STEMI ASSOCIATED WITH SARS-COV-2 INFECTION AND THE USE OF ECMO AS A POTENTIAL THERAPEUTIC APPROACH IN ADDITION TO THE PCI - OXFORD ACADEMIC JOURNALS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Oxford Medical Case Reports, 2021;3,82–85
doi: 10.1093/omcr/omaa148
Case Report
CASE REPORT
STEMI associated with SARS-CoV-2 infection and the
Downloaded from https://academic.oup.com/omcr/article/2021/3/omaa148/6161395 by guest on 30 November 2021
use of ECMO as a potential therapeutic approach in
addition to the PCI
Tanvir Rahman∗,† , Quazim A. Alayo, Sibgha G. Chaudhary,
Reihaneh C. Moghadam, Matthew L. German, Neil A. Ettinger,
Jeremy E. Leidenfrost, Hope A. Cranston-D’amato, Morton R. Rinder and
Julianne E. Donnelly
St. Luke’s Hospital, Chesterfield, MO, USA
∗ Correspondence address. St. Luke’s Hospital, Chesterfield, MO 63017, USA. Tel: +1 636-253-1232; E-mail: tanvir.rahman@stlukes-stl.com
Abstract
A 55-year-old male presented to the emergency department with the complaints of chest pain that started 4 h before
presentation. Pain was located over the anterior chest, 5 out of 10 intensity, with radiation to the left arm. Chest x-ray on
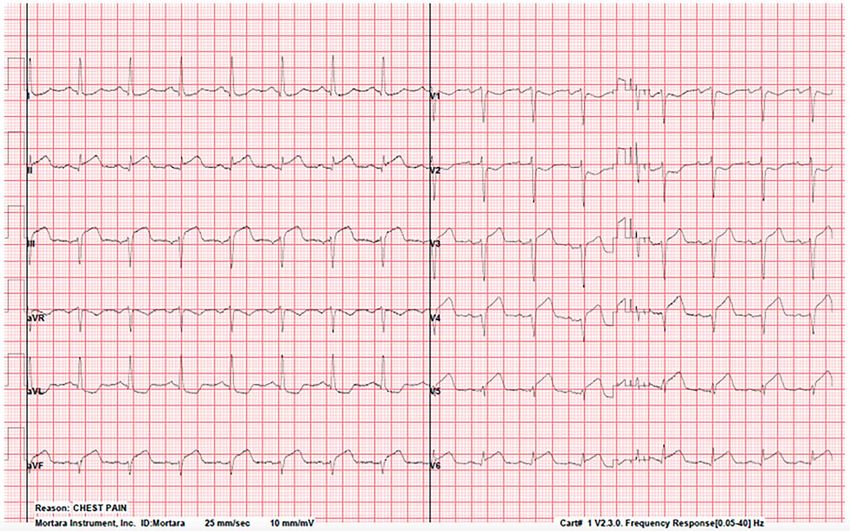
admission showed severe diffuse bilateral pulmonary infiltrates concerning for COVID-19 pneumonia. Electrocardiogram
showed inferior and lateral ST-segment elevation compatible with acute inferolateral myocardial infarction. Successful
percutaneous coronary intervention (PCI) of the proximal and mid-right coronary artery using the balloon angioplasty and
drug-eluting stent was performed. Post-PCI stenosis was 0% with a thrombolysis in myocardial infarction (TIMI) f low of 3.
Five-day course of azithromycin and hydroxychloroquine was completed with no improvement overall. Patient received two
doses of 400 mg of tocilizumab intravenously on hospital days 5 (HD#5) and #6. The patient was proned, on FiO2 100%, PEEP
15 cm H2 O, on epoprostenol sodium and paralytics and eventually received venovenous ECMO, which improved outcome.
INTRODUCTION chest pain that started 4 h before presentation. Pain was 5
out of 10 in intensity, with radiation to the left arm, and no
Thrombosis with severe acute respiratory syndrome coronavirus
associated shortness of breath (SOB). He also reported a 2-week
infection has been reported in the past [1], which is believed to be
history of dry cough and fever. Patient is a police officer, and two
caused from exaggerated cytokine response from the viral infec-
of his coworkers tested positive for SARS-CoV-2 infection. Past
tion. Here, we present a case with severe acute respiratory syn-
medical history significant for hypertension, hyperlipidemia,
drome coronavirus −2 (SARS-CoV-2) infection presenting with
coronary artery disease (CAD) status post-percutaneous coro-
right coronary artery (RCA) thrombosis.
nary intervention (PCI) with drug-eluting stent (DES) in 2005
and coronary artery bypass graft × 4 in 2008, untreated type
CASE REPORT II diabetes mellitus and polycythemia. Differential diagnosis
A 55-year-old male presented to the emergency department in included acute coronary syndrome, acute pulmonary embolism,
April 2020, with the complaints of sudden-onset, left-anterior pneumonia due to corona virus disease-2019 (COVID-19), acute
† Tanvir
Rahman, http://orcid.org/0000-0002-1106-3619
Received: September 4, 2020; Revised: November 11, 2020; Accepted: December 12, 2020
© The Author(s) 2021. Published by Oxford University Press. All rights reserved. For Permissions, please email: journals.permissions@oup.com
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/
licenses/by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited.
