The 1918 Influenza Pandemic: Insights for the 21st Century
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

PERSPECTIVE
The 1918 Influenza Pandemic: Insights
for the 21st Century
David M. Morens and Anthony S. Fauci
Downloaded from https://academic.oup.com/jid/article-abstract/195/7/1018/800918 by guest on 22 March 2020
National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, Maryland
The 1918–1919 H1N1 influenza pandemic was among the most deadly events in recorded human history, killing an estimated
50–100 million persons. Because recent H5N1 avian epizootics have been associated with sporadic human fatalities, concern
has been raised that a new pandemic, as fatal as the pandemic of 1918, or more so, could be developing. Understanding the
events and experiences of 1918 is thus of great importance. However, despite the genetic sequencing of the entire genome
of the 1918 virus, many questions about the 1918 pandemic remain. In this review we address several of these questions,
concerning pandemic-virus origin, unusual epidemiologic features, and the causes and demographic patterns of fatality. That
none of these questions can yet be fully answered points to the need for continued pandemic vigilance, basic and applied
research, and pandemic preparedness planning that emphasizes prevention, containment, and treatment with antiviral med-
ications and hospital-based intensive care.
The spread of H5N1 avian influenza vi- ple in the United States and an estimat- ORIGIN OF THE 1918
ruses from Asia to the Middle East, Eu- ed 50–100 million people worldwide [4]. PANDEMIC INFLUENZA VIRUS
rope, and Africa has heightened interna- This pandemic’s explosive and still-un-
tional alarm that an influenza pandemic explained patterns of rapidly recurrent The 1918–1919 influenza pandemic was
may be imminent [1]. The World Health waves and predilection to kill the young caused by an influenza A virus of the
Organization [2] and many individual and healthy [5–7] cast an element of ur- H1N1 subtype. Sequence analysis suggests
nations, including the United States [3], that the ultimate ancestral source of this
gency over pandemic planning today.
virus is almost certainly avian [10, 11].
have developed plans to detect the emer- Lacking complete explanations for the
This is not an unexpected finding: the en-
gence of pandemic influenza and to limit genesis and epidemiologic behavior of the
teric tracts of waterfowl such as ducks and
its effects. Because no influenza pandemic 1918–1919 pandemic [8], Taubenberger
geese serve as reservoirs for all known in-
has appeared since 1967–1968, such plans and colleagues recently took a critical step
fluenza A viruses [1, 11]. Waterfowl typ-
rely on consideration of this and earli- by sequencing the entire 8-segment ge-
ically experience asymptomatic infection
er pandemics. Of these, the 1918–1919 nome of the 1918 influenza virus, using
and exert little selection pressure on viral
“Spanish flu” pandemic was among the RNA fragments recovered from the lungs
evolution. To jump to new hosts such as
deadliest public-health crises in human of several victims [9, 10]. This scientific
chickens or mammals and infect very dif-
history, killing an estimated 675,000 peo- achievement has spurred many important ferent cell types, such as human lung cells,
avenues of research, including advances rather than duck enteric cells, an influenza
Received 2 October 2006; accepted 9 November 2006; such as the discovery that the 1918 virus virus may have to adapt by accumulating
electronically published 23 February 2007. apparently arose not by gene reassortment
Potential conflicts of interest: none reported.
one or more point mutations or by reas-
Reprints or correspondence: Dr. Anthony S. Fauci, Director, between a human and animal virus but sortment with a gene segment from a dif-
National Institute of Allergy and Infectious Diseases, National by genome adaptation, a previously un-
Institutes of Health, 31 Center Dr., Bldg. 31, Rm. 7A-03 MSC
ferent influenza virus [8, 12]. A third pos-
2520, Bethesda, MD 20892-2520 (AFAUCI@niaid.nih.gov); or Dr. documented mechanism of pandemic- sible genetic mechanism, homologous
David M. Morens, National Institute of Allergy and Infectious virus generation. Despite these insights, recombination between gene segments of
Diseases, National Institutes of Health, 6610 Rockledge Dr., Rm.
4097, Bethesda, MD 20892-6603 (dm270q@nih.gov). many fundamental questions remain. In different viruses, has not yet been shown
The Journal of Infectious Diseases 2007; 195:1018–28 this article, we discuss several issues that to be of importance for the evolution of
This article is in the public domain, and no copyright is claimed.
0022-1899/2007/19507-0016
have implications for modern pandemic human influenza viruses.
DOI: 10.1086/511989 preparedness (table 1). It is unclear which host served as the
1018 • JID 2007:195 (1 April) • PERSPECTIVETable 1. Important questions posed by the 1918 influenza pandemic.
Question Answer
Where did the 1918 virus originate? Unknown; unlike H5N1, from an avian influenza lineage genetically dis-
tinct from those currently known
What was the pathogenesis, and why did so many people die? Different pathogenesis in 1918 not documented: causes of death in 1918
similar to those during other pandemics; most fatalities had secondary
pneumonias caused by common bacteria or, in a minority of cases,
ARDS-like syndromes; higher proportion of severe cases at all ages;
1918 virus-virulence determinants not yet mapped
Why were there so many deaths among the young and healthy? Unknown; unappreciated host or environmental variables possible, such
as robust immunological response to the virus in younger individuals,
resulting in enhanced tissue damage
Downloaded from https://academic.oup.com/jid/article-abstract/195/7/1018/800918 by guest on 22 March 2020
Why was mortality among the elderly lower than expected? Unknown; evidence is consistent with prior exposure to a virus—
conceivably the virus associated with the 1847 pandemic—eliciting
protective immunity
Why were there 3 pandemic waves during 1918–1919, and what Unknown; at least 2 virus variants during second wave; identity of
are the implications for predicting future pandemic spread? viruses during first and third waves not known; epidemiology of
rapidly recurrent waves not understood
Do influenza pandemics occur in predictable cycles? Insufficient evidence for pandemic cyclicity; steps in pandemic
emergence not fully understood
Are we better able to prevent morbidity and mortality today? Yes, in developed world with advanced medical care, antibiotics,
antivirals, and effective public health; preventive vaccines would be
critical if available in time; however, developing world still at great risk
NOTE. ARDS, acute respiratory distress syndrome.
source of the 1918 virus—and how the from disease and perhaps infection [5–7]. birds. The H1N1 and H5N1 viruses thus
virus adapted to humans. Examination of One possible explanation is previous ex- seem to have gone down different evo-
the genome of the 1918 H1N1 influenza posure to an antigenically related virus lutionary paths. Taken together, the in-
virus [9, 10] has not provided complete that had circulated widely. However, evi- formation noted above is consistent with
answers; indeed, it has posed difficult new dence for such a virus is incomplete. the possibility that the precursor to the
questions. Although all 8 gene segments Further complicating the issue is the 1918 virus was hidden in an obscure eco-
of the 1918 virus are clearly avian-like, fact that at least 2 different H1N1 influ- logic niche before emerging in humans.
