Society for Pediatric Pathologists Abstracts of the 2021 Fall Meeting October 8-9, 2021 Virtual Meeting
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Society for Pediatric Pathologists
Abstracts of the 2021 Fall Meeting
October 8-9, 2021
Virtual Meeting
PLATFORM I: Placenta 1 Recurrence risk of villitis of unknown etiology: analysis of a large retrospective cohort study and systematic review L de Koning1, S Crawford2, E Nohr3, J Wright, Jr1, C Horn3, E Chan3 1 University of Calgary, Calgary, Alberta; 2Alberta Health Services, Calgary, Alberta; 3Alberta Precision Laboratories, Calgary, Alberta Background: Recurrence risk of villitis of unknown etiology (VUE) remains uncertain due to heterogeneity of study characteristics such as criteria for placental examination, rule-out of infectious causes, pathologist specialization, and small numbers of initial and recurrent VUE cases. Further, few studies have expressed recurrence risk according to parity and gravida – which may help set ‘lower bounds’ on recurrence risk. Our first objective was to determine recurrence risk of VUE in a large population of placentas sent for pathologic examination by pediatric and perinatal pathologists at our institution using clearly defined and consistent criteria, and to express recurrence risk per parity and gravida. Our second objective was to compare these estimates to others from the literature via systematic review. Methods: Eleven years (2010-2021) of placenta pathology reports on singleton pregnancies ≥ 20 weeks gestation in Calgary, Alberta, Canada were retrieved from the Cerner Millennium lab information system, and candidate reports with villitis were identified using a Perl script searching for ‘villitis’ or VUE’. Cases of acute villitis and chronic villitis due to infections were eliminated via pathologist review. Reports were merged to gestational age, parity and gravida from Alberta Perinatal Health Program data. VUE recurrence risk (among patients with ≥ 2 placentas examined) per patient, parity and gravida were determined. Results were compared to those found among articles and their references identified via an Ovid MEDLINE® (1946-June 2021) search using keywords for VUE and recurrence. Results: We retrieved 29185 placenta pathology reports from 27146 patients. There were 2424 cases of VUE among 2383 patients (8.8% / patient, 4.9% per parity, and 3.7% per gravida). Among 153 patients who had ≥ 2 placentas examined, there were 41 recurrent cases (each only occurring once) of VUE for a recurrence risk of 27% per patient (22% / parity, 19% / gravida). The literature search identified 64 articles, of which 6 were retrieved for data extraction – 1 of which was a conference abstract cited by an article but not identified in the initial search. Reported recurrence risks per patient were 8-56%, with 9-575 initial cases of VUE, and 5-17 recurrent cases. One study, which examined all placentas from all births over a ~3 year period, also found a recurrence risk of 27%. Conclusion: In our study, which is the largest of its kind to date, VUE recurrence risk was ~ 27%. We feel that this result, while lower than in other studies, may better represent actual recurrence risk – especially if parity and gravida are considered.
2 Prevalence of chronic histiocytic intervillositis before and after the COVID-19 pandemic S Ikegami1, L Ernst2 1 University of Cincinnati, Department of Pathology, Cincinnati, Ohio; 2NorthShore University HealthSystem, Department of Pathology, Evanston, Illinois Background: Various placental pathology has been described in association with the coronavirus disease 2019 (COVID-19) in pregnancy, but no distinctive pattern has emerged as specific. However, the pattern of chronic histiocytic intervillositis (CHI) with trophoblast necrosis may be associated with the most severe forms of COVID-19 in pregnancy. Our objective was to examine the prevalence of CHI pre and post COVID-19 pandemic and describe the patterns of pathology seen in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) positive versus negative patients. Methods: We searched our pathology database for the diagnosis of “chronic intervillositis” from 1/1/2017 to 6/1/2021. H&E slides were reviewed, and CHI categorized as “massive” (≥50% involvement) or focal (
3 Examining the Impact of Villitis of Unknown Etiology Histopathological Lesion and Adverse Clinical Neonatal Outcomes in an Eastern Ontario Maternity Population B Osborne1, S Dancey2, I Oltean3, V Bijelic4, S Lawrence5, F Moretti6, J de Nanassy3, S Bainbridge7, D El Demellawy3 1 Children's Hospital of Eastern Ontario Research Institute, Ottawa, Ontario; 2Faculty of Medicine, University of Ottawa, Ottawa, Ontario; 3Department of Pathology, Children's Hospital of Eastern Ontario, Ottawa, Ontario; 4Clinical Research Unit, Children's Hospital of Eastern Ontario, Ottawa, Ontario; 5Department of Pediatrics, Children's Hospital of Eastern Ontario, Ottawa, Ontario; 6 Department of Obstetrics and Gynecology, The Ottawa Hospital, Ottawa, Ontario; 7Faculty of Health Sciences, University of Ottawa, Ottawa, Ontario Background: Villitis of unknown etiology (VUE) is a histopathological lesion affecting 5-15% of term placentas. VUE has previously been linked to intrauterine growth restriction (IUGR), recurrent pregnancy loss, and neurological abnormalities in the newborn. The impact of VUE histopathology features, namely severity and distribution, remains unclear. We seek to define the relationship between VUE diagnosis (severity, distribution) and short-term adverse neonatal outcomes. Methods: A retrospective chart review of placental pathology findings from placentas diagnosed with VUE from 2013-2016 at the Department of Pathology was conducted. Cases of VUE were identified by a search through electronic medical records. Placental pathology reports were examined to confirm the diagnosis of VUE and record severity and distribution according to the Amsterdam Consensus Statement criteria. Control placentas were randomly selected, matching based on gestational age at delivery (+/- 1 week) and fetal IUGR status. Cases of multiple gestation were excluded from the analysis. Neonatal outcomes of interest include: need for newborn resuscitation, neonatal intensive care unit (NICU) admission, APGAR scores (at 1 and 5 minutes) and cord pH. Data are presented as median (IQR) for continuous and frequency (%) for categorical variables. Odds ratios (OR) and 95% confidence intervals (CIs) were calculated with the control cases as the reference group. Results: 226 placentas with VUE, and 232 control placentas without VUE were identified after matching and excluding multiple gestations. Across the entire cohort, the median gestational age was 38 weeks [36-39]. 35% of total placentas were complicated by IUGR. When analysed by severity (low-grade: OR = 4.75 [2.86-8.14], p
4 SARS-CoV-2 Infection of the Placenta Should not be Called “SARS-CoV-2 Placentitis", a Term that is Misleading, Not Supported by the Literature, and Should be Abandoned: A Review of the Literature of Chronic Histiocytic Intervillositis M Luquette University of Minnesota, Department of Pathology, Minneapolis, Minnesota Background: Chronic Histiocytic Intervillositis (CHI) is a pattern of inflammation in the placenta that was first described 34 years ago and has been heavily reported in the last 2 years in cases of maternal Covid-19 infection with vertical transmission across the placenta. CHI has been reported in placentas of patients with malaria, CMV, and autoimmune conditions affecting the placenta, including pedigrees in which fetus specific antibodies target HLA mismatched paternal haplotypes. With an increase in reports using the term "SARS-CoV-2 Placentitis" (SCP) and the referencing of reports that use the term, the question arises, "Is there any evidence that CHI is caused by SARS-CoV-2" thus justifying the term SCP. Methods: To date 122 articles are returned in a PubMed search of "Intervillositis". Full text of these articles was downloaded and the articles were reviewed and data recorded for: year of publication; journal type; a pathologist as an author; type of study; conclusions; reporting of incidence of CHI; type of intervillositis; reporting of gravidity and parity; Covid-19 as a topic; claims that