SYSTEMIC LUPUS ERYTHEMATOSUS FOR THE PCP - Greta Bires PGY2
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

SYSTEMIC LUPUS ERYTHEMATOSUS
FOR THE PCP
Greta Bires PGY2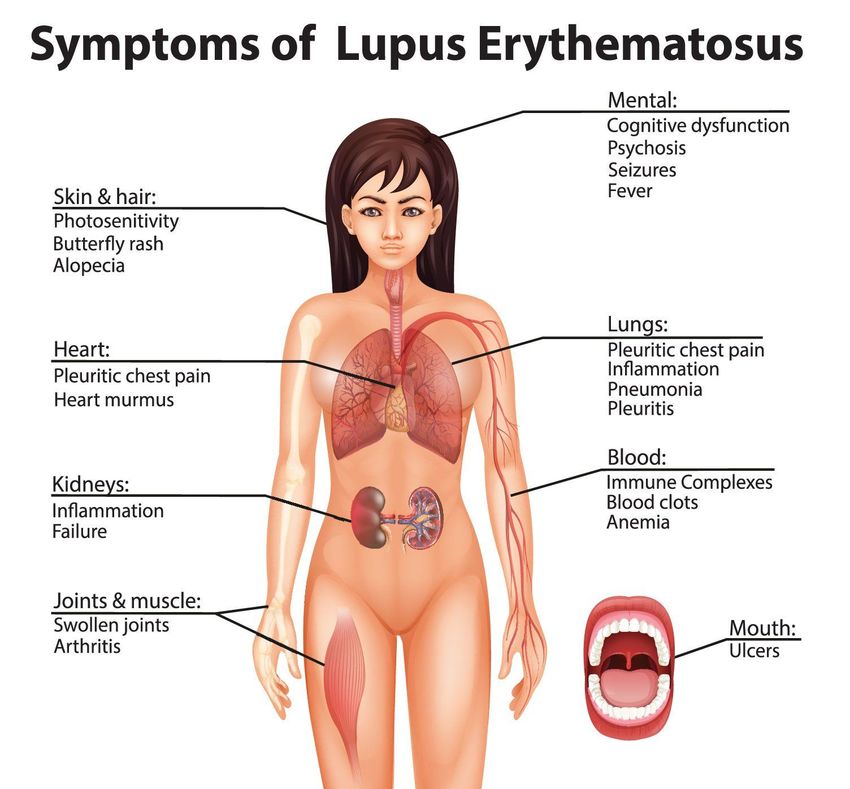
DISCLOSURES • None

• Define Systemic Lupus Erythematosus (SLE) and
understand it’s clinical manifestations and diagnosis
• Become familiar with the treatment of SLE
• Discuss SLE through the life stages including
OBJECTIVES pregnancy counseling and contraceptive use
• Discuss preventative measures for SLE patients
• Develop a better understanding of the role of PCPs
in the care of SLE patients
INSPIRATIONAL PATIENT 32-year-old with “no significant PMH” presents to the office to establish care with a routine physical exam and would also like to go on birth control. She is thinking of getting pregnant in about a year but would like to be protected until that point. She otherwise feels fine. She has intermittent pain in her knees and hands, but she takes NSAIDs and it goes away. She has no other complaints. You review her history, and she goes “oh and I have lupus, but it doesn’t really bother me”….
WHAT IS SYSTEMIC LUPUS
ERYTHEMATOSUS?
