The "No Surprise Billing" Act: Why This Isn't JUST For Hospitals
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The “No Surprise Billing” Act:
Why This Isn’t JUST For
Hospitals
February 24, 2023
0
The Problem
• Patient goes to an in-network hospital for a
surgery by an in-network surgeon.
Unbeknownst to the patient, the
anesthesiologist is out of network.
• The anesthesiologist bills more than the plan
allows, leaving the patient on the hook.
1 © 2023 Fredrikson & Byron, P.A.
1
© 2020 MedLearn Media, Inc. 1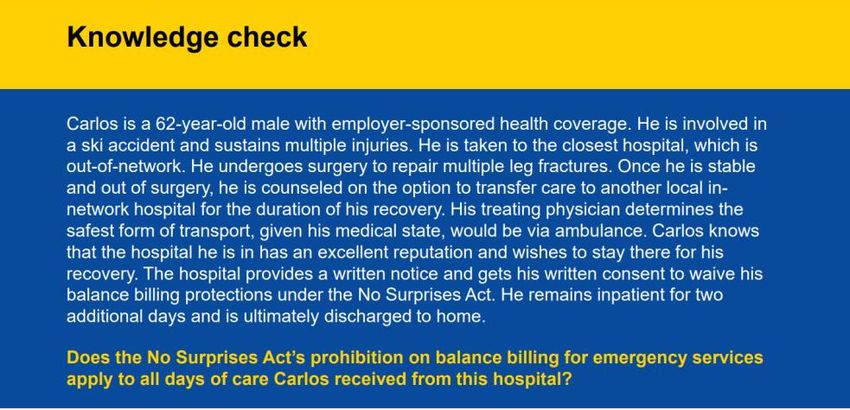
The Solution
• The No Surprises Act, Public Law 116-
260, passed December 27, 2020.
• A variety of state laws.
• Like HIPAA, more restrictive state laws
generally control.
2 © 2023 Fredrikson & Byron, P.A.
2
The Regulatory Framework
• Requirements Related to Surprise Billing;
Part I, 86 Fed. Reg. 36872 (July 13,
2021).
• Requirements Related to Surprise Billing;
Part II, 86 FR 55980 (October 7, 2021).
3 © 2023 Fredrikson & Byron, P.A.
3
© 2020 MedLearn Media, Inc. 2
4 © 2023 Fredrikson & Byron, P.A.
4
Lingo
GFE: Good Faith Estimate
IDR: Independent Dispute Resolution.
NSA: No Surprises Act.
OON: Out-of-Network.
Provider: They mean physician.
QPA: Qualified Payment Amount.
5 © 2023 Fredrikson & Byron, P.A.
5
© 2020 MedLearn Media, Inc. 3
Overview: Two Rules In One?
• Portions apply only to services provided in air
ambulances, hospitals (including CAH) ambulatory
surgical centers, or freestanding emergency rooms.
The rule calls them “facilities.”
• Applies to both the facility’s bill and the bills by medical
professionals for services to patients at the facility.
• This portion generally does NOT apply to services at a
SNF or free-standing clinic.*
6 © 2023 Fredrikson & Byron, P.A.
6
Overview: Two Rules In One?
• Professionals/organizations that take patients to
hospitals or ASCs have a notice requirement.
• The second part of the rule requires a “Good Faith
Estimates” of charges. While it also applies to
“Facilities” the term is defined differently for this
provision.
7 © 2023 Fredrikson & Byron, P.A.
7
© 2020 MedLearn Media, Inc. 4
Key Definition: “Facilities” That
Must Provide a GFE
• Facility: Health care facility (facility) means an institution (such as a
hospital or hospital outpatient department, critical access hospital,
ambulatory surgical center, rural health center, federally qualified health
center, laboratory, or imaging center) in any State in which State or
applicable local law provides for the licensing of such an institution, that
is licensed as such an institution pursuant to such law or is approved by
the agency of such State or locality responsible for licensing such
institution as meeting the standards established for such licensing.
8 © 2023 Fredrikson & Byron, P.A.
