Surgical Treatment of Type 2 Diabetes: Do Surgeons have a Better Treatment? John Bantle, MD - Department of Medicine
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Surgical Treatment of Type 2
Diabetes:
Do Surgeons have a Better Treatment?
John Bantle, MD
Division of Endocrinology and Diabetes
Department of Medicine
University of Minnesota
Disclosure Information
I have no financial relationship to disclose.
I will not discuss off label or investigational
product use in my presentation.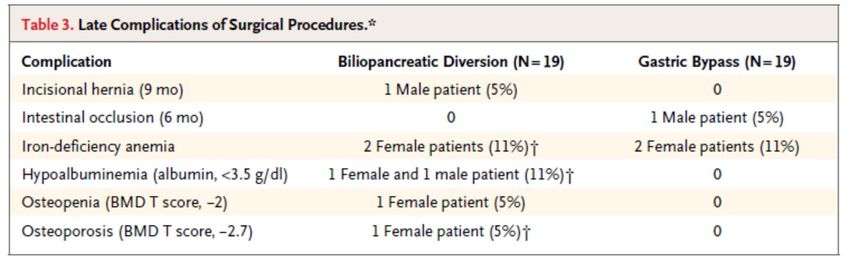
Goals of Presentation
• To review expected weight loss with medical
and surgical treatments.
• To describe the bariatric procedures in
current use.
• To summarize the effects of bariatric surgery
on type 2 diabetes.
• To review potential adverse outcomes of
bariatric surgery.
Natural History of Type 2 Diabetes
350
Postmeal Glucose
Glucose (mg/dL)
300
250
Fasting Glucose
200
150
100
50
Relative Function (%)
250
200 Insulin Resistance
150
100
Prediabetes (IFG, IGT) Clinical Diagnosis
50 -Cell Function
0
-10 -5 0 5 10 15 20 25 30
Onset of
Diabetes Years
Adapted from: Simonson GD, Kendall DM. Coron Artery Dis. 2005;16(8):465-472.
To Avoid Type 2 Diabetes • If you are lean, try to stay lean. • If you are overweight, try to lose weight.

“To lengthen thy life, lessen thy meals” Benjamin Franklin 1733 “and quicken thy heart with exercise”



Action for HEAlth in Diabetes
(Look AHEAD)
• NIH sponsored clinical trial of lifestyle modification
to reduce CV events in type 2 diabetic subjects.
• Random assignment to an intensive lifestyle
intervention or a program of diabetes support and
education (control group).
• 5,145 subjects randomized
• Multicenter
• All participants continued to receive diabetes care
from their own physicianIntensive Lifestyle Intervention
(ILI) Group
Structured hypocaloric, low fat diet
Regular use of meal replacements
Regular exercise (goal 175 minutes per week)
Behavioral components
Weekly group or individual sessions months 1-6, frequent
subsequent contact
Toolbox including orlistat as rescue strategy
Refresher courses and campaigns
Goal to achieve 7% average weight loss in the first 6
months and maintain it thereafterFour Year Results
(Averaged Across All 4 Years)
Arch Intern Med 2010;170:1566
ILI Control P value
Weight loss (% initial) -6.2* -0.9* < 0.001
Fitness gain (METS) +12.7 +2.0 < 0.001
Hb A1c (%) -0.4 -0.1 < 0.001
Systolic BP (mmHg) -5 -3 < 0.001
LDL chol (mg/dl) -11 -13 0.009
HDL chol (mg/dl) +4 +2 < 0.001
Triglycerides (mg/dl) -26 -20 < 0.001
* At 4 years, weight change was -4.7% and -1.1%, respectivelyWhy is Wight Loss so Difficult for Most People to Accomplish? Probably because each of us has a body weight that our hypothalamus works to maintain. This weight may be defended as is, for instance, body temperature. 1) Deficient caloric intake compensated for by decrease in metabolic rate and decrease in physical activity. 2) Excess caloric intake suppresses appetite, some calories dissipated as heat.
Biochemistry of Energy Regulation Leptin: produced in adipose tissue, circulates in proportion to body adiposity. Insulin: circulates in proportion to body adiposity. Neuropeptide Y: potent stimulator of food intake, increases during fasting, inhibited by leptin. Agouti-Related Protein: stimulates appetite. Ghrelin: signals hunger, increases food intake. Peptide YY: signals satiety, decreases food intake, inhibits gut motility. Glucagon-Like Peptide 1: increases satiety.
Bariatric Surgery
Jejunoileal Bypass for Morbid Obesity:
Late Follow-up in 100 Cases
Hocking MP, et al. N Engl J Med 1983;308:995-9.
Results from 100 patients who underwent jejunoileal
bypass and had 5 or more years of follow-up.
