THE CHANGING SITE LANDSCAPE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

appliedclinicaltrialsonline.com Volume 28 Number 9 September 2019
YOU R P EER -R EV IEW ED G UIDE TO G L OBA L C L INICA L T R I A L S M A NAGEMEN T
1992–2019
AC
ACT
ACT
CT
27
ce
Year
o f Se r v i
THE CHANGING
SITE LANDSCAPE
DATA SHARING STUDY START-UP
STEPS TO INTEGRATE REFORM IN ACTION
EXECUTIVE PROFILE TRIAL INSIGHTS CLOSING THOUGHT
Championing Clinical Benchmarking Digital Implementation:
Trial Diversification Rare Disease R&D A Site-First Mindset
An ever-changing journey needs an agile partnership The dynamic nature of drug development and your world, means you need an adaptable partner. By joining forces with you, we provide a highly flexible, expert service covering contract development and manufacturing services for mAbs and viral vectors, product characterization, biosafety testing and toxicology testing services. So whatever direction your project needs to take, we’ll help guide you there. MilliporeSigma, the vibrant M and BioReliance are trademarks of Merck KGaA, Darmstadt, Germany or its affiliates. All other trademarks are the property of their respective owners. Detailed information on trademarks is available via publicly accessible resources. © 2019 Merck KGaA, Darmstadt, Germany and/or its affiliates. All Rights Reserved. The Life Science Business of Merck KGaA, Darmstadt, Germany operates as MilliporeSigma in the US and Canada.

FROM THE EDITOR
Taking Care of Site Business
I
’m really excited about this issue of Applied begin to accredit investigative sites. The Association of Clinical Research
Clinical Trials. Tagged as “The Changing Site Professionals (ACRP) offers certifications of varying clinical research roles,
Landscape,” this is our foray to update in- as does the UK-based International Academy of Clinical Research (IAOCR).
formation presented in September 2018 (see ACRP also rolled out its ACRP Core Competency Framework two years
https://bit.ly/34b0vOf) around different site ago, initiated so industry could begin to level set the various roles at sites
models and bringing clinical trials closer to the and is discussed as a tool used by many in our main feature (see page 24).
point of care. This year, we offer a more in-
depth look at representative models that are Remote Trials. There is some backlash around the terminology of re-
LISA HENDERSON
changing the way investigative sites work. The mote or virtual trials. While many have started calling them decentralized
Editor-in-Chief
“traditional, dedicated research site” is morphing trials, these trials really are around patient centricity and making conve-
to model more efficient, professional, and technologically robust practices nience and location (or inability to get to a site location more specifically)
and processes that rival those of CROs, while specialty physician groups a reality for participants. Clearly, decentralized trials are reserved for the
and large IDNs integrate professional providers that operationalize clinical most appropriate of therapeutic areas and populations. More often than
research within their unique clinical care workflows. Academic centers, not, hybrid trials is the word of the day and means that you offer patients
long the bastion of both innovation and bureaucracy associated with a mix of both on-site and virtual. To that end, sites are incorporating tech-
clinical trial conduct, have instituted change to streamline their business. nologies that enable them to be more competitive for the hybrid models.
And at the Veteran’s Administration, executives are attacking their own
bureaucracies to unify study start-up and make VA clinics a competitive Remove Recruitment from the Site. I attended a meeting where
option for sponsored research. What follows are highlights of trends from physician speakers discussed their role as clinical event adjudicators. One
this issue, as well as trends heard around site practices during the year. view shared was that sponsors or CROs spend about 1% of their time
educating the investigative staff on the study protocol, and 99% on pa-
Professionalism. One recognized problem at sites is the varying levels of tient recruitment. The physicians felt this time allocation should be flipped
performance quality and consistency in staff capabilities. There are many given the importance of protocol adherence for both data and safety
ways now available to help clinical research professionals, as well as sites, reasons. Given the dire straits of patient enrollment, as well as the diverse
establish credibility and professionalism. For example, the Alliance for ways to reach potential participants, it makes sense to take recruitment
Clinical Research Excellence and Safety (ACRES) recently announced it will out of the core site responsibility, and make it a more strategic process.
EDITORIAL OFFICES MARKETING SERVICES MJH LIFE SCIENCESTM
485 Route 1 South, Building F, Second Floor, AUDIENCE DEVELOPMENT MANAGER, CHAIRMAN AND CEO, Mike Hennessy, Sr
Iselin, NJ 08830 USA C.A.S.T. DATA AND LIST INFORMATION VICE CHAIRMAN, Jack Lepping
+1 (732) 346-3080 fax: +1 (732) 647-1235, Melissa Stillwell
PRESIDENT, Mike Hennessy, Jr
EDITOR-IN-CHIEF Lisa Henderson, (218) 740-6831, mstillwell@mmhgroup.com
CHIEF STRATEGY OFFICER & PRESIDENT, AGENCY SERVICES, George Glatcz
lhenderson@mmhgroup.com PERMISSIONS/INTERNATIONAL LICENSING
CHIEF ACCOUNTING OFFICER, David Brennan
MANAGING EDITOR Michael Christel, Alexa Rockenstein, arockenstein@mmhgroup.com
mchristel@mmhgroup.com CHIEF FINANCIAL OFFICER, Neil Glasser, CPA/CFE
REPRINTS Contact our official partner, Wright’s Media,
ASSOCIATE EDITOR Christen Harm, EXECUTIVE VICE PRESIDENT, OPERATIONS, Tom Tolvé
about available usages, license fees, and award seal
charm@mmhgroup.com artwork at ubm@wrightsmedia.com. SENIOR VICE PRESIDENT, CONTENT, Silas Inman
ASSISTANT EDITOR Miranda Schmalfuhs, SENIOR VICE PRESIDENT, I.T. & ENTERPRISE SYSTEMS, John Moricone
mschmalfuhs@mmhgroup.com SUBSCRIPTIONS +1 (888) 527-7008 (toll-free within USA)
SENIOR VICE PRESIDENT, DEVELOPMENT & ENTERPRISE SYSTEMS, JP UVA
+1 (218) 740-6477 (outside USA), fulfill@hcl.com
ART DIRECTOR Dan Ward, SENIOR VICE PRESIDENT, AUDIENCE GENERATION &