SARS-CoV- 2 causes CHI; mention of vertical transmission, an autoimmune process, or trophoblast necrosis; and claims that the Ace2 receptor is a portal of infection. Data were reviewed to answer the above stated question. Results: There were 4 articles that used the term SARS-CoV-2 placentitis, 1with SARS-CoV-2 inflammation, and 1 with SARS-CoV-2 intervillositis. While some of these studies ruled out some viral infections, they do not adequately assess autoimmunity as an etiology for CHI in the reported cases. Seven articles claim either primary viral infection of the trophoblast or that the virus causes CHI. They do not contemplate that the damage may be a mixture of primary autoimmune damage followed by additional damage by SARS-CoV-2 or that a non-covid cause may be the initiator of the CHI. Four studies reporting incidence of CHI in placentas > 36 weeks gestation, pre-covid, show an incidence of 0.098 to 0.4% Two studies of incidence of CHI (not in the intervillositis search) in placentas > 37 weeks gestation, post-covid, show an incidence of 0-0.27%. No data is reported showing an increased incidence in CHI, post-covid. Conclusion: While CHI can easily be appreciated as a portal for placental infection by SARS-CoV-2 that may well magnify trophoblast necrosis beyond what is normally seen in CHI, there is nothing in the literature that proves that CHI or a Covid modified version of CHI is initiated by SARS-CoV-2 vs another etiology, namely an autoimmune condition. Hence the term "SARS-CoV-2 Placentitis" and similar terms are misleading and should be abandoned. Issuing separate diagnoses of CHI and SARS-CoV-2 infection is recommended.
5 Placental Histopathology Associated with SARS-CoV-2 Infection in Pregnancy: Preliminary Data from a Prospective Cohort Study in Ontario, Canada S Fellus1, S Dancey1, Y Nasr2, S Mohammad3, G Vasam3, S Bainbridge4, S Girard5, B de Vrijer6, A Dingwall Harvey3, R Fakhraei3, M Murphy3, D El-Chaâr3, D El-Demellawy7 1 Faculty of Medicine, University of Ottawa, Ottawa, Ontario; 2Faculty of Science, University of Ottawa, Ottawa, Ontario; 3Clinical Epidemiology Program, Ottawa Hospital Research Institute, Ottawa, Ontario; 4 Faculty of Health Sciences, University of Ottawa, Ottawa, Ontario; 5Department of Obstetrics and Gynecology, Université de Montréal, Montreal, Quebec; 6Department of Obstetrics and Gynaecology, Western University, London; 7Department of Paediatric Pathology, Children’s Hospital of Eastern Ontario, Ottawa, Ontario Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been responsible for significant maternal and neonatal morbidity. Examination of placentas from individuals infected with SARS-CoV-2 during pregnancy have demonstrated maternal vascular malperfusion, fetal vascular malperfusion and evidence of inflammation, however studies to date are limited by small sample sizes, paucity of information on maternal comorbidities, and lack of data about infection time point. The objective of this study was to investigate placental findings of cases compared to controls, as well as to compare recovered versus active cases at the time of delivery. Methods: This was a sub-study of a large multi-center prospective cohort study of pregnant women with clinically-confirmed SARS-CoV-2 infection in Ontario, Canada, from March-July 2021. Placentas collected from study participants delivering at a single site were used for this preliminary analysis. Demographic and clinical (i.e., preeclampsia, gestational diabetes, chronic diabetes, and intrauterine growth restriction) data were extracted from patient medical records. Placentas were evaluated for frequency and type of histologic lesions using a placental phenotypic classification tool (Freedman et al., 2021). Findings from cases were compared to those from pregnancies not complicated by SARS-CoV-2. Timing of infection in pregnancy was also considered. Fisher’s exact test was used for comparing categorical data. Continuous data was compared using a 2-sample t-test. Results: A total of 47 women had placental samples available for this analysis, including 33 cases and 14 controls. Among the cases, 8 (24.2%) were positive for SARS-CoV-2 infection at delivery and 25 (75.8%) were recovered from infections earlier in pregnancy. Six (18.2%) cases and 3 (21.4%) controls had comorbidities in pregnancy. The mean gestational age and standard deviation at delivery was 39.06±2.12 weeks, and 7 (21.2%) cases delivered by C-section compared to 7 (50%) of controls. Placental pathology of individuals infected in pregnancy did not differ compared to controls. Individuals infected with SARS-CoV-2 at the time of delivery did not have different rates of placental lesions compared to those infected earlier in pregnancy. Conclusion: In this preliminary analysis we conducted histopathological examinations of placentas from women testing positive for SARS-CoV-2 at any time point during pregnancy as well as from women who had tested negative. Cases and controls had similar rates of placental lesions. Timing of infection did not significantly impact placental pathology. Analysis of the full cohort, including controls matched for gestational age and comorbidities, is forthcoming in order to more robustly assess placental pathology in pregnant women infected with SARS-CoV-2.
6 Intervillositis in Placentas from Gestations Complicated by Maternal SARS-CoV-2 Infection: Fetal and Neonatal Outcomes J Havens1, O Faye-Petersen1, A Lu2, A Feldman1, V Duncan1, N Arora2 1 The University of Alabama at Birmingham Department of Pathology, Birmingham, Alabama; 2The University of Alabama at Birmingham Department of Pediatrics, Birmingham, Alabama Background: Most placentas from SARS-Cov-2 positive mothers are normal or reflect nonspecific pathology. Intervillositis is a severe but rare pattern of injury recently described in placentas of mothers with SARS-CoV-2 infection. Relationships of this pathology to SARS-CoV-2 infection, fetal and neonatal outcomes, and maternal symptomatology are poorly understood. Methods: We report a series of placentas from 6 SARS-CoV-2 positive women collected 3/2020- 8/2021. Gestational age ranged from 22-37 weeks. Placental tissue was collected, stained, and evaluated using standard protocols. In situ hybridization (ISH) specific for SARS-CoV-2 S gene encoding the spike protein was performed on paraffin-embedded tissue. Results: All placentas showed intervillositis accompanied by trophoblast necrosis and variable perivillous fibrinoid deposition. In 5 cases, the inflammation was predominantly monocytic; one case had mixed inflammation with a predominant neutrophilic component. No cases showed significant villitis. The pathology was diffuse in 4 cases and patchy but widespread in 2 cases. All cases showed strong positive ISH staining of the villous trophoblast in a circumferential perivillous pattern. All maternal infections were acute, within about 2 weeks prior to delivery. Outcomes included intrauterine fetal demise in 2 cases and neonatal demise in 1 case. All 3 had diffuse placental inflammation, but all were also complicated by either severe chronic uteroplacental pathology or clinical circumstances preventing emergent delivery. Three babies survived. One baby had low Apgar scores and extended intensive care unit care, and had only patchy placental inflammation. One baby had initial low Apgar scores and metabolic acidosis with diffuse placental involvement. One baby (the only baby born at term) had patchy placental inflammation and did well. All of the liveborn neonates had negative tests at birth for SARS-CoV-2; the term neonate had a subsequent positive test. Maternal symptomatology varied and did not appear to relate to fetal or neonatal outcome. Conclusion: This series, though small, supports an association between placental intervillositis and maternal SARS-CoV-2. Degree of placental compromise is likely an important determinant in fetal/neonatal outcome. However, despite severe placental pathology, mortality in this series occurred only in the setting of comorbid complications, suggesting that timing of delivery and close maternal monitoring is important in mitigating poor outcomes. Further studies are needed to investigate the associations of this rare but severe pattern of placental injury.
