Conflict of Interest Disclosure - I have no financial, intellectual, or personal conflicts of interest with any of the material in today's ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
4/29/21
The Science of Maximizing
Patient Alliance and Engagement
in Physical Therapy Practice
JW Matheson PT, DPT, MS, SCS, OCS, CSCS
1
Conflict of Interest Disclosure
I have no financial, intellectual, or personal
conflicts of interest with any of the material in
today’s presentation.
Thank you for your time and the opportunity
to present this information today.
2
1
4/29/21
Pre-Presentation Questions
1. Why do you think your patients get
better?
2. Why do so many different
interventions and or approaches
seem to work for a patient with non-
surgical knee pain or spine pain?
3
Introduction
• Physical Therapist for 25 years
• Sports Residency 2000-2001
• Have worked in several different hospital, academic, and
private practice settings
• Involved in Sports and Orthopedic Academies of the APTA
• Private practice owner 2013-2020
4
2
4/29/21
Introduction
• Biggest interests
• Translating scientific research into practice
• Meta-research (critical analysis of research methods)
• Teaching and learning from PT students
• Trying to answer these questions
• How to best meet the needs of the patient in front of me?
• Why do patients with the same conditions get better despite all
the different treatments we do?
• What is warranted v. unwarranted practice variation
5
Evidence-Based Practice vs
Patient Centered Practice
• While
“… Worked
both thein hospital,
EBM movementacademia, and private
and the patient centered practice
care movement have challenged
settings
medicine to move forward in an entirely necessary manner – EBM actively insisting that greater
attention should be given to the results of biomedical and technological advance and patient-
• Involved in Sports and Orthopedic Academies of APTA
centered care insisting that greater attention should be given to the needs of the individual
patient – both models ultimately lack a vision of medical practice that logically accords with the
• Private practice owner 2013-2020
Hippocratic ideals and historic mission of medicine as a science-using and compassionate
practice, centered upon the persons of the patient and the clinician(s) engaged in a mutual and
dialogical process of shared decision-making, focused on the patient’s best interests, within a
relationship of equality, responsibility and trust.”
Miles A. From evidence-based to evidence-informed, from patient-focused to
person-centered-The ongoing "energetics" of health and social care discourse as
we approach the Third Era of Medicine. J Eval Clin Pract. 2017;23(1):3-4.
6
3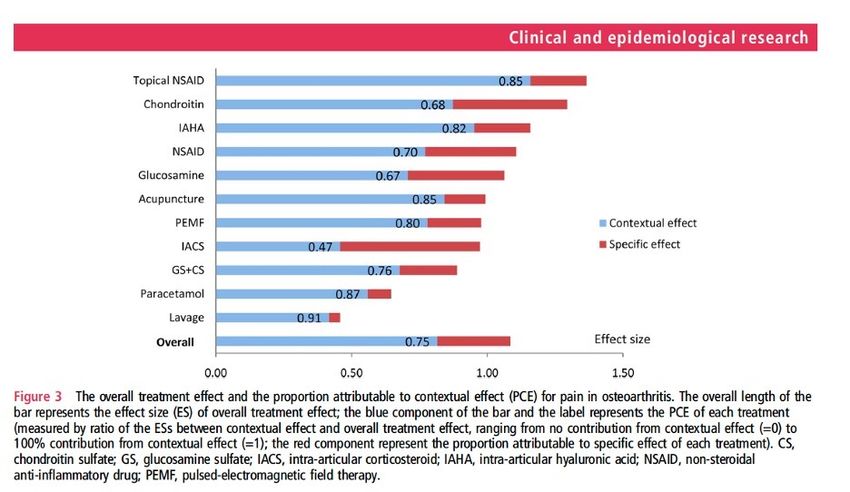
4/29/21
Providing Value-Based Care as a PT
Cook CE, Denninger T, Lewis J, Diener I, Thigpen C. Providing value-based
care as a physiotherapist. Arch Physiother. 2021;11(1):12.
7
Current Favorite Quote
When we are no longer able to change a situation, we are
challenged to change ourselves.
Everything can be taken from an individual but one thing: the
last of the human freedoms—to choose one’s attitude in any
given set of circumstances, to choose one’s own way.
Between stimulus and response there is a space. In that
space is our power to choose our response. In our response
lies our growth and our freedom.
