THE SELF-CONCEPT OF YOUNG PEOPLE WITH SPINA BIFIDA: A POPULATION-BASED STUDY
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
THE SELF-CONCEPT OF YOUNG PEOPLE WITH SPINA BIFIDA: A POPULATION-BASED STUDY P. L . Appleton P. E. Miinchom N. C.Ellis C.E. Elliott V. Boll P. Jones This paper reports a study of self-concept However, samples have tended to be small in young people with spina .bifida. (Campbell ec al. 1977, Spaulding and Previous studies are briefly described, Morgan 1986, Lavigne et a/. 1988); hospital followed by an account of the relevance to out-patient clinic lists have been the physical disability of findings in the predominant source of samples; there developmental psychology of self-concept. have been 10 selection biases in some Interventions by professionals for studies (Campbell er a/. 1977, Spaulding physically disabled young people will need and Morgan 1986, Murch and Cohen increasingly to take account of young 1989); and theoretical models of self- people’s views of themselves, and their concept development and disability have wishes and plans for the future not been employed (Harper 1991). Thus, (Department of Health 1989). It follows for instance, while it is known that able- that the scientific study of self-concept bodied teenagers are concerned with their and self-worth in those with a physical own physical appearance and that this disability is an essential component of the factor is linked very closely to their global knowledge that professionals should be self-worth (Harter 1986), no study has using for designing multi-agency inter- identified the exact association between ventions. Young people’s overall sense of feelings about the body and feelings about self-worth, their motivation to develop the self-as-a-whole of young people with and change, the value they place on spina bifida. Until recently one problem various aspects of personal functioning, has been the lack of appropriate measuring and their sense of social identity, are all instruments. factors which are central to an under- It is now known that self-concept can standing of how best to intervene to help be broken down into dimensions (or young people with physical disabilities ‘domains’), and that children and teen- (Thomas et al. 1989) and how to provide agers can accurately assess what they feel more appropriate developmental oppor- about themselves in relation to these differ- tunities (Rutter 1987). ent domains (Harter 1986, Marsh 1989). To date, the reported studies of global We would expect that children with self-worth (or self-esteem) in spina bifida spina bifida, like able-bodied children, subjects find mean differences between would have individual areas of difficulty spina bifida and control samples to be and individual areas of success in the marginal (Campbell el at. 1977) or non- various domains of self-conceut. In existent (Spaulding and Morgan 1986). general it would be expected that, because
of difficulties with mobility, continence importance reduced.
and intellectual performance, young Harter (1986) and Crocker and Major
people with spina bifida would evaluate (1989) summarised evidence that actively
themselves relatively poorly in the domains reducing the importance of domains in
of athletic, physical and scholastic self- which people perceive themselves to be v
QI
concept. Harter (1985a, 1986, 1990) used less able, i.e. ‘discounting’, optimises Q‘
the term ‘perceived competence’ to refer global self-worth. By placing less impor-
to the evaluation the young person makes tance on (or discounting) a particular
of performance in each domain. I t would aspect of self-development, performance
be useful to know whether perceived com- failures in an identified area are no longer
petence in these key arcas is indeed lower a threat to self-worth. However, this
among physically disabled than among cognitive process could result in decreased
able-bodied young people. motivation for change and development
However, the evaluation placed on (Crocker and Major 1989).
experience or performance in a particular One of the most robust findings in the
domain of self-concept will depend on literature of self-esteem is the correlation
how important that area is to the indi- between a person’s evaluation of their
vidual personally: not being good at physical appearance and their global self-
mathematics may not affect your self- worth. Harter (1986) showed that self-
esteem if it is not important to you rated physical appearance, as one domain
(Harter 1986). of self-concept, correlates more highly
I t is essential, therefore, that self- (0.6 to 0.8) with global self-worth than
concept instruments incorporate a method does any other domain. There is also
of ascertaining the importance that a evidence that this correlation is higher for
child places on each domain, as well as a girls (Harter 1986). So how do young
self-rated measure of competence. I f people with a physical disability cope with
children feel competent in a domain the socio-cultural emphasis, especially for
which is important to them, then self- adolescent girls, on the value of physical
worth is likely t o be boosted. On the other appearance?
hand, competence may be irrelevant for From early adolescence onwards, able-
self-worth if the domain is not important bodied girls are at greater risk for low
or personally valued. Using instruments self-esteem and depression than boys
developed by Harter ( 1 9854, and Renick (Harter 19850, Petersen et al. 1991).
and Harter (1988), it is possible to Studies of self-concept in those with a
measure both competence and importance physical disability have rarely examined
for each domain. The relation between gender, perhaps because of sample-size
these two measures can then be examined. problems. It may be a salient variable,
Following William James’ notion of the acting as an effect modifier, protecting or
ratio of pretension (aspiration or impor- making the disabled child more vulner-
tance) to success (competence), Harter able. For instance, being female and being
calculated a ‘discrepancy’ score (com- adolescent (as distinct from being in
petence minus importance) to convey the middle childhood) might render the
size and direction of disparity for each physically disabled young person more
domain. Harter (1986) demonstrated a susceptible to socio-cultural norms con-
linear relationship between discrepancies cerning the importance of physical
and global self-worth, negative domain appearance.
discrepancies being associated with lower One cognitive process that could be
global self-worth. protective of self-worth is the young
’
How would a child with several areas of person’s choice of a model for comparison
difficulty cope with a range of potentially (Renick and Harter 1989). In a study by
stressful discrepancies between competence Harter (1986), there was evidence to
and importance? If the child feels less suggest that mentally disabled children
competent than peers, but experiences chose to compare themselves primarily
similar aspirations, there is a risk of low with other mentally disabled children.
self-worth. In order to regulate this, Global self-worth is also governed by
competence could be overestimated or the extent to which a young person feels 199supported and accepted by parents, worth. It was'hypothesised that, while the
teachers and peers (particularly class- relationship between discrepancies and
mates). For able-bodied children, these global self-worth would, in general, hold
associations are independent of the across groups, the physical appearance
associations between domain-specific self- discrepancy would be less strongly
evaluations and global self-worth (Harter associated with global self-worth in young
1986). For children with congenital/ people with spina bifida.
