The Search for Meaning-Symptoms and Transvaginal Sonography Screening for Ovarian Cancer
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Original Article
The Search for Meaning—Symptoms
and Transvaginal Sonography
Screening for Ovarian Cancer
Predicting Malignancy
Edward J. Pavlik, PhD1; Brook A. Saunders, MD1; Stacey Doran, BS1; Katherine W. McHugh, BA1;
Frederick R. Ueland, MD1; Christopher P. DeSimone, MD1; Paul D. DePriest, MD1; Rachel A. Ware, MD1;
Richard J. Kryscio, PhD2; and John R. van Nagell, Jr., MD1
BACKGROUND: The mortality rate of ovarian cancer is greater than that of all other major gynecologic
malignancies. Detecting ovarian cancer at an early and curable stage long has been an objective of oncolo-
gists. Recently, it was reported that certain symptom patterns are informative for the presence of ovarian
malignancy. In this article, the authors report on how symptoms and ultrasound predict ovarian malignancy.
METHODS: Two hundred seventy-two women who were participating in annual transvaginal sonography
(TVS) screening were selected from among 31,748 women who were enrolled. Symptom results were corre-
lated with ultrasound and surgical pathology findings. RESULTS: TVS performed better than symptoms
analysis for detecting malignancies (sensitivity, 73.3% vs 20%), and symptoms analysis performed better
for distinguishing benign tumors (specificity, 91.3% vs 74.4%). The use of TVS and symptoms analysis in se-
ries resulted in poorer identification of malignancy (sensitivity, 16.7%) but improved the ability to distin-
guish benign tumors (specificity, 97.9%). Decisions using either symptoms or TVS combined in parallel had
small increases in sensitivity (þ3.3%) and had coordinated, small decreases in specificity (5.8%). CONCLU-
SIONS: Symptoms did identify ovarian malignancies, but not as well as TVS. The current findings indicated
that: 1) tumors that are negative by both ultrasound and a symptoms index are likely to be benign (speci-
ficity, >97%), and 2) adding symptoms information that has weight equal to the weight of ultrasound only
slightly improves the discrimination of malignancy (sensitivity increase, þ3.3%). Thus, a major benefit in dis-
criminating malignancy was achieved through ultrasound, whereas the absence of symptoms in conjunction
with an abnormal ultrasound (characterized by a low morphology index) indicated that the mass was be-
nign and that surgery may not be required. Finally, informative symptoms can be expected to be absent in
80% of patients with ovarian malignancies. Cancer 2009;115:3689–98. V C 2009 American Cancer Society.
KEY WORDS: ovary, screening, symptoms, ultrasound.
Corresponding author: Edward J. Pavlik, PhD, Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of Kentucky
Medical Center, 800 Rose Street, Lexington, KY 40536; Fax: (859) 323-1018; epaul1@uky.edu
1
Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, the University of Kentucky Chandler Medical Center-Markey Cancer
Center, Lexington, Kentucky; 2Department of Biostatistics, the University of Kentucky Chandler Medical Center-Markey Cancer Center, Lexington,
Kentucky
See editorial on pages 3606–8, this issue.
Received: September 12, 2008; Revised: November 4, 2008; Accepted: November 26, 2008
Published online: July 14, 2009 V
C 2009 American Cancer Society
DOI: 10.1002/cncr.24407, www.interscience.wiley.com
Cancer August 15, 2009 3689Original Article
Ovarian cancer remains the fourth leading cause of cystic ovarian tumor with a solid or papillary projection
1
cancer death in US women. This year, the lives of over into its lumen.20 Morphology indexing has been useful in
15,000 women will be claimed by ovarian cancer in the predicting the risk of malignancy21-24 and was performed
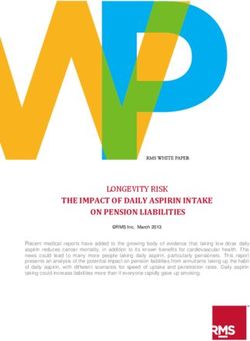
United States alone.2 Pelvic examination is notably inac- according to the classification of Ueland et al.20 Each tu-
curate in detecting subtle changes in ovarian size and mor- mor was given a score of from 1 to 10 according to
phology, particularly in postmenopausal women.3 increasing morphologic complexity and volume, as out-
Although ovarian cancer has been perceived as a ‘‘silent lined in Figure 1, with increasing numerical scores for
killer’’ that produces few specific symptoms, recent studies septa, papillary projections, solid areas, and extratumoral
have indicated that certain symptoms are significantly free fluid. Each final morphology index (MI) score is the
more common in women with ovarian cancer than in sum of the volume score (1-5) and the structure score (1-
women in the general population.4,5 These findings have 5).
resulted in the design of a symptoms index6 that report- Patients with ovarian cancer on frozen section or
edly has utility for identifying early stage ovarian cancer, patients with obvious metastatic disease at laparoscopy
which often is curable by conventional therapy.7,8 It underwent immediate exploratory laparotomy and stag-
appears, then, that the symptoms index could have utility ing. Tumors were classified histologically according to the
in a screening context to detect ovarian cancer at an earlier World Health Organization system and were staged
and more curable stage.9-17 according to the International Federation of Gynecology
Since 1987, the University of Kentucky Ovarian and Obstetrics system.