• Complex autoimmune disease with wide range of organ involvement
• Course is typically recurrent, with periods of relative remission followed by
flares
• Prevalence estimated to be 30-50 per 100,000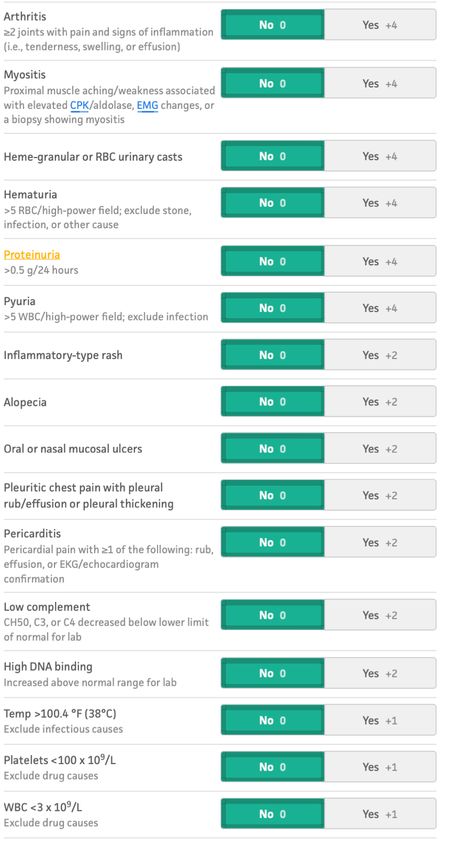
WHAT CAUSES LUPUS? • WHO KNOWS • Triggered in genetically susceptible individuals by exposure to certain environmental risk factors

WHY SHOULD I CARE • SLE patients consult their GP more frequently with relevant clinical features during 5-year period prior to diagnosis • GPs correctly diagnosis on 11% of SLE cases presented in written scenarios • Compared to the general population patients with SLE have at least a 5-fold increase in mortality • 1/3 of patients lose the ability to work within 5 years after disease onset

DOES EARLIER DIAGNOSIS MATTER? • Population based screening not advised • Average time from symptom onset to diagnosis is approximately 2 years • longer lag time for children, males, and late-onset disease • Less than 6-month delay may experience lower flare rates, less healthcare utilization, and costs than those with at least 6 months • Failure to achieve low disease activity in first 6 months after diagnosis with early damage accrual

WHO GETS LUPUS - KAHOOT
WHO GETS LUPUS? • Women in their reproductive years • More common in African Americans, Hispanics, Asian-Americans, Native Americans, Native Hawaiians, pacific islanders • Black women are 3 times more likely to develop lupus than white women • Affects 1 in 250 black women • Patients who have relatives with lupus have 5-13% chance of developing disease themselves
HEALTH DISPARITIES • Among Medicaid enrollees across the US from 2000-2004, prevalence of lupus and lupus nephritis highest in zip code areas of lower SES • Racial/ethnic minorities and low-income individuals less likely to receive recommended healthcare for lupus • Poverty associated with higher mortality and variety of poor outcomes • Low-income individuals less likely to see specialist and likely to have to travel significantly further to see one
MOST COMMON PRESENTATION –
KAHOOTWHEN TO SUSPECT LUPUS • Can affect any organ • Not all manifestations appear simultaneously • Often constitutional symptoms (esp fatigue), mucocutaneous and MSK symptoms present the earliest
CLUES ON PHYSICAL EXAM
• Younger age
• African American
• Painless mouth ulcers
• Arthralgias in hands
• Pregnancy complications
(Fidanoski, 2007)
• Rash
• Chest pain/pericardial symptoms
• Hematuria
• Chronic symptoms
(Tucker, 2019)COMMON AND
SPECIFIC
SYMPTOMS
• Common: fatigue, weight loss, fever without
focal infection
• In up to 90% patients
• Less common
• Malar rash (31%), photosensitivity (23%),
pleuritic chest pain (16%), new-onset
Raynaud phenomenon (16%), mouth
sores (12.5%)
• Strongest physical evidence that favors SLE
