TMR Modern Herbal Medicine
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
TMR Modern Herbal Medicine
homepage: https://www.tmrjournals.com/mhm
Clinical practice guidelines for traditional Chinese medicine and integrated
traditional Chinese and western medicine: a cross-sectional study of data
analysis from 2010 to 2020
Jie Zhou 1, 2, #, Jing Guo 1, 3, #, Jia-Ying Wang 4, Qiao Huang 1, Rong Zhang 5, Zheng-Rong Zhao 6, Hong-Jie Xia
6
, Xiang-Ying Ren 7, Yi-Bei Si 8, Jian-Peng Liao 9, Ying-Hui Jin 1, *, Hong-Cai Shang 10, *
1 Center for Evidence-Based and Translational Medicine, Zhongnan Hospital of Wuhan University, Wuhan
430071, Hubei Province, China.
2 School of Nursing, Wuhan University, Wuhan 430071, Hubei Province, China.
3 The Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing 210029, Jiangsu Province, China.
4 The Affiliated Wuxi People's Hospital of Nanjing Medical University, Wuxi 214000, Jiangsu Province, China.
5 Department of Neurotumor Disease Diagnosis and Treatment Center, Taihe Hospital, Hubei University of
Medicine, Shiyan 442000, Hubei Province, China.
6 College of Acupuncture and Orthopedics, Hubei University of Chinese Medicine, Wuhan 430061, Hubei
Province, China.
7 College of Nursing and Health, Henan University, Kaifeng 475001, Henan province, China.
8 The Second Clinical College, Wuhan University, Wuhan 430071, Hubei Province, China.
9 School of Public Health, Wuhan University, Wuhan 430071, Hubei Province, China.
10 Dongzhimen Hospital, Beijing University of Chinese Medicine, Key Laboratory of Chinese Internal Medicine
of Ministry of Education, Beijing 100700, China.
# They
contributed equally to this paper.
*Correspondence to jinyinghuiebm@163.com (Ying-Hui Jin); shanghongcai@126.com (Prof. Hong-Cai Shang)
Peer review information TMR Abstract
Modern Herbal Medicine thanks Objective With the increasing publication of clinical practice guidelines (CPG)
anonymous reviewers for their for Traditional Chinese Medicine (TCM) and Integrated Traditional Chinese and
contribution to the peer review of this Western Medicine (IM), the standardization and scientifiction of its formulation
work. have gradually attracted many people’s attention. To offer an overview of TCM
and IM CPGs published over the past decade and analyze their general
Citation Zhou J, Guo J, Wang JY, et characteristics and methodological quality.
al. Clinical practice guidelines for Methods The China National Knowledge Infrastructure (CNKI) and
traditional Chinese medicine and WANFANG databases were searched for clinical practice guidelines and expert
integrated traditional Chinese and consensus papers from January 2010 to June 2021. Two researchers
western medicine: a cross-sectional independently completed the literature screening and cross-checking according
study of data analysis from 2010 to to the inclusion and exclusion criteria of CPGs and extracted information on
2020. TMR Modern Herbal Medicine. general characteristics and methodological quality of CPGs.
2022; 5(1):3. Results According to the selection criteria, 231 CPGs (EB-CPGs=119, CB-
CPGs=112) were selected and the number of CPGs published in the 11 years
Executive editor Chao-Yong Wu showed an overall upward trend. The vast majority of CPGs used the Western
naming system for the diseases, and only 11 CPGs were named of TCM diseases
Submitted 13 January 2022 or symptoms. TCM treatments were recommended in 223 CPGs. There were
Accepted 30 January 2022 156 ancient Chinese Medicine literature sources cited in 231 CPGs and opinions
Available online 10 February 2022
© 2022 By Authors. Published by TMR Publishing Group Limited. This is an open access article under the CC-BY
license. (http://creativecommons.org/licenses/BY/4.0/)
Submit a manuscript: https://www.tmrjournals.com/mhm 1doi: 10.53388/MHM2022A0113001 Article
and experiences of 62 TCM experts cited in 37 CPGs. The methodological
quality of EB-CPGs for TCM and IM were significantly better than CB-CPGs
in 11 items. Only 60 EB-CPGs and 7 CB-CPGs designated clear criteria for
grading quality of evidence and strength of the recommendations and 74 CPGs
presented both the level of evidence and the strength of recommendations. We
classified all CPGs according to whether or not they used GRADE, and the
results showed that the CPGs using GRADE had higher methodological quality
and more standardized reports.
Conclusion This research has shown that the quantity and quality of CPGs in
both TCM and IM have improved over the time span, but the methodological
quality, especially evidence citation, and the use of criteria for grading quality
of evidence and strength of the recommendations, still needs to further
improvement in the future.
Keywords Evidence-based CPG, Consensus-based CPG, Traditional Chinese
medicine, Integrated traditional Chinese and western medicine, Methodological
quality
Highlights According to the definition of the Institute of Medicine
(IOM) in 2011 [5], Clinical Practice Guidelines offer
We systematically evaluated the general information optimal guidance for patients with specific clinical
characteristics and methodological characteristics of problems based on evidence formed by systematic
119 EB-CPGs and 112 CB-CPGs on TCM and IM evaluation and comprehensive analysis of the strengths
from 2010 to 2020. We found that the quantity and and weaknesses of various alternative interventions. TCM
quality of CPGs in both TCM and IM have improved and IM have played a unique role in the prevention and
over the time span, but the methodological quality, treatment of diseases, such as SARS, influenza A, tumors,
especially evidence citation, and the use of criteria for cardiovascular and cerebrovascular diseases. Standardized
grading quality of evidence and strength of the development, dissemination and implementation of TCM
recommendations, still needs to further improvement and IM clinical practice guidelines is a viable way to
in the future. internationalize TCM [6].
With the increasing publication of clinical practice
guideline (CPG) for TCM and IM, the standardization and
Background scientifiction of its formulation have gradually attracted
wide attention from researchers and medical practitioners.
As a treasure of Chinese culture, Traditional Chinese The low rigor and credibility of these CPGs leads to them
Medicine (TCM) is widely used in medical practice. having an unsatisfactory clinical utilization rate, so not
However, in the overall medical development and research allowing them to play a real guiding role in clinical
field, Chinese medicine is still in a relatively weak position practice [7-10]. Domestic researchers have surveyed the
[1]. China is the only country in the world that adopts application of TCM guidelines for 11 common diseases
Chinese and Western medicine in primary, secondary, and and found that 54.5% of the guidelines had never been
tertiary treatment systems [2]. In recent years, the cited [11]. At present, there is no systematic in-depth study
development of TCM has attracted the attention of the on the publication and quality of TCM and IM guidelines.
national government. The “Strategic Plan for the Therefore, this paper has searched and analyzed the current
Development of Traditional Chinese Medicine (2016-2030) TCM and IM guidelines published over the past decade to
[3]” identifies the phased objectives of the development of investigate their advantages and disadvantages, with the
TCM, emphasizing that not only does the TCM medical aim of promoting the standardization and normalization of
service system need to be improved, but also a guideline formulation.
standardized system for TCM needs to be established.