Victor Frankl – Man’s Search for Meaning 1946
8
4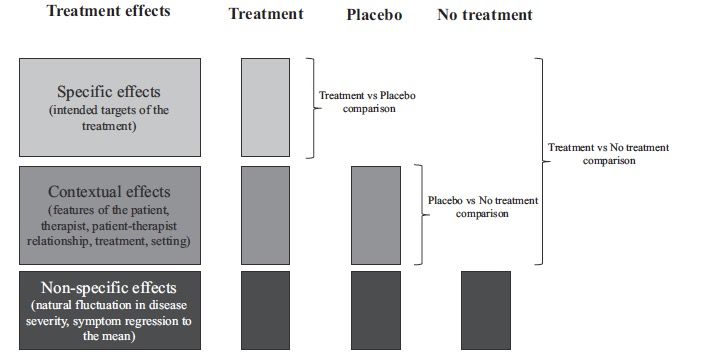
4/29/21
Today’s Objectives
1. Describe the Common Factors model of
Psychotherapeutic practice and be able
to discuss its relationship to the PT
practice model
2. Be able to recognize the contextual
effects of PT evaluation and treatment
9
Today’s Objectives
3. Evaluate one’s ability to maximize the 5
“E’s” of patient engagement to maximize
the contextual effects of a patient
encounter & improve the therapeutic
alliance
4. Be able to apply the BATHE model of
questioning in your next patient evaluation
10
5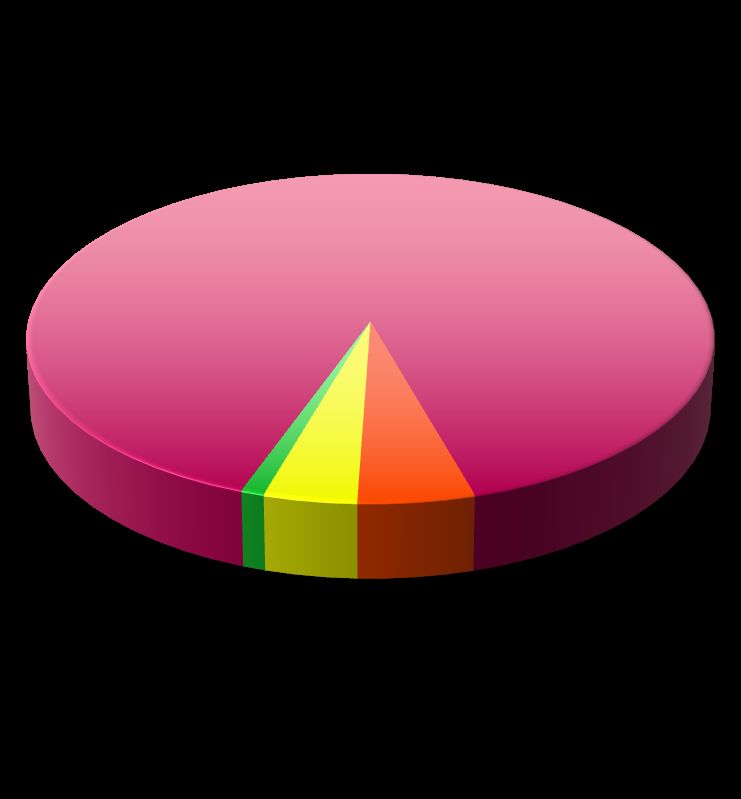
4/29/21
TREATMENT INTERVENTION EFFECTS
Measured improvement after a physical therapy visit
may be the result of the:
1. Specific effects of the treatment
2. Non-specific effects of the treatment
3. General or “Contextual Effects” of the treatment
4. Unexplained variability of the treatment
11
Contextual Effects of PT Treatment
Cashin AG, McAuley JH, Lamb SE, Lee H. Disentangling contextual effects
from musculoskeletal treatments. Osteoarthritis Cartilage. 2021.
12
6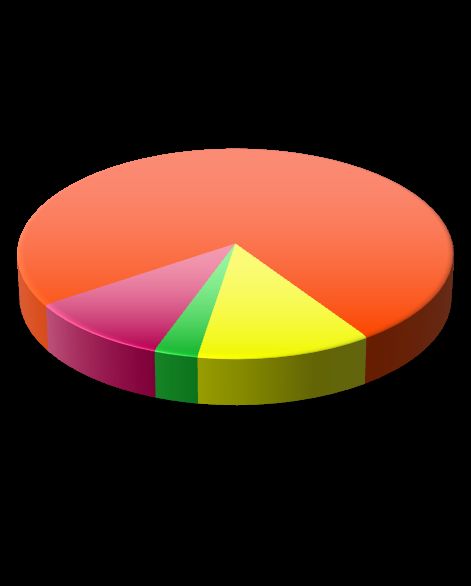
4/29/21
I wish I would have been an Infectious Disease Specialist MD!