• Discoid rash +LR = 18
• Malar Rash +LR = 14
• Unexplained seizures or psychosis +LR
= 13
• Photosensitivity +LR = 11
(Weiss, 2019)DIAGNOSIS - KAHOOT
DIAGNOSTIC STEPS • CBC, TSH, UA • ANA • Low diagnostic specificity • Confirm specific autoantibodies • Anti-dsDNA • Anti-Sm Ab • No diagnostic criteria
CLASSIFICATION CRITERIA
• 3 sets:
• American College of Rheumatology (ACR) criteria (1997)
• Systemic Lupus Erythematosus International Collaborating Clinics (SLICC)/ACR
Criteria (2012)
• European Union League Against Rheumatism/American College of Rheumatology
Criteria (2019)
• Differ in emphasis placed on various immunologic and clinical domains(Huang et al, 2018)
E U RO P E A N U N I O N L E A G U E
A G A I N S T R H E U M AT I S M / A M E R I C A N
C O L L E G E O F R H E U M ATO L O G Y
CRITERIA (2019)
(Fanouriakis et. al, 2019)LUPUS MIMICKERS AND OVERLAP
SYNDROMES
• Autoimmune hepatitis • Sjogren’s syndrome
• Dermatomyositis • Systemic Sclerosis
• Inflammatory myopathies • Viral infections (parvovirus)
• Juvenile idiopathic arthritis • Mixed connective tissue disease
• Primary biliary cirrhosis • Systemic sclerosis
• Rheumatoid arthritis • Polymyositis/dermatomyositis
• Drug-inducedTREATMENT - KAHOOT
TREATMENT – ORGAN SPECIFIC • Hydroxychloroquine is cornerstone of treatment • Low dose glucocorticoids used to treat most manifestations • Use of immunosuppressives and cytotoxic agents depends on body system affected • Immunologic Belimumab
TREATMENT - HYDROXYCHLOROQUINE
• Protects against development of organ involvement and more severe disease
• Takes several months (about 3) to control symptoms
• 300-400mg/d– for remission consider tapering to 200mg/d
• Retinal toxicity
• Recommend dilated eye exam at baseline, at 5 years of use, and annually after 5 years
of use
• Should not be dosed more than 5mg/kg due to risk of retinal disease
• Toxicity related to dose and duration of therapy
• Retinal disease found in 1% after 5 years and sharply increases to 20% after 20 yearsFLARES AND MONITORING - KAHOOT
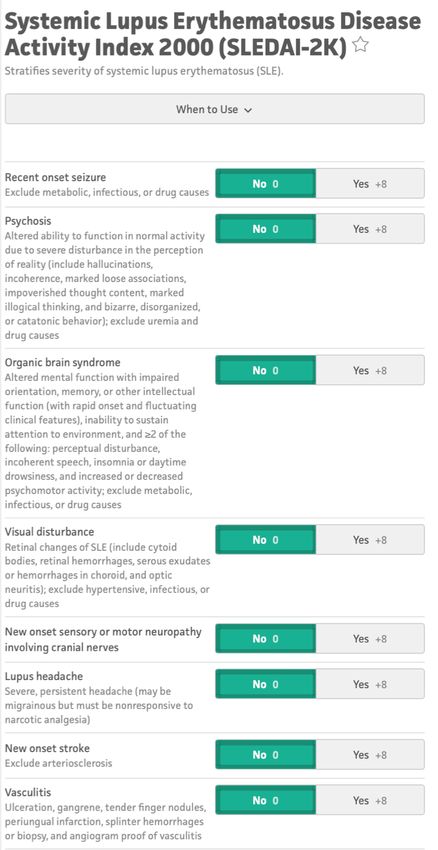
MONITORING OF FLARES
• Disease activity:
• anti-dsDNA
• complements (C3, C4)
• creatinine/RFP
• CBC
• UA/Urine protein analysis
• Every 3-6 months
(Gladman, 2021)
• SLEDAI-2K scoreINSPIRATIONAL PATIENT 32-year-old with “no significant PMH” presents to the office to establish care with a routine physical exam and would also like to go on birth control. She is thinking of getting pregnant in about a year but would like to be protected until that point. She otherwise feels fine. She has intermittent pain in her knees and hands, but she takes NSAIDs and it goes away. She has no other complaints. You review her history, and she goes “oh and I have lupus, but it doesn’t really bother me”….