0
TJ acquired limb deficiencies, low classmate ( 5 ) To explore whether young people with
L
.-
m support is a significant predictor of low SB are more likely to compare themselves
0
.-C self-worth and depressive symptomatology with other physically disabled young
a
vl
(Varni et al. 1992). people or with able-bodied young people
This study tested a number of theor- when assessing their own competencies in
etical predictions, all of which are self-concept domains.
-a
w
relevant to the design of interventions. In (6) To study the impact of the choice of
8
a doing so, we attempted to overcome some social comparison group on self-rated
tli
C
of the methodological problems of competence and global self-worth among
7
previous studies. The objectives and young people with SB. It was hypothesised
> hypotheses were as follows. that comparing oneself with other
L
0
( I ) To examine the multidimensional physically disabled young people would
structure of self-concept in young people be associated with higher competence
with spina bifida (SB) and to compare it scores than when comparing oneself with
r: with that of able-bodied (AH) young AH peers.
vl people who have no known learning (7) To study young people's perceived
difficulties. social support as a function of group, age
(2) To study and compare young people's and gender; to investigate the association
self-rated competence in each of nine self- between social support and global self-
concept domains and in global self-worth, worth.
and to examine the effects of age and
gender on the above measures. In line Method
with the preceding discussion, it was For the purposes of this study, spina
hypothesised that there would be group bifida was defined as open or closed
(AB>SB), gender (M>F), and age (Y>O) myeiomeningocele, with or without
main effects for social acceptance, athletic associated hydrocephalus, with or
competence, physical appearance and without ventricular drainage. All patients
global self-worth. We expected older girls had measurable functional impairment of
with spina bifida to have the very lowest locomotion, continence, intellect or
scores in these domains and in overall physical parameters associated with the
self-worth. spina bifida. They were aged between
(3) To study the personal importance or seven years and 18 years 1 1 months. The
value which young people place on each diagnosis was confirmed in all cases with
self-concept domain, comparing groups, the young person's own medical advisers
and examining the effect of age and and/or by review of the medical notes.
gender. In order to examine the possibility Case notes were obtained in order to
of discounting, it was hypothesised that clarify points in the history and on cases
group would be a main effect (SB < AB) in not seen clinically.
all academic, physical appearance and
athletic domains, with the exception of Subjects .
older girls with spina bifida, among Recruitment for the study was from the
whom the importance of physical appear- adjoining health authority catchment
ance and athletic competence would be at areas of Clwyd, Wirral, Chester and
the same mean levels as AB. Crewe. In order to get as complete a
(4) To study the discrepancies between sample as possible, extensive investigations
importance and self-rated competence in were made with consultant paediatricians,
each domain by group, age and gender, clinical medical officers, the Association
and to investigate the degree to. which for Spina Bifida and Hydrocephalus
200 these discrepancies determine global self- (ASBAH), and the Family Fund (a UKTABLE I -
n
N
Demographic characteristics of study sample 03
0'
Conlrols Spina bi/ida Rejusals
(N= 79) (N= 79) ( N = 17)
Age (yrsmkhhs)
Mean 13:) 13:7 12:ll
SD 47 38 21
Gender
Male 38 38 7
Female 41 41 10
Education/work status
Mainstream 63 49 7
Special school 0 17 8 2
Residential college 0 4 0
Mainstream co,llege 9 1 1
College (SND) 0 3 0
Not in education 7 5 I
'SND= special needs department.
national register of families with a the medical interview, and three further
disabled child claiming a specific benefit). subjects did not receive the medical
All eligible subjects were approached in interview for administrative reasons, but
the first three areas from which ascer- in all these cases the medical records
tainment data were available; in the final enabled a disability severity score
area, subjects were approached on the (Wallander e l a/. 1989) t o be calculated.
basis of random selection to complete our The remaining 70 received detailed
sample. A total of 104 subjects were clinical assessment.
approached. Medical assessments were performed by
Seventeen families indicated that they five assessors (P.E.M.,G.c., v.K., R.P.,R.B.),
did not wish to participate in the research, in a clinical setting rather than at home.
and a further eight children were excluded If there was doubt about details in the
due to either apparent severe cognitive history, these details were verified from
impairment or severe family distress. This medical notes. Generally, parental recall
left 79 cases in the sample. proved accurate. For those nine patients
For each subject with spina bifida we not examined clinically, as much infor-
obtained a comparison subject, matched mation as possible was collated from their
for age (plus or minus six months), gender, hospital and community medical records.
classroom and housing neighbourhood. The medical assessment comprised a
Comparison subjects were selected from detailed medical history, questions on
the same mainstream classroom as that aspects of physical ability and indepen-
attended by the student with spina bifida dence (including continence and
or, in the case of older subjects, from the mobility), a full physical examination and
same/similar workplace, college or em- neurological assessment, and vision and
ployment training scheme. If the child hearing screening.
with spina bifida was not in mainstream
education, the comparison subject was DISABILITY SEVERITY SCORE
chosen from an appropriate local school. Clinical severity for thoracic, lumbar and
The comparison subjects had no known sacral lesions was quantified following the
chronic illness, disability or special criteria of Wallander el al. (1989), who
educational need (Table I). defined the degree of severity of spina
bifida according to six medical parameters
Medical assessment (Table 11). The score was not designed to
The sample comprised 79 pairs of include cervical lesions, and therefore the
subjects. Six subjects chose not t o have three cervical cases have been exctuded. 201TABLE I I
Medical parameters assessed for Wallander and colleagues' severity score
Parameter Disability Clinically Total
score evaluated sample
(N 70)
2 ( N = 79)
h' (%I N (To)
Level o j lesion
Sacral 0 I I (16) I I (14)
Lumbar I 26 (37) 32 (41)
Thoracic 2 30 (43) 33 (42)
Cervical 3 (4 3 (4)
Operations jor ventricular valve
None 0 18 (26) 23 (29)
I I I I (16) I2 ( I S )
22 2 41 (59) 44 (56)
Operationsfor skin ulcer below waist
None 0 61 (87) 69 (87)
21 2 9 (13) 10 (13)
Total surgical operations required
Sone 0
1-2 I
23 2
Level oJ' independent amhulation
No aids 0 16 (23) 18 (23)
Braces I 31 (44) 36 (46)
Wheelchair or carried 2 23 (33) 25 (32)
Bladder junction
Continent 0 14 (20) 16 (20)
Cat heterised I 43 (61) 48 (61)
Collection device 2 I! (19) IS (19)
*Yo1 applicable to cervical lesions.
