The Broken Hearts Club - Medications to Manage Heart Failure in Hospice - Hospice Pharmacy Solutions
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
3/18/2021
The
Broken Hearts Club
Medications to Manage Heart
Failure in Hospice
Pathways to Success
March 18, 2021
Hennie Garza, M.S.Pharm, R.Ph. Vice President Clinical Operations
Hospice Pharmacy Solutions
hgarza@hospicepharmacysolutions.com
1
Disclosures 2
Hennie Garza has no financial conflicts to disclose
2
1
3/18/2021
Objectives / Agenda 3
Objectives Agenda
1. Describe the pathophysiology of • Background
heart failure and resulting • Heart failure definitions
symptoms • Pathophysiology
2. Describe the New York Heart • Introduction to guidelines
Association (NYHA) Classification of • Medications and some
heart failure with corresponding mechanisms
symptoms, function and treatments • Case studies
3. List medications used to treat heart
failure including non-traditional
medications with new indications
for heart failure
3
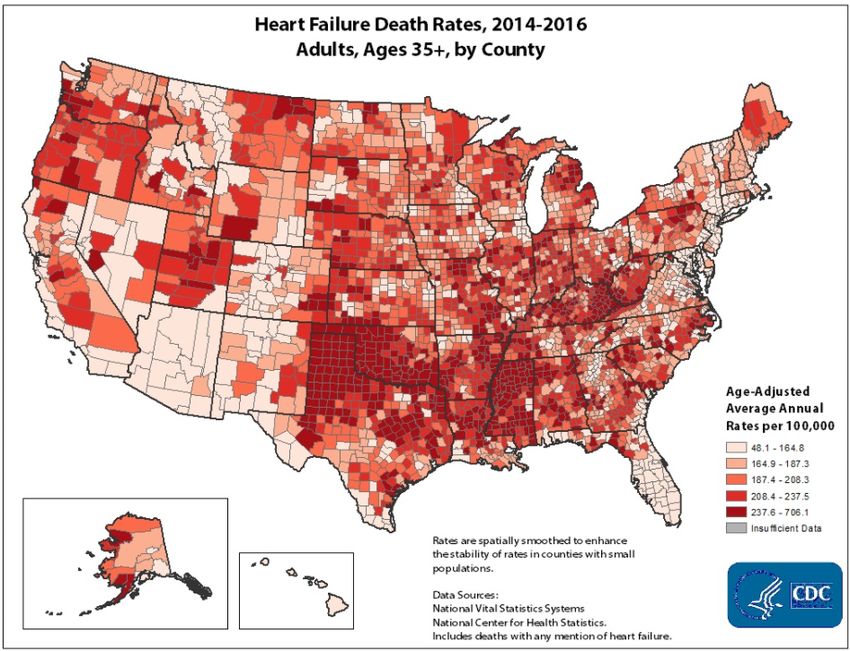
• About 6.2 million adults in the U.S. have heart failure
• In 2018, heart failure was mentioned on 379,800 death
certificates (13.4%)
• Heart failure cost the nation an estimated $30.7 billion
in 2012. This includes cost of health care services,
medications to treat HF and missed days of work.
https://www.cdc.gov/heartdisease/heart_failure.htm
https://www.ahrq.gov/sites/default/files/wysiwyg/data/infographics/heartfailure.pdf
4
4
2
3/18/2021
• 5-year
survival
rate is
approx.
50%
https://www.cdc.gov/heartdisease/heart_failure.htm 5
5
Some Heart Failure Vocabulary 6
• HFrEF = Heart Failure with Reduced Ejection Fraction
• Systolic Heart Failure
• Primary cause is coronary artery disease (CAD)
• Weakened cardiac muscle cannot “squeeze” well
• Less blood pumped out of ventricles
• Ejection Fraction (EF) < 40%
• HFpEF = Heart Failure with Preserved Ejection Fraction
• Diastolic Heart Failure
• Primary cause is hypertension
• Walls of ventricle are thick and rigid
• Less blood fills the ventricle
• Ejection Fraction (EF) > 50%
Snyder s. EMS World Magazine. 2015.
