Trends in Oral Antibiotic Prescription in Dermatology, 2008 to 2016
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Research
JAMA Dermatology | Original Investigation
Trends in Oral Antibiotic Prescription in Dermatology,
2008 to 2016
John S. Barbieri, MD, MBA; Ketaki Bhate, MBBS; Kathleen P. Hartnett, MPH, PhD; Katherine E. Fleming-Dutra, MD;
David J. Margolis, MD, PhD
Editorial
IMPORTANCE Dermatologists prescribe more oral antibiotic courses per clinician than any Author Audio Interview
other specialty, and this use puts patients at risk of antibiotic-resistant infections and
antibiotic-associated adverse events. Supplemental content
OBJECTIVE To characterize the temporal trends in the diagnoses most commonly associated
with oral antibiotic prescription by dermatologists, as well as the duration of this use.
DESIGN, SETTING, AND PARTICIPANTS Repeated cross-sectional analysis of antibiotic
prescribing by dermatologists from January 1, 2008, to December 31, 2016. The setting was
Optum Clinformatics Data Mart (Eden Prairie, Minnesota) deidentified commercial claims
data. Participants were dermatology clinicians identified by their National Uniform Claim
Committee taxonomy codes, and courses of oral antibiotics prescribed by these clinicians
were identified by their National Drug Codes.
EXPOSURES Claims for oral antibiotic prescriptions were consolidated into courses of therapy
and associated with the primary diagnosis from the most recent visit. Courses were stratified
into those of extended duration (>28 days) and those of short duration (ⱕ28 days).
MAIN OUTCOMES AND MEASURES Frequency of antibiotic prescribing and associated
diagnoses. Poisson regression models were used to assess for changes in the frequency of
antibiotic prescribing over time.
RESULTS Between 2008 and 2016 among 985 866 courses of oral antibiotics prescribed by
11 986 unique dermatologists, overall antibiotic prescribing among dermatologists decreased
36.6% (1.23 courses per 100 visits) from 3.36 (95% CI, 3.34-3.38) to 2.13 (95% CI, 2.12-2.14)
courses per 100 visits with a dermatologist (prevalence rate ratio for annual change, 0.931;
95% CI, 0.930-0.932), with much of this decrease occurring among extended courses for
acne and rosacea. Oral antibiotic use associated with surgical visits increased 69.6% (2.73
courses per 100 visits) from 3.92 (95% CI, 3.83-4.01) to 6.65 (95% CI, 6.57-6.74) courses per
100 visits associated with a surgical visit (prevalence rate ratio, 1.061; 95% CI, 1.059-1.063).
CONCLUSIONS AND RELEVANCE Continuing to develop alternatives to oral antibiotics for
noninfectious conditions, such as acne, can improve antibiotic stewardship and decrease
complications from antibiotic use. In addition, the rising use of postoperative antibiotics after
surgical visits is concerning and may put patients at unnecessary risk of adverse events.
Future studies are needed to identify the value of this practice and the risk of adverse events.
Author Affiliations: Author
affiliations are listed at the end of this
article.
Corresponding Author: John S.
Barbieri, MD, MBA, Department of
Dermatology, University of
Pennsylvania Perelman School of
Medicine, Perelman Center for
Advanced Medicine South Tower 7,
3400 Civic Center Blvd, Philadelphia,
JAMA Dermatol. doi:10.1001/jamadermatol.2018.4944 PA 19104 (john.barbieri@uphs.
Published online January 16, 2019. upenn.edu).
(Reprinted) E1
© 2019 American Medical Association. All rights reserved.
Downloaded From: by a University of Pennsylvania User on 01/16/2019Research Original Investigation Trends in Oral Antibiotic Prescription in Dermatology, 2008 to 2016
A
ntibiotic resistance is a growing concern both for the
effectiveness of therapies for dermatologic disease and Key Points
for the treatment of infectious diseases.1-4 Dermatolo-
Question In what settings do dermatologists most frequently
gists prescribe more oral antibiotic courses per clinician than prescribe antibiotics, and how is this use changing over time?
any other specialty, and many of these courses of antibiotics
Findings Between 2008 and 2016 among 985 866 courses of
are prescribed for several months in duration.5-8 Oral antibi-
oral antibiotics prescribed by 11 986 unique dermatologists in this
otics are frequently used for acne, rosacea, and other inflam-
repeated cross-sectional analysis, there was a decrease in overall
matory conditions due to their potential anti-inflammatory antibiotic prescribing from 3.36 to 2.13 courses per 100 visits.
properties.9-15 In addition, dermatologists also prescribe peri- However, there was an increase in prescribing associated with
operative and postoperative oral antibiotics to prevent surgi- surgical visits from 3.92 to 6.65 courses per 100 visits.
cal complications.
Meaning Overall antibiotic use by dermatologists is declining;
This antibiotic use can have clinical consequences, includ- however, the use of oral antibiotics after surgical visits is
ing the development of antimicrobial resistance.16 Oral anti- increasing, and the value of this practice should be carefully
biotic therapy in the treatment of acne is associated with dis- evaluated.
ruption of the normal oropharyngeal flora and resultant
pharyngitis.17-21 The use of tetracycline-class antibiotics may
also be associated with the development of inflammatory Informed consent of participants was not applicable because
bowel disease and collagen vascular diseases.22-24 Further- this was a claims database study.