Since the 1980s, the government has attached increasing Methods
importance to the development of TCM and the
construction of a standardized system. The features and Search strategy
importance of TCM in health care have become The CPGs included in this study were based on previous
increasingly prominent and the number of guidelines for retrieval work done by the research team. The key words
TCM including integrated traditional Chinese and Western for the searches included Chinese words for terms such as
medicine (IM) has also increased rapidly [4]. ‘guidelines’, ‘practice guideline’, ‘clinical guideline’,
‘clinical practice guideline’, ‘consensus’, ‘expert
2 Submit a manuscript: https://www.tmrjournals.com/mhmTMR Modern Herbal Medicine doi: 10.53388/MHM2022A0113001
consensus’, ‘expert consensus statements’, ‘professional individuals including working groups and committees),
consensus’, ‘recommendation’. We searched for these number of pages of CPGs document, number of references,
terms in title fields from China National Knowledge guideline type(EB-CPG or CB-CPG), classification of
Infrastructure (CNKI) and WANFANG from January 2010 TCM or IM, theme (diagnosis, treatment, prevention,
to June 2021. prevention and treatment, diagnosis and treatment, nursing,
rehabilitation, infectious disease prevention and control),
Eligibility criteria CPGs users target population (under or over 18 years),
Inclusion criteria: (1) conforming to the definition of Grading quality of evidence and strength of
clinical practice guidelines proposed by IOM in 1990 [12] recommendations, TCM recommendation (decoction,
or 2011 [5]. (2) Chinese version of original guidelines and Chinese patent medicine, TCM injection, traditional
consensus in the field of TCM and IM published in China exercises, acupuncture, external TCM therapies including
and available as full text. We classified the guidelines into Tuina (therapeutic massage), enema, application by
two types based on their title definition of CPGs, which patching or mounting, cupping, fumigation, herb bath, etc.).
were evidence-based CPG (EB-CPG) and consensus- Diseases were classified according to the International
based CPG (CB-CPG). Usually when evidence is only of Classification of Disease revision 11 (ICD-11).
low quality, guideline development groups label them as Through the consensus process, we extracted the
expert opinions and consensus statements. In this research following 11 information categories from the 23 items of
we describe both expert opinions and consensus statements AGREE II to reflect the current methodological status of
as CB-CPGs. The classification into EB-CPGs or CB- CPGs for TCM or IM. (1) Multidisciplinary development
CPGs and the differentiation between TCM or IM is based teams: these were described as diverse groups including
on the reports of their titles and verification from the text. more than two of the following representatives: relevant
Exclusion criteria: (1) Interpretation class, compilation, technical experts or health professionals, end-users,
adaptation CPGs. (2) Translated versions of foreign representatives of groups most affected by the
guidelines. (3) Incomplete CPGs which omitted important recommendations, methodologists (assessing evidence and
information, such as brief versions that only include developing guidelines informed by evidence, or health
introductions, directories, abstracts and recommendations. economist or technical experts in equity and human rights).
If several published versions of one CPG existed, only (2) Systematic literature searching: the article clearly
the version containing the greatest detail was included for points out accessing and rigorously searching at least 4
research. If CPGs are updated, both previous and updated databases in English and Chinese, (e.g., PubMed,
versions were included in the assessment. If CPGs are Cochrane library, CNKI). (3) Identifies the characteristics
published in several parts, they were merged into one of TCM evidence in retrieval and selection of evidence,
complete CPG for assessment. such as the search or use of ancient books and literature on
TCM, opinions and experience of TCM experts. (4)
Data extraction Recommendations based on evidence of systematic
The research team members formed the data extraction reviews of the scientific literature: at least one piece of the
table for CPGs based on the general characteristics of evidence supporting a recommendation came from a
CPGs and some items from the Appraisal of Guidelines for systematic review or meta-analysis. Systematic review
Research and Evaluation Ⅱ (AGREE-Ⅱ) instrument. The was described as “a review of a clearly formulated question
general characteristics and methodological quality of that uses explicit and systematic methods to identify, select,
CPGs reflected the development of CPGs in China over the and critically assess relevant research, and to extract and
past 11 years. Two researchers independently completed analyze data from the studies that are included in the
the literature screening and cross-checking according to review”. (5) Quality evaluation of included literature. (6)
the inclusion and exclusion criteria of the guidelines. Any Clear criteria for grading quality of evidence and strength
disagreement was resolved through discussion with a third of recommendations used, and whether they are based on
author. Before data extraction, three evaluation members or combined with TCM evidence. (7) The designation of
in the group were trained, and then two pre-tests were level of evidence. (8) The presentation of strength of
conducted. In order to reduce bias in understanding the recommendations. (9) The declaration of conflicts of
extracted items, the extraction work was only commenced interest. (10) The identification of sources of funds:
after a relatively consistent understanding of the data divided into national, provincial and municipal
extraction content was reached. governmental funds which come from governmental
Information on general characteristic included guideline organizations; hospitals and universities; medical specialty
title, year of publication, year of updating and interval societies and no funding (including not funded and no
between updates, development body and its classification report). (11) The consideration of factors such as
(National Health Commission of the People's Republic of feasibility, economy, security, equity, acceptability, values,
China, medical specialty societies including their branches,
Submit a manuscript: https://www.tmrjournals.com/mhm 3doi: 10.53388/MHM2022A0113001 Article
and patient preferences in the formulation of each
recommendation.
Data analysis
This paper reports only descriptive statistics, using
Microsoft Excel software entry and collation of data to
give a frequency and percentage summary. Inter-rater
reliability was assessed by Kappa statistics. Comparisons
of EB-CPGs and CB-CPGs in methodological
characteristics were conducted using chi-square test or
Fisher’s exact test. Mann Kendall Trend Test (M-K test), a
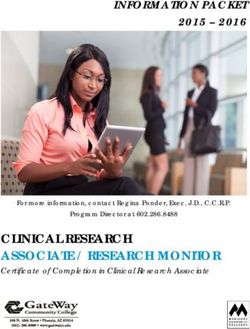
non-parametric method, was adopted to identify Figure 2. Trends in the number of CPGs for TCM and
monotonically increasing or decreasing trends of IM from 2020 to 2021
methodological characteristics over years, a positive z
value indicated a monotonic upward trend and a negative General characteristics of guidelines
one indicated downward trend. The statistical software Number and themes of CPGs From 2010 to 2020, the
SPSS 25.0 was used for data analysis and a two-sided P numbers of CPGs published for TCM and IM have shown
value of < 0.05 was considered as statistically significant. an overall upward trend, and the number of CB-CPGs
publications in the past four years was significantly higher
Results than that of EB-CPGs. The total number of CPG
publications was the lowest in 2013, and the number of
Flow of included studies publications increased rapidly from 2018 to 2020, reaching
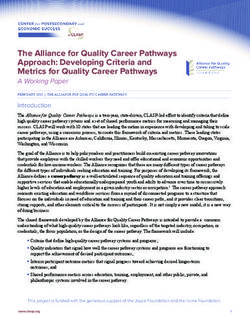
A total of 29,186 articles were identified, of which 18,078 a maximum of 58 in 2020, accounting for 25.11% (58/231)
were considered potentially relevant; after selection, a total of the total publications, including 31 EB-CPGs and 27
of 450 guidelines were eligible. 231 guidelines (EB- CB-CPGs (See Figure 2).
CPGs=119, CB-CPGs=112) were selected according to the Diagnosis and treatment were the main themes of CPGs,
selection criteria (See Figure 1). There was high agreement accounting for 69.70% (161/231). In addition, the
between the authors extracting data (Kappa= 0.835; 95% remaining CPGs themes were treatment (15.15%),
CI 0.675~0.883; P < 0.001). Two authors discussed the diagnosis (0.87%), prevention and control of infectious
differences in data extraction with the third author, and diseases (6.06%), prevention and treatment (4.33%),
reached a consensus by re-examining the CPGs. nursing (0.43%), rehabilitation (3.46%). According to the
classification of CPGs in the field of TCM and IM, there
were 154 CPGs for TCM and 77 CPGs for IM, accounting
for 66.67% (154/231) and 33.33% (77/231), respectively.
Classification of TCM therapies in recommendations
According to the recommendations given in the article, the
most widely used TCM treatment method is decoction,
accounting for 90.91% (210/231) of the total number of
publications, including 108 EB-CPGs and 102 CB-CPGs.
