Tricuspid Valve - Where are we? - Miami Valves 2023 - Azeem Latib MD
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Miami Valves 2023
Tricuspid Valve – Where are we?
Azeem Latib MD
Montefiore Medical Center
New York, USA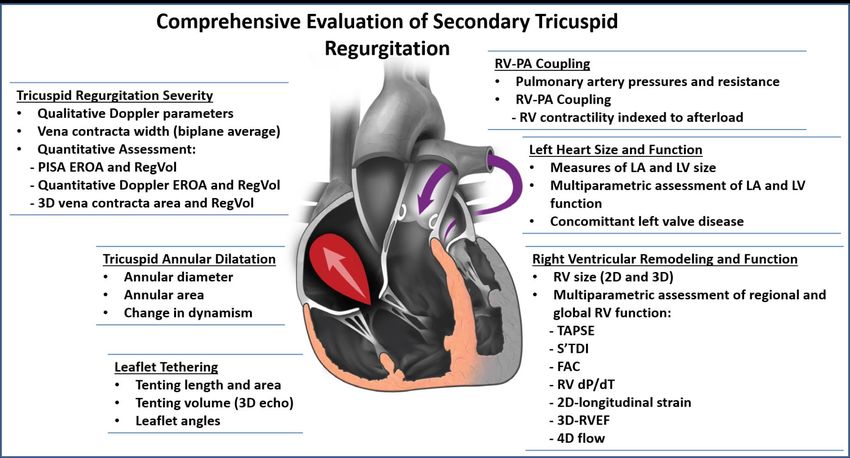
Disclosure Statement of Financial Interest
Within the past 12 months, I or my spouse/partner have had a financial
interest/arrangement or affiliation with the organization(s) listed
below.
Affiliation/Financial Relationship Company
• Grant/Research Support Medtronic, Edwards Lifesciences, Philips,
Abbott, Boston Scientific
Medtronic, Edwards Lifesciences, Shifamed,
• Consulting Fees/Honoraria Philips, Abbott Vascular, CorFlow, Neochord, V-