they are genetically distinct from any of enza-virus strains that had markedly dif-
the hundreds of avian or mammalian in- ferent receptor-binding specificities and PATHOGENESIS AND EXCESS
fluenza viruses collected and examined be- that were fatal to humans were circulating MORTALITY IN 1918–1919
tween 1917 and 2006, primarily because simultaneously in 1918 [13]. One strain
of greater-than-expected numbers of silent contained variations in both the 190 and In healthy children and adults, influenza
nucleotide changes. Moreover, the genes 225 codons (mutations E190D and D225G, is usually an uncomplicated febrile illness
of the 1918 virus apparently have evolved respectively) of the H1 gene. These changes that may incapacitate but rarely kills [16].
together in parallel, possibly in an uni- enable the hemagglutinin (HA) protein of Many typical seasonal influenza infections
dentified host [8]. Thus, unlike the 1957 the virus to bind only to a(2–6) sialic-acid are asymptomatic or cause only mild or
and 1968 pandemics, each of which re- receptors found on human/mammalian vague symptoms. Others cause “classical”
sulted from reassortment between circu- cells. The second circulating strain con- influenza: 4 or 5 days of fever, chills, head-
lating descendants of the 1918 human vi- tained only the E190D change, rendering ache, muscle pain, weakness, and, some-
rus and circulating avian influenza strains, it capable of binding to both mammalian times, upper-respiratory-tract symptoms
the 1918 pandemic apparently arose by a(2–6) receptors and avian a(2–3) sialic- and cough. Severe complications and
genetic adaptation of an existing avian vi- acid receptors [14, 15]. Although the 1918 deaths can occur, especially in infants, the
rus to a new (human) host [8, 10–12]. virus appears to be descended from an elderly, and individuals with chronic con-
The obscurity of the viral origin of the avian virus, before the 1918 pandemic ditions such as diabetes mellitus and heart
1918 influenza poses a paradox. The there were few if any reports of unusual disease. Among the most severe compli-
lower-than-expected mortality among in- die-offs of wild waterfowl or domestic cations is pneumonia, which can be asso-
dividuals who were 145 years old in 1918 poultry, as has occurred with the modern ciated with secondary bacterial infection.
(i.e., those born before 1873; see the dis- H5N1 virus, indicating that the earlier vi- The first widely studied influenza pan-
cussion below) implies partial protection rus was not then highly pathogenic for demic occurred during 1889–1893 [17,
PERSPECTIVE • JID 2007:195 (1 April) • 101918]. To older physicians in 1918, obvious nual seasonal recurrences. Moreover, mor- have been an acute aggressive broncho-
similarities to the 1889 pandemic included tality during the latter 2 of the 3 1918– pneumonia featuring epithelial necrosis,
its highly contagious nature, with clinical 1919 waves was much higher, at all ages microvasculitis/vascular necrosis, hemor-
attack rates typically in the 20%–60% except among the elderly, than that during rhage, edema, and widely variant pathol-
range. In both pandemics, most deaths 1889, and it featured an enormous mor- ogy in different parts of the lung, from
resulted from respiratory complications, tality peak in healthy young adults (figure which pathogenic bacteria could usually
such as pneumonia with bacterial inva- 2B), an age group believed to have been be cultured at autopsy (figure 1; also see
sion; however, in 1918 there also were at low risk of death in all other pandemics [28]). In a few autopsies, severe broncho-
seemingly new and severe clinical forms up to that time. For purposes of compar- pneumonia was seen without evidence of
of disease. In 1889 many deaths due to ison, the 1957 and 1968 influenza pan- bacteria, but studies generally showed a
pneumonia were attributed to familiar demics, both caused by descendants of the close correlation between the distribu-
conditions such as subacute bacterial lobar 1918 virus, produced relatively low mor- tions of pulmonary lesions and cultured
Downloaded from https://academic.oup.com/jid/article-abstract/195/7/1018/800918 by guest on 22 March 2020
pneumonia, whereas in 1918 this “back- tality overall, did not produce rapidly suc- bacteria [34, 35], identifying the major
ground” influenza mortality was greatly cessive waves or multiple annual recur- bacteria as the organisms now known
augmented both by cases of aggressive rences of high mortality, and settled more as Streptococcus pneumoniae, S. pyogenes,
fatal bronchopneumonia and by acute quickly into familiar patterns of annual and, less commonly, Haemophilus influen-
deaths associated with progressive cya- seasonal endemic circulation [19–21]. zae and Staphylococcus aureus [22, 36–40].
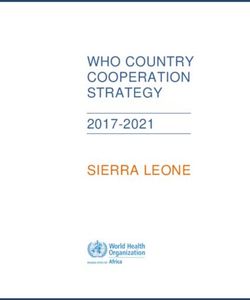
nosis and collapse (figure 1). Clinical and autopsy series [22–33] sug- Scientists have long suspected that the
Unlike the 1889–1893 pandemic, which gest that excess influenza deaths (i.e., pathogenesis of the 1918 virus was aug-
made 3 or more successive annual and deaths above the expected background mented by concomitant infection with the
largely seasonal reappearances, the 1918 level for influenza) during 1918–1919 virus and with bacteria such as S. pneu-
pandemic spread in 3 rapidly recurring seem to have been associated with 2 over- moniae and S. pyogenes [41].
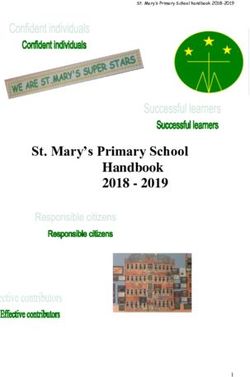
waves within an ∼9-month interval (figure lapping clinical-pathologic syndromes The second syndrome, comprising per-
2A), before settling into a pattern of an- (figure 1). The most common appears to haps 10%–15% of fatal cases, was a severe
Figure 1. Histological appearance of lung sections from 3 fatal cases of influenza during 1918, showing distinct clinical-pathologic forms. A, Severe
and rapidly progressing necrotizing/hemorrhagic bronchopneumonia, which is consistent with cytolytic viral damage and secondary bacterial invasion
by respiratory-tract pathogens and which is associated with some (probably a minority of) deaths. B, Severe bacterial bronchopneumonia from which
Streptococcus pneumoniae, S. pyogenes, Haemophilus influenzae, or, less frequently, Staphylococcus aureus could be cultured and which is associated
with the majority of deaths. The extent to which secondary bacterial pneumonia may have followed primary necrotizing viral pneumonia is unclear,
because early signs of viral cytolytic damage had typically been obliterated by the time of autopsy. C, Another clinical form of disease, which, although
it had not been characterized when the culture was performed, is thought to be similar to acute respiratory distress syndrome (ARDS) [42] and appears
to have been associated with a minority of fatal cases. Patients with this form experienced extremely rapid progression of the disease and may have
literally drowned because of fluid-filled alveoli, often in the absence of bacteria or inflammatory infiltrate. Varying degrees of the same pathologic
features seen in this ARDS-like form were also seen in many or most patients with the severe cytolytic form (see panel A). (Photographs courtesy
of Jeffery K. Taubenberger, National Institute of Allergy and Infectious Diseases, National Institutes of Health.)