Dward@hcl.com BACK OR CURRENT ISSUES +1 (800) 598-6008, PRODUCT FULFILLMENT, Joy Puzzo
WASHINGTON EDITOR Jill Wechsler +1 (218) 740-6480 (outside USA) VICE PRESIDENT, HUMAN RESOURCES & ADMINISTRATION,
+1 (301) 656-4634 fax: +1 (301) 718-4377 Shari Lundenberg
PRODUCTION OFFICES VICE PRESIDENT, BUSINESS INTELLIGENCE, Chris Hennessy
PRODUCTION MANAGER Karen Lenzen
SALES SERVICES 131 W. 1st Street, Duluth, MN 55802 USA VICE PRESIDENT, CORPORATE BRANDING & B2B MARKETING, Amy Erdman
GROUP PUBLISHER Todd Baker +1-248-823-7808 fax: +1 (408) 962-1125 EXECUTIVE CREATIVE DIRECTOR, CREATIVE SERVICES, Jeff Brown
+1 (732) 346-3002. fax: +1 (732) 647-1235,
APPLIED CLINICAL TRIALS (Print ISSN: 1064-8542, Digital ISSN: 2150-623X) is published 4 times/year in March, June, Sept & Dec by MJH Life SciencesTM, 325 W 1st
tbaker@mmhgroup.com Street, STE 300 Duluth, MN 55802. Subscription rates: $70 for 1 year (4 issues), $120 for 2 years (8 issues) in the United States and possessions; $90 for 1 year, $140 for 2
DIRECTOR OF ADVERTISING Wayne K. Blow years in Canada and Mexico; all other countries $130 for 1 year, $235 for 2 years. Single copies (prepaid only): $23 in the United States and possessions; $28 in all other
countries. Add $6.50 per order for shipping and handling. Periodicals postage paid at Duluth, MN 55806 and additional mailing offices. POSTMASTER: Please send
UK: +44 1244 629 304 fax: +44 1925 732 798, wblow@ address changes to APPLIED CLINICAL TRIALS, P.O. Box 6115, Duluth, MN 55806-6115. PUBLICATIONS MAIL AGREEMENT NO. 40612608, Return Undeliverable Canadian
mmhgroup.com Addresses to: IMEX Global Solutions, P. O. Box 25542, London, ON N6C 6B2, CANADA. Canadian G.S.T. number: R-124213133RT001. Printed in the U.S.A. Digital-only
editions will publish 6 times/year in Jan/Feb, April, May, July/Aug, Oct, and Nov.
NATIONAL SALES MANAGER Bill Campbell
©2019 MJH Life SciencesTM. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical
+1 (847) 283-0129 fax: +1 (847) 282-1456, including by photocopy, recording, or information storage and retrieval, without permission in writing from the publisher. Authorization to photocopy items for internal/
wcampbell@mmhgroup.com educational or personal use, or the internal/educational or personal use of specific clients is granted by MJH Life SciencesTM for libraries and other users registered with
the Copyright Clearance Center, 222 Rosewood Dr. Danvers, MA 01923, 978-750-8400 fax 978-646-8700 or visit http://www.copyright.com online. For uses beyond those
REGIONAL SALES DIRECTOR Vahé Akay listed above, please direct your written request to Permission Dept. email: ARockenstein@mmhgroup.com.
+1 (609) 819-5209 MJH Life SciencesTM provides certain customer contact data (such as customers’ names, addresses, phone numbers, and e-mail addresses) to third parties who wish
vakay@mmhgroup.com to promote relevant products, services, and other opportunities that may be of interest to you. If you do not want MJH Life SciencesTM to make your contact information
available to third parties for marketing purposes, simply call toll-free 866-529-2922 between the hours of 7:30 a.m. and 5 p.m. CST and a customer service representative
SALES SUPPORT COORDINATOR Kristi Stevenson will assist you in removing your name from MJH Life Sciences’TM lists. Outside the U.S., please phone 218-740-6477.
+1 (732) 346-3006 fax: +1 (732) 596-0012, Applied Clinical Trials does not verify any claims or other information appearing in any of the advertisements contained in the
kstevenson@mmhgroup.com publication, and cannot take responsibility for any losses or other damages incurred by readers in reliance of such content.
To subscribe, call toll-free 888-527-7008. Outside the U.S. call 218-740-6477.
ACT CHESTER UK OFFICE: +44 1244 393 100
September 2019 appliedclinicaltrialsonline.com APPLIED CLINICAL TRIALS 3
CONTENTS
APPLIED CLINICAL TRIALS
VOLUME 28, N UMBER 9
FEATURED
24 The Changing Landscape
JAKKAPAN - STOCK.ADOBE.COM
for Clinical Trial Sites
Cindy H. Dubin
Exploring how clinical research sites are redefining their business
models to be more flexible, collaborative, and customized.
30 Improving Information EXECUTIVE PROFILE EYE ON PATIENT ADVOCACY
Exchange in Clinical Trials 22 Creating Medicines 20 Retention Strategies for
Jason Methia ‘Appropriate for All’ Keeping Participants Engaged
Executives from across the clinical Christen Harm The MJFF Recruitment
research enterprise converge Bristol-Myers Squibb’s cardiovascular and Retention Team
to discuss the steps—and development leader Charlotte Findings and learnings from a
technology—needed to strengthen Jones-Burton on the importance case study of the Parkinson’s
industrywide data sharing. of diversifying clinical trials for Progression Markers Initiative.
better patient outcomes.
18 The VA Gets
Real on Reform COMMENTARY
NEWS AND ANALYSIS
Sony Salzman
6 WASHINGTON REPORT A CLOSING THOUGHT
After years of siloed focus—and
slow study start-ups—the U.S. 7 EU REPORT 34 Putting Sites First When
Veterans Affairs agency embarks 10 Q&A Implementing New Trial Technology
on implementing its multi-year
initiative to bolster clinical research.
16 CLINICAL TRIAL INSIGHTS KK Rumrill
EDITORIAL ADVISORY BOARD
Moe Alsumidaie Srini Dagalur, PhD Michael R. Hamrell, PhD, RAC VIcky Parikh, MD, MPH
Thought Leader and Expert in the Specialist Leader, Life Sciences President Executive Director
Application of Business Analytics Technology Strategy MORIAH Consultants Mid-Atlantic Medical Research Centers
Towards Clinical Trials and Healthcare Deloitte Huntington Beach, CA Hollywood, MD
New York, NY Parsippany, NJ
Wayne Kubick Prof Stephen Senn, PhD, FRSE
Kiran Avancha, PhD, RPh Yakov Datsenko, MD Chief Technology Officer Consultant Statistician
Chief Operating Officer Senior Clinical Research Physician Health Level Seven International Edinburgh, UK
HonorHealth Research Institute Team Leader Immunology/Respiratory Chicago, IL
HonorHealth Boehringer Ingelheim Pharma GmbH &
Scottsdale, AZ Co. KG
Darshan Kulkarni, PharmD, Esq
Principal Attorney
Biberach, Germany
Townsend N. Barnett, Jr. The Kulkarni Law Firm
Vice President, Global Head Edward Stewart Geary, MD Philadelphia, PA
of Pre-Clinical and Clinical QA Chief Medical Officer &
Vice President
Jeffrey Litwin, MD
UCB Pharma S.A.