PCLTIBECED SEVERITY SCORE between 17 years and 18 years 11 months,
This functional severity assessment, the WAIS-R. The short form comprised
originally devised by Lindon (1963), was Arithmetic, Vocabulary, Picture Arrange-
used in the modified form described by ment and Block Design for both the
Thomas et al. (1989). I t is not specific to WISC-R (Kaufman 1976, 1979) and the
spina bifida. It uses a scoring of 12 items WAIS-R (Silverstein 1982, 1987). In
(Table 111). scored from 1 to 4 according addition, all children were administered
to defined degrees of severity. Digit Span.
The disability can be graded in a
number of ways, according to (a)the total THE REY AUDITORY LEARHING TEST
number of problems across the scales, (b) This test (Rey 1958, Lezak 1983), admin-
whether the main disabilities relate to istered, to all children, involved presen-
physical function (items 1 to 5 , 11 and 12) 'tation of a 15-word list for five trials with
or behavioural or communication diffi- free recall after each trial. A second
culties (items 6 to lo), and (c) the 15-word (interference) list was then pre-
functional severity of the problem. sented once for free recall, immediately
followed by an unprompted recall trial
Psychological interview and a recognition trial for the first list.
As part of an interview, we used the Recorded responses were scored for
revised versions of the Wechsler lntelligence words correctly recalled, repeats and
Scale for Children (wISC-R) and the intrusions.
Wechsler Adult Intelligence Scale (WAIS-R).
All children received a four-subtest THE SELF-PERCEPTION PROFILE FOR
short form of the age-appropriate test: up L E A R N I N G ~ I S A B L E STUDENTS
D (HSPPLDS)
202 to 16 years ll'months, the WISC-R; and This self-report instrument (Renick andTABLE I l l
N
Capacity assessed for Pultibeced Severity of Disability Score (N=70) I
00
Q’
Severrry Crude 6
M
I 2 3 4
h’ (%) N (To) N (070) N (4’0)
-
Physical capacity 24 (34) 23 (33) 20 (29) 3 (4)
Upper limbs-arms 49 (70) 17 (24) 4 (6) 0 (0)
Upper limbs-hands 36 (15) 33 (47) 1 (I) 0 (0)
Locomotion 4 (6) I 5 (21) IS (21) 36 (51) 2
Toileting 10 (14) 4 (6) 34 (49) 22 (31)
Intellectual function 5 (7) 43 (61) 16 (23) 6 (9) G
Behaviour 41 (59) 8 (11) 21 (30) 0 (0)
Eyesight/vision 41 (59) 14 (20) 10 (14) 5 (7)
Communication-speech 61 (87) 9 (13) 0 (0) 0 (0)
Communication- hearing 65 (93) 3 (4) I (1) I (1)
Eating and feeding 66 (94) 4 (6) 0 (0) 0 (0)
Dressing 36 (51) 5 (7) 26 (37) 3 (4)
Harter 1988) is based on the Self- tered to young people aged nine years and
Perception Profile for Children (Harter over. This questionnaire asks children to
19850). It is designed for the assessment identify how important each of the nine
of learning-disabled and normally achiev- domains of self-concept is to them per-
ing children’s domain-specific judgements sonally. Items are scored on a four-point
of their competence or adequacy in nine rating scale; high scores indicating greater
self-concept domains, and their feelings perceived importance and low scores
of global self-worth. The instruments representing lesser perceived importance.
have well established validity and re- For calculation of importancdcom-
liability (Harter 1985~.Renick and Harter petence discrepancy scores, Renick and
1988). The 10 subscales independently tap Harter (1988)-advised a cut-off of 3 on the
children’s self-perceptions in the follow- four-point importance scale. Discrepancy
ing areas: (1) general intellectual ability, scores (both domain-specific and overall
(2) reading competence, (3) spelling discrepancy) therefore represent data
competence, (4) writing competence, ( 5 ) solely on those domains in which indi-
mathematics competence, (6) social vidual children place special personal
acceptance, (7) athletic competence, (8) importance. Discrepancy scores were
behavioural conduct, (9) physical appear- calculated by subtracting importance
ance, and (10) global self-worth. The ratings from their respective competence
separate domains for specific academic scores. In most cases this value was
areas have been found to be useful for negative, since importance ratings tend to
children with specific learning difficulties. be higher than competence scores. A
Children were asked to evaluate their mean discrepancy score was calculated by
perceived competence by completing three taking the sum of the discrepancy scores
separate questionnaires entitled, ‘What I and dividing by the number of domains
am like-first presentation’ (self-ratings rated as important.
of competence in each self-concept
domain), ‘Who I am like’ (specification THE SOCIAL SUPPORT SCALE FOR
of chosen comparison group for each CHILDREN (SSSC)
domain), and ‘What I am like-second This scale (Harter 19856)’ of well estab-
presentation’ (repeated competence ratings lished reliability and validity, measures
based on the comparison group not used the degree to which others like the child
in the first presentation of the scale). the way he or she is, treat the child like a
A questionnaire entitled, ‘How impor- person, care about his or her feelings, and a
tant are these things to how you feel about act as if they feel that the child matters.
yourself as a person?’ was thgn adrninis- The four sources of social support or 203i
positive regard in this instrument are information was not available in two
z
CJ parents, teachers, classmates and close cases. At birth, six of the lesions were
friends. Each item is scored on a scale of covered by skin. 47 of the open lesions
1 to 4, I representing the lowest level of were operated on within the first week of
support and 4 representing the highest. life. Hydrocephalus was present in 56
The format is similar to the i1SPPI.DS. cases, of whom 52 had valves in sifu.