PREGNANCY COUNSELING - KAHOOT
PREGNANCY IN LUPUS • NOT associated with decreased fertility • A lot of medications are teratogenic • Up to 1/3 require C-section • Up to 1/3 with preterm birth • Increased risk of Preeclampsia, gestational diabetes mellitus, infection • Major risk factors for adverse maternal and fetal outcomes: • active/flaring disease (particularly active lupus nephritis) • history of lupus nephritis • presence of antiphospholipid Ab/antiphospholipid syndrome
PREGNANCY COUNSELING
• Plan pregnancy – delay conception until at least 6 months remission (6-12m)
• Off risky medications
• Teratogenic: cyclophosphamide, ACEi, ARBs, warfarin, methotrexate, mycophenolate
mofetil
• Continue important medications: hydroxychloroquine, azathioprine,
corticosteroids when appropriate
• Low dose ASAANTIPHOSPHOLIPID SYNDROME
• Associated with autoantibody having an apparent specificity for negatively charged
phospholipids with venous thrombosis, arterial thrombosis, and/or pregnancy loss
• Antiphospholipid AB present in 1/3 lupus patients
• 1/3 of those will have ≥1 clinical manifestation
• Consider if
• ≥1 unexplained death at ≥10 weeks gestation
• ≥ 1 preterm birth (< 34wk gestation) due to severe preE, eclampsia, or placental
insufficiency
• ≥3 consecutive miscarriages < 10-week gestationCONTRACEPTION - KAHOOT
CONTRACEPTION
(CDC, 2020)NEONATAL COMPLICATIONS
• Anti-Ro and Anti-La
• Cutaneous features: annular erythematous rash (Sechi et. Al, 2020)
• Often photosensitive
• Transient
• Cardiac disease: 1-3rd degree heart block
• May be permanent and require pacing
(Haebich et al, 2015)• 15-20% of SLE presents in childhood
• Hormonal influence on presentation (rare• Onset 50+
• 5-15% of all lupus patients
• Still predominantly women, higher percentage whites
• Drug-induced should be ruled out
• Incidence of false positive ANA increases with age
LATE ONSET LUPUS • Characteristics
• Reduced likelihood of proteinuria, cellular casts, and
seizures
• Reduced prevalence of anti-RNP, anti-Sm, and anti-
dsDNA ab
• Low complement levels
• Lower levels of disease activityINSPIRATIONAL PATIENT 32-year-old with “no significant PMH” presents to the office to establish care with a routine physical exam and would also like to go on birth control. She is thinking of getting pregnant in about a year but would like to be protected until that point. She otherwise feels fine. She has intermittent pain in her knees and hands, but she takes NSAIDs and it goes away. She has no other complaints. You review her history, and she goes “oh and I have lupus, but it doesn’t really bother me”….
COMORBIDITY - KAHOOT
• Frequently have a variety of comorbidities
• Males have higher rates cardiovascular disease/stroke and cancer
• Female patients have higher rates infection and osteoporosis
• Prevalence:
• Dyslipidemia 36% at diagnosis to 60% after 3 years
SLE MULTI- • Diabetes 2.7-7% and increases over time to 14%
MORBIDITY • Obesity in 1/3 patients
• Most common cause of death in SLE patients
AND • Heart disease and stroke (1.7x general population)
MORTALITY • Hematologic malignancies and lung cancer (2.1x general
population)
• Infection (5x general population)
• Renal disease (7.9x general population)ACCELERATED ATHEROSCLEROSIS • Atherosclerotic events among leading causes of mortality in lupus patients • Rate of MI 50-fold higher in 35–44-year-olds • 1st cardiac event occurs at ≤55 in more than 2/3 patients • Vasculitis extremely rare • Control modifiable risk factors: blood pressure, glucose, tobacco exposure, cholesterol, sedentary lifestyle at young ages • EKG and stress test when indicated based on history and exam • Value of statins tests in RCTs which failed to show clear benefit over placebo • Low dose ASA may be considered for primary prevention of CVD
PREVENTATIVE MEASURES – SMOKING
CESSATION
• Smoking triggers SLE onset
• HR 1.86 of more than 10 pack year smoking with SLE risk
• Smoking cessation reduces risk to that of nonsmokers
• Smoking increases cutaneous manifestations, flares, organ damage
• Worse therapeutic results
• Interferes with efficacy of anti-malarials
• Raises pulmonary pressures
• Associated with greater degree of inflammatory arthritis