Cancer Screening Project has examined the efficacy of an- The selection group consisted of those members of
nual transvaginal sonography (TVS) as a screening the source group who underwent surgery after an
method for ovarian cancer, providing free screening to
over 31,000 women who participate in this program. The
results of this screening study have been reported
recently.18 The current report applies the symptoms index
analysis6 to this large study group as a validation study to
determine whether its addition improves the performance
of ovarian cancer screening.
MATERIALS AND METHODS
Patients enrolled in the University of Kentucky Ovarian
Cancer Screening Project from January 1987 to June
2008 composed the source group (n ¼ 31,748). Approval
was received from the University of Kentucky Institu-
tional Review Board. Eligibility, exclusions, instrumenta-
tion, protocol, criteria for designating an abnormality,
and data collected were as recently reported.18 Partici-
pants in the screening program received free annual
screening after a normal result (ie, 74.2% were scheduled
11-13 months after a normal screen, and 7.8% were
scheduled even earlier, whereas 17.9% were scheduled
later). After an abnormal screening result, free repeat
screening was scheduled at 4 to 6 weeks. Criteria for ab-
normality included ovarian volume (values >2 standard
FIGURE 1. Morphology index schematic is shown.
deviations above the mean volume of normal ovaries in
premenopausal and postmenopausal women)19 and any
3690 Cancer August 15, 2009Symptoms & TVS Screening for Ovarian CA/Pavlik et al
abnormal TVS finding (n ¼ 450) and included women level. Analysis of receiver operating characteristic (ROC)
with either malignant or benign tumors. The study group curves also was performed.25-27
was formed from the selection group and was made up of
women in the selection group who had returned confident
responses on the symptoms index questionnaire (n ¼ 272; RESULTS
60.4%). Excluded from this group were 178 women who There were 31,748 women who enrolled in the University
had died (1 stage II and 3 stage III ovarian tumors), had with- of Kentucky ovarian screening study from January 1987
drawn from the study, who were unwilling to take the symp- to June 2008, and a family history of ovarian cancer was
toms survey, or who were not confident in their answers. documented in 22.5% of these women.
Symptoms Index Analysis Clinical Characteristics of the Women
The symptoms survey in the form published by Goff et al6 Selected for Study on the Basis of Surgery
was used and occupied an entire 8.5 11-inch page Related to TVS Screening
printed in landscape format. The only deviations from the The candidates who were selected for the current study all
symptoms survey published by Goff et al6 were that 1) were involved actively in the University of Kentucky
dark-contrast symptoms space separators replaced the Ovarian Screening Program and had undergone surgery
open white spaces used by Goff et al6, and 2) a single con- because of an abnormal TVS result. The selection group
fidence assessment query was added. The dark-contrast contained 450 women who underwent surgery related to
space separators improved the readability of the form and a TVS finding, and a family history of ovarian cancer was
were intended to prevent visual errors arising from row or documented in 123 of those women (27.4%). Members
column cross-over. The confidence query question was of the selection group who had confident responses to the
‘‘How confidently did you answer these questions?’’ symptoms questionnaire defined the study group of 272
Response choices for the query were 0 ¼ no confidence, women. Twenty-seven percent of women in the study
1 ¼ minimally sure, 2 ¼ more than minimally sure, 3 ¼ group reported a family history of ovarian cancer. The
pretty sure, 4 ¼ sure, and 5 ¼ absolutely sure of accuracy.’’ clinical characteristics of the patients screened are shown
The response query was used to identify recall bias or in Table 1. There were no significant differences between
responses that were affected by the respondent’s memory. the selection group and the study group with respect to
Thirteen individuals without malignancies were excluded age, gravidity, parity, weight, height, body mass index
because they did not have a confidence response >3, and (BMI), body surface area, CA 125, family history of ovar-
165 individuals were excluded because they did not wish to ian, breast, or colon cancer, use of hormone-replacement
participate or because they could not be contacted. The cri- therapy, or nulliparity (Table 1). There was no significant
teria reported by Goff et al for any specific symptom (pelvic difference between the histopathologies of the selection
pain, abdominal pain, increased abdominal size, bloating, group and the study group (ie, responders to the symp-
feeling full, and difficulty eating), frequency (>12 times toms questionnaire) (Table 2).
per month), and duration (12 days per
month with a durationOriginal Article
Table 1. Clinical Characteristics of the Selection Group (n¼450), the Study Group (n¼272), and the Nonparticipating
Group (n¼178)
Selection Group Study Group Nonparticipating Group
Variable* Mean6SEM Range No. (%) Mean6SEM Range No. (%) Mean6SEM Range No. (%)
Age, y 58.40.5 32-89 450 58.40.6 32-89 272 58.40.8 34-84 178
Gravidity 2.50.08 0-12 450 2.60.1 0-12 272 2.40.1 0-7 178
Parity 2.20.07 0-10 450 2.30.1 0-10 272 2.10.1 0-6 178
Weight, pounds 163.31.7 80-350 450 164.32.2 99-350 272 161.82.6 80-300 178
Height, inches 64.50.12 54-72 450 64.50.2 54-72 272 64.50.2 57-71 178
BMI, lbs/in2 27.60.3 15.1-57.8 450 27.70.4 18-58 272 27.40.4 15-51 178
BSA, m2 1.80.01 1.3-2.8 450 1.80.01 1.4-2.8 272 1.80.02 1.2-2.5 178
CA 125, U/mL 37.111 1-1500 148 36.913.9 1-1550 113 3711.9 2-279 35
Family history
Ovarian cancer 123 (27) 73 (27) 50 (28)
Breast cancer 196 (44) 116 (43) 81 (45)
Colon cancer 100 (22) 70 (26) 30 (17)y
History of HRT 145 (32) 99 (36) 55 (26)
Nulliparous 58 (13) 30 (11) 28 (16)
SEM indicates standard error of the mean; BMI, body mass index; BSA, body surface area; HRT, hormone-replacement therapy.