more, chronic antibiotic use has been linked in some
studies25,26 to an increased risk of colon and breast cancer, Study Design and Study Population
which is thought to be mediated through disruption of the mi- Dermatology clinicians were identified by their National Uni-
crobiome. As a result, there have been calls to reduce antibi- form Claim Committee taxonomy codes. The analysis was lim-
otic use throughout medicine. Multiple clinical guidelines for ited to courses of oral antibiotics, with prescriptions identi-
acne recommend reducing antibiotic use through nonantimi- fied by their National Drug Codes. Claims for oral antibiotic
crobial therapies and by limiting the duration of antibiotic prescriptions were consolidated into courses of therapy, with
therapy.4,27-32 the start date defined as the date of the first prescription of the
While antibiotics are prescribed for a variety of condi- series and the end date defined as the date of the last prescrip-
tions in dermatology, the frequency and duration of the use tion in the series, plus the number of days of medication sup-
of oral antibiotics by dermatologists for conditions other than plied. To account for potential delays between prescriptions
acne have not been well characterized. In addition, because due to nonadherence, prior authorizations, or other factors,
there are few randomized clinical trials demonstrating effi- prescriptions separated by less than 30 days were considered
cacy of antibiotic therapy and even fewer comparing the ef- to be part of the same course of therapy.6-8,34,35
fectiveness of antibiotic and nonantibiotic therapies in der- Courses of therapy were stratified into those of extended
matology, identifying the most frequent areas of use can guide duration (>28 days) and those of short duration (≤28 days). This
future studies to evaluate optimal prescribing practices in these cutoff was chosen to attempt to separate prescriptions that may
settings. The objective of this study was to characterize the tem- be given for acute infections (eg, Lyme disease) from those for
poral trends in the diagnoses most commonly associated with more chronic dermatologic diseases (eg, acne and hidradeni-
oral antibiotic use by dermatologists, as well as the duration tis suppurativa). These courses of therapy were then associ-
of this use. ated with the primary diagnosis from the most recent clinic
visit to a dermatologist before the date when the prescription
was filled by the patient. For visits with multiple diagnoses, a
tier system was used to associate the antibiotic prescription
Methods with the most likely diagnosis for which it was prescribed
Data Source (eTable in the Supplement). The diagnosis in the highest tier
This study was a repeated cross-sectional analysis of antibi- was considered the primary diagnosis. Surgical visits were de-
otic prescribing by dermatologists from January 1, 2008, to fined by Current Procedural Terminology codes for a destruc-
December 31, 2016, using Optum Clinformatics Data Mart tion, excision, repair, or Mohs surgery. When multiple diag-
(Eden Prairie, Minnesota) commercial claims data. This noses from the same tier were present, the first diagnosis coded
source includes deidentified administrative commercial was chosen as the primary diagnosis. Prescriptions filled more
claims data for approximately 12 to 14 million privately than 28 days after the most recent visit with a dermatologist
insured patients annually in the United States. The patient were excluded.
population available in the data source is similar to the
demographics of the US population with respect to sex, age, Statistical Analysis
and geographic distribution. 33 These data include both To account for varying frequency of dermatology encoun-
medical and pharmacy claims, as well as patient demo- ters between years, prescription counts were divided by the
graphic information, such as age and sex. This study was number of dermatology visits with the associated diagnosis
deemed exempt from review and approval by the Institu- to calculate annual rates per 100 visits. Poisson regression
tional Review Board of the University of Pennsylvania. models were used to assess for changes in the frequency of
E2 JAMA Dermatology Published online January 16, 2019 (Reprinted) jamadermatology.com
© 2019 American Medical Association. All rights reserved.
Downloaded From: by a University of Pennsylvania User on 01/16/2019Trends in Oral Antibiotic Prescription in Dermatology, 2008 to 2016 Original Investigation Research
antibiotic prescribing over time. When appropriate, data are
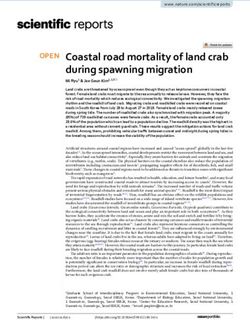
Figure 1. Antibiotic Prescribing Trends Between 2008 and 2016
summarized using descriptive statistics. Statistical analyses
were performed using a software program (Stata, version 14; 3
StataCorp LP).
Extended courses >28 d
Short courses ≤28 d
Courses of Oral Antibiotics per
2
100 Dermatology Visits
Results
Cohort
Between 2008 and 2016, there were 985 866 courses of oral
1
antibiotics prescribed by 11 986 unique dermatologists. The me-
dian time between the date of the associated visit and the date
on which the prescription was filled was 0 days (interquartile
range, 0-2 days). The most commonly prescribed antibiotics
0
were doxycycline hyclate (26.3%), minocycline (25.8%), and 2008 2009 2010 2011 2012 2013 2014 2015 2016
cephalexin (19.9%). Year
Dark blue bars show prescribing of antibiotic courses of extended duration,
Trends in Overall Prescribing defined as more than 28 days. Light blue bars show prescribing of antibiotic
Between 2008 and 2016, overall antibiotic prescribing courses of short duration, defined as 28 days or less. To account for varying
frequency of dermatology encounters between years, prescription counts were
among dermatologists decreased 36.6% (1.23 courses per
divided by the number of dermatology visits to calculate rates per 100
100 visits) from 3.36 (95% CI, 3.34-3.38) to 2.13 (95% CI, dermatology encounters.
2.12-2.14) courses per 100 visits with a dermatologist
(Figure 1), with a prevalence rate ratio (PRR) estimating an
annual change in prescribing rate of 0.931 (95% CI, 0.930-
Short Courses
0.932). For courses of extended duration, prescribing
Skin and soft-tissue infections and surgical visits were the most
decreased 53.2% (1.30 courses per 100 visits) from 2.45
common diagnoses associated with short courses of antibi-
(95% CI, 2.43-2.47) to 1.15 (95% CI, 1.14-1.16) courses per 100
otic therapy. Adjusted for the frequency of the diagnosis, skin
visits with a dermatologist (PRR, 0.900; 95% CI, 0.899-
and soft-tissue infections, surgical visits, hidradenitis suppu-
0.901). For courses of short duration, prescribing increased
rativa, and cysts were the most common diagnoses associ-
8.4% (0.07 courses per 100 visits) from 0.91 (95% CI, 0.90-
ated with short courses of antibiotic therapy (Figure 2B).
0.92) to 0.98 (95% CI, 0.98-0.99) courses per 100 visits with
Between 2008 and 2016, oral antibiotic use associated with
a dermatologist (PRR, 1.018; 95% CI, 1.014-1.023 for 2008-
surgical visits increased 69.6% (2.73 courses per 100 visits) from
2011 and PRR, 0.990; 95% CI, 0.987-0.993 for 2012-2016).