The second most widely used TCM treatment method was
Chinese patent medicine treatment, which was
recommended by 98 EB-CPGs and 79 CB-CPGs,
accounting for 76.62% (177/231) of the total number of
publications. A total of 87 EB-CPGs and 78 CB-CPGs
recommended acupuncture therapy, accounting for 71.43%
(165/231). 68 EB-CPGs and 51 CB-CPGs recommended
external TCM treatment, accounting for 51.52% (119/231),
of which 21.21% (49/231) recommended Tuina. In
addition, 13.42% (31/231) of CPGs recommended
traditional exercises, and 9.96% (23/231) recommended
treatment using TCM injections The remaining 8 CPGs did
not recommend TCM-related diagnosis and treatment
methods, which were (1) Guideline for Western Medicine
Diagnosis and TCM Syndrome Differentiation of IgA
Figure 1. Guideline selection Nephropathy, (2) Guideline for TCM pediatric clinical
4 Submit a manuscript: https://www.tmrjournals.com/mhmTMR Modern Herbal Medicine doi: 10.53388/MHM2022A0113001
diagnosis and treatment of children with insufficiency of establishment of a working group or committee), and the
the spleen using medicated cuisine (formulation), (3) remaining 1 EB-CPG did not report the development
Traditional Chinese Medicine Treatment Guidelines for organizations. Details are shown in Supplementary Table
Coronary Heart Disease Before and After Percutaneous 1.
Coronary Intervention, (4) Standardization Guidelines for CPGs covered a broad range of diseases. The most
Chinese Medicine Rehabilitation, (5) Expert consensus on addressed diseases were digestive system diseases
phase I cardiac rehabilitation after coronary artery bypass (25.54%), followed by circulatory system diseases
grafting in the integrative medicine, (6) Traditional (9.96%), certain infectious or parasitic diseases (9.96%),
Chinese medicine core nursing knowledge and practical respiratory system diseases (6.93%), symptoms, signs or
ability training standards: an expert consensus, (7) Expert clinical findings, not elsewhere classified (6.94%),
Consensus on Selection Criteria for Ancient Medical diseases of the skin (6.49%), diseases of the
Cases of Sepsis in Traditional Chinese Medicine, (8) musculoskeletal system or connective tissue (6.06%),
Expert Consensus on study and application of Traditional diseases of the genitourinary system (4.33%). The
Chinese Medicine Knowledge by Western Pharmacists in classification of diseases is shown in Table 1.
General Hospitals (Beijing, 2020). Among the 231 CPGs, there were 11 CPGs using the
Development organizations and diseases addressed by TCM disease or syndrome naming system, including 7
CPGs Eighty EB-CPGs and 95 CB-CPGs were formulated using the TCM disease names (chest obstruction with pain,
by the medical specialty societies, accounting for 75.76% snake strand sore, nasal obstruction, syndrome of
(175/231) of the total number of publications, followed by malnutrition, sweating syndrome, snoring, bloody semen)
47.62% (110/231) Chinese Association of Traditional and 3 TCM syndrome names (syndrome of heat and stasis,
Chinese Medicine, 21.21% (49/231) Chinese Society of constitution of spleen deficiency, stagnation of blood),
Integrated Traditional Chinese and Western Medicine, 5.19% accounting for 4.76% (11/231) of the total number of
(12/231) World Federation of Chinese Medicine publications. There were two management consensuses in
Associations. There were 23.81% (55/231) of CPGs CB-CPGs, including Traditional Chinese medicine core
developed by individuals (only describing the nursing knowledge and practical ability training standard:
Table 1. The classification of diseases in CPGs from 2020 to 2021
EB-CPGs CB-CPGs Proportion
Classification of diseases (ICD-11)
(n/%) (n/%) %
01 Certain infectious or parasitic diseases 11 12 9.96%
02 Neoplasms 0 2 0.87%
03 Diseases of the blood or blood-forming organs 1 1 0.87%
04 Diseases of the immune system 1 1 0.87%
05 Endocrine, nutritional or metabolic diseases 6 1 3.03%
06 Mental, behavioral or neurodevelopmental disorders 4 1 2.16%
07 Sleep-wake disorders 1 0 0.43%
08 Diseases of the nervous system 6 2 3.46%
09 Diseases of the visual system 1 1 0.43%
11 Diseases of the circulatory system 12 11 9.96%
12 Diseases of the respiratory system 10 6 6.93%
13 Diseases of the digestive system 18 41 25.54%
14 Diseases of the skin 2 13 6.49%
15 Diseases of the musculoskeletal system or connective tissue 11 3 6.06%
16 Diseases of the genitourinary system 10 0 4.33%
17 Conditions related to sexual health 2 1 1.30%
20 Developmental anomalies 1 0 0.43%
21 Symptoms, signs or clinical findings, not elsewhere classified 8 7 6.49%
23 External causes of morbidity or mortality 1 0 0.43%
24 Factors influencing health status or contact with health services 2 0 0.87%
26 Supplementary Chapter Traditional Medicine Conditions-
5 1 2.60%
Module I
X Extension Codes 3 5 3.46%
Literature of TCM diseases not found in ICD-11 3 2 2.16%
Management literature not found in ICD-11 0 2 0.87%
Submit a manuscript: https://www.tmrjournals.com/mhm 5doi: 10.53388/MHM2022A0113001 Article
an expert consensus; Expert Consensus on study and Damage was cited most frequently, which was cited by 36
application of Traditional Chinese Medicine Knowledge EB-CPGs and 35 CP-CPGs, accounting for 30.74%
by Western Pharmacists in General Hospitals (Beijing, (71/231), followed by 29.00% (67/231) Beneficial
2020). Formulas from the Taiping Imperial Pharmacy, 25.97%
Target population and CPGs users Thirty-four (14.72%) (60/231) Essentials from the Golden Cabinet, 23.38%
CPGs targeted patients under 18 years old of which only 1 (54/231) Correction of Errors in Medical Works, 22.51%
CPG was for infants, and 57 (24.68%) CPGs targeted (55/231) The Complete Works of [Zhang] Jing-yue. The
patients over 18 years old. The remaining 140 CPGs did top 20 citations of ancient books and literatures of TCM
not specify the target population, accounting for 60.61% are presented in Table 2.
(140/231) of the total number of publications. Thirty-seven CPGs cited opinions and experiences of 62
CPGs users included 6.49% (15/231) TCM doctors, 8.23% TCM experts, 19 CPGs cited National Famous Chinese
(19/231) TCM and Western Medicine doctors, 1.73% Medicine Practitioner; 17 CPGs cited National physician
(4/231) TCM and IM doctors, TCM, 2.16% (5/231) master; 10 CPGs cited Provincial Famous Chinese
Western Medicine and IM doctors. There were 188 CPGs Medicine Practitioner; 5 CPGs cited Municipal Famous
which did not report CPGs users, accounting for 81.39% Chinese Medicine Practitioner; 4 CPGs cited Qi Huang
(188/231) of the total number of publications. scholars' treatment experience and opinions; 1 CB-CPGs
quoted the opinions and experience of ancient Chinese
Methodological characteristics of guidelines medicine expert Wang Bing in traditional exercises for
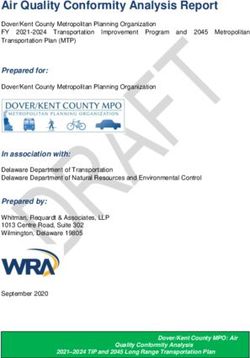
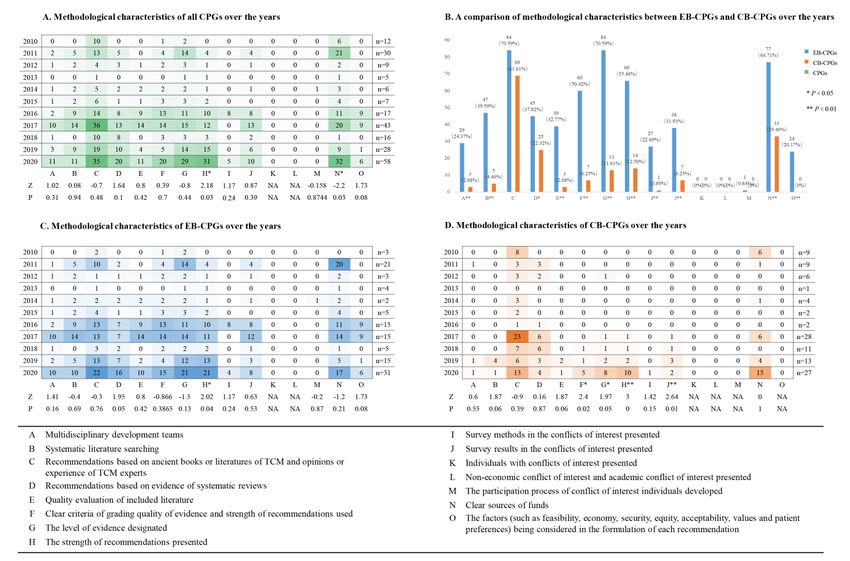
The results of methodological information assessment of heart disease and 19 CPGs cited other TCM experts.
