Subsyndromal depressive symptoms in patients with bipolar
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Journal of Affective Disorders 107 (2008) 169 – 174
www.elsevier.com/locate/jad
Brief report
Subsyndromal depressive symptoms in patients with bipolar and
unipolar disorder during clinical remission
E. Vieta a,⁎, J. Sánchez-Moreno b , J. Lahuerta c , S. Zaragoza d
For the EDHIPO Group (Hypomania Detection Study Group)
a
Bipolar Disorder Programme. Institut Clínic de Neurociencies. Hospital Clinic, Universitat de Barcelona, IDIBAPS, REM-TAP, Barcelona, Spain
b
Bipolar Disorder Programme. Red de Enfermedades Mentales REM-TAP, Instituto de Salud Carlos III, Madrid, Spain
c
Neurosciences Area. Medical Department. GlaxoSmithKline S.A. Tres Cantos, Madrid, Spain
d
Neuropsychological Research Organization, PSYNCRO, Barcelona, Spain
Received 24 May 2007; received in revised form 9 August 2007; accepted 10 August 2007
Available online 17 September 2007
Abstract
Background: Subsyndromal depressive symptoms seem to be quite prevalent in mood disorders although very few studies have
assessed them in patients considered to be in remission by clinical and psychometric criteria. This study sought to evaluate the
presence of subsyndromal depressive symptoms in bipolar and unipolar patients in clinical remission.
Methods: One-hundred seventy-six patients with DSM-IV bipolar (62 bipolar I, 58 bipolar II) or unipolar mayor depression (n = 58)
in clinical remission and 60 healthy subjects were assessed using several psychometric instruments including the 17 items
Hamilton Depression Rating Scale (HDRS). To be considered in clinical remission patients assessed with the Clinical Impression
for Bipolar Disorder-Modified (CGI-BP-M) had to be stable for 6 months and scoring 6 or less in the Young Mania Rating Scale
(YMRS) and 8 or less in the HDRS.
Results: Both Unipolar Disorder (UD) and Bipolar Disorder (BD) patients in clinical remission presented statistically significant
higher HRSD scores, than healthy subjects. The HRSD scores were statistically higher in UD patients under remission than in BD
patients. The subsyndromal symptoms more strongly associated with a clinical diagnosis of either UD or BD were Depressed
Mood, Somatic Anxiety, Impact on Work and Activities, Psychic Anxiety, Gastrointestinal and Somatic Symptoms, Retardation
during the Interview and Genital Symptoms.
Conclusion: Subsyndromal depressive symptoms are present in affective disorder patients, both UD and BD, who apparently are in
clinical remission. Remitted unipolar patients may have more residual symptoms than bipolar patients, particularly in items related
to anxiety and somatic complaints.
© 2007 Elsevier B.V. All rights reserved.
Keywords: Bipolar disorder; Subsyndromal depression; Control group; Healthy subjects; Major depression; Detection
1. Introduction
A large number of patients who have suffered acute
mood disorder episodes continue presenting subsyn-
⁎ Corresponding author. dromal symptoms during remission periods of apparent
E-mail address: evieta@clinic.ub.es (E. Vieta). clinical stability (Benazzi, 2002). Several studies have
0165-0327/$ - see front matter © 2007 Elsevier B.V. All rights reserved.
doi:10.1016/j.jad.2007.08.007170 E. Vieta et al. / Journal of Affective Disorders 107 (2008) 169–174
focused on the comorbidity pattern in patients with questions were addressed by comparing baseline clinical
bipolar disorder (BD) during remission periods; among results between three mood disorder patients' groups
BD type I patients, comorbidity with other psychiatric (BDI, BDII and MDD) and healthy controls.
conditions has been reported in 31% of patients of the
studied samples (Vieta et al., 2001a, 2001b); this 2. Methods
comorbidity having a definite relevance in the course
and outcome of bipolar disorder patients. Comorbidity In order to assess subsyndromal depressive symp-
studies on BD type II patients, showed a prevalence of toms in apparently euthymic DSM-IV depressed bipolar
axis I disorders of 35%; suicidal ideation and suicide I, II and unipolar patients, 60 healthy control subjects
attempts are more frequent in patients exhibiting this (CS), 62 bipolar I(BDI), 56 bipolar II(BDII) and 58
comorbidity (Vieta et al., 2000). unipolar patients(UD) in remission were enrolled in the
More specifically, in prospective studies in BD EDHIPO study (Table 1). The baseline cross-sectional
patient samples, comorbid symptoms have been de- of this study results are being used for this analysis.