8
Overview
• Some provisions apply to health plans,
others apply to “facilities” and
professionals.
• Unfortunately, the law uses the term
“provider” to refer to “professionals.”
9 © 2023 Fredrikson & Byron, P.A.
9
© 2020 MedLearn Media, Inc. 5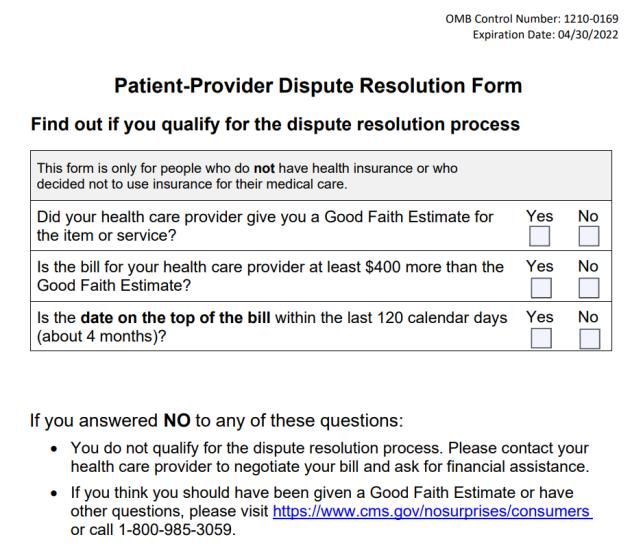
10
10
Overview
• Emergency Services: applies to services
at out-of-network hospitals and the
professionals providing services there.
• Non-emergency Services: applies to
services by professionals at a
participating hospital/ASC.
11 © 2023 Fredrikson & Byron, P.A.
11
© 2020 MedLearn Media, Inc. 6
Leap of Faith
• Health plans are required to do many
calculations.
• Professionals and facilities are largely at
their mercy.
12 © 2023 Fredrikson & Byron, P.A.
12
Emergency Services
• For EMTALA services, the patient should be
treated as if in-network. Co-pays/deductibles are
the same as if it was an in-network service.
• Co-pay calculated at the lower of median rate/
billed charge.
• Plans can’t use diagnosis code to determine
coverage.
13 © 2023 Fredrikson & Byron, P.A.
13
© 2020 MedLearn Media, Inc. 7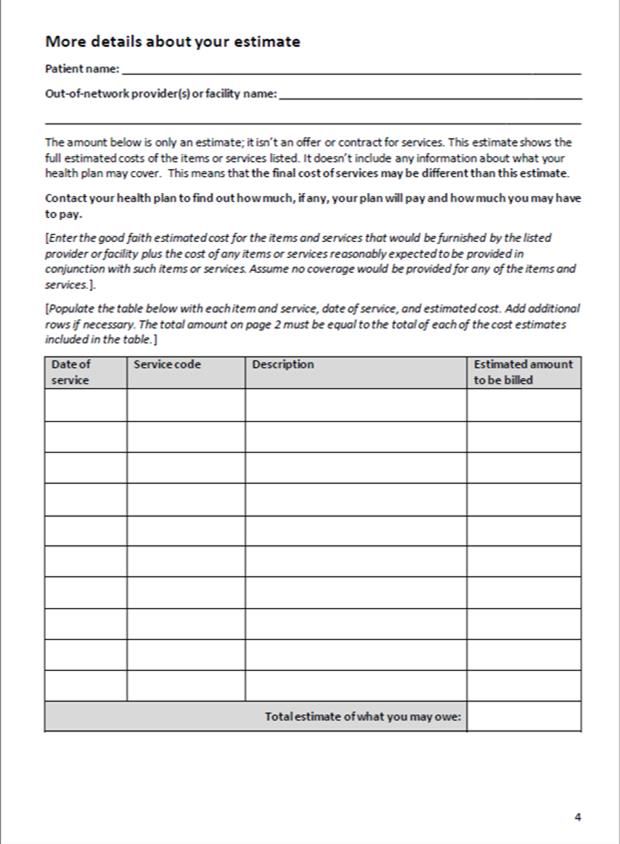
Emergency Services
• The “emergency” continues post-
stabilization until the patient can reasonably
transfer considering distance, patient’s
condition, etc.