3.92 (95% CI, 3.83-4.01) to 6.65 (95% CI, 6.57-6.74) courses per
100 visits associated with a surgical visit (PRR, 1.061; 95% CI,
Extended Courses 1.059-1.063). Prescribing associated with cysts increased 35.3%
In 2016, a total of 57.5% of prescriptions for an extended (0.44 courses per 100 visits) from 1.24 (95% CI, 1.17-1.31) to 1.68
course of antibiotic therapy were associated with acne, and (95% CI, 1.62-1.74) courses per 100 visits associated with a
13.5% of prescriptions for an extended course of antibiotic diagnosis of a cyst (PRR, 1.004; 95% CI, 0.999-1.008).
therapy were associated with rosacea. Adjusted for the fre-
quency of the diagnosis, acne, rosacea, and hidradenitis Course Duration and Antibiotic Classes Prescribed
suppurativa were the diagnoses most commonly associated Throughout the study period, course duration remained simi-
with extended courses of antibiotic therapy (Figure 2A). lar across major diagnostic categories, including acne, rosa-
Between 2008 and 2016, prescribing associated with acne cea, surgical visits, and cysts (Table). The most commonly
decreased 28.1% (3.31 courses per 100 visits) from 11.76 prescribed antibiotics associated with a diagnosis of acne were
(95% CI, 11.65-11.86) to 8.45 (95% CI, 8.36-8.54) courses per doxycycline hyclate, minocycline, and extended-release mi-
100 visits with a diagnosis of acne (PRR, 0.960; 95% CI, nocycline. The most commonly prescribed antibiotics associ-
0.959-0.961). Prescribing associated with rosacea decreased ated with a diagnosis of rosacea were doxycycline hyclate,
18.1% (1.97 courses per 100 visits) from 10.89 (95% CI, 10.67- extended-release doxycycline, and minocycline. The most
11.11) to 8.92 (95% CI, 8.73-9.11) courses per 100 visits with a commonly prescribed antibiotics associated with surgical vis-
diagnosis of rosacea (PRR, 1.086; 95% CI, 1.073-1.100 for its were cephalexin and doxycycline hyclate, and the median
2008-2011 and PRR, 0.927; 95% CI, 0.924-0.931 for 2012- duration was 7 days (interquartile range, 5-10 days) for these
2016). Prescribing associated with hidradenitis suppurativa courses (Figure 3).
increased by 3.2% (0.27 courses per 100 visits) from 8.75 During the study period, prescribing of brand-name,
(95% CI, 7.75-9.74) to 9.02 (95% CI, 8.41-9.63) courses per extended-release preparations of minocycline for acne
100 visits with a diagnosis of hidradenitis (PRR, 1.137; 95% decreased from 21.3% to 17.1%. Similarly, prescribing of
CI, 1.080-1.197 for 2008-2011 and PRR, 0.958; 95% CI, brand-name, extended-release preparations of doxycycline
0.947-0.970 for 2012-2016). for rosacea decreased from 24.6% to 17.0%. In both cases,
jamadermatology.com (Reprinted) JAMA Dermatology Published online January 16, 2019 E3
© 2019 American Medical Association. All rights reserved.
Downloaded From: by a University of Pennsylvania User on 01/16/2019Research Original Investigation Trends in Oral Antibiotic Prescription in Dermatology, 2008 to 2016
Figure 2. Antibiotic Prescribing Trends Between 2008 and 2016 for the Most Common Diagnoses Among Extended Courses and Short Courses
A Extended courses B Short courses
Acne Cysts
Rosacea Dermatitis
SSTI Atopic dermatitis
14 14 Hidradenitis suppurativa Surgical visit
Courses of Oral Antibiotics per 100 Visits
Courses of Oral Antibiotics per 100 Visits
12 12
10 10
With Diagnosis
With Diagnosis
8 8
6 6
4 4
2 2
0 0
2008 2009 2010 2011 2012 2013 2014 2015 2016 2008 2009 2010 2011 2012 2013 2014 2015 2016
Year Year
A and B, Extended courses are more than 28 days, and short courses are 28 dermatology visits for the associated diagnosis to calculate rates per 100
days or less. To account for varying frequency of dermatology encounters dermatology encounters with the associated diagnosis. SSTI indicates skin and
between years, prescription counts were divided by the number of soft-tissue infection.
Table. Antibiotic Course Duration for Common Associated Visit Categories
Median (IQR), d
Extended
Variable Courses, % 2008-2010 2011-2013 2014-2016
SSTI 27.4 14 (10-30) 10 (10-30) 10 (10-30)
Acne 96.1 30 (30-128) 30 (30-125) 30 (30-100)
Rosacea 94.4 30 (30-103) 30 (30-102) 30 (30-95)
Hidradenitis suppurativa 85.5 30 (30-73.5) 30 (30-86) 30 (30-81.5)
Surgical visit 5.2 7 (5-10) 7 (5-10) 7 (7-10) Abbreviations: IQR, interquartile
range; SSTI, skin and soft-tissue
Cysts 32.3 14 (10-30) 14 (7-30) 10 (7-30)
infection.
prescribing for doxycycline monohydrate increased. For Much of the decrease in extended courses of antibiotic
hidradenitis suppurativa, the use of clindamycin increased therapy is associated with visits for acne and rosacea.
during the study period from 3.0% to 8.8% and for rifampin Although recent guidelines27 suggest limiting the duration
from 3.8% to 5.9% (Figure 3). of therapy in this patient population, course duration has
remained stable over time, suggesting that this decrease
may be due to fewer patients being treated with antibiotics
rather than patients being treated for a shorter duration.29,34
Discussion Another possible cause of decreased antibiotic use may be
This repeated cross-sectional analysis demonstrated that an- patient preference. Given increasing concerns about compli-
tibiotic prescribing among dermatologists has substantially de- cations associated with antibiotic use, patients may be more
creased over the past decade. In the context of the 39 million reluctant to opt for extended courses of antibiotics. It is also
annual office visits to dermatologists,36 this absolute change possible that improved topical treatments and increased use
of 1.23 courses per 100 visits is estimated to result in almost of alternative systemic treatments may have decreased reli-
480 000 fewer antibiotic courses per year being prescribed by ance on oral antibiotics for the treatment of these condi-
dermatologists in 2016 than in 2008. Given that dermatolo- tions. For instance, there is increasing evidence to support
gists were identified in 2013 as the most frequent prescribers the use of spironolactone as an alternative to oral antibiotics
of oral antibiotics per clinician,5 this decreased overall use is for women with acne, and the use of spironolactone has
encouraging. While the prescribing frequency for antibiotic grown in recent years.8,37-40
courses of extended duration (>28 days) decreased substan- The increasing use of postoperative antibiotics associ-
tially during the study period, there has been growth in the use ated with visits for surgical procedures is concerning. The
of antibiotic courses of short duration (≤28 days), particularly risk of surgical site infections resulting from dermatologic
among those associated with surgical visits. procedures, including Mohs surgery, is low. Procedures in
E4 JAMA Dermatology Published online January 16, 2019 (Reprinted) jamadermatology.com
© 2019 American Medical Association. All rights reserved.