CEO
Chemin du Foriest, Belgium Eisai Co., Ltd.
MedAvante-ProPhase
Tokyo, Japan
Kenny Blades, PhD Princeton, NJ
Director, Global Project Management Ashok K. Ghone, PhD
VP, Global Services Barrie Nelson
DOCS International
Chief Standards Officer
Kent, UK MakroCare
Nurocor
Newark, NJ
Anthony J. Costello Austin, TX The expertise of Editorial Advisory Board mem-
Vice President, Mobile Health Rahlyn Gossen bers is essential to the credibility and integrity of
Medidata Founder Applied Clinical Trials. These clinical trials experts
share with the editors the wisdom gained through
San Francisco, CA Rebar Interactive their experience in many areas of drug develop-
New Orleans, LA ment. EAB members review manuscripts, suggest
Domenico Criscuolo, MD, PhD, FFPM
topics for coverage, and advise the editors on
Chief Executive Officer Uwe Gudat, MD industry issues. All manuscripts must first be
Genovax Head of Safety, Biosimilars submitted to the Editor-in-Chief, Applied Clinical
Colleretto Giacosa, Italy Merck Serono Trials, 485 Route 1 South, Building F, Second Floor,
Geneva, Switzerland Iselin, NJ 08830 USA.
4 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com September 2019
make your research
altogether
better
IRB
Integrated Research Compliance Services
Solutions to Streamline Your Study
Advarra is your partner in advancing better research. With an extraordinary
breadth and depth of regulatory compliance and human subject protection
IBC
expertise, a client-centric service model, and innovative technology,
Services
Advarra provides convenient solutions performed with exceptional quality.
Expert Guidance | Uncompromising Integrity | Rapid Turnaround Consulting
Services
Trust Advarra’s integrated solutions and collaborative approach
to make your research altogether better.
Get started at
V
advarra.com
NEWS
WASHIN GTO N RE P OR T
SPONSORS, REGULATORS procedures, and processes, as outlined in ter,” he commented. An analysis of 334 OSI
CAUTIOUS ABOUT RISK-BASED guidance issued in 2013 and updated earlier clinical investigation summaries over three
OVERSIGHT OF CLINICAL TRIALS this year. Such situations can be described years reveals relatively few “active recom-
Despite the high cost and extensive re- in risk-based monitoring (RBM) strategies mendations” that raise questions about
sources involved in monitoring the con- laid out in RBM plans. application quality likely to delay approval.
duct of and data produced by clinical trials, Despite these efforts, biopharma com- The vast majority of clinical inspections find
the research community has been slow to panies have been slow to adopt RBM ap- appropriate compliance with requirements.
embrace strategies for reducing on-site proaches, as seen at a public workshop in Similar efforts by the European Medi-
oversight to reflect risk. Sponsors appear July organized by the Margolis Center for cines Agency (EMA) support risk-based
willing to spend more to ensure that results Health Policy at Duke University to gain approaches to clinical trial monitoring to
meet regulatory expectations and avoid more feedback from stakeholders on the ensure that studies generate reliable in-
raising issues that could delay the review challenges and barriers influencing the formation, while protecting study subjects,
and approval of a market application. FDA adoption of RBM. Jacqueline Corrigan- commented Camelia Mihaescu, of the EMA
and other regulators are responding with Curay, director of the Office of Medical Committees and Inspections Department.
support for more flexible monitoring of Policy in the Center for Drug Evaluation Risk-based approaches, she noted, should
clinical investigators and review of study and Research (CDER), opened the meeting reflect trial-specific issues.
records in order to limit study monitoring to by emphasizing the importance of lever- Yet, regional differences in monitoring
situations where less oversight raises clear aging tools and methods to improve the practices, inspection procedures, and ac-
difficulties for investigators, participants, efficiency and reliability of clinical trials. ceptance of RBM by regulatory agencies
and data integrity. FDA wants to make risk-based monitoring create barriers to wider adoption of RBM,
To this end, FDA has encouraged spon- “a reality for everyone,” she said, and is observed Tim Rolfe, director of research-
sors to focus on risk in monitoring clinical reviewing comments from the recent draft based monitoring at GlaxoSmithKline. Spon-
trials, similar to agency initiatives to modify guidance to move forward. sors have concerns about ensuring qual-
pharmaceutical plant inspections and pre- The process begins with risk assessment ity data at multiple study sites that follow
approval of product changes to situations to help shape the resulting clinical research a range of research methods, with large,
likely to compromise product quality and protocol, explained David Burrow, direc- complex trials raising issues that differ with
safety. Instead of using on-site monitoring tor of the Office of Scientific Investigations very small studies. He advised FDA to up-
for every clinical site to verify study data (OSI) in CDER’s Office of Compliance. An date its inspection guide for clinical sites
and conduct, FDA advises sponsors to limit RBM plan then can be built to support prod- and to train inspectors in RBM expectations
oversight to the most critical data elements, uct approval and reduce errors “that mat- through case examples. Research sites ex-
perience “general discomfort” with RBM
approaches, according to a study by the
F DA N OTES Society for Clinical Research Sites, and often
feel left out of planning for RBM approaches,
which vary notably with each sponsor.
The FDA recently released the following 7/30/19: Rare Pediatric Disease Priority Burrow of OSI was optimistic that recent
industry guidance documents: Review Vouchers changes in FDA’s Office of Regional Affairs
(ORA) to create specialized teams of clinical
8/13/19: Gastroparesis: Clinical Evalua- The following committee meetings were site inspectors may address some inspec-
tion of Drugs for Treatment scheduled for September: tion issues. But OSI still finds problems with
• Allergenic Products Advisory initial RBM efforts, particularly with record
8/7/19: Fabry Disease: Developing Drugs
Committee, Sept. 13. Discuss the sampling and source-data verification, and
for Treatment
safety and efficacy of Peanut Allergen limited coordination between sponsors
Powder, indicated to reduce the and CROs can be a problem. FDA officials
8/2/19: Testing and Labeling Medical
risk of anaphylaxis after accidental advise sponsors to involve all stakehold-
Devices for Safety in the Magnetic Reso-
exposure in patients aged 4 to 17 with a ers in the RBM process,
nance (MR) Environment
confirmed diagnosis of peanut allergy. which should be adapt-
7/31/19: E8 (R1) General Considerations able and promote hu-
• Patient Engagement Advisory man subject protection
for Clinical Studies
Committee, Sept. 10. Discussed and and data integrity.