• The treating physician is the sole arbiter of
when/how far the patient may go/when
“emergency” ends.
14 © 2023 Fredrikson & Byron, P.A.
14
Emergency Services
• Limited impact on plan payment to facility/professional.
– If there is a state All-Payer Model agreement, it controls.
(MD/VT.)
– If state law, it controls.
– Otherwise, parties negotiate. Absent agreement, use dispute
resolution.
• Plan must make “initial” payment on clean claim within
30 days.
15 © 2023 Fredrikson & Byron, P.A.
15
© 2020 MedLearn Media, Inc. 8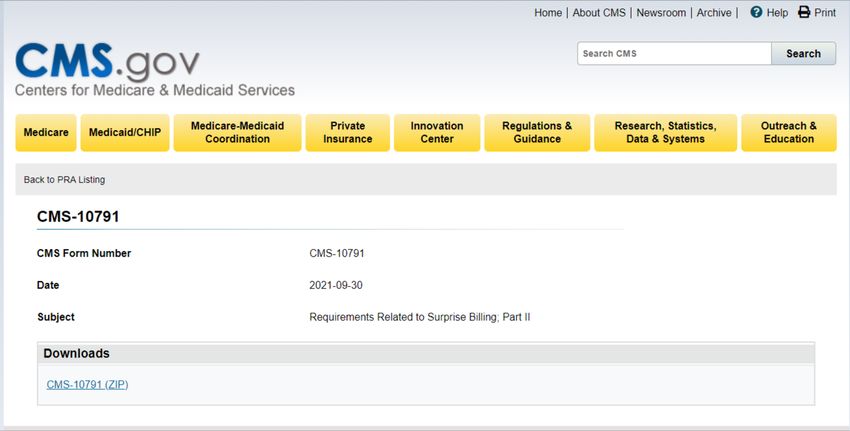
Non-Emergency Services
• For some non-emergency services, the
facility/professional can condition treatment
on the patient agreeing to permit balance
billing.
• Patient consent is required.
• There is a HUGE exception. Can’t seek
consent for “ancillary services.”
16 © 2023 Fredrikson & Byron, P.A.
16
“Ancillary Services”
• Items and services “related to” emergency medicine,
anesthesiology, pathology, radiology and neonatology.
(Mentions physicians and non-physician practitioners)
• Items and services “provided by” assistants at surgery,
hospitalists and intensivists.
• “Diagnostic services” such as radiology and laboratory.
• Any item or service provided by a non-participating
professional if there is no participating professional who
could provide the service.
17 © 2023 Fredrikson & Byron, P.A.
17
© 2020 MedLearn Media, Inc. 9
Independent Dispute Resolution (IDR)
• Determines payment rate for items and services
when the facility or professional and plan can’t
agree.
• Baseball-arbitration.
• Presumption that QPA is the appropriate
amount. (The focus of NSA litigation.)
18 © 2023 Fredrikson & Byron, P.A.
18
Ongoing Litigation
• Texas Medical Ass’n, et al. v United States
Department of Health and Human Services,
et al.
– Struck portions of regulations
implementing the QPA as the default
outcome of the arbitration process
– Did not impact any other rulemaking
19 © 2023 Fredrikson & Byron, P.A.
19
© 2020 MedLearn Media, Inc. 10IDR Action Timeline
Initiate open negotiation period (one party) 30 business days, starting on the day of initial payment or notice
of denial of payment
Initiate IDR process (either party) 4 business days, starting the business day after the open
negotiation period ends
Mutually pick IDR entity 3 business days after the independent dispute resolution
*NOTE: Departments select certified independent dispute initiation date
resolution entity in the case of no conflict-free selection by
parties
Submit payment offers and additional information to certified 10 business days after the date of certified independent dispute
independent dispute resolution entity resolution entity selection
Payment determination made 30 business days after the date of certified independent dispute
resolution entity selection
Payment submitted to the applicable party 30 business days after the payment determination
20
20
21 © 2023 Fredrikson & Byron, P.A.