CPGs are shown in Figure 3. Among the cited TCM experts, 3 EB-CPGs cited the
Citation of ancient literature of TCM and experience experience of Professor Xu Jingfan, a master of TCM, in
and opinion of TCM experts A total of 153 (66.23%) of the treatment of digestive system diseases. The three CB-
the 231 CPGs cited ancient books and literatures of TCM CPGs cited the experience and methods of Professor Li
and experience and opinions of TCM experts including Junxiang, a scholar of Qi and Huang, in the treatment of
70.59% (84/119) EB-CPGs and 61.61% (69/112) CP- liver cirrhosis and ascites diseases. Specific references to
CPGs. TCM expert opinions and experiences are contained in
A total of 156 ancient Chinese medicine literature Table 3.
sources were cited in 231 CPGs, of which Treatise on Cold
Table 2. Top 20 citations of ancient books and literatures of TCM cited in CPGs from 2020 to 2021
EB-CPGs CB-CPGs Proportion
Ancient literature sources
(n/%) (n/%) %
Treatise on Cold Damage 36 35 30.74%
Beneficial Formulas from the Taiping Imperial Pharmacy 41 26 29.00%
Essentials from the Golden Cabinet 36 24 25.97%
Correction of Errors in Medical Works 28 26 23.38%
The Complete Works of [Zhang] Jing-yue 24 28 22.51%
Huangdi Neijing 11 24 15.15%
Systematic Differentiation of Warm Diseases 20 13 14.29%
Teachings of [Zhu] Dan-xi 14 11 10.82%
Golden Mirror of the Medical Tradition 19 2 9.09%
Zhengzhi Zhunsheng 13 8 9.09%
Yifang Jijie 10 11 9.09%
Yixue Xinwu 13 6 8.23%
Neiwai Shangbian Huolun 14 4 7.79%
Xiaoer Yaozheng Zhijue 13 4 7.36%
Jishengfang 10 5 6.49%
Beiji Qianjin Yao Fang 9 6 6.49%
Treatise on the spleen and stomach 9 4 5.63%
Gujin Mingyi Fanglun 5 6 4.76%
Theory of Cholera 2 9 4.76%
Revised Effective Prescriptions for Women 7 3 4.33%
6 Submit a manuscript: https://www.tmrjournals.com/mhmTMR Modern Herbal Medicine doi: 10.53388/MHM2022A0113001
Table 3. TCM expert opinions and experiences cited in CPGs from 2020 to 2021
EB-CPGs CB-CPGs Proportion
TCM Experts Classification
(n/%) (n/%) %
Bing Wang Ancient Chinese medicine experts 0 1 0.43%
Tietao Deng National physician master 1 1 0.87%
Jixue Ren National physician master 1 1 0.87%
Qi Wang National physician master 0 1 0.43%
Jibai Xiong National physician master 1 0 0.43%
Jingfan Xu National physician master 3 0 1.30%
Boshou Xue National physician master 1 0 0.43%
Dexin Yan National physician master 2 0 0.87%
Zhenghua Yan National physician master 1 0 0.43%
Xuewen Zhang National physician master 1 0 0.43%
Xuewen Zhou National physician master 1 0 0.43%
Liangchun Zhu National physician master 2 0 0.87%
Qingqi Zeng Clinical TCM experts 0 1 0.43%
Zhanjie Chang Clinical TCM experts 0 1 0.43%
Danan Cheng Clinical TCM experts 1 0 0.43%
Tianshu Gao Clinical TCM experts 1 0 0.43%
Shuhan Ge Clinical TCM experts 1 0 0.43%
Guisheng Guo Clinical TCM experts 0 1 0.43%
Xianpei Heng Clinical TCM experts 1 0 0.43%
Desheng Ji Clinical TCM experts 0 1 0.43%
Hongyi Li Clinical TCM experts 0 1 0.43%
Xiaomei Lu Clinical TCM experts 0 1 0.43%
Fuzhou Pu Clinical TCM experts 1 0 0.43%
Fenghua Qin Clinical TCM experts 0 1 0.43%
Weiqun Sang Clinical TCM experts 0 1 0.43%
Jingming Shao Clinical TCM experts 2 0 0.87%
Jinchen Sun Clinical TCM experts 1 0 0.43%
Ruixia Wang Clinical TCM experts 0 1 0.43%
Yongyan Wang Clinical TCM experts 1 0 0.43%
Siping Wu Clinical TCM experts 0 1 0.43%
Junxiang Li Qi Huang scholar 0 3 1.30%
Hong Shen Qi Huang scholar 1 0 0.43%
Zhaowei Shan National Famous Chinese Medicine Practitioner 1 0 0.43%
Ying Ding National Famous Chinese Medicine Practitioner 1 0 0.43%
Zhongying Gao National Famous Chinese Medicine Practitioner 1 0 0.43%
Fazhi Li National Famous Chinese Medicine Practitioner 0 1 0.43%
Gui Li National Famous Chinese Medicine Practitioner 0 1 0.43%
Shoushan Li National Famous Chinese Medicine Practitioner 1 0 0.43%
Yi Lin National Famous Chinese Medicine Practitioner 0 1 0.43%
Lihua Lou National Famous Chinese Medicine Practitioner 0 1 0.43%
Heng Ouyang National Famous Chinese Medicine Practitioner 0 1 0.43%
Ying Qian National Famous Chinese Medicine Practitioner 0 1 0.43%
Hao Sun National Famous Chinese Medicine Practitioner 1 0 0.43%
Xinhua Tan National Famous Chinese Medicine Practitioner 0 1 0.43%
Shouchuan Wang National Famous Chinese Medicine Practitioner 1 0 0.43%
Xu Wu National Famous Chinese Medicine Practitioner 1 0 0.43%
Fusong Xu National Famous Chinese Medicine Practitioner 0 1 0.43%
Yongjie Zhang National Famous Chinese Medicine Practitioner 1 0 0.43%
Submit a manuscript: https://www.tmrjournals.com/mhm 7doi: 10.53388/MHM2022A0113001 Article
Wenxia Zhao National Famous Chinese Medicine Practitioner 0 2 0.87%
Fusheng Zhou National Famous Chinese Medicine Practitioner 0 1 0.43%
Ruli Ai Provincial Famous Chinese Medicine Practitioner 0 1 0.43%
Yun Cui Provincial Famous Chinese Medicine Practitioner 0 1 0.43%
Ruiqiang Fan Provincial Famous Chinese Medicine Practitioner 0 1 0.43%
Maoliang Qiu Provincial Famous Chinese Medicine Practitioner 2 0 0.87%
Lining Wang Provincial Famous Chinese Medicine Practitioner 1 1 0.87%
Jingri Xie Provincial Famous Chinese Medicine Practitioner 1 0 0.43%
Baochun Zhang Provincial Famous Chinese Medicine Practitioner 1 0 0.43%
Heping Zhao Provincial Famous Chinese Medicine Practitioner 0 1 0.43%
Ping Liu Municipal Famous Chinese Medicine Practitioner 1 1 0.87%
Lingtai Wang Municipal Famous Chinese Medicine Practitioner 1 0 0.43%
Peifen Yue Municipal Famous Chinese Medicine Practitioner 1 0 0.43%
Peiting Zhu Municipal Famous Chinese Medicine Practitioner 1 0 0.43%
Figure 3. Methodology characteristics of all CPGs from 2020 to 2021
Grading quality of evidence and strength of item of presenting the level of evidence over the time-span
recommendations A total of 84 EB-CPGs and 13 CB- (Item G, P < 0.05) (See Figure 3D). CPGs, (P < 0.05) EB-
CPGs designated the level of evidence, 66 EB-CPGs and CPGs (P < 0.05) and CB-CPGs (P < 0.01) all have
14 CB-CPGs presented the strength of recommendations, improved significantly in the item of presenting the
and 74 of 231 (32.03%) CPGs presented both the level of strength of recommendations over the time-span (Item H,
evidence and the strength of recommendations. Significant See Figure 3A, 3C and 3D).