• “kill bug, don’t kill bug”
Intervention Effect %
• Less variability than when
90%
dealing with pain
• The influence of contextual 1%
4% 5%
effects is limited on the
desired outcome Specific Contextual Non-Specific Unexplained
13
What really happens in an episode of PT with a
“Patient in Pain?”
Combination of interventions having a percentage of specific, non-specific,
contextual and unexplained treatment effects
Intervention Effect Intervention Effect Intervention Effect
% % %
75 % 40%
30% 70% 10%
10% 25%
12% 15%
5% 5%
3%
Specific Contextual Specific Contextual Specific Contextual
Non-Specific Unexplained Non-Specific Unexplained Non-Specific Unexplained
14
7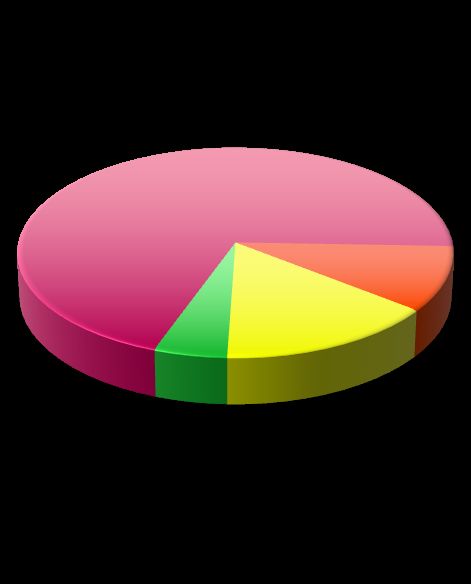
4/29/21
Contextual Effects of PT Treatment
Whiteside N, Sarmanova A, Chen X, et al. Proportion of contextual effects in the
treatment of fibromyalgia-a meta-analysis of randomized controlled trials. Clin
Rheumatol. 2018;37(5):1375-1382.
15
Zou K, Wong J, Abdullah N, et al. Examination of overall treatment effect and the proportion
attributable to contextual effect in osteoarthritis: meta-analysis of randomized controlled trials. Ann
Rheum Dis. 2016;75(11):1964-1970.
16
8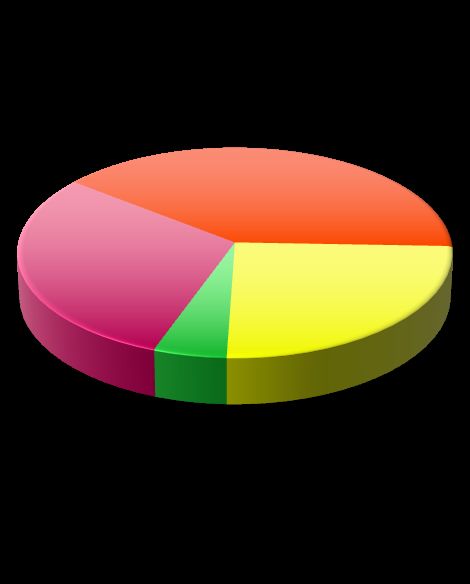
4/29/21
The Dodo Bird Debate and Common Factors
Theory in Psychotherapy
• Dodo bird verdict coined by Psychologist Saul
Rosenweig in 1936 to illustrate the notion that all
therapies are equally effective
• Debate is focused on if the specific components of
different treatments lead some treatments to
outperform other treatments for specific disorders
17
The Dodo Bird Debate and Common Factors
Theory in Psychotherapy*
Proponents contend that all psychotherapies are equivalent because of
"common factors" that are shared in all treatments (i.e., having a relationship
with a therapist who is warm, respectful, and has high expectations for client
success).
Opponents of the Dodo bird verdict argue that the specific techniques used
in different therapies are important, and that all therapies do not produce
equivalent outcomes for specific mental disorders.
*Wikipedia link here
18
94/29/21
Common Factors Theory in PT
Evidence from systematic reviews of hands-on physical
therapy techniques indicate that common factors (e.g., non-
specific and/or contextual) across interventions contribute
more to treatment outcomes than effects associated with the
specific technical intervention.
Miciak et al, A Review of the psychotherapeutic ‘common factors’ model and it’s application in physical therapy: the need to
consider general effects in physical therapy practice. Scandinavian J Caring Sci, 26:394-403.
Miciak et al, A framework for establishing connections in physiotherapy practice, Physiotherapy Theory and Practice, DOI:
10.1080/09593985.2018.1434707
Miciak et al. The necessary conditions of engagement for the therapeutic relationship in physiotherapy: an interpretive
description study Archives of Physiotherapy (2018) 8:3
19
How does this relate to PT/OT practice?
