 1.056 2.906 0.380–22.233 0.304
L (109 L−1) 1.538 1.284 4.653 0.326–66.481 0.257
are positively correlated with the CURB-65 score and can
D–D 0.092 3.712 1.096 0.998–1.203 0.054
distinguish the severity of CAP, which is consistent with
(mg L−1)
what is reported in the literature. Therefore, NLR and PLR ALB (g L−1) 0.094 0.958 1.098 0.910–1.324 0.328
may be potential predictors of the CAP's severity. NLR 0.087 0.778 1.091 0.899–1.324 0.378
CAR is the ratio of hs-CRP to ALB, and both hs-CRP PLR 0.000 0.004 1.000 0.993–1.007 0.949
and ALB are associated with inflammation. hs-CRP belongs CAR 2.173 5.995 8.789 1.543–50.064 0.014
(mg g−1)
to the acute phase reaction protein response, which is
FAR −0.004 0.199 0.996 0.979–1.013 0.655
increased in inflammatory conditions [22]. At the same (mg g−1)
time, inflammation can reduce plasma albumin synth-
esis, resulting in hypoalbuminaemia [9], and thus CAR
is a more sensitive predictor of inflammatory status. CAR are elevated in patients with CAP and that a significant
has been widely used in the evaluation of the post opera- increase in the levels of CAR is observed in patients with
tive survival rate of pancreatic ductal adenocarcinoma medium–high-risk CAP compared with patients with low-
patients, the prognosis of colorectal cancer patients after risk CAP. At the same time, CAR was positively correlated
surgery, the activity of rheumatoid arthritis, and coronary with NLR, PLR, hs-CRP, and the CURB-65 score, and CAR
heart disease severity [7–10]. However, thus far, nothing was an independent risk factor for severe CAP compared
has been published on the relationship between CAR and with the NLR and PLR. This study suggests that CAR may
the severity of CAP. To the best of our knowledge, this be an inflammatory parameter and a potential predictor
is the first clinical study that has shown that CAR levels of CAP severity.
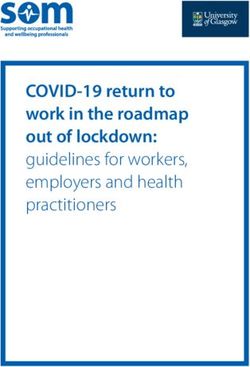
Figure 3: Correlation analysis of FAR with NLR, PLR, and hs-CRP in patients with CAP, FAR, and NLR (a); FAR and PLR (b); and FAR and
hs-CRP (c).90 Bing Luo et al.
Similar to CAR and FAR (ratio of FIB to ALB), FIB Data availability statement: The datasets generated
is also involved in the acute phase reaction protein during and/or analysed during the current study are
response, which is increased in inflammatory conditions available from the corresponding author on reasonable
[23], and inflammatory conditions will reduce the serum request.
albumin levels [9]. In addition, FIB and ALB are asso-
ciated with CAP [24,25], and these findings have aroused
our interest in combining FIB and ALB as a new potential
indicator and exploring its relationship with the severity References
of CAP. In this study, we found a significant increase
in the FAR in patients with CAP, whereas the FAR in [1] Lanks CW, Musani AI, Hsia DW. Community-acquired pneu-
patients with medium–high-risk CAP was further increased monia and hospital-acquired pneumonia. Med Clin North Am.
compared with patients with low-risk CAP. However, 2019;103(3):487–501.
no statistically significant difference was found in FIB [2] Sparham S, Charles PG. Controversies in diagnosis and
management of community-acquired pneumonia. Med J Aust.
between the low- and medium–high-risk CAP group.
2017;206(7):316–9.
Therefore, FAR is superior to FIB in predicting the sever- [3] Mikolajewska A, Witzenrath M. Ambulant erworbene
ity of CAP, and FAR was positively correlated with NLR, Pneumonie bei Erwachsenen [community-acquired pneumonia
PLR, hs-CRP, and the CURB-65 score; therefore, FAR may in adults]. Dtsch Med Wochenschr. 2020;145(6):359–70.
be an important marker that can be used to assess the [4] Zhang HF, Ge YL, Wang HY, Zhang Q, Li WQ, Chen Y, et al.
Neutrophil-to-lymphocyte ratio improves the accuracy and
severity of CAP.
sensitivity of pneumonia severity index in predicting 30-day
This study has several limitations that should be
mortality of CAP patients. Clin Lab. 2019;65:10.
discussed. The study's first constraint is a limited retro- [5] Ge YL, Zhang HF, Zhang Q, Zhu XY, Liu CH, Wang N, et al.
spective case-control study with relatively small sample Neutrophil-to-lymphocyte ratio in adult community-acquired
size and possible selection bias. The second limitation is pneumonia patients correlates with unfavorable clinical out-
that other inflammatory markers related to CAP, such as comes. Clin Lab. 2019;65:5.
[6] Lee JH, Song S, Yoon SY, Lim CS, Song JW, Kim HS. Neutrophil
procalcitonin and interleukins, were not evaluated. The
to lymphocyte ratio and platelet to lymphocyte ratio as diag-
third limitation is that we did not evaluate the effect of nostic markers for pneumonia severity. Br J Biomed Sci.
treatment on the FAR, CAR, NLR, and PLR. 2016;73(3):140–2.