21
© 2020 MedLearn Media, Inc. 11Four Patient-facing “Forms”
Standard Disclosure “Universal”
Good Faith Estimate
• 42 CFR § 149.430
• 42 CFR § 149.610
• Model form (CMS Form No. 10780)
• Model form (CMS Form No. 10791)
Standard Notice & Consent Standard Notice & Consent
OON Non-Emergency Services OON Post Stabilization Emergency
• 42 CFR § 149.20 Services
• 42 CFR § 149.10
• Mandatory form (CMS Form No. 10780)
• Mandatory form (CMS Form No. 10780)
22 © 2023 Fredrikson & Byron, P.A.
22
Four Patient-facing “Forms”
Standard Disclosure “Universal”
Good Faith Estimate
• 42 CFR § 149.430
• 42 CFR § 149.610
• Model form (CMS Form No. 10780)
• Model form (CMS Form No. 10791)
Standard Notice & Consent Standard Notice & Consent
OON Non-Emergency Services OON Post Stabilization Emergency
• 42 CFR § 149.20 Services
• 42 CFR § 149.10
• Mandatory form (CMS Form No. 10780)
• Mandatory form (CMS Form No. 10780)
23 © 2023 Fredrikson & Byron, P.A.
23
© 2020 MedLearn Media, Inc. 1224 © 2023 Fredrikson & Byron, P.A.
24
25 © 2023 Fredrikson & Byron, P.A.
25
© 2020 MedLearn Media, Inc. 13Model Disclosure: CMS Form No. 10780
Hospitals, ASCs, Freestanding EDs and
“physician or health care providers” must:
• Post on website.
• Have a sign posted prominently at the
location of facility or provider.
• 2 sided, 12-point font form provided to
insured patients.
26 © 2023 Fredrikson & Byron, P.A.
26
Must SNFs Post The Sign?
• Not a “facility” for this part of the rule.
• A “physician or health care provider” is a “physician or
other health care provider who is acting within the
scope of practice of that provider’s ciense or
certification under applicable State law, but does not
include a provider of air ambulance services.”
• “Physician or health care provider” would seem to be
people. But why the underlined phrase?
27 © 2023 Fredrikson & Byron, P.A.
27
© 2020 MedLearn Media, Inc. 14How Many Signs Do We Need?
• 149.430:
28 © 2023 Fredrikson & Byron, P.A.
28
Do We Have To Give The
Notice Every Visit? Annually?
• 149.430 requires you to “provide to
any individual” a copy of the notice.
• Can notice ever be “unprovided?”
29 © 2023 Fredrikson & Byron, P.A.
29
© 2020 MedLearn Media, Inc. 1530 © 2023 Fredrikson & Byron, P.A.
30
No. 2 – Universal Good Faith Estimate
• This is UNIVERSAL! Applies broadly to licensed health care
entities.
31 © 2023 Fredrikson & Byron, P.A.
31
© 2020 MedLearn Media, Inc. 16“Facilities” That Must Provide a
GFE:
• Facility: Health care facility (facility) means an institution (such as a
hospital or hospital outpatient department, critical access hospital,
ambulatory surgical center, rural health center, federally qualified health
center, laboratory, or imaging center) in any State in which State or
applicable local law provides for the licensing of such an institution, that
is licensed as such an institution pursuant to such law or is approved by
the agency of such State or locality responsible for licensing such
institution as meeting the standards established for such licensing.
32 © 2023 Fredrikson & Byron, P.A.
32
No. 2 – Universal Good Faith Estimate
• This is UNIVERSAL! Applies broadly to licensed health care
entities.
• Must provide in “clear and understandable language” the “good
faith estimate” of the “expect charges for providing scheduled
services and items.”
• CMS Form No. 10791
– Appendix 1: Right to Receive a Good Faith Estimate of Expected Charges
Notice.
– Appendix 2: Good Faith Estimate Template.