scribed during remission, these being predominantly To determine the stability of the disease in the first
depressive in about a 45% of the patients (Post et al., study visit, we assessed all the participants using the
2003; Judd et al., 2003, 2002); BD type I patients can Young Mania Rating Scale (YMRS) (Colom et al., 2002),
spend a third of the year suffering from depression when the 17-item Hamilton Depression Rating Scale (HDRS-
they are evaluated with Life Chart Method techniques 17) (Bobes et al., 2003), and the Modified Clinical Global
combined with regular clinical interviews during follow- Impression Scale for Bipolar Disorder (CGI-BP-M)
up. In a recent study involving 759 adult outpatients, (Vieta et al., 2002), all assessments were conducted at
subsyndromal depressive symptoms were associated the same visit. At all participating centres, the interviewers
with functional impairment in several life domains i.e. were senior clinical mood disorder psychiatrists. The
work, home functioning roles and relations with family group of healthy subjects were administered the ques-
and friends (Altshuler et al., 2006). More generally, it has tionnaires following the same procedure as with the
been suggested that BD outpatients during remission groups of patients; for healthy subjects the assessment
show specific clinical features (Perlis et al., 2006). included a comprehensive medical history and a screening
These data seem to suggest an association between for psychiatric disorders.
depression, suicidality and comorbidity in BD. Thus, an Clinical remission was defined as stability of the mood
accurate description and a better definition of disease- disorder in the last 6 months and verified by standard
specific symptoms during remission, could help to im- psychometric techniques for all patients, as a score of 6
prove detection of BD patients presenting with a variety or less on the Young Mania Rating Scale (YMRS) (Colom
of complaints in everyday psychiatric practice. et al., 2002), and a score of 8 or less on the Hamilton rating
Moreover, it has been described that subsyndromal scale for depression (HRSD) (Ramos-Brieva and Cor-
symptoms upon remission have a strong prognostic dero, 1986).This definition of remission has been used
value in mood disorders in general (Fava, 1999), and and validated in several previous studies (Vieta et al.,
may predict relapse into syndromal depression specif- 2001a, 2001b). To be enrolled, patients had to be in
ically in BD (Altshuler et al., 2006). remission for at least 6 months as assessed with the CGI-
Baseline data from the hypomania detection study BP-M (Vieta et al., 2002).
(EDHIPO) (Vieta et al., 2006) to validate into Spanish After informing the participants and obtaining their
BD screening instruments, provide the opportunity to consent, the investigators recorded their sociodemo-
gain a clinically useful insight of the presence and nature graphic and clinical variables, administering the YMRS,
of subsyndromal depressive symptoms in psychiatric HDRS-17 and CGI-BP-M to confirm the stability of the
patients with mood disorders and healthy controls. patient's condition and the absence of psychopathology
The following questions were posed for this post-hoc for healthy subjects.