* There were no significant differences in age, parity, gravidity, weight, height, BMI, BSA, or CA 125; P < .9; Student t test) or in family history, use of HRT, or
nulliparity (chi-square value, 3.285; P¼.511).
y Significantly different (P¼.052).
Table 2. Histologic Findings in the Selection Group Table 3. Summary of Reported Symptoms (n¼272)*
(n¼450) and the Study Group (n¼272)*
No. of Patients (%)
No. of Patients (%)
Symptom Goff Positive Goff Negative
Finding Selection Study
Group Group Back pain NA 85 (31.3)
Frequent urination NA 84 (30.9)
Primary ovarian cancer 49 (10.9) 30 (11) Urinary urgency NA 80 (29.4)
Malignant 32 (7.1) 15 (5.5) Fatigue NA 79 (29)
GC/LMP 17 (3.8) 15 (5.5) Constipation NA 74 (27.2)
Serous cystadenoma 192 (42.7) 114 (41.9) Abdominal bloating 14 (5.1) 65 (23.9)
Endometrioma 30 (6.7) 18 (6.6) Pelvic pain 15 (5.5) 59 (21.7)
Mucinous cystadenoma 24 (5.7) 14 (5.1) Pain with intercourse NA 59 (21.7)
Cystic teratoma 21 (4.7) 12 (4.4) Indigestion NA 58 (21.3)
Hemorrhagic cyst 9 (2) 6 (2.2) Leg swelling NA 58 (21.3)
Fibroma/thecoma/Brenner tumor 33 (7.7) 22 (8.1) Increased abdominal size 15 (5.5) 50 (18.4)
Leiomyomata 19 (4.2) 16 (5.9) Irregular menses NA 50 (18.4)
Hydrosalpinx/paratubal 29 (6.4) 16 (5.9) Diarrhea NA 49 (18)
Other 44 (9.4) 24 (8.8) Difficulty breathing NA 45 (16.5)
Bleeding after menopause NA 33 (12.1)
Nausea/vomiting NA 32 (11.8)
GC/LMP, granulosa cell tumor/tumor with low malignant potential. Bleeding with intercourse NA 31 (11.4)
* No significant differences were observed between the selection group ver- Palpable abdomen NA 28 (10.3)
sus the study group (chi-square statistic, 5.616: P¼.898). Feels full quickly 9 (3.3) 21 (7.7)
Weight loss NA 21 (7.7)
Abnormal eating 3 (1.1) 14 (5.1)
(Table 3). Approximately the same number of women NA indicates not applicable.
* Based on the symptoms survey in the form published by Goff et al.6
reported having no symptoms (n ¼ 124; 45.6%) as
reported symptoms that were not considered positive (n ¼ women with ovarian cancer in the study group who
121; 44.5%) on the Goff symptoms index (Table 4). Of the responded to the symptoms questionnaire, 6 women (20%)
27 women who were positive on the Goff symptoms index, satisfied the Goff et al criteria for being symptoms-positive,
6 women had ovarian cancers (4 malignancies and 2 tumors and 80% did not. The study group was very similar to the
of low malignant potential) (Table 5). Thus, of the 30 selection group with respect to tumor stage, and 75% had
3692 Cancer August 15, 2009Symptoms & TVS Screening for Ovarian CA/Pavlik et al
Table 4. Response to Symptoms Questionnaire (n¼272) Table 6. Tumor Stage
Reported Symptoms No. of Patients (%) No. of Patients (%)
Reported experiencing no symptoms 124 (45.6) Group Early Stage Late Stage
Reported symptoms not 121 (44.5) (I/II) (III)
considered positive
Selection group (n¼450) 37 (75.5) 12 (24.5)
on the symptoms index
Study group (n¼272) 23 (76.7) 7 (23.3)
Reported symptoms 27 (9.9)
Informative symptoms 6 (100) 0 (0)
considered positive on
positive: TP
the Goff symptoms index
TP indicates true positive.
Table 5. Histologic Findings in Women With a Positive
Symptoms Index (n¼27)
Table 7. Predictive Ability of the Symptoms Index on
Initial or Subsequent Screening Visits (n¼272)*
Histologic Finding No. of Women
Primary ovarian cancer 6 No. of Patients
Malignant 4 Prediction First Subsequent
GC/LMP 2 Status Encounter Encounters
Simple serous cyst 11
Cystic teratoma 1 True positive 4 2
Hemorrhagic cyst 1 False positive 12 9
Fibroma/thecoma/Brenner tumor 1 True negative 116 105
Leiomyomata 2 False negative 9 15
Hydrosalpinx/paratubal 2
Other 3
* There were no statistically significant differences (chi-square statistic,
2.779; P¼.669).