7 Recurrence of placental lesions in a pathology sample A Freedman1, L Ernst2 1 Northwestern University, Evanston, Illinois; 2NorthShore University HealthSystem, Evanston, Illinois Background: Several placental lesions are known to recur in subsequent pregnancies. However, estimates of recurrence are often based on risk, which does not include a comparison group. A comparison group, as included in the risk ratio, helps to account for the baseline prevalence of the lesion in the sample, which can be affected by differences in the underlying population, indications for pathologic review, and sampling techniques. Our goal was to estimate the recurrence risk ratio for the major placental lesion categories. Methods: The study sample included placentas submitted for pathologic review at a single hospital between January 2009 and March 2018. During the study period, 21,917 patients had two deliveries and 883 patients had placental pathology reports available for both deliveries. Pathology reports were completed by perinatal pathologists and placental lesions were classified based on Amsterdam consensus criteria: acute placental inflammation (API), chronic placental inflammation (CPI), maternal vascular malperfusion (MVM), and fetal vascular malperfusion (FVM). Log-binomial models were used to estimate recurrence risk ratios for the four major placental lesion categories. Models were adjusted for maternal and pregnancy characteristics, including race/ethnicity, interpregnancy interval, and maternal age and parity at the time of the first study pregnancy. Inverse probability weights were used to partially account for selection into the pathology sample. Results: In our pathology-based sample, the prevalence of recurrent pathology was 27.0% for API, 22.5% for CPI, 21.7% for MVM, and 12.2% for FVM. The recurrence risk ratio (RR) was strongest for CPI, indicating that those with CPI in the first pregnancy were 1.61 times as likely to develop CPI in the subsequent pregnancy as compared to those without CPI in the first pregnancy (95% confidence interval [CI]: 1.40, 1.84). Similarly, those with MVM in the first pregnancy were 1.55 times as likely to develop MVM in the subsequent pregnancy (95% CI: 1.29, 1.86) and those with FVM in the first pregnancy were 1.23 times as likely to develop FVM in the subsequent pregnancy (95% CI: 1.04, 1.44). API in the first pregnancy was not associated with API in the subsequent pregnancy after controlling for covariates and accounting for selection bias (RR: 1.10; 95% CI: 0.95, 1.27). Conclusion: Our results suggest that CPI, MVM, and FVM may recur in a subsequent pregnancy, even after controlling for covariates and partially accounting for selection bias. We did not observe evidence of recurrence for API. Additional research is needed to understand recurrence risk in a representative sample, to evaluate whether grade of pathology is important, and to explore whether specific lesions are driving recurrence estimates.
8 Impact of Co-existing Placental Pathologies in Pregnancies complicated by Placental Abruption and Acute Neonatal Outcomes I Oltean1, D Mavedatnia2, J Tran2, V Bijelić1, S Lawrence3, D El Demellawy3 1 Children's Hospital of Eastern Ontario Research Institute, Ottawa, Ontario; 2University of Ottawa School of Medicine, Ottawa, Ontario; 3Children's Hospital of Eastern Ontario, Ottawa, Ontario Background: Placental abruption (PA) is a critical concern for maternal and neonatal morbidity and mortality. Adverse perinatal outcomes in the setting of PA, include higher risk of fetal-growth restriction, stillbirth, prematurity, and birth asphyxia. Placental pathologies as defined by the Amesterdam consensus include maternal vascular malperfusion (MVM), fetal vascular malperfusion (FVM), acute chorioamnionitis, and villitis of unknown etiology (VUE), among others. These pathologies are independently associated with the presence of perinatal complications. The aim of this present study is to investigate if placental pathologies can adversely affect acute neonatal outcome in pregnancies complicated with PA. Methods: A retrospective cohort study was conducted. All placentas with the pathologic or clinical diagnosis of PA and/or retroplacental hematoma from October 1st 2013 to April 30th 2020 were identified from the pathology archives using Epic-Hyperspace. A clinical diagnosis of abruption was confirmed via ultrasound or the clinical presentation of vaginal bleeding, abdominal pain, uterine contractions, or uterine tenderness, as defined on the electronic medical records (EMRs). The pathological diagnosis was then confirmed post-delivery with placental examination for the presence of MVM, FVM, acute chorioamnionitis and VUE. The presence of retroplacental clot(s) were also assessed as additional coexisting pathologies. Our outcomes were NICU admission, BD 10-15.9 or BD >=16, cord pH
PLATFORM II: Perinatal and Pediatric 9 Prior cesarean section correlates with higher invasiveness grade in patients with Placenta Accreta Spectrum: Questioning the concept of uterine scar dehiscence G Neville, A Sharma, C Parra-Harran Brigham and Women's Hospital, Boston, Massachusetts Background: Placenta accreta spectrum disorders (PAS) are an increasingly common obstetric challenge associated with significant maternal morbidity and mortality. Recent guidelines have established that the diagnosis and classification of PAS on hysterectomy material requires distinction between placental tissue at the site of scar dehiscence and true myometrial invasion. It remains uncertain whether such distinction can be made on histologic examination and whether it is clinically important. Methods: The aim of this study was to establish differences between PAS associated with a cesarean section (CS) scar or prior instrumentation and PAS without such a history. We retrieved slides from gravid hysterectomies with a diagnosis of PAS in our institution. Each case was reviewed along with obstetric history and clinical outcomes. PAS grade was assigned following recent recommendations (PMID: 32415266). A trichrome stain was applied to all cases to aid in this assessment. Results: Of 61 histologically confirmed PAS cases, 80.3% (n=49) had a history of prior CS. Of the remaining, 13.1% (n=8) had a history of uterine instrumentation, whereas 6.6% (n=4) had no prior history of CS or uterine instrumentation (one had undergone in vitro fertilization (IVF)). Of those with a history of prior CS, most (n=42, 85.7%) had the placental bed in the anterior lower uterine segment (area of the prior CS scar). Six of the 7 remaining cases had a prior hysteroscopic resection for retained production of conception. Patients with prior CS section were significantly more likely to present with advanced PAS grade: 28.6% (n=14) were grade 1, 12.2% (n=6) were grade 2, 20.4% (n=10) were grade 3a and 38.8% (n=19) were grade 3D. In contrast, of those with prior instrumentation per PAS grading system; 62.5% (n=5) were grade 1, 25% (n=2) were grade 2 and 12.5% (n=1) 3a. Of those with no prior instrumentation or CS per PAS grading system; 50% (n=2) were grade 1, 25% (n=1) were grade 2 and 25% (n=1) were grade 3d. Fisher’s t-test confirmed a significantly higher PAS grade in the CS group compared to other PAS cases (p*