– Appendix 11: Good Faith Estimate Data Elements.
33 © 2023 Fredrikson & Byron, P.A.
33
© 2020 MedLearn Media, Inc. 17Who Gets the Estimate?
January 1, 2022 Future
If patient is insured, the estimate will
If patient is not using insurance, the go to the insurance company to
inform the advanced EOB that the
estimate goes to the patient.
company must provide the insured
patient.
34 © 2023 Fredrikson & Byron, P.A.
34
Who Gives the Estimate?
Eventually one estimate generated cooperatively by all
responsible parties:
• “Convening health care provider” or “convening
health care facility”: Whoever schedules.
• “Co-health care provider” or “co-health care facility”:
Everyone else.
• The 1/1/23 date has been indefinitely delayed.
35 © 2023 Fredrikson & Byron, P.A.
35
© 2020 MedLearn Media, Inc. 18Who Is The Convenor?
• The “convening” professional or facility is the
party that receives the initial estimate
request and who is or, in the case of a
request, would be responsible for scheduling
the primary item or service.
• 42 CFR 149.610(a)(2)(ii)
36 © 2023 Fredrikson & Byron, P.A.
36
37
© 2020 MedLearn Media, Inc. 19Who Is The Convenor?
• The “convening” professional or facility is the
party that receives the initial estimate
request and who is or, in the case of a
request, would be responsible for scheduling
the primary item or service.
• 42 CFR 149.610(a)(2)(ii)
38 © 2023 Fredrikson & Byron, P.A.
38
Responsibilities of Convening
Professional or Facility
• Make information about the availability of requesting an estimate readily
available online and in accessible formats, including language of patient.
• “Do you plan to use insurance to pay for the visit?”
• If not, inform them orally and in writing of the availability of a good faith estimate
of expected charges.
• Provide an estimate if patient requests appointment, asks for estimate, or
inquires about costs.
• If there is a co-professional or co-facility, contact within one business day of
scheduling the appointment OR a request for an estimate.
39 © 2023 Fredrikson & Byron, P.A.
39
© 2020 MedLearn Media, Inc. 20Co-professional or Co-facility
(Not Enforced Yet)
• Provide good faith estimate to convening professional/facility no later than one business
day after request received from convening professional/facility.
• Estimate must include:
– Patient name and date of birth.
– Itemized list of items or services expected to be provided by the co-provider or co-facility that
are reasonably expected to be furnished in conjunction with the primary item or service as
part of the period of care.
– Applicable diagnosis codes, expected service codes, and expected charges associated with
each listed item or service.
– Name, National Provider Identifiers, and Tax Identification Numbers of the co-provider or co-
facility, and the State(s) and office or facility location(s) where the items or services are
expected to be furnished by the co-professional or co-facility.
– A disclaimer that the good faith estimate is not a contract and does not require the uninsured
(or self-pay) individual to obtain the items or services from any of the co-professional or co-
facilities identified in the good faith estimate.
40 © 2023 Fredrikson & Byron, P.A.
40
What Does the Patient’s Good Faith
Estimate Need to Include?
Highlights:
• Patient’s name, DOB, NPI, Tax ID.
• Diagnosis codes (ICD).
• Expected service codes (CPT, HCPCS, DRG, NDC).
• “Expected charges” associated with each listed item or service.
“Expected charge” means, for an item or service, “the cash pay rate or rate
established by a provider or facility for an uninsured (or self-pay) individual,
reflecting any discounts for such individuals, where the good faith estimate is
being provided to an uninsured (or self-pay) individual; or the amount the provider
or facility would expect to charge if the provider or facility intended to bill a plan or
issuer directly for such item or service when the good faith estimate is being
furnished to a plan or issuer.”
41 © 2023 Fredrikson & Byron, P.A.
41
© 2020 MedLearn Media, Inc. 21Can I Share Price Information With
Others?
• Some fear of sharing pricing data is
overblown. Agreement on price is illegal.
Knowledge is not.
• Here the law requires it.
• How much protection does that provide?
42 © 2023 Fredrikson & Byron, P.A.