Downloaded From: by a University of Pennsylvania User on 01/16/2019Figure 3. Most Frequently Used Oral Antibiotics for Common Conditions
A Acne
Doxycycline Trimethoprim- Amoxicillin-
Monohydrate, Doxycycline Doxycycline- Doxycycline- Minocycline, Minocycline- sulfamethox- Cephalexin, Amoxicillin, Clavulanate, Azithromycin, Erythromycin, Clindamycin, Rifampin,
Year % Hyclate, % LD, % ER, % % ER, % azole, % % % % % % % %
jamadermatology.com
2008-2010 5.4 29.4 0.5 2.0 22.5 21.3 8.6 2.9 3.1 0.3 1.1 2.3 0.6 0.0
2011-2013 8.2 29.3 0.4 2.7 23.8 17.2 8.4 3.3 3.2 0.3 1.1 1.6 0.5 0.0
2014-2016 9.5 26.0 1.1 2.2 25.9 17.1 8.4 4.1 2.9 0.3 1.1 0.6 0.6 0.1
B Rosacea
Doxycycline Trimethoprim- Amoxicillin-
Monohydrate, Doxycycline Doxycycline- Doxycycline- Minocycline, Minocycline- sulfamethox- Cephalexin, Amoxicillin, Clavulanate, Azithromycin, Erythromycin, Clindamycin, Rifampin,
Year % Hyclate, % LD, % ER, % % ER, % azole, % % % % % % % %
2008-2010 4.6 32.6 2.4 24.6 20.3 7.5 2.1 1.5 1.1 0.1 0.8 1.9 0.3 0.0
2011-2013 6.4 35.2 2.2 24.7 20.8 4.1 1.7 1.3 1.1 0.1 0.8 1.4 0.2 0.0
2014-2016 11.6 34.6 5.1 17.0 21.6 3.5 1.8 1.9 1.1 0.1 0.9 0.5 0.2 0.1
Downloaded From: by a University of Pennsylvania User on 01/16/2019
Trends in Oral Antibiotic Prescription in Dermatology, 2008 to 2016
C Hidradenitis suppurativa
Doxycycline Trimethoprim- Amoxicillin-
Monohydrate, Doxycycline Doxycycline- Doxycycline- Minocycline, Minocycline- sulfamethox- Cephalexin, Amoxicillin, Clavulanate, Azithromycin, Erythromycin, Clindamycin, Rifampin,
Year % Hyclate, % LD, % ER, % % ER, % azole, % % % % % % % %
2008-2010 2.1 32.3 0.1 1.3 23.2 5.9 13.4 9.1 1.1 1.7 1.2 1.6 3.0 3.8
2011-2013 5.0 32.0 0.4 0.7 22.7 3.7 11.8 6.7 1.0 1.3 0.6 1.4 6.6 6.0
2014-2016 11.3 32.5 0.2 0.6 18.3 3.0 9.6 6.2 1.1 1.5 0.8 0.1 8.8 5.9
D Surgical visit
Doxycycline Trimethoprim- Amoxicillin-
Monohydrate, Doxycycline Doxycycline- Doxycycline- Minocycyline, Minocycline- sulfamethox- Cephalexin, Amoxicillin, Clavulanate, Azithromycin, Erythromycin, Clindamycin, Rifampin,
Year % Hyclate, % LD, % ER, % % ER, % azole, % % % % % % % %
2008-2010 0.5 8.9 0.0 0.3 1.8 0.4 6.8 67.4 1.6 0.9 7.6 0.5 3.1 0.1
© 2019 American Medical Association. All rights reserved.
2011-2013 1.1 13.3 0.0 0.3 2.8 0.1 5.3 65.0 1.6 0.9 5.7 0.3 3.6 0.0
2014-2016 3.4 13.1 0.1 0.0 4.3 0.1 8.7 61.4 1.8 0.7 3.8 0.0 2.5 0.0
Green, yellow, and red boxes show more frequent, intermediate, and less frequent antibiotic classes, respectively. ER indicates extended release; LD, low dose.