Three patients with hydrocephalus had
m
'13 Orher measures and inlerviews not had valves inserted, and one had had
w
The psychological interview also involved the valve removed.
m quantitative measures of depression and
.-cn
v)
coping not reported here. A qualitative SUBSEQUEST SURGERY
section allowed young people to reflect on Details of orthopaedic, urological and
--
5
3 the development of their relationships. other surgery were collected. Patients had
Separate interviews were conducted with a total number of surgical procedures
parents or carers, and an occupational ranging from 0 to 36 (mean 8.2), with 53
00
C
therapy assessment was offered to a having five operations or more and 21
2
0 subsample of young people. These data having 10 operations or more.
t. will be the subject of further papers.
%-
0 SUBSEQUENT MEDICAL PROBLEMS
Procedure A variety of medical problems were
The research was agreed by the Research recorded. 1 1 patients had had seizures at
Ethics Committees of all participating some stage and four were currently
health districts, and directors of education regarded as epileptic. Elevated blood
gave their consent to the research being pressure was noted in three patients.
conducted in participating schools. If the
family indicated that they were willing to MOBILITY
take part in the study, written consent was Sixteen walked independently and required
then obtained from both the young no bracing. 23 were dependent on wheel-
person and the parent or guardian. chairs. 52 young people required a
Psychological data were collected by manual wheelchair for at least part of the
four graduate research assistants, specially time, and six had the use of electric
trained in interviewing skills. Extensive wheelchairs. 20 of the wheelchair users
training was given to the interviewers on were unable to transfer independently.
the administration and scoring of the
WISC-R and WAIS-R under the supervision URINARY CONTINENCE
of C.E.E. Practice interviews (using video Sixteen cases were fully continent and 15
cameras and one-way mirrors) were totally incontinent. The majority, 41,
completed with volunteer subjects before appeared to be managing their continence
the interviewing of research subjects took independently. Intermittent catheterisation
place. Interviews were carried out in a was used by 39 and long-term catheter-
confidential setting within the school/ isation by five. Six patients had artificial
college/workplace. Four older subjects urinary sphincters. Four had urinary
who were living in a residential college for ' diversions.
young people with special needs preferred
a home-based interview. BOWEL CONTINENCE
Twenty-four cases were fully continent,
Results with 36 soiling intermittently and 10
Physical findings totally incontinent. 29 managed their
An outline of the medical findings, levels bowels independently.
of mobility and continence is shown in
Table 11. CLINICAL FINDINGS
Problems relating to the skin (ulceration,
' INITIAL MANAGEMENT oedema, poor circulation) were found in
In only two cases had there been an ante- 48 patients.
natal diagnosis of s ~ In. 66 cases there Spinal deformity was present in 47
204 had been no diagnosis before birth, and cases. Though most spinal scars wereTABLE IV
Mean short-form IQscores for both groups
Score Controls Sph P
Mean (SO) bifda
Mean (SO)
.-
Estimated IQ 100.8 (14.;) 78.9 (17.9)-
4
L
U TABLE V I
Self-rated competence measures (llarter SelEPerccption Profile for Learning-Disabled
Students)
Competence doniain Controls .Spina bifida Paired-t test p
Mean (SO) Mean (SD! I (dfl
i
a General intellectual ability 2-87 (0.56) 2.66 (0.71) 2-12 (78) 0.04
0
0 Reading competence 3.28 (0.72) 2.92 (0.86) 3.00 (78) 0.004
.-
b Writing competence 2.05 (0.83) 2.55 (0.88) 2.99 (78) 0.004
m Spelling competence 3.03 (0.80) 3.00 (0.97) 0.22 (78) 0.83
.-2
Maths competence 2.85 (0.83) 2.36 (0-94) 3-42 (78) 0-001
c Social acceptance 3.30 (0.57) 3.03 (0.80) 2.39 (78) 0.02
rn Athletic competence 2.70 (0.76) 2.27 (0.84) 3.39 (78) 0.001
Behavioural conduct 3.06 (0.63) 2.95 (0.78) 1.06 (78) 0.29
Physical appearance 2.74 (0.67) 2.65 (0.91) 0.82 (78) 0.42
0, Global self-worth 3.17 (0.58) 2.98 (0.78) 1.69 (78) 0.10
n
8
P
b
0
e
41 and stable across groups. The scales were
c
0
U therefore appropriate for this study popu-
zY lation, and the scoring system recom-
c mended by Harter to derive subscale
!2 scores was also appropriate.
COMPETENCE (HSPPLDS)
We conducted I tests for related samples,
comparing groups. As can be seen from
Table VI, young people with spina bifida
regarded themselves as less competent
than did controls in four of five academic
domains. Mathematics competence was
"
Females Males regarded as low, both when compared
with control scores and when compared
M S p i n a bifida m A b l e - b o d i e d
with other domains. Young people with
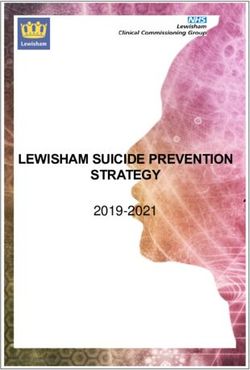
Fig. 2. Imporlance o j physical appearance as a spina bifida also regarded themselves as
function of group and gender (IISSPLDS).
less socially accepted and less athletically
competent than did controls. At this level
of analysis there were no group differences
evident in the domains of behavioural
41
conduct, physical appearance or global
self-worth.