GC/LMP, granulosa cell tumor/tumor with low malignant potential.
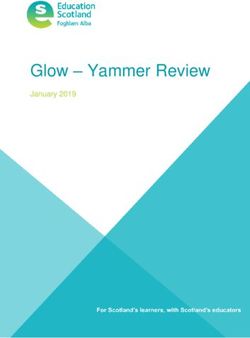
early stage disease (Table 6). All of the women who had between the TP rate (TPR) ‘‘benefits’’ and the FP rate
true-positive (TP) results identified by informative symp- (FPR) ‘‘costs,’’ was used to examine the effectiveness of
toms had early stage disease (Table 6). TVS alone and when combined with the symptoms index
Because symptoms that persisted for >12 months (Fig. 2). The TPR and the FPR were defined as noted by
could be more likely to occur on the first screening encounter Suojanen with regard to correctness.28,29 Screening per-
than on subsequent annual return screens, results originating formance was graphed at and above each MI score with
from the entry screen were compared with results originating TVS alone in the selection group (n ¼ 450) and in the
on subsequent screens. There were no significant differences study group (n ¼ 272) (Fig. 2, open squares). A line of no
in TP, false-positive (FP), true-negative (TN), or false-nega- discrimination describing a random guess or outcome (ie,
tive (FN) results that were identified on the entry screen ver- flipping a coin) is included on Figure 2 as a dashed diago-
sus subsequent screens (Table 7). Consequently, no effect on nal line. For the study group, the distance from the line of
the symptoms reporting was observed because of the possibil- no discrimination was greatest at MI scores >4 to 5, a
ity of symptoms persisting for >12 months on the first visit, relation that was mirrored in the selection group (Fig. 2).
supporting the examination of symptoms results without Combining the symptoms index with TVS screening
regard to the number of screening visits. moved the ROC space plot dramatically closer to the line
of no discrimination, drastically reducing both the area
Identification of Malignancy: Comparisons under the ROC curve and the area between the ROC
With the Symptoms Index Alone and With TVS curve and the line of no discrimination (Fig. 2, open
Does the symptoms index in conjunction with circles). By using a logistic regression analysis, the MI
transvaginal sonography improve the identification score alone (Fig. 2, open squares) significantly (POriginal Article
chosen negative result calculated at 0.816. Adding the
symptoms results (Fig. 2, open circles) resulted in an in-
significant improvement (P ¼ .08; AUC ¼ 0.820) on this
model.
The performance of symptoms alone for identifying
malignancy (Table 8, Group A) was examined in relation
to TVS alone in the study group using the 2 dichotomiza-
tions shown in Figure 2 that had the best ROC perform-
ance (ie, Group B [MI score 4] and Group C [MI score
5]) (Table 8). TVS (based on either the Group B or the
Group C dichotomization) had much higher sensitivity
FIGURE 2. Receiver operating characteristic analysis of trans- and lower specificity than the symptoms index. Combin-
vaginal sonography (TVS) and symptoms analysis is shown.
The performance of TVS alone is represented by solid circles ing the symptoms index with TVS (Table 8, Groups D
for the selection group and by open squares for the study and E) in series improved specificity but reduced sensitiv-
group. Open circles represent the discrimination of malignancy
by both TVS and symptoms together. The points were plotted
ity. The results reported here with the symptoms index
with respect to malignancy index values greater than or equal (Table 8, Group A) resulted in lower sensitivity (Table 8,
to the number above each symbol. The diagonal dashed line Group H) and higher specificity than reported by Goff
(line of no discrimination) describes a random guess or out-
come. Ranges for sensitivity and specificity were obtained from et al6. Because sensitivity and specificity are derived inde-
the 2007 report by Goff et al6 and were used for maximal and pendently of each other, we examined the range of sensi-
minimal calculations (the box marked Published Symptoms
Data). Solid squares at a true-positive (TP) rate (TPR) between
tivities and specificities reported by Goff et al6 (Table 8,
0.8 and 0.9 near origin of the false-positive (FP) rate (FPR) Group H) in an ROC curve context, Figure 2 (the boxed
superimpose the overall results from TVS in the entire Univer- window identified as ‘‘Published Symptoms Data
sity of Kentucky screening group (for sensitivity and specificity
source values, see Table 9, Group J). Sensitivity ¼ TP/(TP þ [Goff]’’). The published symptoms results underper-
FN) ¼ the positive rate ¼ TPR. FPR ¼ 1specificity. TPR and formed TVS alone, and a portion of these results reached
FPR were defined according to Suojanen.28,29
and crossed below the line of no discrimination. The
Table 8. Performance of Either the Symptoms Index or Transvaginal Sonography for Identifying Malignancies When Used
Together in the Study Group (n¼272)
Group* TP TN FP FN No. Sensitivity, Specificity, PPV, NPV, ACC,
%† %‡ % % %
A: Symptoms positive 6 221 21 24 272 20 91.3 22.2 90.2 83.5
B: TVS, MI4 27 135 107 3 272 90 55.8 20.1 97.8 59.6
C: TVS, MI5 22 180 62 8 272 73.3 74.4 26.2 95.7 74.3
D: Symptoms positive and MI4 5 235 7 25 272 16.7 97.1 41.7 90.4 88.2
E: Symptoms positive and MI5 5 237 5 25 272 16.7 97.9 50 90.5 89
F: Symptoms positive or MI4 28 121 121 2 272 93.3 50 18.8 98.4 54.8
G: Symptoms positive or MI5 23 164 78 7 272 76.7 67.8 22.8 95.9 68.8
Reference basis
H: Goff 20076 — — — — 233§ 33-47 61-75 — — —
I: TVS: van Nagell 200718 51 24,954 313 9 25,327 85 98.7 14 -27.1| 99.96 98.7
J: TVS: Up to June 2008 62 31,287 388 11 31,748 84.9 98.8 13.8-20.6| 99.96 99.8
TP indicates true positive; TN, true negative; FP, false positive; FN, false negative; PPV, positive predictive value (TP/[TPþFP]); NPV, negative predictive value
(TN/[TNþFN]); ACC, accuracy ([TPþTN]/[TPþTNþFPþFN]); TVS, transvaginal sonography; MI, morphology index.