42
When Is the Estimate Required?
• Estimate is required if appointment is scheduled for 3 or more
business days in advance:
‒ When the appointment is scheduled 3-9 business days out, the notice
must be provided within 1 business day of the date the appointment
was scheduled.
‒ If scheduled for 10 or more business days out, the estimate must be
provided within 3 business days of the date the appointment was
scheduled.
• Patient can also request an estimate without scheduling an
appointment, in which case the estimate must be provided within
3 business days.
43 © 2023 Fredrikson & Byron, P.A.
43
© 2020 MedLearn Media, Inc. 22How Do We Count Business Days?
• The government counts the day of the
call:
– Call Friday, estimate needed for visits
Wednesday or later.
• Is that right? We shall see.
• Note it is NOT hours.
44 © 2023 Fredrikson & Byron, P.A.
44
What If the Estimate Changes?
• Provide the uninsured (self-pay) patient a new estimate no
later than one business day before the appointment.
• If change occurs less than one business day before
appointment is scheduled, the replacement professional or
facility must use the good faith estimate of expected
charges.
45 © 2023 Fredrikson & Byron, P.A.
45
© 2020 MedLearn Media, Inc. 23Patient-Provider Dispute Resolution
• Patient can use this process IF ALL 5 conditions are met:
– They’re uninsured or self-pay
– They scheduled and received the medical items or services on
or after January 1, 2022
– They have a good faith estimate from your provider or the
facility who provided your care
– They got a bill within the last 120 calendar days
– The difference between the good faith estimate and the bill is
at least $400
46 © 2023 Fredrikson & Byron, P.A.
46
How is the $400 Calculated?
• It is the total per “provider”.
• The examples from the government
don’t make it clear if each “professional”
is a provider.
• The examples don’t have one situation
where an estimate is LOWER than the
bill!
47 © 2023 Fredrikson & Byron, P.A.
47
© 2020 MedLearn Media, Inc. 2448 © 2023 Fredrikson & Byron, P.A.
48
Important Notes
• Estimates are considered part of medical
record.
• Meeting a similar state requirement does
NOT meet federal requirement.
• Reminder: Future rulemaking for insured
patients.
49 © 2023 Fredrikson & Byron, P.A.
49
© 2020 MedLearn Media, Inc. 25No. 3 – Standard Notice & Consent
• OON professionals at in-network facilities
cannot balance bill for non-emergency
services unless:
– They obtain the “Standard Notice & Consent”, AND
– The service is more than 3 hours out, AND
– The services are NOT ancillary services.
50 © 2023 Fredrikson & Byron, P.A.
50
When Can Balancing Billing Protections
Be Waived?
• Non-emergency care.
• Non-ancillary services.
• Not prohibited by state law.
• In network care is available.
• Timing:
– If appointment is scheduled at least 72 hours or more out, provide Notice & Consent at least
72 hours before the appointment.
– If appointment is scheduled within the next 72 hours, provide Notice & Consent the same day
appointment is made and at least 3 hours prior to rendering the services or items.
– If treatment will occur within 3 hours, patient cannot consent to be balance billed.
51 © 2023 Fredrikson & Byron, P.A.
51
© 2020 MedLearn Media, Inc. 26What Must the Standard Notice &
Consent Include?
HHS has created a MANDATORY document (CMS Form No.
CMS-10780).
– 4 pages:
• Page 1 – Notice
• Pages 2 & 4 – Estimate of services
• Page 3 – Consent
– It CANNOT be modified (except filling in bracketed sections).
– It CANNOT be attached or incorporated with other documents.
– Patient MUST be able to choose to receive electronically or in paper.
– Make available in 15 languages most commonly used in region.
– Must include date notice provided to patient and the date AND time
patient signs.
52 © 2023 Fredrikson & Byron, P.A.
52
Pages 2
&4–
Estimate
53 © 2023 Fredrikson & Byron, P.A.
53
© 2020 MedLearn Media, Inc. 27How to Calculate Estimate?