10 Association of Placental Pathology with Growth Arrest Line Formation in Fetal Growth Restriction T Chu, W Parks, P Shannon University of Toronto, Toronto, Ontario Background: Asymmetric fetal growth restriction (GR) is a common consequence of severe gestational uterine and placental pathology. Although bone shortening and irregular growth are a hallmark of GR, there are no systematic studies correlating bone growth with placental pathology. In this study, we examine the relationship between growth arrest lines (GAL) and placental pathology in a large cohort of pathologically investigated cases of fetal asymmetrical GR. Methods: We used text word searching of our laboratory information system to identify all fetal or neonatal autopsies demonstrating growth arrest lines or growth restriction over a period of 5/12 years. Each case was reviewed for the severity of growth restriction and associated pathologies We excluded cases of symmetrical growth restriction, aneuploidy, multiple congenital anomalies, and multiple pregnancies. The accompanying uteroplacental, and umbilical cord pathologies were reviewed and categorized as placental pathologies (maternal vascular malperfusion, fetal vascular malperfusion, significant intervillous or subchorial haematoma, chronic villitis, intervillositis, pervillous fibrinoid deposition, delayed villous maturation., placenta accreta spectrum) or umbilical cord pathology (abnormalities of coiling, insertion or thrombosis). Associated histology of whole mounted long bone growth arrest lines was also retrieved. Results: We searched 2,108 fetal post mortems, and retrieved 112 cases of non-syndromic, isolated asymmetrical growth restriction. Of these, 16 (14%) had growth arrest lines. 5 further cases had GAL without GR. In asymmetric GR, GAL were associated with a wide variety of placental diseases, but most commonly with fetal and maternal vascular malperfusion. The presence of GAL did not correlate with the severity of the GR, nor were GAL associated with specific placental pathologies. 5 histologically demonstrated cases of GAL in asymmetric GR were retrieved: all showed (from epiphysis towards metaphysis) subchondral radiodensity, followed by a zone of radiolucency, followed by a zone of radiodensity. The radiolucency corresponds to a zone of poor trabecular bone formation, with the sclerotic zone in the metaphysis to coarse trabeculae with poor remodeling. Conclusion: GAR are thought to represent episodic severe slowing of fetal growth; however, we found GAL in the presence of placental pathologies usually thought to be steadily progressive (e.g. maternal vascular malperfusion, histiocytic intervillositis). Further the histological pattern is not that of a simple period of slow growth. We conclude that GAL can accompany a wide variety of placental diseases, but that their biology is poorly understood.
11 Fetal Vascular Ectasia Can Be an Artifact of Placental Fixation P Katzman, L Metlay University of Rochester Medical Center, Rochester, New York Background: As part of our perinatal pathology service, our institution processes placentas from multiple outlying hospitals. In contrast to in-house placentas, these placentas are formalin-fixed en route to our laboratory. We identified that the chorionic, stem villus, and umbilical vessels in these fixed placentas are often ectatic in a greater frequency than in our in-house fresh placentas. In order to identify whether fixation was associated with this increased rate of vascular ectasia, we fixed all our incoming in-house placentas for a period of time to compare with these outside cases. Methods: We searched our LIS for third trimester placentas using the keywords “ectasia” or “ectatic” over a period of 12 months. We also fixed all incoming in-house placentas over a two-week period for approximately 24-72 hours and tabulated fixation time and the presence or absence of ectasia of chorionic, stem villus, and umbilical vessels, as defined by Parast et al, 2008, as vascular distension to at least four times the diameter of an adjacent muscular vessel of similar caliber. Statistical comparisons were performed using www.medcalc.org. Results: The LIS search identified 51/83 (61%) of placental cases from outlying hospitals that had ectatic vessels versus 56/2110 (3%) in in-house placentas (p
12 Congenital Cytomegalovirus (CMV) Infection But Negative Second Trimester Maternal CMV IgM Antibodies – A Report of 4 Cases E Chan1, H Zhou2 1 University of Calgary, Calgary, Alberta; 2Alberta Precision Laboratories, Calgary, Alberta Background: Congenital cytomegalovirus (cCMV) is the most common congenitally acquired viral infection. Pregnant women are not routinely tested for CMV infection; maternal CMV IgG/IgM testing typically occurs following suspicious prenatal ultrasound (US) findings. The diagnosis of a recent CMV infection is often considered less likely if CMV IgM is -ve. Methods: We described 4 cases of cCMV infection with placental and/or autopsy findings, in which the 2nd trimester maternal CMV IgM was -ve. Results: Case 1. A 20-year-old (yo) G2P0 woman presented with prenatal US findings suggestive of intrauterine infection at 24 1/7 weeks gestational age (GA). Maternal CMV IgG/IgM performed at 25 weeks GA were +ve and -ve respectively. Placental examination following fetal demise at 30 3/7 weeks GA revealed CMV-associated villitis. Case 2. A 26 yo G2P0 woman with fetal hydrops diagnosed at 19 5/7 weeks GA had CMV testing at 21 1/7 weeks GA; IgG was +ve and IgM was -ve. At 21 6/7 weeks, amniotic fluid CMV PCR was +ve. In light of this finding, CMV IgG avidity was performed on the 21 1/7 weeks GA maternal blood sample and it showed low avidity. Placental examination following termination of pregnancy (TOP) at 24 4/7 weeks GA confirmed cCMV. Case 3. A 39 yo G1P0 woman presented with simple fetal ascites at 19 2/7 weeks GA. Maternal CMV IgG was +ve and IgM was -ve at 19 3/7 weeks GA. TOP due to fetal intracranial bleed occurred at 22 weeks GA. Autopsy/placental examination revealed cCMV. Subsequently, CMV serologies performed on the mother’s stored blood sample from 11 4/7 weeks GA demonstrated +ve IgM and low IgG avidity, suggesting maternal CMV infection around the time of conception. Case 4. A 33 yo G4P2 woman whose prenatal US at 20 4/7 weeks GA showed mildly increased abdominal circumference had c-section at 26 weeks GA for abruption. At the time of delivery, maternal CMV IgG was +ve and IgM was -ve. The baby had respiratory distress and thrombocytopenia, and died on day 5 of life. Autopsy revealed diffuse CMV infection. Testing performed on the mother’s stored prenatal blood sample (collected at 9 5/7 weeks GA) demonstrated +ve CMV IgG/IgM and low IgG avidity, indicating maternal CMV infection around the time of conception. Conclusion: In each of these 4 cases, maternal CMV IgM performed in 2nd trimester was -ve; thus, cCMV infection was not originally suspected. Yet, autopsy and/or placental examination demonstrated CMV infection in all 4 cases. In 2 of these cases, stored maternal blood samples from 1st trimester demonstrated +ve CMV IgG, +ve IgM, and low IgG avidity, confirming maternal CMV infection around the time of conception. These cases illustrated that CMV IgM response can be short-lived; thus, cCMV should not be ruled out based on a -ve maternal CMV IgM result in 2nd or 3rd trimester.