* Screening findings were dichotomized on the basis of an MI4 versus an MI5. Patients who had an MI4 made up Groups B, D, and F; and patients who
had TVS findings with an MI5 made up Groups C, E, and G.
y Sensitivity¼TP/(TPþFN)¼TP rate.
z Specificity¼TN/(TNþFP).
§ The number of patients in the group that received ultrasound.
| The PPV lower value was for the entire screening group and the higher value in range was for the period from 2000 to the present, when patients did not
undergo surgery for simple cysts.
3694 Cancer August 15, 2009Symptoms & TVS Screening for Ovarian CA/Pavlik et al
Table 9. Age and the Performance of Either the Symptoms Index or Transvaginal Sonography for Identifying Malignancies
Group* TP TN FP FN Sensitivity, Specificity, PPV, NPV, ACC,
% % % % %
Premenopausal (N¼45)
A: Symptoms positive 1 36 6 2 33.3 85.7 14.3 94.7 33.3
B: TVS, MI4 2 25 17 1 66.7 59.5 10.5 96.2 66.7
C: TVS, MI5 2 32 10 1 66.7 76.2 16.7 97 66.7
D: Symptoms positive and MI4 0 39 3 3 0 92.9 0 92.9 0
E: Symptoms positive and MI5 0 40 2 3 0 95.2 0 93 0
F: Symptoms positive or MI4 3 22 20 0 100 52.4 13 100 100
G: Symptoms positive or MI5 3 28 14 0 100 66.7 17.6 100 100
Postmenopausal (N¼227)
H: Symptoms positive 5 185 15 22 18.5 92.5 25 89.4 18.5
I: TVS, MI4 25 110 90 2 92.6 55 21.7 98.2 92.6
J: TVS, MI5 20 148 52 7 74.1 74 27.8 95.5 74.1
K: Symptoms positive and MI4 5 196 4 22 18.5 98 55.6 89.9 18.5
L: Symptoms positive and MI5 5 197 3 22 18.5 98.5 62.5 90 18.5
M: Symptoms positive or MI4 25 99 101 2 92.6 49.5 19.8 98 92.6
N: Symptoms positive or MI5 20 136 64 7 74.1 68 23.8 95.1 74.1
TP indicates true positive; TN, true negative; FP, false positive; FN, false negative; PPV, positive predictive value (TP/[TPþFP]); NPV, negative predictive value
(TN/[TNþFN]); ACC, accuracy ([TPþTN]/[TPþTNþFPþFN]); TVS, transvaginal sonography; MI, morphology index.
* Pair-wise chi-square tests were not significant at P < .05 (PAH¼.03311; PBI¼.3593; PCJ¼.5795; PDK¼.1053; PEL¼.2228; PFM¼.6299; PGN¼.8399).
performance of TVS for ovarian cancer screening is sum- formation with TVS MI scores (Table 8, Groups D and
marized in terms of the large group published results F) indicated that, when both TVS and symptoms crite-
(Table 8, Group I) and subsequent accrual results up to ria are met, there is a reduction of FP results. This
June 2008 (Table 8, Group J), both of which indicate reduction, although it improves the positive predictive
better sensitivities and specificities than those produced value (PPV), is at the expense of identifying TPs so that
by the symptoms index alone (Table 8, Group A) or in sensitivity suffers (Table 8). When either TVS or symp-
combination with TVS (Table 8, Groups D and E). toms criteria are met (Table 8, Groups F and G), sensi-
Finally, decision making was examined on the basis of tivity is affected positively, but specificity is
meeting either symptoms or TVS criteria in parallel. In compromised, with the ability to distinguish malignant
this context, TVS results for scores of both MI scores from benign (PPV) becoming similar to that of TVS
4 and MI scores 5 were explored to broadly test the alone (Table 8, Groups B and C).