• Worsens Raynaud'sPREVENTATIVE MEASURES – WEIGHT
CONTROL
• Increased weight leads to decreased functional capacity, more fatigue, increased
risk metabolic syndrome
• Physical activity hard secondary to joint pain, osteoporosis, neuropathy but can
enhance quality of life
• Improved pulmonary function
• Diminishes fatigue
• Increases endurance
• Increased BMI associated with poorer prognosisPREVENTATIVE MEASURES -
IMMUNIZATIONS
• Pneumococcus and influenza
• Live virus vaccines are contraindicated when patient receiving
immunosuppressive treatment
• Including prednisolone at dose >20mg/day
• SLE itself is NOT a contraindication
• Avoid in patients on mycophenolate, cyclophosphamide, other immunosuppressive
medications
• Patients as young as 40 may benefit from herpes zoster vaccines
• Give HPVPREVENTATIVE MEASURES – BONE
DENSITY
• Females with lupus are nearly 5x more likely to experience fracture from
osteoporosis
• Recommend adequate Ca and vitamin D intake and weight bearing activity for
patient on chronic prednisone
• Vitamin D has been postulated to be an environmental trigger for autoimmune diseases
• ≥3 months of prednisolone (2.5mg/d)
• elemental Ca (1000-1200 mg/d)
• cholecalciferol (600-800 IU/d)
• Patients on chronic high dose steroids (>20mg prednisone) or with history of
fractures warrant more aggressive monitoringPREVENTATIVE MEASURES – CANCER
SCREENINGS
• Overall risk of cancer 10-15% higher than the general population
• Increased risk of non-Hodgkin’s Lymphoma (3-4x) compared to general
population
• Lack of studies comparing enhanced cancer screening in lupus patients
• Recommendation for the same screening as the general population
• Potentially enhanced screening for cervical dysplasia/cancer especially in those
who received high potency immunosuppressive therapyPREVENTATIVE MEASURES - OTHER
• Sun protection
• SPF 30 absorbs/reflects 97% UV light
• use 30 or above 30 minutes before going out into sun to all exposed body parts
and reapply after 1-2 hours
• Avoidance of unnecessary sun exposure remains most important behavioral
modification
• Hats, protective clothing, and umbrellas are blocking
• No evidence for anti-inflammatory dietWHEN TO REFER • All SLE patients should have a Rheumatologist • When physical exam is not suggestive of clinically overt disease and lab tests show only isolated low-titer positive ANA
SUMMARY • SLE is a complex autoimmune disease with a wide spectrum of organ involvement and presentation • Classic presentation is women in reproductive years • Initial work up: CBC, TSH, UA • High sensitivity test: ANA • High Specificity test: anti-dsDNA • Flares: anti-dsDNA, C3, C4, CBC, Up:cr, UA, RFP • Treatment: hydroxychloroquine, glucocorticoids, immunosuppressants
SUMMARY • 6-12m of disease control before pregnancy and need MFM involvement • Copper IUD is best form of contraception unless severe thrombocytopenia • Avoid the patch • SLE patients often have accelerate atherosclerosis • Preventative measures including: • UV protection • Smoking cessation • Bone density monitoring • Immunizations • Cancer screenings • Blood pressure, lipid, BMI monitoring
(Huang et al, 2018)
THANK YOU! Questions?
REFERENCES 1. #171 Lupus in Primary Care with Beth Jonas MD. The Curbsiders. Published September 9, 2019. Accessed March 1, 2021. https://thecurbsiders.com/podcast/171-lupus 2. 10 Challenges in Treating Lupus. Rheumatology Network. Accessed March 1, 2021. https://www.rheumatologynetwork.com/view/10-challenges-treating-lupus 3. Fanouriakis A, Kostopoulou M, Alunno A, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis. 2019;78(6):736-745. doi:10.1136/annrheumdis-2019-215089 4. Haebich G, Blackford S, Lygas A. A neonate with a rash. BMJ. 2015;350(feb13 1):h452-h452. doi:10.1136/bmj.h452 5.Choi MY, Flood K, Bernatsky S, Ramsey-Goldman R, Clarke AE. A review on SLE and malignancy. Best Practice & Research Clinical Rheumatology. 2017;31(3):373-396. doi:10.1016/j.berh.2017.09.013 6. Sechi A, Patrizi A, Cangemi J, Galletti S, Neri I. Congenital onset of neonatal lupus erythematosus. Archives of Disease in Childhood - Fetal and Neonatal Edition. 