ANOVAS were conducted for each
domain, allowing us to study the impact
of gender and age (greater vs. less than
160 months), as well as group. In addition
to the group effects there were gender
main effects (hl>F) for athletic com-
petence (b11,150)= 13-75, p F) (F(1,150) =
13.01, p M ) (F(1,150)=7.77, pc0.01) and
" Young Young Older 0:der global self-worth (F(1,150)=5.19, p <
females males lema!es males 0.05). In the area of global self-worth,
M S p t n a btftda BAbIe-bodied not only did gender appear as a main
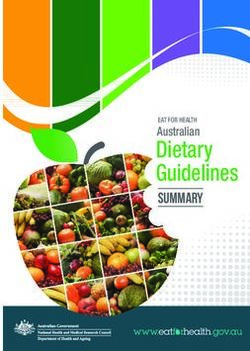
Fig. 3. Importance o j physical appearance as a effect-girls demonstrating lower self-
206 junction of group, age and gender (HSSPLDS). worth than boys-but a significant three-TABLE VII v)
Self-rated importance measures (Harter Self-Perception Profile for LearningDisabled
Students)
~
a-
m
Comperence domain Controls Sprna brfida
Mean (SO) Mean (SD)
General intellectual ability 2.93 (0.86) 3.03 (0.92) 0.66 (71) 0.51
Reading competence 2.92 (0.81) 3.03 (1.001 0.70 (71) 0.48
Writing competence 2.72 (0.78) 2-85 (1.01) 0.88 (71) 0.38
Spelling competence 2.83 (0-91) 3.11 (0.89) 1-91 (71) 0.06
Marhs competence 2-81 (0.91) 3.03 (0,971 1.39 I711 0.17
Social acceptance 2.87 (0.811 3.07 (0.89) 1 . 5 1 (71) 0.14
Athletic competence 2.51 (0-96) 2-33 (1.05) 1.25 ( 7 1 ) 0.22
Rehat ioural conduct 3.35 (0.68) 3.42 (0.71) 0.56 (71) 0.58
Physical appearance 2.90 (0.81) .3.03 (1.07) 0.96 (71) 0-34 P
way interaction was also evident between athletic competence, there was a highly
group, age and gender (F(1,150)=3.75, significant age effect (F(1,137) = 14.75,
p = 0.055). Examination of the tabulated pCO-OOl), older children feeling that this
three-way ANOVA interaction indicated area was less important to them. In
that older girls with spina bifida had the addition, there was a gender x age effect
lowest mean self-worth scores and young (1.11,137)=4.80, pp M )
for physical appearance (~11.92)= 8.12,
pTABLE V l l l -
vl
N
Spearman rho correlations between domain discrepancy scores and m
I
global self-worth 0'
~~ ~~
Domain A l l subjects Control
group m
d
m
General intellectual ability 0.34 0.31 0.35
(96)' (46) (50)
pTABLE X
Effects of different comparison groups on competence scores (HSPPLDS) of joung people with spina bifida
-
e
0
h Domoin Non -disabled Dira bled d Paired i iesi P
3
T
Meun (SO) Meun (SO) i (dj)
General intellectual ability 2.59 (0.82) 3.04 (0.89) 0.45 4.60 (76) 0~0001
Reading competence 2.87 (0.95) 3.12 (0.97) 0.25 2.06 (77) 0.04
Maths competence ' 2.34 (1.00) 2.70 (1.08) 0.36 3.07 (75) 0.003
Social acceptance 2-96 (0.83) 3.10 (0.83) 0.14 1-46 (74) 0.15
Athletic competence 2-07 (0.81) 2-70 (0.93) 0.63 7.13 (76) 0.001
Behavioural conduct 2-94 (0-84) 2.95 (0.83) 0.01 0.17 (73) 0.86
Physical appearance 2.61 (0.91) 3.06 (0.88) 0.45 5.12 (77) 0.001
Global self-worth 2.88 (0.77) 3 . 1 7 (0.73) 0.28 4.36 (75) 0.001
TABLL XI
Scores on Harter Social Support Scale for Children
Conirols Spino hrjido Poired I iesi p
Mean (SO) Meon (SO) i (df,
--
Parental support/regard 3.55 (0.56) 3.49 (0.61) 0.69 (78) . 0.49
Classmate supportlregard 3.38 (0.44) 3.05 (0.66) 3.41 (78) 0.001
Teacher support/regard 3.27 (0.56) 3.46 (0.59) 2.18 (78) 0.03
Close friend supportlregard 3-53 (0-61) 3-57 (0.58) 0.53 (78) 0-59
themselves with able-bodied peers across except spelling and writing. The data in
all domains. This finding may well reflect Table X show that the subjects felt
the fact that 74 per cent of the physically relatively less competent in academic,
disabled subjects were in mainstream athletic and physical appearance domains
schools. An analysis by school placement when comparing themselves with able-
shows that those young people who were bodied peers than when comparisons were
in a special school were much more likely made with other disabled young people.
to compare themselves with physically The same effect was evident in global self-
disabled peers, whereas those in main- worth. No significant differences were
stream schools were very much more found in the areas of social acceptance
likely to compare themselves with able- and behavioural conduct.
bodied peers. For instance, in the domain In summary, hypothesis 6-that com-
of general intellectual ability, 43 of 49 parison with other physically disabled
young people in mainstream schools young people would be associated with
compared themselves with able-bodied higher competence scores-wa$ largely
peers, in contrast to four out of 16 in confirmed. However, the majority of the
special schools (x2(2)=26.26, pC0-001). disabled group spontaneously compared
The mean scores for the non-disabled themselves with able-bodied peers, an
controls were close t o the mean com- effect associated with being in mainstream
petence scores shown in Table VI. a school.
further indication of the reliability of
response in the spina bifida group. Young SOCIAL SUPPORT (SSSC)
people with spina bifida were asked to We conducted f tests for related samples,
rate themselves again o n the HSPPLDS comparing the groups for different
using a comparison group which they had aspects of social support. As can be seen
not chosen on the first occasion. The from Table XI, young people with spina
210 second presentation tapped all domains bifida felt equally as supported by parentsand friends as did their able-bodied peers. TABLE XI1
This contrasted with the finding for Spearman rho correlations between sources of social
classmate support (SB < AB). A significant support and global self-worth
difference in the opposite direction was W
0
Spino brjida Controls
found for teacher support (SB > AB). (N = 79) ( N - 79)
Three-factor ANOVAS were conducted
to investigate the effects of group, gender Parental support 0.42 0.26
and age. For parental support there was a po) (F(1,150)= Classmate support 0.28
p=0*014
0.15
p=0.175
5.72, p < 0 . 0 5 ) and an interaction of Teacher support 0.30 0.05
groupxgender (fll.150)=5.69, p < p = 0.006 p = 0.686 2
0.05). girls with spina bifida reporting Close friend support 0.20 -0.12 2
significantly less parental support than p : 0.083 p=0.283 g
others. For teacher support, there was a 0,
E
main effect for age ( Y > 0 ) (~11,150)= 2
h
5 - 5 3 . pdefences we examined. In fact, given the relationship, i.e. that with a parent. This
group differences in discrepancies, and perception could be based on feelings of
the correlations between discrepancies ‘not being worthy of love’. I t is not
and global self-worth, it is surprising that possible to discriminate between these
global self-worth was not lower in the possibilities with the current data set.