analysis: 1) How strong is the association between HRSD total scores were compared between the four
subsyndromal depressive symptoms and particular different groups. Also, the presence of specific symptoms
mood disorders including BD and major depression between subject groups, as evaluated by this scale
(MD) diagnosed patients? 2) Are there special features (classified each symptom as either “present” or “absent”),
of subclinical symptoms during clinical remission that was analysed. Likewise, for BD patients, the relationship
would improve detection of BD patients at this stage? between the depressive symptoms observed, i.e. HDRD
3) Is there a relationship between subsyndromal total score, and the most recent type of mood disorder
symptoms and the course duration of BD? These episode suffered by the patient (classified either asE. Vieta et al. / Journal of Affective Disorders 107 (2008) 169–174 171
Table 1
Sociodemographic and clinical characteristics
Variable Total (N = 236) Type I bipolar Type II bipolar Major Control group
disorder disorder depression (n = 60)
(n = 62) (n = 56) (n = 58)
Mean SD Mean SD Mean SD Mean SD Mean SD
Age (years) 43.5 11.9 40.0 12.1 44.1 11.4 50.9 10.4 39.4 10.1
Age of onset (years) a 31.2 12.4 25.0 8.7 28.4 8.9 40.4 13.3 – –
Time of evolution of the disorder (in years) 13.8 10.9 15.4 11.8 15.6 9.9 10.4 10.4 – –
Young Mania Scale 1.0 1.6 1.1 1.6 1.1 1.7 0.7 1.4 0.9 1.6
Hamilton Depression Scale 2.2 2.2 2.2 2.2 2.3 2.4 3.4 2.3 1.2 1.4
N % N % N % N % N %
Gender
Man 80 33.9 28 45.2 17 30.4 14 24.1 21 35
Woman 156 66.1 34 54.8 39 69.6 44 75.9 39 65
Educational level
No education completed 7 2.9 3 4.8 1 1.8 2 3.5 1 1.7
Primary 65 27.8 18 29 14 25.5 25 43.9 8 13.3
Secondary 87 37.2 24 38.7 23 41.8 19 33.3 21 35
University 75 32.1 17 27.4 17 30.9 11 19.3 30 50
Most recent episode a
Single manic episode (296.0×) 12 6.8 12 19.4 – – – – – –
Hypomanic episode (296.40) 9 5.1 9 14.5 – – – – – –
Manic episode (296.4×) 24 13.6 24 38.7 – – – – – –
Mixed episode (296.6×) 3 1.7 3 4.8 – – – – – –
Depressive episode (296.5×) 14 7.9 14 22.6 – – – – – –
Unspecified episode (296.7) 0 0 0 0 – – – – – –
Hypomanic episode 25 14.1 – – 24 42.9 – – – –
Depressive episode 32 18.1 – – 32 57.1 – – – –
Depressive disorder-single episode (296.2×) 19 10.7 – – – – 19 32.8 – –
Depressive disorder-recurring (296.3×) 39 22 – – – – 39 67.2 – –
a
For this variable related to clinical episodes, the descriptives refer to bipolar disorder and major depression groups only.
depressive episode or other type) was investigated. The factors were used to adjust the regression models, duration
relationship between depressive symptoms and the course of illness, polarity of the most recent acute episode (either
of the disease was also analysed. depressive or manic–hypomanic), and gender.
Data related to BD groups, BD type I and BD type II, is
presented as pooled data (BD). We used the Kruskal 3. Results
Wallis non-parametric test to study the differences in the
total HRSD score obtained and the Mann Whitney U test UD patients under clinical remission exhibited the
to study the contrasts. Bonferroni's correction was applied highest HRSD scores with a mean value of 3.4 (± 2.3).
for multiple comparisons. To compare proportions, groups For the rest of the study groups, the HRSD mean scores
were analysed by the chi-square test, or Fisher's test when were 2.2 (±2.3) for the BD group and 1.2 (± 1.4) for the
the former was not possible. The relationship between the CS group. These differences were significant. Patients
subsyndromal symptoms of BD patients and prior episode with UD under remission presented higher HRSD scores
was studied by the biserial correlation coefficient between than the BD patients (p = 0.006) and healthy subjects
the HRSD score and diagnosis of precedent episode, (p b 0.000). Also, compared to healthy subjects, BD
classified either as depressive episode or other, this patients under remission presented higher HRSD scores
comprising hypomanic, manic or mixed episodes). (p = 0.001).
Spearman's correlation coefficient (a non-parametric When considering the presence or absence of each of
test) was used to study the relationship between the individual symptoms evaluated by the HRSD scale,
subsyndromal symptoms i.e. HDRS total score and the it was found that patients with BD, as well as patients
time since onset of disease. Logistic regression models who have suffered from UD, continue to present
were used to test the predictive value of HRSD items in residual depressive symptoms during the remission
relation to diagnosis (BD I, BD II and MD); the following periods (Fig. 1). Indeed, both BD and UD patients in172 E. Vieta et al. / Journal of Affective Disorders 107 (2008) 169–174
remission exhibited symptoms in nearly half of the areas The length of duration of the symptoms was 15.5
assessed by the HRSD scale; in other words, we (±10.9) years in the patients with BD. No relationship was
observed statistically significant differences between observed between the duration of the disorder and the
all three groups in 8 out 17 items. The symptoms more depressive symptoms recorded in the HDRS (r = 0.16961).