Procedure: end-to-side anastomosis of the jejunum 30 cm
from the ligament of Treitz to the ileum 10 cm from the
ileocecal valve.
Mean weight loss at 5 years was 46.6 kg.
Complications (n): progressive hepatic abnormalities (29),
cirrhosis (7), nephrolithiasis (21), cholelithiasis (14),
chronic diarrhea (58), chronic hypokalemia (33).
The investigators abandoned the procedure.Bariatric Surgical Procedures
in Current Use
1) Vertical banded gastroplasty
2) Laparoscopic gastric banding
3) Roux-en-Y gastric bypass
4) Biliopancreatic diversion with
duodenal switch
5) Sleeve gastrectomyMeta-analysis: Surgical Treatment of
Obesity
Maggard MA, et al. Ann Intern Med 2005;142:547-59.
Meta-analysis of 147 studies of bariatric surgery for
obesity.
Weight loss 12 months > 36 months
Gastric banding 30.2 kg 34.8 kg
Gastric bypass 43.5 kg 41.5 kg
Duodenal switch 51.9 kg 53.1 kgMaggard MA, et al (continued) Mortality < 30 Days > 30 days Gastric banding 0.02 % 0.1 % Gastric bypass 0.3 % 0.6 % Duodenal switch 0.9 % 0.3 % Adverse Events All GI* Other+ Gastric banding 7.0 % 13.2 % Gastric bypass 16.9 % 18.7 % Duodenal switch 37.7 % ?# ------------------------------------------------------------------------------------------------ * Including reflux, vomiting, dysphagia, dumping syndrome and others. + Including anastomotic leak, stenosis, bleeding, need for reoperation and others. # Not reported in all categories.
Lifestyle, Diabetes and Cardiovascular Risk Factors 10 Years after Bariatric Surgery Sjostrom L, et al. N Engl J Med 2004;351:2683-93. 641 Swedish obese subjects who chose to undergo bariatric surgery compared to 647 control subjects who received nonsurgical treatment for obesity as was customary at their medical center. Subjects in the two groups were matched on 18 variables including gender, age, weight, height, systolic BP and diabetes status. After 10 years, weight changes were: control group +1.6+12%, gastric banding group -13+13%, vertical banded gastroplasty group -16+11% and gastric bypass group -25+11% (control vs. surgery, p
Sjostrom L, et al (continued)
Control Surgery P Value
Group Group
Recovery from pre-
existing diabetes 13% 36% 0.001
Incidence of new
diabetes 24% 7%Effects of Bariatric Surgery on Mortality in
Swedish Subjects
Sjostrom L, et al. N Engl J Med 2007;357:741-52.
Overall mortality of 4047 Swedish obese subjects
during an average follow-up of 10.9 years
reported.
129 (6.3%) subjects in the control group and 101
(5.0%) subjects in the surgical group died.
Hazard ratio for surgical group was 0.76 when
compared to the control group (95% CI 0.59 to
0.99, p=0.04).
Most common causes of death were MI (control
25, surgery 13) and cancer (control 47, surgery
29).Long-Term Mortality after Gastric Bypass
Surgery
Adams TD, et al. Engl J Med 2007;357:753-61
Retrospective cohort study comparing 7,925
patients who underwent gastric bypass surgery
for obesity to 7,925 obese subjects who applied
for driver’s licenses; matching based on gender,
age and BMI.
During mean follow-up of 7.1 years, adjusted
mortality in the surgery group decreased by 40%
as compared to the control group (37.6 vs. 57.1
deaths per 10,000 person years, pPories, W.J., et al., Who would have thought it? An operation proves to be the most effective therapy for adult‐onset diabetes mellitus. Ann Surg, 1995. 222(3): p. 339‐50; discussion 350‐2.
Porries WJ, et al (continued)
Long-term follow-up of 608 patients who underwent
open gastric bypass
n Mean Mean BMI
Weight (kg) (kg/m2)
Pre-op 608 138.4 49.7
1 year 506 87.4 31.5
5 years 317 93.4 33.7
10 years 158 93.7 34.7Porries WJ, et al (continued) 121 of 146 (83 %) patients with diabetes developed and maintained normal blood glucose and A1c without medications. Complications: Perioperative mortality 1.5 % Reoperation 2.8 % Wound infections 8.7 % Anastomotic stenosis 3.0 % Splenic tears 2.5 % Subphrenic abscess 2.5 % Incisional hernia 24 % B12 deficiency 40 % Anemia 39 % Cholelithiasis 11 % Hypoglycemia 5.7 %
Weight and Type 2 Diabetes After
Bariatric Surgery: Systematic Review and
Meta-analysis
Buchwald H, et al. Am J Med 2009;122:248-56.