2020;105(4):356-356. doi:10.1136/archdischild-2020-319172 7. Wallace DJ. Improving the prognosis of SLE without prescribing lupus drugs and the primary care paradox. Lupus. 2008;17(2):91-92. doi:10.1177/0961203307086267 8. Tucker, Rod. Is it sunburn, rosacea or systemic lupus erythematosus. BJFM. Published July 2019. Accessed March 1, 2021. https://www.bjfm.co.uk/you-re-the-doctor-a-case-of-sunburn-rosacea-or-systemic-lupus-erythematosus 9.. Ludici M, Fasano S, Gabriele Falcone L, et al. Low-dose aspirin as primary prophylaxis for cardiovascular events in systemic lupus erythematosus: a long-term retrospective cohort study. Rheumatology. 2016;55(9):1623-1630. doi:10.1093/rheumatology/kew231 10. D’Arrigo T. Lupus presentation may be an ‘imitator.’ Accessed March 1, 2021. https://acpinternist.org/archives/2014/11/lupus.htm 11. Donald Thomas. Lupus update for Primary Care Providers 2014. Health & Medicine presented at the: 14:10:42 UTC. Accessed March 1, 2021. https://www.slideshare.net/LupusEncyclopedia/lupus-update-for-primary-care-providers-2014 12. Management of Systemic Lupus Erythematosus (SLE). Accessed March 1, 2021. https://www.dynamed.com/management/management-of-systemic-lupus-erythematosus-sle 13. Dörner T, Furie R. Novel paradigms in systemic lupus erythematosus. The Lancet. 2019;393(10188):2344-2358. doi:10.1016/S0140-6736(19)30546-X 14. Mina R, Brunner HI. Pediatric Lupus—Are There Differences in Presentation, Genetics, Response to Therapy, and Damage Accrual Compared with Adult Lupus? Rheumatic Disease Clinics of North America. 2010;36(1):53-80. doi:10.1016/j.rdc.2009.12.012 15. Mina and Brunner - 2010 - Pediatric Lupus—Are There Differences in Presentation.pdf. Accessed March 1, 2021. https://thelupusinitiative.org/slides/pdf/PP_Lifespan.pdf 16. PP_HealthDisparities.pdf. Accessed March 1, 2021. https://thelupusinitiative.org/slides/pdf/PP_HealthDisparities.pdf
REFERENCES 17. PP_Morbidity.pdf. Accessed March 1, 2021. https://thelupusinitiative.org/slides/pdf/PP_Morbidity.pdf 18. PP_Overview.pdf. Accessed March 1, 2021. https://thelupusinitiative.org/slides/pdf/PP_Overview.pdf 19. Reproductive Health Considerations in Women with Systemic Lupus Erythematosus (SLE). Accessed March 1, 2021. https://www.dynamed.com/management/reproductive-health-considerations-in-women-with-systemic-lupus-erythematosus-sle 20. Rheum2Learn Systemic Lupus Erythematosus. Accessed March 1, 2021. https://www.rheumatology.org/Learning-Center/Educational-Activities/Rheum2Learn/Systemic-Lupus-Erythematosus 21. Summary Chart of U.S. Medical Eligibility Criteria for Contraceptive Use .pdf. Accessed March 1, 2021. https://www.cdc.gov/reproductivehealth/contraception/pdf/summary-chart-us-medical-eligibility-criteria_508tagged.pdf 22. Petri M. Systemic Lupus Erythematosus.pdf. Accessed March 1, 2021. https://www.acog.org/-/media/project/acog/acogorg/clinical/files/clinical-updates/2020/07/systemic-lupus-erythematosus.pdf 23. Systemic Lupus Erythematosus (SLE). Accessed March 1, 2021. https://www.dynamed.com/condition/systemic-lupus-erythematosus-sle 24. Systemic Lupus Erythematosus (SLE) | CDC. Published October 18, 2018. Accessed March 1, 2021. https://www.cdc.gov/lupus/facts/detailed.html 25. Gladman, Dafna. Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K). MDCalc. Accessed March 3, 2021. https://www.mdcalc.com/systemic-lupus-erythematosus-disease-activity-index-2000-sledai-2k 26. Gergianaki I, Bertsias G. Systemic Lupus Erythematosus in Primary Care: An Update and Practical Messages for the General Practitioner. Front Med. 2018;5:161. doi:10.3389/fmed.2018.00161 27. Boban Fianoski. Systemic Lupus Erythematosus-Oral Manifestations and adverse effects of Lupus in oral cavity. Published August 2007. Accessed March 3, 2021. http://www.fidanoski.ca/sle/ 28. Lam N-C, Ghetu MV, Bieniek ML. Systemic Lupus Erythematosus: Primary Care Approach to Diagnosis and Management. AFP. 2016;94(4):284-294. 29. Department of Medicine, Tuen Mun Hospital, Tuen Mun, Hong Kong, Mok C. Systemic lupus erythematosus: what should family physicians know in 2018? Hong Kong Med J. Published online September 28, 2018. doi:10.12809/hkmj187319
You can also read