Yancy CW, et al. J Am Coll Cardiol. 2013;62(16):e147‐239
6
3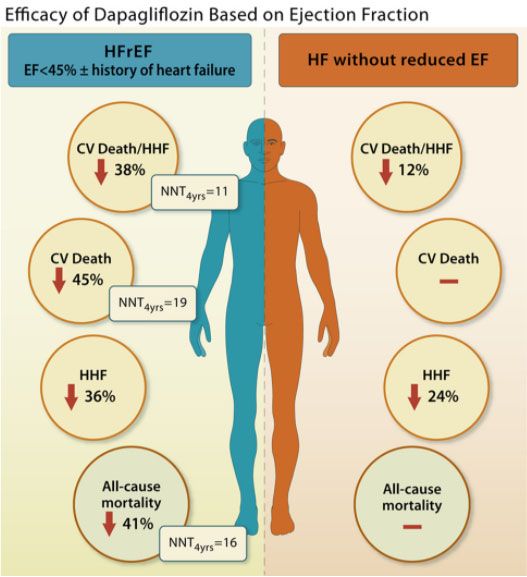
3/18/2021
Some Pathophysiology – Heart Failure 7
• Heart failure is characterized by
changes in the renin-
angiotensin-aldosterone,
sympathetic, and other
hormonal systems, resulting in
a catabolic state.
• Pro-inflammatory cytokines are
activated in HF, leading to
insulin resistance, cachexia,
anorexia and contributing to the
catabolic state.
• These hormonal and cytokine
alterations result in respiratory
and skeletal muscle atrophy
and weakness, which contribute
to symptoms of fatigue,
dyspnea and limited exercise
capacity.
Sarah Goodlin, Palliative Care in Congestive Heart Failure JACC vol. 54 no.5, 2009 doi:10.1016/j.jacc.2009.02.078 7
7
Self Assessment Question 1 8
Which of the following symptoms result from the catabolic state
of heart failure?
a. Rash, Weight Gain, Constipation and Alopecia
b. Dyspnea, Anxiety, Fatigue and Anorexia
c. Itching, Agitation, Urinary Tract Infection and Increased
appetite
Correct answer: b
8
4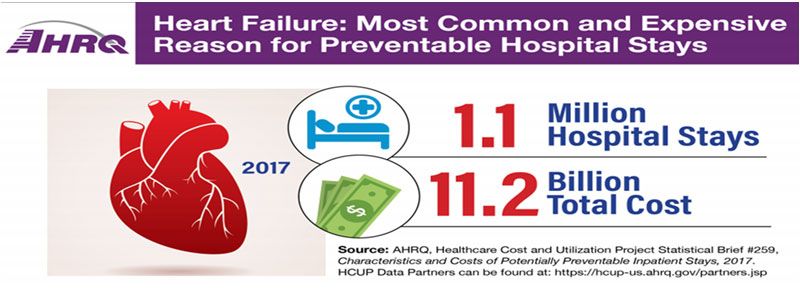
3/18/2021
Self Assessment Question 2 9
True or False:
The primary cause of HFreF (aka Systolic Heart Failure) is
coronary artery disease.
Answer: True
9
Introduction to Guidelines 10
• Have you ever wondered why Heart Failure patients come to hospice on
so many medications?