Meta-analysis of 621 studies published between 1/1/1990
and 4/30/2006; 73% single arm and 58%
retrospective.
135,246 patients; 22.3% (30,160 patients) had diabetes.
Mean weight loss < 2 years 36.6 kg; > 2 years 41.6 kg.
Diabetes resolution (no diabetes meds, A1c < 6.0% and/or
fasting glucoseBuchwald H, et al (continued) Overall 30 day or less mortality was 0.28% “The available information on nonfatal adverse effects of the bariatric surgery procedures is so heterogeneous, sparse and poorly reported that it does not allow… meaningful review.”
Mechanisms of Improvement 1. Reduced need for glucose disposal 2. Weight loss induced increase in insulin sensitivity 3. Weight loss induced decreases in lipotoxicity and inflammation 4. Changes in gut hormones (increases in GLP-1 and peptide YY, decrease in ghrelin)
Randomized Clinical Trials
Adjustable Gastric Banding and Conventional Therapy
for Type 2 Diabetes: A Randomized Controlled Trial
Dixon JB, et al. JAMA 2008;299:316-323.
60 obese (BMI 30-40 kg/m2) patients with diabetes of less than 2
years duration randomly assigned to conventional therapy or
laproscopic adjustable gastric banding.
Conventional therapy included lifestyle modification with
structured low fat diet, 200 minutes physical activity per week,
contact every 6 weeks, and diabetes and weight loss
medications (no GLP-1 mimetics).
Baseline A1c values: Conventional 7.6%, Surgery 7.8%.
Follow-up lasted 2 years.
Dropouts: 4 Conventional therapy patients and 1 Surgery patient.Dixon: Outcomes at 2 Years
Conventional Surgery P value
Weight loss 1.5 + 5.4 21.1 + 10.5 < 0.001
(kg)
Hb A1c (%) 7.2 + 1.4 6.0 + 0.8 < 0.001
Glucose 140 + 38 106 + 30 0.002
(mg/dl)
Insulin (uU/ml) 24 + 14 10 + 5 < 0.001Dixon, et al (cont.) • 73 % (22/30) of Surgery and 13% (4/30) of Conventional patients achieved remission of diabetes. • Amount of weight loss, not the method, was related to remission of diabetes. • Diabetes medication use was less in Surgery than Conventional patients (4 vs 28 patients). • There were no serious complications in either group.
Bariatric Surgery versus Intensive Medical
Management in Obese Patients with Diabetes
Schauer PJ, et al. New Engl J Med 2012;366:1567-76.
150 obese (BMI 27-43 kg/m2) patients with type 2 diabetes and
Hgb A1c > 7.0% randomly assigned to intensive medical
therapy or gastric bypass or sleeve gastrectomy.
Conventional therapy included lifestyle counseling for weight loss
and all approved diabetes medications.
Primary endpoint: percentage of patients with Hgb A1c < 6.0%
(with or without medications).
Follow-up lasted 1 year.
Dropouts: 9 conventional therapy and 1 sleeve gastrectomy
patients.Schauer: Outcomes at 1 Year
Medical Gastric Sleeve
Therapy Bypass Gastrectomy
Weight Loss 5.2+7.7% 27.5+7.3%* 24.7+6.6%*
A1c < 6.0% 5 of 41 21 of 50* 18 of 49*
(12%) (42%) (37%)
* p < 0.01 vs Medical TherapyBariatric Surgery versus Conventional Medical
Therapy for Type 2 Diabetes
Mingrone G, et al. N Engl J Med:366:1577-85.
60 obese (BMI > kg/m2) patients with type 2 diabetes for at least
5 years and Hgb A1c > 7.0% randomly assigned to
conventional medical therapy or gastric bypass or
biloipancreatic diversion.
Conventional therapy included lifestyle modification and
diabetes medications as necessary.
Primary endpoint: diabetes remission.
Follow-up: 2 years.
Dropouts: 2 conventional therapy, 1 gastric bypass and 1
biliopancreatic diversion patients.Mingrone: Outcomes at 2 Years
Medical Gastric Biliopancreat
Therapy Bypass Diversion
Weight Loss 4.7+6.4% 33.3+7.9%* 33.8+10.2%*
Remission 0 of 20 15 of 20* 19 of 20*
of Diabetes (75%) (95%)
* p < 0.001 vs Medical TherapyDiabetes Surgery Study (DSS) Multicenter clinical trial comparing gastric bypass surgery to intensive medical management in people with type 2 diabetes. Participating centers: University of Minnesota, Columbia University, Mayo Clinic and University of Taiwan. 120 type 2 diabetic volunteers have been randomly assignment to treatment arm.