(Reprinted) JAMA Dermatology Published online January 16, 2019
Original Investigation Research
E5Research Original Investigation Trends in Oral Antibiotic Prescription in Dermatology, 2008 to 2016
the groin, skin grafts, wedge excisions of the lip or ear, and may be related to the high cost of these medications and the
procedures below the knee may be associated with higher dramatic price increases for generic doxycycline hyclate56 that
surgical site infection risk, and single-dose perioperative occurred around 2012. There has also been an increase in the
antibiotics may help decrease the risk of surgical site infec- use of clindamycin and rifampin among courses of antibiotics
tion for these higher-risk cases.41-43 However, multiple pro- associated with visits for hidradenitis suppurativa. The results
spective studies of clean-contaminated head and neck pro- of 2 retrospective case series57,58 suggested that such treat-
cedures, including those that breach the mucosa, have not ment can be effective for patients with hidradenitis suppura-
identified increased efficacy between regimens of 24 hours tiva. Given the growth in the use of these antibiotics, addi-
and longer regimens of 3 to 7 days, although these studies tional prospective controlled studies or comparative
were not conducted in an office-based surgery setting.44-47 effectiveness studies may be warranted to better characterize
In addition, a 2008 advisory statement on antibiotic pro- the efficacy of this treatment regimen for patients with
phylaxis recommends single-dose perioperative antibiotics hidradenitis suppurativa. There has also been an increase in
for patients at increased risk of surgical site infection. 48 the use of tetracycline-class antibiotics associated with surgi-
Finally, guidelines from the American Heart Association49 cal visits. While the underlying factors related to this shift are
and the American Academy of Orthopedic Surgeons50 rec- unclear, it is possible that the increased prescribing may be
ommend limited use of single-dose perioperative antibiotics related to efforts to improve scar cosmesis through inhibition
for the prevention of infective endocarditis and joint infec- of matrix metalloproteases by tetracycline antibiotics.59 How-
tions, respectively, and neither guideline supports pro- ever, evidence to support this practice is limited. A 2007
longed courses of postoperative antibiotics. study60 reported smaller mean scar size in 4 rabbits random-
While guideline recommendations generally do not sup- ized to receive a maximum subtoxic dose of minocycline than
port extended postoperative courses of oral antibiotics, a 2012 in 4 control rabbits, but clinical studies supporting the effec-
survey51 sent to American College of Mohs Surgery members tiveness of oral tetracycline-class antibiotics to improve scar
identified that many antibiotic prescribing practices reported cosmesis are lacking.59
by surgeons were not aligned with guideline recommenda-
tions and concluded that dermatologic surgeons prescribe more Limitations
antibiotics than needed for infection prevention. In addition, The results of this study should be interpreted in the context
only about 70% of surgeons reported that they were familiar of the study design. Because dermatology visits may have
with the 2007 guidelines of the American Heart Association48 multiple diagnosis codes and antibiotic courses may be pre-
and the 2008 advisory statement on antibiotic prophylaxis in scribed for reasons other than the diagnoses coded at the
dermatologic surgery.51 visit, there is the possibility for misclassification herein with
It is estimated that approximately 1 in 1000 oral antibi- respect to the associated diagnoses for the antibiotic course.
otic prescriptions results in an emergency department visit However, the antibiotics were prescribed by dermatologists,
for associated complications.52 Overuse of oral antibiotics is and by using a tier system to identify the most relevant diag-
also associated with significant changes to the microbiome, noses (eg, for a visit with diagnoses coded for cellulitis, actinic
and prior exposure to antibiotics is also associated with keratosis, and a surgical visit, the prescription would be asso-
increased risk for the development of Clostridium difficile ciated with cellulitis), we have attempted to reduce the influ-
and antibiotic-resistant infections.53,54 Given the low rate of ence of this potential source of bias. Since the International
infectious complications, even for Mohs surgery, and the Classification of Diseases, Ninth Revision was replaced with the
lack of evidence to support the use of prolonged rather than International Classification of Diseases and Related Health
single-dose perioperative regimens, the postoperative Problems, Tenth Revision, Clinical Modification in 2015, it is
courses of antibiotics identified in this study may increase important to consider coding differences when examining
risks to patients without substantial benefits. Just as the trends across these periods. These coding changes may help
shift from topical antibiotics to plain white petrolatum has explain the decrease in antibiotic prescribing rates for skin
improved outcomes at reduced cost for postoperative and soft-tissue infections in 2015 and 2016; for more com-
wound care, there may be an opportunity to optimize oral monly associated diagnoses, such as acne, rosacea, hidradeni-
antibiotic prescribing in dermatologic surgery.55 Additional tis suppurativa, and surgical visits, there were no significant
evidence, including data from well-controlled prospective changes in coding between revisions. Finally, because peri-
studies, is needed to determine the appropriate role for operative antibiotics administered in the office may not gen-
perioperative and postoperative oral antibiotics for derma- erate an associated pharmacy claim, we were unable to exam-
tologic procedures, particularly for Mohs surgery, in which ine trends in the in-office use of perioperative antibiotics.
the risk of postoperative complications may be higher and
the morbidity of these complications is more significant.
For many of the conditions evaluated herein, the most
common antibiotics prescribed remained constant through-
Conclusions
out the study period. There was a decrease in prescribing of While dermatologists were once the most frequent prescrib-
brand-name, extended-release preparations of doxycycline ers of antibiotics per clinician, the prescribing of antibiotics by
and minocycline for acne and rosacea, as well as a shift dermatologists is declining, particularly for extended courses
toward increased use of doxycycline monohydrate, which of antibiotics given to patients with chronic dermatologic con-
E6 JAMA Dermatology Published online January 16, 2019 (Reprinted) jamadermatology.com
© 2019 American Medical Association. All rights reserved.
Downloaded From: by a University of Pennsylvania User on 01/16/2019Trends in Oral Antibiotic Prescription in Dermatology, 2008 to 2016 Original Investigation Research
ditions, such as acne and rosacea. Opportunities may exist to tibiotics associated with visits for surgical procedures, which
improve antibiotic stewardship further, and the Centers for Dis- may put patients at unnecessary risk of adverse events given
ease Control and Prevention has developed a framework for the available evidence and guideline recommendations. Fu-
improved antibiotic stewardship in the outpatient setting.61 ture studies are needed to identify the value of this practice
There is rising use of prolonged postoperative courses of an- with respect to patient outcomes and antibiotic stewardship.
ARTICLE INFORMATION 2. Luk NM, Hui M, Lee HC, et al. Antibiotic-resistant 2013;149(6):758-760. doi:10.1001/jamadermatol.
Accepted for Publication: November 6, 2018. Propionibacterium acnes among acne patients in a 2013.2977
regional skin centre in Hong Kong. J Eur Acad 14. Andersen RK, Jemec GB. Treatments for
Published Online: January 16, 2019. Dermatol Venereol. 2013;27(1):31-36. doi:10.1111/j.
doi:10.1001/jamadermatol.2018.4944 hidradenitis suppurativa. Clin Dermatol. 2017;35(2):
1468-3083.2011.04351.x 218-224. doi:10.1016/j.clindermatol.2016.10.018
Author Affiliations: Department of Dermatology, 3. Dreno B, Thiboutot D, Gollnick H, et al; Global
University of Pennsylvania Perelman School of 15. Mason JM, Chalmers JR, Godec T, et al; U.K.