7/31/19: General Clinical Pharmacology made recommendations on the topic
Considerations for Neonatal Studies for “Cybersecurity in Medical Devices:
Drugs and Biological Products Communication That Empowers Patients.” — Jill Wechsler
6 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com September 2019
NEWS
EU REP OR T
NO END IN SIGHT TO EUROPEAN fully manage the contacts its evaluators ing pre-submission activities needs be im-
DEBATES ABOUT DRUG FIRMS’ have with medicine developers during the proved to enhance the objectivity of how
INFLUENCE ON REGULATORS pre-submission phase,” and that “EMA medicines are evaluated,” remarked the
Persistent concerns that European drug should provide greater transparency on its Ombudsman’s decision.
evaluators are too cozy with pharmaceu- pre-submission activities, with the aim of The criticisms focused partly on the risk
tical companies are unlikely to be fully maintaining public trust in its work.” But of bias where the same individuals are in-
allayed by a recent decision from the some of those who have levelled strident volved in providing scientific advice and in
European Ombudsman that “no further and repeated attacks on the agency’s op- subsequently evaluating that same medi-
inquiries are justified” into the provision erations in the last five years will not be so cine. EMA should widen its pool of experts,
of early scientific advice. The two-year in- easily appeased. and where it was absolutely necessary to
quiry into possible maladministration at have such overlap, EMA should publicly
the European Medicines Agency (EMA) has Keeping things separate justify it. And there was also frequent criti-
intensified as much as it has resolved long- EU law specifically allows for medicine de- cism of the lack of transparency over the
running controversies over potential con- velopers to seek advice from EMA’s ex- procedures and calls for the scientific ad-
flicts of interest and lack of transparency perts long before they submit a marketing vice provided to be open to public scrutiny.
within the agency. authorization application. It is considered Health Action International (HAI) cited
It was two years ago that the Ombuds- legitimate for companies to seek advice on allegations purporting to come from EMA
man—an official European Union body— the relevant procedures, the requirements staff that “manufacturers see pre-sub-
decided to follow up on anxieties among for demonstrating that medicines are safe mission processes as a way to lobby the
many healthcare campaigners and aca- and effective, or the design or conduct of agency.” The European Public Health Al-
demics about the risk of what they saw as clinical trials. liance warns of “regulatory capture.” The
a hazardous overlap: the EMA’s roles both But questions have been posed for years International Society of Drug Bulletins says:
in giving early scientific advice to drug about whether EMA’s recommendations on “EMA’s confidential pre-submission “sci-
entific advice” to companies jeopardizes
its ability to make independent decisions.
Pre-submission activities effectively make
Questions have been posed for years EMA a co-developer of the medicine, yet
about whether EMA’s recommendations on it is subsequently called upon to issue its
opinion on whether or not the medicine
authorization of a medicine is influenced should be granted marketing authorization.”
by the prior interaction its evaluators Critic s make complaint s ab out the
negative impact of the confidentiality sur-
have with medicine developers. rounding the process. EPHA warns of the
dangers of giving scientific advice “be-
hind closed doors” and of how EMA “black
developers, and its subsequent engage- authorization of a medicine is influenced boxes” and “revolving doors” impede
ment in evaluating marketing authorization by the prior interaction its evaluators have transparency. ISDB says “companies that
applications from the very same products with medicine developers. The Ombudsman request pre-submission scientific advice
it had advised on. “These ‘pre-submis- could exert control from an early stage
chose to assess how far this may have hap-
sion activities’ may have some positive over ever ybody involved in the assess-
pened, or even be perceived to happen. And
consequences for public health,” said the ment of marketing authorization applica-
it concluded that not much needs to change.
formal inquiry, but it insisted that it was tions at both national and European level.”
also “important to avoid even the percep- Plenty of interest, plenty of ambition According to HAI, “It is impossible to know
tion that the eventual opinions of EMA on Among the numerous representations from the onset the advice a company has
medicines were influenced by these earlier made to the Ombudsman during the in- requested, and the EMA has subsequently
interactions.” quiry, national medicine evaluation authori- provided, even though this would be rel-
This summer, after extensive consulta- ties and the pharmaceutical industry felt evant information to patients who are con-
tions and discussions, the outcome was the system was broadly sound and pro- sidering enrolling in a clinical trial, and to
nothing more than “a number of sugges- tected the public adequately from risk of independent clinical trial reviewers.” By
tions for improvement”—and the decision overlap. But “by way of contrast, many providing “tailored and confidential advice
to, in effect, drop the case. The Ombuds- civil society organizations and academics to one company only,” EMA may even be
man merely urged that “EMA should care- argued that the current practice concern- in breach of competition law, it suggests.
September 2019 appliedclinicaltrialsonline.com APPLIED CLINICAL TRIALS 7
NEWS
EU REP OR T
HAI has made clear its concerns that trials, and maximize the value of the data words of welcome from EMA for some el-
“at the time of assessing an application for that clinical trials generate; and by avoid- ements of the decision cannot disguise
marketing authorization, (the relevant com- ing misunderstandings in the assessment the reality that it will continue to proceed
mittee) members might feel bound by the process, it can ease administrative burdens as before, despite its commitments to a
advice that the very same committee they and cut the risk of preventable delays at a few equally soft additional gestures toward
represent gave in the past to a company/ later stage. transparency.
marketing authorization applicant.” It says The agency maintained stoutly through- The more trenchant criticisms of the sys-
EMA should draw a firm line to prevent out that a scrupulous distinction is main- tem will, therefore, remain unsatisfied—
overlaps: “A clear separation of roles be- tained between the two levels of inter- and, hence, they will continue to feature
tween advisors and marketing authoriza- action, so as to give a guarantee of fair just as much as before in the public dis-
tion assessors should be established.” dealing and impartiality, Scientific advice course about EMA’s independence from
And the European Consumer Organi- is not a pre-evaluation of the data gath- industry influence.
zation (BEUC) says it wants to know how ered during clinical trials. It is prepared by The fact that the sharpest criticisms are
EMA’s pre-submission activities contrib- nominated experts who report to a specific made by only a relatively small number of
ute to the development of safe and ef- working party, and not by the committee contributors to the inquiry does not reduce
fective medicines. “A growing number of
medicines seem to come to the market for
which less robust data is available. How do
pre-submission activities contribute to the The fact that the sharpest criticisms are
availability of robust and useful data, while made by only a relatively small number
also minimizing the number of unneces-
sary clinical trials?,” the bureau asks.