1020 • JID 2007:195 (1 April) • PERSPECTIVEDownloaded from https://academic.oup.com/jid/article-abstract/195/7/1018/800918 by guest on 22 March 2020 Figure 2. A, Monthly influenza-associated mortality in Breslau, Silesia (now Wroclaw, Poland), from June 1918 through December 1922. On this graph, reproduced on the basis of data reported by Lubinski [44], we have superimposed indications of the 3 waves (W1, W2, and W3) of the 1918– 1919 pandemic, as well as the first 3 annual winter postpandemic recurrences during 1919–1920 (R1), 1920–1921 (R2), and 1921–1922 (R3). During 1918–1919, many locales experienced these 3 waves. B, Age-specific influenza-associated mortality in Breslau, from July 1918 to April 1922. The unbroken line combines influenza-associated mortality during waves W2 and W3 of the 1918–1919 pandemic; the dashed line denotes influenza- associated mortality during the first winter recurrence, from January to April 1920 (R1); the dotted line denotes influenza-associated mortality during the R3 winter recurrence, from December 1921 to April 1922. The peak young-adult mortality, documented worldwide, is evident in the W2+W3 and R1 curves of 1919–1921 but has completely disappeared by 1922.
acute respiratory distress–like syndrome young adults, which was responsible for cases of H5N1 infection in humans [52],
(ARDS) [42] in which patients developed approximately half of the total influenza experimental studies of H5N1 in macro-
a peculiar “heliotrope cyanosis” char- deaths, including the majority of excess phages [53], and other information on im-
acterized by blue-gray facial discolora- influenza deaths [8] (figure 2B). munopathogenesis [54, 55], which sug-
tion and essentially drowned from “huge Explaining the extraordinary excess in- gests that human infection with influenza
[amounts of] … thin and watery bloody fluenza mortality in persons 20–40 years viruses, including the 1918 virus [56, 57],
exudates in the lung tissue and bronchi- of age in 1918 is perhaps the most im- can result in excessive release of cytokines.
oles” [24, p. 650]. There are few if any portant unsolved mystery of the pan- Experimental animal studies of recon-
representative data to document these per- demic. These young adults were part of structed 1918 influenza-virus infection
centages exactly, and there are marked dif- an age cohort born during 1878–1898; evi- have also shown up-regulation of acute
ferences between various published series dence suggests that, during that 20-year inflammatory cytokines [56–59]; for ex-
and between military and civilian popu-
Downloaded from https://academic.oup.com/jid/article-abstract/195/7/1018/800918 by guest on 22 March 2020
time span, there was wide circulation only ample, intranasal challenge of mice with
lations. Nor is it certain that deaths due of an H3 influenza virus [45], which ap- the reconstituted 1918 virus led to a highly
to either the ARDS-like syndrome or peared as a pandemic in 1889, in the mid- lethal and rapidly progressing pulmo-
bronchopneumonias lacking massive bac- dle of the birth-risk interval. nary disease characterized by high viral
terial invasion represented primary viral Host and environmental variables have growth, a histological picture of necro-
pneumonias. Although these 2 pathologic not been systematically investigated as pos- tizing bronchitis/bronchiolitis, alveolitis,
pictures may not be unique to the 1918 sible causes of increased mortality in the alveolar hemorrhage and edema, and
pandemic [43], they clearly occurred with young and healthy. It is possible that vig- overexpression of acute inflammatory cy-
significantly greater frequency than they orous immune responses directed against tokines [58]. Comparison of pathologic
had during other known influenza pan- the virus in healthy young persons could findings during 1918–1919, cases of fatal
demics. It seems reasonable to propose have caused severe disease in 1918; for ex- human H5N1 infections [52], and 2 un-
that in the 1918 pandemic many excess ample, an unusually brisk and paradoxi- related viral pulmonary diseases—namely,
deaths resulted from a disease process that cally pathogenic antiviral immune re- severe acute respiratory symdrome [60,
began with a severe acute viral infection sponse has been observed when patients 61] and severe hantavirus pulmonary syn-
that spread down the respiratory tree, with AIDS respond to treatment with an- drome [47, 62]—thought to be associated
causing severe tissue damage that often tiretroviral drugs; return of immune func- with cytokine storms suggests that, al-
was followed by secondary bacterial in- tion leads to severe inflammatory re- though they differ in pathologic features,
vasion. More-definitive answers regarding sponses to viruses and microorganisms ARDS may be a common end point.
disease pathogenesis may be fostered by a infecting the patients (the immune-recon- However, it must also be remembered
comprehensive reexamination of 1918 au- stitution inflammatory syndrome [46]). that in 1918 many or most severe cases
topsy series.
Another viral cause of severe ARDS—han- of influenza-related pulmonary disease
tavirus pulmonary syndrome [47], es- featured both severe bronchopulmon-
EXCESS DEATHS AMONG
pecially in association with the North ary tissue damage and severe secondary
THE YOUNG AND HEALTHY
American Sin Nombre virus—features an bacterial infection [8].
Two unique epidemiologic features ac- unexplained preponderance of cases in Immunopathogenesis may also differ
count for most excess mortality in 1918– young adults, a preponderance that ap- between various age groups because peo-
1919: a high case-fatality rate at all ages, pears not to be due solely to higher rates ple of different ages have been exposed to
and a surprising excess of mortality among of exposure among this age group [48, 49]. different viruses at different times and be-
20–40-year-old individuals, an age group It is conceivable that aberrant inflamma- cause response to a new virus may depend
at comparatively low risk for influenza tory responses play a role in this situation. on the history of previous exposures. In
mortality in pandemics before and since. The notion that a so-called cytokine this regard, antibody-dependent enhance-
Curves of influenza mortality by age at storm, a deleterious overexuberant release ment of infection, which has been sus-
death are typically U-shaped, reflecting of proinflammatory cytokines such as in- pected as a cause of dengue hemorrhagic
high mortality in the very young and the terleukin-6 and -8 and tissue necrosis fac- fever in association with second dengue
very old, with low mortality at all ages tor–a, could have contributed to the high infections, has been demonstrated in vitro
between [8]; in contrast, the 1918–1919 mortality and excessive number of deaths with influenza viruses [63]. Alternatively,
pandemic and succeeding winter epidemic among the young and otherwise healthy the W-shaped mortality pattern could be
recurrences in 1919 and 1920 [44] pro- during the 1918 pandemic has been fre- consistent with an environmental expo-
duced W-shaped mortality curves, which quently proposed [50, 51]. This theory is sure peculiar to young adults (e.g., smok-
featured a third mortality peak, in healthy bolstered by recent observations of fatal ing or aspirin use); however, data ex-
1022 • JID 2007:195 (1 April) • PERSPECTIVEamining this possibility have not been the 1889 pandemic virus could have been 1918–1919 pandemic seems to have spread
reported, and thus the 1918 W-shaped of H3N8 identity. The 1847 pandemic in at least 3 distinct waves within an ∼9-
mortality curve and the extremely high might explain 1918 H1N1 protection in month interval. Not all influenza pandem-
mortality in young adults remain to be individuals 170 years old, but only if it ics have had such prominent recurrences,
fully explained. was caused by an H1 or, less likely, N1 and those that did have tended to return
virus that was closely related antigenically at yearly intervals (e.g., 1889–1893), mak-
LOWER-THAN-EXPECTED but much less pathogenic. ing them difficult to distinguish, in kind
MORTALITY AMONG if not in impact, from normal seasonal
THE ELDERLY THE 3 PANDEMIC WAVES
influenza [8, 83]. Globally, the first wave
IN 1918–1919: IMPLICATIONS
of the 1918 pandemic, W1, occurred dur-
Although both mortality and the case-fa- FOR PREDICTING FUTURE
ing spring-summer 1918 (as recognized in
tality rate in 1918–1919 were higher, at all PANDEMIC PATTERNS
Downloaded from https://academic.oup.com/jid/article-abstract/195/7/1018/800918 by guest on 22 March 2020
the Northern Hemisphere) and was as-
ages, than would be expected on the basis
Understanding patterns of pandemic sociated with high morbidity but low mor-
of prior (and subsequent) pandemics/ep-
spread is important in planning preven- tality. The 2 following waves, in summer-
idemics, and although the expected pat-
tion strategies and anticipating public- fall 1918 (W2) and winter 1918–1919
tern of markedly increased mortality with
advancing age was clearly present, it is health and medical burdens. Unlike all (W3), were both deadly [7, 44] (figure 2).