• Scientific Advisory Board dyne, Boston Scientific, Bolt Medical, Advanced
NanoTherapies, Centerline Biomedical, Paladin
Supira, CorFlow, Neochord, Vvital,
• Equity Interest NuevoSono, Centerline Biomedical,
Coramaze
Background Technologies Future
Background
Background
• TR is common
• Majority of TR is
functional
• TR is associated with a
poor prognosis
Wang N et al. European Heart Journal (2019) 40, 476–484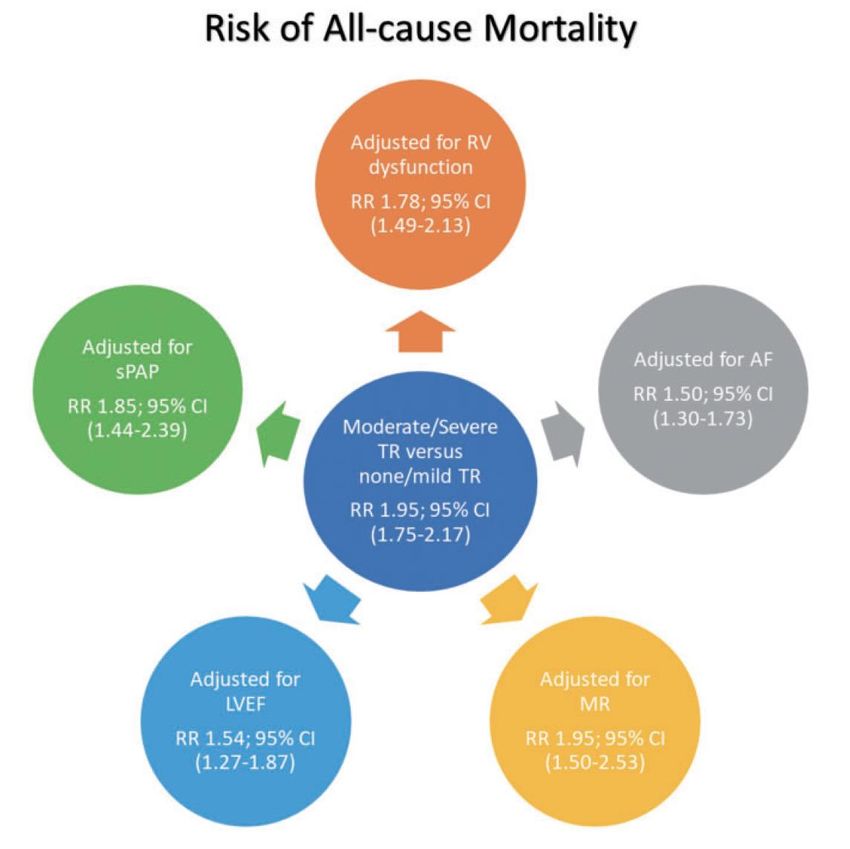
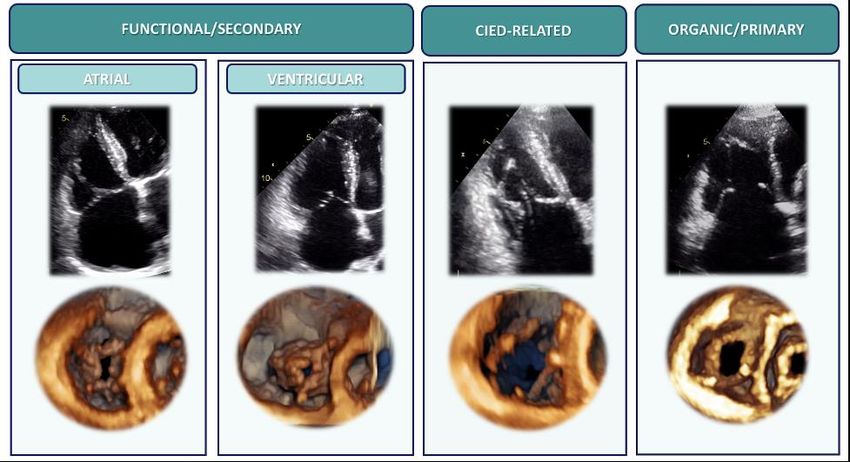
Proposal of New Pathophysiologic TR Classification
No longer «Idiopathic» or «Isolated» TR
Carpentier type I Carpentier type IIIb Carpentier type I-III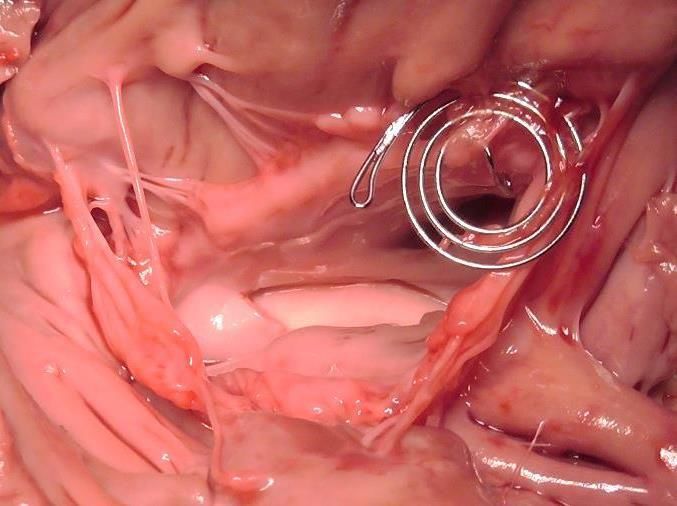
Anatomic variability of the TV
The tricuspid valve is often not three leaflets!