13 Pulmonary Complications after Bone Marrow Transplantation at a large Pediatric Institution. N Cortes-Santiago1, J Pogoriler2, K Patel1, S Sartain1, M Silva-Carmona1, S Bhar1, G Deutsch3 1 Texas Children's Hospital, Baylor College of Medicine, Houston, Texas; 2Children's Hospital of Philadelphia, Philadelphia, Pennsylvania; 3Seattle Children's Hospital, Seattle, Washington Background: Physiology and pathologic features of non-infectious post-BMT pulmonary complications are poorly understood making interpretation of lung biopsies challenging in this patient population. In this study, we characterize the primary lung pathologic findings in 30 post-BMT patients at a large pediatric hospital with correlation to patient’s clinical course and clinical suspicion of pulmonary complications, including graft-versus-host disease (GVHD) and idiopathic pneumonia syndrome (IPS). Methods: Pathology database was queried from 2009-2019 to identify post-BMT patients who had undergone lung biopsy or lung transplantation. Electronic medical record was reviewed for pertinent clinical and demographic data. Pathology material was reviewed by two pathologists (NCS and GD). Findings related to airway and airspace disease, interstitial disease, vasculopathic changes and infectious processes were documented. Primary disease process was classified according to aggregate clinical- pathologic data. Results: Thirty patients met inclusion criteria: median age, 14.4 yrs (10 mo – 24.6 yrs), M:F ratio, 2:1, median age at BMT, 12.8 yrs (7 mo - 24.2 yrs) and median post-BMT interval at biopsy, 7 months (8 d–11 yrs). Reasons for BMT were malignant (17) and benign (12) hematologic and metastatic medulloblastoma (1). BMT types were 1 autologous, 7 matched related donor (MRD), 10 matched unrelated donor (MUD), 4 mismatched RD (MMRD) and 8 MMUD. At the time of this study, 18 patients were deceased, 9 alive and 3 were lost to follow up. Death occurred at a median of 49 days after biopsy (6-102 d). Seven of 18 patients with available information received total body irradiation. Clinical impression was infectious in most cases (18); others were GVHD (3), cryptogenic organizing pneumonia (1) and unknown or undetermined (8), one of which had a diagnosis of IPS. Pathologic findings included bronchiolitis obliterans in 5 of 23 (22%) adequate cases, including 2 explants. Vasculopathic changes were seen in 25 of 28 (89%) adequate cases. Three major pathologic classifications were noted: infectious (12), GVHD (5) and likely toxicity (9); 4 remained of unclear etiology. Clinicopathologic concordance was 30%, all infectious. Five of the 8 patients with unknown clinical diagnosis were deemed to be likely toxic injury on pathologic exam. Biopsy led to change in management in 9 of 17 (53%) patients with available information. Conclusion: Infection continues to be a major cause of morbidity and mortality post-BMT. Vasculopathic changes are exceedingly common, presumably related to drug/radiation toxicity. This argues for a significant role of vascular injury in non-infectious post-BMT pulmonary complications, particularly in those patients with an unclear clinical picture including those with a diagnosis of IPS.
14 Comparing Temperature-Controlled and Direct-to-Freezer Cryopreservation on Cell Viability and PDX Engraftment in Wilms Tumor L Rutherford1, T Bhat2, V Chow1, S Vercauteren1, C Lim2, J Bush1 1 BC Children's and Women's Hospital, Vancouver, British Columbia; 2BC Children's Hospital Research Institute, Vancouver, British Columbia Background: Pediatric malignant solid tumors are typically triaged in the fresh state into multiple potential pathways, which may include formalin-fixation, touch preparations, snap-freezing, and glutaraldehyde. These methods provide adequate clinical diagnostic information, but are not typically amenable to establishing cell lines or patient-derived xenografts (PDXs). This could serve as a limitation at both the bench and bedside as more clinical and research studies have moved towards personalized medicine. Additionally, cryopreservation is often associated as needing specialized temperature- controlled freezing apparatuses, which may provide a barrier to adoption. We sought to test various types of cryopreservation media and dissociation methods using Wilms tumor (WT) as a tumor model through post-thaw cell counts and chorioallantoic membrane (CAM) xenograft success. Methods: Fresh WT tissue was processed for cryopreservation and freezing at -80C using four methods: 2 x 3mm chunks in 10% DMSO, 2 x 3mm chunks in CELLBANKER 2 (CB2, Amsbio LLC) freezing media, single cells dissociated by density-gradient separation in 10% DMSO, and single cells dissociated using GentleMACs dissociator in 10% DMSO. After four weeks, the samples were thawed and the chunks frozen in 10% DMSO and CB2 were dissociated into single cells. Cell counts were obtained from all samples and tumour spheroids were prepared from dissociated cells by mixing cell suspension and Matrigel in 1:1 ratio and incubated overnight before implantation. Matrigel encapsulated cells were on- planted into the chicken CAM model to assess tumour growth. Ethics approval was obtained. Results: By day three, all four methods showed tumour growth in the CAM, with the GentleMACS and density-gradient methods of dissociation exhibiting an objectively fuller looking tumour mass than the other methods. By day six, growth expansion plateaued and day nine was the final day of imaging and termination of the CAM model. PDXs were harvested on days 5 and 6 for future cryopreservation and for histologic examination. Conclusion: The use of CB2 for cryopreservation showed no inferiority to 10% DMSO in terms of cell viability nor CAM expansion. Dissociation of tissues into single cells pre-freeze displayed no marked advantage to tumour growth in CAM compared to freezing in chunks. Our findings would suggest the use of either a temperature-controlled method (10% DMSO) or direct-to-freezer method (CB2) for cryopreservation, and that additional pre-freeze preparation by dissociation does not effect viability or growth in Wilms tumor. These pilot results may support the use of CB2 at pathology sites that would not significantly impact fresh-tissue triaging workflows and do not have established modelling capabilities.