of contributors to the inquiry does not
On the fence
reduce their significance. Both HAI and
The Ombudsman came down firmly in the EPHA are influential organizations.
middle of this divergence of views. Yes,
there is an element of risk in overlap, in
acknowledgement of the critics—but, over-
that conducts evaluations of marketing au- their significance. Both HAI and EPHA are
all, the system offers protection against
thorization applications. In the rare cases influential organizations—both of them are
undue influence, it concluded, in line with
where the same expert contributes to both represented on EMA’s own bodies—and
most comments from regulators and indus-
scientific advice and product evaluation, it they command a prominent position in
try. So there is not a lot that needs to be
is because of scarcity of experts in certain European public debates about health and
done. The toughest recommendation the
areas of science and medicine, and public medicines. They and the other organiza-
Ombudsman makes is that “to the great-
health could be impaired by a prohibition tions that share their views will ensure that
est extent possible, EMA should ensure
of this practice. If EMA identifies possible the debate will continue to grow over the
that there is a separation between those
conflicting interests among any of the ex- role of EMA and the influence of the drug
responsible for providing scientific advice
perts, it can exclude them from partici- industry on regulatory decision-making.
to a medicine developer and those subse-
pating in discussions on particular topics. And this at a particularly crucial moment
quently involved in evaluating” it.
And it is not binding, since it is based by for European rulemaking in general, with
The operational result is that EMA’s own
definition on the current state of the art, a new European Parliament and European
arguments—essentially that scientific ad-
and may consequently be superseded as Commission just about to take up the man-
vice is a force for good and should not be
understanding advances. agement of policy for the next five years.
tampered with lightly—largely prevailed in
the Ombudsman’s decision. No change, but no relief
The Ombudsman’s decision leaves the
EMA defense
situation unchanged. EMA will continue
EMA argued that the provision of scientific
to maintain that on balance, the system
advice can minimize the risks of exposing
is good and fair. Critics will continue to
patients to useless or less useful clinical
say the balance is wrong, and that partial-
trials, and maximize the value of the data
ity remains built into the system. And the
that clinical trials generate; and by avoid-
Ombudsman’s views, taking some from
ing misunderstandings in the assessment
column A and some from column B, and of-
process, it can ease administrative burdens
fering no more than a heavily-qualified sug-
and cut can minimize the risks of exposing
gestion of maximum caution, fully satisfies
patients to useless or less useful clinical — Peter O’Donnell
neither side. The flurry of soft diplomatic
8 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com September 2019

NEWS
Q& A
WORKFORCE READINESS tion across a diverse set of study sites and
TECHNOLOGY MINIMIZES asked if ArcheMedX could help.
RISK IN CLINICAL TRIALS We ultimately enabled them to design
Clinical trials often encounter operational and deliver an innovative site readiness
challenges and sponsors and CROs seek program powered by the ArcheMedX plat-
effective site-readiness practices. In this form that accelerated site initiation for a
interview, Joel B. Selzer, co-founder and CEO, neurology focused trial. That effort opened
ArcheMedX, Inc., discusses the impact that our eyes to the operational challenges thou-
healthcare technology has on clinical trials, sands of trials encounter and led us to ex-
focusing on the development of the com- plore the industry further. In the course of
pany’s workforce readiness platform. our market research, we conducted infor-
mational interviews with dozens of spon- Joel Selzer
Q: Can you tell us a bit about yourself? sors, CROs, and other trial stakeholders and
Joel Selzer: I have spent the past 15 years the critical need to more effectively evalu-
envisioning and delivering innovative technol- ate and improve the preparedness of staff
ogy and data-driven solutions across the life therapeutics and advanced protocol simula-
and sites became increasingly clear.
sciences and healthcare industries as an en- tions to data-driven workforce improvement,
The result was the development and
trepreneur, board member, and advisor. Dur- the industry can more rapidly and accu-
launch of Ready.
ing this time, I have co-founded and led three rately analyze novel sources of data that will
technology companies, Medical Funding Ser- inform better decision-making, decrease
Q: We are seeing more technologies the costs of clinical trials, and provide the
vices, Ozmosis, and currently ArcheMedX. coming from healthcare into clinical
In each venture, we have applied creative trials, which is but one part of the right therapies to the right patients.
approaches to improve the lives of our cus- overall healthcare picture. Why do
you think that is? What impact will Q: Investigative site burden is
tomers, thousands of clinicians, and most quite often a topic of concern
that continue to have in clinical trials?
importantly millions of patients. in this industry. Does the
JS: There are a number of macro trends driv- implementation of Ready increase
Q: Can you give us a brief ing the adoption of technology within clinical a site’s burden of tasks?
overview of your product? trials. For example, rising trial costs, increas- JS: Many sites today are already struggling
JS: Ready is an operational intelligence ing complexity, the continued low success to implement a dozen or more trial appli-
and workforce readiness platform that re- rates of getting to market, and the extreme cations, ever-changing study tools, and in-
duces the risks and costs associated with challenges of recruiting and retaining par- creasingly complex protocols. Adding to this
underperforming clinical trials. The plat- ticipants are all multiplied by the continued burden, they are rushed through training on
form enables clinical operations leaders to
evaluate and improve the preparedness of
project teams and site personnel by ana-
lyzing the behavior of each participant as Sponsors and CROs are now using advanced
they engage in personalized learning ex- data analytics and deep learning to more
periences that are designed and delivered
within the platform. Ready serves as an
effectively design and implement clinical trials
early warning detection system to identify that result in more personalized and consumable
risks sooner, ensure resources are more ef-
therapies that benefit patients and providers.
fectively deployed, and enhance staff and
site performance.
Q: This product came out of a growth of active clinical studies. This creates each system and protocol and often lack the
healthcare and continuing medical
education history. What made you a great deal of opportunity for technology- time and interest to properly focus on critical
choose clinical trials for this service? based solutions to make a positive impact. information. By centralizing and personaliz-
J S: We sp en t t h e f ir s t si x ye ar s a t In particular, clinical trials are accelerating ing each training experience, Ready makes it
ArcheMedX powering hundreds of online the adoption of digital tools and data-driven easier and more enjoyable for site personnel
medical education activities for national strategies. Sponsors and CROs are now to engage in critical content over time, in-
medical societies, leading academic medical using advanced data analytics and deep creasing their confidence and interest in the
and research centers, global medical educa- learning to more effectively design and im- study or tool. Ready can also be integrated
tion providers, and major pharmaceutical plement clinical trials that result in more via web services with nearly any IT system
firms. One of our academic research part- personalized and consumable therapies that making it simple to create a seamless user
ners ran into challenges standardizing initia- benefit patients and providers. From digital experience and securely share data.