differences between EB-CPGs and CB-CPGs were 50.42% (60/119) EB-CPGs and 6.25% (7/112) CB-
observed in this methodological characteristic (Item G and CPGs designated clear criteria for grading quality of
H, P < 0.01), which is shown in Figure 3B. Compared with evidence and strength of the recommendations. EB-CPGs
EB-CPGs, CB-CPGs have improved significantly in the were better developed than CB-CPGs in this item, and
8 Submit a manuscript: https://www.tmrjournals.com/mhmTMR Modern Herbal Medicine doi: 10.53388/MHM2022A0113001 there was a significant statistical difference between the P < 0.01) (See Figure 3B). The remaining 199 CPGs did two (Item F, P < 0.01) (See Figure 3B). Compared with not report multidisciplinary cooperation, accounting for EB-CPGs, CB-CPGs have improved significantly in this 86.15% (199/231) of the total number of publications. item over the time-span (Item F, P < 0.05) (See Figure 3D). The expert groups of 27 CPGs include clinical experts From 2010 to 2020, there are 6 criteria for grading and methodological experts (experts in evidence-based quality of evidence and strength of the recommendations: medicine, statistics, health economics, philology, clinical 12.12% (28/231) the grading standards for TCM literature epidemiology, and guidelines development methodology). by Professor Wang Shouchuan [13]; 9.09% (21/231) the Among 154 CPGs for TCM, 25 have developed Grading of Recommendations Assessment, Development multidisciplinary cooperation. Among them, 9 CPGs and Evaluation (GRADE) criteria by the International inviting Western medicine clinical experts accounted for Evidence Classification Working Group [14] ; 7.79% 5.84% (9/154), and 6 CPGs inviting IM clinical experts (18/231) Evidence Classification of Clinical Research accounted for 3.90% (6/154). Based on Evidence Body by Professor Liu Jianping [15]; Retrieval and Appraisal of evidence 22.51% (52/231) 3.46% (8/231) Delphi classification standard proposed by CPGs were based on a complete literature search, International Infection Forum (ISF) in 2001; 0.87% (2/231) including 39.50% (47/119) of EB-CPGs and 4.46% (5/112) National Clinical Guidelines Database Evidence Rating of CB-CPGs. It was clear that there was a significant System; 0.43% (1/231) Oxford Centre For Evidence Based difference between EB-CPGs and CB-CPGs (Item B, P < Medicine, OCEBM. 0.01) (See Figure 3B). 3.03% (7/231) of CPGs had more Among the 21 CPGs using GRADE, 4 EB-CPGs used than 100 references, all of which are EB-CPGs. modified GRADE criteria named from 1 to 4. Among them, From 2010 to 2020, there were 30.30% (70/231) of the Modified GRADE 4 was combined with the evidence EB-CPGs whose recommendations were based on characteristics of the guidelines for TCM and IM, so as to evidence of systematic reviews, which consisted of 37.82% make it more suitable for the guidelines in this field. The (45/119) EB-CPGs and 22.32% (25/112) CB-CPGs. There grading standards for TCM literature by Professor Wang was a statistically significant difference between EB-CPGs Shouchuan; Evidence Classification of Clinical Research and CB-CPGs (Item D, P < 0.05) (see Figure 3B). Based on Evidence Body by Professor Liu Jianping and There were 42 CPGs citing quality evaluation, self-defined criteria for grading quality of evidence and accounting for 18.18% (42/231) of the total number of strength of the recommendations also reflect the TCM publications. Among them, there were 39 EB-CPGs and 3 features in criteria for grading quality of evidence. A total CB-CPGs, accounting for 32.77% (39/119) and 2.68% of 34.45% (41/119) of EB-CPGs and 5.36% (6/112) of (3/112) of the total number of publications, respectively. CB-CPGs use above mentioned TCM related criteria. There were significant differences between the EB-CPGs Details are shown in Table 4. and CB-CPGs (Item E, P < 0.01) (see Figure 3B). Sources of funding for guidelines A total of 110 (47.62%) Developing recommendations Among the 231 CPGs, CPGs indicated where there were clear sources of funding, only 24 EB-CPGs took into account the feasibility, including 64.71% (77/119) EB-CPGs and 29.46% (33/112) economy, security, equity, acceptability, values, and patient CB-CPGs. Although CPGs have improved in this area of preferences in the formation of recommendations, the methodological quality over the time-span (P < 0.05, accounting for 20.17% (24/119). There were significant Item N) (See Figure 3A), a significant statistical difference differences between EB-CPGs and CB-CPGs (Item O, P < still remains between EB-CPGs and CB-CPGs (P < 0.01, 0.01) (see Figure 3B). Item N) (See Figure 3B). Conflicts of interest A total of 45 (19.48%) CPGs Most funding (26.41%, 61/231) came from the National published from 2010 to 2020 stated the conflicts of interest Administration of Traditional Chinese Medicine, including survey results of the drafters, including 31.93% (38/119) 46.22% (55/119) EB-CPGs and 5.36% (6/112) CB-CPGs. in the EB-CPGs and 6.25% (7/112) in the CB-CPGs. The In addition, 12.99% (30/231) were supported by national difference between the two was statistically significant projects, 2.60% (6/231) by provincial projects, 8.66% (Item J, P < 0.01) (see Figure 3B). CB-CPGs have (20/231) by municipal projects and 0.87% (2/231) by improved significantly in the item of reporting the survey associations. 51.52% (119/231) CPGs did not report a clear results of conflicts of interest over the time-span (Item J, P source of funding. < 0.01) (See Figure 3D). Multidisciplinary development teams 13.85% (32/231) Among the 231 CPGs, 12.12% (28/231) described the of the CPGs established multidisciplinary development conflicts of interest survey method, of which EB-CPGs groups during the formulation process and the expert group accounted for 22.69% (27/119) and CB-CPGs accounted consisted of professionals from at least two different for 0.89% (1/112). The difference between the two was disciplines, this included 29 EB-CPGs and 3 CB-CPGs. statistically significant (Item I, P < 0.01) (see Figure 3B). EB-CPGs scored significantly higher for this item (Item A, Submit a manuscript: https://www.tmrjournals.com/mhm 9
doi: 10.53388/MHM2022A0113001 Article
Table 4 Criteria for grading quality of evidence and strength of the recommendations used in the published guidelines from 2010-2020
Based on TCM evidence (ancient CB-
Criteria for grading quality of evidence and The strength of EB-CPGs
The level of evidence literature of TCM or experience CPGs
strength of the recommendations recommendations (n/%)
and opinion of TCM experts) (n/%)
Wang Shouchuan, the grading standards for
Ⅰ, Ⅱ, Ⅲ, Ⅳ, Ⅴ A, B, C, D, E Yes 20/16.81% 4/3.57%
TCM literature
Recommended, Selectively
Liu Jianping, Evidence Classification of Ⅰa, Ⅰb, Ⅱa, Ⅱb, Ⅲa, Ⅲb,
Recommended, Not Yes 5/4.20% -
Clinical Research Based on Body of Evidence Ⅳ, Ⅴ
Recommended, Prohibited
Liu Jianping, Evidence Classification of
Clinical Research Based on Body of Evidence Ⅰa, Ⅰb, Ⅱa, Ⅱb, Ⅲa, Ⅲb,
- Yes 4/3.36% 1/0.89%
without criteria for strength of the Ⅳ, Ⅴ
recommendations
Delphi classification standard proposed by
Ⅰ, Ⅱ, Ⅲ, Ⅳ, Ⅴ A, B, C, D, E No 5/4.20% -
International Infection Forum (ISF) in 2001
Wang Shouchuan, the grading standards for
TCM literature for level of evidence
Delphi classification standard proposed by Ⅰ, Ⅱ, Ⅲ, Ⅳ, Ⅴ A, B, C, D, E Yes 3/2.52% -
International Infection Forum (ISF) in 2001
for strength of the recommendations