information added by symptoms. Only a minor increase Finally, when age was overlaid on these considera-
in sensitivity occurred when either TVS MI scores 4 tions, the symptoms index alone appeared to have more
or the symptoms index was applied in parallel (Table 8, sensitivity in premenopausal women (Table 9, Group A)
Group F vs Group B). Similarly, a minor increase in but less specificity than in postmenopausal women (Table
sensitivity occurred when either TVS MI scores 5 or 9, Group H). Conversely, TVS alone appeared to have
the symptoms index was applied in parallel (Table 8, more sensitivity in postmenopausal women (Table 9,
Group G vs Group C) with concomitant decreases in Groups I and J) with slightly higher specificity in premeno-
specificity when symptoms were applied with TVS MI pausal women (Table 9, Groups B and C). When combin-
scores 4 or 5. To explain how these findings were ing symptoms criteria in series with TVS, specificity
made, 1 TP entered Group F (Table 8) because of a pos- appeared high in both premenopausal women (Table 9,
itive symptoms index, and that case was not included in Groups D and E) and postmenopausal women (Table 9,
Group B (Table 8) because of an MI scoreOriginal Article
group (Table 9, Groups F and G vs Groups M and N). >97%). Second, adding in parallel symptoms informa-
However, differences between premenopausal and post- tion with equal weight to that of ultrasound (either/or)
menopausal women were only apparent, because none only slightly improved the discrimination of malignancy
were significant (P < .05; chi-square test). (1 additional TP with a sensitivity increase of þ3.3%).
These results strongly indicate that the major screening
benefit in discriminating malignancy is achieved with
DISCUSSION ultrasound findings, whereas symptoms information can
Our experience from nearly 20 years of screening has posi- aid in reducing surgery for women who have benign con-
tioned us to reach certain conclusions regarding the bene- ditions that generate an ultrasound abnormality.
fits and limitations of TVS as a screening method for A distinction between the data reported here and
ovarian cancer, especially in relation to safety, patient those reported by Goff et al6 is that they differ in composi-
acceptability, time-efficiency, costs, and interobserver var- tion: the Goff et al study was composed of 37% early stage
iation.30-32 In this regard, we believed that it would be disease versus 75% in the current study. This variation in
beneficial to determine how symptoms information could stage distribution alone could account for differences
improve TVS screening for ovarian cancer. It is notewor- between the reports in sensitivity and specificity, particu-
thy that, as the basis for this study, we were in a position larly if symptoms are more apparent in late-stage ovarian
to draw on a group of patients all of whom had a sufficient cancer. We have used exclusion based on reported patient
TVS abnormality that led to surgery and histologic evalu- uncertainty to constrain recall bias, whereas Goff et al6
ation of the ovarian tumor removed. used symptoms queries limited to the present. Even more
For a screening test to be effective, sensitivity, speci- significant is the overall difference in the selection of the
ficity, PPV, and negative predictive value should be study group. The study group that we used in the current
high.33 With periodic use, screening should decrease stage report was composed of women from the general popula-
at detection and should increase disease-specific survival tion who were actively participating in the University of
in the screened population.34 TVS may be questioned as a Kentucky Ovarian Screening Program. In contrast, Goff
screening method for ovarian cancer because of its moder- et al6 constructed a study group that surveyed 149 women
ate sensitivity and relatively low PPV.18 Although TVS with ovarian cancer (55 early stage, 88 late-stage, 6
screening accurately predicted the presence of cancer unknown stage), 225 high-risk women who were enrolled
involving the ovary in 62 asymptomatic women, there in an ovarian cancer early detection study, and 233
were 11 patients who developed ovarian cancer within 12 women with conditions indicating that they should
months of a normal scan (Table 8, Group J, FN column), receive an ultrasound. It is entirely possible that this con-
so that the addition of information from a symptoms index struction does not mirror the same cross-section of
would have the potential of reducing both the FN and the women with and without symptoms that we observed in
FP screening results. Such a reduction would have its great- our large screening effort in the general population. In
est impact by increasing the PPV so that screening would addition, Daly and Ozols35 have presented a commentary
better differentiate malignant from benign lesions. The on issues that may involve limitations of the control group
results reported herein when both TVS and symptoms cri- used by Goff et al.6 An additional consideration is pre-
teria are met, indicate a reduction of FP results. This reduc- sented in the 2008 report by Anderson et al that combines
tion, although it improves the PPV, is at the expense of the Goff symptoms index with CA 125 to improve detec-
identifying TP results, so that sensitivity suffers (Table 8). tion of ovarian cancer.36 In that report,36 sensitivity and
When either TVS or symptoms criteria are met, sensitivity specificity of the symptoms index alone were considerably
is affected positively, but specificity is compromised, and higher than first reported.6 The ranges reported initially
the ability to distinguish malignant from benign (PPV) were 33% to 47% sensitivity and 61% to 75% specific-
becomes similar to that of TVS alone (Table 8). ity6; whereas, in the recent report,36 the ranges were
The clinical significance of the results reported here 52.1% to 74.8% for sensitivity and 83.6% to 91.9% for
is that a screen that is negative by both ultrasound and the specificity. These differences raise several questions. First,
symptoms index is highly likely to be benign (specificity, because the sample for the recent study is described as a
3696 Cancer August 15, 2009Symptoms & TVS Screening for Ovarian CA/Pavlik et al
subgroup of the previous study, indicating that different 6 malignancies in 27 women who were positive for in-
study groups were not used, what accounts for the formative symptoms (22%) and 24 women with malig-
increased sensitivity and specificity in the recent report? nancies that were absent informative symptoms among 30
Second, if the subgroup that was reported36 differed women who had malignancies (80%). It is possible that the
intrinsically from the originating group from which it was informative symptoms coincided only serendipitously with
drawn,6 does this indicate that there will be considerable malignancy; however, this can be neither substantiated nor
variability in the results obtained with the symptoms refuted by the current study. Moreover, in the study
index? Although there are differences in study design, our reported here, all women had a successful TVS. Performing
findings indicate that the evaluation of informative symp- a definitive TVS should be the first line of response when
toms as identified by Goff and collaborators6 can be useful encountering a patient who has informative symptoms.