15 Beta-hydroxybutyrate and the Forensic Pediatric Autopsy: A Retrospective Case Series A Lafrenière1, C Milroy2, J Parai2 1 Texas Children's Hospital, Baylor College of Medicine, Houston, Texas; 2The Ottawa Hospital, The Eastern Ontario Regional Forensic Pathology Unit, Ottawa, Ontario Background: Beta-hydroxybutyrate (BHB) is used both clinically and in the autopsy setting as a marker for diabetic and alcoholic ketoacidosis in addition to other causes of ketoacidosis. In the adult, post-mortem BHB concentrations in non-ketoacidotic deaths ranges from 0.05 – 2.44 mmol/L. Adult BHB values for the post-mortem diagnosis of ketoacidosis vary, with published threshold fatal values ranging from 1 mmol/L upwards. Post-mortem values for the diagnosis of ketoacidosis have not been assessed in the pediatric population. Methods: The records of the Forensic Pathology Unit were searched for pediatric deaths (decedent less than 18 years of age) with elevated levels of vitreous (>2 mmol/L) or blood (>200 mg/L) BHB between January 1, 2010 to December 31, 2020. Autopsy reports were reviewed to obtain demographic information, clinical symptoms, post-mortem biochemistry, and pathology. Histology of the heart, lung, liver, and kidneys were reviewed by two authors blinded to the autopsy information. Statistical analyses were performed to compare histological changes with BHB levels and to assess for any associations between the histologic features. Results: 400 pediatric autopsies were performed during the study period, of which 16 met the inclusion criteria. The mean age was 7.03 years with a median age of 4.5 years. The cause of death was attributed to diabetic ketoacidosis in two cases, one of which was related to maternal diabetic ketoacidosis in a case of intrauterine death. Other causes included infections (n=5), trauma (n=2), congenital heart disease (n=2), unascertained (n=3), malignancy, and mixed drug toxicity. The mean concentration of vitreous BHB was 3.56 mmol/L (median 2.52 mmol/L; n=13 cases) and blood BHB demonstrated a range from
16 Spectrum of Autopsy Findings in COVID-19 Related Pediatric and Fetal Deaths: 4 Cases from a Tertiary Care Children’s Center F Malik, J Kasten, K VandenHeuvel, D Leino, A Bernieh Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio Background: Although Coronavirus disease 19 (COVID-19)-associated mortality is correlated with age and specific pre-existing morbidities, pediatric infection is common, represents an increasing percentage of overall incident infection, is occasionally lethal, and may be rarely associated with the delayed and potentially critical Multisystem Inflammatory Syndrome in Children (MIS-C). The virus crosses the placenta in infected pregnant women, causing placental complications and intrauterine fetal demise (IUFD). We examine the cross-sectional spectrum of pediatric COVID-19 autopsy pathology. Methods: All post-mortem examinations of deaths due to maternal or pediatric antemortem COVID-19 infection performed at a tertiary children’s hospital from June 2020 to August 2021 were reviewed. Results: Two cases each of fetal and pediatric deaths were reviewed. In all cases, COVID-19 infection was confirmed either by serology or polymerase chain reaction (PCR) testing. Examination of each pediatric case was restricted to body only and brain only. IUFDs: The anatomically normal fetuses died at 24 and 36 weeks gestation, respectively. The cause of death in both was placental insufficiency secondary to massive perivillous fibrin deposition, and chronic histiocytic intervillositis with trophoblast necrosis. COVID-19 was confirmed by IHC (2/2) and PCR (1/2) on formalin fixed paraffin embedded placental and fetal liver tissue. Both mothers presented with mild symptoms. Childhood Deaths: The pediatric deaths were in females aged 9 years and 19 years, respectively. Recent COVID-19 infection was confirmed by serology. Brain exam in the 9-year-old showed massive, multiple infarct-like parenchymal necrosis, hemorrhage, cystic cavitation, and perivascular lymphohistiocytic infiltrate without thrombi or flow abnormalities. Additional testing did not reveal other causes. The 19-year-old had Ebstein anomaly, 13 years status post orthotopic heart transplant with high-grade acute cellular rejection. Death was caused by cardiac tamponade and multi-organ failure due to pulmonary artery origin massive hemomediastinum (1000 ml), attributed to COVID-19 related MISC-C causing coagulopathy. Acute vasculitis and prominent endothelial cells rendered histologic support for recent COVID infection. Conclusion: We present autopsy findings in 4 cases of pediatric and fetal deaths due to recent COVID-19 infection. Observed placental lesions leading to insufficiency and IUFD are consistent with previously published reports. The CNS findings of hypoxic-ischemic encephalopathy are attributed to the direct viral damage, previously documented in adults. To the best of our knowledge, this series highlights the first pediatric autopsy findings in a cardiac transplant recipient succumbing to sequelae of COVID-19 related MISC-C.
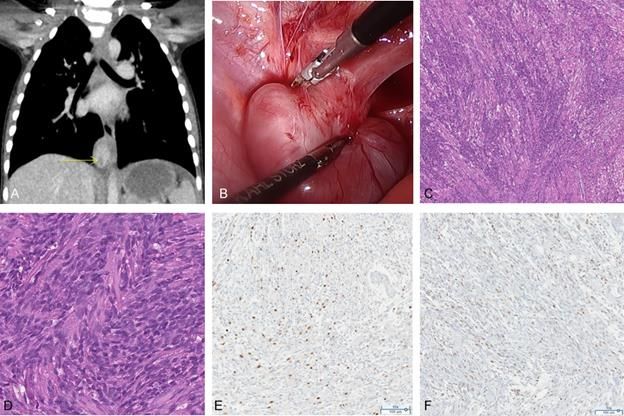
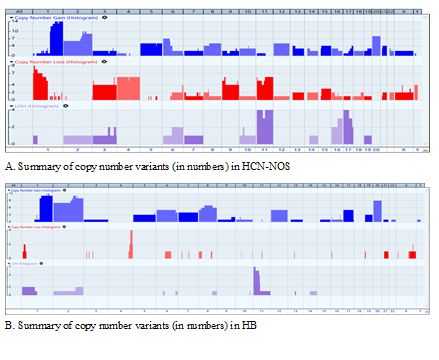
PLATFORM III: Neoplasia 17 Hepatocellular malignant neoplasm, NOS exhibits distinct and more complex copy number alterations than conventional hepatoblastoma S Zhou, D Estrine, D Ostrow, M warren, N Shillingford, L Wang, R Schmidt, G Raca, L Mascarenhas, J Biegel, J Ji Children's Hospital Los Angeles, Los Angeles, California Background: Hepatocellular malignant neoplasm, not otherwise specified (HCN-NOS) is a rare and poorly understood primary liver cancer with overlapping histology features of conventional hepatoblastoma (HB); thus, it is often diagnostically challenging to distinguish HCN-NOS from HB. As a major source of genomic variations driving tumor initiation and evolution, DNA copy number variants (CNVs) have been associated with numerous tumor types. Detection of recurrent CNVs may provide diagnostic as well as prognostic biomarkers to assist clinical diagnosis and management. So far, it is unknown whether HCN-NOS and HB show different CNV profiles. Methods: Chromosomal microarray analysis using OncoScan/Cytoscan HD (Thermo Fisher Scientific) was performed on a total of 13 primary tumors and one recurrent tumor from 13 HCN-NOS patients, and 20 primary tumors and one recurrent tumor from 20 HB patients. Copy number profiles were compared between the two groups. Results: CNVs were detected in 14/14 HCN-NOS specimens (Figure A). In contrast, 18 of 21 HB specimens had CNVs and there were more gains than losses (Figure B). HCN-NOS showed the following recurrent CNVs with an overall frequency higher than 20%: gain of 1q (100%), 2q (64.3%), 20 (57.1%), 6p (50%), 2p (42.9%), 5 (35.7%), 8 (35.7%), 12 (35.7%), 15 (28.6%), 17q (28.6%), 21 (28.6%), and 10 (21.4%); loss of 1p (50%), 4 (42.9%), 11q (42.9%), 9p (35.7%), 11p (35.7%), 3 (28.6%), 9q (28.6%), Y (28.6%), and 15 (21.4%); and copy neutral loss of heterozygosity (CN-LOH) in chromosome 11 (28.6%) and 17p (28.6%). For HBs, there were recurrent gains of 1q (52.4%), 2q (47.6%), 20 (42.8%), 2p (38.1%), 8 (33.3%), 6 (23.8%), 12 (23.8%), 17 (23.8%), 7 (19.0%), and 5 (14.3%); recurrent losses of 4q (19.0%) and 1p (9.5%); and CN-LOH of 11p15.5 (33.3%). Gain of 1q (p = 0.002), losses of 3 (p = 0.019), 4p (p = 0.002), 9 (p = 0.019), 11p (p = 0.006), 11q (p = 0.002) and Y (p = 0.019), and CN-LOH in 17p (p=0.019) were more frequently observed in HCN-NOS group compared to the HB group. There were no significant differences in gains of 2q (p = 0.491) and 20 (p = 0.5), loss of 4q (p = 0.151), or CN-LOH of 11p15.5 (p = 1.0) between the two groups. The recurrent HCN-NOS tumor showed additional CNVs compared to the primary tumor. For the HB case with both primary and recurrent tumors, there were no clinically significant CNVs identified in either tumor. No high‐level gene amplification events were found in any
tumor. Conclusion: HCN-NOS showed frequent and more complex CNVs than HB. Chromosome 1q gain was predominant in both groups but appeared to be more common in the HCN-NOS group. Loss of chromosomes 3, 9 and Y, as well as CN-LOH in 17p were seen exclusively in the HCN-NOS group.