strongly associated with a clinical diagnosis of either Multiple logistic regression was used to find which
UD or BD were Depressed Mood, Somatic Anxiety HDRS symptoms were independent predictors of each
(p b 0.0001), Impact on Work and Activities, Psychic patient group (BP-I versus BP-II, BP-II versus MD and
Anxiety, Gastrointestinal and Somatic Symptoms BP-I versus MD). Among the most frequent HDRS
(p b 0.001), Retardation during the Interview and Ge- symptoms (i.e. Depressed Mood, Feelings of Guilt, In-
nital Symptoms (p b 0.05). somnia Early, Insomnia Middle, Insomnia Late, Work and
Furthermore, when comparing the presence or Activities, Retardation, Psychic Anxiety, Somatic Anxiety,
absence of symptoms between the UD and BD groups, Somatic Symptoms) the significant independent predictors
Somatic Anxiety followed by Gastrointestinal Symptoms, in the two out three of models resulted to be Somatic
Depressed Mood and Psychic Anxiety were more Anxiety and Depressed Mood. The logistic regression
commonly found among patients in remission of an UD model that was built with the groups BP-I versus BP-II
episode than in patients with BD. could not find any statistically significant differential item.
On the other hand, Retardation during the Interview The final model for BP-II versus MD, included So-
and Agitation, symptoms usually described to be more matic Anxiety OR = 0.199, 95% CI (0.075 to 0.528),
common in BD than UD patients, were found in our p = 0.0012, showing that the absence of somatic anxiety
study to be present with the same frequency in the two increases 5-folds the probability of a BP-II diagnosis in
patient groups. a cross-sectional design.
Our data shows no relationship between the type of The final model for BP-II versus MD, included both
prior episode suffered by the BD patients and the depres- Depressed Mood OR = 0.265, 95% CI (0.096 to 0.733),
sive symptoms detected in the patient during clinical p = 0.0105 and Somatic Anxiety OR = 0.181 95% CI
stability (r = 0.27005). (0,066 to 0.492), p = 0.0008; showing that the absence
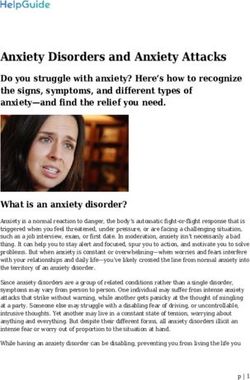
Fig. 1. Number of individuals (%) by group showing symptoms as assessed by the HDRS. aSymptoms are classified as either “present” or “absent”.
Statistically significant differences between all three groups in 8 out 17 items (Depressed Mood, Somatic Anxiety, Impact on Work and Activities,
Psychic Anxiety, Gastrointestinal, Somatic Symptoms, Retardation during the Interview and Genital Symptoms) were observed. As shown in the
figure, certain symptoms are more frequent among MD patients than BD patients during clinical remission: Somatic Anxiety, Gastrointestinal
Symptoms, Depressed Mood and Psychic Anxiety (⁎ p b 0.05, ⁎⁎ p b 0.01, ⁎⁎⁎ p b 0.000). HC, Healthy Control Subjects; BD, Bipolar Disorder
Pateints; MD, Major Depression Patients.E. Vieta et al. / Journal of Affective Disorders 107 (2008) 169–174 173
of Depressed Mood or Somatic Anxiety increase 3.8- knowledge and by contributing to clinician's sensitivity to
folds or 5.5-folds respectively the probability of a BP-I this phenomena. Clinicians should probe for history of
diagnosis in a cross-sectional design. hypomania when symptoms that are highly frequent in
UD patients under remission, like Somatic Anxiety, Gas-
4. Discussion trointestinal, Depressed Mood or Psychic Anxiety, other-
wise are absent in a patient during follow-up visits.