Alliance to Improve Outcomes in Acne. Antibiotic Dermatology Clinical Trials Network BLISTER Study
Medicine, Philadelphia (Barbieri, Bhate, Margolis); stewardship in dermatology: limiting antibiotic use
Division of Healthcare Quality Promotion, Centers Group. Doxycycline compared to prednisolone
in acne. Eur J Dermatol. 2014;24(3):330-334. doi: therapy for patients with bullous pemphigoid:
for Disease Control and Prevention, Atlanta, 10.1684/ejd.2014.2309
Georgia (Hartnett, Fleming-Dutra); Epidemic cost-effectiveness analysis of the BLISTER trial. Br J
Intelligence Service, Centers for Disease Control 4. Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Dermatol. 2018;178(2):415-423. doi:10.1111/bjd.16006
and Prevention, Atlanta, Georgia (Hartnett); United Prevalence of inappropriate antibiotic prescriptions 16. Adler BL, Kornmehl H, Armstrong AW.
States Public Health Service Commissioned Corps, among us ambulatory care visits, 2010-2011. JAMA. Antibiotic resistance in acne treatment. JAMA
Rockville, Maryland (Hartnett); Department of 2016;315(17):1864-1873. doi:10.1001/jama.2016.4151 Dermatol. 2017;153(8):810-811. doi:10.1001/
Biostatistics and Epidemiology, University of 5. Centers for Disease Control and Prevention. jamadermatol.2017.1297
Pennsylvania Perelman School of Medicine, Outpatient antibiotic prescriptions: United States, 17. Levy RM, Huang EY, Roling D, Leyden JJ,
Philadelphia (Margolis). 2013. https://www.cdc.gov/antibiotic-use/ Margolis DJ. Effect of antibiotics on the
Author Contributions: Dr Barbieri had full access community/pdfs/Annual-ReportSummary_2013. oropharyngeal flora in patients with acne. Arch
to all of the data in the study and takes pdf. Updated October 1, 2018. Accessed November Dermatol. 2003;139(4):467-471. doi:10.1001/
responsibility for the integrity of the data and the 17, 2018. archderm.139.4.467
accuracy of the data analysis. 6. Lee YH, Liu G, Thiboutot DM, Leslie DL, Kirby JS. 18. Levy RM, Leyden JJ, Margolis DJ. Colonisation
Concept and design: Barbieri, Bhate, Hartnett, A retrospective analysis of the duration of oral rates of Streptococcus pyogenes and
Margolis. antibiotic therapy for the treatment of acne among Staphylococcus aureus in the oropharynx of a young
Acquisition, analysis, or interpretation of data: adolescents: investigating practice gaps and adult population. Clin Microbiol Infect. 2005;11(2):
Barbieri, Fleming-Dutra, Margolis. potential cost-savings. J Am Acad Dermatol. 2014;71 153-155. doi:10.1111/j.1469-0691.2004.01042.x
Drafting of the manuscript: Barbieri, Bhate, (1):70-76. doi:10.1016/j.jaad.2014.02.031
Margolis. 19. Margolis DJ, Fanelli M, Kupperman E, et al.
7. Straight CE, Lee YH, Liu G, Kirby JS. Duration of Association of pharyngitis with oral antibiotic use
Critical revision of the manuscript for important oral antibiotic therapy for the treatment of adult
intellectual content: Barbieri, Hartnett, for the treatment of acne: a cross-sectional and
acne: a retrospective analysis investigating prospective cohort study. Arch Dermatol. 2012;148
Fleming-Dutra, Margolis. adherence to guideline recommendations and
Statistical analysis: Barbieri, Margolis. (3):326-332. doi:10.1001/archdermatol.2011.355
opportunities for cost-savings. J Am Acad Dermatol.
Obtained funding: Margolis. 2015;72(5):822-827. doi:10.1016/j.jaad.2015.01.048 20. Bowe WP, Hoffstad O, Margolis DJ. Upper
Administrative, technical, or material support: respiratory tract infection in household contacts of
Barbieri, Bhate, Fleming-Dutra. 8. Barbieri JS, Hoffstad O, Margolis DJ. Duration of acne patients. Dermatology. 2007;215(3):213-218.
Supervision: Margolis. oral tetracycline-class antibiotic therapy and use of doi:10.1159/000106579
topical retinoids for the treatment of acne among
Conflict of Interest Disclosures: None reported. general practitioners (GP): a retrospective cohort 21. Margolis DJ, Bowe WP, Hoffstad O, Berlin JA.
Funding/Support: This study was funded in part by study. J Am Acad Dermatol. 2016;75(6):1142-1150.e1. Antibiotic treatment of acne may be associated
award 1P30AR069589-01 from the National doi:10.1016/j.jaad.2016.06.057 with upper respiratory tract infections. Arch Dermatol.
Institute of Arthritis and Musculoskeletal Skin 2005;141(9):1132-1136. doi:10.1001/archderm.141.9.
9. Cevasco NC, Bergfeld WF, Remzi BK, de Knott 1132
Diseases (NIAMS). Dr Barbieri is supported by HR. A case-series of 29 patients with lichen
award T32-AR-007465 from the NIAMS and planopilaris: The Cleveland Clinic Foundation 22. Margolis DJ, Fanelli M, Hoffstad O, Lewis JD.
receives partial salary support through a Pfizer experience on evaluation, diagnosis, and treatment. Potential association between the oral tetracycline
Fellowship Grant to the Trustees of the University J Am Acad Dermatol. 2007;57(1):47-53. doi:10. class of antimicrobials used to treat acne and
of Pennsylvania. 1016/j.jaad.2007.01.011 inflammatory bowel disease. Am J Gastroenterol.
Role of the Funder/Sponsor: The funding sources 2010;105(12):2610-2616. doi:10.1038/ajg.2010.303
10. Webster GF, Toso SM, Hegemann L. Inhibition
had no role in the design and conduct of the study; of a model of in vitro granuloma formation by 23. Schlienger RG, Bircher AJ, Meier CR.
collection, management, analysis, and tetracyclines and ciprofloxacin: involvement of Minocycline-induced lupus: a systematic review.
interpretation of the data; preparation, review, or protein kinase C. Arch Dermatol. 1994;130(6):748- Dermatology. 2000;200(3):223-231. doi:10.1159/
approval of the manuscript; and decision to submit 752. doi:10.1001/archderm.1994.01690060078008 000018387
the manuscript for publication. 24. Margolis DJ, Hoffstad O, Bilker W. Association
11. Monk E, Shalita A, Siegel DM. Clinical
Meeting Presentation: This study was presented applications of non-antimicrobial tetracyclines in or lack of association between tetracycline class
as a poster at the International Investigative dermatology. Pharmacol Res. 2011;63(2):130-145. antibiotics used for acne vulgaris and lupus
Dermatology 2018 Meeting; May 18, 2018; Orlando, doi:10.1016/j.phrs.2010.10.007 erythematosus. Br J Dermatol. 2007;157(3):540-546.