10 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com September 2019"_b[bm]r-uঞ1br-ঞom
bm1Ѵbmb1-Ѵ|ub-Ѵv=uol
|_;1Ѵbmb1-m7bm|o
|_;r-ঞ;m|Ľv_ol; Recognized as the industry leader,
"1b;m1;ƒƕĽvmub-Ѵ;7;r;uঞv;Ō
along with our comprehensive
rѴ-oul-m71om1b;u];ŊѴ;;Ѵ
v;ub1;vŌ;mvu;|_-| ;1-ml;;|
you at any point along the virtual
clinical trial journey.
TELEMEDICINE
PHYSICIAN VISITS
STUDY SUPPLIES
HIGHLY SKILLED SHIPPED DIRECTLY TO
COORDINATORS THE PATIENT’S HOME
COORDINATED
AT-HOME
CLINIC VISITS WHEN
NURSE VISITS
NECESSARY
Reimagine clinical research with us.
www.science37.comNEWS
Q& A
Q: How would you envision Ready the protocol or other content they may have ered by Ready are often delivered during
changing the way sponsors plan skipped or struggled with and will continually study start-up, the insights the platform
their investigator meetings and
measure their engagement and response. provides into the readiness and mindset of
subsequent site training?
Ready can also power a virtual SIV and any participants serve as an early warning de-
JS: Ready creates opportunities for spon-
subsequent site training, such as protocol tection system that compliments traditional
sors to augment, re-focus, or even replace
amendments and the sharing of recruitment risk-based data and strategies. This unique
their investigator meetings, and subsequent
best practices. In each of these use cases, analysis of behavioral data drives risk mitiga-
site training. By deploying Ready prior to an
Ready will analyze the unique behavioral data tion, as well as more effective allocation and
deployment of resources that leads to better
staff and site performance.
This unique analysis of behavioral data drives
Q: There is also a lot of positive
risk mitigation, as well as more effective change in the industry to raise the
allocation and deployment of resources that level of education and professional
credentials at the site level. How
leads to better staff and site performance. does Ready help sites raise their bar?
JS: More than 40,000 clinicians have already
improved their knowledge, competence,
investigator meeting, the insights it gener- and confidence with ArcheMedX and this
it captures to provide insights that help spon- positive change continues to raise the bar at
ates can help to focus the meeting on the
sors focus where additional training, site visits, sites across the globe. By deploying Ready,
areas of greatest need and risk. This can re-
and/or remote monitoring may be required. sponsors and CROs can now accelerate this
sult in a more engaging and targeted meet-
ing that accelerates site initiation, better change by more effectively measuring and
Q: Does Ready impact other
enrollment, and overall compliance. oversight practices such as risk- improving the competence, readiness, and
Ready can be utilized in place of an inves- based monitoring (RBM)? mindset of their staff and sites. Ready can
tigator meeting to significantly reduce meet- JS: Yes. The operational intelligence and enable the industry to identify skill and knowl-
ing costs and provide more measurable data workforce readiness data generated by edge gaps across roles, years of tenure, certi-
and insights that identify which PIs (principal Ready creates early insight around areas fication levels, and therapeutic areas and then
investigators) are most likely to struggle. The of clinical operation risk and are key pieces target workforce improvement efforts on the
platform can then automatically re-engage of information for any RBM strategy. Since segments of staff and sites that need it most.
any participant to focus on critical aspects of the personalized learning experiences pow- — Staff Report
ACT O NLINE
GO TO: eLEARNING: the print! The Digital Edition Archive (link
While risk management efforts in drug devel- below) features a quick list of the contents
appliedclinicaltrialsonline.com
to read these exclusive stories opment have focused mostly on post-mar- for each issue.
keting drug safety, the clinical trials process http://bit.ly/2k0Amzl
and other featured content.
has its own mix of potential risks waiting to
TOP 3 SOCIAL MEDIA derail a company’s multimillion-dollar devel- Medical monitors play an integral role in
opment programs. This webcast focuses on ensuring patient safety, as trials increase in
1. Big CROs Dive into Offering complexity and as the volume of participant
why risk management and assessment are
AI/ML Solutions medical data grows. Medical Monitor Mod-
most effective when integrated into clini-
http://bit.ly/2lUX4cB
cal trials from the beginning (study start-up ernist: Driving Productivity Protecting Sub-
phase), rather than as an afterthought. jects is our latest e-book that shows how
2. Five Strategies for Conducting
Successful Pediatric Trials http://bit.ly/2kghywc the medical monitor role is evolving. It also
http://bit.ly/2kgbmEq explores how new, intuitive data visualization
As Applied Clinical Trials continues its move and analysis software technology is helping
3. How AI is Transforming Clinical to a more enhanced digital experience, be medical monitors identify outliers and trends
Trials: A Look Into the Code sure to visit our online digital edition of the in clinical trial data.
http://bit.ly/2lwv7b3 magazine, with the same look and feel as http://bit.ly/2kqOMZG
12 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com September 2019With Five Decades of Clinical Research
Experience – We Are the “Gold Standard”
in Ethical Review
For more than years
we have overseen more research
than all other IRBs combined.
Every day, WCG supports:
More than 10,000 protocols
Nearly 24,000 investigators
More than 112,000 sites
Consider - WCG participates in over 90%
of all FDA New Drug Approvals.
Learn more about working with the gold standard in IRB review:
www.wcgclinical.com/services/irb/
wcgclinical.comNEWS
DATA SH A RIN G
MIXED PATIENT SUPPORT OF risks that their information may otherwise many institutions do not have a culture
DATA-SHARING INITIATIVES be shared with third parties without their that promotes new data-sharing initia-
Do patients really want to share their data? consent, and be used in a context different tives. And researchers remain subject not
The question goes to the heart of the digi- from the one in which they disclosed it. only to geographic, institutional, or disci-
tal health revolution that strategists love It includes recommendations to policy- plinary boundaries, but often governed by
to celebrate—and the strategists will be makers, researchers, funders, and patient “silo mentalities” that see sharing data as a
heartened by the results of a new poll by Eu- organizations creating data-sharing initia- risk to personal and professional benefits
rope’s leading rare disease organization, Eu- tives, centered on issues of trust. Gover- conferred by data ownership. Increasingly
rordis. The vast majority of the 2,000+ rare nance should be in the hands of people prominent attacks on—and sensitivity to—
disease patients responding to an interna- whom patients consider impartial—such data security compound the difficulties. One
tional survey are supportive of data-sharing as general practitioners—and serious at- of the key recommendations, accordingly,
initiatives to foster research and improve tention should be given to keeping patients is that policymakers should pursue cultural,
healthcare, and willing to share their data informed about progress and outcomes of technological, and infrastructural changes to
to help research and treatment on diseases research for which their data has been used. make a reality of international data sharing.