young people with spina bifida. Several It is not at all clear why correlations
points are relevant. First, as noted above, between social support and global self-
the most powerful disability effects in this worth were attenuated for able-bodied
study were those that emerged in inter- children. These findings are different
m action with gender, rather than main from published data on US samples
.-C
P
cn effects. Second, Harter (1986) viewed (Harter 19856). Support from parents,
global self-worth as a ‘core variable’, in- teachers and classmates were significantly
fluenced by (and presumably influencing) correlated with global self-worth in the
a wide range of component parts of the disabled group.
person’s psychosocial experience. Un- Harter (1986) regarded self-concept
to
C
measured compensatory factors in the domains and social support areas as
a experience of the physically disabled independent variables, predictive of global
0
L
group may have been important, and self-worth. It seems to us that, with
0
possibly would have emerged in a current information, it is equally plausible
qualitative study. Third, an over-emphasis that global self-worth has reciprocal
on group difference methodology influence on specific domains and per-
precludes investigation of factors within ceived support. For instance, low support
the spina bifida group that promote or may indeed cause a lowering of self-
impede the development of optimum self- worth, but low self-worth may in turn
esteem. A series of studies of psychosocial cause the disabled young person to attend
adjustment in physical disability by selectively to negative aspects of experience
Wallander and others’(see review by Varni (Gotlib and Hammcn 1992) such as
and Wallander 1988) has used a within- scholastic problems and problems of
group design. physical appearance, thereby setting in
It is encouraging that, on a simple motion cognitive-interpersonal negative
group-comparison basis, the young chain-reactions (Rutter 1987). i.ongitudina1
people with spina bifida felt equally as and intervention research designs are
supported by friends and parents as their required to address these questions.
able-bodied peers. The disabled group felt What are the implications for prac-
more supported by teachers, perhaps an titioners? First, that the use of instru-
effect associated with the special classes ments such as the HSPPIBS can be useful
and greater amount of individual as part of multidisciplinary assessment.
attention required by a physically disabled The primary focus of assessment, around
child. It is of concern that disabled girls which other assessments are built, must
appeared to feel less supported by parents now be the young person’s own view of
than did able-bodied children and dis- his or her life situation, wishes, interests
abled boys. This finding requires and plans (Department of Health 1989).
replication, but is another indication of Tools such as the HSPPLDS allow prac-
the importance of gender as a potential titioners to plan management, and
effect modifier in psychosocial aspects of evaluate change and outcome, using
physical disability. If the finding is not variables that are relevant to the young
spurious, then at least two causal interpre- person. Treatment plans failing to take
tations are possible. First, disabled girls account of these fundamental sources of
may objectively be more difficult to care motivation are likely to prove less fruitful
for in adolescence because of their (Harter 1991).
relatively low self-esteem and associated Second, peer social acceptance and
factors, leading to a relative reduction in social comparison appear to be key issues.
received parental support. Second, because Work with the able-bodied peer-group
of low self-esteem, the disabled girls may itself can be valuable (e.g. Armstrong ef
perceive themselves as receiving less al. 1987). Work with disabled young
212 support from the most important close people o n social skills (Inderbitzen-Pisaruk and Foster 1990) must recognise (Department of Health 1989), on self-
the distinction between individual perceptions of the body and how these are
friendship-making skills, and the linked, in each case, to overall self-
experience of feeling ‘part of’ a peer esteem. Such cognitive-behavioural work
group (Parker and Asher 1993). Our data, (Harter 1991, Gotlib and Hammen 1992) i
01
and Harter’s data (1986) on able-bodied may be viewed as a first stage, or Q‘
children, suggest that the latter set of foundation stage, out of which the young
group processes is as important as indi- person may wish to engage in specific
vidual friendships, if not more so. Much pieces of collaborative work on self-care.
is known about the cognitive and social
aspects of group integration (see Turner Accepied for publication 81h August 1993.
1991); application of this knowledge to
Acknowledgements -
special-needs settings is important. ‘By the We are very grateful to the young people and P
time children reach adolescence, peer families who participated in the study. We are
group identities and the feeling of being grateful to ASBAH for generous funding, and
ctrong interest and support. Clwyd Social Services
part of a larger community are very and Clwyd Health Authority also provided funding.
important aspects of the young person’s Research Assistants Val Lawson. Colin Clerkin,
life (Widdicombe 1988, Parker and Asher Ann Llewelyn and I’rish Gilroy, and Medical
Interviewers Dr Val Klirnach, Dr Gill Clements, Dr
1993). Robert Pugh and Dr Roger Blackmore. made the
Finally, it is clear that the young study possible. Participating schools were interested
and supportive. Dr Martin Rax, Medical Adviser to
person’s self-perception of physical ASBAH. was most helpful, especially in the early
appearance may need addressing as part planning stages of the project. Parts of this paper
of an overall intervention programme. were reported at the European Academy of
Childhood Disability, Italy, 1992.
While it may be true that physically
disabled young people find other sources Auihors ’ Appointments
of reward in their lives, there is little ‘Peter Appleton, Clinical Psychology Services
doubt that many (especially girls) are Manager;
Colin Elliott. Principal Clinical Psychologist,
distressed by their physical disabilities and Wrexham Child and Family Service;
appearance. This will have specific impli- Clwydian Community Care.
cations for attitudes towards developing Philip Minchom. Consultant Paediatrician,
Wrexham Maelor Hospital.
continence and other self-care skills. I f Nick Ellis, Senior Lecturer in Psychology,
young people have negative perceptions University of Wales, Bangor.
Vicki Boll. Team Manager, Child Health and
of their physical appearance, and this is Disability Service;
closely tied to their overall view of them- Pat Jones, Rehabilitation Officer;
selves, motivation for self-care pro- South Divisions, Clwyd Social Services.
grammes is likely to be low. Therapists’
*Correspondence lo firs1 author at Wrexham
attention should therefore focus, in Maelor Hospital. Croesnewydd Road, Clwyd. Wales
partnership with the young person LL13 7TD, UK.