20
104/29/21
From Miciak et al. , 2012
“Similar to evidence from psychotherapy research, it
appears that divergent interventions with different
theoretical underpinnings and anticipated specific treatment effects
result in comparable clinical outcomes.”
“In fact, even interventions tailored to address broader bio-
psychosocial factors have found only modestly improved results when
compared with traditional exercise-based physical therapy (18–21).”
21
From Miciak et al. , 2012
“The current evidence provides little support for choosing one
approach over another. More critically, the evidence provides little
support for any of the theories underlying these different
therapeutic modalities.”
“It is quite likely that at least a component of the positive outcomes
are the result of general effects arising from the common
therapeutic factors, in addition to any specific effects from the
interventions."
22
114/29/21
Therapeutic Alliance in PT/OT
23
The Therapeutic or Working Alliance
• When patients arrive at a PT/OT appointment, they expect to find
clinicians with whom they can develop a close professional
relationship
• Patients expect that their therapists will want the same outcomes for
them that they want for themselves
• They expect that therapists will suggest ways to attain these goals
that they will find acceptable.
24
124/29/21
The Therapeutic or Working Alliance
1. Therapist & Patient agreement on goals
2. Therapist & Patient agreement on interventions
(tasks)
3. Affective bond between patient & therapist
Bodin, Psychotherapy: Theory, Research, and Practice, 1979
25
How Therapeutic Alliance is Measured
• Working Alliance Inventory
• 36-item long form with 7-point Likert scale
• Translated into many languages
• Short forms and other modifications have been investigated
• Has been adapted to be completed by therapist as well as
patient
• May be found at https://wai.profhorvath.com/downloads
26
134/29/21
Influence of Alliance on PT Outcomes in Patients
with Low Back Pain
• One hundred eighty-two patients with chronic LBP who volunteered for a
RCT that compared the efficacy of exercises and spinal manipulative
therapy rated their alliance with physical therapists by completing the
Working Alliance Inventory at the second treatment session.
• Primary outcomes of function, global perceived effect of treatment, pain,
and disability were assessed before and after 8 weeks of treatment.
• Linear regression models were used to investigate whether the alliance
was a predictor of outcome or moderated the effect of treatment.
Ferreira PH, Ferreira ML, Maher CG, et al. The therapeutic alliance between clinicians
and patients predicts outcome in chronic low back pain. Phys Ther. 2013;93(4):470-478.
27
Influence of Alliance on PT Outcomes in Patients
with Low Back Pain
• The therapeutic alliance was consistently a predictor of
outcome for all the measures of treatment outcome.
• Higher levels of therapeutic alliance were associated
with greater improvements in perceived effect of
treatment, function, and reductions in pain and
disability.
Ferreira PH, Ferreira ML, Maher CG, et al. The therapeutic alliance between clinicians
and patients predicts outcome in chronic low back pain. Phys Ther. 2013;93(4):470-478.
28
144/29/21
Recent reviews of the limited research on the
therapeutic alliance in musculoskeletal care
illustrates that we have more questions than
answers in 2021
Babatunde F, MacDermid J, MacIntyre N. Characteristics of therapeutic
alliance in musculoskeletal physiotherapy and occupational therapy practice:
a scoping review of the literature. BMC Health Serv Res. 2017;17(1):375.
29
More research questions on Alliance
between PT/OT and Patient
– What is the role of the Alliance in physical therapy (PT)? Can we study it
as a construct?
– What is the relation between a positive Alliance and success in PT?
– What is the path of Alliance over time? (Longitudinal change)
– What are the variables that predispose individuals to develop a strong
Alliance?
– What are the in-session factors that influence the development of a
positive Alliance?
Babatunde F, MacDermid J, MacIntyre N. Characteristics of therapeutic alliance in
musculoskeletal physiotherapy and occupational therapy practice: a scoping review of the
literature. BMC Health Serv Res. 2017;17(1):375.