P2
S2
S P2 S1
P1 S
A P1
A A
Hahn et a., JACC Img 2021; 14(7):1299
2 leaflet 4 leaflet 5 leaflet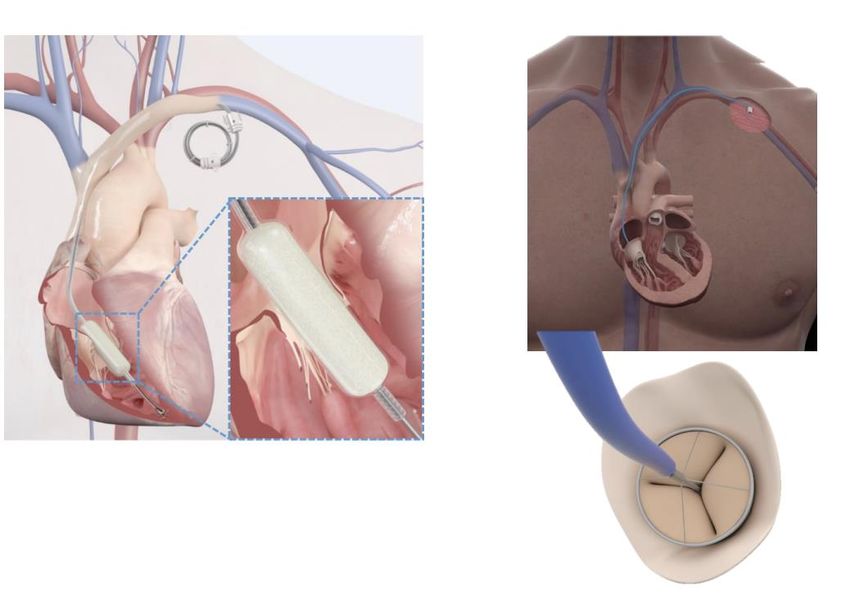
Does leaflet configuration matter?
69% 2.1% 27% 1.4%
3 2 4 5
Residual TR Clinical outcomes
vs
1 Sugiura, et al. JACC Cardiovasc Interv 2021;14(20):2260-70
2 Kitamura, et al. JACC Cardiovasc Interv 2021;14(14):1616-18
Evaluation of TR is Complex! Hahn RT et al JACC Cardiovasc Imaging 2019
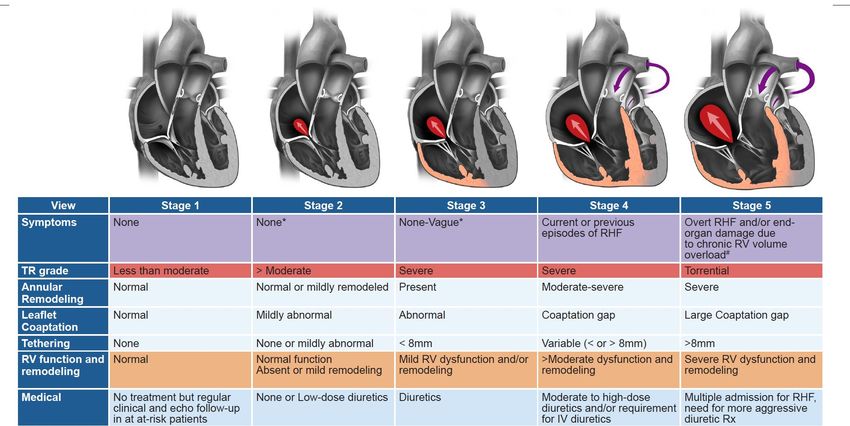
Extended Grading of TR
Prognostically important or developed to allow evaluation of devices that have
only minimal impact on TR?
MILD MODERATE SEVERE MASSIVE TORRENTIAL
RT Hahn and JL Zamorano. European Heart Journal - Cardiovascular Imaging
(2017) 00, 1–2. doi:10.1093/ehjci/jex139TR population is heterogenous!