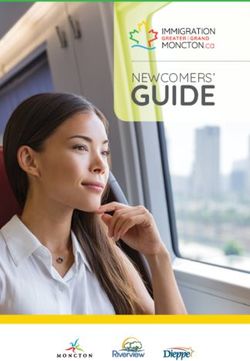
noteworthy that, although increased, mor- previous and subsequent pandemics, the It is difficult to make epidemiologic
tality in the elderly was less pronounced
than that in the other age groups (figure
3). It has been speculated that this might
be due to previous exposure to an anti-
genically related influenza virus [64–66].
Yet, other than regional outbreaks [67, 68]
and an 1872 American epizootic of equine
influenza, which was associated with only
mild human illnesses [69, 70], there is little
evidence for major interpandemic influ-
enza events during the period before 1889
[71]. Moreover, none of the 3 pandemics
during the century before 1918 (in 1830,
1847, and 1889) are thought to have been
associated with multiple, rapidly succes-
sive waves; W-shaped mortality curves;
a predominance of aggressive broncho-
pneumonias; or marked hemorrhagic fea-
tures characteristic of the 1918 pandemic
[8, 17, 18, 72–79]. The 1889 pandemic,
which occurred too closely in time to have
offered protection only for older individ-
uals in 1918, appears to have been caused
by an H3 influenza virus [45]. The pos-
sibility of immunoprotection mediated by
neuraminidase (NA), rather than by HA,
during 1918 is intriguing [80], but there
are few data bearing on this possibility: Figure 3. Influenza-associated mortality in New South Wales, Australia, during the 1891 and
the identity of the 1889 NA is not known 1919 influenza pandemics [65]. The severe waves of the 1918–1919 pandemic in Australia were
with certainty, although serologic data delayed until (the Southern Hemisphere) winter of 1919. Because population data by age in 1891
were not available, and because the mortality in males was similar to that in females, the 1891
from 2 independent sources are consistent
data are based on published male/female mortality-rate means. In all age groups except persons
with an N8 virus appearing in approxi- 165 years old, the mortality per 1000 persons per age group during 1919 (—) were higher
mately 1889 and circulating until some than those during 1891 ( — ), and the age-specific mortality curve was W-shaped, featuring
time before 1918 [81, 82], suggesting that a middle peak of mortality in young adults.
PERSPECTIVE • JID 2007:195 (1 April) • 1023sense of this pattern. If some combination PREDICTING INFLUENZA Edwin Kilbourne, Sr., articulated both the
of rising population immunity and un- PANDEMICS widely held conviction about pandemic
favorable seasonality had reduced W1 cir- cyclicity and its scientific rationale. Ex-
culation during the spring of 1918, it is The occurrences of 3 influenza pandemics amination of more-recent evidence, how-
hard to explain how W2 could have begun during the 19th century and of another 3 ever, leads Kilbourne to conclude that
during the 20th century [1] have led some “there is no predictable periodicity or pat-
almost immediately thereafter—and in the
experts to conclude that pandemics occur tern” of major influenza epidemics and
summer, normally the least favorable time
in cycles and that we are now overdue. that “all differ from one another” [90, p.
for influenza-virus circulation. Also, it is
Belief in influenza cyclicity can be traced 9]; without pandemic cycles there can
difficult to explain why, at least in some
to epidemiologic efforts during the mid be little basis for predicting pandemic
locales, the early-summer end of W1 was
19th century; after the 1889–1893 pan- emergence.
largely free of mortality whereas the late-
demic, interest in examining the patterns
Downloaded from https://academic.oup.com/jid/article-abstract/195/7/1018/800918 by guest on 22 March 2020
summer/early-fall onset of W2, appearing It has become clear that pandemic
of influenza recurrence was renewed [86].
so soon thereafter, was associated with ex- emergence can result from at least 2 very
By the 1950s, cumulative historical infor-
traordinarily high mortality. different mechanisms: de novo emergence
mation [5–7, 67, 68, 72–79] seemed to
The question arises whether different of a completely unique avian-descended
suggest that pandemics appear in regular
influenza viruses caused the different virus (as in 1918) or modification of a
cycles. This seemed to make biological
waves. In this regard, all of the viruses so circulating human-adapted virus by im-
sense: the most recent pandemics (in 1889,
far identified by the Taubenberger labo- portation, via genetic reassortment, of a
1918, and 1957) had apparently been
ratory are from W2 [8]. It would be useful novel HA, either with concomitant im-
caused by different viruses with novel HA
to know whether illness during W1 pro- portation of a novel NA (e.g., the 1957
genes imported from a large, naturally ex-
H2N2 pandemic) or without such con-
tected against illness during W2 and W3, isting avian pool. At approximately the
comitant importation (e.g., the 1968 H3N2
which would imply viral antigenic simi- same time, it was becoming clear that high
pandemic) [8]. There is no reason to sup-
larity or identity. However, there are few levels of population immunity pressured
pose that these 2 different pandemic
good data addressing this issue, and those postpandemic viruses to drift antigenically
mechanisms should be capable of pro-
which exist are both imperfect and con- and that surface protein–encoding genes
ducing the same cyclic intervals—or that
tradictory [84]. Although the most reliable could potentially mix with other HA and
other, competing adaptational mecha-
data demonstrate W2 protection against NA genes to which humans lacked im-
munity [87]. It was reasonable to assume nisms, such as reassortment with closely
W3, they also suggest that W1 protection
that such an intimate viral-immunologic related HAs [91] or changing population
against W2 or W3 illness was minimal at
relationship would have a predictable life immunity induced by increasing use of
best [85]. It is also possible that mutation
span. immunologically complex vaccines, could
of the pandemic virus, leading to greater
Around the time of the 1957 and 1968 not disrupt cycles that might otherwise oc-
pathogenicity, was occurring during mid-
pandemics, the prevailing view was that cur. It has also become clear that, despite
1918; however, this possibility does not in
pandemics tended to recur as frequently a large catalog of naturally occurring in-
itself explain generation of apparently low
as every 10–11 years; however, in 1976 a fluenza surface-protein genes theoretically
protective immunity after high attack rates capable of causing new pandemics by reas-
fatal H1N1 “swine flu” outbreak raised
in W1. The implication that 2 H1N1 phe- sorting themselves into human-adapted
considerable alarm without causing a pre-
notypes were circulating during the fall strains, only 3 of 16 known HAs (i.e., H1,
dicted pandemic [88], and, a year later,
wave (W2), discussed above, also remains H2, and H3) and 2 of 9 known NAs (i.e.,
after 20 years of natural “extinction,” an
to be explained, given (1) that W2 did N1 and N2) are known to have done so
H1N1 descendant of the 1918 virus sud-
appear to protect against illness in W3 and during the past 117 years [87, 92].