SUMMARY
Seventy-nine young people with spina bifida were given a psychological, medical. carer and
occupational therapy assessment. 79 matched able-bodied young people received the psychosocial
interview. The disabled group felt themselves to be less competent in academic, athletic and social
aspects of self-concept, less supported by classmates, equally supported by parents and friends and
more supported by teachers than the able-bodied group. Disabled subjects did not discount the
importance of any area of personal-social functioning, and experienced greater discrepancies between
competence and importance in most academic, athletic, social and physical appearance aspects of
self-concept. Disabled girls assigned very high importance to physical appearance. Physical
appearance was more strongly associated with general self-esteem than any other area of
self-concept.
RGSUMG
L ‘appreciation de soi de jeunes spina bifida: une elude de population
Une entrevue concernant les aspects psychologiques, medicaux de prise en charge de soins et de
reeducation a ete proposee a 79 jeunes spina bifida. La mOme entrevue psychosocial fut proposke a
79 jeunes sujets valides apparies. Les mcmbres du groupe avec incapacites, se sentaient moins
competents dans une auto-evaluation sur les aspects scolaires. athletiques et sociaux, moins aidCs par
leurs camarades de classes, egalement aides par leurs parents et amis, et mieux aides par leurs
professeurs que les jeunes du groupe de valides. Les sujets avec incapacites en minimisaient
I’importance d’aucun aspect de I’activite individuelle et sociale, et faisaient une plus grande . 213distinction entre competence et importance dans la plupart des aspects d’auto-evaluation sur les do-
maines scolaires, sportifs, sociaus et d’apparence physique. Les filles avec incapacites attribuaient
une tres grande importe h I’apparence physique. L’apparence physique etait plus fortement associee
avec I’estime d e soi generale qu’i n’import quelle autre aspect d’auto-evaluation.
ZUSAMMENFASSUNG
Die Selbsteinsciibt:img junger Leute niit Spina byida: eine Populationssludic
79 junge Leute mit Spina bifida wurden anhand von Interviews beziiglich ihrer psychologischen,
tnedizinschen, pflegerischen und beschaftigungsthcrapeutischen Situation befragt. 79 gesunde
Kontrollen wurden mit einem psychosozialen Interview untersucht. Die behinderten Probanden
fuhlten sich in akademischen, sportlichen und sozialen Bereichen weniger kompetent, durch
Klassenkameraden weniger, durch Eltern und Freunde gleich und durch Lehrer mehr unterstutzt als
die gesunden Kindern. Die behinderten Patienten waren sich der Bedeutung der allgemeinen
psychosozialen Eingliederung bewuflt und machten die Erfahrung groflerer Diskrepanzen zwischen
ihren Fahigkeiten und der Bedeutung, die sie den meisten akademischen, sportlichen, sozialen und
korperlichen Erscheinungsbildern in ihrer Selbsteinschatzung zuschrieben. Behinderte Madchen legten
sehr grossen Wert auf die korperliche Erscheinung. Umgekehrt war die korperliche Erscheinung
starker mit dem allgemeinen Selbstwertgefuhl vernknupft als irgendein anderer Bereich der
Selbsteinschatzung.
RESUM EN
A irtoconcepto de jovenes con espina bi5da. Estudio de poblacion
Setenta y neuve jovenes con espina bifida pasaron una entrevista psicologica, medica, de cuidador y
de terapia ocupacional. Otro grupo de 79 jovenes sin minusvalencia fisica pasarori por una entrevista
psicosocial. El grupo con minusvalencia se sentia menos competente en 10s conceptos academico,
atletico y social d e su autoconcepto menos apoyados por 10s compalleros d e clase, igualmente
apoyados por padres y amigos y m i s apoyados por 10s profesores, que el grupo sin minusvalencia.
Los individuos minusvalentes no descontaban la impoitancia de ninguna area del functionamiento
personal y social y experimentaban grandes discrepancias entre la competencia y la importancia de la
mayoria de 10s aspectos academicos, atleticos, sociales y aspecto fisico del autoconcepto. k.as chicas
minusvhlidas daban una muy gran importancia al aspecto fisico. El aspecto fisico estaba mas
fuertemente asociado con la autoestima en general, que con cualquier otra area del autoconcepto.
References
Armsrrong, K. W., Rosenbaum, P. I . . . King. S. 31. A . (Ed. 1 Chtlditood Assessnrent: Through the
(1987) ‘A randomized controlled trial of a ‘buddy’ Eyes of a Child. Boston, MA: Allyn & Bacon.
programme to improve children’s attitudes -- (1991) ‘Developmental differences in the nature
toward the disabled.’ Developnrental Medicine of self-representations: implications for the
and Child Neurology. 29, 327-336. understanding, assessment. and treatment of
Campbell, M. M., Hayden. P. W., Davenport. maladaptive behaviour.’ Cognitive Therupy und
S. L. t i . (1977) ‘Psychological adjustment of Research, 14, 113-142.
adolescents with myelodysplasia.’ Journal of Hinde. R. A.. Dennis, A. (1986) ‘Categorizing
Youth and Adolescence. 6, 397-407. individuals: an alternative to linear analysis.’
Crocker, J . , Major, B. (1989) ‘Social stigma and International Journal of Rehavioitral Develop-
self-esteem: the self-protective properties of ment. 9, 105-1 19.
stigma.’ Psychological Review. 96,608-630. Inderbitzen-Pisaruk, H., Foster, S. I.. (1990)
Cull. C., Wyke, M. A . (1984) ‘Memory function of ‘Adolescent friendships and peer acceptance:
. children with spina bifida and shunted hydro- implications for social skills training.’ Clinical
cephalus.’ Developmental Medicine and Child Psychology Review, 10, 425-439.
Neurology, 26, 177- 183. Kaufman, A. S. (1976) ‘A four-test short form of
Department of Health (1989) Children Acr Guidance the WISC-R.’ Contemporary Educational ’
and Regulations, Vol. 6: Children with Dis- PSychology, 1, I 80- 196.
abilities. London: HMSO. - (1979) Intelligence Testing with the WISC-R.
Gotlib, 1. ti., Hammen, C. L. (1992) Psychological New York: John Wiley.