other than their own. The full report is published in the Or- Eurordis and its numerous fellow advo-
But this is no carte blanche. Nearly half phanet Journal of Rare Diseases and makes cates of data sharing had better factor the
the respondents are against their data being challenging reading. It identifies the “numer- results of this survey into their planning.
shared outside the medical field, and even ous technical and regulatory boundaries Because for all the potential of digital health,
within the medical field, nearly all of them that make sharing difficult and for many without access to the data, not much is ever
want something close to full control over researchers, clinicians and institutions, still going to change.
the data they share, both over who gets it, not standard practice.” Aside from tech-
and what it is to be used for. They see big nical issues, Eurordis also points out that —Peter O’Donnell
NE WS NOTES
NEW COLLABORATION TARGETS sphere leading us down a path to the clinic, shareholders receive an upfront payment
PANCREATIC CANCER and commercial development of a lead can- of $52.5 million and have the potential to
Genisphere LLC and University Hospitals didate for the treatment of pancreatic cancer.” receive additional payments of up to $260
Cleveland Medical Center are partnering to Harbour BioMed and PPD team up million upon the achievement of certain clini-
study and develop unique strategies to treat Harbour BioMed (HBM), a global clinical- cal, regulatory, and commercial milestones.
pancreatic cancer. According to their agree- stage biopharmaceutical company, and the Cavion, a clinical-stage biotech and now
ment, investigators will optimize 3DNA®- CRO PPD have entered into a strategic col- a wholly-owned subsidiary of Jazz, creates
based therapeutics designed to target and laboration to develop HBM’s therapeutics therapies aimed at modulating the T-type
kill pancreatic tumors. Projects will include in the fields of oncology and immunology. calcium channel for the treatment of chronic
delivering a variety of therapeutic cargos, The selection of PPD as a preferred CRO and rare neurological diseases.
including small molecules and siRNA, formu- partner enables HBM, which has operations Pact focused on mRNA-based drugs
lated with pancreatic tumor-targeting mol- in the U.S., the European Union, and China, Biopharma company CureVac AG has struck
ecules on Genisphere’s 3DNA® nanocarrier. to conduct global clinical studies on its in- a collaborative research agreement with Yale
Jordan Winter, MD, chief of the Division research pipeline. HBM’s portfolio includes University for discovery research into mRNA-
of Surgical Oncology at University Hospitals five clinical-stage, in-licensed compounds based pulmonary therapeutic candidates.
Cleveland Medical Center and director of sur- and drugs generated by its internal discov- Under terms of the deal, the Yale University
gical services at UH Seidman Cancer Center, ery efforts, as well as co-discovery/develop- team will perform discovery research on tar-
is the lead researcher on the project. “My lab ment collaborations with academic institu- gets related to pulmonary diseases and pres-
studies the harsh, nutrient-deprived micro- tions and biopharmaceutical companies. ent therapeutic candidates to CureVac for
environment of pancreatic cancer to exploit Jazz Pharmaceuticals acquires Cavion preclinical and subsequent clinical develop-
metabolic vulnerabilities,” he said. “By spe- Jazz Pharmaceuticals Inc. announced the ment. CureVac will provide all funding for the
cifically targeting these hypoxic pathways in acquisition of Cavion Inc. last month through discovery research and retains the option to
a multifaceted approach, we can shut down a merger with a Jazz subsidiary. Under the acquire any rights regarding the candidates.
tumor progression. I see our work with Geni- terms of the agreement, the former Cavion — Wire reports
14 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com September 2019NEWS
CLINICA L TRIA L INSIG HTS
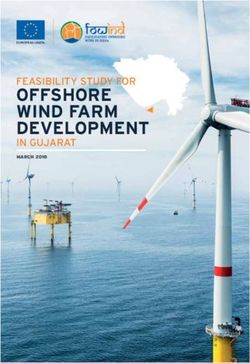
PROLIFERATION OF RARE (MEANS PER NO. OF NO. OF PATIENTS
DISEASE R&D NECESSITATING CLINICAL TRIAL) SITES PATIENTS PER SITE
NOVEL STRATEGIES
Phase I Rare Diseases 6 31 5
Interest in benchmark data on the Phase I Non-Rare Diseases 1 20 20
scope, performance, and economics
of these efforts has grown Phase II Rare Diseases 14 107 8
Phase II Non-Rare Diseases 27 268 10
Ken Getz
Phase III Rare Diseases 42 524 13
Phase III Non-Rare Diseases 65 3,434 62
Nearly every week, the Tufts Center for the
Source: Tufts CSDD
Study of Drug Development (Tufts CSDD)
receives a request for benchmark data Table 1. Comparing the average enrollment for rare and non-rare
on rare disease drug development perfor- disease clinical trials during the 2014 to 2018 time period.
mance and economics. These benchmarks
have been hard to come by, as a large per- Recent Tufts CSDD research suggests that Clinical trial challenges
centage of companies active in this space rare disease drug development presents and their Impact
are privately held. Sponsor companies and scientific and operational challenges that Sponsor-company investment in R&D for
contract research organizations (CROs) will necessitate — and perhaps acceler- rare diseases has seen substantial growth
have been looking for this benchmark data ate—the adoption of novel and less tradi- in global, FDA-regulated Phase I-III clinical
to guide portfolio and development project tional clinical development strategies, op- trial activity. In total, between 2014 and
planning and optimization. Tufts CSDD has erating practices, and solutions. Consider 2018, there have been more than 4,000
compiled some useful benchmarks. a few key findings: FDA-regulated clinical trials initiated world-
At the present time, rare disease drug wide for rare disease treatments. In 2018
• The average direct cost to conduct
development is one of the most active and alone, there were 372 new Phase I clinical
a Phase III pivotal trial of an
fastest growing areas in drug R&D. Rare trial starts; 422 new Phase II clinical trial
investigational rare disease treatment
diseases are defined as medical conditions starts; and 148 new Phase III clinical trial
is approximately half that of
that affect 200,000 or fewer people in the starts.
investigational treatments for non-rare
U.S. or fewer than five people per 10,000 The vast majority (84%) of active stud-
diseases ($103 million vs. $193 million).