Florida. doi:10.1111/j.1365-2133.2007.08056.x
12. Barbieri JS, James WD, Margolis DJ. Trends in
prescribing behavior of systemic agents used in the 25. Cao Y, Wu K, Mehta R, et al. Long-term use of
REFERENCES antibiotics and risk of colorectal adenoma. Gut.
treatment of acne among dermatologists and
1. Mills O Jr, Thornsberry C, Cardin CW, Smiles KA, nondermatologists: a retrospective analysis, 2018;67(4):672-678. doi:10.1136/gutjnl-2016-313413
Leyden JJ. Bacterial resistance and therapeutic 2004-2013. J Am Acad Dermatol. 2017;77(3):456- 26. Velicer CM, Heckbert SR, Lampe JW, Potter JD,
outcome following three months of topical acne 463.e4. doi:10.1016/j.jaad.2017.04.016 Robertson CA, Taplin SH. Antibiotic use in relation
therapy with 2% erythromycin gel versus its to the risk of breast cancer. JAMA. 2004;291(7):
vehicle. Acta Derm Venereol. 2002;82(4):260-265. 13. Steen T, English JC. Oral minocycline in
treatment of cutaneous sarcoidosis. JAMA Dermatol. 827-835. doi:10.1001/jama.291.7.827
doi:10.1080/000155502320323216
jamadermatology.com (Reprinted) JAMA Dermatology Published online January 16, 2019 E7
© 2019 American Medical Association. All rights reserved.
Downloaded From: by a University of Pennsylvania User on 01/16/2019Research Original Investigation Trends in Oral Antibiotic Prescription in Dermatology, 2008 to 2016
27. Zaenglein AL, Pathy AL, Schlosser BJ, et al. spironolactone compared to oral tetracycline-class Interdisciplinary Working Group. Circulation. 2007;
Guidelines of care for the management of acne antibiotics for women with acne: a retrospective 116(15):1736-1754. doi:10.1161/CIRCULATIONAHA.106.
vulgaris. J Am Acad Dermatol. 2016;74(5):945- cohort study 2010-2016. J Drugs Dermatol. 2018;17 183095
973.e33. doi:10.1016/j.jaad.2015.12.037 (6):632-638. 50. Watters W III, Rethman MP, Hanson NB, et al;
28. Gollnick H, Cunliffe W, Berson D, et al; Global 41. Futoryan T, Grande D. Postoperative wound American Academy of Orthopedic Surgeons;
Alliance to Improve Outcomes in Acne. infection rates in dermatologic surgery. Dermatol American Dental Association. Prevention of
Management of acne: a report from a Global Surg. 1995;21(6):509-514. doi:10.1111/j.1524-4725. orthopaedic implant infection in patients
Alliance to Improve Outcomes in Acne. J Am Acad 1995.tb00255.x undergoing dental procedures. J Am Acad Orthop
Dermatol. 2003;49(1)(suppl):S1-S37. doi:10.1067/ 42. Dixon AJ, Dixon MP, Askew DA, Wilkinson D. Surg. 2013;21(3):180-189. doi:10.5435/JAAOS-21-03-
mjd.2003.618 Prospective study of wound infections in 180
29. Thiboutot D, Gollnick H, Bettoli V, et al; Global dermatologic surgery in the absence of 51. Bae-Harboe YS, Liang CA. Perioperative
Alliance to Improve Outcomes in Acne. New prophylactic antibiotics. Dermatol Surg. 2006;32 antibiotic use of dermatologic surgeons in 2012.
insights into the management of acne: an update (6):819-826. doi:10.1111/j.1524-4725.2006.32167.x Dermatol Surg. 2013;39(11):1592-1601. doi:10.1111/
from the Global Alliance to Improve Outcomes in 43. Kimyai-Asadi A, Goldberg LH, Peterson SR, dsu.12272
Acne group. J Am Acad Dermatol. 2009;60(5) Silapint S, Jih MH. The incidence of major 52. Shehab N, Patel PR, Srinivasan A, Budnitz DS.
(suppl):S1-S50. doi:10.1016/j.jaad.2009.01.019 complications from Mohs micrographic surgery Emergency department visits for
30. Zaenglein AL, Thiboutot DM. Expert performed in office-based and hospital-based antibiotic-associated adverse events. Clin Infect Dis.
committee recommendations for acne settings. J Am Acad Dermatol. 2005;53(4):628-634. 2008;47(6):735-743. doi:10.1086/591126
management. Pediatrics. 2006;118(3):1188-1199. doi:10.1016/j.jaad.2005.03.023 53. Dantes R, Mu Y, Hicks LA, et al. Association
doi:10.1542/peds.2005-2022 44. Liu SA, Tung KC, Shiao JY, Chiu YT. Preliminary between outpatient antibiotic prescribing practices
31. Dréno B, Bettoli V, Ochsendorf F, Layton A, report of associated factors in wound infection and community-associated Clostridium difficile
Mobacken H, Degreef H; European Expert Group on after major head and neck neoplasm operations: infection. Open Forum Infect Dis. 2015;2(3):ofv113.