Oxford Centre For Evidence Based Medicine,
Ⅰ, ⅡA, ⅡB, ⅡC, Ⅲ A, B, C No 1/0.84% -
OCEBM
Liu Jianping, Evidence Classification of
Clinical Research Based on Body of Evidence
for level of evidence Ⅰa, Ⅰb, Ⅱa, Ⅱb, Ⅲa, Ⅲb,
A, B, C No 2/1.68% -
National Clinical Guidelines Database Ⅳ, Ⅴ
Evidence Rating System for strength of the
recommendations
10 Submit a manuscript: https://www.tmrjournals.com/mhmTMR Modern Herbal Medicine doi: 10.53388/MHM2022A0113001
High, Moderate, Low,
GRADE Strong, Weak No 6/5.04% 1/0.89%
Very low
Modified GRADE 1 # Ⅰ, Ⅱ-1, Ⅱ-2, Ⅱ-3, Ⅲ Strong, Weak No 1/0.84% -
Modified GRADE 2 # A, B, C Strong, Weak No 1/0.84% -
Modified GRADE 3 # A, B, C Ⅰ, Ⅱ, Ⅱa, Ⅱb, Ⅲ No 1/0.84% -
Modified GRADE 4 # Ⅰ, Ⅱa, Ⅱb, Ⅲ, Ⅳ Strong, Weak Yes 1/0.84% -
GRADE and Wang Shouchuan, the grading
Ⅰ, Ⅱ, Ⅲ, Ⅳ, Ⅴ
standards for TCM literature for level of
High, Moderate, Low, Strong, Weak, Not recommended Yes 1/0.84% -
evidence ##
Very low
GRADE for strength of the recommendations
GRADE and Liu Jianping, Evidence High, Moderate, Low,
Classification of Clinical Research Based on Very low
Strong, Weak Yes 1/0.84% -
Body of Evidence for level of evidence * Ⅰa, Ⅰb, Ⅱa, Ⅱb, Ⅲa, Ⅲb,
GRADE for strength of the recommendations Ⅳ, Ⅴ
Liu Jianping, Evidence Classification of
Clinical Research Based on Body of Evidence Ⅰa, Ⅰb, Ⅱa, Ⅱb, Ⅲa, Ⅲb,
Strong, Weak Yes 4/3.36% 1/0.89%
for level of evidence Ⅳ, Ⅴ
GRADE for strength of the recommendations
GRADE without criteria for strength of the High, Moderate, Low,
- No 3/2.52% -
recommendations Very low
Ⅰa, Ⅰb, Ⅱa, Ⅱb, Ⅲa, Ⅲb,
Self-defined criterion** - Yes 1/0.84% -
Ⅳ, Ⅴ
#: 4 EB-CPGs used modified GRADE criteria named from 1 to 4.
##: The reported literature was based on GRADE and the literature from TCM books was based on the grading standards for TCM literature by Professor Wang Shouchuan to grade
the quality of evidence.
*: GRADE was used to appraisal the bodies of evidence and recommendations; the body of evidence and recommendation of TCM prescriptions were graded by Evidence
Classification of Clinical Research Based on the Body of Evidence by Professor Liu Jianping.
**: the self-defined criterion was formulated with reference to GRADE, Liu Jianping 's Evidence Classification of Clinical Research Based on the Body of Evidence, and evidence-
based clinical practice guidelines of TCM, combined with the clinical characteristics of the disease.
Submit a manuscript: https://www.tmrjournals.com/mhm 11doi: 10.53388/MHM2022A0113001 Article
Only 0.84% (1/119) of EB-CPGs presents the participation feasibility, economy, security, equity, acceptability, values,
process of individual conflicts of interest guidelines. and patient preferences in the formation of their
recommendations. Of CPGs that reported conflicts of
Effect of GRADE on the methodological quality of interest surveys the methods and results of the drafters
CPGs were unsatisfactory.
In 2010-2020, there were 9.09% (21/231) CPGs that used Both EB-CPGs and CB-CPGs were included in this
GRADE methodology of which 10.65% (19/119) were study, and they differed significantly in quality. From the
EB-CPGs and 4.72% (2/112) were CB-CPGs. We evaluation results of this study, EB-CPGs were superior to
statistically analyzed 15 methodological quality evaluation CB-CPGs in several methodological quality evaluation
items of those using GRADE and those not using it. From items. Particularly, EB-CPGs showed higher quality in the
the following statistical analysis, it can be concluded that evaluation and citation of evidence. However, in terms of
the methodological quality of CPGs using GRADE quality improvement over time, the EB-CPGs included in
classification system is relatively high in the formulation this study showed significant quality improvement only in
process. There were significant differences in the presenting the strength of recommendations; whereas the
methodological quality in 9 items of CPGs using GRADE methodological quality of the CB-CPGs showed more
and those not using it (P < 0.01). Supplementary Figure 1 significant improvement over time, mainly in specifying
shows the details. criteria for grading quality of evidence and strength of the
recommendations, designating the level of evidence and
Discussion the strength of recommendations, and reporting the
conflicts of interest survey results. EB-CPGs are optimal
After descriptive and analytical data analysis of the general guidelines for patient-specific clinical problems, based on
information characteristics and methodological evidence from systematic review and a comprehensive
characteristics of 119 EB-CPGs and 112 CB-CPGs on balance of pros and cons of various alternative
TCM and IM from 2010 to 2020, it was found that the interventions [5]. In contrast to EB-CPGs, CB-CPGs
number of CPGs published in the 11 years showed an usually lack a uniform definition and are defined
overall upward trend, which was consistent with the differently by different international guideline
current focus on the development of CPGs standards and development organizations. At present, it is generally
guidelines for TCM and IM. The vast majority of CPGs accepted that CB-CPG is an industry guidance document
used the Western diseases naming system, and only 11 that is less rigorously produced than EB-CPG. A CB-CPG
CPGs were found to be named using the TCM diseases or is a recommendation in a particular medical field that is
symptoms naming system. A total of 223 CPGs formulated by medical specialty societies or experts
recommended TCM treatment, including decoction, having a certain influence in a certain field based on
Chinese patent medicine, acupuncture, external TCM consensus approach (e.g., Delphi method) and limited
therapies, Tuina, traditional exercises and TCM injection. evidence [2, 16]. In our study, the CB-CPGs were not
As the most widely used and the most equipped TCM highly cited for evidence, and only a small proportion of
treatment, decoction was recommended in most CPGs. In them were developed based on systematic evaluation,
our study, over the eleven-year time span, CPGs were of quality assessment of the included literature, and clear
poor quality in the item of clearly identifying the target indications of criteria for grading quality of evidence and
population and guideline users, with 60.61% and 81.39% strength of the recommendations; mostly
of CPGs not reporting the target population and guideline recommendations were reached through the expert
users, respectively, and no patient version of the guidelines consensus process only. It is important to clarify that CB-
were found. In additional, only a few CPGs have been CPGs are not only experts’ opinions, but also need to be
updated in this study. The methodological quality of the supported by relevant evidence, otherwise biased
TCM and IM CPGs included in this study was generally recommendations may be obtained, which may result in
poor. Only one-seventh of the CPGs established a poor clinical guidance [17-18]. A more rigorous
multidisciplinary expert panel in the development of recommendation based on higher-level evidence and a
guidelines and there was low participation of standardized development process may be an important
methodological experts in the development process. Less direction for future guidelines and consensus development
than a quarter of CPGs conducted sufficient evidence in the field of TCM and IM [19].