The results of this post-hoc analysis of data from the In conclusion, subsyndromal depressive symptoms
EDHIPO study show that patients with bipolar disorder I are common in patients with mood disorders even in
and II considered to be clinically stable both by clinical those who are apparently well. During clinical remission
impression and after an evaluation with standard psycho- periods, in general, UD patients showed higher scores on
metric instruments, continue in fact to present depressive the depression questionnaires than BP and most residual
symptoms such as Depressed Mood, Somatic Anxiety, symptoms. Specifically, we have noticed certain symp-
Impact on Work and Activities, Psychic Anxiety, Gastro- toms more frequently represented among UD patients
intestinal and Somatic Symptoms, Retardation during the than BD subjects; patients suffering from BD may show
Interview and Genital Symptoms. These, although not as subsyndromal symptoms with a different profile than
severe as during an acute episode, may have an impact on those frequently showed by patients suffering from MD.
both the patient's overall condition and performance in In BP those subsyndromal symptoms seem to be equally
daily functioning, as shown in recent publications present irrespective of the duration of the disease or the
(Altshuler et al., 2006; Martinez-Aran et al., 2007). polarity of the most recent acute episode — either
Although no clear set of subsyndromal symptoms depressive or manic–hypomanic. The persistence of
present in BD patients under remission, different to that of subthreshold depressive symptoms may explain the gap
UD patients, was found, Somatic Anxiety, Gastrointestinal between syndromal recovery and functional recovery.
Symptoms, Depressed Mood and Psychic Anxiety were
more common in the latter, thus providing some clues
Role of funding source
about the possible diagnosis of a patient seen following a This study was funded by GlaxoSmithKline, S.A. Tres Cantos
mood episode. (Madrid), Spain.
During routine follow-up visits, therefore, attention
should be paid to such symptoms, even when the patient is Conflict of interest
apparently clinically stable, in order to minimise their Eduard Vieta, has acted as a consultant, received grants, or been
possible impact on the patient's quality of live and general hired as a speaker by the following companies: Almirall, AstraZeneca,
Bial, Bristol-Myers-Squibb, Eli Lilly, GlaxoSmithKline, Janssen-
functioning. When considering the symptoms of these Cilag, Lundbeck, Merck Sharp & Dohme, Novartis, Organon, Otsuka,
patients, a detailed study of the clinical profile may reveal Pfizer, Sanofi Aventis, Servier, UCB. He has acted as consultant and
some features that may help to establish or confirm a has received grants from the Spanish Ministry of Health, Instituto de
diagnosis. Salud Carlos III, RETICS RD06/0011 (REM-TAP) and from the
In this direction, future research should consider that Stanley Medical Research Institute.
Jose Sanchez-Moreno, none.
our results in the present study are affected by the design, Juan Lahuerta is an employee of GlaxoSmithKline, S.A.
i.e. the proportion of cases with the diagnoses under study Silvia Zaragoza, is an employee of the company contracted by
was established beforehand for research purposes. In our GlaxoSmithKline S.A. to perform the data analysis of the study.
study either MDD patients and healthy subjects are likely
to be underrepresented. We studied groups of patients/ Acknowledgements
healthy subjects of equal size, but rather than this, to have
more precise and epidemiologically meaningful results, The authors thank M. Puig Palma (Psyncro) and M.
the sample sizes should ideally be based on the prevalence Gracia (Psychology Dept. Basic Psychology Area,
figures of each studied condition. Universitat de Girona) for their help in the analysis of
Despite limited effect size, our results are relevant for data and review of manuscript.