18 Clinicopathologic study of hepatic adenomas: A Children's Hospital Experience. Y Estrella, N Cortes-Santiago, M Blessing, K Patel Texas Children's Hospital, Houston, Texas Background: To study clinicopathologic features of hepatic adenomas in children; including background liver, and identify differences, if any, from adult population. Methods: Pathology database was queried to identify all cases of hepatic adenomas from 2003 to 2021. Medical records and archived pathology material was reviewed in a retrospective manner. Results: Of the 22 patients identified, 12 were females with median age at diagnosis 12 years (1.5 to 21 yrs). Background liver showed: cirrhosis (6), steatosis (4), NRH (1), hepatoblastoma (2), sickle cell disease (3), post chemotherapy for hepatic angiosarcoma (1), and normal (4). Cirrhosis was secondary to congenital hepatic fibrosis (1), cryptogenic (1), biliary atresia (1), alpha1-anti trypsin deficiency (1), FXR deficiency (1), and sclerosing cholangitis (1). Hepatic steatosis with or without obesity was limited to females. History of prednisone was noted in 8 patients (5F:3M) and oral contraceptive pills in 2 females of whom 1 was transitioning to male with subsequent exposure to androgens. Ten patients had multiple lesions on imaging of whom 5 underwent transplantation, 1 right hepatectomy and 4 are under observation with or without growth in mass. Six out of 8 patients with a solitary lesion underwent partial resection, 1 transplantation and 1 is under follow up. Four patients had no mass on imaging and adenoma was diagnosed incidentally in 3 from the cirrhotic explanted liver. Vast majority (16/22, 72.7%) of adenomas were composed of large, pale, vacuolated and variably steatotic hepatocytes with loss of LFABP expression in 7 out of 9 cases studied and HNF1alpha mutation in 2 out of 4 cases tested. Of the 6 non-steatotic lesions, peliosis was a dominant feature in 4 (2 showing dilated sinusoids engorged with sickled cells), and cholestasis in 2. Lesional inflammation was predominantly lymphocytic, mild and limited to the stroma around the unpaired vessels. All were negative for glutamine synthetase and GPC-3 expression. Only one adenoma occurring in a FAP patient had nuclear reactivity for beta catenin, the rest were membranous. CD34 was largely perivascular (86.6%) and rarely diffuse (13.3%). None showed significant cytologic atypia. Three patients were lost to follow up, one was deceased (graft dysfunction); none showed recurrence of adenoma. Conclusion: In contrast to adults, vast majority of pediatric hepatic adenomas occur in cirrhotic or abnormal livers (~82%). Outside of cirrhosis, hepatic steatosis seems to be a predisposing factor in females. Adenomas were frequently steatotic with loss of LFABP expression that did not necessarily correlate with HNF1alpha mutation on few samples that were tested. Long term clinical outcome is dependent on patients’ underlying medical condition with no recurrence of adenoma in our series.
19 Histologic Characterization of Pediatric Mesenchymal Neoplasms with Kinase Alterations Treated with Targeted Therapy E Baranov1, J Davis2, K Winsnes2, M Breen1, K Janeway3, S DuBois3, A Church1, A Al-ibraheemi1 1 Boston Children's Hospital, Nahant; 2Oregon Health & Science University, Portland, Oregon; 3Dana- Farber/Boston Children's Cancer and Blood Disorders Center, Boston, Massachusetts Background: Recurrent alterations involving receptor tyrosine or cytoplasmic kinase genes have been described in soft tissue neoplasms such as infantile fibrosarcoma (IFS) and inflammatory myofibroblastic tumors (IMT). Recent trials and regulatory approvals for targeted inhibitors against the kinase domains of these oncoproteins have allowed for increased use of targeted therapies in these patients. We aim to characterize the histologic features of pediatric mesenchymal neoplasms with kinase alterations treated by targeted inhibition. Methods: Eight children with tyrosine kinase-altered mesenchymal neoplasms with pre- and post- treatment material were identified. Clinical, radiologic, and molecular information was collected and a detailed histologic review was performed Results: Tumors occurred in 5 females and 3 males with a median age at presentation of 6.5 years (range 0-15 years). Median radiologic tumor size at presentation was 7.5 cm (range 4.2 – 15.7 cm). Tumor sites included somatic soft tissue (n=5) and viscera (n=3). Pre-treatment diagnoses were: IMT (n=3), epithelioid inflammatory myofibroblastic sarcoma (n=1), and descriptive diagnoses (n=4) such as “kinase-driven spindle cell tumor”. Fusions identified were ETV6-NTRK3 (n=2), TPM3-NTRK1, SEPT7- BRAF, TFG-ROS1, KLC1-ALK, RANBP2-ALK, and MAP4-RAF1. Patients were treated with larotrectinib (n=3), ALK inhibitors (n=3), and MEK inhibitors (n=2) prior to resection/biopsy. Duration of treatment prior to biopsy/resection ranged from 5-24 months (median 9 months). Pre-treated tumors were moderately to markedly cellular, and composed of spindled to plump ovoid cells in a variably myxoid to collagenous stroma. Inflammation was marked in half of cases. In contrast, post-treatment tumors exhibited marked decrease in cellularity (7/8), collagenous stroma (7/8) with extensive glassy hyalinization (5/8). Necrosis and mitoses were largely absent (7/8). In 2 cases, abundant coarse or psammomatous calcifications were seen and in one case prominent perivascular hyalinization was noted. Inflammation was typically sparse. Residual viable tumor was seen in 3/8 cases (75% in 2/8 cases) Conclusion: Mesenchymal neoplasms with tyrosine kinase alterations treated with kinase inhibitors show a constellation of histologic features markedly different from the original pre-treatment tumors. These features include significantly decreased cellularity, collagenous or fibrous stroma (often with extensive glassy hyalinization), absent mitotic figures, occasionally prominent stromal calcifications and sparse to moderate lymphoplasmacytic inflammation. Presence of these histologic features may be helpful in assessing tumor response after treatment with kinase inhibitors