retrieval and literature quality appraisal. Less than one About two-thirds of the CPGs in this study cited ancient
third of the CPGs clearly pointed out the criteria for literature of TCM and TCM experts experience or opinions
grading quality of evidence and strength of the as sources of evidence. TCM has a long history and
recommendations. 41.99% and 34.63% CPGs of the CPGs inherits the wisdom of the Chinese people for about five
presented evidence level and recommendations strength, thousand years, and ancient literature and experts
respectively. Only one-fifth EB-CPGs considered the
12 Submit a manuscript: https://www.tmrjournals.com/mhmTMR Modern Herbal Medicine doi: 10.53388/MHM2022A0113001 experience or opinions in Chinese medicine are the system, and then develop evidence through research. In all, characteristic evidence of TCM. Ancient literature has expert experience can also be proved through real world significant advantages in serving as a basis for decision studies by future generations, and effective dialectical making in TCM [20]. Firstly, the large number of ancient ideas and treatments strategies can be passed down. literature sources in TCM, covering a wide range of Modern medical evidence based on expert experience and disease areas, can provide supporting evidence for most opinion to support guideline development may be a future diseases; secondly, citing ancient literature as evidential trend. support is more in accordance with the characteristics of Over the past century, the clinical TCM has been facing clinical decision-making in TCM. However, there are still competition and challenges from Western medicine. It is a obstacles to using the citation of ancient literature as an new trend in the development of TCM to realize the evidence source for clinical evidence-based TCM as complementarity between Chinese and Western medicine evidence formulated in the guidelines often has an by giving full play to the advantages of TCM. For example, incomplete evaluation system [20-21]. The methodology the examination and diagnosis of diseases and the of guideline development requires classification and understanding of diseases through modern medicine grading of evidence, but the existing evidence provide TCM with more accurate and reliable objects for classification methods, especially the international evidence-based treatment, and the combination of recognized evidence classification and grading methods, evidence-based and disease-based diagnosis further are based on modern medical evidence, so this presents a improves the diagnosis and evidence-based level of TCM. problem when using ancient literature as evidence and how There are significant differences between the theoretical to complete the classification and grading in the guideline and practical systems of TCM and Western Medicine [38]. development process is a question yet to be solved. In our In some CPGs [39-41], there was a mixed use of multiple study, a certain number of CPGs were unable to be graded criteria for grading the quality of evidence or strength of using the internationally unified grading criteria for the recommendations. For example, the reported literature evidence quality and recommendations. Although some was based on the international evidence grading system, scholars [21-27] in China have developed grading while the TCM-related evidence quality grading standards standards for ancient literature they are only dealing with were mainly used for the grading of TCM ancient literature this one issue, they are unable to make a comprehensive and TCM expert opinions. We do not advocate the using evaluation with the evidence of modern medical research of multiple evidence quality or recommendation criteria in and still cannot promote and disseminate ancient literature the development of a guideline, mainly because the internationally. At the same time, more and more high- systemic and holistic nature of classification and grading quality TCM studies have been published in international criteria in the development and formulation process can be authoritative medical journals [28-31], laying the interrupted with the fragmentation or combination of foundation for the modernization and internationalization different criteria. For instance, GRADE is based on the of TCM. Therefore, based on previous research body of evidence of different study types and different conclusions [32-35] and our considerations, we initial evidence levels before applying rating down and recommend that real-world studies based on ancient rating up factors [42]. For different clinical problems, literature should be conducted and applied as a source of confidence in best estimates of magnitude of effects, evidence for CPGs. Modern medical evidence in TCM not feasibility, as well as the cost of transformation of evidence only reflects the important methods and interventions in to decision making are taken into account in the GRADE ancient literature, but also translates ancient literature into model, which are not fully available in other criteria. modern medical studies, which will facilitate its In this study, we classified all CPGs according to dissemination internationally and its standardization of whether they used the GRADE or not, and the results criteria for evidence quality and grading of showed that the CPGs using GRADE had higher recommendations in the guideline development process. methodological quality and showed more standardized The experience and opinion of TCM experts mainly reporting. There are still many challenges in the refers to the experienced prescriptions or opinions of application of the international evidence classification and ancient and modern famous TCM practitioners. The grading system to TCM and IM CPGs, but it is undeniable classification of expert opinion is not consistent among the that they are the scientific standard and so the way forward. existing TCM evidence quality standards [13,22,24,36]. Some scholars [43-45] believed that GRADE is still one of Liu Jianping [37] has put forward the path from the most effective methods for the construction of the “experience” to “evidence” for TCM diagnosis and TCM clinical system, and recommend the application of treatment characteristics: which is, to obtain information the GRADE to TCM/IM clinical practice guidelines. As through observation of TCM medical experience, integrate the methodology of CPGs in TCM and TCM continued to the information and refine theories to build a knowledge mature and the quality of the included studies gradually Submit a manuscript: https://www.tmrjournals.com/mhm 13
doi: 10.53388/MHM2022A0113001 Article
improves, the application of GRADE in CPGs of TCM and CPG, evidence-based CPG; consensus-based CPG;
IM will gradually mature and increase [45]. In addition, we AGREE-Ⅱ, Appraisal of Guidelines for Research and
noticed that four EB-CPGs [46-49] attempted to use Evaluation Ⅱ.
GRADE in the development process. However, due to the
unavailability of GRADE for TCM evidence, they adapted Acknowledgments
GRADE without detailing the adaptation method of the This work was supported by the National Natural
modified GRADE criteria. These challenges are mainly Science Foundation of China (No. 82174230 and No.
caused by the lack of classification and grading of TCM- 81904055). We express our gratitude to Jean Glover
related evidence included in internationally accepted from Tianjin Golden Framework Consulting for
common standards. As mentioned above, we do not English editing.
advocate the using of modified GRADE criteria and
transforming TCM evidence into modern medical Author contributions
evidence before being cited by CPGs can solve these Jie Zhou and Jing Guo were the main writers of the article;
problems. Similarly, real-world studies based on TCM they completed the collection and analysis of relevant
evidence can be classified and graded using GRADE. literatures and written the initial draft (including
This paper has some limitations: (1) We only searched substantive translation and revision). Jie Zhou, Zheng-
the CNKI and Wanfang without searching for English Rong Zhao, Hong-Jie Xia, Xiang-Ying Ren, Yi-Bei Si and
guidelines and consensus statements developed by Jian-Peng Liao participated in the collection and check of
Chinese researchers. When screening the literature, we literatures and materials. Jie Zhou, Qiao Huang and Rong
only classify TCM and IM from the literature titles, so Zhang completed data analysis and visualization. Ying-
some literature may have been missed. (2) In this study, Hui Jin, Hong-Cai Shang and Jia-Ying Wang were the
the complete form of AGREE II was not used for designers in charge of the project and directed the article
methodological quality evaluation in the included writing. All authors read and agreed on the final text.
literature, so it does not provide a systematic
understanding of the literature quality and the research Competing interests
perspective is relatively limited. The authors declare no competing interests.