the routine clinical practice in psychiatry during ambula-
tory follow-up visits. At specialized clinical settings, References
clinicians should appraise the diagnosis of patients already
identified as UD, when BD is suspected due to either
Altshuler, L.L., Post, R.M., Black, D.O., Keck Jr., P.E., Nolen, W.A.,
clinical course, family history or to clinical symptom Frye, M.A., Suppes, T., Grunze, H., Kupka, R.W., Leverich, G.S.,
profile during remission periods. Our findings aim to be a McElroy, S.L., Walden, J., Mintz, J., 2006. Subsyndromal
contribution towards this appraisal, by increasing the depressive symptoms are associated with functional impairment174 E. Vieta et al. / Journal of Affective Disorders 107 (2008) 169–174 in patients with bipolar disorder: results of a large, multisite study. Perlis, R.H., Brown, E., Baker, R.W., Nierenberg, A.A., 2006. Clinical J. Clin. Psychiatry 67, 1551–1560. features of bipolar depression versus major depressive disorder in Benazzi, F., 2002. Residual depressive symptoms in bipolar depres- large multicenter trials. Am. J. Psychiatry 163, 225–231. sion. Am. J. Psychiatry 159, 882. Post, R.M., Denicoff, K.D., Leverich, G.S., Altshuler, L.L., Frye, M.A., Bobes, J., Bulbena, A., Luque, A., Dal-Re, R., Ballesteros, J., Ibarra, Suppes, T.M., Rush, A.J., Keck Jr., P.E., McElroy, S.L., Luckenbaugh, N., Grupo de Validacion en Español de Escalas Psicometricas, D.A., Pollio, C., Kupka, R., Nolen, W.A., 2003. Morbidity in 258 2003. A comparative psychometric study of the Spanish versions bipolar outpatients followed for 1 year with daily prospective ratings with 6, 17, and 21 items of the Hamilton Depression Rating Scale. on the NIMH life chart method. J. Clin. Psychiatry 64, 680–690. Med. Clin. 120, 693–700 (Barc). Ramos-Brieva, J.A., Cordero, V.A., 1986. Validation of the Castillian Colom, F., Vieta, E., Martinez-Aran, A., Garcia-Garcia, M., Reinares, version of the Hamilton Rating Scale for Depression. Actas Luso-Esp. M., Torrent, C., Goikolea, J.M., Banus, S., Salamero, M., 2002. Neurol. Psiquiatr. Cienc. Afines 14, 324–334. Spanish version of a scale for the assessment of mania: validity and Vieta, E., Colom, F., Martinez-Aran, A., Benabarre, A., Reinares, M., reliability of the Young Mania Rating Scale. Med. Clin. (Barc.) Gasto, C., 2000. Bipolar II disorder and comorbidity. Compr. 119, 366–371. Psychiatry 41, 339–343. Fava, G.A., 1999. Subclinical symptoms in mood disorders: Vieta, E., Colom, F., Corbella, B., Martinez-Aran, A., Reinares, M., pathophysiological and therapeutic implications. Psychol. Med. Benabarre, A., Gasto, C., 2001a. Clinical correlates of psychiatric 29, 47–61. comorbidity in bipolar I patients. Bipolar Disord. 3, 253–258. Judd, L.L., Akiskal, H.S., Schettler, P.J., Endicott, J., Maser, J., Vieta, E., Gasto, C., Colom, F., Reinares, M., Martinez-Aran, A., Solomon, D.A., Leon, A.C., Rice, J.A., Keller, M.B., 2002. The Benabarre, A., Akiskal, H.S., 2001b. Role of risperidone in bipolar long-term natural history of the weekly symptomatic status of II: an open 6-month study. J. Affect. Disord. 67, 213–219. bipolar I disorder. Arch. Gen. Psychiatry 59, 530–537. Vieta, E., Torrent, C., Martínez-Arná, A., Colom, F., Reinares, M., Judd, L.L., Akiskal, H.S., Schettler, P.J., Coryell, W., Endicott, J., Benabarre, A., Comes, M., Goikolea, J.M., 2002. A user-friendly Maser, J.D., Solomon, D.A., Leon, A.C., Keller, M.B., 2003. A scale for the short and long term outcome of bipolar disorder: the prospective investigation of the natural history of the long-term CGI-BP-M. Actas Esp. Psiquiatr. 30, 301–304. weekly symptomatic status of bipolar II disorder. Arch. Gen. Vieta, E., Sanchez-Moreno, J., Bulbena, A., Chamorro, L., Ramos, J.L., Psychiatry 60, 261–269. Artal, J., Perez, F., Oliveras, M.A., Valle, J., Lahuerta, J., Angst, J., for Martinez-Aran, A., Vieta, E., Torrent, C., Sanchez-Moreno, J., the EDHIPO (Hypomania Detection Study) group, 2006. Cross Goikolea, J.M., Salamero, M., Malhi, G.S., Gonzalez-Pinto, A., validation with the mood disorder questionnaire (MDQ) of an in- Daban, C., Alvarez-Grandi, S., Fountoulakis, K., Kaprinis, G., strument for the detection of hypomania in Spanish: the 32 item Tabares-Seisdedos, R., Ayuso-Mateos, J.L., 2007. Functional hypomania symptom check list (HCL-32). outcome in bipolar disorder: the role of clinical and cognitive factors. Bipolar Disord. 9, 103–113.
You can also read