Surgical outcomes of TV surgery
5,005 isolated TV operations between 2004-2013 12,567 patients undergoing TV Repair & Replacement between 2003-2014
(~20% of cases in US)
No of patients undergoing TV surgery for TR increased by 48% from
TV repair in 40.8%: TV replacement in 59.2%
3100 in 2003 to 4600 in 2014
TV Repair (n=7132) TV Replacement (n=2062)
Isolated TVR in 38.6%
Isolated TVr in 14.8%
In-Hospital Mortality
In-Hospital Mortality is still 8.8%
Fahad Alqahtani et al. J Am Heart Assoc 2017;6:e007597Technologies
Transcatheter Tricuspid Landscape
Trialign Cardioband TriCinch Millipede PASTA DaVingi
MIA
Annuloplasty
Edge-to-Edge Mitralix
Coaptation
Enhancement
TriClip Pascal Dragonfly
Evoque Intrepid V-Dyne Navigate Trisol Lux Topaz
Orthotopic
Replacement
TricValve TriCento Trillium Forma Croi Coramaze Tri-Flow
Heterotopic
Spacer Spacers
ReplacementIndications/Advantages:
• First-line therapy
• Procedures are relatively safe
Tricuspid TEER
• Reduction in TR grade results in
improvement in symptoms TriClip PASCAL Dragonfly
Challenges:
• Anatomical challenges:
• Gaps >8mm
• Septal leaflet tethering
• Quadricuspid
• Dense Chords
• Pacemaker Leads • >3000 cases worldwide • >500 cases
• Device and Procedure • CE-mark approval in 2002 worldwide • FIH started
• Highly dependent on good TRILUMINATE Pivotal • CE-mark approval in • Only
imaging & leaflet started 2020 available in
visualization • G4 now available: 4 Clip • CLASP-TR Pivotal China
• Residual TR sizes; independent started
• Septal “hugging” and ability grasping. • 2 devices available;
to be coaxial • Dedicated delivery system ACE in tricuspid
• Procedural length for Tricuspid • Early in learning
• Follow-up • Large amount of clinical curve
• Durability data
• SLDA • Likely to be 1st FDA
• Gradients & TV stenosis approved deviceWhat have the trials demonstrated? • Procedures are relatively safe • ~50% reduction in EROA • Improvement in clinical symptoms – Comparable to what was seen with MitraClip – Durability of benefit unclear • Patients often present with torrential TR
Challenges of TEER TR Severity
Tricuspid Annuloplasty
Indications/Advantages:
• Atrial Functional TR is common
• Stand alone therapy or combination to
decrease coaptation gaps
• Leaves future options open
Cardioband DaVingi Annuloplasty SystemOther Repair Technologies
Indications/Advantages:
• Ability to treat TEER unfavorable cases • Suture-based TEER
• Stand alone therapy or combination to • Septal leaflet enhancement
decrease coaptation gaps
• Leaves future options open • Non-ring annuloplasty devices
• Chordal/Leaflet approximationTR Reduction and Clinical Improvement
TEER Direct Annuloplasty
TR NYHA TR NYHA
Modest reductions in TR seem to be associated with clinical benefit!
Kodali S et al. J Am Coll Cardiol. 2021 Feb 2;77(4):345-356 Davidson CJ et al. JACC Cardiovasc Interv. 2021 Jan 11;14(1):41-50Transcatheter Tricuspid Valve Replacement
Indications/Advantages:
• First-line therapy
Evoque Lux Intrepid
• TEER-unsuitable cases with large
gaps, pacing leads, 4/5 leaflets,
severe tethering
• Complete elimination of TR
Challenges:
• Large annular size requiring large
valves
• RV size not large enough for • Transfemoral • Transatrial; Anchoring in RV • Transfemoral
• 29Fr delivery system • >100 pts treated (China & • Sizes: 44mm, 48mm
delivery system
• Sizes: 44mm, 48mm, Canada) • EFS underway
• Interaction with leads, prominent • TF under development
52mm
papillary muscles, apex • Pivotal underway
• Coaxiality and deliverability • >100 pts treated
highly dependent on IVC-TA • Highly imaging
relationship and RA size dependent
• Early and late impact on RV
• PM/ICD implantation: leadless,
CS, epicardial Diastole Systole
• Life-long anticoagulationTranscatheter Tricuspid Landscape – New Tools
EMERGING DEVICES WITH INNOVATIVE CONCEPTS
Tricuspid Valve Spacers
Forma CroíValve DUO Coramaze Bridging untreatable gaps
High ease-of-use with potentially
quick procedure
Spacer + central valve (Croí)Transcatheter Tricuspid Landscape – New Tools
EMERGING DEVICES WITH INNOVATIVE CONCEPTS
Tricuspid Valve Replacement
V-dyne