denly reemerged to reestablish postpan-
(2) that, after several years had passed, in- demic cocirculation with one of its own Drawing on the earlier theories pro-
fluenza mortality declined to baseline lev- further descendants, the H3N2 influenza posed by Thomas Francis, Jr. [93], and
els, a finding consistent with powerful virus [89], setting up nearly 3 decades of others, Maurice Hilleman attempted to
population immunity and emergence of endemic cocirculation of former pan- reconcile these complications by propos-
less pathogenic viruses. Thus, the 3 waves demic viruses that has continued until to- ing a form of “macrocyclicity” in which
of the 1918–1919 pandemic remain un- day (2006). reappearances of H1, H2, and H3 (ap-
explained, and there is, thus far, little basis Fading belief in pandemic cycles has proximately every 68 years) are driven by
for predicting the recurrence pattern of the been acknowledged by influenza author- cycles of waning population immunity
next pandemic. ities. For decades, noted influenza expert that have approximately the same dura-
1024 • JID 2007:195 (1 April) • PERSPECTIVEtion as does the mean human life span that if a novel virus as pathogenic as that programs featuring annual vaccination
[87]. Because scientific evidence of viral of 1918 were to reappear today, a sub- with up-to-date influenza and pneumo-
identity extends backward for only 117 stantial proportion of a potential 1.9 mil- coccal vaccines, and a national and inter-
years, it will take many future generations lion fatalities (assuming 1918 attack and national prevention infrastructure. Also
to fully test Hilleman’s hypothesis. case-fatality rates in the current US pop- important for pandemic response are 2
Historical evidence of pandemic occur- ulation) could be prevented with aggres- classes of antiviral drugs (adamantanes
rences provides no obvious cyclic patterns sive public-health and medical interven- and neuraminidase inhibitors), one or
during the past 3 centuries [67, 68, 72– tions. In an age of frequent air travel, we both of which have proven effective, in
79, 94–97] (figure 4). Presumably, mutable might expect global spread to proceed rap- culture, against most of the currently cir-
viruses producing high population im- idly and to be difficult to control, but culating H5N1 viruses. However, antiviral
munity will eventually drive their own hardly much more so than the 1918 pan- resistance might appear fairly quickly, and
evolutionary changes; however, if pan-
Downloaded from https://academic.oup.com/jid/article-abstract/195/7/1018/800918 by guest on 22 March 2020
demic, in which most of the world was circulating H5N1 strains in several coun-
demic cycles do occur, they must be so affected by W2 within a matter of a few tries have already been shown to be ada-
irregular as to confound predictibility. weeks. mantane resistant [99]. We also have an-
Almost all “then-versus-now” compar- tibiotics to treat pneumonias caused by all
PREVENTING MORBIDITY
isons are encouraging, in theory. In 2007, of the major bacteria implicated in the
AND MORTALITY IN FUTURE
public health is much more advanced, 1918 pandemic; hospital-based intensive
PANDEMICS
with better prevention knowledge, good care and supportive therapy, including
The weight of evidence, supported by influenza surveillance, more trained per- ventilatory support for patients with se-
mathematical modeling data [98], suggests sonnel at all levels, established prevention vere ARDS; and a biomedical research ca-
Figure 4. Influenza pandemic occurrence, 1600–2000. Information was compiled from historical references [67, 68, 72–79, 94–97] and from scientific
publications from 1889 to the present (not cited). Interpandemic intervals are noted at the top of the graph. Pandemics are associated with (1) abrupt
and widespread epidemicity in multiple locales in 2 or more geographic regions, (2) rapid progression through large open populations, (3) high clinical-
illness rates affecting a broad range of ages, and (4) no other pandemic activity within 5 years (to adjust for the possibility of slow and interrupted
pandemic spread before the mid 19th century). Especially before 1697, pandemics may be difficult to verify and track, because of slower spread [87]
as a result of slower and less frequent human travel. Some cited sources suggest different interpretations than those presented here (see text and
references [67, 68, 72–79, 89–92]). The black bars () denote pandemics; the white bars () denote major widespread epidemics that do not meet
pandemic criteria. The 1977 reemergence and global spread of an “extinct” descendant of the 1918 pandemic virus, denoted by the asterisk (*), is
included here as a pandemic emergence, although it might also be considered as reflecting the continuing spread of the original pandemic virus.
PERSPECTIVE • JID 2007:195 (1 April) • 1025pacity rapidly compiling critical knowl- able evolution of the several related pan- Vaughn HF, Palmer GT. Epidemiology in
public health: a text and reference book for
edge about many aspects of influenza. demic influenza viruses that have ap- physicians, medical students, and health
The most difficult challenge would peared and circulated during the past workers. St. Louis: CV Mosby, 1922:297–408.
probably not be to increase medical century. The more that we learn about 7. Jordan EO. Epidemic influenza: a survey.
Chicago: American Medical Association, 1927.
knowledge about treatment and preven- these viruses and about what they are ca-
8. Taubenberger JK, Morens DM. 1918 Influ-
tion but to increase medical capacity and pable of doing to maintain their deadly enza: the mother of all pandemics. Emerg
resource availability (e.g., hospital beds, relationship with the human species, the Infect Dis 2006; 12:15–22.