Aspects of Depression: Toward a Cognitive Lavigne, 1. V., Nolan, D., McLone, D. G. (1988)
Interpersonal Integration. Chichester: John Wiley. ‘Temperament, coping, and psychological adjust-
Harper, D. C. (1991) ‘Paradigms for investigating ment in young children with myelomeningocele.’
rehabilitation and adaptation to childhood dis- Journal of Pediatric Psychology, 13, 363-378.
ability and chronic illness.’ Journal of Pediatric Lezak. M. D. (1983) Neuropsychological Assess-
Psychology, 16. 533-542. ment. 2nd Edn. New York: Oxford University
llarter, S. (1985a) Manual for the Self-Perception Press.
Profile for Children. Denver: University of Lindon, R. L. (1963) ‘Pultibec system for the
Denver Press. medical assessment of handicapped children.’
- ( 1 9856) Manual for the Social Support Scalefor Developmenral Medicine and Child .Veurology. 5.
Children. Denver: University of Denver Press. 125-145.
- (1986) ‘Processes underlying the construction. Lord, J.. Varzos. N.. Behrman. B., Wicks. J.,
maintenance, and enhancement of the self- Wicks, D. (1990) ‘Implications of mainstream
concept in children.’ I n Suls, J., Greenwald, A . classrooms for adolescents with spina bifida.’
G . (Eds.) Psychological Perspectives On The Sey. Developmental Medicine and Child Neurology.
Vol. 3. London: Erlbaum. 32, 20-29.
- (1990) ‘Issues in the assessment of the self- Marsh. H. W. (1989) ‘Age and sex effects in multiple
214 concept of children and adolescents.’ In La Greca, dimensions of self-concept: preadolescence toearly adulthood.’ Journal of Educational ~sychology,43, 7 14-721.
Psycholo,~y.81, 417-430. Spaulding. 13. R., Morgan, S. B. (1986) ‘Spina bifida
Murch, R. L.. Cohen. L. H . (1989) ‘Relationships children and their parents: a population prone to
among life stress, perceived family environment, family dysfunction’?’ Journal of Pediatric
and the psychological distre5s of spina bifida PSyChology, I I , 359-374.
adolescents.’ Journal of Pediarric Psychology. 14, Thomas. A. P.. Has, M. C. 0.. Smyth, D. P. 1..
193-214. (1989) 7he Health and Social Needs of Y O U I I ~
’arkcr, J . G., Asher, S. K. (1993) ‘Friendship and Adults wirh Physical Disabiliries. Clinics i n
friendship quality in middle childhood: links with De\’elopmental Medicine. No. 106. London: Mac
peer group acceptance and feelings of lonelincss Keith Press.
and social dissatisfaction.’ Developtrrenial Turner, J. C. (1991) Social Injluence. Milton
Psychology. 29, 4. 61 1-621. Keynes: Open University Press.
’earson. A . M. (1985) 7he self-concepr o j i’arni, J . W., Wallander, J. L. (1988) ‘Pediatric
adolescen/s wi/h spina bi’ftda. (Thesis .) Un iversi t y chronic disabilities: hemophilia and spina bifida
of London, Institute of Education. as examples.’ I n Routh. D. K. (Ed.) Handbook of
Perersen. A. C., Sariyiani, P. A.. Kennedy, R. E . Pediatric Psychology. New York: Guilford Press.
( I Y Y I ) ‘Adolescent depression: why more girls?’ - Rubenfield, M. A,, Talbot. D., Setoguchi, Y .
Journal o j Youth and Adolescence, 20, 247-27 I . (1989) ‘Determinants of self-esteem in children
Pope, A. W.,Mctlale, S. IM., Craighead, W. E. with congenital/acquired limb deficiencies.’
( 1988) Self-esreem Enhancement with Children De velopmenral and Beha vioural Paediarrics. 10.
and Adolescents. Oxford: Pergamon Press. 13-16.
Renick, %I. J., Harter, S. (1988) Manual for [he - Setoguchi, Y., Rappaport, 1.. R., Talbot, D.
Self-perception Profile for Learning Disabled (1992) ‘Psychological adjustment and perceived
Srudenrs. Denver: University of Denver Press. social support in children with congenital/
- - (19x9) ‘Impact of social comparisons on acquired limb deficiencies.’ Journal of
the developing $elf-perceptions of learning Behavioural Medicine, 15, 3 1-44.
disabled students.’ Joirrnal of Educarional Wallander. J. L., Feldman. b‘. S., Varni, J . W.
PSYChOIORy. 81, 631-638. (1989) ‘Physical status and psychosocial adjust-
Rey, A . (1958) I. ’examen Clinique en Psychologie. ment in children with spina bifida.’ Journal of
Paris: Presses Universitaircs. Pediatric Psychology. 14, 89- 102.
Rutter. bl. (1987) ‘Psychosocial resilience and Wechsler, D. (1974) Manual for /he Wechsler
protective mechanisms.’ American Journal of Inrelligence Scale for Children-Revised. Kew
Orlhopsychiarry. 57, 317-331. York: Psychological Corporation; Windsor,
- (1989) ‘Age as an ambiguous variable in Berks: NFER.
developmental research: some epidemiological - (1986) A Brirish Supplemenr 10 the Manual of
considerations from developmental psycho- the Wechsler Adult Intelligence Scale- Revised.
pathology.’ International Journal of Behavioural London: Harcourt Brace Jovsnovich.
Development, 12, 1-34. Widdicombe, S . (1988) ‘Dimensions of adolescent
Silverstein, A. 8 . (1982) ‘Two- and four-subtest identity.’ f?uropean Journal of social psycho log^.
short forms of the Wechsler Adult Intelligence 18,471-483.
Scale-Revised.’ Journal of Consulring and Wills, K. E., Holmbeck, G. N., Dillon, K., .Mcl.one,
Clinical Psychology, 50, 41 5-418. D. G . (1990) ‘Intelligence and achievement in
- (1987) ‘Equal weighting vs. differential weight- children with myelomeningocele.’ Joirrnal of
ing of Subtesl scores on short forms of Wechsler’s Pedrarric Psychology, 15, 16 I - 176.
Intelligence Scales.’ Journal of Clinical
215You can also read