For commercial re-use, please contact journals.permissions@oup.com
82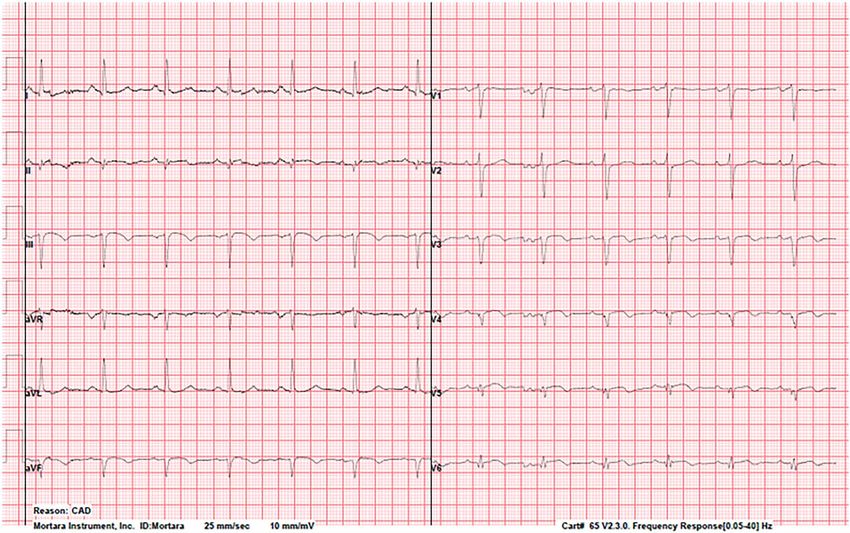
STEMI associated with SARS-CoV-2 infection 83
11:40 h. STEMI protocol was activated and patient was taken to
the cardiac catheterization lab. Left heart catheterization with
coronary angiography and graft injection showed 90% stenosis
of both proximal and mid-portion of the RCA with a TIMI flow
of 3. Saphenous vein grafts to mid-diagonal artery and mid-
obtuse marginal artery were patent. Left ventricular ejection
fraction was 55%. Successful PCI of the proximal and mid-RCA
using the balloon angioplasty and DES was performed. Post-PCI
stenosis was 0% with TIMI flow of 3 (Fig. 3). Severe hypoxia out of
proportion to the CAD was noted during the procedure. ECG post-
PCI showed near normalization of the ST-segment elevation
(Fig. 4). He was given prasugrel and started on eptifibatide drip
Downloaded from https://academic.oup.com/omcr/article/2021/3/omaa148/6161395 by guest on 30 November 2021
and was transferred to the medical intensive care unit. Even
though his chest pain improved following the PCI, he was still
complaining of SOB requiring up to 10 L of oxygen by high-
flow nasal cannula (HFNC). Because of the rapid and abrupt
decompensation, he was intubated on the hospital day 1 (HD#1).
Five-day course of azithromycin and hydroxychloroquine was
completed with no significant improvement. Patient received
Figure 1: CXR on admission showing diffuse bilateral infiltrates involving almost two doses of intravenous tocilizumab on HD#5 and #6. Refractory
all of the lung fields. hypoxemia (arterial blood gases: pH 7.41, pCO2 53.4, pO2 72.4,
HCO3 34) persisted despite maximal ventilator settings (proned,
on chronic heart failure exacerbation, myocarditis, pericarditis, FiO2 100%, PEEP 15 cm H2 O, epoprostenol sodium and paralytics).
tension pneumothorax and costochondritis. Therefore, given his young age and otherwise healthy status, it
Chest X-ray (CXR) on admission showed severe diffuse bilat- was decided to place him on venovenous (VV) ECMO support.
eral pulmonary infiltrates with air bronchograms (Fig. 1), which He was cannulated at the bedside with 25 French inferior vena
was concerning for COVID-19 pneumonia. Electrocardiogram cava cannula and 25 French right internal jugular cannula. Flow
(ECG) showed acute inferolateral ST-segment elevation myocar- of 6 L/minute was provided with FiO2 of 100% and sweep of 8.