9. Taubenberger JK, Reid AH, Krafft A, Bij-
medical personnel, drugs, and supplies) more remarkable they seem. The challenge
waard KE, Fanning TG. Initial genetic char-
and public-health and community-crisis for us humans is to learn as much about acterization of the 1918 “Spanish” influenza
responses to an event in which 25–50% influenza viruses as they have already virus. Science 1997; 275:1793–6.
of the population could fall ill during a learned about us. Arguably, we have not 10. Taubenberger JK, Reid AH, Lourens RM,
Wang R, Jin G, Fanning TG. Characterization
yet done so, but we are clearly gaining
Downloaded from https://academic.oup.com/jid/article-abstract/195/7/1018/800918 by guest on 22 March 2020
few weeks’ time. Health-care systems of the 1918 influenza polymerase genes. Na-
could be rapidly overwhelmed by the sheer ground, and there is good reason to believe ture 2005; 437:889–93.
volume of cases; ensuring production and that the next decade will yield significant 11. Reid AH, Taubenberger JK, Fanning TG. Evi-
dence of an absence: the genetic origins of
delivery of sufficient quantities of antivi- advances in fundamental knowledge and,
the 1918 pandemic influenza virus. Nat Rev
rals, vaccines, and antibiotics, as well as more importantly, in prevention and con- Microbiol 2004; 2:909–14.
providing widespread access to medica- trol. Today, nearly a century after the 12. Scholtissek C, Rohde W, Von Hoyningen V,
Rott R. On the origin of the human influenza
tions and medical care, particularly in im- event, mysteries surrounding the 1918 in-
virus subtypes H2N2 and H3N2. Virology
poverished regions, would be a sobering fluenza pandemic remain largely unex- 1978; 87:13–20.
challenge. And the just-in-time nature of plained. However, we must continue to 13. Reid A, Janczewski TA, Lourens RM, et al.
examine and investigate this long-ago 1918 Influenza pandemic caused by highly
our supply chain of necessary medications conserved viruses with two receptor-binding
and equipment for medical care could eas- tragedy, allowing it to stand clearly before variants. Emerg Infect Dis 2003; 9:1249–53.
ily be disrupted by such a global public- us as a challenge to complacency, as a 14. Glaser L, Stevens J, Zamarin D, et al. A single
modern problem with future implications, amino acid substitution in 1918 influenza vi-
health catastrophe. rus hemagglutinin changes receptor binding
Moreover, because most of the world and as a grim reminder of the importance,
specificity. J Virol 2005; 79:11533–6.
would not have access to the same level to humanity, of continuing the fight 15. Stevens J, Blixt O, Glaser L, et al. Glycan
of prevention and medical care as is avail- against emerging and reemerging infec- microarray analysis of the hemagglutinins
from modern and pandemic influenza vi-
able to developed countries, the greatest tious diseases.
ruses reveals different receptor specificities. J
burden of pandemic influenza would fall Mol Biol 2006; 355:1143–55.
16. Glezen WP, Cherry JD. Influenza viruses. In:
on those least privileged. The best hope Acknowledgment Feigin RD, Cherry JD, eds. Textbook of pe-
for everyone may rest on the future de- diatric infectious diseases (3rd ed.). Vol II. Phil-
We thank Jeffery K. Taubenberger for helpful
velopment and stockpiling of vaccines comments and criticisms, as well as for the his- adelphia: WB Saunders, 1992:1688–1704.
tologic photographs in figure 1. 17. Parsons HF; Local Government Board. Re-
that are more broadly efficacious—for
port on the influenza epidemic of 1889–90.
example, “universal” influenza vaccines Parliament [Great Britain]. Papers by com-
based on either immunogenic antigens References
mand [C. 6387]. London: Eyre & Spottis-
woode, 1891.
shared by all influenza viruses [100] or
1. Webster RG, Peiris M, Chen H, Guan Y. 18. Parsons HF; Local Government Board. Fur-
multivalent HAs and NAs [101], both of ther report and papers on epidemic influ-
H5N1 outbreaks and enzootic influenza.
which are currently being developed. In Emerg Infect Dis 2006; 12:3–8. enza, 1889–92. Parliament [Great Britain].
the meantime, efforts must be directed to- 2. World Health Organization. WHO global in- Papers by command [C.-7051]. London:
fluenza preparedness plan: the role of WHO Eyre & Spottiswoode, 1893.
ward prevention based on improved un- 19. Dauer CC, Serfling RE. Mortality from in-
and recommendations for national measures
derstanding of pandemic risks, increased before and during pandemics. Geneva: fluenza 1957–1958 and 1959–1960. Am Rev
surveillance, development of countermea- World Health Organization, 2005. Respir Dis 1961; 83:15–28.
3. US Department of Health and Human Ser- 20. Housworth WJ, Spoon MM. The age distri-
sures, logistical planning, and an aggres- bution of excess mortality during A2 Hong
vices. HHS pandemic influenza plan. Wash-
sive and broad research agenda. ington, DC: US Government Printing Office, Kong influenza epidemics compared with
It is noteworthy that influenza research 2005. earlier A2 outbreaks. Am J Epidemiol 1971;
4. Johnson NPAS, Mueller J. Updating the ac- 94:348–50.
during the past decade has simultaneously
counts: global mortality of the 1918–1920 21. Kilbourne ED. Epidemiology of influenza.
looked both forward and backward in “Spanish” influenza pandemic. Bull Hist In: Kilbourne ED, ed. The influenza viruses
time, not merely to connect the dots but Med 2002; 76:105–15. and influenza. New York: Academic Press,
5. Vaughan WT. Influenza: an epidemiologic 1975:483–538.
to identify slowly unfolding patterns that
study. Monograph ser 1. Am J Hyg (Balti- 22. Holman WL. The bacteriology of epidemic
can only be revealed when examined in more), 1921. influenza with a discussion of B. influenzae
their entirety—for example, the remark- 6. Vaughn VC. Influenza. In: Vaughn VC, as the cause of this and other infective pro-
1026 • JID 2007:195 (1 April) • PERSPECTIVEcesses. In: Members of the Faculty of the 39. Walker OJ. Pathology of influenza-pneu- the haemagglutinin of the 1918 pandemic
School of Medicine, University of Pittsburgh. monia. J Lab Clin Med 1919–1920; 5:154–75. virus. Nature 2004; 431:703–7.
Studies on epidemic influenza comprising 40. Birge EG, Havens LC. A comparison of the 58. Tumpey TM, Basler CF, Aguilar PV, et al.
clinical and laboratory investigations by bacteriology of pneumonia, antemortem and Characterization of the reconstructed 1918
members of the faculty of the School of Med- postmortem. New York Med J 1919; 109: Spanish pandemic influenza virus. Science
icine, University of Pittsburgh. Pittsburgh: 544–5. 2005; 310:77–80.
University of Pittsburgh, 1919:161–205. 41. McCullers JA, Bartmess KC. Role of neura- 59. Kash JC, Tumpey TM, Proll SC, et al. Ge-
23. Klotz O. The pathology of epidemic influ- minidase in lethal synergism between influ- nomic analysis of increased host immune
enza. In: Members of the Faculty of the enza virus and Streptococcus pneumoniae. J and cell death responses induced by 1918
School of Medicine, University of Pittsburgh. Infect Dis 2003; 187:1000–9. influenza virus. Nature 2006; 443:578–81.