population in the European Union. In 2018, ies on rare diseases are currently in early-
approximately one-third (31%) of all prod- • Although clinical trials for rare disease stage clinical development. But sustained
ucts in the global R&D pipeline targeted drugs recruit fewer patients, clinical long-term pharmaceutical company in-
treatments for rare disease indications. phase through approval durations vestment in rare diseases is driving up the
This is up from 15% only 10 years ago. And for rare disease drug development volume of later-stage clinical trial activ-
nearly six-out-of-10 (58%) drug and biologic take, on average, four years longer ity. New clinical trials initiated for Phase II
approvals in 2018 were for rare diseases; than those for non-rare diseases and III clinical trials are increasing at three
up from 26% in 2008. due to site and patient recruitment times the rate as those for Phase I trials
Biopharmaceutic al companies have and retention challenges. (12% vs. 4%).
substantially increased R&D investment Pharmaceutical companies and CROs
in rare diseases, not only to meet unmet What follows are benchmarks that Tufts have noted the unprecedented challenges
medical needs, but also to support devel- CSDD —and others— have been compil- they face in finding clinical research pro-
opment programs at lower relative cost, ing. We analyzed data on 4,562 clinical fessionals with expertise and experience
with fewer competitors, strong demand trials for all rare disease medicines in ac- in specific rare diseases and in identifying
from patient advocates, and greater op- tive FDA-regulated clinical trials worldwide and enrolling patients who are managing
portunities for favorable pricing. This latter between 2014 and 2018. This data was and living with specific rare diseases. To
expectation in particular appears aspira- gathered from the www.clinicaltrials.gov address these challenges, sponsors and
tional given current public perceptions and website. Data on the economics of rare CROs have typically engaged a much larger
the political climate. disease drug development comes from relative number of clinical investigators in
As more data is gathered characterizing EvaluatePharma. The author thanks Beth early-stage clinical trials to each enroll a
the scope, performance, and economics Harper (Clinical Performance Par tners) smaller number of patients. To put this into
of rare disease drug development, the op- for her input and assistance on analyzing perspective and characterize the magnitude
portunity for pharmaceutical and biotech- rare disease clinical trial recruitment and of this challenge during the 2014 – 2018
nology companies appears more nuanced. retention rates. timeframe (see table above):
16 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com September 2019NEWS
CLINICA L TRIA L INSIG HTS
• For Phase I clinical trials of rare diseases, class observed during the 2014-2018 pe- Analysts and observers anticipate that
sponsors and CROs engaged, on average, riod: for example, they were 41% longer for sponsor company reliance on data and
six times the number of investigative all cancer-related diseases; 79% longer for sophisticated analy tics to identif y rare
sites to recruit one quarter of the all endocrine diseases; and 64% longer for disease-focused investigators and eligi-
number of patients per study, compared CNS diseases. ble patients will intensify. The adoption
with those for non-rare diseases. Given unmet medical need, regulatory of patient-centric approaches is also ex-
review durations are four months faster, pected to accelerate. Sponsors and CROs
• For Phase II and III clinical trials of rare
on average, for rare disease drug applica- will increasingly look to virtual (direct-to-
diseases, sponsors and CROs engaged
tions, compared to review time for non- patient) and hybrid (investigative site with
half to 60% of the average total number
of investigative sites, respectively, to
enroll as few as 15% of the total average
number of study volunteers per trial. Analysts and observers anticipate that sponsor
The challenges associated with rare dis-
company reliance on data and sophisticated
ease patient recruitment and retention analytics to identify rare disease-focused
are even clearer in the substantially higher
observed screen and randomization failure
investigators and eligible patients will intensify.
rates relative to those rates for non-rare
diseases. Eight-out-of-10 (81%) patients
screened for clinical trials for rare diseases
rare diseases across all therapeutic areas. intermittent direct-to-patient) models and
are not eligible to enroll, compared to 57%
Submission to approval decisions for rare convenience-enhancing approaches (e.g.,
screen failure rates for non-rare diseases
disease drug applications are 47% faster in home nursing, telemedicine, wearable and
(all therapeutic areas). More than half (56%)
CNS diseases; 30% faster in endocrine dis- mobile devices, and patient assistance
of rare disease study volunteers fail to be
eases; and 10% in cancer-related illnesses. programs) to bring clinical trials to wher-
randomized, compared to 36% randomiza-
ever it is easiest and the most efficient for
tion failure rates for non-rare diseases. Responding to a new
study volunteers to participate. Observers
But once rare disease patients have risk-return profile
and analysts also expect sponsor and CRO
enrolled in a clinical trial, they’re far less The high proportion of rare diseases in
demand for clinical trials embedded within
likely to drop out. The premature termina- R&D and the growing number achieving
clinical care settings to increase, as will
tion rate —associated with all causes— commercialization will necessitate the
demand for real-world data and evidence
of rare disease patients randomized for adoption of new clinical development
to supplement, and even replace, tradi-
clinical trials is 14%, compared to 21% for models to accelerate timelines and drive
tional clinical research data.
those in non-rare disease clinical trials. greater efficiency. Very small relative mar-
And at Tufts CSDD, we can expect a
kets and long relative development dura-
growing number of inquiries into base-
Drug development and tions challenge the traditional risk-return
line and benchmark data on the impact
approval durations profile for new drug therapies.
of these approaches on rare disease drug
Major difficulties finding and engaging in- Worldwide, in 2018 an estimated 3,500
development performance and economics.
vestigative sites and identifying and enroll- small and large molecules targeting rare
ing study volunteers in rare disease clinical diseases were active in R&D. This is more
trials adds considerable time and delays than double the level observed 10 years
recouping development investment. Over- ago. And during the past 25 years, there
all development durations (i.e., IND filing has been a six-fold increase in the num-
to regulatory decision) for rare disease ap- ber of orphan designations granted by the
plications are four years longer than for all FDA—growing from 301 designations in
other disease segments. the four-year timeframe between 1994 to
Between 2014 and 2018, clinical dura- 1998 to 1,800 designations in the 2014 to — Ken Getz, MBA, is the
tions—overall Phase I-III cycle time—for 2018 period. As the volume of designations Director of Sponsored
rare disease investigational drugs took 131 has increased, so too has the absolute Research at the Tufts
months, on average. This was 68% lon- number of approvals: The total number of CSDD and Chairman
ger than the average 78 months for all orphan drug approvals increased from 84 of CISCRP, both based
non-rare diseases. Rare disease clinical in the 1994 to 1998 timeframe to 316 in the in Boston, MA. email:
durations are longer in every therapeutic 2014 to 2018 period. kenneth.getz@tufts.edu
September 2019 appliedclinicaltrialsonline.com APPLIED CLINICAL TRIALS 17You can also read