20 FGFR1-rearrangements in pediatric spindle cell tumors A Al-Ibraheemi1, L Wang2, D Parham2, C Beadling3, C Lockwood4, E Rudzinski5, J Davis3 1 Boston Children's Hospital, Boston, Massachusetts; 2Children's Hospital Los Angeles, Los Angeles, California; 3Oregon Health & Science University, Portland, Oregon; 4University of Washington Medical Center, Seattle, Washington; 5Seattle Children's Hospital, Seattle, Washington Background: Recurrent genetic alterations in kinases within the MAP kinase pathway are described in infantile fibrosarcoma (IFS)/cellular congenital mesoblastic nephroma (cCMN) and the group of spindle cell tumors provisionally designated “NTRK-rearranged” spindle cell tumors. These tumors demonstrate overlapping morphologies, immunophenotype, and spectrum of kinase alterations including in NTRK1/2/3, RET, MET, ABL1, ALK, RAF1, and BRAF. The relationship between IFS/cCMN and the provisional entity is not fully elucidated. To-date, one case in an adult patient with a uterine fibrosarcoma-like tumor (placed in the category of "NTRK rearranged" spindle cell tumor) has been reported to harbor an activating FGFR1 gene fusion. Herein we describe 2 pediatric patients with IFS-like tumors, both harboring FGFR1 gene fusions. Methods: Two FGFR1-rearranged pediatric mesenchymal neoplasms were identified; 1 as part of a prior research study on NTRK tumors and 1 through routine clinical practice. Clinicopathologic features were assessed. Both underwent partner agnostic targeted NGS on clinically validated platforms. Results: Patient 1 was an infant female who presented at 3 months with a 4.2 cm perirectal soft tissue tumor. The tumor was biopsied and then resected via proctectomy. The diagnosis was that of a low-grade spindle cell neoplasm, with a variant of infantile fibrosarcoma favored. The resection had negative margins and no further therapy was pursued. At 5 years of follow-up, the patient was alive with no evidence of disease. As part of a separate study, NGS was performed showing a FGFR1-PARD68 fusion. Patient 2 was an infant male who presented at 9 months with a 7.5 cm intrapelvic to thigh soft tissue tumor. The tumor was biopsied and diagnosed as spindle and round cell neoplasm with FGFR1- EBF2 gene fusion. The patient was started on lenvatinib therapy (multi-tyrosine kinase inhibitor with activity against FGFR1). The patient is now 3 months into therapy with stable disease. Morphology of both cases were similar, including intratumoral heterogeneity, variable cellularity with spindled to ovoid cells embedded in a spectrum of minimal to robust collagenized stroma and focal areas of myxoid change. Both showed strong, patchy staining of CD34; no expression of S100 or other immunomarkers was present. Conclusion: We present the first series of FGFR1-rearrangements in IFS-like pediatric tumors, including a patient treated with lenvatinib therapy. Our series expands the spectrum of kinase drivers within IFS-like tumors and reinforces the compelling overlap between IFS/cCMN-like tumors and the provisional entity of “NTRK-rearranged spindle cell tumors.” Knowledge of potential genetic alterations in this spectrum of tumors is a key for diagnostic and targeted therapeutic purposes.
21 Spatial Gene Expression in Childhood Ependymoma Reveals Tumor Cell Subpopulations and Their Locations In Situ N Willard1, A Griesinger2, R Fu2, K Riemondy2, J Hesselberth2, G Norris1, V Amani2, F Harris2, E Grimaldo2, N Foreman1, A Donson1 1 Children's Hospital Colorado, Aurora, Colorado; 2University of Colorado, Aurora, Colorado Background: Ependymoma (EPN) is an aggressive childhood CNS tumor with high recurrence rates. Posterior fossa (PF) EPN is divided into two molecular subgroups, Group A (PFA) and Group B (PFB). PFA, particularly relapsed PFA, is fatal with limited treatment options. Thus, there is a need to better understand PFA biology. While single cell RNA sequencing (scRNAseq) has defined tumor cell subpopulations within PFA EPN, it does not provide any architectural expression data. Though immunohistochemistry (IHC) can help, it is a piecemeal approach. Here, we us spatial transcriptomics to overcome this. Methods: Frozen tissue from 10 PFA EPN was embedded, sectioned, and permeabilized on a Visium slide (10x Genomics) containing 5000 RNA capture spots. Barcoded libraries were generated for each spot and sequenced (Illumina HiSeq6000). Data was deconvoluted, aligned to the genome, and analyzed to identify clusters of transcriptionally-related spots. Expression data was superimposed onto H&E using Loupe Browser. Analysis packages were applied to detect lineage trajectories (Slingshot) and cell-cell crosstalk based on ligand-receptor pair expression (CellChatDB). Results: Mapping of transcripts to PFA histology robustly detects tumor subpopulations identified by scRNAseq. Tumors consist largely of transportive cells (TEC), ciliated cells (CEC) restricted to rosettes, and mesenchymal cells (MEC) in perinecrotic zones. Further localization was observed, such as ciliation, a function of differentiation, being a feature of hypocellular regions. Because this technique allows analysis of gene expression at a light microscopy level, we examined mitotic genes in subpopulations, revealing that mitotically active cells were restricted to the TEC subpopulation. This novel finding impacts our understanding of the lineage trajectory and identifies potentially relevant tumor progenitors. To this end we have refined lineage trajectories to include the physical proximity of cells, showing concordance of trajectories with transitioning of cell types across the tumor from areas of TEC to CEC and MEC cells. These data can also be used to refine ligand-receptor pair analyses by factoring in the proximity of ligand-receptor pairs, and was used to identify discrete cell-cell signaling pathways in TEC and MEC zones. Conclusion: This transformative technology enables gene expression analysis at a histologic level. We can map subpopulations identified by scRNAseq to tumor architecture more definitively and rapidly than IHC. We demonstrate that bioinformatic approaches to detect cell lineage trajectories and cellular crosstalk in scRNAseq can be refined with spatial transcriptomic data. These novel insights advance our understanding of PFA EPN, a critical step in improving treatment options for children with this disease.
You can also read

















