• Medications added / changed as HF progresses according to guidelines
Sarah Goodlin, Palliative Care in Congestive Heart Failure JACC vol. 54 no.5, 2009 doi:10.1016/j.jacc.2009.02.078
10
10
5
3/18/2021
NYHA Symptoms Class ACC-AHA Stage Stage Function and Treatment
Class (adapted from The Cleveland Clinic)
I Asymptomatic A No objective A Treat underlying conditions (smoking, HTN, DM, HLP)
Activity does not evidence of CVD, no ACE/ARB for CAD, HTN, Vascular conditions, Beta
cause symptoms symptoms, no Blocker if HTN
No limitation of limitation in ordinary
physical activity. activity
II Symptoms with B Evidence of minimal B No symptoms – ECHO – EF < 40%
moderate exertion - CVD. Mild Treat as in A – ACE/ARB BB if Hx MI + EF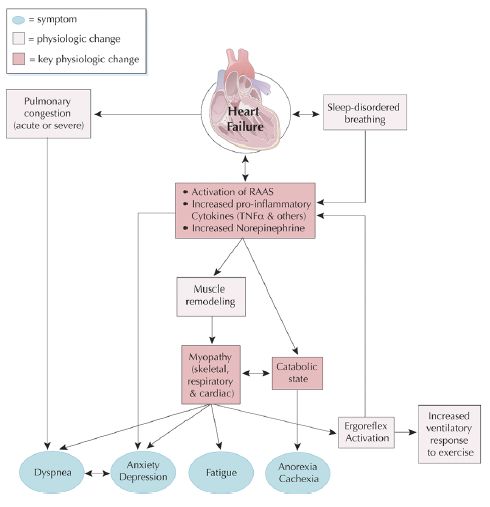
3/18/2021
Quick Mechanism of Action Review – “MOAs Matter”
• Ivabradine (Corlanor™)
– inhibits the cardiac pacemaker If current in the sinoatrial node resulting in a dose-dependent
reduction in heart rate
• Sacubitril (Entresto™ - Sacubitril + Valsartan)
– Sacubitril inhibits neprilysin. Neprilysin degrades endogenous vasoactive peptides including
natriuretic peptide. Inhibition of neprilysin results in increased concentrations of the
vasoactive peptides and results in vasodilation, natriuresis and diuresis
– Should not be used in patients with history of angioedema
• Spironolactone (Aldactone™)
– Inhibits effects of aldosterone on the distal tubules in the kidney. Unlike amilioride and
triamterene, spironolactone exhibits diuretic effect ONLY in the presence of aldosterone.
Antagonism of aldosterone enhances sodium, chloride, and water excretion and reduces the
excretion of potassium, ammonium and phosphate.
– Blocks androgen receptors by competitively inhibiting dihydrotestosterone at its receptor sites
– Aldosterone is the main mineralocorticoid steroid hormone produced by adrenal cortex
essential for sodium conservation in the kidney, salivary glands, sweat glands and colon.
13
13
Guideline focus on pharmacology updates
14
14
7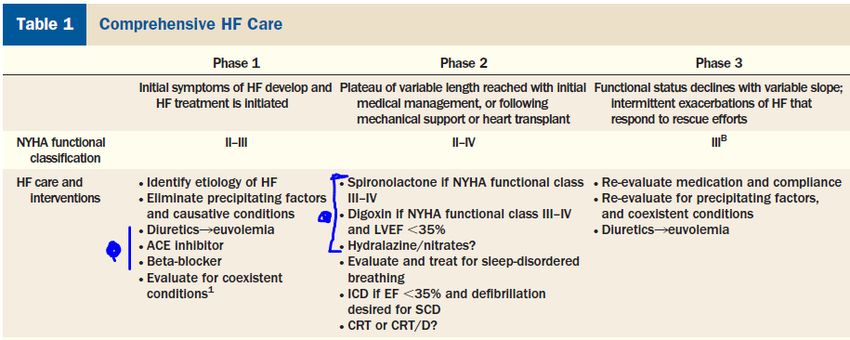
3/18/2021
GDEM = Guideline Directed Evaluation and Management
JACC Vol 68, No.13, 2016: 2016 ACC/AHA/HFSA Focused update on New Pharmacological Therapy for Heart Failure 15
15
Self Assessment Question 3 16
You are admitting a new patient to your hospice service. You
notice the patient has a diagnosis of NYHA class III heart failure.
Do you expect the patient to have symptoms of heart failure at
rest without any exertion?
YES or NO
Correct answer: No
16
8
3/18/2021
Self Assessment Question 4 17
Your patient with heart failure is on the medication Lisinopril, an
ACE inhibitor. The patient’s primary Cardiologist orders
Sacubitril/Valsartan, an ARNI, and wants the patient to start
taking the following day.
Can you add Sacubitril/Valsartan to this patient tomorrow?