Studies on epidemic influenza comprising 42. Esteban A, Fernández-Segoviano P, Frutos- 60. Jiang Y, Xu J, Zho C, et al. Characterization
clinical and laboratory investigations by Vivar F, et al. Comparison of clinical criteria of cytokine/chemokine profiles of severe
members of the faculty of the School of Med- for the acute respiratory distress syndrome acute respiratory syndrome. Am J Respir Crit
icine, University of Pittsburgh. Pittsburgh: with autopsy findings. Ann Intern Med 2004; Care Med 2005; 171:850–7.
University of Pittsburgh, 1919:207–94. 141:440–5. 61. Baas T, Taubenberger JK, Chong PY, Chui P,
Downloaded from https://academic.oup.com/jid/article-abstract/195/7/1018/800918 by guest on 22 March 2020
24. LeCount EA. The pathologic anatomy of in- 43. Stengel A. The influenza epidemics of 1889 Katze MG. SARS-CoV virus-host interac-
fluenzal bronchopneumonia. JAMA 1919; and 1918. Med Clin North Am 1918; 2: tions and comparative etiologies of acute re-
72:650–2. 645–69. spiratory distress syndrome as determined by
25. LeCount EA. Disseminated necrosis of the 44. Lubinski H. Statistische Betrachtungen zur transcriptional and cytokine profiling of for-
pulmonary capillaries in influenzal pneu- Grippepandemie in Breslau 1918–22. Zen- malin-fixed paraffin-embedded tissues. J In-
monia. JAMA 1919; 72:1519–20. tralbl Bakteriol Parasitenkd Infektionskrank- terferon Cytokine Res 2006; 26:309–17.
26. Lyon MW. Gross pathology of epidemic in- heiten 1923–1924; 91:372–83. 62. Mori M, Rothman AL, Kurane I, et al. High
fluenza at Walter Reed General Hospital. 45. Dowdle WR. Influenza A virus recycling re- levels of cytokine-producing cells in the lung
JAMA 1919; 72:924–9. visited. Bull WHO 1999; 77:820–8. tissues of patients with fatal hantavirus pul-
27. Wohlbach SB. Comments on the pathology 46. Hirsh HH, Kaufmann G, Sendi P, Battegay monary syndrome. J Infect Dis 1999; 179:
and bacteriology of fatal influenza cases, as M. Immune reconstitution in HIV-infected 295–302.
observed at Camp Devens, Massachusetts. patients. Clin Infect Dis 2004; 38:1159–66. 63. Morens DM. Antibody-dependent enhance-
Bull Johns Hopkins Hosp 1919; 30:104–9. 47. Zaki SR, Greer PW, Coffield LM, et al. Han- ment of infection and the pathogenesis of
28. Oberndorfer. Ueber die pathologische Ana- tavirus pulmonary syndrome: pathogene- viral disease. Clin Infect Dis 1994; 19:500–12.
tomie der influenzaartigen Epidemie im Juli sis of an emerging infectious disease. Am 64. Frost WH. The epidemiology of influenza.
1918. Munch Med Wochenschr 1918; 65: J Pathol 1995; 146:552–79. Public Health Rep 1919; 34:1823–61.
811–2. 65. Legislative Assembly, New South Wales [Aus-
48. Khan AS, Khabbaz RF, Armstrong LR, et al.
29. MacCallum WG. Pathological anatomy of tralia]. Report of the director-general of pub-
Hantavirus pulmonary syndrome: the first 100
lic health, New South Wales, for the year
pneumonia associated with influenza. Johns US cases. J Infect Dis 1996; 173:1297–1303.
1919, including a report on the influenza ep-
Hopkins Hosp Rep 1920; 20:149–249. 49. Ferrés M, Vial P. Hantavirus infection in chil-
idemic, 1919. Sydney: William Applegate
30. Tobias JW. Anatomı́a patológica de la grippe dren. Curr Opin Pediatr 2004; 16:70–5.
Gullick, 1920.
pandémica. Rev Univ B Aires 1920; 17:109–99. 50. Snelgrove R, Williams A, Thorpe C, Hussell
66. Luk J, Gross P, Thompson WW. Observa-
31. Winternitz MC, Wason IM, McNamara FP. T. Manipulation of immunity to and pa-
tions on mortality during the 1918 influenza
The pathology of influenza. New Haven, CT: thology of respiratory infections. Expert Rev
pandemic. Clin Infect Dis 2001; 33:1375–8.
Yale University Press, 1920. Anti Infect Ther 2004; 2:413–26.
67. Hirsch A. Influenza. In: Hirsch A. Handbuch
32. Levinthal W, Kuczynski MH, Wolff E. Epi- 51. Osterholm MT. Preparing for the next pan-
der historisch-geographischen Pathologie.
demiologie, Ätiologie, Pathomorphologie und demic. N Engl J Med 2005; 352:1839–42.
Zweite, vollständig neue Bearbeitung. Erste
Pathogenese der Grippe. Munich: JF Berg- 52. Peiris JS, Yu WC, Leung CW, et al. Re-emer- Abtheilung. Die allgemeinen acuten Infec-
mann, 1921. gence of fatal human influenza A subtype tionskrankheiten vom historisch-geograph-
33. McIntosh J. Privy Council, Medical Research H5N1 disease. Lancet 2004; 363:617–9. ischen Standpunkte und mit besonderer Be-
Council. Studies in the aetiology of epidemic 53. Cheung CY, Poon LL, Lau AS, et al. Induc- rücksichtigung der Ætiologie. 1. Stuttgart:
influenza. London: Medical Research Coun- tion of proinflammatory cytokines in human Ferdinand Enke, 1881:5–40.
cil, 1922. macrophages by influenza A (H5N1) viruses: 68. Finkler D. Influenza. In: Stedman TL, ed.
34. French H. The clinical features of the influ- a mechanism for the unusual severity of hu- Twentieth century practice. Vol 15: Infectious
enza epidemic of 1918–19. In: Great Britain man disease? Lancet 2002; 360:1831–7. diseases. New York: William Wood, 1898:
Ministry of Health. Reports on public health 54. Garcı́a-Sastre A. Virus-host interactions: role 1–249.
and medical subjects, no. 4: Report on the of the innate antiviral response in the path- 69. Law J. Influenza in horses. In: Commissioner
pandemic of influenza, 1918–19. London: ogenicity of pandemic influenza viruses. of Agriculture. Report of the commissioner
His Majesty’s Stationery Office, 1920:66–109. Emerg Infect Dis 2006; 12:44–54. of agriculture for the year 1872. Washington,
35. Hirsch EF, McKinney M. An epidemic of 55. Neumann G, Kawaoka Y. Host range restric- DC: Government Printing Office, 1872:
pneumococcus bronchopneumonia. J Infect tion and pathogenicity in the context of in- 203–48.