dial infarction (STEMI). ST-segment depression in V1 and V2 Ventilator mode was set to pressure-regulated volume control,
suggested posterior myocardial injury (Fig. 2). Initial cardiac tro- very low tidal volume at 300 mL, 15 breaths/min, minute volume
ponin I (TnI) was 0.02 ng/L (reference range < 19 ng/L) at 7 h. 4.5 L/min, PEEP 12 cm H2 O, FiO2 60%. On HD#9, interleukin 6
Reverse transcription–polymerase chain reaction was positive (IL-6) level was 86.9 pg/ml (a 12-fold decrease), and ECMO was
for SARS-CoV-2. decannulated on the HD#13. He was extubated on the HD#16
On physical examination, he was diaphoretic, heart rate 100 and was breathing on 10 L oxygen by HFNC. He remained only
beats/minute (bpm), elevated blood pressure at 148/100 mm hg on dexmedetomidine, was awake and followed commands. On
and hypoxic on room air. Repeat TnI was elevated at 19 ng/L at HD#17, oxygen weaned to 4 L, and on HD#18, he was off of oxygen
Figure 2: ECG on admission showing marked ST-segment elevation (lead II, III, aVF and V4–V6).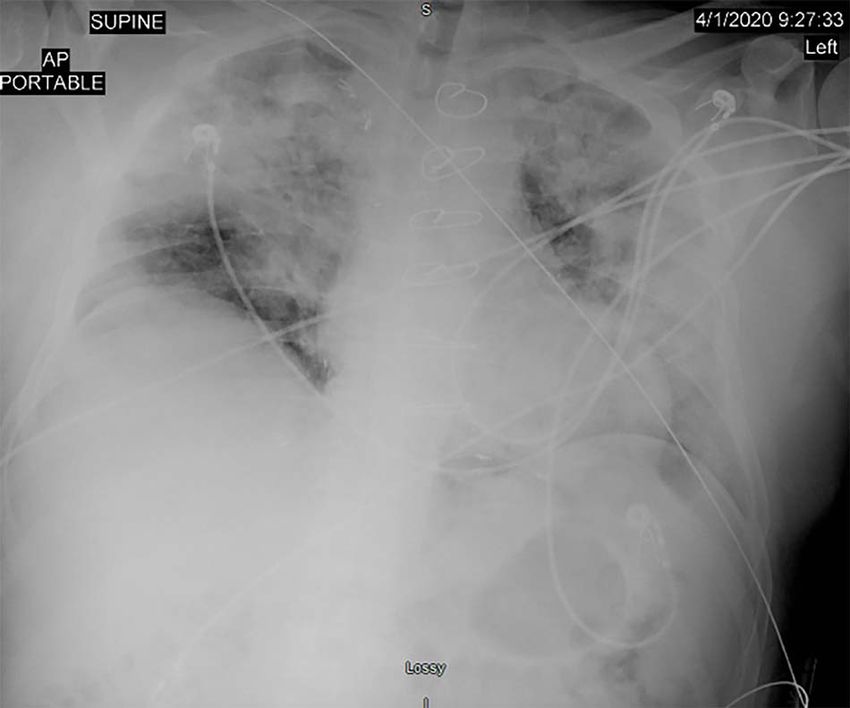
84 T. Rahman et al.
Figure 3: (A) LHC showing 90% stenosis in the proximal and mid-RCA. (B) Guidewire insertion in the RCA. (C) Deployment of the DES in the RCA. (D) Restored perfusion
Downloaded from https://academic.oup.com/omcr/article/2021/3/omaa148/6161395 by guest on 30 November 2021
with 0% stenosis in the RCA after DES deployment.
Figure 4: Normalization of the ST-segment after LHC and PCI.
Table 1: Inflammatory markers pre- and post-tocilizumab and ECMO
Inflammatory markers and Before anti-IL-6 After receiving
cytokine and ECMO anti-IL-6 and
ECMO
IL-6 (reference range (RR): 1054.5 86.9
0.0–15.5 PG/ml)
Crp (RR: 0.0–0.9 mg/dl) 42.8 16
D-dimer (RR:
STEMI associated with SARS-CoV-2 infection 85
DISCUSSION ETHICAL APPROVAL
SARS-CoV-2 uses angiotensin-converting enzyme-2 receptor as No ethical approval was needed for this case report.
a portal of entry into target cells, including endothelium and
cardiac myocytes making heart tissue a common target for
the SARS-CoV-2 [2]. Several observational studies have reported
CONSENT
cardiovascular complications of SARS-CoV-2 infection, including
myocardial injury and myocarditis, acute coronary syndrome, Used for educational purpose with full confidentiality of
acute heart failure, cardiomyopathies, elevated troponins, patient information. Patient’s written consent was obtained and
cardiac dysrhythmias and venous thromboembolic events submitted.