In conclusion, the development of novel biomarkers [7] Ikuta S, Aihara T, Yamanaka N. Preoperative C-reactive protein
and the joint assessment of the severity of CAP are to albumin ratio is a predictor of survival after pancreatic
resection for pancreatic ductal adenocarcinoma. Asia Pac J Clin
urgently needed and will provide more diagnostic infor-
Oncol. 2019;15(5):e109–14.
mation. To the best of our knowledge, this is the first
[8] Tamagawa H, Aoyama T, Tamagawa A, Komori K, Maezawa Y,
clinical study to explore the relationship between CAR, Kano K, et al. Influence of the preoperative C-reactive
FAR, and the severity of CAP. A significant increase in protein-to-albumin ratio on survival and recurrence in
CAR and FAR was observed in patients with CAP, com- patients with esophageal cancer. Anticancer Res.
pared with low-risk CAP patients, and CAR and FAR 2020;40(4):2365–71.
[9] Wei-ming Y, Wei-heng Z, Hou-qun Y, Yan-mei X, Jing Z, Qing-
in patients with medium–high-risk CAP were further
hua M, et al. Two new inflammatory markers associated with
increased. Additionally, CAR and FAR were positively disease activity score-28 in patients with rheumatoid arthritis:
correlated with the severity of the CAP CURB-65 score. albumin to fibrinogen ratio and C-reactive protein to albumin
As a result, the CAR and FAR might be two new biomar- ratio. Int Immunopharmacol. 2018;62:293–8.
kers for the evaluation of CAP severity, and because their [10] Çağdaş M, Rencüzoğullari I, Karakoyun S, Karabağ Y, Yesin M,
Artaç I, et al. Assessment of relationship between C-reactive
detection is fast and inexpensive, and they both are easy
protein to albumin ratio and coronary artery disease severity in
to analyze, they are worthy of clinical application.
patients with acute coronary syndrome. Angiology.
2019;70(4):361–8.
Funding: This study was funded by the National Natural [11] Li R, Song S, He X, Shi X, Sun Z, Li Z, et al. Relationship
Science Foundation of China (No. 81803938) and the between fibrinogen to albumin ratio and prognosis of gastro-
Natural Science Key Project Foundation of Anhui intestinal stromal tumors: a retrospective cohort study. Cancer
Manag Res. 2020;12:8643–51.
Province Education Department (No. KJ2019A1099).
[12] Tang S, Lin L, Cheng J, Zhao J, Xuan Q, Shao J, et al. The
prognostic value of preoperative fibrinogen-to-prealbumin
Conflict of interest: The authors state no conflict of ratio and a novel FFC score in patients with resectable gastric
interest. cancer. BMC Cancer. 2020;20(1):382.Two markers related to the CURB-65 score for disease severity in patients with CAP 91
[13] Jackson CD, Burroughs-Ray DC, Summers NA. Clinical guide- recipients with severe community-acquired pneumonia.
line highlights for the hospitalist: 2019 American Thoracic Pathogens. 2020;9(11):E913.
Society/Infectious Disease Society of America update on [20] Kuang ZS, Yang YL, Wei W, Wang JL, Long XY, Li KY, et al.
community-acquired pneumonia. J Hosp Med. 2020 Aug Clinical characteristics and prognosis of community-acquired
19;15(12):743. doi: 10.12788/jhm.3444. Epub ahead of print. pneumonia in autoimmune disease-induced immunocompro-
PMID: 32853142. mised host: a retrospective observational study. World J Emerg
[14] Roussel L, Houle F, Chan C, Yao Y, Bérubé J, Olivenstein R, et al. Med. 2020;11(3):145–51.
IL-17 promotes p38 MAPK-dependent endothelial activation [21] Kartal O, Kartal AT. Value of neutrophil to lymphocyte and
enhancing neutrophil recruitment to sites of inflammation. platelet to lymphocyte ratios in pneumonia. Bratisl Lek Listy.
J Immunol. 2010;184:4531–7. 2017;118:513–6.
[15] Jian-Guo G. Interaction of vascular endothelial cells with [22] Song Y, Liu Y, Zhou Z, Yang W, Zhou Y. The clinical study of
leukocytes, platelets and cancer cells in inflammation, serum hs-CRP, TNF-α, PCT and IL-6 in patients with acute
thrombosis and cancer growth and metastasis. Acta exacerbation of chronic obstructive pulmonary disease. Int J
Pharmacol Sin. 2003;24:1297–300. Clin Exp Med. 2017;10:13550–6.
[16] Fathi N, Rezaei N. Lymphopenia in COVID-19: therapeutic [23] Vitorino de Almeida V, Silva-Herdade A, Calado A, Rosário HS,
opportunities. Cell Biol Int. 2020;44(9):1792–7. Saldanha C. Fibrinogen modulates leukocyte recruitment in
[17] Ruta VM, Man AM, Alexescu TG, Motoc NS, Tarmure S, vivo during the acute inflammatory response. Clin Hemorheol
Ungur RA, et al. Neutrophil-to-lymphocyte ratio and systemic Micro. 2015;59:97–106.
immune-inflammation index-biomarkers in interstitial lung [24] Li TH, Yu HY, Hou WN, Li ZY, Han CF, Wang LH. Evaluation of
disease. Medicina (Kaunas). 2020;56(8):381. variation in coagulation among children with Mycoplasma
[18] Şahin F, Koşar AF, Aslan AF, Yiğitbaş B, Uslu B. Serum bio- pneumoniae pneumonia: a case-control study. J Int Med Res.
markers in patients with stable and acute exacerbation of 2017;45:2110–8.
chronic obstructive pulmonary disease: a comparative study. [25] Chen L, Lu XY, Zhu CQ. Prognostic value of albumin-red
J Med Biochem. 2019;38(4):503–11. cell distribution width score in patients with severe
[19] Qiu Y, Su Y, Tu GW, Ju MJ, He HY, Gu ZY, et al. Neutrophil-to- community-acquired pneumonia. Ann Palliat Med.
lymphocyte ratio predicts mortality in adult renal transplant 2020;9(3):759–65.You can also read