Oral Antibiotics in Acne. European does the duration of prophylactic antibiotic matter? doi:10.1093/ofid/ofv113
recommendations on the use of oral antibiotics for J Laryngol Otol. 2008;122(4):403-408. doi:10. 54. Bryce A, Hay AD, Lane IF, Thornton HV,
acne. Eur J Dermatol. 2004;14(6):391-399. 1017/S0022215107007529 Wootton M, Costelloe C. Global prevalence of
32. Nast A, Dréno B, Bettoli V, et al; European 45. Miles BA, Potter JK, Ellis E III. The efficacy of antibiotic resistance in paediatric urinary tract
Dermatology Forum. European evidence-based postoperative antibiotic regimens in the open infections caused by Escherichia coli and association
(S3) guidelines for the treatment of acne. J Eur Acad treatment of mandibular fractures: a prospective with routine use of antibiotics in primary care:
Dermatol Venereol. 2012;26(suppl 1):1-29. doi:10. randomized trial. J Oral Maxillofac Surg. 2006;64 systematic review and meta-analysis. BMJ. 2016;
1111/j.1468-3083.2011.04374.x (4):576-582. doi:10.1016/j.joms.2006.01.003 352:i939. doi:10.1136/bmj.i939
33. Optum.com. Optum research data assets. 46. Andrews PJ, East CA, Jayaraj SM, Badia L, 55. Smack DP, Harrington AC, Dunn C, et al.
https://www.optum.com/content/dam/optum/ Panagamuwa C, Harding L. Prophylactic vs Infection and allergy incidence in ambulatory
resources/productSheets/5302_Data_Assets_Chart_ postoperative antibiotic use in complex surgery patients using white petrolatum vs
Sheet_ISPOR.pdf. Accessed September 6, 2018. septorhinoplasty surgery: a prospective, bacitracin ointment: a randomized controlled trial.
34. Feldman SR, Camacho FT, Krejci-Manwaring J, randomized, single-blind trial comparing efficacy. JAMA. 1996;276(12):972-977. doi:10.1001/jama.1996.
Carroll CL, Balkrishnan R. Adherence to topical Arch Facial Plast Surg. 2006;8(2):84-87. doi:10. 03540120050033
therapy increases around the time of office visits. 1001/archfaci.8.2.84 56. Barbieri JS, Margolis DJ, Brod BA. Influence of
J Am Acad Dermatol. 2007;57(1):81-83. doi:10.1016/ 47. Rajan GP, Fergie N, Fischer U, Romer M, market competition on tetracycline pricing and
j.jaad.2007.04.005 Radivojevic V, Hee GK. Antibiotic prophylaxis in impact of price increases on clinician prescribing
35. Ryskina KL, Goldberg E, Lott B, Hermann D, septorhinoplasty? a prospective, randomized study. behavior. J Invest Dermatol. 2017;137(12):2491-2496.
Barbieri JS, Lipoff JB. The role of the physician in Plast Reconstr Surg. 2005;116(7):1995-1998. doi: doi:10.1016/j.jid.2017.07.835
patient perceptions of barriers to primary 10.1097/01.prs.0000191181.73298.b3 57. Mendonça CO, Griffiths CE. Clindamycin and
adherence with acne medications. JAMA Dermatol. 48. Wright TI, Baddour LM, Berbari EF, et al. rifampicin combination therapy for hidradenitis
2018;154(4):456-459. doi:10.1001/jamadermatol. Antibiotic prophylaxis in dermatologic surgery: suppurativa. Br J Dermatol. 2006;154(5):977-978.
2017.6144 advisory statement 2008. J Am Acad Dermatol. doi:10.1111/j.1365-2133.2006.07155.x
36. Centers for Disease Control and Prevention. 2008;59(3):464-473. doi:10.1016/j.jaad.2008.04. 58. Gener G, Canoui-Poitrine F, Revuz JE, et al.
National Ambulatory Medical Care Survey: 031 Combination therapy with clindamycin and
factsheet: dermatology. https://www.cdc.gov/nchs/ 49. Wilson W, Taubert KA, Gewitz M, et al; rifampicin for hidradenitis suppurativa: a series of
data/ahcd/namcs_2010_factsheet_dermatology.pdf. American Heart Association Rheumatic Fever, 116 consecutive patients. Dermatology. 2009;219
Published 2010. Accessed September 6, 2018. Endocarditis, and Kawasaki Disease Committee; (2):148-154. doi:10.1159/000228334
37. Charny JW, Choi JK, James WD. Spironolactone American Heart Association Council on 59. Reish RG, Eriksson E. Scars: a review of
for the treatment of acne in women, a retrospective Cardiovascular Disease in the Young; American emerging and currently available therapies. Plast
study of 110 patients. Int J Womens Dermatol. 2017; Heart Association Council on Clinical Cardiology; Reconstr Surg. 2008;122(4):1068-1078. doi:10.
3(2):111-115. doi:10.1016/j.ijwd.2016.12.002 American Heart Association Council on 1097/PRS.0b013e318185d38f
Cardiovascular Surgery and Anesthesia; Quality of
38. Grandhi R, Alikhan A. Spironolactone for the Care and Outcomes Research Interdisciplinary 60. Henry SL, Concannon MJ, Kaplan PA,
treatment of acne: a 4-year retrospective study. Working Group. Prevention of infective Diaz-Arias AA. The inhibitory effect of minocycline
Dermatology. 2017;233(2-3):141-144. doi:10.1159/ endocarditis: guidelines from the American Heart on hypertrophic scarring. Plast Reconstr Surg.
000471799 Association: a guideline from the American Heart 2007;120(1):80-88. doi:10.1097/01.prs.0000263325.
39. Park JH, Bienenfeld A, Orlow SJ, Nagler AR. Association Rheumatic Fever, Endocarditis, and 73400.f8
The use of hormonal antiandrogen therapy in Kawasaki Disease Committee, Council on 61. Sanchez GV, Fleming-Dutra KE, Roberts RM,
female patients with acne: a 10-year retrospective Cardiovascular Disease in the Young, and the Hicks LA. Core elements of outpatient antibiotic
study. Am J Clin Dermatol. 2018;19(3):449-455. doi: Council on Clinical Cardiology, Council on stewardship. MMWR Recomm Rep. 2016;65(6):1-12.
10.1007/s40257-018-0349-6 Cardiovascular Surgery and Anesthesia, and the doi:10.15585/mmwr.rr6506a1
40. Barbieri JS, Choi JK, Mitra N, Margolis DJ. Quality of Care and Outcomes Research
Frequency of treatment switching for
E8 JAMA Dermatology Published online January 16, 2019 (Reprinted) jamadermatology.com
© 2019 American Medical Association. All rights reserved.
Downloaded From: by a University of Pennsylvania User on 01/16/2019You can also read