Dis 1919; 24:594–617. fluenza pandemic. Emerg Infect Dis 2006; 70. Board of Health of the Health Department
36. MacCallum WG. Pathology of the pneu- 12:881–6. of the City of New York. “C”: Report of
monia following influenza. JAMA 1919; 72: 56. Kash JC, Basler CF, Garcı́a-Sastre A, et al. the epizootic influenza among horses in
720–3. Global host immune response: pathogenesis 1872–’73. In: Board of Health of the Health
37. Dick GH, Murray E. Observations on the and transcriptional profiling of type A influ- Department of the City of New York. Third
bacteriology of influenza and bronchopneu- enza viruses expressing the hemagglutinin Annual Report. April 11, 1872, to April 30,
monia. J Infect Dis 1919; 25:6–17. and neuraminidase genes from the 1918 pan- 1873. New York: D Appleton, 1873:242–91.
38. Lamb FH. Primary and post-influenzal demic virus. J Virol 2004; 78:9499–511. 71. Registrar-General [Great Britain]. Fifty-first
pneumonia: a comparison of the laboratory 57. Kobasa D, Takada A, Shinya K, et al. En- annual report of the registrar-general of
findings. JAMA 1919; 72:1133–4. hanced virulence of influenza A viruses with births, deaths, and marriages in England
PERSPECTIVE • JID 2007:195 (1 April) • 1027(1888). London: Her Majesty’s Stationery neuraminidase antibodies in man (36245). 92. Masurel N, Marine WM. Recycling of Asian
Office, 1889. Proc Soc Exp Biol Med 1972; 139:825–6. and Hong Kong influenza A virus hemag-
72. Wilson JC, Da Costa JM. Influenza. In: Wil- 82. Kendal AP, Minuse E, Maassab HF, Hen- glutinins in man. Am J Epidemiol 1973; 97:
son JC, Da Costa JM. A treatise on the con- nessey AV, Davenport FM. Influenza neu- 44–9.
tinued fevers. New York: William Wood, raminidase antibody patterns in man. Am J 93. Francis T. Influenza: the newe acquayan-
1881:10–45. Epidemiol 1973; 98:96–103. tance. Ann Intern Med 1953; 39:203–21.
73. Kusnezow ACh, Herrmann FL. Influenza: 83. Vaughan WT. Significant phenomena of 94. Saillant C-J. Tableau historique et raisonné
eine geschichtliche und klinische Studie: influenza pandemics. J Lab Clin Med des épidémies catarrhales, vulgairement dites
nach dem Russischen Bearbeitet von Dr Jos 1919–1920; 5:754–62. la grippe: depuis 1510 jusques et y compris
V Drozda. Vienna: Josef Šafář, 1890. 84. Ministry of Health [Great Britain]. Reports celle de 1780; avec l’indication des traite-
74. Symes Thompson E. Influenza or epidemic on public health and medical subjects, no. 4: ments curatifs & des moyens propres à s’en
catarrhal fever: an historical survey of past Report on the pandemic of influenza, préserver. Paris: Didot Jeune, 1780.
epidemics in Great Britain from 1510 to 1918–19. London: His Majesty’s Stationery 95. Webster N. Of the influenza, or epidemic
1890. London: Percival, 1890. Office, 1920. catarrh. In: Webster N. A brief history of
75. Creighton C. Influenza. In: Creighton C. A 85. Niven J. Report on the epidemic of influenza epidemic and pestilential diseases; with the
Downloaded from https://academic.oup.com/jid/article-abstract/195/7/1018/800918 by guest on 22 March 2020
history of epidemics in Britain. Vol 1: From in Manchester, 1918–19. In: Ministry of principal phenomena of the physical world,
AD 664 to the extinction of the plague. Cam- Health [Great Britain]. Reports on public which precede and accompany them, and
bridge: Cambridge University Press, 1891: health and medical subjects, no. 4: Report observations deduced from the facts stat-
397–413. on the pandemic of influenza, 1918–19. IV. ed. Vol II, sec XII. Hartford, CT: Hudson &
76. Creighton C. Influenza. In: Creighton C. A London: His Majesty’s Stationery Office, Goodwin, 1799:30–36.
history of epidemics in Britain. Vol 2: From 1920:471–520. 96. Schweich H. Die Influenza: ein historischer
the extinction of the plague to the present 86. Eichel O. The long-time cycles of pandemic und ätiologischer Versuch, mit einer Vorrede
time. Cambridge: Cambridge University influenza. J Am Stat Assoc 1922; 18:446–54. von Dr JFC Hecker. Berlin: Theodor Chris-
Press, 1894:300–433. 87. Hilleman MR. Realities and enigmas of hu- tian Friedrich Enslin, 1836.
77. Tarchetti P. Rivista storico-clinica delle prin- man viral influenza: pathogenesis, epidemi- 97. Thompson T. Annals of influenza, or epi-
cipali epidemie d’influenza dal secolo xvi ai ology and control. Vaccine 2002; 20:3068–87. demic catarrhal fever in Great Britain from
nostri giorni. Alessandria: G. Panizza, 1892. 88. Gaydos J, Top FH, Hodder RA, Russell PK. 1510 to 1837. London: Sydenham Society,
78. Clemow FG. Influenza. In: Clemow FG. The Swine influenza A outbreak, Fort Dix, New 1852.
geography of disease. Cambridge: Cambridge Jersey, 1976. Emerg Infect Dis 2006; 12:23–8. 98. Mills CE, Robbins JM, Lipsitch M. Trans-
University Press, 1903:187–203. 89. Oxford JS. Influenza A pandemics of the 20th missibility of 1918 pandemic influenza. Na-
79. Leichtenstern O, Sticker G. Geschichte, Ep- century with special reference to 1918: vi- ture 2004; 432:904–6.
idemiologie und Ätiologie der Influenza. In: rology, pathology, and epidemiology. Rev 99. Cheung C-L, Rayner JM, Smith GJD, et al.
Nothnagel H, ed. Spezielle Pathologie und Med Virol 2000; 10:119–33. Distribution of adamantine-resistant H5N1
Therapie: Influenza. I Teil. Vienna: Alfred 90. Kilbourne ED. Influenza pandemics of the avian influenza variants in Asia. J Infect Dis
Hölder, 1912:16–91. 20th century. Emerg Infect Dis 2006; 12:9–14. 2006; 193:1626–9.
80. Kilbourne ED. Influenza immunity: new in- 91. Holmes EC, Ghedin E, Miller N, et al. Whole 100. Gerhard W, Mozdzanowska K, Zharikova D.
sights from old studies. J Infect Dis 2006; genome analysis of human influenza A virus Prospects for a universal influenza virus vac-
193:7–8. reveals multiple persistent lineages and reas- cine. Emerg Infect Dis 2006; 12:569–74.
81. Fedson DS, Huber MA, Kasel JA, Webster sortment events among recent H3N2 viruses. 101. Luke CJ, Subbarao K. Vaccines for pandemic
RG. Presence of A/Equi-2 hemagglutinin and Plos Biol 2005; 3:e300. influenza. Emerg Infect Dis 2006; 12:66–72.
1028 • JID 2007:195 (1 April) • PERSPECTIVEYou can also read