30
154/29/21
Maximizing the Therapeutic Alliance With
Every Patient During a PT Session
31
Engage the patient
Adapted from Table 2 from Jamison, Nonspecific
Treatment Effects in Pain Medicine IASP, 2011
• Understand the patient’s expectations and concerns
• Greet in a warm, present, and friendly manner and maintain good eye contact
Empathize with the patient
• Be aware of feelings, values, and thoughts
• Employ humor where appropriate
Educate the patient
• Assess what the patient understands
• Address key concerns
Enlist the patient
• Seek patient’s input on treatment plan
• Negotiate priorities
End the visit
• Anticipate and forecast the end of the visit
• Restate the plan and express personal confidence, caring and hope
The 5 “E’s” to Maximize Contextual Effects
32
164/29/21
Context and Expectations are Critical
• PSRs are “Directors of
First Impressions”
• Consistent scripting is key
• Dad Jokes Rule
• Open gym concept
• All staff must engage with
the patients
33
Engage the patient
Adapted from Table 2 from Jamison, Nonspecific
Treatment Effects in Pain Medicine IASP, 2011
• Understand the patient’s expectations and concerns
• Greet in a warm, present, and friendly manner and maintain good eye contact
Empathize with the patient
• Be aware of feelings, values, and thoughts
• Employ humor where appropriate
Educate the patient
• Assess what the patient understands
• Address key concerns
Enlist the patient
• Seek patient’s input on treatment plan
• Negotiate priorities
End the visit
• Anticipate and forecast the end of the visit
• Restate the plan and express personal confidence, caring and hope
The 5 “E’s” to Maximize Contextual Effects
34
174/29/21
The Profession Needs Research on Shared-Decision Making
(SDM)
PRISMA guidelines were followed for this attempted Systematic
Review. To be considered for review, the study had to meet all the
following criteria:
1. Were prospective studies that involved treatment decision-making
2. Were a RCT design
3. Involved patients faced with having to make a treatment decision
4. Compared SDM with a control intervention
5. Included one or more of the following outcome measures: well-being,
costs, health-related pain or disability measures, or quality of life.
Tousignant-Laflamme Y, Christopher S, Clewley D, et al. Does shared decision making
results in better health related outcomes for individuals with painful musculoskeletal
disorders? A systematic review. J Man Manip Ther. 2017;25(3):144-150.
35
The Profession Needs Research on Shared-Decision Making
(SDM)
• Authors reported that they did not find a single study that
looked at the true effect of SDM on patient reported
outcomes in a population with musculoskeletal pain.
• “Would be wise to explore the effectiveness of SDM before
forcing its large-scale implementation in rehabilitation”
Tousignant-Laflamme Y, Christopher S, Clewley D, et al. Does shared decision making
results in better health related outcomes for individuals with painful musculoskeletal
disorders? A systematic review. J Man Manip Ther. 2017;25(3):144-150.
36
184/29/21
The BATHE Psychotherapeutic Questioning Technique
37
The BATHE Questioning Technique
• Completed after hearing the patient’s chief complaint and determining the patient's
main concern
• Problems are listed and notes are arranged in SOAP fashion. BATHEing your
patients as you SOAP them will give the clinician useful information, takes only 1-2
minutes, screens for emotional problems, and may be therapeutic for the patient.
• The BATHE technique is a simple patient-centered procedure that consists of a
series of 4 specific questions about the patient's background, affect, troubles, and
handling of the current situation, followed by an empathic response.
Lieberman J, Stuart M. The BATHE Method: Incorporating Counseling and
Psychotherapy into the Everyday management of Patients. 1999.
38
194/29/21
The BATHE Questioning Technique
• Using your words and relationship with patients as procedures to affect patients' views of their
reality. (e.g., Alliance).
• Empowers patients to trust themselves and others, confirm their positive feelings about
themselves, and enhance their ability to control the circumstances of their lives.
• The BATHE technique serves as a rough screening test for anxiety, depression, or situational
stress disorders and should be routinely employed.
• The BATHE technique is a specific verbal procedure, thus must be practiced
Lieberman J, Stuart M. The BATHE Method: Incorporating Counseling and
Psychotherapy into the Everyday management of Patients. 1999.
39
The BATHE Technique
– B = Background = “What is going on in Your
Life?”
– A = Affect (Feeling State) = “How does that
make you feel?
– T = Trouble = “What about this situation troubles
you the most?”
– H = Handling = “How are you handling this
situation?”
– E = Empathy – “This must be difficult for you?”
40
204/29/21
41
Leave You With Three Clinical Pearls
1. Instead of asking your patients at the end of the session – “Do you
have any questions?” instead ask “What questions do you have
for me today?”
2. Also ask the patient to repeat back a synopsis of the PT plan of
care. Also ask after 3-4 visits – “Am I meeting your expectations?”
3. What three non-clinical fun facts did you learn about the patient
– (Hobbies, Interests, kids, pets, etc.)
42
214/29/21
Maximize Alliance & Contextual Effects in all
Patient Encounters!
• Ask the BATHE questions
• Accomplish the “5 E’s”
• Be Knowledgeable
• Apply your interventions in a consistent and reproducible manner
• (Have a Plan, Have a Contingency Plan)
• Encourage self-efficacy and patient activation
• Manage both patient and clinician expectations
43
Thank You!! Let’s Discuss!
44
22You can also read

















