in helping distinguish benign disease when used in con- Unfortunately, TVS may not be reliable in clinical settings
junction with TVS. Symptoms information cannot be if a large uterus is present or if the patient’s BMI is exces-
ignored and is an important element in communication sive. In these cases, thorough assessment of a patient with
between patient and physician. The efforts of Goff et al6 informative symptoms using other diagnostic testing is
have done much to erode the idea that ovarian cancer has essential. It is important to educate patients that informa-
no symptoms until it is advanced. In this regard, efforts tive symptoms should not be ignored and that the degree
still are needed to define how this information frequents to which symptoms are a resultant indicator of early stage
and affects the general population. ovarian malignancy has yet to be determined.
With regard to the clinical outlook, the following In the absence of early detection, most patients with
considerations are evident: 1) TVS alone performs better ovarian cancer will continue to present with advanced-
than informative symptoms evaluation in identifying stage disease in which the cost of treatment is high and the
malignancy, whereas informative symptoms evaluation in cure rate is low.40 We intend to continue to use symptoms
concert with TVS improves sensitivity only modestly. 2) analysis prospectively in combination with TVS to evalu-
The frequency of informative symptoms cannot be dis- ate more fully the performance of screening for ovarian
missed because, even when they are present in only 20% cancer. As specific biomarkers are added to TVS ovarian
of ovarian malignancies, the risk for these patients is screening protocols that include symptoms analysis, the
higher than that for patients without informative symp- protection afforded by annual screening from ovarian can-
toms. 3) The evaluation of informative symptoms is facile, cer mortality should improve.
in that it is simple, quick, and inexpensive.
Taken together, these considerations point in a clear Conflict of Interest Disclosures
clinical direction. TVS performs with credibility in Supported by grants from the Telford Foundation, and the
women who are both symptom-free and in those who Department of Health and Human Services, Commonwealth of
Kentucky.
report symptoms. By itself, TVS performs as well as or
better than mammography,37 mammography-assisted by
References
sonography,38 or mammography combined with mag-
netic resonance imaging,39 even with regard to PPV. In 1. Jemal A, Murray T, Ward E, et al. Cancer statistics 2005.
CA Cancer J Clin. 2005;55:10-30.
this sense, TVS lives up to the performance standards
2. Jemal A, Siegel R, Ward W, et al. Cancer statistics, 2008.
used and accepted for screening. In a population in which CA Cancer J Clin. 2008;58:71-96.
informative symptoms accompany malignancy in 20% of 3. Ueland FR, DePriest P, DeSimone C, et al. The accuracy of
cases, informative symptoms evaluation in parallel equally examination under anesthesia and transvaginal sonography in
weighted with TVS (Table 8, Groups F and G) carries a evaluating ovarian size. Gynecol Oncol. 2005;99:400-403.
3% to 4% improvement in detection (sensitivity). How- 4. Goff BA, Mandell L, Muntz HG, Melancon CH. Ovarian
carcinoma diagnosis. Results of a national ovarian cancer
ever, for the additional positive case that is detected, the
survey. Cancer. 2000;89:2068-2075.
data reported here indicate that from 4 to 14 additional
5. Goff BA, Mandelm LS, Melacon CH, Muntz H. Fre-
women without malignancy will undergo surgery. The in- quency of symptoms of ovarian cancer in women present-
formation that needs to be emphasized is that we observed ing to primary care clinics. JAMA. 2004;291:2705-2712.
Cancer August 15, 2009 3697Original Article
6. Goff BA, Mandel LS, Drescher CW, et al. Development of 22. DePriest PD, Shenson D, Fried A, et al. A morphology
an ovarian cancer symptom index. Cancer. 2007;109:221-227. index based on sonographic findings in ovarian cancer.
7. Young RC, Walton LA, Ellenberg SS. Adjuvant therapy in Gynecol Oncol. 1993;51:7-11.
stage I and II epithelial ovarian cancer: results of 2 prospec- 23. Bailey CL, Ueland FR, Land GL, et al. Malignant potential
tive randomized trials. N Engl J Med. 1990;322:1021-1027. of small cystic ovarian tumors in postmenopausal women.
8. Ries LA, Kosary CL, Hankey BF, et al, eds. SEER Cancer Gynecol Oncol. 1998;69:3-7.
Statistics Review, 1973-1995. Bethesda, Md: National Can- 24. Modesitt SC, Pavlik EJ, Ueland FR, et al. Risk of malig-
cer Institute; 1998. nancy in unilocular ovarian cystic tumors less than 10 cen-
9. Campbell S, Bhan V, Royston P, et al. Transabdominal timeters in diameter. Obstet Gynecol. 2003;102:594-599.
ultrasound screening for early ovarian cancer. BMJ. 25. Zweig MH, Campbell G. Receiver-operating characteristic
1989;299:1363-1367. (ROC) plots: a fundamental evaluation tool in clinical
10. van Nagell JR, Higgins RV, Donaldson ES, et al. Transva- medicine. Clin Chem. 1993;39:561-577.
ginal sonography as a screening method for ovarian cancer: 26. Pepe MS. The Statistical Evaluation of Medical Tests for
a report of the first 1000 cases screened. Cancer. Classification and Prediction. New York, NY: Oxford Uni-
1990;65:573-577. versity Press; 2003.