Side-ways delivery for large valve
Tricares Topaz
Trisol
Flexible prosthesis for free & mobile RV base
Single leaflet design w/ potential afterload
decreaseTranscatheter Tricuspid Landscape – New Tools
EMERGING DEVICES WITH INNOVATIVE CONCEPTS
Heterotopic Valves
NVT Tricento
TricValve Trillium Sidestepping untreatable TV anatomies
with massive RA/RV dilation
Treatment gap in late stage TV disease
Tackling systemic component of
longstanding TR by unloading organsFuture
4D ICE Catheters
Biosense Webster NuVision Philips VeriSight Pro
4D NuVera ICE Catheter™
>360° transducer rotation
x 3 cm extension
• 4D intracardiac echo
• Wide 90° x 90° field of view
10F x 90 cm
torqueable and • 10F size
deflectable shaft
• Independent rotation and extension
• Tricuspid imaging potential
• Conscious sedation
Transducer orientation
adjustment
Shaft deflection
Connector
CableTricuspid TEER with 4D-ICE
A
A
P
A
S
S
P
3D en face Biplane inflow-outflow/grasp
P A S
Biplane inflow- P
outflow/graspBiplane inflow-outflow/grasp
P
A
S
TTVR with 4D-ICE
LPivotal Randomized Studies in TR
The Edwards PASCAL TrAnScatheter Valve RePair System
Patients with symptomatic severe TR despite medical therapy
Pivotal Clinical Trial (CLASP II TR) (N=825)
Prospective, multicenter, randomized, controlled pivotal trial
• ≥ severe TR as assessed by echo
Multidisciplianry core lab
Heart Team • NYHA Class II-IVa
• ≥ intermediate mortality risk with
Purpose: Assessment tricuspid valve surgery
Evaluate the safety and effectiveness of the PASCAL Repair System
and optimal medical therapy (OMT) compared to OMT alone in
patients with symptomatic severe TR
PASCAL Repair System
Principle Investigators: OMT alone
+ OMT
‒ Charles Davidson, MD
‒ Scott Chadderdon, MD
Follow-up: 30 days, 6 months, 1 year and annually through 5 years
‒ Robert L. Smith, MD
Primary Endpoint at 24 months
Hierarchical composite endpoint of all-cause mortality, heart failure hospitalization,
Trial Oversight: need for surgery on the tricuspid valve, and improvement of quality of life
‒ Central screening committee
‒ Data safety monitoring board
‒ Clinical events committee
Recruiting (NCT04097145)
‒ Echocardiography imaging core laboratory
‒ Quality of life core laboratory
‒ Economic core laboratory
Edwards Transcatheter Tricuspid Valve Replacement: Patients with Symptomatic ≥ Moderate
Investigation of Safety and Clinical Efficacy Using a Tricuspid Regurgitation
Novel Device
• Functional or degenerative TR ≥
moderate
Prospective, multicenter, randomized, controlled Heart Team
• Signs and/or symptoms or prior heart
Assessment
pivotal trial failure hospitalizations from TR despite
optimal medical therapy
• Purpose | Evaluate the safety and performance of
the transfemoral EVOQUE Valve Replacement
System
EVOQUE Valve
Replacement System
• Principal Investigator | Susheel K. Kodali, MD
Follow-up: 30 days, 6 months, 1 year and annually through 5 years
• Clinical Trial Oversight:
• Data safety monitoring board Primary Endpoint: Freedom from device or procedure-related
• Clinical events committee major adverse events at 30 days
• Central screening committee
• Echocardiography imaging core laboratory
Currently recruiting patients (NCT04221490)Final Messages
TTVI Selection Praz F et al. EuroIntervention 2021;17:791-808
New patients?
NEXT PATIENTS/TARGET POPULATION
The course of TR • Asymptomatic severe TR
• Symptomatic moderate TR
• Multivalvular dx w/ concomitant TR
PREREQUISITES
➢ Know natural history of TR & which
patients progress
➢ Have device solutions that prevent
progression & leave future options
Chang et al., EHJ 2019New Tools for New patients
Treatment & Safety Effectiveness Prevention
Number of Procedures
Asymptomatic
severe TR
Symptomatic
Severe TR Severe TR Severe TR moderate TR
Torrential TR Torrential TR
with severe after left-sided
undergoing due to due to PPM
tethering, surgery with TMVI/R chronic AF leads Combined/staged
unresponsive multiple Multi-valvular proc
to diuretics comorbidities
2014 Current practice Ideal Target
Compassionate Experimental Real-world use & first commercial cases
TimeYou can also read