[3, 4]. Little is known about the pathophysiology of acute
coronary syndrome (ACS) in SARS-CoV-2 infection. Multiple
mechanisms have been postulated including direct myocardial
GUARANTOR
Downloaded from https://academic.oup.com/omcr/article/2021/3/omaa148/6161395 by guest on 30 November 2021
injury, plaque rupture due to severe acute inflammation,
aggravation of preexisting CAD, altered myocardial demand– Julianne E. Donnelly, MD.
supply ratio, coronary thrombosis. It is plausible that, the COVID-
19 infection facilitated the thrombosis in the RCA by inducing
a hypercoagulable state [5] in a patient already prone to ACS
from preexisting CAD and polycythemia (admission hemoglobin REFERENCES
17.9 g/dl and hematocrit 51.1%). IL-6 plays a significant role 1. WL-m Y X-h, Ai-bin L, Zhu G. Severe acute respiratory syn-
to cause ‘cytokine storm’ in acute inflammatory settings and drome and venous thromboembolism in multiple organs.
reported to be associated with myocardial injury [6]. In our Am J Respir Crit Care Med 2010;182:436–7. doi: 10.1164/ajr-
patient, administration of tocilizumab and VV ECMO was ccm.182.3.436.
associated with a positive outcome with significant decrease 2. Gheblawi M, Wang K, Viveiros A, Nguyen Q, Zhong JC, Turner
in the inflammatory markers and IL-6 possibly by slowing down AJ, et al. Angiotensin-converting enzyme 2: SARS-CoV-2
the vicious inflammatory process. There is emerging evidence receptor and regulator of the renin-angiotensin system: cel-
on the beneficial effect of ECMO in the treatment of COVID-19 ebrating the 20th anniversary of the discovery of ACE2. Circ
including improved survival rate [7, 8], and similar mortality Res 2020;126:1456–74. doi: 10.1161/CIRCRESAHA.120.317015.
in patients with severe adult respiratory distress syndrome 3. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clin-
regardless of the COVID-19 status [9]. ical features of patients infected with 2019 novel coron-
Cui et al. reported an increased incidence of venous throm- avirus in Wuhan, China. The Lancet 2020;395:497–506. doi:
boembolism (VTE) and associated mortality in their patient pop- 10.1016/S0140-6736(20)30183-5.
ulation with COVID-19 [10]. Our patient was discharged on apix- 4. Klok FA, Kruip M, NJM v d M, Arbous MS, Gommers D, Kant
aban in addition to clopidogrel, rosuvastatin and metoprolol KM, et al. Incidence of thrombotic complications in critically
due to this potential risk of developing VTE from SARS-CoV-2 ill ICU patients with COVID-19. Thromb Res 2020;191:145–147.
infection and having a recent RCA thrombosis. doi: 10.1016/j.thromres.2020.04.013.
5. Connors JM, Levy JH. Thromboinflammation and the
ACKNOWLEDGEMENTS hypercoagulability of COVID-19. J Thromb Haemost
2020;18:1559–1561. doi: 10.1111/jth.14849.
We thank all the authors mentioned hereby and the Department 6. Ritschel VN, Seljeflot I, Arnesen H, Halvorsen S, Weiss T,
of Internal Medicine, Department of Cardiology, Department of Eritsland J, et al. IL-6 signalling in patients with acute ST-
Radiology, Department of Infectious Diseases, Department of elevation myocardial infarction. Res Immunol 2014;4:8–13. doi:
Pulmonary and Critical Care Medicine, Department of Cardio- 10.1016/j.rinim.2013.11.002.
thoracic surgery, staff members of the medical and surgical 7. Kon ZN, Smith DE, Chang SH, Goldenberg RM, Angel LF,
ICU. We would also like to mention our gratitude to Dr Fred Carillo JA, et al. Extracorporeal membrane oxygenation
J. Balis, Program Director, St Luke’s Hospital Internal Medicine support in severe COVID-19. Ann Thorac Surg 2020. doi:
Residency Program and St Luke’s Hospital Internal Medicine 10.1016/j.athoracsur.2020.07.002.
Residency. 8. Li X, Guo Z, Li B, Zhang X, Tian R, Wu W, et al. Extra-
corporeal membrane oxygenation for coronavirus disease
2019 in Shanghai, China. ASAIO J 2020;66:475–81. https://doi.
CONFLICT OF INTEREST
org/10.1097/MAT.0000000000001172.
None. 9. Barbaro RP, Mac Laren G, Boonstra PS, Iwashyna TJ, Slutsky
AS, Fan E, et al. Extracorporeal membrane oxygenation sup-
port in COVID-19: an international cohort study of the extra-
FUNDING
corporeal life support organization registry. The Lancet 2020;
None. 396:1071–8. https://doi.org/10.1016/S0140-6736(20)32008-0.
10. Cui S, Chen S, Li X, Liu S, Wang F. Prevalence of venous
thromboembolism in patients with severe novel coronavirus
DISCLOSURE pneumonia. J Thromb Haemost 2020;18:1421–4. https://doi.
None. org/10.1111/jth.14830.You can also read

















