11. Jacobs IJ, Bridges J, Reynolds C, et al. Multimodal approach 27. Fawcett T. An introduction to ROC analysis. Pattern Recog-
to screening for ovarian cancer. Lancet. 1988;2:268-271. nit Lett. 2006;27:861-874.
12. Bourne TH, Campbell S, Reynolds KM, et al. Screening 28. Suojanen JN. False false positive rates [letter]. N Engl J
for early familial ovarian cancer with transvaginal ultraso- Med. 1999;341:131.
nography and colour blood flow imaging. BMJ. 29. [Noauthors listed]Correction: false false positive rates [let-
1993;306:1025-1029. ter]. N Engl J Med. 1999;341:624.
13. DePriest PD, Gallion HH, Pavlik EJ, Kryscio RK, van 30. Pavlik EJ, van Nagell JR, DePriest PD, et al. Participation
Nagell JR. Transvaginal sonography as a screening method in transvaginal ovarian cancer screening: compliance, corre-
for the detection of early ovarian cancer. Gynecol Oncol. lation factors, and costs. Gynecol Oncol. 1995;57:395-400.
1997;65:408-414.
31. Pavlik EJ, Johnson TL, DePriest PD, Andrykowski MA,
14. Jacobs I, Skates SJ, MacDonald N, Menon U, Rosenthal A, Kryscio RJ, van Nagell JR. Continuing participation sup-
Prys Davies A. Outcome of a pilot randomised controlled ports ultrasound screening for ovarian cancer. Ultrasound
trial of ovarian cancer screening. Lancet. 1999;253:1207- Obstet Gynecol. 2000;15:354-364.
1210.
32. Higgins RV, van Nagell JR, Woods CH, Thompson EA,
15. Sato S, Yokoyama Y, Sakamoto T, et al. Usefulness of mass Kryscio RJ. Interobserver variation in ovarian measurements
screening for ovarian carcinoma using transvaginal ultraso- using transvaginal sonography. Gynecol Oncol. 1990;39:69-71.
nography. Cancer. 2000;89:582-588.
33. Prorok PC. Evaluation of screening program for the early
16. van Nagell JR, DePriest P, Reedy M, et al. The efficacy of detection of cancer. Statistical methods for cancer studies
transvaginal sonographic screening in asymptomatic women (edited by RG Cornell). Natl Cancer Inst Stat Textbk
at risk for ovarian cancer. Gynecol Oncol. 2000;77:350-356. Monogr. 1984;51:267-328.
17. Buys SS, Partridge E, Greene MH, et al. Ovarian cancer 34. Hulka BS. Cancer screening: degrees of proof and practical
screening in the Prostate, Lung, Colorectal and Ovarian application. Cancer. 1989;62:1776-1789.
(PLCO) Cancer Screening Trial: findings from the initial
35. Daly MB, Ozols RF. Symptoms of ovarian cancer—where
screen of a randomized trial. Am J Obstet Gynecol.
2005;193:1630-1639. to set the bar? JAMA. 2004;291:2755-2756.
18. van Nagell JR, DePriest PD, Ueland FR, et al. Ovarian 36. Anderson MR, Goff BA, Lowe KA, et al. Combining a
cancer screening with annual transvaginal sonography. symptoms index with CA 125 to improve detection of
Findings of 25,000 women screened. Cancer. 2007; ovarian cancer. Cancer. 2008;113:484-489.
109:1887-1896. 37. Humphrey LL, Hefland M, Chan BKS, Woolf SH. Breast can-
19. Pavlik EJ, DePriest PD, Gallion HH, et al. Ovarian volume cer screening: a summary of the evidence for the US Preventive
related to age. Gynecol Oncol. 2000;77:410-412. Services Task Force. Ann Intern Med. 2002; 137:347-360.
20. Ueland F, DePriest P, Pavlik E, Kryscio R, van Nagell JR. 38. Elmore JG, Armstrong K, Lehman CD, Fletcher SW.
Preoperative differentiation of malignant from benign ovar- Screening for breast cancer. JAMA. 2005;293:1245-1256.
ian tumors: the efficacy of morphology indexing and Dopp- 39. Lehman CD, Gatsonis C, Kuhl CK, et al. MRI evaluation
ler flow sonography. Gynecol Oncol. 2003;91:46-50. of the contralateral breast in women with recently diag-
21. Sassone M, Timor-Tritsch I, Artner A, Westhoff C, Warren nosed breast cancer. N Engl J Med. 2007;356:1295-1303.
WB. Transvaginal sonographic characterization of ovarian 40. Cooper AL, Nelson DF, Doran S, et al. Long-term survival
disease: evaluation of a new scoring system to predict ovar- and cost of treatment in patients with stage IIIC epithelial
ian malignancy. Obstet Gynecol. 1991;78:70-76. ovarian cancer. Current Women’s Health Reviews. 2009;5:44-50.
3698 Cancer August 15, 2009You can also read