Conclusion References
High-quality, clinically relevant CPGs for TCM and IM are 1. Bai X. Establishment and method of evaluation
needed to guide practitioners to make more rational system for clinical practice guidelines of traditional
clinical decisions, standardize medical practices, direct the Chinese medicine. Beijing: Beijing University of
active development of TCM, and promote the Chinese Medicine; 2020: 1–90 (Chinese)
standardization and internationalization of TCM [50]. This 2. Hesketh T, Zhu W. Health in China: traditional
research has shown that the quantity and quality of CPGs Chinese medicine: one country, two systems. BMJ
in TCM and IM have improved over the time span. With 1997; 315(7100): 115–117.
the increasing development of CPGs in TCM and IM, it is 3. State Council of the People’s Republic of China.
hoped that the methodological quality, especially evidence Notice of the state council on the issuance of the
citation, and the use of criteria for grading quality of strategic outline for the development of Chinese
evidence and strength of the recommendations, will medicine (2016–2030). State Council Gazette of the
become more standardized and scientific so promoting People’s Republic of China, 2016, No. 1547(08): 21–
standardization and internationalization of CPGs in TCM 29. (Chinese)
and IM. 4. Chen YL, Liu X, Wang YP, et al. Western medical
guidelines and traditional Chinese medical guidelines:
Data availability improving together through mutual learning. Medical
Supplementary data are available online at TMR Modern Journal of Peking Union Medical College Hospital
Herbal Medicine. Correspondence and requests for 2020; 11(5): 615–620. (Chinese)
materials should be addressed to jinyinghuiebm@163.com 5. Institute of Medicine (US) Committee on Standards
(Prof. Ying-Hui Jin). for Developing Trustworthy Clinical Practice
Guidelines, Graham R, Mancher M, Miller Wolman
Abbreviations D, Greenfield S, Steinberg E, editors. Clinical
CPG, Clinical Practice Guidelines; TCM, Traditional practice guidelines we can trust. Washington (DC):
Chinese Medicine; IM, integrated traditional Chinese and National Academies Press (US) 2011.
Western medicine; CNKI, China National Knowledge 6. Wang YY, Li YY, Jia BT, et al. Quality evaluation of
Infrastructure; IOM, Institute of Medicine; EB-CPG, CB- clinical practice guidelines and expert consensus of
14 Submit a manuscript: https://www.tmrjournals.com/mhmTMR Modern Herbal Medicine doi: 10.53388/MHM2022A0113001
integrated Chinese and western medicine in China. science and technology——proceedings of 12
Chinese Journal of Integrated Traditional and standards leading the summit forum on academic
Western Medicine 2020; 40(6): 672–678. (Chinese) innovation and development of traditional Chinese
7. Wu MJ, Zhang SJ, Zhou ZC, et al. Use and demand medicine. China Association for Science and
of clinical practice guidelines in China. Chinese Technology, Jilin Provincial People's Government:
Journal of Medical Library and Information Science Academic Department of China Association for
2016; 25(1): 37–42. (Chinese) Science and Technology 2017; 1. (Chinese)
8. Li YW, Liu YF, Cui J, et al. Quality assessment of 18. Zhao SH. Scientific cognition of clinical practice
clinical practice guidelines of traditional Chinese guideline and expert consensus. Chinese Journal of
medicine for coronary heart diseases. Chinese Journal Radiology 2021; 55(4): 340–342. (Chinese)
of Evidence-Based Medicine 2021; 21(6): 696–702. 19. Liao X, Xie YM, Zhang JH, et al. The technical
(Chinese) specification of expert consensus statement in
9. Li N, Jin XY, Pang WT, et al. Citations and evidence developing clinical practice guidelines of traditional
types in clinical guidelines of traditional Chinese Chinese medicine. China Journal of Chinese Materia
medicine: an analysis of data from 2016 to 2019. Medica 2019; 44(20): 4354–4359. (Chinese)
Journal of Traditional Chinese Medicine 2021; 20. Li HQ, Zou YH, Yao YN, et al. Application of
62(12): 1086–1091. (Chinese) evidence-based research in ancient books of
10. Zhang F. Evaluation of integrated Chinese and traditional Chinese medicine (TCM) in the
western medicine clinical practice guidelines for development of TCM clinical practice guideline.
acute bronchitis based on clinical audit evaluation Chinese Journal of Evidence-Based Medicine 2018;
paradigm. Liaoning: Liaoning University of 18(02): 225–229. (Chinese)
Traditional Chinese Medicine; 2019: 1–111 21. Yao YN, Cao KG, Tuo T, et al. Construction of
(Chinese). evidence grading and recommendation system for
11. Yu WY, Shi NN, Wang LY, et al. Development of ancient Chinese medicine books through expert’s
clinical practice guidelines in 11 common diseases questionnaire survey. Journal of Traditional Chinese
with Chinese medicine interventions in China. Medicine 2021; 62(07): 572–576. (Chinese)
Chinese Journal of Integrative Medicine 2012; 18(2): 22. Wang J, He QY, Yao KW, et al. Research on system
112. of classification and rating of clinical evidence on
12. Institute of Medicine. Clinical practice guidelines: traditional Chinese medicine. China Association for
directions for a new program. Washington, DC: Science and Technology, Fujian Provincial People 's
National Academies Press 1990: 38. Government. Transformation of economic
13. Wang SC, Yu S, Zhao X, et al. Status and strategies development mode and independent innovation——
of evidence-based guidelines for clinical practice in the 12th annual conference of China association for
traditional Chinese medicine. China Journal of science and technology (Volume III). China
Traditional Chinese Medicine and Pharmacy 2012; Association for Science and Technology, Fujian
27(11): 2759–2763. (Chinese) Provincial People 's Government: Academic
14. GRADE Working Group. Grading quality of Department of China Association for Science and
evidence and strength of recommendations. BMJ Technology 2010; 5. (Chinese)
2004; 328: 1490–1497. 23. Zhong JB. Suggestion for evaluation method of
15. Liu JP. The composition of evidence body of clinical evidence for guideline of diagnosis and
traditional medicine and recommendations for its treatment in traditional Chinese medicine. China
evidence grading. Chinese Journal of Integrated Journal of Traditional Chinese Medicine and
Traditional and Western Medicine 2007; (12): 1061– Pharmacy 2016; 31(04): 1146–1148. (Chinese)
1065. (Chinese) 24. Lv ZX, Guo Y, Chen ZL, et al. Evaluation method of
16. Chen YL, Luo XF, Wang JY, et al. How to distinguish evidence body for acupuncture and moxibustion
between clinical practice guidelines and expert clinical practice guidelines: the stratified evidence
consensus. Medical Journal of Peking Union Medical evaluation method. Chinese Acupuncture &
College Hospital 2019; 10(04): 403–408. (Chinese) Moxibustion 2018; 38(10): 1115–1118. (Chinese)
17. Xie YM, Liao X, Hu J. Technical specification for 25. Qian JH, Guo ZL. Construct a clinical evidence
“consensus” formation methods and processes in evaluation system suitable for the characteristics of
clinical practice guidelines of traditional Chinese traditional Chinese medicine. China Journal of
medicine. China Association for Science and Traditional Chinese Medicine and Pharmacy 2018;
Technology, Jilin Provincial People 's Government. 33(10): 4302–4304. (Chinese)
The 19th annual conference of China association for
Submit a manuscript: https://www.tmrjournals.com/mhm 15You can also read