DSS (continued) Primary endpoint: composite of A1c < 7.0%, LDL cholesterol < 100 mg/dl and systolic BP < 130 mmHg.
Postoperative Management After
Bariatric Surgery
• Intake of 60-120 g protein daily
• After gastric bypass and duodenal
switch, supplementation with:
Multivitamin with folate and thiamine
Iron
Vitamin B12
Calcium
Vitamin DSuggested Schedule for Postoperative Monitoring(1)
Preop 1m 3m 6m 12 m 18 m 24 m Annual
CBC, LFTs, glucose, x x x x x x x x
creatinine, electrolytes
Ferritin x x x x x x
Albumin x x x x x x
Folate x x x x x x
Vitamin B1 x x x x x x x
Vitamin B12 x x x x x x
Calcium, PTH, 25-OH D x x x x x x
DEXA x x x x
(1) Heber D, et al. Endocrine and Nutritional Management of the Post-Bariatric Surgery Patient:
An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2010;95:4823.DAVID 50 year old man who had undergone roux-en- Y gastric bypass for obesity. Preoperative weight was 140.5 kg and BMI 41.2 kg/m2. Following surgery, he lost 46 kg. Two years after surgery, he started having episodes of transient loss of consciousness for which no explanation could be found.
David Test Results
High Carb Meal Low Carb Meal
Glucose Insulin Glucose Insulin
(mg/dl) (uU/L) (mg/dl) (uU/L)
Fasting 93 5 92 9
30 min 228 541 92 24
60 min 48 196 94 17
90 min 28 50 95 10
120 min 69 20 91 8
180 min 86 10 88 7Post-Gastric Bypass
Hyperinsulinemic Hypoglycemia
First described by GJ Service and colleagues (N Engl
J Med 2005;353:249-54).
Six patients with postprandial neuroglycopenia after
gastric bypass.
Mechanistic possibilities:
1) Rapid absorption of ingested nutrients coupled
with failure to adaptively decrease insulin secretion
after gastric bypass-induced weight loss.
2) Increase in beta cell mass post-gastric bypass
induced by increased GLP-1 or other beta cell
trophic peptides.Hyperinsulinemic Hypoglycemic
Developing Late After Gastric Bypass
Bantle JP, et al. Obesity Surgery 2007:592-94.
Diagnostic criteria:
1) Postprandial hypolycemia with
neuroglycopenia developing > 1 year after
gastric bypass,
2) Spontaneous correction of hypoglycemia,
3) Normal fasting glucose and serum insulin,
4) Hyperinsulinemia at the time of
hypoglycemia or, after a mixed meal,
plasma glucose < 50 mg/dl and serum
insulin > 50 uU/L.Treatment of Post Gastric Bypass Hyperinsulinemic Hypoglycemia • Low carbohydrate diet • Acarbose with meals containing carbohydrate • Glucose tablets (1 or 2) at first symptoms of hypoglycemia • Feeding through gastrostomy tube placed in remnant stomach • Partial pancreatectomy • Reversal of gastric bypass
Conclusions on Bariatric Surgery for Diabetes
Potential Benefits of Bariatric Surgery • Weight loss: Duodenal Switch > Gastric Bypass > Laparoscopic Gastric Banding • Reduced need for medications • Improved diabetes control • Remission of diabetes • Improvements in blood pressure, blood lipids, sleep apnea, osteoarthritis, quality of life • Reduced long-term mortality
Potential Risks of Bariatric Surgery
• Perioperative (early) mortality rate of 0.02 - 0.9%
• Anastomotic leaks
• Wound infections
• Thromboembolic events
• Pneumonia
• Late complications including nausea, vomiting,
anastamotic ulcers, internal hernias, gallstones,
oxalate nephropathy, dumping syndrome,
nutritional deficiencies (iron, calcium, vitamins
B1, B12, D) and, perhaps, hypoglycemiaNIH Consensus Development Panel Statement on Bariatric Surgery for Diabetes* Should be considered only in people: 1) who are motivated and well informed, 2) in whom the operative risks are acceptable, and 3) with BMI > 35 kg/m2. Surgery should be performed by a surgeon with substantial experience in obesity surgery. -------------------------------------------------------------- * National Institutes of Health Consensus Development Panel. Gastointestinal surgery for severe obesity. Ann Intern Med 1991;115:956.
My Conclusions Bariatric surgery should be considered in type 2 diabetic patients with BMI > 35 kg/m2; patients with BMI 30-35 kg/m2 may also benefit but this has not been established. Laparoscopic gastric bypass is the preferred procedure. The earlier surgery is done the better; remission of diabetes is predicted by short duration of diabetes, need for few diabetes medications and high postprandial C- peptide.
Thanks For Your Attention
You can also read