• Use definition of the “expected charge” that
would apply when the good faith estimate is
provided to a plan or issuer.
• PROBLEM: We don’t have this guidance yet
from HHS and the non-enforcement position
does not extend to the requirement to provide a
good faith estimate.
‒ HHS is seeking comment.
54 © 2023 Fredrikson & Byron, P.A.
54
Page 3 – Consent
55 © 2023 Fredrikson & Byron, P.A. © 2023 Fredrikson & Byron, P.A.
55
© 2020 MedLearn Media, Inc. 28Steps to Provide Notice & Consent
• Determine if you plan to balance bill.
• If yes, determine if waiver of protections is allowed here.
• Provide the notice & consent during applicable timing.
• Mail or email copy of the signed written notice and consent to the patient
(patient preference).
• Must retain, or ensure someone else is, a copy of the consent & notice for
at least 7-year period after date care provided.
• Notify the plan or issuer that care was provided during a visit.
56 © 2023 Fredrikson & Byron, P.A.
56
No. 4 – Notice & Consent
(Post Stabilization Emergency Care)
• Generally, a nonparticipating emergency facility and
nonparticipating professional cannot bill patients more than
cost-sharing for emergency services.
• BUT, may if 4 conditions are met.
57 © 2023 Fredrikson & Byron, P.A.
57
© 2020 MedLearn Media, Inc. 29Condition #1
• Attending emergency physician or treating provider
determines (taking into account the individual’s medical
condition):
– Patient can travel using nonmedical transportation or
nonemergency medical transportation.
– Available participating provider or facility located within a
reasonable travel distance.
58 © 2023 Fredrikson & Byron, P.A.
58
Condition #2
• Meet OON notice and consent criteria for non-
emergency services (42 CFR§149.420(c) through (g)).
• PLUS
– If a participating emergency facility and a nonparticipating professional,
notice and consent must include list of any participating professionals at the
facility able to provide the items and services involved and notification that
the patient may be referred, at their option, to such a participating provider.
– If a nonparticipating emergency facility, notice must include good faith
estimated amount that the patient may be charged for items or services
provided by the nonparticipating emergency facility or nonparticipating
professionals with respect to the visit at such facility.
59 © 2023 Fredrikson & Byron, P.A.
59
© 2020 MedLearn Media, Inc. 30Condition #3
• Attending emergency physician or
treating provider, using appropriate
medical judgment, determines patient
can:
‒ Receive the notice & consent and
– Provide informed consent.
60 © 2023 Fredrikson & Byron, P.A.
60
Condition #4
• Any additional requirements or
prohibitions as may be imposed under
state law.
61 © 2023 Fredrikson & Byron, P.A.
61
© 2020 MedLearn Media, Inc. 31Steps to Provide OON Post Stabilization
Emergency Care Services Notice & Consent
• Determine if you plan to balance bill.
• If yes, determine if waiver of protections is allowed here (can you meet the 4
conditions?).
• Provide the notice & consent within timing requirements.
• Mail or email copy of the signed written notice and consent to the patient (patient
preference).
• A participating health care facility (with respect to non-participating professional)
must retain copy of the consent & notice for at least 7-year period after date care
provided. IF the nonparticipating professional obtains the notice & consent (as
opposed to the facility obtaining on behalf of the professional), the professional may
either (1) coordinate with facility to retain it OR (2) the professional can retain it.
• Notify the plan or issuer that care was provided during a visit.
62 © 2023 Fredrikson & Byron, P.A.
62
CMS Slideshow
• https://www.cms.gov/files/document/a27
4577-1a-training-1-balancing-
billingfinal508.pdf
63 © 2023 Fredrikson & Byron, P.A.
63
© 2020 MedLearn Media, Inc. 32Knowledge Checking The Knowledge Check
64 © 2023 Fredrikson & Byron, P.A.
64
Knowledge Checking The Knowledge Check
65 © 2023 Fredrikson & Byron, P.A.
65
© 2020 MedLearn Media, Inc. 33Do They Know What “Or” Means?