YES or NO
Correct answer: No
17
Medications That Can Cause or Make HF worse 18
Mechanism Medication(s)
Negative ionotropic effects (reduced • Antiarrhythmics (except amiodarone & dofetilide)
strength of heart muscle • Beta-blockers (benefits with certain agents)
contraction) • Calcium channel blockers (diltiazem, verapamil)
• Itraconazole (unknown mechanism)
Cardiotoxin • Alcohol, excessive amounts in some patients
• Chemotherapy agents (paclitaxel, cyclophosphamide and others)
Sodium and water retention • Hormones, androgens / estrogens
• NSAIDs including COX-2 inhibitors (celecoxib, ibuprofen etc.)
• Glucocorticoids (prednisone, dexamethasone)
• Salicylates – in high doses
• Thiazolidinediones (rosiglitazone, pioglitazone)
Osmotic agents • Albumin and blood products
Miscellaneous • Sympathomimetics (amphetamine, cocaine, pseudoephedrine)
• TNF antagonists (etanercept, infliximab)
Cardiovascular Pharmacotherapy, Chapter 8, Table 8‐3
18
93/18/2021
Medications with new indications for Heart Failure
• Sodium-Glucose co-transporter 2 (SGLT2)
inhibitors: Dapagliflozin, Empagliflozin
– Block reabsorption of glucose by the kidney
resulting in increased glucose excretion
– FDA indication: Reduce cardiovascular mortality
due to major cardiovascular events (MACE)
– FDA indication: Reduce hospitalizations due to
heart failure in patients with Type 2 Diabetes
Mellitus (T2DM) with established cardiovascular
disease
• Studies in heart failure: HHF =
Hospitalizations
– 2015 EMPAG-REG OUTCOME due to HF
– 2019 DECLARE-TIMI 58
– 2019 DAPA-HF
– 2020 EMPEROR-reduced Trial
– 4 years needed to see benefit/outcome
Circulation Vol.139 Issue 22, May 2019 The Serendipitious Story of SGLT2 Inhibitors in Heart Failure;
NEJM More Evidence for SGLT2 Inhibitors in Heart Failure October 2020
19
19
Cautions with SGLT-2 Inhibitors
• 4 years time to benefit for Adverse Reaction / Side Effect Canagliflozin Dapagliflozin Empagliflozin Ertugliflozin
Heart Failure balanitis
candidiasis
3.8 ‐ 4.2%
10.6 ‐ 11.6%
2.7 ‐ 2.8%
2.7 ‐ 8.4%
1.6 ‐ 3.1%
1.6 ‐ 6.4%
3.7 ‐ 4.2%
3.7 ‐ 12.2%
• Several FDA warnings cystitis 4.4 ‐ 5.9% 4.3 ‐ 5.7% 7.6 ‐ 9.3% 4%
“pre-emergent” adverse diuresis >10% >10% >10% >10%
hypercholesterolemia Reported 2.1 ‐ 2.5% 4.6 ‐ 6.5% Reported
events hyperlipidemia Reported3/18/2021
Self Assessment Question 5 21
True or False
All beta blocker drugs are safe to use in heart failure
Correct answer: false
21
Self Assessment Question 6 22
Your heart failure patient (NYHA class III) is complaining of
some general arthritis-type pain that he has had for many years.
He wants to take the over-the-counter Ibuprofen for a few days
as this has always helped him in the past.
What do you advise him to do?
a. Take the ibuprofen but not more than 200mg twice daily
b. Call the pharmacy to ask them
c. Advise to use a different pain medication like acetaminophen
d. Have physician e-prescribe Ibuprofen 800mg
Correct answer: c
22
113/18/2021
Case study AJ 92 yo female 23
23
23
Case Study – AJ – Current Meds – 17 medications 24
24
123/18/2021
Simplify medication regimen to 8 medications? 25
25
Case Study NT – 55 yo female 26
26
26
133/18/2021
NT’s Current Medications-23 27
27
27
Summary 28
• Medical management of heart failure can be complex and
patients can be quite different in presentation
• At the core of heart failure is a catabolic state that results in
four main categories of symptoms:
• Dyspnea
• Anxiety / depression
• Fatigue
• Anorexia / cachexia
• Guideline directed evaluation and management of heart
failure can contribute to the addition of several medications to
patients’ medication regimens
28
143/18/2021
29
15You can also read