• The attending emergency physician or treating provider
determines that the participant, beneficiary, or enrollee is able
to travel using nonmedical transportation or nonemergency
medical transportation to an available participating provider or
facility located within a reasonable travel distance, taking into
account the individual's medical condition. The attending
emergency physician's or treating provider's determination is
binding on the facility for purposes of this requirement.
• 42 CFR 149.410(b)(1)
66 © 2023 Fredrikson & Byron, P.A.
66
Bottom Line
• 4 Patient facing “forms”:
– Standard Disclosure.
– Universal Good Faith Estimate Notice.
– OON Non-emergency Services Notice & Consent.
– OON Post Stabilization Emergency Care Notice & Consent.
• Put processes in place:
– Update website and physical space with Standard Disclosure.
– When/how to provide Universal Good Faith Estimate.
– When/how to provide OON Notices & Consents.
– How to handle IDR open negotiation period.
– How to handle patient-provider dispute resolution open negotiation period.
67 © 2023 Fredrikson & Byron, P.A.
67
© 2020 MedLearn Media, Inc. 34Commonly Asked Questions
68
How to Issue a GFE When Charging a
Flat Monthly or Annual Fee
• Examples: Concierge services, direct primary care
• Letter from American Academy of Family
Physicians, dated December 3, 2021, requested
HHS issue future regulations
• Current advice: Technically required, consider
issuing an annual GFE
69 © 2023 Fredrikson & Byron, P.A.
69
© 2020 MedLearn Media, Inc. 35Must GFE Be Translated?
• Unlike the Standard Notice and
Consent, there is no specified number
of languages.
• If the patient contests a bill, and the
notice wasn’t in their native tongue,
regs suggest they didn’t receive notice.
70 © 2023 Fredrikson & Byron, P.A.
70
Should We Use The Model GFE?
71 © 2023 Fredrikson & Byron, P.A.
71
© 2020 MedLearn Media, Inc. 36Does a SNF Need to Give A GFE?
• Legal and practical answer may differ.
• They are licensed.
• Is the patient using insurance to pay?
72 © 2023 Fredrikson & Byron, P.A.
72
The Hospital is OON the Dr. In-
Network. Does NSA Apply?
• Is it an emergency service?
• If not, then nope!
73 © 2023 Fredrikson & Byron, P.A.
73
© 2020 MedLearn Media, Inc. 37Must We Give GFE to Medicare
Pts. Getting A Physical?
74 © 2023 Fredrikson & Byron, P.A.
74
The Patient Doesn’t Want
Their Birthdate on the GFE!
• No provision explicitly permits the
patient to decline.
• This is a patient protection measure.
Can the patient waive?
75 © 2023 Fredrikson & Byron, P.A.
75
© 2020 MedLearn Media, Inc. 38How Long Must We Keep GFEs?
• Must provide for 6 years.
• Must consider it a part of the medical
record.
• 149.610(f)
76 © 2023 Fredrikson & Byron, P.A.
76
When Will the Rules Be Issued?!
• GFE requirements for insured
patients?
• Penalties! Namely, what is the exact
consequence of NOT issuing a GFE?
• Maybe May 2022????*
*Def.’s Reply Memo in Support of Their Cross-Motion For Summary Judgment, Texas Medical Association v.
U.S. Department of Health and Human Services (Civil Action No. 6:21-cv-00425-JDK), filed February 2, 2022,
https://affordablecareactlitigation.files.wordpress.com/2022/02/13362908-0-79761.pdf.
77 © 2023 Fredrikson & Byron, P.A.
77
© 2020 MedLearn Media, Inc. 39RESOURCES
DOL Website
– https://www.dol.gov/agencies/ebsa/laws-
and-regulations/laws/no-surprises-act
CMS Website
– https://www.cms.gov/nosurprises/Policies-
and-Resources/Overview-of-rules-fact-
sheets
78 © 2023 Fredrikson & Byron, P.A.
78
Questions?
David Glaser
Fredrikson & Byron, P.A.
612.492.7143
dglaser@fredlaw.com
79
© 2020 MedLearn Media, Inc. 40You can also read